 Wenwen Yin1†Yuli Pan2†Linhua Zhou1†
Wenwen Yin1†Yuli Pan2†Linhua Zhou1† Qiaoyue Wei1Shengjie Zhang3Hong Hu4Qinghong Lin1Shuibo Pan1Chenyangzi Dai1
Qiaoyue Wei1Shengjie Zhang3Hong Hu4Qinghong Lin1Shuibo Pan1Chenyangzi Dai1 Junduan Wu1,5*
Junduan Wu1,5*- 1Department of Psychology, School of Public Health, Guangxi Medical University, Nanning, China
- 2Department of Guangxi Zhuang Autonomous Region Center for Disease Control and Prevention, Nanning, China
- 3Department of Graduate Management, Guangxi Medical University Cancer Hospital, Nanning, China
- 4Department of Medical Institution, Guangxi Nanning Fifth People's Hospital, Nanning, China
- 5Department of School of Public Health, Guangxi Medical College, Nanning, China
Background: Not all adolescents who have endured childhood trauma will develop depressive symptom, nor will they all experience the same level of depressive symptom. According to previous research, cognitive emotion regulation strategies may explain a portion of the variance. Observe the connection between childhood trauma and depressive symptom and investigate whether cognitive emotion regulation strategies mediate or moderate this association.
Methods: In October 2019, a cross-sectional study measuring childhood trauma, cognitive emotion regulation strategies, and depressive symptom among Zhuang adolescents was done in one senior high school and two junior highs in Chongzuo, Guangxi, China, using a self-report questionnaire. To examine the hypothesis of mediating and moderating effects, SPSS PROCESS was utilized.
Results: In this study, there was a positive relationship between childhood trauma and depressive symptom, whereas there were positive correlations between expressive suppression and childhood trauma and depressive symptom (r = 0.380, 0.246, and 0.089, respectively, p < 0.01). The 5,000-sample bootstrap procedure revealed that the indirect relationship between the independent variable (childhood trauma or emotional abuse) and the dependent variable (depressive symptom) was statistically significant (β = 0.0154 95% CI: 0.0019, 0.0165, β = 0.0442 95% CI: 0.0008, 0.0117). The statistical significance of the interaction effect enhanced the R-square value of the moderating effect when the independent variable was the total childhood trauma score (ΔR2 = 0.0044, 0.0089).
Conclusions: Our findings corroborated the conclusion of prior research that cognitive emotion regulation strategies mediate and moderate the development of depressive symptom. Although we demonstrate that cognitive emotion regulation strategies play a mediating and moderating role in the relationships between childhood trauma and depressive symptom, the mediating effects on the relationships between the other types of childhood traumas, including physical abuse and neglect, sexual abuse, emotional neglect, and depressive symptom, did not emerge.
Introduction
According to the World Health Organization (WHO), over a third of the global population has suffered childhood trauma. An estimated one-fifth of women and one-thirteenth of males have experienced sexual abuse in childhood, while around one-quarter of adults have experienced physical abuse in childhood (1). Additionally, 28.9 % of individuals with mental disorders reported having experienced childhood trauma, and the repercussions of early trauma may last a lifetime. As demonstrated by numerous earlier studies, childhood trauma was considered a particularly substantial risk factor for the onset, symptomatology, and course of depressive symptom (2, 3). As a major psychiatric disorder, depression poses a formidable public health concern. Around the world, 264 million people of all ages suffered from depression (4), with adolescents being particularly at risk (5). As a subclinical stage of depression, depressive symptom has garnered great attention due to their ubiquity. According to the Global School-based Student Health Survey (GSHS), 28.7 % of 67,077 teenagers exhibited depression symptom (6). Multiple areas' research conducted in China revealed that 20.3% of adolescents experienced depressive symptom (7). Therefore, in order to investigate the pathogenesis, prevention, and treatment of adolescent depression, it is vitally important to examine depressive symptom. A significant correlation exists between childhood trauma and adolescent depressive symptom, and adolescents who have suffered childhood trauma are more likely to develop depressive symptom than those who have not (8). The concept that childhood trauma is connected with the emergence and recurrence of depressive symptom is supported by abundant research (9). The study of the genesis of depressive symptom revealed that persons who suffer negative life occurrences are susceptible to depressive symptom (10). When confronted with the same condition, however, individuals react differently: some suffer depressive symptom, while others do not. This phenomenon enlightens individuals about the fact that certain variables determine stress situations that lead to depressive symptom. According to studies, depressive symptom may develop due to acute or chronic life stress, particularly in individuals who have undergone childhood trauma (11).
However, Insufficient research has been conducted on the causative mechanisms between childhood trauma and the eventual development of depressive symptom. In a large number of extant studies on childhood trauma and depressive symptom, the variables that influence the link between childhood trauma and depressive symptom can be categorized into two major groups: psychosocial and neurobiological. Psychosocial aspects include cognitive elements (12, 13), emotion regulation components (14) and personality factors (15). Furthermore, diverse putative mediators of the association between childhood trauma and depressive symptom have been identified, but elucidating research remains scant. A mediator variable in a mediation model can be used to further explain the relationship between a predictor variable and an outcome variable (16). The literature has so far identified a number of putative mediators of the link between childhood trauma as a youngster and depressive symptom. In a nationally representative epidemiological investigation, self-criticism was discovered to be a mediator of the relationship between parental verbal abuse and internalizing symptom (depressive symptom and anxiety) in adulthood (17). Additionally, it has been discovered that patterns of vulnerability to harm, shame, and self-sacrifice modulate the impact of emotional abuse on anxiety and depressive symptom that develop later in teenagers (18).
The inadequate development of effective cognitive emotion control techniques after childhood maltreatment may be another important factor linking childhood trauma to depression in adults (19). Cognitive emotion regulation strategies are the cognitive response of an individual attempting to control the quantity and kind of their own emotional experience and the event itself in response to an emotion-eliciting stimulus (20). Gross and John identified cognitive reappraisal and expressive suppression as the two fundamental mechanisms for emotion regulation (21). Furthermore, cognitive reappraisal is an antecedent-focused strategy that refers to analyzing emotionally arousing situations to modify their emotional impact, whereas expression suppression is a response-oriented strategy that involves suppressing an individual's outward displays of emotional state. Cognitive reappraisal was associated with better emotions and enhanced functioning, whereas expressive suppression was linked to negative emotions and decreased functioning. A meta-analysis of emotion regulation strategies reveals that emotion-related disorders are more strongly associated with emotion regulation strategies than other problems, and maladaptive strategies are more consistently associated with psychopathology than adaptive ones (22). Furthermore, psychological issues have been demonstrated to be closely connected with emotion regulation strategies (23). In addition, early negative experiences may contribute to the creation of latent sad cognitive schema, which influences the emotions, behaviors, and ideas of depressive symptom patients (24). For example, physical abuse during childhood is associated with schemas of danger and mistrust, while emotional neglect is associated with schemas of value and belonging (25, 26). Individuals who experience childhood trauma usually struggle to interpret their feelings due to a lack of sufficient environmental feedback. Therefore, they employ avoidance and reflection as coping mechanisms, which might easily result in negative adaptation (27). The ability to use emotion regulation strategies is developed early in life, and some studies suggest that exposure to maltreatment as a youngster may have a negative impact on that child's subsequent ability to use emotion regulation strategies (28, 29). Additionally, it has been demonstrated that a number of mental health problems are linked to deficiencies in emotion regulation (30, 31). In summary, traumas in childhood may impact depressive symptom through cognitive emotion regulation strategies. Existing research has also investigated the role of cognitive emotion regulation as a mediator between later mental health disorders and childhood trauma (32, 33).
In this study, the Childhood Trauma Questionnaire-Short Form (CTQ-SF), the Emotional Regulation Questionnaire (ERQ), and the Patient Health Questionnaire-9 (PHQ-9) were used to examine the childhood trauma, cognitive emotion regulation mechanisms, and depressive symptom of teenagers individually. Compared to earlier investigation on mediation analysis of cognitive emotion regulation strategies, in which they are derived for these two regulation strategies (34), We measured the Zhuang adolescents' experiences of childhood trauma using the widely established CTQ-SF scale; another research utilized the CTQ scale but evaluated it exclusively from the standpoint of emotional and physical abuse (35). Moreover, little research has sought to simultaneously analyze cognitive emotion regulation strategies' mediating and moderating effects on the relationship between depressive symptom and childhood trauma in Chinese Zhuang adolescents. However, there is a paucity of comparative studies on Chinese ethnic minorities. Previous research has shown that young Zhuang people, as an ethnic minority, encounter greater obstacles than their Chinese peers due to their different language and lower levels of education, income, and professional opportunities (36, 37). These challenges may place Zhuang children at a substantial mental health disadvantage (38). In summary, this study used Zhuang adolescents as participants to analyze the connection between childhood trauma and depressive symptom and to determine whether cognitive emotion regulation strategies mediate and moderate this connection.
Measurements and methods
Participants
In October 2019, a cross-sectional study was undertaken using stratified cluster sampling at three schools (one senior high school and two junior highs) in Chongzuo, Guangxi, China. First, we randomly chose three campuses in Chongzuo, Guangxi. Second, ten classes were selected at random from the class roster. Thirdly, we invited all middle youngsters to complete questionnaire and collected them throughout the class. The questionnaire has a 60-min deadline for completion. Before providing informed consent and completing the questionnaire, all participants were informed about potential hazards and the complete confidentiality of information. Then, 1,494 questionnaires were returned, excluding those who declined to participate in the research. Due to insufficient data and logical errors in the survey, 362 questionnaires were excluded from the final analysis, leaving 1,132 questionnaires for analysis. Participants needed to be between 12 and 18 years old and of Zhuang descent to be included in the study. Additionally, the questionnaire was input using a response sheet and machine-readable card, which is accurate and efficient. The Institutional Ethical Committee authorized the research conducted at Guangxi Medical University (Approval Number: 20160302-13).
Measurements
Participants' general information
Participants' basic demographic information was gathered, including age, gender, parental marital status, place of residence, resident student, only child, parental absence, teacher criticism, and study stress.
Childhood trauma
The Childhood Trauma Questionnaire Short-Form (CTQ-SF) was utilized to evaluate childhood trauma (39), a 28-item self-report questionnaire examining five varieties of traumas a child or adolescent has experienced: emotional and physical neglect; emotional, physical and sexual abuse. A 5-point frequency scale is used to grade items (1 = never true to 5 = very often true), with the total score for each type of trauma ranging from 5 to 25, with higher scores indicating more severity. Additionally, the Chinese version of the CTQ-SF has been confirmed (40). Moreover, in this study, Cronbach's alpha coefficient for the CTQ-SF was 0.737.
Emotional regulation questionnaire
The ERQ is a 10-item self-report instrument based on the process model of emotion regulation created by Gross (1998) (41). This model categorizes emotion regulation strategies based on how early they are triggered in the process of emotion creation and hypothesizes that different regulation strategies may have distinct outcomes. The ERQ is designed to examine the use of two regulation mechanisms by individuals: an antecedent-focused strategy called cognitive reappraisal (six items; e.g., “When I am faced with a stressful situation, I make myself think about it in a way that helps me stay calm”) where a person attempts to alter his or her perception of a circumstance in order to alter its emotional impact, and a response-focused strategy called expressive suppression (four items; e.g., “I keep my emotions to myself”) where an individual attempts to suppress the behavioral expression of their feelings (21). These two regulatory strategies are assigned distinct scale scores. Each item is graded on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores indicating greater utilization of the method. In addition, Cronbach's alpha coefficient for the ERQ was 0.845.
Patient health questionnaire-9 items
This study utilized the patient health questionnaire-9 (PHQ-9) (42). The PHQ-9 was designed using the DSM-IV diagnostic criteria for depressive symptom. Participants evaluated their level of irritation with each item on a four-point Likert scale ranging from 0 (“not at all”) to 3. (“nearly every day”). Our recall period was 2 weeks. The overall score ranged from 0 to 27, with higher scores indicating greater depressive symptom severity as indicated by the individual. With a sensitivity of 80% and specificity of 92%, a total score of ≥ 10 predicted the possibility of severe depressive symptom (43, 44). Previously, psychometric characteristics of the PHQ-9 were validated in the Chinese population (42). In addition, Cronbach's alpha coefficient for the PHQ-9 was 0.878.
Statistical analysis
The variables were subjected to descriptive and correlational statistical analyses using IBM SPSS version 25. The SPSS PROCESS macro was employed to examine the mediating and moderating effects hypotheses following Hayes' recommendations. The bootstrap procedure, thought to be the most precise by Hayes et al. was used to estimate the mediating effect of expressive suppression. The independent variable's direct impact on the mediator, including three direct effects and its total effect, the independent variable's direct effect on the dependent variable, the mediator's direct effect on the dependent variable, and the total effect of the independent variable on the dependent variable was evaluated, automatically. Whether the independent variable has a considerable impact on the dependent variable when the mediating effect has a significant impact determines whether there has been full or partial mediation. The moderator effect, the moderator's influence on the dependent variable, and the interaction effect on the dependent variable must all be statistically significant to test for a moderating effect. The statistical test was significant at the level of P < 0.05, according to the significance level.
Results
Participants' characteristics
The average age of 1,132 middle school students in this sample was 14.66 ± 1.441; 49.4% of the students were males, 73.4% were rural residents, and 12.6% were in the unstable marital status of parents, 21.6 % were the only child in their families, and 36.7% were parental absence. 9.3% of the students were never criticized by teacher, and most adolescents had the frequency of “teacher's criticism” sometimes. Furthermore, 91.3% of the students had study stress. The mean score of types of childhood trauma was 5.48–10.97. The mean score of CTQ-SF (Childhood trauma) was 28.4 ± 9.2; the expressive suppression score (Cognitive emotion regulation strategy), cognitive reappraisal score (Cognitive emotion regulation strategy), and the PHQ-9 score (Depressive symptom) is also shown in Table 1.
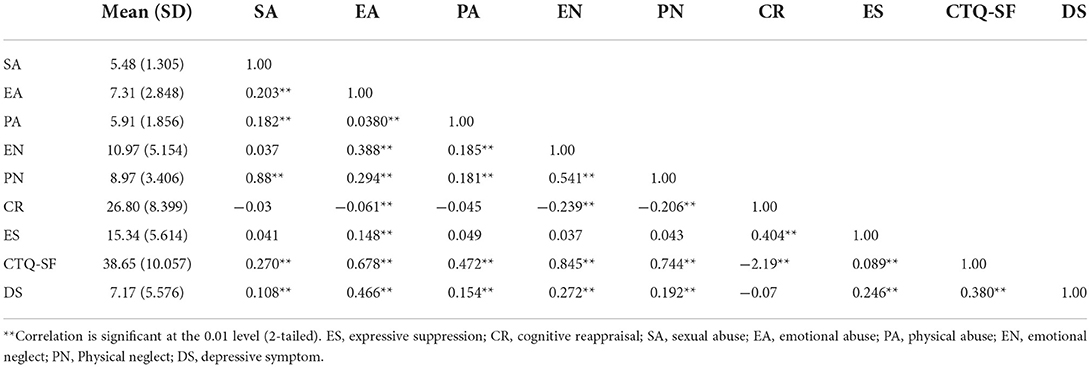
Table 1. Correlations of variable.
Correlation
Child trauma, the types of childhood trauma, emotion regulation (including expressive suppression and cognitive reappraisal), and depressive symptom were subjected to a bivariate Pearson correlation analysis; the correlation coefficients are shown in Table 1 below. Depressive symptom were favorably connected with childhood trauma, while expressive inhibition was positively associated with depressive symptom and childhood trauma (r = 0.380, 0.246, and 0.089, respectively, p < 0.01). Each type of childhood trauma had a positive connection with depressive symptom. Moreover, emotional abuse, a type of childhood trauma, was also positively related to depressive symptom, whereas expressive suppression was positively connected with depressive symptom and emotional abuse (r = 0.466, 0.246, and 0.148, respectively, p < 0.01). Additionally, cognitive reappraisal was negatively connected with childhood trauma, emotional abuse, and it was positively associated with expressive suppression (r = −2.19, −0.061 and 0.404, respectively, p < 0.01). The severity of childhood trauma correlates with the prevalence of expressive suppression and the risk of depressive symptom. Additionally, the same collection exists in emotional abuse. Consequently, the relation between cognitive reappraisal and depressive symptom had not statistically significant. (r = −0.07, p > 0.01), it was not included in the subsequent models. Furthermore, the relationship between other various childhood trauma, except for emotional abuse and expressive suppression, was not statistically significant. Hence, they were not included in the subsequent models.
Mediating and moderating effects of expressive suppression
The correlations among the three variables were statistically significant and satisfied the requirements for examining the mediating and moderating effects. The score on childhood trauma or emotional abuse was the independent variable, the score on depressive symptom was the dependent variable, and the score on expressive suppression was the mediator or moderator variable; The scores were input into model 1 or 4 of SPSS PROCESS, and the variables age, gender, marital status of parents, place of residence, resident student, only child, parental absence, teachers' criticism, study stress was input as covariates. The results of the mediating effect are shown in Table 2. The statistical significance of each impact demonstrated the existence of a mediating influence.
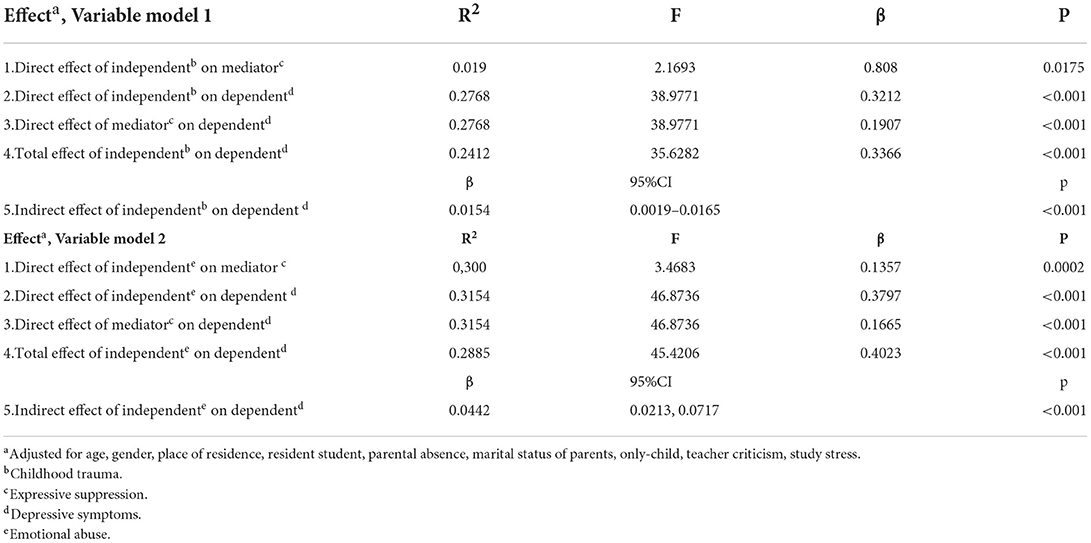
Table 2. Result from PROCESS macro testing expressive suppression mediation model 1 and model 2.
The bootstrap method with 5,000 samples revealed that the indirect influence of the independent variable (childhood trauma or emotional abuse) on the dependent variable (depressive symptom) was statistically significant (β = 0.0154 95% CI: 0.0019, 0.0165, β = 0.0442 95% CI: 0.0008, 0.0117). The ratio of the effect of mediation to the total effect was 45.75, or 10.98%. Figure 1 illustrates the mediating impact of expressive suppression. Childhood trauma increased the expressive suppression score, which in turn increased the depressive symptom score, hence increasing the risk of depressive symptom in adolescents. Emotional abuse has the same mechanism as Childhood trauma.
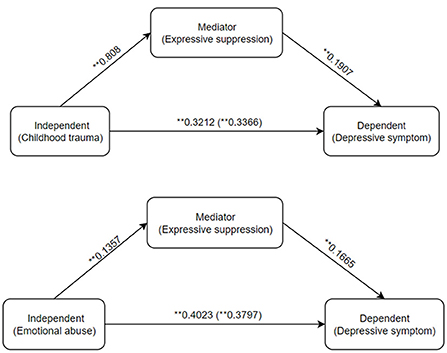
Figure 1. Output model of expressive suppression mediation. The ** symbol indicates the mediating effect is significant at the 0.01 level (2-tailed).
Table 3 show the results of the moderating effect. In Table 3, the R2 increased due to the statistical significance of the interaction effect (ΔR2 = 0.0044, p= 0.0089). The bootstrap analyses of 5,000 samples revealed that the interaction effect was likewise statistically significant (β = 0.063, 95% CI: 0.0008,0.0117). However, in Table 3, the interaction effect was not statistically significant, according to the 5,000-sample bootstrap procedure (β = 0.0011, 95% CI: −0.0071, 0.0311). With growth of one standard deviation in expressive suppression, the childhood trauma to depressive symptom slope increased by 0.0063 standard deviations. Accidentally, the moderating effect of expressive suppression between emotional abuse and depressive symptom makes no sense. Figure 2 illustrates the moderating effect of expressive suppression.
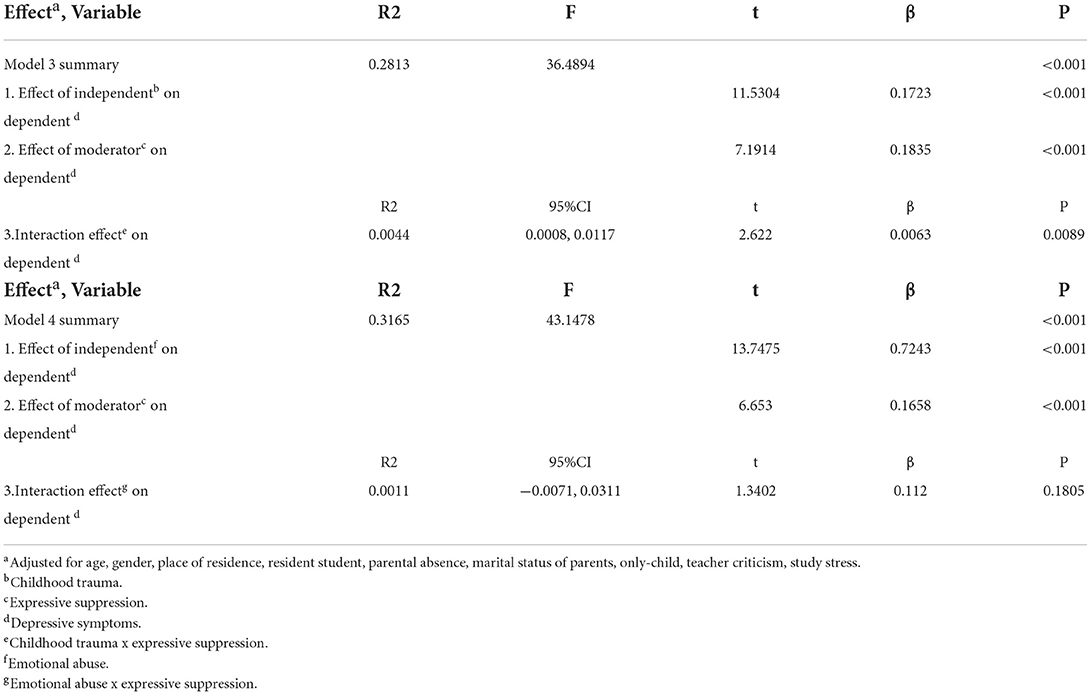
Table 3. Result from PROCESS macro testing expressive suppression moderation model 1 and model 2.
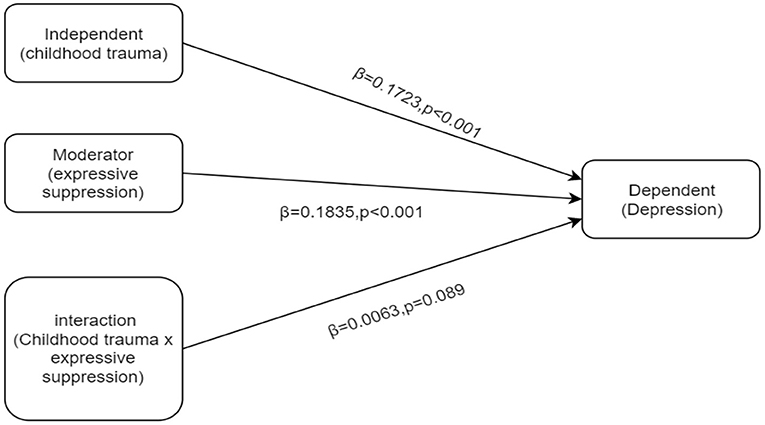
Figure 2. Output model of expressive suppression moderation.
Discussion
A noteworthy finding from our study was that childhood trauma, including neglect and abuse, emotion regulation, and depressive symptom, were all significantly associated among Zhuang teenagers who participated in this research. The score for childhood trauma was positively linked with the score for expressive suppression. Expressive suppression, that is, people occasionally control their emotions by preventing the behavioral expression of emotion after an emotional response has been generated (41); the depressive symptom score was positively correlated with the total childhood trauma score among Zhuang teenagers who participated in this study. A meta-analysis of 184 research revealed that childhood trauma is related to the incidence, onset, age, and duration of depressive symptom (10). Moreover, many individuals with dissociative depressive symptom reported early school dropout and sexual abuse in childhood (45). Our research revealed a correlation between a teenager's childhood trauma score and his or her depressive symptom score. Moreover, various childhood trauma both connect with depressive symptom. Moreover, a second meta-analysis revealed that distinct types of traumas in childhood have distinct consequences on depressive symptom (46). Since our study utilized the total childhood trauma score as the observation variable and simultaneously analyzed several types of traumas, the total childhood trauma score and emotion abuse score, respectively served as the observation variable. The cross-sectional study demonstrating a correlation between expressive suppression and depressive symptom in adults and adolescents (47) has often been interpreted as reflecting the impact of expressive suppression on depressive symptom. Concerning the effect of expressive suppression on depressive symptom, our study revealed a positive correlation between the expressive suppression score and the depressive symptom score. The current study provides more evidence in favor of our earlier research (48), suggesting a unidirectional association between depressive symptom and increased expressive suppression use.
Another result was that expressive suppression had to mediate and moderate effects on childhood trauma and depressive symptom. The findings demonstrated that childhood trauma positively predicted the Zhuang adolescents' expressive suppression and indirectly affected the Zhuang adolescents' depressive symptom through expressive suppression. However, for specific types of traumas, expressive suppression only had to mediate effects on emotional abuse and depressive symptom. Consistent with the hypothesis of ironic mental control processes (49), this study indicated that emotional maltreatment affected both depressive symptom and problem behaviors indirectly via expressive repression. In addition, the moderating effect demonstrated that expressive suppression amplified the effect of childhood trauma on the future development of depressive symptom (50–52). Consistent with earlier research, this study discovered that adolescents are particularly vulnerable to faulty emotion regulation, which may raise their risk for a psychiatric disorder (53). That is, expressive suppression, as a cognitive emotion regulation strategy, is harmful to human development (54). The passing of time cannot be reversed for adolescents but childhood traumas are irrevocable, although expressive repression can lessen their usage. For example, the preview study (55) indicated that expressive suppression had more depressive symptom, life satisfaction, greater self-esteem, and general well-being than cognitive reappraisal. Moreover, suppression of emotion suggests that the suppressed feeling continues to persist and build in an unresolved condition (21), and suppression efforts paradoxically make the target of suppression more accessible (49). This raises negative feelings but not behavioral issues, resulting in an increase in depressive symptom. According to these studies, individual differences in these two strategies may be linked to the development and maintenance of depressive disorders (56).
A study found an association between expressive suppression and unfavorable interpersonal outcomes, such as lower levels of liking, relationship satisfaction, and relationship quality (57). Through the adjustment of cognitive affective, individuals can improve their presentation and interpretation of events with the assistance of parental and peer support (58). As an essential factor influencing depressive symptom, expressive suppression can be practiced to limit its use with the assistance of family and friends, as well as cognitive intervention training. Therefore, reducing expressive suppression can be used as an intervention object and even as a treatment to lessen the risk of depressive symptom in Zhuang adolescents.
In summary, we investigated whether expressive suppression, as a cognitive emotion regulation approach, mediated and moderated the association between childhood trauma and increased risk of depressive symptom in a sample of Zhuang teenagers in China. Our findings validated prior findings that expressive suppression mediates and moderates the relationship between childhood trauma and depressive symptom. In addition, we elucidate the role of cognitive emotion regulation strategies in greater detail by examining various types of childhood trauma, and expressive suppression only had mediating effects on the connection between emotional abuse and higher risk of depressive symptom in this study.
Limitations and strengths
This study is restricted by its cross-sectional methodology, which prohibited the identification of a causal association between childhood trauma and depressive symptom. Additionally, the sample was not necessarily representative of all Zhuang adolescents. Additionally, because the sample was single, mediating effects on the relationship between the other types of childhood traumas: emotional neglect, physical abuse and neglect, sexual abuse and depressive symptom did not appear. Future studies need further validation and discussion. We studied a sample of more than one thousand people, and the response rate was high; this was a strength of the study, therefore, the conclusions we found can be considered reliable. Our study confirmed that cognitive emotion regulation strategies attenuate modest relationships between childhood trauma and depressive symptom, providing a great empirical endorsement for previous research.
Conclusions
This study's findings confirmed previous research indicating that the development of depressive symptom is mediated and moderated by the cognitive emotion management technique of expressive suppression. Inducing expressive repression can not only avoid depressive symptom among middle school adolescents but also enhance their future ability to overcome adversity. Although we demonstrate that cognitive emotion regulation strategies play a mediating and moderating role in the links between childhood trauma and depressive symptom, the mediating effects on the relationships between the other types of childhood traumas, including physical abuse and neglect, sexual abuse, emotional neglect, and depressive symptom, did not emerge.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
WY managed the literature search and analyses. YP, QW, and SZ designed the study and wrote the protocol. HH undertook the statistical analysis. LZ and WY wrote the first draft of the manuscript. QL, SP, and CD participated in data collection. JW participated in coaching as a leader. All authors contributed to and have approved the final manuscript.
Funding
This research was supported by the Chinese National Nature Science Foundation (No. 81660569). The funders played no role in the study design, data collection and analysis, publication decision, or manuscript preparation.
Acknowledgments
The authors are grateful to the Chinese National Nature Science Foundation for funding this study (No. 81660569).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kessler RC, McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, et al. Childhood adversities and adult psychopathology in the WHO world mental health surveys. Br J Psychiatry. (2010) 197:378–85. doi: 10.1192/bjp.bp.110.080499
2. Gibb BE, Chelminski I, Zimmerman M. Childhood emotional, physical, and sexual abuse, and diagnoses of depressive and anxiety disorders in adult psychiatric outpatients. Depress Anxiety. (2007) 24:256–63. doi: 10.1002/da.20238
3. Horan JM, Widom CS. Cumulative childhood risk and adult functioning in abused and neglected children grown up. Dev Psychopathol. (2015) 27:927–41. doi: 10.1017/S095457941400090X
4. GBD 2017 disease and injury incidence and prevalence collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
5. Haglund ME, aan het Rot M, Cooper NS, Nestadt PS, Muller D, Southwick SM, et al. Resilience in the third year of medical school: a prospective study of the associations between stressful events occurring during clinical rotations and student well-being. Acad Med. (2009) 84:258–68. doi: 10.1097/ACM.0b013e31819381b1
6. Vancampfort D, Stubbs B, Firth J, Van Damme T, Koyanagi A. Sedentary behavior and depressive symptoms among 67,077 Adolescents Aged 12-15 years from 30 low- and middle-income countries. Int J Behav Nutr Phys Act. (2018) 15:73. doi: 10.1186/s12966-018-0708-y
7. Zhou M, Zhang G, Rozelle S, Kenny K, Xue H. Depressive symptoms of Chinese children: prevalence and correlated factors among subgroups. Int J Environ Res Public Health. (2018) 15:283. doi: 10.3390/ijerph15020283
8. Infurna MR, Reichl C, Parzer P, Schimmenti A, Bifulco A, Kaess M. Associations between depression and specific childhood experiences of abuse and neglect: a meta-analysis. J Affect Disord. (2016) 190:47–55. doi: 10.1016/j.jad.2015.09.006
9. Lok A, Bockting CL, Koeter MW, Snieder H, Assies J, Mocking RJ, et al. Interaction between the Mthfr C677t polymorphism and traumatic childhood events predicts depression. Transl Psychiatry. (2013) 3:e288. doi: 10.1038/tp.2013.60
10. Nelson J, Klumparendt A, Doebler P, Ehring T. Childhood maltreatment and characteristics of adult depression: meta-analysis. Br J Psychiatry. (2017) 210:96–104. doi: 10.1192/bjp.bp.115.180752
11. Mandelli L, Petrelli C, Serretti A. The role of specific early trauma in adult depression: a meta-analysis of published literature. Childhood trauma and adult depression. Eur Psychiatry. (2015) 30:665–80. doi: 10.1016/j.eurpsy.2015.04.007
12. Lara ME, Klein DN. Psychosocial processes underlying the maintenance and persistence of depression: implications for understanding chronic depression. Clin Psychol Rev. (1999) 19:553–70. doi: 10.1016/S0272-7358(98)00066-X
13. Rose DT, Abramson LY. Developmental predictors of depressive cognitive style: research and theory. In: Cicchetti D, Toth SL, editors. Developmental Perspectives on Depression. University of Rochester Press (1992). p. (323–49).
14. Hopfinger L, Berking M, Bockting CL, Ebert DD. Emotion regulation mediates the effect of childhood trauma on depression. J Affect Disord. (2016) 198:189–97. doi: 10.1016/j.jad.2016.03.050
15. Gui-ying Y, Ai-ling D, Shi-chang Y, Dong-jun Z, Hong-li G, Ren-e M. et al. Mediating effects of personality on the relationship between childhood psychological abuse and depression of undergraduates Chinese. J Clin Psychol. (2019) 19:70–2.
17. Sachs-Ericsson N, Verona E, Joiner T, Preacher KJ. Parental verbal abuse and the mediating role of self-criticism in adult internalizing disorders. J Affect Disord. (2006) 93:71–8. doi: 10.1016/j.jad.2006.02.014
18. Wright MO, Crawford E, Del Castillo D. Childhood emotional maltreatment and later psychological distress among college students: the mediating role of maladaptive schemas. Child Abuse Negl. (2009) 33:59–68. doi: 10.1016/j.chiabu.2008.12.007
19. Crow T, Cross D, Powers A, Bradley B. Emotion dysregulation as a mediator between childhood emotional abuse and current depression in a low-income African-American sample. Child Abuse Negl. (2014) 38:1590–8. doi: 10.1016/j.chiabu.2014.05.015
20. Aldao A, Nolen-Hoeksema S. Specificity of cognitive emotion regulation strategies: a transdiagnostic examination. Behav Res Ther. (2010) 48:974–83. doi: 10.1016/j.brat.2010.06.002
21. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. (2003) 85:348–62. doi: 10.1037/0022-3514.85.2.348
22. Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev. (2010) 30:217–37. doi: 10.1016/j.cpr.2009.11.004
23. Buhle JT, Silvers JA, Wager TD, Lopez R, Onyemekwu C, Kober H, et al. Cognitive reappraisal of emotion: a meta-analysis of human neuroimaging studies. Cereb Cortex. (2014) 24:2981–90. doi: 10.1093/cercor/bht154
24. Parker G, Gladstone G, Mitchell P, Wilhelm K, Roy K. Do early adverse experiences establish a cognitive vulnerability to depression on exposure to mirroring life events in adulthood? J Affect Disord. (2000) 57:209–15. doi: 10.1016/S0165-0327(99)00091-9
25. Schulz P, Beblo T, Ribbert H, Kater L, Spannhorst S, Driessen M, et al. How is childhood emotional abuse related to major depression in adulthood? The role of personality and emotion acceptance Child Abuse Negl. (2017) 72:98–109. doi: 10.1016/j.chiabu.2017.07.022
26. Akbaba Turkoglu S, Essizoglu A, Kosger F, Aksaray G. Relationship between dysfunctional attitudes and childhood traumas in women with depression. Int J Soc Psychiatry. (2015) 61:796–801. doi: 10.1177/0020764015585328
27. Grant KE, Lyons AL, Finkelstein J-AS, Conway KM, Reynolds LK, O'Koon JH, et al. Gender differences in rates of depressive symptoms among Low-Income, Urban, African American youth: a test of two mediational hypotheses. J Youth Adolesc. (2004) 33:523–33. doi: 10.1023/B:JOYO.0000048066.90949.be
28. Alink LR, Cicchetti D, Kim J, Rogosch FA. Mediating and moderating processes in the relation between maltreatment and psychopathology: mother-child relationship quality and emotion regulation. J Abnorm Child Psychol. (2009) 37:831–43. doi: 10.1007/s10802-009-9314-4
29. Burns E, Jackson J, Harding H. Child maltreatment, emotion regulation, and posttraumatic stress: the impact of emotional abuse. J Aggress Maltreat Trauma. (2010) 19:801–19. doi: 10.1080/10926771.2010.522947
30. Berking M, Wupperman P. Emotion regulation and mental health: recent findings, current challenges, and future directions. Curr Opin Psychiatry. (2012) 25:128–34. doi: 10.1097/YCO.0b013e3283503669
31. Burns EE, Fischer S, Jackson JL, Harding HG. Deficits in emotion regulation mediate the relationship between childhood abuse and later eating disorder symptoms. Child Abuse Negl. (2012) 36:32–9. doi: 10.1016/j.chiabu.2011.08.005
32. Huh HJ, Kim KH, Lee HK, Chae JH. The relationship between childhood trauma and the severity of adulthood depression and anxiety symptoms in a clinical sample: the mediating role of cognitive emotion regulation strategies. J Affect Disord. (2017) 213:44–50. doi: 10.1016/j.jad.2017.02.009
33. Zhang F, Liu N, Huang C, Kang Y, Zhang B, Sun Z, et al. The relationship between childhood trauma and adult depression: the mediating role of adaptive and maladaptive emotion regulation strategies. Asian J Psychiatr. (2020) 48:101911. doi: 10.1016/j.ajp.2019.101911
34. Chu Q, Wang X, Yao R, Fan J, Li Y, Nie F, et al. Childhood trauma and current depression among Chinese university students: a moderated mediation model of cognitive emotion regulation strategies and neuroticism. BMC Psychiatry. (2022) 22:90. doi: 10.1186/s12888-021-03673-6
35. Zhou X, Zhen R. How do physical and emotional abuse affect depression and problematic behaviors in adolescents? The roles of emotional regulation and anger. Child Abuse Negl. (2022) 129:105641. doi: 10.1016/j.chiabu.2022.105641
36. Li L, Chen X, Wu D, Li H. Effects of attending preschool on adolescents' reading literacy: evidence from the ethnic minority children in China. Child Youth Serv Rev. (2020) 116:105211. doi: 10.1016/j.childyouth.2020.105211
37. Grey A. A polity study of minority language management in China focusing on Zhuang. Curr Issues Lang Plan. (2018) 20:1–60. doi: 10.1080/14664208.2018.1502513
38. Li L, Liu Y, Peng Z, Liao M, Lu L, Liao H, et al. Peer relationships, motivation, self-efficacy, and science literacy in ethnic minority adolescents in China: a moderated mediation model. Child Youth Serv Rev. (2020) 119:105524. doi: 10.1016/j.childyouth.2020.105524
39. Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, et al. Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse Negl. (2003) 27:169–90. doi: 10.1016/S0145-2134(02)00541-0
40. Min Z. Reliablity and validity of the Chinese version of Ctq-Sf. Chin J Public Health. (2011) 27:147–8. doi: 10.11847/zgggws-2011-27-05-71
41. Gross JJ. Antecedent- and response-focused emotion regulation: divergent consequences for experience, expression, and physiology. J Pers Soc Psychol. (1998) 74:224–37. doi: 10.1037/0022-3514.74.1.224
42. Yu X, Tam WW, Wong PT, Lam TH, Stewart SM. The patient health questionnaire-9 for measuring depressive symptoms among the general population in Hong Kong. Compr Psychiatry. (2012) 53:95–102. doi: 10.1016/j.comppsych.2010.11.002
43. Chin WY, Chan KT, Lam CL, Wong SY, Fong DY, Lo YY, et al. Detection and management of depression in adult primary care patients in hong kong: a cross-sectional survey conducted by a primary care practice-based research network. BMC Fam Pract. (2014) 15:30. doi: 10.1186/1471-2296-15-30
44. Manea L, Gilbody S, McMillan D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (Phq-9): a meta-analysis. CMAJ. (2012) 184:E191–6. doi: 10.1503/cmaj.110829
45. Sar V, Akyüz G, Oztürk E, Alioglu F. Dissociative depression among women in the community. J Trauma Dissociation. (2013) 14:423–38. doi: 10.1080/15299732.2012.753654
46. Song JM, Min JA, Huh HJ, Chae JH. Types of childhood trauma and spirituality in adult patients with depressive disorders. Compr Psychiatry. (2016) 69:11–9. doi: 10.1016/j.comppsych.2016.04.003
47. Betts J, Gullone E, Allen J. An examination of emotion regulation, temperament, and parenting style as potential predictors of adolescent depression risk status: a correlational study. Br J Dev Psychol. (2009) 27:473–85. doi: 10.1348/026151008X314900
48. Larsen J, Vermulst A, Geenen R, van Middendorp H, English T, Gross J, et al. Emotion regulation in adolescence: a prospective study of expressive suppression and depressive symptoms. J Early Adolesc. (2012) 33:184–200. doi: 10.1177/0272431611432712
49. Wegner DM. Ironic Processes of mental control. Psychol Rev. (1994) 101:34–52. doi: 10.1037/0033-295X.101.1.34
50. Garnefski N, Kraaij V, Spinhoven P. Negative life events, cognitive emotion regulation and emotional problems. Pers Individ Dif. (2001) 30:1311–27. doi: 10.1016/S0191-8869(00)00113-6
51. Weckbacher LE, Baker LR. Partners' depressive symptoms moderate the effects of expressive suppression. J Fam Psychol. (2018) 32:1120–9. doi: 10.1037/fam0000483
52. Lee M, Lee ES, Jun JY, Park S. The effect of early trauma on North Korean refugee youths' mental health: moderating effect of emotional regulation strategies. Psychiatry Res. (2020) 287:112707. doi: 10.1016/j.psychres.2019.112707
53. Gross JJ. Emotion regulation: taking stock and moving forward. Emotion. (2013) 13:359–65. doi: 10.1037/a0032135
54. Pechtel P, Pizzagalli DA. Effects of early life stress on cognitive and affective function: an integrated review of human literature. Psychopharmacology. (2011) 214:55–70. doi: 10.1007/s00213-010-2009-2
55. Stein JA, Leslie MB, Nyamathi A. Relative contributions of parent substance use and childhood maltreatment to chronic homelessness, depression, and substance abuse problems among homeless women: mediating roles of self-esteem and abuse in adulthood. Child Abuse Negl. (2002) 26:1011–27. doi: 10.1016/S0145-2134(02)00382-4
56. Cai RY, Richdale AL, Foley K-R, Trollor J, Uljarević M. Brief report: cross-sectional interactions between expressive suppression and cognitive reappraisal and its relationship with depressive symptoms in autism spectrum disorder. Res Autism Spectr Disord. (2018) 45:1–8. doi: 10.1016/j.rasd.2017.10.002
57. Chervonsky E, Hunt C. Suppression and expression of emotion in social and interpersonal outcomes: a meta-analysis. Emotion. (2017) 17:669–83. doi: 10.1037/emo0000270
58. Larsen JK, Vermulst AA, Eisinga R, English T, Gross JJ, Hofman E, et al. Social coping by masking? Parental support and peer victimization as mediators of the relationship between depressive symptoms and expressive suppression in adolescents. J Youth Adolesc. (2012) 41:1628–42. doi: 10.1007/s10964-012-9782-7
Keywords: childhood trauma, depression, expressive suppression, the Zhuang adolescents, emotional abuse in childhood
Citation: Yin W, Pan Y, Zhou L, Wei Q, Zhang S, Hu H, Lin Q, Pan S, Dai C and Wu J (2022) The relationship between childhood trauma and depressive symptom among Zhuang adolescents: Mediating and moderating effects of cognitive emotion regulation strategies. Front. Psychiatry 13:994065. doi: 10.3389/fpsyt.2022.994065
Received: 14 July 2022; Accepted: 15 August 2022;
Published: 06 September 2022.
Edited by:
Yuan Yuan Wang, De Montfort University, United KingdomReviewed by:
Hui Zhong, Anhui Mental Health Center, ChinaMengge Li, South China Normal University, China
Copyright © 2022 Yin, Pan, Zhou, Wei, Zhang, Hu, Lin, Pan, Dai and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junduan Wu, d3VqdW5kdWFuQGd4bXUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship