 Melanie van der Velde-van Buuringen1,2,3*
Melanie van der Velde-van Buuringen1,2,3* Rosalie Hendriks-van der Sar3
Rosalie Hendriks-van der Sar3 Hilde Verbeek4,5
Hilde Verbeek4,5 Wilco P. Achterberg1,2Monique A. A. Caljouw1,2
Wilco P. Achterberg1,2Monique A. A. Caljouw1,2- 1University Network for the Care Sector Zuid-Holland, Leiden University Medical Center, Leiden, Netherlands
- 2Department of Public Health and Primary Care, Leiden University Medical Center, Leiden, Netherlands
- 3Zorginstellingen Pieter van Foreest, Delft, Netherlands
- 4Department of Health Services Research, Care and Public Health Research Institute (CAPHRI), Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, Netherlands
- 5Living Lab in Ageing and Long-Term Care, Maastricht University, Maastricht, Netherlands
Objectives: Considering the importance of going outside in a natural environment for people in general, and people living with dementia in particular, we want to unravel the aspects by which garden use affects quality of life (QoL) and behavioral and psychological symptoms of dementia (BPSD) in people living with dementia in nursing homes.
Design: Systematic review.
Setting and participants: People living with dementia in nursing homes.
Methods: This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Eight electronic bibliographic databases were searched (May 2022). Quantitative, qualitative and mixed-methods studies describing the effect of garden use on QoL, BPSD, or other outcomes related to QoL or BPSD in people living with dementia in nursing homes were included. The methodological quality of individual studies was assessed with the Mixed Methods Appraisal Tool (MMAT) and a narrative synthesis of the results was performed.
Results: After screening title and abstract (N = 498), and full-text assessment (N = 67), 19 publications were included. These described 17 studies and three types of interventions: (1) interventions regarding the evaluation of effects of specifically designed nursing home gardens, (2) participation of the people living with dementia in outside activities, and (3) other interventions, for example, garden visits and different seasons.
Conclusions and implications: Overall, first studies appear to suggest positive effects of garden use on QoL, BPSD, or other outcomes related to QoL or BPSD (stress, sleep, and mood) in people living with dementia in nursing homes. However, consensus regarding measurements and key outcomes, taking into account the physical, social, and organizational aspects when designing the garden use intervention, is necessary for the reliable evaluation of these interventions.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=283267, identifier: CRD42021283267.
1. Introduction
Dementia is categorized as a major neurocognitive disorder, and is an irreversible disorder with a progressive decline in various cognitive functions that influences intellectual, social and physical functioning (1, 2). Most of the people living with dementia in nursing homes spend their day inactive in a lying down or sitting position, and on average more than 90% of the residents stay inside their ward during the day (3). They experience a major loss of quality of life (QoL), defined by “the multidimensional evaluation of the person-environment system of the individual, in terms of adaptation to the perceived consequences of the dementia” (4, 5). Some of the aspects that influence QoL are behavioral and psychological symptoms of dementia (BPSD), for example agitation (2, 6). BPSD is defined as “signs and symptoms of disturbed perception, thought content, mood, and behavior” (6, 7). Possible causes of the symptoms are neurobiologically related disease factors, unmet needs such as hunger or pain, caregiver factors and environmental triggers (7).
Various interventions have been developed to tackle the problems as mentioned above. One of these interventions is the passive and active use of gardens of nursing homes (8). Garden use consists of a variety of activities, some individual, some communal. The definition of gardens and garden use differs widely in terms of scale, function, and activity (9). Gardens are often thought of as intimate private spaces attached to private households but they can also be large private or formal gardens part of nursing homes (9). There are different possibilities regarding the use of gardens in nursing homes, for example horticultural therapy, which uses plant-related activities as a therapeutic modality to achieve goals (10), or green care farms that combine agricultural with care activities (11).
In this systematic review the term garden use refers to any activity in the nursing home garden that is a person-centered activity and fits within the usual activities in daily nursing home practice, meaning going outside into the nursing home garden and doing an activity outside that is usually done inside. Examples of person-centered garden activities are sitting, walking, having a conversation, drinking a beverage, having lunch, gardening, or receiving therapy (12). Person-centered care is a care approach built around the needs of an individual. It recognizes that all people are unique and have their own personal needs. The task of the caregivers is to be aware of behaviors that undermine the person's wellbeing (and to do that as little as possible) and enhance the person's wellbeing (and to do that as much as possible) to deliver optimum levels of care. The activities are tailored to the residents' wishes and preferences (13, 14).
Being in the garden can provide a physical and psychological distance from stress and attention evoking stimuli (15). There are different theories about how being in a natural environment such as a garden can promote more rapid and complete restoration of (the consequences of) stress than other environments, but two contrasting theories dominate this field (15). The psychoevolutionary theory places emphasis on stress reduction whereby contact with nature can very rapidly evoke positive affect, which in turn blocks negative thoughts and feelings and fosters reduction of physiological activation (15–17). The attention restoration theory places emphasis on recovery of the capacity to focus attention, whereby effortless attention engaged by intrinsically interesting aspects of nature enables rest for a fatigued neurocognitive inhibitory mechanism engaged when wilfully directing attention (15, 18).
In recent years, interest in the effects of garden use on people living with dementia in nursing homes has increased. More and more studies from different disciplines are finding positive effects of different aspects of garden use. For example, one review suggested an overall positive effect of the creation of dementia-friendly gardens on agitation, apathy and engagement, despite concerns about the methodological approaches (19). Another review examined the barriers and facilitators affecting nursing home residents' use of outdoor space, as perceived by residents, their family members, and staff (20). This study showed that, in addition to specific aspects in the design of the garden, cultural change at an organizational level is also necessary, for example by addressing perceptions of safety. Whear et al. (21) showed promising results for the effect of garden use on agitation.
Despite the increasing number of studies on this topic, there is no systematic review done of recent specific data on the effect of garden use on QoL and BPSD in people living with dementia in nursing homes. Considering the importance of going outside in a natural environment for people in general (15), and people living with dementia in particular (21), we want to unravel which aspects of garden use affect QoL and BPSD in people living with dementia in nursing homes. This systematic review therefore addressed the following research question: “What is the effect of garden use on QoL and BPSD in people living with dementia in nursing homes?”
2. Methods
This systematic review was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (22). The search and analysis methods were specified in advance in a protocol. The protocol is registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42021283267).
2.1. Search strategy
The search strategy was developed together with an information specialist and included terms related to garden use, dementia, QoL, BPSD, and nursing homes. For the complete search strategy see the Supplementary material online attached to the electronic version of this paper. Searches were conducted in eight electronic bibliographic databases for the period 1946 to May 2022: PubMed, MEDLINE, Embase, Web of Science, COCHRANE Library, Emcare, PsycINFO, and Academic Search Premier. The search in the electronic bibliographic databases was conducted on May 12, 2022.
2.2. Eligibility criteria
Research articles describing the effect or measuring the effect of the intervention of garden use (outdoor spaces, outside, wander garden, therapeutic garden, and healing garden in the nursing home environment) on QoL (wellbeing and life quality), and BPSD (BPSD, neuropsychiatric symptoms of dementia) in people living with dementia in nursing homes [nursing homes by the definition of Sanford et al. (23) “A facility with a domestic-styled environment that provides 24-h functional support and care for people who require assistance with ADLs and who often have complex health needs and increased vulnerability,” institutional care] were eligible for inclusion. In addition, quantitative, qualitative and mixed-methods studies in English/Dutch/German/French were eligible for inclusion. Letters to the editor, reviews, studies describing the effects of horticultural therapy, or taking place at facilities without 24-h functional care were excluded.
2.3. Study selection
Two researchers (MVB and RHS) independently assessed which studies retrieved in the searches met the inclusion criteria based on titles and abstracts. This was followed by full-text assessments. Differences were discussed until consensus was reached, and when necessary by consulting a third researcher (MAAC).
2.4. Methodological quality of individual studies
The Mixed Methods Appraisal Tool (MMAT) version 2018 (24) was used to assess the methodological quality of all included individual studies. One researcher (MVB) carried out the assessment, which was checked by a second researcher (RHS). Again, consensus was reached through discussion, and when necessary by consulting a third researcher (MAAC).
2.5. Data extraction and analysis
A standardized data extraction form was developed to extract the data of the included studies. A description of the included studies was summarized in a table by extraction of year and country of publication, study design, study population, intervention, outcome measures, and study quality (MMAT). Studies were not excluded from the review based on their quality.
Included studies were anticipated to be very diverse in terms of intervention and outcome measures, making pooling impossible. Therefore, a narrative synthesis of the findings was given in a table structured by outcome (study design, participants, type of intervention, QoL, BPSD, other outcomes related to QoL or BPSD, and methodological quality) and description of the aim/objective of the study and main findings. This synthesis was carried out by two researchers (MVB and RHS), and a third author (MAAC) was available if agreement was not reached.
3. Results
3.1. Study selection
The process of screening and selection is shown in the flow diagram in Figure 1. After removal of duplicates, 498 publications remained. After screening title and abstract on inclusion criteria, 431 publications were excluded. The remaining 67 publications were screened full text, after which 31 publications were excluded. The remaining 36 publications were assessed for eligibility and finally 19 publications were included in this review.
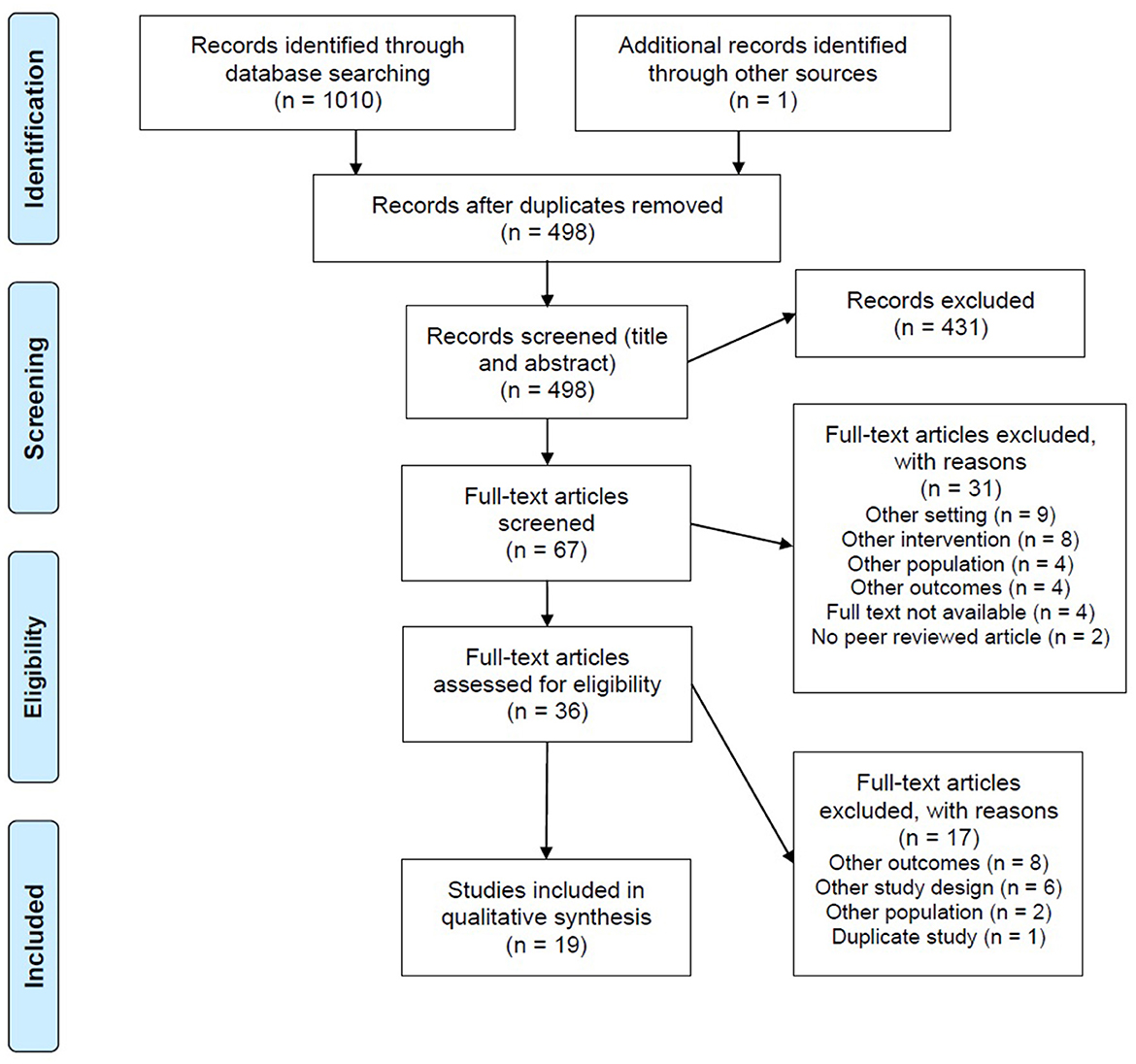
Figure 1. Flow diagram of the study screening and selection.
3.2. Study characteristics
The 19 publications included in this review described 17 different studies. The publications of Detweiler et al. (25), Detweiler et al. (26), and Murphy et al. (27) reported on different aspects of the results of the same study. The characteristics of the included studies are presented in Table 1.
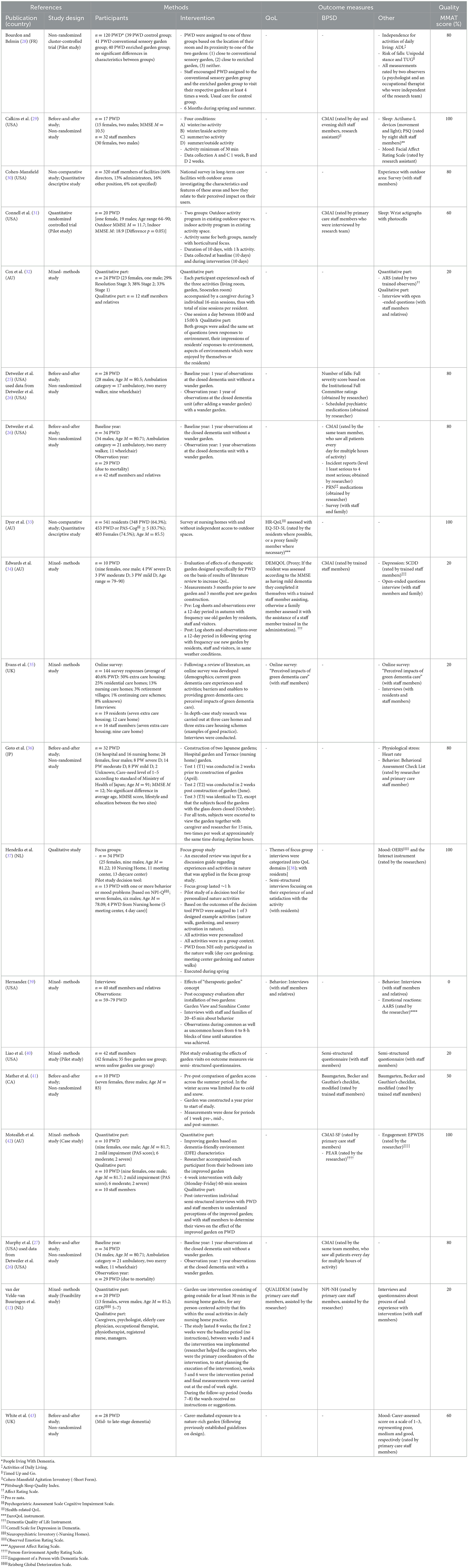
Table 1. Description of included publications (N = 19).
3.3. Study design
Seven publications used a before-and-after non-randomized design (25–27, 36, 41, 43), and seven had a mixed-methods design (12, 32, 34, 35, 39, 40, 42). A non-comparative quantitative descriptive study design was used in two publications (33), one used a quantitative randomized controlled trial design (31), one was a non-randomized clustered controlled trial (28), and one had a qualitative study design (37). Four studies were pilot or feasibility studies (12, 28, 31, 40).
3.4. Participants
The number of participants included in the publications ranged from 10 people living with dementia (34, 41) to 541 residents [of whom 453 people living with dementia (83.7%) or a score of ≥ 5 on the Psychogeriatric Assessment Scale Cognitive Impairment Scale (PAS-Cog)] (33). Ten publications included only people living with dementia as participants (25, 27, 28, 31, 33, 34, 36, 37, 41, 43), while seven included people living with dementia as well as staff members and relatives as participants (12, 26, 29, 32, 35, 39, 42), and two only included staff members as participants (30, 40).
3.5. Interventions
A wide variety of interventions are described. They can be grouped into interventions regarding the evaluation of (1) effects of specifically designed nursing home gardens, (2) participation of the people living with dementia in activities in the garden of the nursing home, and (3) other interventions. Eight studies described an evaluation of the effects of specifically designed gardens (25–28, 34, 36, 39, 42), three regarded interventions in which the people living with dementia participated in activities that took place in different environments, for example, the garden vs. the living room (29, 31, 32), and the rest of the publications described a range of other interventions, like an evaluation of the effects of garden visits (40, 43), garden visits in different seasons (29, 41), of (not) having independent access to the outdoor spaces (33), and creating and testing a decision tool for personalized nature activities (37). Furthermore (a number of), sessions were part of the intervention in only three publications (32, 36, 42).
3.6. Outcome measures
Overall, there was a wide variety in outcome measures. The results of the publications were divided based on outcome: QoL, BPSD, and other outcomes related to QoL or BPSD (see Table 1). The outcome QoL was measured both quantitatively (12, 33, 34, 39), and qualitatively (35, 37, 39). The measurements of BPSD showed the most homogeneity: eight of the 10 publications used quantitative measures, of which six the Cohen-Mansfield Agitation Inventory [-Short Form; CMAI (-SF)] (26, 27, 29, 31, 34, 42). Other measurements used were the number of falls, number of incidents, scheduled and pro re nata psychiatric medications, the modified Baumgarten, Becker and Gauthier's checklist, the Person-Environment Apathy Rating Scale (PEAR), and the Neuropsychiatric Inventory Nursing Homes (NPI-NH) (12, 25, 26, 41, 42). Only three publications (also) used qualitative measures, namely a survey, a semi-structured questionnaire, and a semi-structured interview (26, 40, 42). Other quantitative QoL- or BPSD-related outcome measures used were, for example, heart rate (stress), wrist actigraphy with photocells (sleep), and the Cornell Scale for Depression in Dementia (SCDD; depression). The qualitative outcome measures consisted mostly of (semi-structured) questionnaires or surveys. Due to the considerable heterogeneity of the used measures, it is very difficult to compare the effectiveness of the different interventions.
3.7. Methodological quality of individual publications
The results of the assessment of the methodological quality of individual publications are presented in Table 1. The overall MMAT score ranged from 0% (39) to 100% (29, 33, 37, 42). Of the 19 publications, one scored 0% (39), five scored 20% (12, 32, 34, 35, 40), and 13 scored 50% or higher. Most of the studies using mixed methods made insufficient use of the potential of this type of design. For example, they did not describe if and how the different components of the study were effectively integrated to answer the research question, nor did they adequately address the divergences and inconsistencies between quantitative and qualitative results. Overall, however, the independent quantitative and qualitative components of these studies were of good quality.
3.8. Results of individual studies
3.8.1. Quality of life
The results regarding QoL are summarized in Table 2. All six publications described a positive effect of garden use on QoL in people living with dementia in nursing homes (12, 33–35, 37, 39). Some publications show an overall positive effect of garden use on QoL (34, 39). Others found a more specific positive effect on QoL. Van der Velde-van Buuringen et al. (12) for example, found that people living with dementia showed an increase in the domain positive affect and a decrease in the domain social isolation of the QUALIDEM during the intervention period of going outside. Another example is the study by Dyer et al. (33) which found that going outdoors daily was significantly associated with better Health-related QoL (HR-QoL) of residents. However, going outdoors multiple times (1–6 times) per week but not daily was not significantly associated with better HR-QoL. Based on focus group interviews Hendriks et al. (37) found eight key themes concerning the question what kind of experiences persons living with dementia find important for their wellbeing and QoL when in nature: Pleasure, relaxation, feeling fit, enjoying the beauty of nature, feeling free, the social aspect of nature, feeling useful, and memories. In Evans et al. (35) staff members mentioned many ways in which they felt nature-based activities had a positive effect on the wellbeing of persons living with dementia, including high levels of engagement, a sense of freedom, creativity, increased social interaction, inter-generational contact with families, and the calming effect of contact with animals. Of the five publications with qualitative data (12, 33, 35, 37, 39), only two (35, 37) publications (also) asked the people living with dementia directly about their experiences, instead of only staff members and/or relatives on the behalf of the people living with dementia. Three (12, 35, 37) of the publications were suitable for further in-depth data synthesis. In these papers, five themes were identified that appear to capture the overall experiences of people living with dementia, staff members, and relatives of the effect of garden use on QoL: sense of freedom (35, 37), social interaction (35, 37), calming effect (12, 35, 37), reminiscence (12, 37), and pleasure (35, 37).
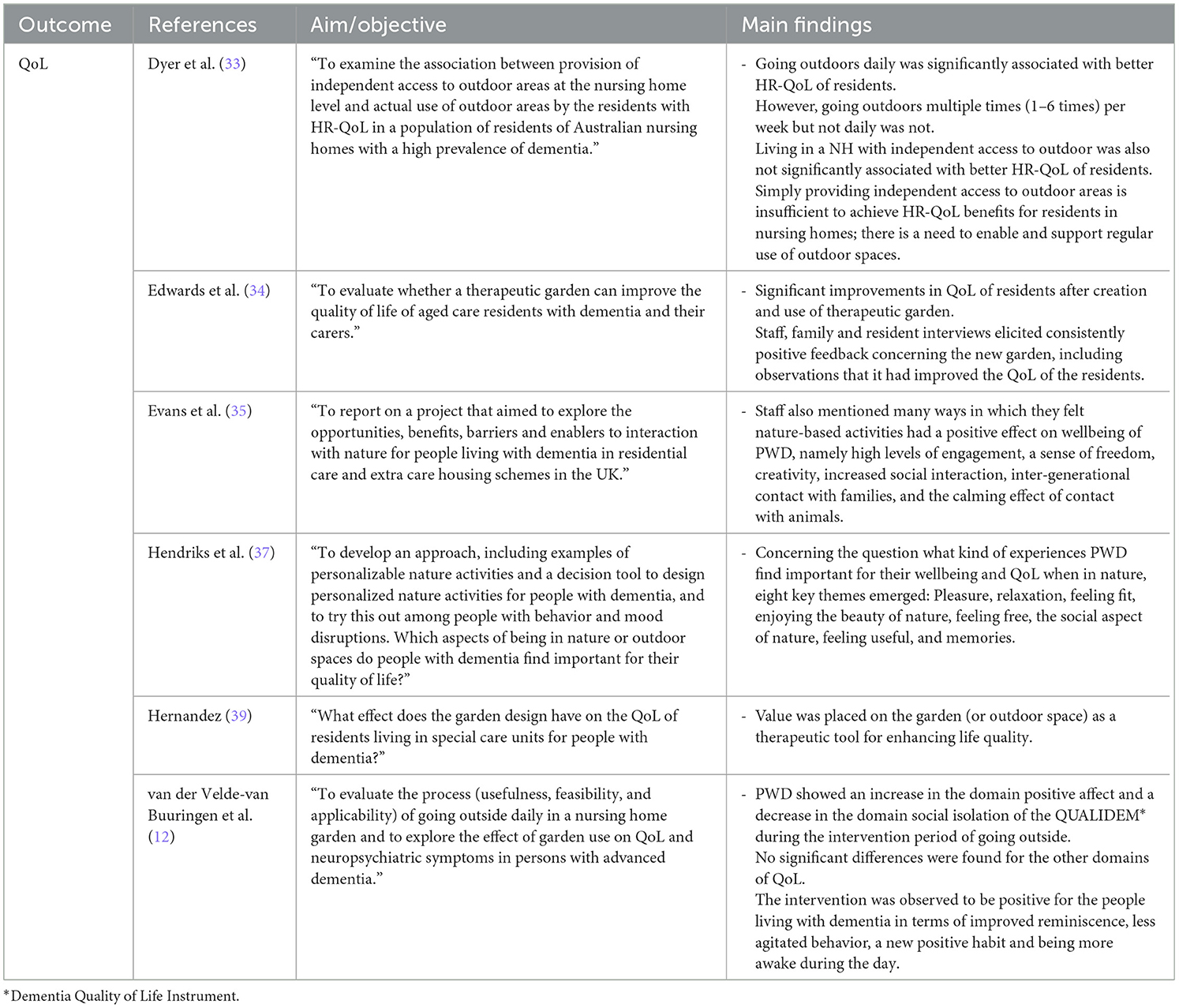
Table 2. Main findings on outcome measure QoL (n = 6).
3.8.2. Behavioral and psychological symptoms of dementia
The results regarding BPSD are summarized in Table 3. Seven of the 10 publications describe positive effects of garden use on BPSD (25–27, 31, 34, 40, 42). Some publications describe an overall positive effect on BPSD (26, 33), others a more specific effect, for example on the frequency of verbal agitation (31). Murphy et al. (27) showed that the degree to which the average numbers of days spent in the wander garden is associated with decreased agitation scores is dependent on baseline agitation scores and ambulation ability. There was more effect for the people living with dementia who had higher levels of agitation at the beginning of the study than for those who had lower levels of agitation. Also, when residents could walk without assistance, a low, medium and high usage of the garden reduced agitation, with a higher frequency corresponding with a greater decrease in agitation. For the merry walker chair and wheelchair users, those who had a high number of garden visits showed decreased agitation levels, but medium or low garden usage was associated with unchanged or increased agitation. Detweiler et al. (25) found variations in effects of low or high frequency garden use. The high frequency garden use group showed a decreased need for scheduled high-dose and intermediate-dose antipsychotics, eliminated and reduced the need for scheduled secondary antidepressants, and scheduled intermediate-dose hypnotics compared to the low frequency garden use group. Also, increased garden use appeared to be related to a decreased frequency and severity of falls. The rest of the publications showed no significant positive effects, or inconclusive or contradictory effects of garden use on BPSD (12, 29, 41, 42). Both van der Velde-van Buuringen et al. (12) and Motealleh et al. (42) found no significant differences in the quantitative data measured with the NPI-NH and CMAI, but when conducting semi-structured interviews with people living with dementia and staff members, reduced agitated behavior was mentioned as one of the positive results of garden use. Calkins et al. (29) found changes that were contradictory, namely fewer resident-requests for attention during the day as observed by the research assistant, but more requests for attention in the evening as observed by the evening shift staff members. An explanation given by the researcher is that because the people living with dementia are sleeping better, they don't want to go to bed as early and therefore request attention. Liao et al. (40) showed that garden visits had positive effects on behavioral problems, through multisensory stimulation, a feeling of independence, provoking a recall of memories, and relieving stress. Of the three publications with qualitative data (12, 40, 42), only one publication (42) (also) asked the people living with dementia directly about their experiences, instead of only staff members on the behalf of the people living with dementia. All three of the publications were suitable for further in-depth data synthesis, whereby one theme was identified: Garden use had a positive effect on agitation (12, 40, 42).
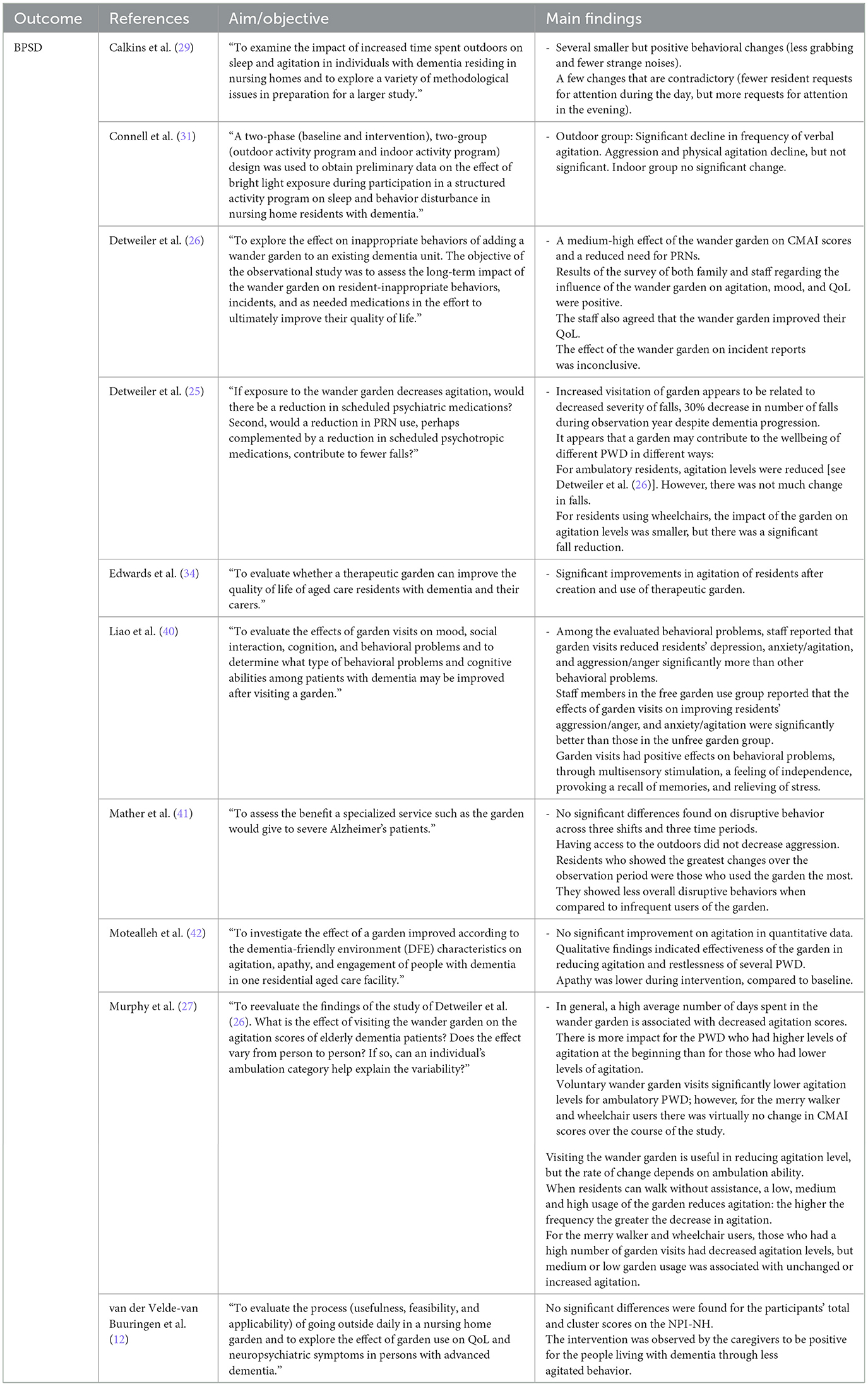
Table 3. Main findings on outcome measure BPSD (n = 10).
3.8.3. Other outcomes related to QoL or BPSD
Other outcomes related to QoL or BPSD included stress, sleep, and mood (see Table 1). Regarding stress, Goto et al. (36) showed that when residents observed a Japanese garden with the door open, their physiological stress was relieved, as reflected in a sustained drop in the pulse rate of the residents. The blunting of the effect when the viewing was through a glass door hints at the importance of the sense of immersion in the scene. A number of publications found positive, but also contradictory effects of garden use on sleep. For example, the study by Connell et al. (31) showed no significant change in number of wakes when comparing an outdoor and indoor group during an intervention study. By contrast, Mather et al. (41) found that residents who used the garden often showed less sleep disruption when compared to infrequent users of the garden. Lastly, most of the publications showed an overall positive effect of garden use on mood (32, 34, 35, 40, 43). White et al. (43) found a more specific time-dependent effect on mood, namely time spent outside was a non-linear predictor of change in mood score. Marked improvements in mood were associated with outdoor time of only 20 min duration and the greatest benefits were associated with an outdoor time of 80–90 min duration. After this point, the extent of positive change in mood score declined with more time spent outside.
4. Discussion
Overall, the results of the included studies suggested positive effects of garden use on QoL, BPSD, and other outcomes related to QoL or BPSD in people living with dementia in nursing homes. All six publications regarding QoL described positive effects of garden use on QoL in people living with dementia in nursing homes. Two thirds of the publications regarding BPSD described positive effects of garden use on BPSD in people living with dementia in nursing homes, and one third showed no significant positive, inconclusive, or contradictory effects.
Some of the publications describe an overall positive effect on QoL and BPSD, while others show a more specific effect. Perhaps there are different mechanisms that affect the influence of garden use on QoL and BPSD. For example, Hartig et al. (15) present a framework of pathways (and possibilities for effect modification by individual or contextual variables) through which the natural environment might affect the health of broad segments of the populations. The framework shows that there are direct beneficial effects of nature on stress and indirect beneficial effects, through contact with nature, on physical activity and social contacts and therefore also on health and wellbeing (15).
This systematic review found that studies examining the effect of garden use on QoL and BPSD in people living with dementia in nursing homes mostly focused on the evaluation of effects of specifically designed gardens. However, the question is whether an intervention of specifically designed nursing home gardens for people living with dementia is sufficient and adequate, or does the complex care environment of nursing homes need a more complex intervention that includes the social and organizational aspects (44–46). The theoretical framework in de Boer et al. (45) states that the literature indicates three environmental components within residential dementia care settings that impact everyday life and functioning of persons living with dementia: Physical aspects (e.g., design), social aspects (e.g., interactions with staff), and organizational aspects (e.g., attitudes that guide behavior of staff). There are barriers to garden use by people living with dementia in nursing homes, which may negatively influence the frequency of garden use, and therefore also negatively influence QoL and BPSD (20). For example, apart from the design of the garden, one of the main barriers is the perceived risk of independent use of the outdoor space, resulting in for example locked doors (20).
A limitation of this systematic review is that pooling and meta-analysis of the results of the interventions were not possible due to the use of different methods, interventions, and outcome measures in the individual studies. Overall, the majority of the studies did not describe the interventions in sufficient detail to be able to repeat the study, and very few publications provided effect sizes in the results. Whear et al. (21) discussed this problem and suggested that research in this field may benefit from an agreed set of tools to measure key outcomes, such as QoL, agitation, use of medication, or falls. However, measuring the possible effects of interventions on the daily lives of people living with dementia is difficult, because daily life is a dynamic and multidimensional concept. It involves more than just activities, for example the physical and social environments of the nursing homes (47). Future research regarding the effects of garden use on people living with dementia in nursing homes could benefit from the development of such measures that incorporate the context of the physical and social environments of the nursing homes.
Given the positive effects of garden use on QoL and BPSD in people living with dementia in nursing homes, one might expect that garden use is already incorporated in daily nursing home practice. This is, however, not the case, as demonstrated by the low numbers of people living with dementia who go outside (3). It is important to recognize that current interventions regarding garden use with a focus on changing the physical aspects in the garden environment might not be sufficient to solve this problem. Future research should focus on including all aspects (i.e., physical, social, and organizational) in the garden use intervention, for example by providing training and activities to empower staff to implement garden use in the daily life of the people living with dementia and embedding it in the culture of the nursing home. Incorporating daily garden use does not necessarily mean an additional task, but rather rearranging priorities and moving the usual activities outside part of the time (12).
4.1. Conclusions and implications
Garden use seems to have a positive effect on QoL and BPSD in people living with dementia in nursing homes. However, consensus regarding measurements and key outcomes, taking into account the physical, social, and organizational aspects when designing the garden use intervention, is necessary for the reliable evaluation of these interventions.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
MV-v, HV, WA, and MC: study design, writing the study protocol, and writing of the manuscript. MV-v: database search. MV-v, RH-v, HV, WA, and MC: data analysis and interpretation. All authors read and approved the final version of the manuscript.
Funding
This research was made possible in cooperation with Zorginstellingen Pieter van Foreest, Delft, Netherlands.
Acknowledgments
We thank Jan Schoones, information specialist Directorate of Research Policy (formerly: Walaeus Library, Leiden University Medical Center, Leiden, Netherlands) for helping with the search.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1044271/full#supplementary-material
References
1. Sachdev PS, Blacker D, Blazer DG, Ganguli M, Jeste DV, Paulsen JS, et al. Classifying neurocognitive disorders: The DSM-5 approach. Nat Rev Neurol. (2014) 10:634–42. doi: 10.1038/nrneurol.2014.181
2. Banerjee S, Samsi K, Petrie CD, Alvir J, Treglia M, Schwam EM, et al. What do we know about quality of life in dementia? A review of the emerging evidence on the predictive and explanatory value of disease specific measures of health related quality of life in people with dementia. Int J Geriatr Psychiatry. (2009) 24:15–24. doi: 10.1002/gps.2090
3. den Ouden M, Bleijlevens MHC, Meijers JMM, Zwakhalen SMG, Braun SM, Tan FES, et al. Daily (In)Activities of nursing home residents in their wards: An observation study. J Am Med Dir Assoc. (2015) 16:963–8. doi: 10.1016/j.jamda.2015.05.016
4. Nederland A, Vilans. Zorgstandaard Dementie. (2013). Available online at: https://www.zorgvoorbeter.nl/docs/beteroud/ngn/zorgstandaard-dementie-2013.pdf
5. Ettema TP, Dröes R-M, de Lange J, Ooms ME, Mellenbergh GJ, Ribbe MW. The concept of quality of life in dementia in the different stages of the disease. Int Psychogeriatr. (2005) 17:353–70. doi: 10.1017/S1041610205002073
6. Finkel SI, Silva JC, Cohen G, Miller S, Sartorius N. Behavioral and psychological signs and symptoms of dementia: A consensus statement on current knowledge and implications for research and treatment. Int Psychogeriatr. (1996) 8:497–500. doi: 10.1017/S1041610297003943
7. Kales HC, Gitlin LN, Lyketsos CG. Assessment and management of behavioral and psychological symptoms of dementia. Br Med J. (2015) 350:bmj.h369. doi: 10.1136/bmj.h369
8. Abraha I, Rimland JM, Trotta FM, Dell'Aquila G, Cruz-Jentoft A, Petrovic M, et al. Systematic review of systematic reviews of non-pharmacological interventions to treat behavioural disturbances in older patients with dementia. The SENATOR-OnTop series. Br Med J Open. (2017) 7:e012759. doi: 10.1136/bmjopen-2016-012759
9. Buck D. Gardens Health: Implications for Policy Practice. The King's Fund (2016). Available online at: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Gardens_and_health.pdf
10. Nicholas SO, Giang AT, Yap PLK. The effectiveness of horticultural therapy on older adults: A systematic review. J Am Med Direct Assoc. (2019) 20:1351.e1. doi: 10.1016/j.jamda.2019.06.021
11. de Boer B, Hamers JPH, Zwakhalen SMG, Tan FES, Beerens HC, Verbeek H. Green care farms as innovative nursing homes, promoting activities and social interaction for people with dementia. J Am Med Dir Assoc. (2017) 18:40–6. doi: 10.1016/j.jamda.2016.10.013
12. van der Velde-van Buuringen M, Achterberg WP, Caljouw MAA. Daily garden use and quality of life in persons with advanced dementia living in a nursing home: A feasibility study. Nurs Open. (2020) 2020:740. doi: 10.1002/nop2.740
13. Kitwood TM, Kitwood T. Dementia Reconsidered: The Person Comes First. Vol. 20. Buckingham: Open University Press (1997).
14. Mitchell G, Agnelli J. Person-centred care for people with dementia: Kitwood reconsidered. Nurs Stand. (2015) 30:46–50. doi: 10.7748/ns.30.7.46.s47
15. Hartig T, Mitchell R, de Vries S, Frumkin H. Nature and health. Ann Rev Publ Health. (2014) 35:207–28. doi: 10.1146/annurev-publhealth-032013-182443
16. Ulrich RS. Aesthetic and affective response to natural environment. In:I Altman, JF Wohlwill, , editors, Behavior and the Natural Environment. Springer US: Boston, MA. (1983). p. 85–125. doi: 10.1007/978-1-4613-3539-9_4
17. Ulrich RS, Simons RF, Losito BD, Fiorito E, Miles MA, Zelson M. Stress recovery during exposure to natural and urban environments. J Environ Psychol. (1991) 11:201–30. doi: 10.1016/S0272-4944(05)80184-7
18. Kaplan S. The restorative benefits of nature: Toward an integrative framework. J Environ Psychol. (1995) 15:169–82. doi: 10.1016/0272-4944(95)90001-2
19. Motealleh P, Moyle W, Jones C, Dupre K. Creating a dementia-friendly environment through the use of outdoor natural landscape design intervention in long-term care facilities: A narrative review. Health Place. (2019) 58:102148. doi: 10.1016/j.healthplace.2019.102148
20. van den Berg MEL, Winsall M, Dyer SM, Breen F, Gresham M, Crotty M. Understanding the barriers and enablers to using outdoor spaces in nursing homes: A systematic review. Gerontologist. (2020) 60:E254–69. doi: 10.1093/geront/gnz055
21. Whear R, Coon JT, Bethel A, Abbott R, Stein K, Garside R. What is the impact of using outdoor spaces such as gardens on the physical and mental well-being of those with dementia? A systematic review of quantitative and qualitative evidence. J Am Med Dir Assoc. (2014) 15:697–705. doi: 10.1016/j.jamda.2014.05.013
22. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Br Med J. (2009) 339:b2535. doi: 10.1136/bmj.b2535
23. Sanford AM, Orrell M, Tolson D, Abbatecola AM, Arai H, Bauer JM, et al. An international definition for “nursing home”. J Am Med Direct Assoc. (2015) 16:181–4. doi: 10.1016/j.jamda.2014.12.013
24. El-Awaisi A, Joseph S, Hajj MSE, Diack L. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inform. (2018) 34:1–7. doi: 10.3233/EFI-180221
25. Detweiler MB, Murphy PF, Kim KY, Myers LC, Ashai A. Scheduled medications and falls in dementia patients utilizing a wander garden. Am J Alzheimers Dis Other Demen. (2009) 24:322–32. doi: 10.1177/1533317509334036
26. Detweiler MB, Murphy PF, Myers LC, Kim KY. Does a wander garden influence inappropriate behaviors in dementia residents? Am J Alzheimers Dis Other Demen. (2008) 23:31–45. doi: 10.1177/1533317507309799
27. Murphy PF, Miyazaki Y, Detweiler MB, Kim KY. Longitudinal analysis of differential effects on agitation of a therapeutic wander garden for dementia patients based on ambulation ability. Dementia. (2010) 9:355–73. doi: 10.1177/1471301210375336
28. Bourdon E, Belmin J. Enriched gardens improve cognition and independence of nursing home residents with dementia: A pilot controlled trial. Alzheimers Res Ther. (2021) 13:116. doi: 10.1186/s13195-021-00849-w
29. Calkins M, Szmerekovsky JG, Biddle S. Effect of increased time spent outdoors on individuals with dementia residing in nursing homes. J Hous Elderly. (2007) 21:211–28. doi: 10.1300/J081v21n03_11
30. Cohen-Mansfield J. Outdoor wandering parks for persons with dementia. J Hous Elderly. (2007) 21:35–53. doi: 10.1300/J081v21n01_03
31. Connell BR, Sanford JA, Lewis D. Therapeutic effects of an outdoor activity program on nursing home residents with dementia. J Hous Elderly. (2007) 21:195–209. doi: 10.1300/J081v21n03_10
32. Cox H, Burns I, Savage S. Multisensory environments for leisure: Promoting well-being in nursing home residents with dementia. J Gerontol Nurs. (2004) 30:37–45. doi: 10.3928/0098-9134-20040201-08
33. Dyer SM, Liu E, Gnanamanickam E, Harrison SL, Milte R, Crotty M. Associations between quality of life and outdoor access in nursing homes: A cross-sectional study. Ann Longterm Care. (2021) e1–7. doi: 10.25270/altc.2021.02.00001
34. Edwards CA, McDonnell C, Merl H. An evaluation of a therapeutic garden's influence on the quality of life of aged care residents with dementia. Dementia. (2013) 12:494–510. doi: 10.1177/1471301211435188
35. Evans SC, Barrett J, Mapes N, Hennell J, Atkinson T, Bray J, et al. Connections with nature for people living with dementia. Work Older People. (2019) 23:142–51. doi: 10.1108/WWOP-01-2019-0003
36. Goto S, Shen X, Sun M, Hamano Y, Herrup K. The positive effects of viewing gardens for persons with dementia. J Alzheimers Dis. (2018) 66:1705–20. doi: 10.3233/JAD-170510
37. Hendriks IH, van Vliet D, Gerritsen DL, Dröes R-M. Nature and dementia: Development of a person-centered approach. Int Psychogeriatr. (2016) 28:1455–70. doi: 10.1017/S1041610216000612
38. Dröes R-M, Knoop ECCB-VD, Bos J, Meihuizen L, Ettema TP, Gerritsen DL, et al. (2006). Quality of life in dementia in perspective: an explorative study of variations in opinions among people with dementia and their professional caregivers, and in literature. Dementia Int J. 5:533–58. doi: 10.1177/1471301206069929
39. Hernandez RO. Effects of therapeutic gardens in special care units for people with dementia: Two case studies. J Hous Elderly. (2007) 21:117–52. doi: 10.1300/J081v21n01_07
40. Liao M-L, Ou S-J, Hsieh CH, Li Z, Ko C-C. Effects of garden visits on people with dementia: A pilot study. Dementia Int J Soc Res Practice. (2020) 19:1009–28. doi: 10.1177/1471301218793319
41. Mather JA, Nemecek D, Oliver K. The effect of a walled garden on behavior of individuals with Alzheimer's. Am J Alzheimer's Dis. (1997) 12:252–7. doi: 10.1177/153331759701200603
42. Motealleh P, Moyle W, Jones C, Dupre K. The impact of a dementia-friendly garden design on people with dementia in a residential aged care facility: A case study. HERD. (2022) 15:196–218. doi: 10.1177/19375867211063489
43. White PC, Wyatt J, Chalfont G, Bland JM, Neale C, Trepel D, et al. Exposure to nature gardens has time-dependent associations with mood improvements for people with mid- and late-stage dementia: Innovative practice. Dementia. (2018) 17:627–34. doi: 10.1177/1471301217723772
44. Grol R, Wensing M. What drives change? Barriers to and incentives for achieving evidence-based practice. Med J Austr. (2004) 180:S57–60. doi: 10.5694/j.1326-5377.2004.tb05948.x
45. de Boer B, Bozdemir B, Jansen J, Hermans M, Hamers JPH, Verbeek H. The homestead: Developing a conceptual framework through co-creation for innovating long-term dementia care environments. Int J Environ Res Public Health. (2021) 18. doi: 10.3390/ijerph18010057
46. Buist Y, Verbeek H, de Boer B, de Bruin SR. Innovating dementia care; implementing characteristics of green care farms in other long-term care settings. Int Psychogeriatr. (2018) 30:1057–68. doi: 10.1017/S1041610217002848
Keywords: dementia, nursing homes, quality of life, behavioral and psychological symptoms of dementia, garden use, systematic review
Citation: Velde-van Buuringen Mvd, Hendriks-van der Sar R, Verbeek H, Achterberg WP and Caljouw MAA (2023) The effect of garden use on quality of life and behavioral and psychological symptoms of dementia in people living with dementia in nursing homes: a systematic review. Front. Psychiatry 14:1044271. doi: 10.3389/fpsyt.2023.1044271
Received: 14 September 2022; Accepted: 27 March 2023;
Published: 12 April 2023.
Edited by:
Susan Kurrle, The University of Sydney, AustraliaCopyright © 2023 Velde-van Buuringen, Hendriks-van der Sar, Verbeek, Achterberg and Caljouw. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Melanie van der Velde-van Buuringen, bS52YW5fZGVyX3ZlbGRlQGx1bWMubmw=