 Sophia Dückert1*
Sophia Dückert1* Sabine Bart1,2Petia Gewohn1,3Hannah König4Daniel Schöttle3Alexander Konnopka4Pascal Rahlff1Frank Erik1
Sabine Bart1,2Petia Gewohn1,3Hannah König4Daniel Schöttle3Alexander Konnopka4Pascal Rahlff1Frank Erik1 Kai Vogeley5
Kai Vogeley5 Holger Schulz1
Holger Schulz1 Nicole David1
Nicole David1 Judith Peth1
Judith Peth1- 1Department of Medical Psychology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 2Department Health Sciences, Faculty Life Sciences, Hamburg University of Applied Sciences, Hamburg, Germany
- 3Department of Psychiatry and Psychotherapy, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 4Department of Health Economics and Health Services Research, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 5Department of Psychiatry, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany
Introduction: Family members of autistic individuals often provide support for their autistic relative throughout the lifespan which can lead to massive burden themselves. Reduced health-related Quality of Life (HRQoL) in family caregivers is assumed; however, only a handful studies on the HRQoL of family caregivers providing care to adult relatives exist as opposed to autistic children. Thus, the current study aimed to (i) investigate the current state of physical and mental HRQoL of family caregivers of autistic adults compared to the general population, and (ii) examine caregiver-related (e.g., age, subjective caregiver burden) and care recipient-related variables (e.g., symptom severity, utilization of formal services) explaining variance in the caregivers’ HRQoL.
Methods: N = 149 family caregivers completed a nationwide online survey, including the Short-Form Health Survey (SF-8) in order to assess the HRQoL. T-tests were used to compare the HRQoL of family caregivers with the general population. Bivariate correlational and multiple linear regression analyses were conducted in order to identify predictors explaining variance in family caregivers’ HRQoL.
Results: Family caregivers of autistic adults reported significantly lower physical (M = 46.71, SD = 8.72, Cohen’s d = 0.42) and mental HRQoL (M = 40.15, SD = 11.28, Cohen’s d = 1.35) compared to the general population. Multiple linear regression with the mental HRQoL as the outcome showed a significant model (F(11, 95) = 5.53, p <.001, adj. R2 =.32) with increased subjective burden explaining most of the variance in mental HRQoL (ß =.32, GDW =.141, p <.001). Multiple linear regression analysis with the outcome physical HRQoL did not reveal a statistically significant model (F(11,95) = 1.09, p =.38). However, bivariate analyses also showed a positive correlation with the subjective caregiver burden (r=.20, p <.05).
Discussion: Findings highlight the need to consider HRQoL (and caregiver burden) of family caregivers of autistic adults in several healthcare settings to monitor a potential comprised health status in early stages, with the long-term goal to improve family caregivers’ HRQoL.
1 Introduction
Core symptoms for the diagnosis of Autism Spectrum Disorder (ASD) include persistent specifics in social communication/interaction and restrictive, repetitive, and inflexible behavior patterns (1). In addition, somatic and mental comorbidities and challenging behaviors (e.g., aggression, self-injuring, and attempting suicide) are common (2, 3). One-third to one-half of autistic individuals have an accompanying intellectual disability (ID) (4, 5). In ASD, these specifics are very heterogeneous but often result in the need for support/assistance/care (for purpose of simplification, mentioned as “care” below). Typical caregiving demands include assistance with housekeeping, transportation, personal care (e.g., dressing, eating, toileting) (6) as well as distinct challenges, such as the need for mediation in social interactions, inflexible daily routines, or inappropriate behaviors (7, 8).
Usually, family caregivers are the most important source of support for autistic individuals (7). Accordingly, “diagnosis of autism affects not just the individual, but the entire family” [p. 45, (9)]. Especially when transitioning into adulthood and massive barriers impede adequate healthcare for autistic adults (e.g., pediatric services are no longer available, lack of funding, long waiting lists for diagnostics/treatment), autistic adults rely on the support of family caregivers [(e.g., grand) parents, partners/spouses, siblings, adult children] (9–11). Although caring for a loved one with autism also include positive effects on family caregivers (12), caregiving is typically time-intensive and exhausting (13). As autistic relatives enter adulthood, the duration and ongoing demands of caregiving can accumulate and lead to increased stress for family caregivers (14, 15), and have several negative effects on their lives, as shown by increased subjective caregiver burden (16, 17). Many family caregivers of autistic adults struggle with the care-associated responsibilities, while balancing everyday life, social interactions, and occupational responsibilities (15, 18–20). Loss of employment and high costs associated with care were discussed to lead to major financial burden (15, 20). Family caregivers of autistic adults also seem to be experiencing increased physical and mental health problems (21–23). For example, this population reported significantly higher emotional distress compared to caregivers of patients with schizophrenia and are at higher risk to develop health problems themselves (24).
Furthermore, compromised levels of health-related Quality of Life (HRQoL) in autistic adults’ family caregivers were reported (25, 26), which refers to “how well a person functions in their life and his or her perceived wellbeing in physical, mental, and social domains of health” (27). HRQoL captures information on both physical and mental health status and its impact on Quality of Life (QoL). It is a useful indicator of overall health and is suitable for prevention and early detection of physical or mental diseases (28–32). As a so-called “patient-reported outcome,” HRQoL comprises the perspective of patients, making it suitable for validating healthcare services and interventions and ensuring the provision of high-quality services (33). However, evidence on HRQoL in family caregivers of autistic adults is lacking, with only a handful of international studies on this topic (25, 26, 34–36), and no data from Europe. Still, existing evidence indicates that HRQoL of family caregivers of autistic adults is reduced – without HRQoL scores having been compared with other populations yet.
In attempt to identify the underlying mechanisms of this (presumed) finding, a number of potential predictors have been investigated. For instance, a systematic review by Sonido et al. (37) (N = 23 included studies) scrutinized potential predictors of mental wellbeing of family caregivers of autistic adults. Due to the limited amount of available evidence, a broad variety of outcomes were considered (e.g., psychological stress, mental wellbeing, HRQoL, QoL), without categorizing them as discrete components to provide discriminant evidence. In addition, the picture on several potential predictors is less clear-cut. Discrepant or lacking evidence has been identified for various caregiver-related and care recipient-related predictors: Regarding caregiver-related, and especially sociodemographic predictors, two studies found older caregivers having better mental wellbeing (26, 38), while other studies could not support this finding (39, 40). Furthermore, Grootscholten et al. (24) reported that parental and spousal caregivers show higher psychological burden (i.e., stress, depression, anxiety) compared to other family caregivers (e.g., siblings, children). With respect to school education, Greenberg et al. (40) found higher educated mothers to experience better psychological wellbeing, whereas other studies did not support such finding (22, 26, 38). In addition, predictors directly related to caregiving demands were examined: The higher the subjective caregiver burden, the lower the parental HRQoL (41). However, no significant associations were found between parental financial burden and actual time spent due to caregiving demands and HRQoL (26, 35).
Besides caregiver-related predictors, different care recipient-related predictors were assumed to be associated with family caregivers’ wellbeing, focusing on clinical and healthcare utilization outcomes. Rattaz et al. (22) found that more severe ASD symptoms in care recipients predicted lower caregivers’ global QoL. This prediction was not confirmed in other studies (21, 26) or only between severity of behavioral symptoms and parental HRQoL (42). Contradictory results were also found with respect to the presence of care recipients’ comorbid ID, with one study showing improved caregiver mental HRQoL when the care recipient has an ID (26), while other studies did not (39, 43). No significant associations were found between utilization of formal services by the care recipient and mental wellbeing outcomes in caregivers (26, 39). Moreover, in parents of autistic children, depressive symptoms increased when the child was diagnosed with ASD at a higher age (44). However, age at ASD diagnosis as a potential predictor of HRQoL and in caregivers of autistic adults has not been examined yet.
These previous published studies provide important evidence but reveal some limitations. First, the observed primary outcome differed highly over studies (e.g., psychological distress, mental-wellbeing, QoL, HRQoL). HRQoL was found to be a valuable outcome in various healthcare settings, but most predictors were investigated only in the context of the aforementioned related constructs. Moreover, when considering HRQoL, also very little is known about the distinction between mental and physical HRQoL. Second, the picture for several potential predictors is less clear. Inconsistent or lacking evidence has been identified for various caregiver-related and care recipient-related variables. Third, most studies included mainly parental caregivers and did not investigated, for example, partners/spouses and siblings (39, 42). Moreover, as comparisons to reference populations (e.g., non-clinical populations, family caregivers of relatives with other chronic diseases) are lacking, existing evidence cannot be interpreted properly.
Thus, the present study aimed for the first time to (i) investigate the current state of physical and mental HRQoL in family caregivers of autistic adults compared to the general population in Germany, and (ii) analyze a comprehensive set of previously reported caregiver-related and care recipient-related predictors of both physical and mental HRQoL in family caregivers of autistic adults. To our knowledge, this is the first broad investigation of physical and mental HRQoL in family caregivers of autistic adults. Results from this study might contribute important information by identifying parameters associated with impaired HRQoL in family caregivers and, consequently, providing an indication of the need for action within professional healthcare settings, with the long-term goal of improving the HRQoL in this underserved population, as called for by the scientific community (9, 37, 45).
2 Methods
This cross-sectional observational study was conducted as part of the research project BarrierfreeASD (46). Ethical approval was obtained from the Local Psychological Ethics Committee at the Center for Psychosocial Medicine at the University Medical Center Hamburg-Eppendorf (#LPEK-0227; Dec. 2020), and the study was conducted in accordance with the Declaration of Helsinki. Participation was voluntary and anonymous and informed consent was obtained before participation. An inconvenience allowance was not paid. The BarrierfreeASD project has been preregistered with the Open Science Framework.1 Two autistic researchers were part of the BarrierfreeASD project and were involved in developing the online survey, the data collection and the interpretation of the results. Furthermore, research was conducted in close collaboration with the study’s collaborative network, including autism-related associations and family caregiver-related associations, which guided the research process throughout. This manuscript was conducted in accordance with the Journal Article Reporting Standards for Quantitative Research in Psychology (JARS) (47).
2.1 Participants
This study analyzed data from N = 149 family caregivers of autistic adults. Participants were recruited throughout Germany using purposive, quota and snowball sampling methods via the study’s network of collaborating partners, publicly available contacts from autism-related associations (including self-help and caregiver groups), and social media. Therefore, response rates could not be calculated. Participants were included if they were at least 18 years old, a first- or second-degree relative or partner/spouse of an autistic adult (care-recipient), and had sufficient language skills. The nationwide online survey was distributed using LimeSurvey (48). The data collected included questions on sociodemographic and clinical information about the family caregiver, details about the autist adult, and details about the informal care provided (see measurement section for details). Sample characteristics of caregivers and care recipients are presented in Table 1.
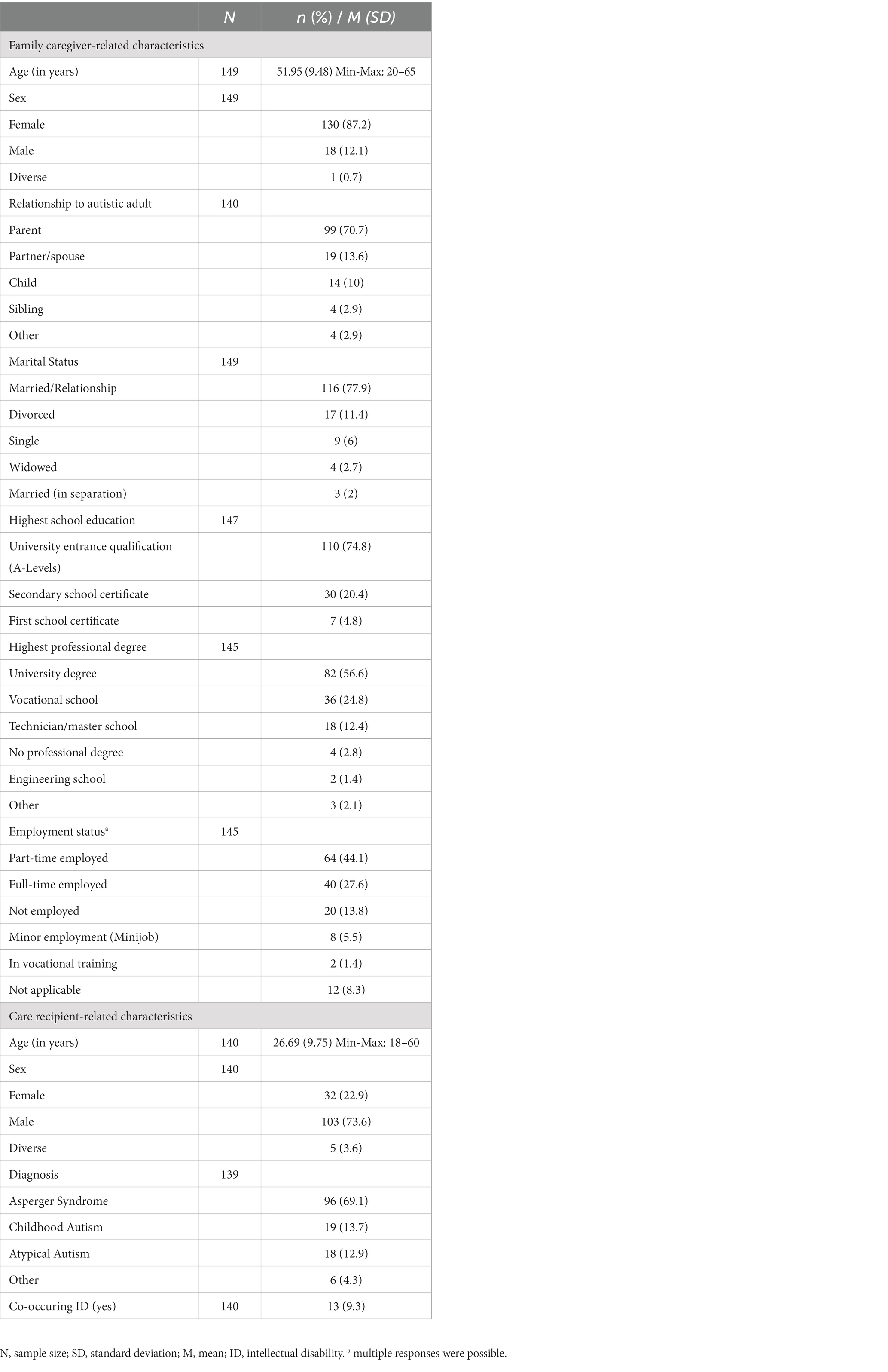
Table 1. Sample characteristics (N = 149).
2.2 Measurement
2.2.1 Caregiver-related measurements
Sociodemographic data about family caregivers included age, sex, marital status, relationship to an autistic relative, school education, and employment status. Treatment-related expenses were measured using the questionnaire of Mory et al. (49) which assesses treatment-related expenses (e.g., medication, co-payments for therapies), practical living support (e.g., rent, help in the household), and extraordinary expenses (e.g., debt repayments, special purchases) for the autistic relative in the past year (sum in Euro). Subjective caregiver burden was measured using the CarerQol-7D as a feasible, valid and reliable instrument (50, 51). Seven dimensions were included in the CarerQol-7D: fulfillment, relational, mental health, social, financial, perceived support, and physical dimension. Each item measured one dimension and was rated with “no,” “some,” or “a lot.” Tariff-based sum scores were calculated, ranging from 0 (worst informal care situation) to 100 (best informal care situation) (52). Objective caregiver burden. Self-developed items were used to measure the capacity of informal care. Participants were asked to indicate whether they had provided informal care for the adult relative with autism in the past 6 months. If they agreed, the number (in days) and the average duration per appointment (in hours) of each type of informal care (household, personal care, intake of medication, visits to administrative authorities, doctor’s appointments, finances, other) were estimated. For the purposes of this study, the total time for informal care (in hours) was calculated.
2.2.2 Care recipient-related measurements
Clinical information on the care recipient comprised the age at ASD diagnosis and the presence of an ID. As there was no standardized proxy measurement to assess the care-recipients’ symptom severity of ASD, family caregivers rated their relatives’ symptom severity based on two self-developed items analogous to the “Diagnostic and Statistical Manual of Mental Disorders” (DSM-5) (1) classification of severity/required support for the two main diagnostic criteria (A. Persistent deficits in social communication and social interaction, B. Restricted, repetitive patterns of behavior, interests, or activities). Family caregivers rated the following two items on a 5-point Likert scale (“1 = none” to “5 = severe”): “How much does your autistic relative require support due to difficulties in interpersonal communication and social interactions?” and “How much does your autistic relative require support because she/he is holding on to behavioral habits, routines, or interests (e.g., difficulties in self-organization or dealing with change)?” Ratings for the two domains were used as separate independent variables for the analyses. Number of received professional healthcare and support services in the past 6 month were collected using modified versions of the German Questionnaire for the Assessment of Health Services in Old Age (FIMA) (53) and the Questionnaire on the Utilization of Medical and Nonmedical Care Services in Mental Disorders (FIMPsy) (54).
2.2.3 Health-related quality of life (outcome)
Health-related Quality of Life (HRQoL) was measured using the Short-Form Health Survey (SF-8) because it is a generic instrument to assess HRQoL in physically and mentally health as well as in burdened populations (55). As a parsimonious and user-friendly instrument, each of the eight single-items assessed one dimension of the longer SF-36 health survey and allowed the calculation of a physical component scale (PCS) and a mental component scale (MCS) (56). Items were scored on a 5-point Likert scale and the PCS and MCS were derived using an algorithmic norm-based scoring procedure, with higher scores indicating better HRQoL (0–100) (55). The SF(−8/−12/−36) is used both nationally and internationally, which allows comparisons between different populations. Previous research has shown strong reliability (parallel test reliability r = 0.82) and validity of the MCS (55).
2.3 Data analysis
Data were analyzed using IBM SPSS version 27 (57). Missing data were not imputed. All decisions regarding the statistical significance of findings were made using a criterion alpha level of 0.05.
Three distinct analyses were performed. First, both physical and mental HRQoL scores (PCS and MCS of the SF-8) were compared with those of the general population in Germany (N = 2,552) using two two-tailed t-tests for independent samples (58). Normative data were taken from a study by Beierlein et al. (59). Interpretation of effect size (Cohen’s d) were based on the conventions of Cohen (60) (small effect size: d = 0.2, medium effect size: d = 0.5, large effect size: d = 0.8).
Second, bivariate correlational analyses (Pearson’s correlation for metric variables, point-biserial correlations for one dichotomous and one metric variable, and Phi coefficients for both dichotomous variables) were performed in order to examine correlations between physical and mental HRQoL and variables. Interpretation of effect sizes (r) were based on the conventions of Cohen (60) (small effect size: r = 0.10, medium effect size: r = 0.30, large effect size: r = 0.50).
Third, two multiple linear regression models (PCS and the MCS of the SF-8 as dependent variables) were calculated to examine potential predictors of the family caregivers’ physical and mental HRQoL as a comprehensive set of predictors. An a priori power calculation revealed a required sample size of N = 87, assuming a moderate to high effect of R2 = 0.18, based on effect sizes of previous studies, with a statistical power of 0.80 and an alpha level of 0.05 for 11 predictors (61). Multicollinearity between predictors was assessed using the variance inflation factor [VIF; critical VIF > 2.5 (62)]. All other assumptions of multiple regression analysis could also be verified (linearity, normality, homoscedasticity, independence of errors). Predictors were entered into regression analyses in continuous or binary categorical data format in one block. To be included in regression analyses, categorical variables with more than two values/categories were recoded into dichotomous format, e.g., relationship to care recipient (1 = parental caregiver, 0 = non-parental caregiver), education (1 = A-levels/tertiary school education, 0 = no A-levels), ID (1 = ID, 0 = no ID, see Table 2). Interpretations of effects sizes (R2) were based on the recommendations of Cohen (60) (small effect size: R2 = 0.01, medium effect size: R2 = 0.09, large effect size: R2 = 0.25). In order to compare the relative importance of predictors, dominance analysis was performed using R version 3.6.2 (63) package “yhat” (64). The General Dominance Weights (GDW) of predictors were calculated by averaging the squared semipartial correlations across all of the possible subset models. This measure indexes a variable’s contribution to the prediction of the dependent variable, by itself and in combination with the other predictors (65).
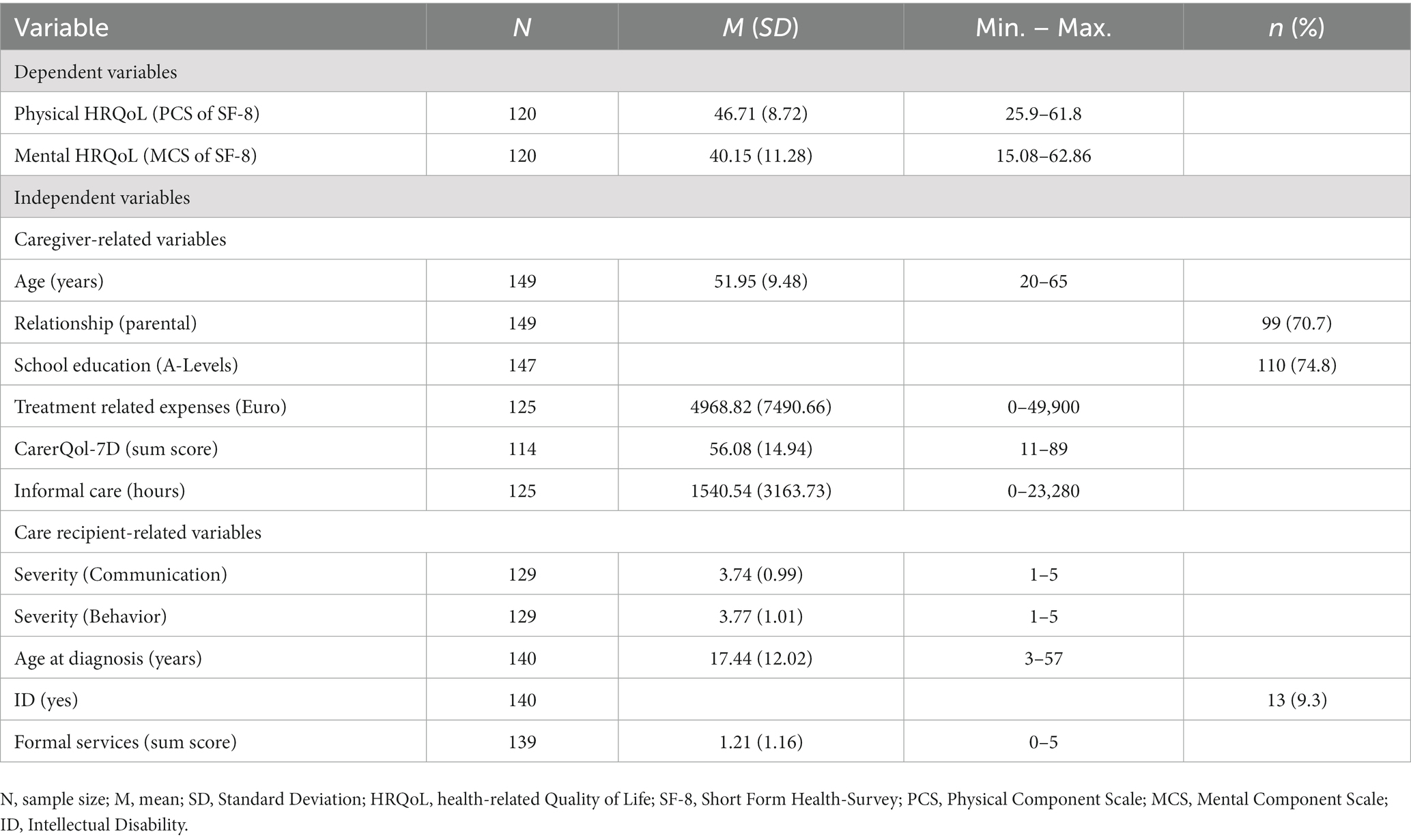
Table 2. Descriptive statistics of variables.
3 Results
Descriptive statistics of the dependent and independent variables are shown in Table 2.
3.1 Comparison of HRQoL with general population
Physical HRQoL. Data of the study (N = 120) showed a mean PCS score of M = 46.71 (SD = 8.72; see Figure 1). The German normative sample (N = 2,552) (59) rated a mean PCS score of M = 50.3 (SD = 8.39,). T-test for independent samples indicated that the difference between the two samples was statistically significant for the PCS [t(129.58) = 4.42, p < 0.001, Cohen’s d = 0.42], indicating a significantly lower physical HRQoL for caregivers of autistic adults compared to the general population with a small effect (60).
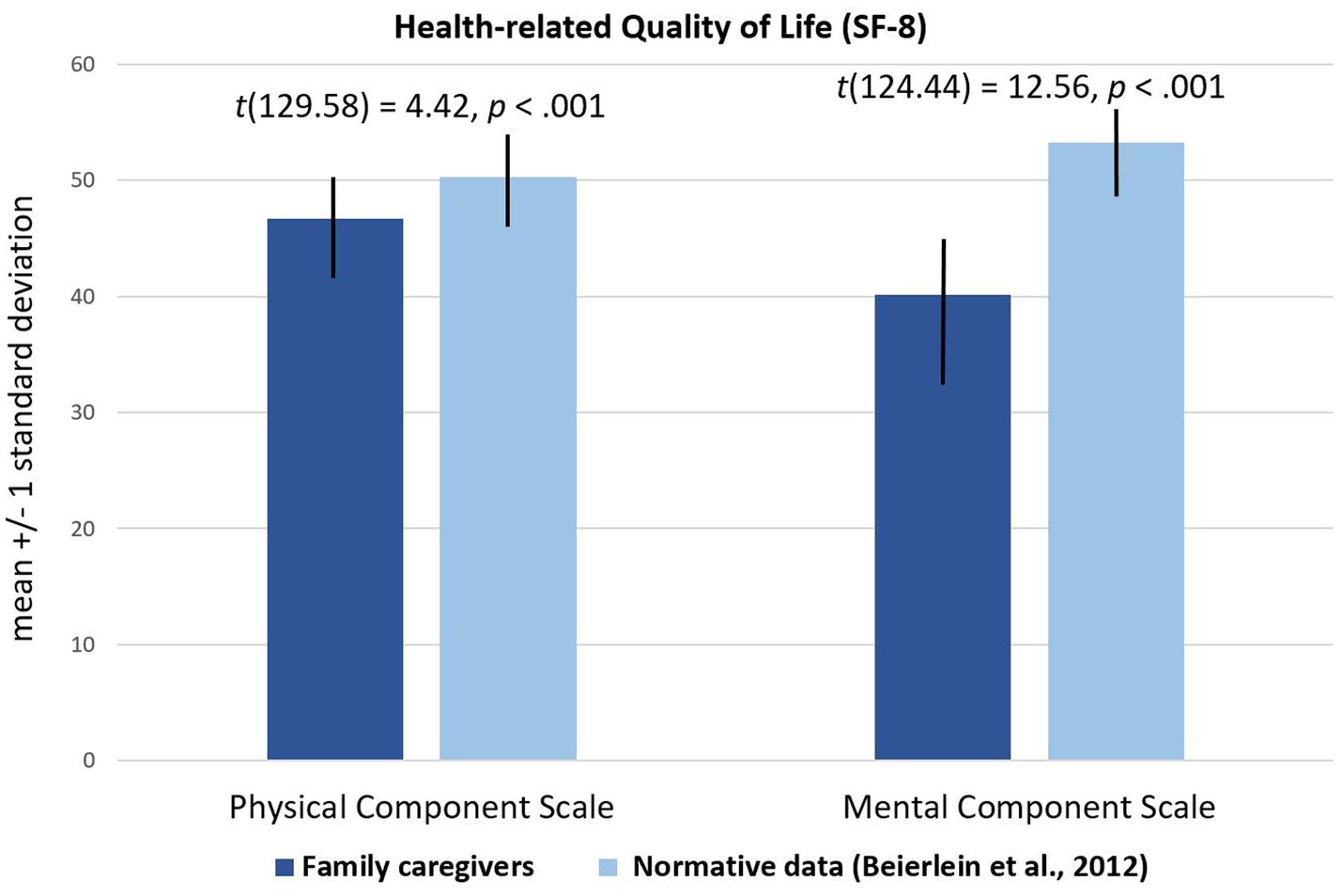
Figure 1. Comparison of HRQoL in family caregivers of autistic adults and in the general population.
Mental HRQoL. Data of the study (N = 120) showed a mean MCS score of M = 40.15 (SD = 11.28; see Figure 1). Normative data from Germany (59) reported for the general population (N = 2,552) a mean MCS score of M = 53.23 (SD = 7.82). T-test for independent samples revealed statistically significant difference for MCS scores [t(124.44) = 12.56; p < 0.001, Cohen’s d = 1.35], indicating a significantly lower mental HRQoL for caregivers of autistic adults compared to the general population with a large effect (60).
3.2 Correlation analyses
Bivariate analyses found several significant weak to high correlations between included HRQoL and predictors (see Table 3 for details) (60). Physical HRQoL was significantly positively correlated with the subjective caregiver burden (r = 0.20, p = 0.031) and negatively correlated with the symptom severity regarding behavior symptoms (r = −0.21, p = 0.024). Mental HRQoL was positively correlated with caregiver’s age (r = 0.19, p = 0.035), subjective caregiver burden (r = 0.44, p < 0.001), care recipient’s comorbid ID (r = 0.18, p = 0.048), and the amount of received formal services (r = 0.21, p = 0.005). Inverse correlations were found with the school education (r = −0.27, p = 0.003) and the symptom severity regarding behavior symptoms (r = −0.27, p = 0.005). Remaining variables did not show significant correlations with the physical and mental HRQoL.
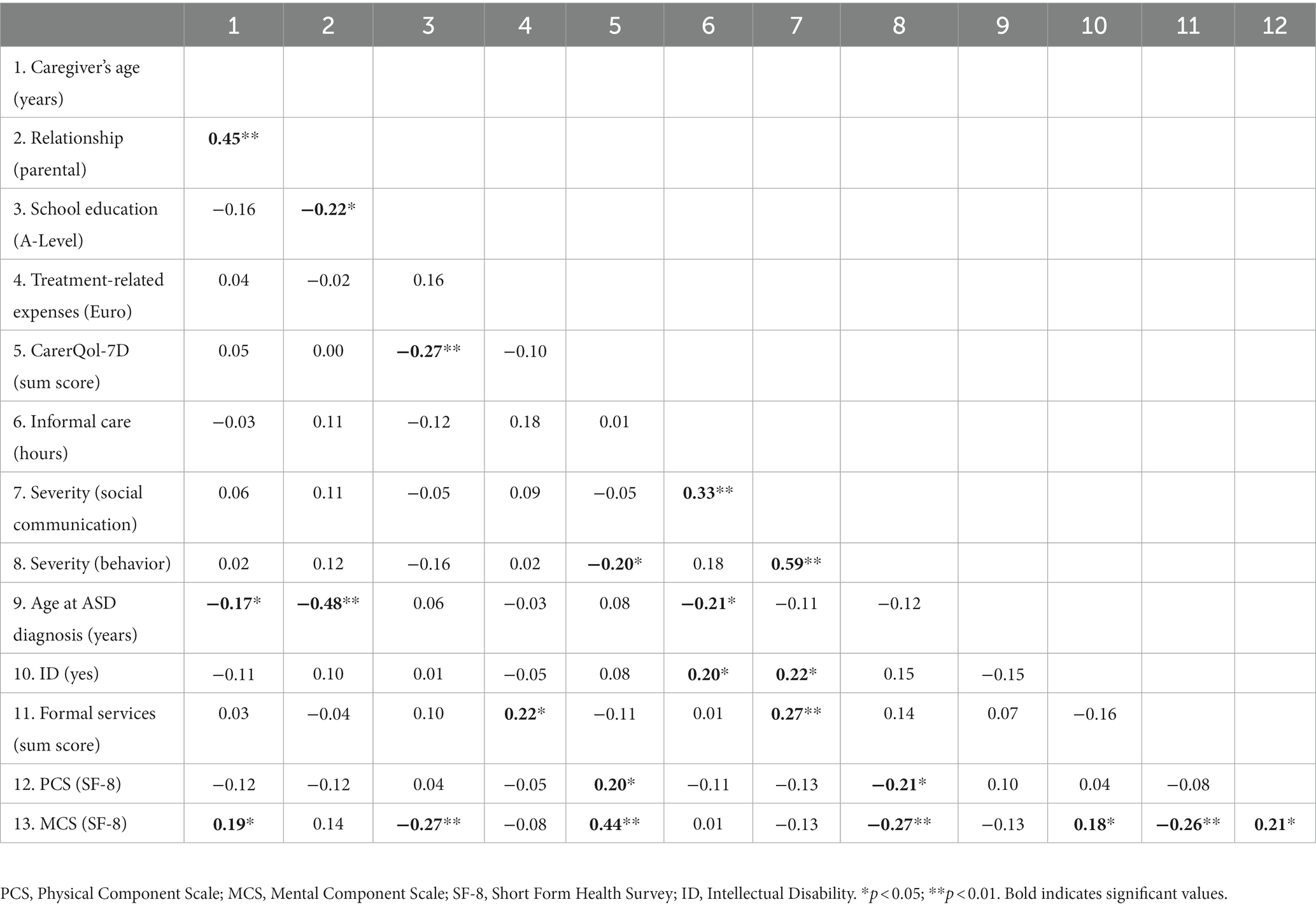
Table 3. Correlation matrix (N = 120).
3.3 Predictors of HRQoL
Multiple linear regression analysis with the outcome PCS scores did not reveal a statistically significant model [F(11, 95) = 1.09, p = 0.38]. For details, see Table 4.
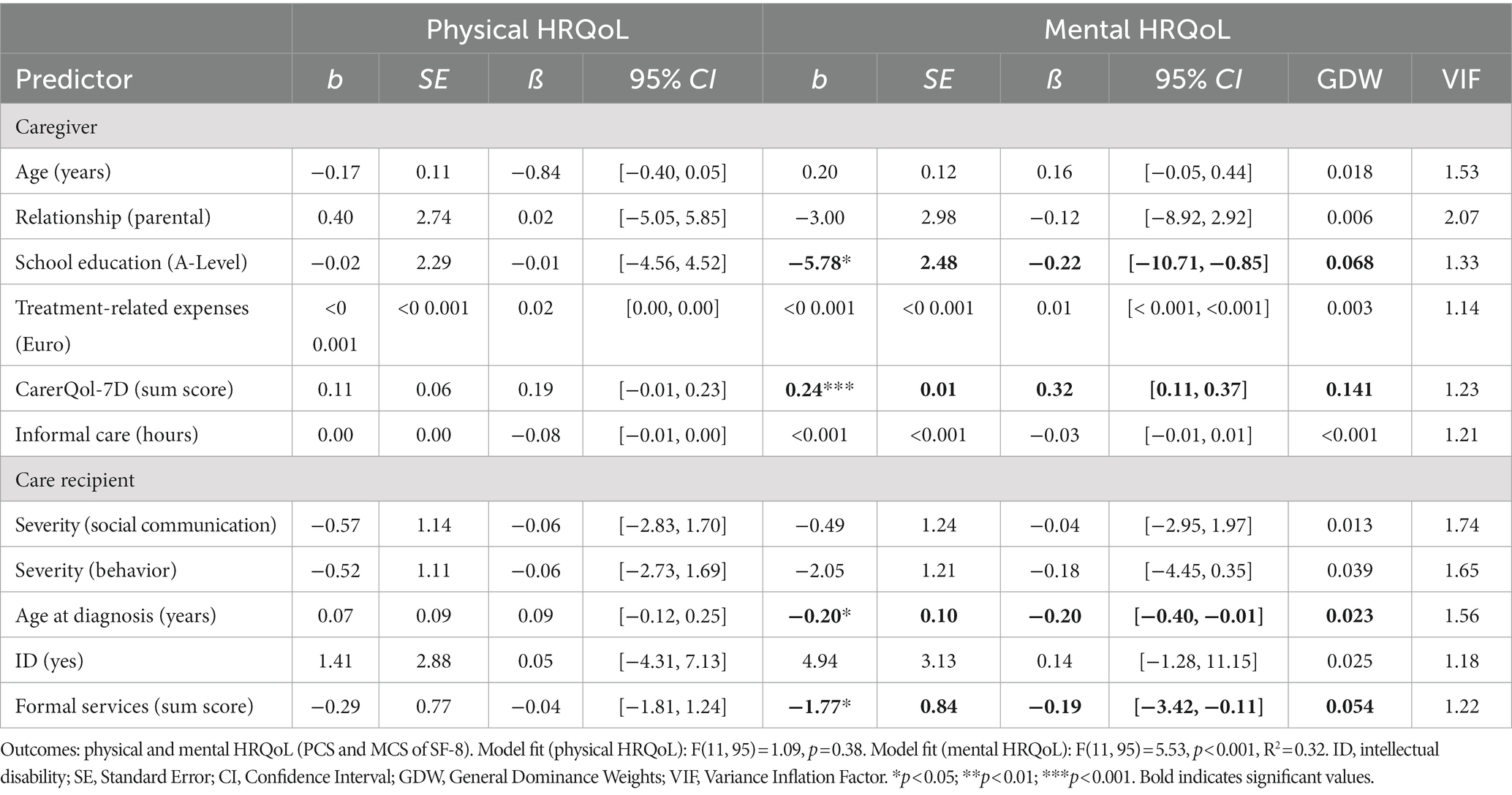
Table 4. Multiple linear regression analyses (N = 107).
Multiple linear regression with the mental HRQoL as the outcome showed a significant model [F(11, 95) = 5.53, p < 0.001], with an adjusted R2 of 0.32 (see Table 4). Significant results were obtained for the following caregiver variables: school education (ß = −0.22, GDW = 0.068, p < 0.05) and CarerQol-7D sum score (ß = 0.32, GDW = 0.141, p < 0.001). Higher school education and lower CarerQol-7D sum scores predicted lower MCS scores. For care recipient variables, the age at diagnosis (ß = −0.20, GDW = 0.023, p < 0.05) and the number of formal services (ß = −0.19, GDW = 0.054, p < 0.05) were significant predictors: high age at diagnosis and a higher number of formal services used by the autistic adult predicted lower mental HRQoL. Remaining predictors were not significant.
4 Discussion
To our knowledge, the present study is the first to provide an assessment of physical and mental HRQoL in family caregivers of autistic adults in Germany. The main results show that both mental and physical HRQoL were significantly reduced compared to the German normative population. Especially family caregivers’ mental HRQoL was considerably lower than that of the normative population. To shed light on the reduced HRQoL, bivariate analyses was conducted in order to detect correlations between the physical and mental HRQoL and the variables: Subjective caregiver burden and ASD severity in terms of repetitive and restrictive behaviors, interests, and activities correlated with both physical and mental HRQoL. Furthermore, a comprehensive set of potential predictors of HRQoL was examined: The set of variables investigated in this study showed that the strongest predictor of mental HRQoL was the subjective caregiver burden. Understanding the underlying causes of reduced HRQoL in family caregivers of autistic adults might help to inform professionals in the healthcare system about especially vulnerable individuals and to develop and decide about adequate support strategies.
4.1 Reduced HRQoL in family caregivers of autistic adults
In contrast to previous studies, the reported HRQoL scores were compared to the general population to provide a reference. Here, family caregivers of autistic adults reported significantly lower physical and mental HRQoL compared to the German general population. The HRQoL scores found in the current study are comparable to a study from the United States that investigated HRQoL in parental caregivers of young autistic adults (25), suggesting a ubiquitously reduced HRQoL in caregivers of autistic adults regardless of country of origin. However, the mental HRQoL scores in our study were slightly lower than the findings of Lee and Shivers (25). In addition, compared to family caregivers of patients with severe mental illness (66) or Down Syndrome (67), participants in the current study reported the lowest mental HRQoL scores. It is questionable whether, for example, autism-specific care needs or differences in healthcare structures due to regional disparities or inequalities in the healthcare of autistic adults and their family caregivers compared to other mental or physical disorders lead to these findings. As poor HRQoL scores are associated with several negative outcomes in the general population such as multimorbidity (68) or higher mortality risk (69), these findings are a matter of great concern and should motivate the development of support systems. Furthermore, the findings emphasize the importance of HRQoL as a relevant outcome not only in autistic adults but also in their family caregivers in order to obtain early indications of the family caregivers’ health status (70). Professionals working with autistic adults and their families should be aware that provided care may have an impact on the physical and mental health status (41). In addition, the findings highlight the need to address the lack of evidence on physical HRQoL in future research.
4.2 Bivariate and multiple regression analyses of family caregivers’ HRQoL
The results of this study revealed caregiver-related and care recipient-related predictors explaining variance of HRQoL in family caregivers of autistic adults, which were predominantly differing between the two outcomes physical and mental HRQoL. However, two variables showed significant correlations with both physical and mental HRQoL in the bivariate analyses: Subjective caregiver burden and ASD severity regarding repetitive and restrictive behaviors, interests, and activities. Also in the multiple regression model with the mental HRQoL as dependent variable, subjective caregiver burden explained most variance in family caregivers’ mental HRQoL. That is, the lower the perceived caregiver burden, the higher the mental HRQoL [in line with (26, 41)]. As described before, caregiver burden entails the demands, challenges, and stressors experienced by those who are providing care (41) on several dimensions, i.e., negative feelings resulting from informal caregiving, lack of support from family and friends, relationship problems, mental and physical health problems, problems with activities of daily living, and financial problems due to caregiving responsibilities (50). The present results indicate that the sum of these dimensions of caregiver burden explain variance in the mental (and in the bivariate analyses also in the physical) HRQoL, but it remains unclear whether certain dimensions clarify more/less variance in HRQoL compared to others, so that precise support approaches to reduce perceived caregiver burden cannot yet be defined. Interestingly, more objective indicators of caregiver burden (i.e., capacity of informal care) did not significantly predict the HRQoL (26), suggesting that it is not the actual care provided, but the individual’s perception of the care situation that has an impact on the HRQoL. This provides an initial benchmark for developing appropriate services, such as psychosocial interventions. Evidence is lacking, but first data on interventions for parents of autistic youth and adults seem promising, as mindfulness-based group interventions significantly reduced parental stress (71, 72). In addition to formal services, informal social support (i.e., support from unpaid sources such as family members, friends, or acquaintances) was found to reduce both subjective caregiver burden and mental HRQoL (41).
Better school education has previously been reported to increase maternal mental well-being (40). Interestingly, our data revealed a significant inverse association, indicating that higher school education predicted lower mental HRQoL. It is possible that family caregivers with higher school education tend to have, in turn, higher ambitions for their own lives and for the life of their care recipients, but are constrained by the demands of caregiving. Well-educated people were found to have higher levels of dissatisfaction, and mental distress was largely reduced by paid work (73), but employment is often negatively affected by caregiving demands among caregivers of autistic adults. Such associations need to be investigated in future research.
To our knowledge, this is the first study to show an association between care recipient’s age at ASD diagnosis and family caregiver’s mental HRQoL with an inverse relationship: Higher age at diagnosis predicted lower mental HRQoL. As mentioned in the Introduction, autistic adults face massive healthcare barriers, such as long waiting lists for diagnostics (3, 9, 10, 74). Delayed diagnosis might lead to delayed receipt of appropriate formal support. Such associations need further investigation, but it can be assumed that inadequate healthcare structures for autistic adults affect the whole family.
As expected by Sonido et al. (37), a higher amount of received formal services predicted lower mental HRQoL among family caregivers. The number of formal services could be a proxy for care recipients’ symptom severity and/or treatment needs. However, there was only a weak correlation between formal services and the severity of social interaction and communication symptoms. Recent studies have shown that the presence of care recipient’s depression (26) and general health deterioration (75) are associated with reduced caregiver well-being, but associations with HRQoL need to be clarified in future research. Furthermore, many family caregivers have had negative experiences with formal services (18), which may account for the negative association. In addition, in line with previous research, the presence of an ID (26) and higher caregiver’s age (26, 38) correlated with better mental HRQoL (only) in the bivariate analyses. Previous evidence confirmed that autistic adults without ID often report higher healthcare needs and barriers to accessing appropriate healthcare (76–78).
The remaining predictors were not found to significantly explain the variance of mental HRQoL in the current study, as was the relationship with the autistic adult. In contrast to Grootscholten et al. (24), the current study mainly included parental caregivers, which may result in a lack of variance to detect potential differences between different relationship groups (i.e., parents, siblings, spouses). Moreover, differences between maternal and paternal caregivers were not examined in the current study. Research on parents has shown that mothers often focus on caring for the autistic child and thus have a more intense bonding (79, 80). Nonetheless, in a recent meta-analysis, parental gender did not emerge as a significant moderator of proportions of levels of parental psychopathology, but the authors called for further investigation (81). Moreover, treatment-related costs were not associated with the family caregivers’ mental HRQoL even when family caregivers reported high amounts of care-related costs (35). This finding differed from qualitative findings (20), as almost all participating parental caregivers complained about the financial constraints they faced. Buescher et al. (82) also reported substantial costs for caregivers of autistic adults, such as medical services, employment support or accommodations, which can have a tremendous impact on families. Due to the high proportion of highly educated caregivers in the current study, the income of the sample is expected to be relatively high. In addition, the positive correlation between school education and treatment-related expenses showed that family caregivers with higher education reported more treatment-related expenses. Therefore, further research should examine the subjective financial burden.
Similar to mental HRQoL findings, subjective caregiver burden also correlated with the physical HRQoL with a small effect size, as caregiving may have negative long-term physical effects (e.g., fatigue, muscular tension, physiological exhaustion). Another correlation was found between the physical HRQoL and the severity of care-recipients’ ASD symptoms of repetitive, restrictive, and stereotype behaviors with an expected inverse relationship: The more severe the symptoms, the lower the physical HRQoL (22, 42). Managing the behavioral characteristics of care recipients may be a stressor for family caregivers, which is in accordance with research on caregivers of Alzheimer’s patients (83). In contrast, ASD symptom severity regarding specifics of social interactions and communication did not explain variance in this study [cf. (42)].
Nonetheless, the multiple linear regression model with physical HRQoL as the outcome was not statistically significant. The selection of predictors in this study was based on previous evidence that mainly focused on mental HRQoL without considering physical HRQoL, which could explain the lack of significance. Other variables that were not included in our analyses could explain more variance in family caregivers’ physical HRQoL, such as family caregivers’ mental and physical illness, social support, or coping strategies (26, 66).
4.3 Limitations and future directions
There are limitations that need to be considered in future research. First, because this was a cross-sectional study, no conclusions about causal relationships between variables and HRQoL can be drawn. Longitudinal studies would help to further describe the HRQoL of family caregivers of autistic adults over time in order to identify possible well-suited time points for different types of interventions to support caregivers. Second, a post-hoc analysis to attempt to estimate the power of the regression coefficients showed insufficient power (84). A sample size of approximately 250 relatives would have been required to achieve adequate power. Third, as no more recent SF-8 normative data from Germany exists, normative data collected in 2004 were used (59). Recent longitudinal data from the German general population showed that the overall HRQoL increased in the meantime (85). Taking this finding into account, the difference between the normative sample and the caregiver sample might be even larger, but further investigations are needed. In addition, study population and normative population were not stratified, for example, by age or gender, because these data were not available from the normative sample. Fourth, the generalizability of the data was limited by the characteristics of the sample. For example, the majority of the current sample were mothers with high levels of education and professional degree. Maternal perspectives are important but may not necessarily reflect those of other family members (8). Equal proportions of family members are needed, to examine possible differences in terms of different relationships with the autistic adult (e.g., spouses, siblings, children). Finally, family caregivers rated their relative’s symptom severity using self-developed items without prior psychometric validation.
5 Conclusion and implications
Family caregivers of autistic adults represent a highly under-recognized population in clinical research, healthcare, society, and policy. To our knowledge, this is the first study to comprehensively assess the physical and mental HRQoL of this population in Germany, not only by comparing the HRQoL of family caregivers with the general population, but also by identifying potential predictors. The results outlined considerably lower physical and mental HRQoL compared to the general population, emphasizing the need for action to improve family caregivers’ HRQoL, as well as certain implications for future research and healthcare. Especially the subjective burden of care was found to have impact on both dimensions of HRQoL in this study and seems to be a promising candidate for interventions. In addition to the few emerging studies on family caregivers’ mental HRQoL, the current findings reveal that physical HRQoL might depend on other predictors as mental HRQoL. There is a lack of research investigating this aspect: What causes the lower physical HRQoL? Moreover, healthcare providers working with autistic adults and their families should be aware of the potential impairment of caregivers’ health status and form a routine to assess and monitor caregivers’ HRQoL, for example as part of the intake assessment or in primary care (86). Further longitudinal research assessing diverse samples of family caregivers of autistic adults is needed, to elucidate specific underlying mechanisms and potential risk factors for HRQoL in this heterogeneous, complex population (9, 26, 45).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Local Psychological Ethics Committee at the Center for Psychosocial Medicine at the University Medical Center Hamburg-Eppendorf. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SD: Conceptualization, Data curation, Formal analysis, Investigation, Supervision, Visualization, Writing – original draft, Writing – review & editing. SB: Formal analysis, Writing – original draft, Writing – review & editing. PG: Investigation, Writing – original draft, Writing – review & editing. HK: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. DS: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing. AK: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing. PR: Investigation, Writing – original draft, Writing – review & editing. FE: Writing – original draft, Writing – review & editing, Investigation. KV: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing. HS: Conceptualization, Data curation, Funding acquisition, Investigation, Project administration, Writing – original draft, Writing – review & editing, Supervision, Validation. ND: Conceptualization, Funding acquisition, Investigation, Project administration, Writing – original draft, Writing – review & editing. JP: Conceptualization, Formal analysis, Funding acquisition, Investigation, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by the Innovation Fund of the German Federal Joint Committee of Health Insurance Companies [Gemeinsamer Bundesausschuss, G-BA, study title “BarrierefreiASS” (01VSF19011)] and we acknowledge financial support from the Open Access Publication Fund of UKE – University Medical Center Hamburg-Eppendorf and DFG – German Research Foundation. The funding body had no role in the design of the study or in writing the manuscript, nor did they have a role in data collection, analyses or interpretation of data.
Acknowledgments
The authors sincerely thank all participants, who took part in the study. Furthermore, we would like to acknowledge the support of our cooperation partners in recruitment of study participants: the Autism Research Cooperation (afk), autSocial e.V., the Federation of Autism in Germany (Autismus Deutschland e.V.), the Parent Association Autismus Hamburg e.V., the Autism Institute of Hamburg, the Autism Institute of Lübeck, the Autism Strategy for Bavaria (Prof. M. Witzmann & E. Kunerl), Practice for Psychotherapy Aida Knabe, and the Department of Child and Adolescence Psychiatry and Psychotherapy of the University Medical Center Hamburg-Eppendorf. In addition, we would like to thank Tabea Horstmann, a student research assistant, who supported data preparation. Finally, we would like to thank Lukas Lange-Drenth, PhD for his excellent support in the statistical analyses.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. VA: Arlington (2013).
2. Croen, LA, Zerbo, O, Qian, Y, Massolo, ML, Rich, S, Sidney, S, et al. The health status of adults on the autism spectrum. Autism. (2015) 19:814–23. doi: 10.1177/1362361315577517
3. Vohra, R, Madhavan, S, and Sambamoorthi, U. Comorbidity prevalence, healthcare utilization, and expenditures of Medicaid enrolled adults with autism spectrum disorders. Autism. (2017) 21:995–1009. doi: 10.1177/1362361316665222
4. Maenner, MJ, Shaw, KA, Baio, J, Washington, A, Patrick, M, DiRienzo, M, et al. Prevalence of autism Spectrum disorder among children aged 8 years — autism and developmental disabilities monitoring network, 11 sites, United States, 2016. Morb Mortal Wkly Rep. (2020) 69:1–12. doi: 10.15585/mmwr.ss6904a1
5. Postorino, V, Fatta, LM, Sanges, V, Giovagnoli, G, De Peppo, L, Vicari, S, et al. Intellectual disability in autism Spectrum disorder: investigation of prevalence in an Italian sample of children and adolescents. Res Dev Disabil. (2016) 48:193–201. doi: 10.1016/j.ridd.2015.10.020
6. Järbrink, K, Fombonne, E, and Knapp, M. Measuring the parental, service and cost impacts of children with autistic Spectrum disorder: a pilot study [article]. J Autism Dev Disord. (2003) 33:395–402. doi: 10.1023/a:1025058711465
7. Cadman, T, Eklund, H, Howley, D, Hayward, H, Clarke, H, Findon, J, et al. Caregiver burden as people with autism spectrum disorder and attention-deficit/hyperactivity disorder transition into adolescence and adulthood in the United Kingdom. J Am Acad Child Adolesc Psychiatry. (2012) 51:879–88. doi: 10.1016/j.jaac.2012.06.017
8. Cridland, EK, Jones, SC, Magee, CA, and Caputi, P. Family-focused autism spectrum disorder research: a review of the utility of family systems approaches. Autism. (2014) 18:213–22. doi: 10.1177/1362361312472261
9. Lord, C, Charman, T, Havdahl, A, Carbone, P, Anagnostou, E, Boyd, B, et al. The Lancet Commission on the future of care and clinical research in autism. Lancet. (2022) 399:271–334. doi: 10.1016/S0140-6736(21)01541-5
10. Dückert, S, Gewohn, P, Konig, H, Schottle, D, Konnopka, A, Rahlff, P, et al. Barriers and needs in mental healthcare of adults with autism spectrum disorder in Germany: a qualitative study in autistic adults, relatives, and healthcare providers. BMC Psychiatry. (2023) 23:528. doi: 10.1186/s12888-023-05026-x
11. Malik-Soni, N, Shaker, A, Luck, H, Mullin, AE, Wiley, RE, Lewis, MES, et al. Tackling healthcare access barriers for individuals with autism from diagnosis to adulthood. Pediatr Res. (2022) 91:1028–35. doi: 10.1038/s41390-021-01465-y
12. Phelps, KW, Hodgson, JL, McCammon, SL, and Lamson, AL. Caring for an individual with autism disorder: a qualitative analysis. J Intellect Dev Disabil. (2009) 34:27–35. doi: 10.1080/13668250802690930
13. Swaab, L, McCormack, L, and Campbell, LE. Distress and psychological growth in parenting an adult child with autism Spectrum disorder and aggression. Advan Neurodevelop Disor. (2017) 1:260–70. doi: 10.1007/s41252-017-0033-5
14. Altiere, MJ, and von Kluge, S. Searching for acceptance: challenges encountered while raising a child with autism. J Intellect Dev Disabil. (2009) 34:142–52. doi: 10.1080/13668250902845202
15. Marsack, CN, and Perry, TE. Aging in place in every community: social exclusion experiences of parents of adult children with autism Spectrum disorder. Res Aging. (2018) 40:535–57. doi: 10.1177/0164027517717044
16. Marsack-Topolewski, CN, and Wang, F. Dimensions of caregiver burden between compound and noncompound caregivers of adults with autism. J Gerontol Soc Work. (2022) 65:402–20. doi: 10.1080/01634372.2021.1969609
17. Marsack, CN, and Hopp, FP. Informal support, health, and burden among parents of adult children with autism. Gerontologist. (2019) 59:1112–21. doi: 10.1093/geront/gny082
18. Hare, DJ, Pratt, C, Burton, M, Bromley, J, and Emerson, E. The health and social care needs of family carers supporting adults with autistic spectrum disorders. Autism. (2004) 8:425–44. doi: 10.1177/1362361304047225
19. Hines, M, Balandin, S, and Togher, L. The stories of older parents of adult sons and daughters with autism: a balancing act. J Appl Res Intellect Disabil. (2014) 27:163–73. doi: 10.1111/jar.12063
20. Oti-Boadi, M, Oppong Asante, K, and Malm, EK. The experiences of ageing parents of young adults with autism Spectrum disorders (ASD) [article]. J Adult Dev. (2020) 27:58–69. doi: 10.1007/s10804-018-09325-6
21. Barker, ET, Hartley, SL, Seltzer, MM, Floyd, FJ, Greenberg, JS, and Orsmond, GI. Trajectories of emotional well-being in mothers of adolescents and adults with autism. Dev Psychol. (2011) 47:551–61. doi: 10.1037/a0021268
22. Rattaz, C, Michelon, C, Roeyers, H, and Baghdadli, A. Quality of life in parents of young adults with ASD: EpiTED cohort. J Autism Dev Disord. (2017) 47:2826–37. doi: 10.1007/s10803-017-3197-y
23. Tomeny, T, Barry, T, Fair, E, and Riley, R. Parentification of adult siblings of individuals with autism Spectrum disorder [article]. J Child Fam Stud. (2017) 26:1056–67. doi: 10.1007/s10826-016-0627-y
24. Grootscholten, IAC, van Wijngaarden, B, and Kan, CC. High functioning autism Spectrum disorders in adults: consequences for primary caregivers compared to schizophrenia and depression. J Autism Dev Disord. (2018) 48:1920–31. doi: 10.1007/s10803-017-3445-1
25. Lee, GK, and Shivers, CM. Factors that affect the physical and mental health of caregivers of school-age children and transitioning young adults with autism spectrum disorder. J Appl Res Intellect Disabil. (2019) 32:622–34. doi: 10.1111/jar.12556
26. Sonido, MT, Hwang, YI, Srasuebkul, P, Trollor, JN, and Arnold, SRC. Predictors of the quality of life of informal Carers of adults on the autism Spectrum. J Autism Dev Disord. (2022) 52:2997–3014. doi: 10.1007/s10803-021-05178-3
27. Hays, RD, and Reeve, BB. Measurement and modeling of health-related quality of life In: J Killewo, HK Heggenhougen, and SR Quah, editors. Epidemiology and demography in public health. US: Academic Press (2010). 195–205.
28. Palermo, TM, Long, AC, Lewandowski, AS, Drotar, D, Quittner, AL, and Walker, LS. Evidence-based assessment of health-related quality of life and functional impairment in pediatric psychology. J Pediatr Psychol. (2008) 33:983. doi: 10.1093/jpepsy/jsn038
29. Revicki, DA, Kleinman, L, and Cella, D. A history of health-related quality of life outcomes in psychiatry. Dialogues Clin Neurosci. (2014) 16:127–35. doi: 10.31887/DCNS.2014.16.2/drevicki
30. Romero, M, Vivas-Consuelo, D, and Alvis-Guzman, N. Is health related quality of life (HRQoL) a valid indicator for health systems evaluation? Springer Plus. (2013) 2:664. doi: 10.1186/2193-1801-2-664
31. Ware, JE, Kosinski, M, and Keller, SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. (1996) 34:220–33. doi: 10.1097/00005650-199603000-00003
32. Yin, S, Njai, R, Barker, L, Siegel, PZ, and Liao, Y. Summarizing health-related quality of life (HRQOL): development and testing of a one-factor model. Popul Health Metr. (2016) 14:22. doi: 10.1186/s12963-016-0091-3
33. Churruca, K, Pomare, C, Ellis, LA, Long, JC, Henderson, SB, Murphy, LED, et al. Patient-reported outcome measures (PROMs): a review of generic and condition-specific measures and a discussion of trends and issues. Health Expect. (2021) 24:1015–24. doi: 10.1111/hex.13254
34. Marsack-Topolewski, CN. Quality of life among compound caregivers and noncompound caregivers of adults with autism. J Gerontol Soc Work. (2020b) 63:379–91. doi: 10.1080/01634372.2020.1765063
35. Marsack-Topolewski, CN, and Church, HL. Impact of caregiver burden on quality of life for parents of adult children with autism Spectrum disorder. Am J Intellect Dev Disabil. (2019) 124:145–56. doi: 10.1352/1944-7558-124.2.145
36. Marsack, CN, and Samuel, PS. Mediating effects of social support on quality of life for parents of adults with autism. J Autism Dev Disord. (2017) 47:2378–89. doi: 10.1007/s10803-017-3157-6
37. Sonido, MT, Hwang, YI, Trollor, JN, and Arnold, SRC. The mental well-being of informal Carers of adults on the autism Spectrum: a systematic review. Rev J Autism Develop Disor. (2019) 7:63–77. doi: 10.1007/s40489-019-00177-8
38. Smith, LE, Hong, J, Seltzer, MM, Greenberg, JS, Almeida, DM, and Bishop, SL. Daily experiences among mothers of adolescents and adults with autism Spectrum disorder. J Autism Dev Disord. (2010) 40:167–78. doi: 10.1007/s10803-009-0844-y
39. Burke, M, and Heller, T. Individual, parent and social-environmental correlates of caregiving experiences among parents of adults with autism spectrum disorder. J Intellect Disabil Res. (1997) 60:401–11. doi: 10.1111/jir.12271
40. Greenberg, JS, Seltzer, MM, Krauss, MW, Chou, RJ, and Hong, J. The effect of quality of the relationship between mothers and adult children with schizophrenia, autism, or down syndrome on maternal well-being: the mediating role of optimism. Am J Orthopsychiatry. (2004) 74:14–25. doi: 10.1037/0002-9432.74.1.14
41. Marsack-Topolewski, CN. Mediating effects of social support on caregiver burden and quality of life for compound and noncompound caregivers. Families in Society: J Contemporary Soc Services. (2021) 102:240–52. doi: 10.1177/1044389420947229
42. Marsack-Topolewski, CN, and Maragakis, A. Relationship between symptom severity and caregiver burden experienced by parents of adults with autism. Focus on Autism Other Develop Disab. (2020) 36:57–65. doi: 10.1177/1088357620956927
43. Herrema, R, Garland, D, Osborne, M, Freeston, M, Honey, E, and Rodgers, J. Mental wellbeing of family members of autistic adults [article]. J Autism Dev Disord. (2017) 47:3589–99. doi: 10.1007/s10803-017-3269-z
44. Gray, DE, and Holden, WJ. Psycho-social well-being among the parents of children with autism. Australia and New Zealand J Develop Disab. (2009) 18:83–93. doi: 10.1080/07263869200034841
45. AWMF. (2021). S3 guidelines report: Autism spectrum disorders in childhood, adolescence and adulthood, part 2: Therapy (028–047). Available at: https://www.awmf.org/leitlinien/detail/ll/028-047.html.
46. David, N, Dückert, S, Gewohn, P, Konig, H, Rahlff, P, Erik, F, et al. Mixed-methods investigation of barriers and needs in mental healthcare of adults with autism and recommendations for future care (Barrierfree ASD): study protocol. BMJ Open. (2022) 12:e061773. doi: 10.1136/bmjopen-2022-061773
47. Appelbaum, M, Cooper, H, Kline, RB, Mayo-Wilson, E, Nezu, AM, and Rao, SM. Journal article reporting standards for quantitative research in psychology: the APA publications and communications board task force report. Am Psychol. (2018) 73:3–25. doi: 10.1037/amp0000191
48. Lime Survey GmbH. LimeSurvey: An open source survey tool/LimeSurvey GmbH, Hamburg, Germany. (2020). Available at: http://www.limesurvey.org
49. Mory, C, Jungbauer, J, Bischkopf, J, and Angermeyer, MC. Finanzielle Belastungen von Partnern psychisch Erkrankter. [financial burden on spouses of Patiens suffering from schizophrenia, depression or anxiety disorder.]. Fortscht Neurol Psychiat. (2002) 70:71–7. doi: 10.1055/s-2002-19919
50. Brouwer, WB, van Exel, NJ, van Gorp, B, and Redekop, WK. The Carer Qol instrument: a new instrument to measure care-related quality of life of informal caregivers for use in economic evaluations. Qual Life Res. (2006) 15:1005–21. doi: 10.1007/s11136-005-5994-6
51. Hoefman, RJ, van Exel, NJ, Foets, M, and Brouwer, WB. Sustained informal care: the feasibility, construct validity and test-retest reliability of the Carer Qol-instrument to measure the impact of informal care in long-term care. Aging Ment Health. (2011) 15:1018–27. doi: 10.1080/13607863.2011.575351
52. Hoefman, RJ, van Exel, J, and Brouwer, WBF. Measuring care-related quality of life of caregivers for use in economic evaluations: Carer Qol tariffs for Australia, Germany, Sweden, UK, and US. Pharmacoeconomics. (2017) 35:469–78. doi: 10.1007/s40273-016-0477-x
53. Seidl, H, Bowles, D, Bock, JO, Brettschneider, C, Greiner, W, Konig, HH, et al. FIMA--questionnaire for health-related resource use in an elderly population: development and pilot study. Gesundheitswesen. (2015) 77:46–52. doi: 10.1055/s-0034-1372618
54. Grupp, H, Konig, HH, Riedel-Heller, S, and Konnopka, A. FIMPsy - questionnaire for the assessment of medical and non medical resource utilisation in mental disorders: development and application. Psychiatr Prax. (2018) 45:87–94. doi: 10.1055/s-0042-118033
55. Ware, J., Kosinski, M., Dewey, J., Gandek, B., Kisinski, M., Ware, J., et al. (2001). How to score and interpret single-item health status measures: A manual for users of the SF-8™ health survey. Boston: QualyMetric.
56. Ware, J, and Gandek, B. Overview of the SF-36 health survey and the international quality of life assessment (IQOLA). Project J Clin Epidemiol. (1998) 51:903–12. doi: 10.1016/S0895-4356(98)00081-X
57. IBM Corp. IBM SPSS statistics for windows. (version 27.0; Computer Software). US: IBM Corp (2020).
58. Ruxton, GD. The unequal variance t-test is an underused alternative to Student's t-test and the Mann–Whitney U test. Behav Ecol. (2006) 17:688–90. doi: 10.1093/beheco/ark016
59. Beierlein, V, Morfeld, M, Bergelt, C, Bullinger, M, and Brähler, E. Messung der gesundheitsbezogenen Lebensqualität mit dem SF-8. Diagnostica. (2012) 58:145–53. doi: 10.1026/0012-1924/a000068
61. Hemmerich, W. (2019). StatistikGuru: Poweranalyse und Stichprobenberechnung für Regression. Available at: https://statistikguru.de/rechner/poweranalyse-regression.html
62. Johnston, R, Jones, K, and Manley, D. Confounding and collinearity in regression analysis: a cautionary tale and an alternative procedure, illustrated by studies of British voting behaviour. Qual Quant. (2018) 52:1957–76. doi: 10.1007/s11135-017-0584-6
63. R Core Team. (2019). R: A language and environment for statistical computing. In R Foundation for Statistical Computing. Available at: https://www.R-project.org/
64. Nimon, K. F., Oswald, F. L., and Roberts, K. J. (2021). Yhat: Interpreting regression effects. R package (version 2.0–3). Available at: https://cran.r-project.org/package=yhat
65. Azen, R, and Budescu, DV. Comparing predictors in multivariate regression models: an extension of dominance analysis. J Educ Behav Stat. (2006) 31:157–80. doi: 10.3102/10769986031002157
66. Leng, A, Xu, C, Nicholas, S, Nicholas, J, and Wang, J. Quality of life in caregivers of a family member with serious mental illness: evidence from China. Arch Psychiatr Nurs. (2019) 33:23–9. doi: 10.1016/j.apnu.2018.08.010
67. Hedov, G, Annerén, G, Fau-Wikblad, K, and Wikblad, K. Self-perceived health in Swedish parents of children with Down's syndrome. Qual Life Res. (2000) 9:415–22. doi: 10.1023/A:1008910527481
68. Makovski, TT, Schmitz, S, Zeegers, MP, Stranges, S, and van den Akker, M. Multimorbidity and quality of life: systematic literature review and meta-analysis. Ageing Res Rev. (2019) 53:100903. doi: 10.1016/j.arr.2019.04.005
69. Phyo, AZZ, Freak-Poli, R, Craig, H, Gasevic, D, Stocks, NP, Gonzalez-Chica, DA, et al. Quality of life and mortality in the general population: a systematic review and meta-analysis. BMC Public Health. (2020) 20:1596. doi: 10.1186/s12889-020-09639-9
70. Hand, C. Measuring health-related quality of life in adults with chronic conditions in primary care settings: critical review of concepts and 3 tools. Can Fam Physician. (2016) 62:e375–83.
71. Lunsky, Y, Albaum, C, Baskin, A, Hastings, RP, Hutton, S, Steel, L, et al. Group virtual mindfulness-based intervention for parents of autistic adolescents and adults [article]. J Autism Dev Disord. (2021) 51:3959–69. doi: 10.1007/s10803-020-04835-3
72. Lunsky, YP, Hastings, R, Weiss, JAM, Palucka, A, Hutton, S, and White, K. Comparative effects of mindfulness and support and information group interventions for parents of adults with autism Spectrum disorder and other developmental disabilities. J Autism Dev Disord. (2017) 47:1769–79. doi: 10.1007/s10803-017-3099-z
73. Ross, CE, and Van Willigen, M. Education and the subjective quality of life. J Health Soc Behav. (1997) 38:275–97. doi: 10.2307/2955371
74. Nicolaidis, C, Raymaker, DM, Ashkenazy, E, McDonald, KE, Dern, S, Baggs, AE, et al. "respect the way I need to communicate with you": healthcare experiences of adults on the autism spectrum. Autism. (2015) 19:824–31. doi: 10.1177/1362361315576221
75. Hoshino, J, Tamakoshi, K, Hori, Y, and Sakakibara, H. Association between caregivers' health-related quality of life and care recipients' health outcomes. Int J Nurs Pract. (2022) 28:e13044. doi: 10.1111/ijn.13044
76. Bishop-Fitzpatrick, L, and Rubenstein, E. The physical and mental health of middle aged and older adults on the autism Spectrum and the impact of intellectual disability. Res Autism Spectr Disord. (2019) 63:34–41. doi: 10.1016/j.rasd.2019.01.001
77. Bradshaw, P, Pellicano, E, van Driel, M, and Urbanowicz, A. How can we support the healthcare needs of autistic adults without intellectual disability? Curr Dev Disord Rep. (2019) 6:45–56. doi: 10.1007/s40474-019-00159-9
78. Vogan, V, Lake, JK, Tint, A, Weiss, JA, and Lunsky, Y. Tracking health care service use and the experiences of adults with autism spectrum disorder without intellectual disability: a longitudinal study of service rates, barriers and satisfaction. Disabil Health J. (2017) 10:264–70. doi: 10.1016/j.dhjo.2016.11.002
79. Benson, PR. Coping, distress, and well-being in mothers of children with autism. Res Autism Spectr Disord. (2010) 4:217–28. doi: 10.1016/j.rasd.2009.09.008
80. Bonis, SA, and Sawin, KJ. Risks and protective factors for stress self-Management in Parents of children with autism Spectrum disorder: an integrated review of the literature. J Pediatr Nurs. (2016) 31:567–79. doi: 10.1016/j.pedn.2016.08.006
81. Schnabel, A, Youssef, GJ, Hallford, DJ, Hartley, EJ, McGillivray, JA, Stewart, M, et al. Psychopathology in parents of children with autism spectrum disorder: a systematic review and meta-analysis of prevalence. Autism. (2020) 24:26–40. doi: 10.1177/1362361319844636
82. Buescher, AV, Cidav, Z, Knapp, M, and Mandell, DS. Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatr. (2014) 168:721–8. doi: 10.1001/jamapediatrics.2014.210
83. Goode, KT, Haley, WE, Roth, DL, and Ford, GR. Predicting longitudinal changes in caregiver physical and mental health: a stress process model. Health Psychol. (1998) 17:190–8. doi: 10.1037/0278-6133.17.2.190
84. Aberson, C, Rodriguez, J, and Siegel, D. Power analysis for regression coefficients: the role of multiple predictors and power to detect all coefficients simultaneously. Quant Methods Psychol. (2022) 18:142–51. doi: 10.20982/tqmp.18.2.p142
85. Klar, MK, Geyer, S, Safieddine, B, Tetzlaff, F, Tetzlaff, J, and Sperlich, S. Trends in healthy life expectancy between 2002 and 2018 in Germany - compression or expansion of health-related quality of life (HRQOL)? SSM Popul Health. (2021) 13:100758. doi: 10.1016/j.ssmph.2021.100758
86. Willet, M, Dorstyn, D, Due, C, and Li, W. Applying Andersen’s model to explain service use and quality of life among Australian caregivers of children with autism Spectrum disorder. J Dev Phys Disabil. (2018) 30:339–54. doi: 10.1007/s10882-018-9589-x
Abbreviations

Keywords: autism spectrum disorder, adults, family caregivers, quality of life, mental wellbeing, caregiver burden
Citation: Dückert S, Bart S, Gewohn P, König H, Schöttle D, Konnopka A, Rahlff P, Erik F, Vogeley K, Schulz H, David N and Peth J (2023) Health-related quality of life in family caregivers of autistic adults. Front. Psychiatry. 14:1290407. doi: 10.3389/fpsyt.2023.1290407
Edited by:
Bernadette Roge, Université de Toulouse, FranceReviewed by:
Quentin Guillon, Université Toulouse - Jean Jaurès, FranceCorneliu Bolbocean, University of Oxford, United Kingdom
Copyright © 2023 Dückert, Bart, Gewohn, König, Schöttle, Konnopka, Rahlff, Erik, Vogeley, Schulz, David and Peth. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sophia Dückert, cy5kdWVja2VydEB1a2UuZGU=