 Chunlu Li
Chunlu Li Jing Gu
Jing Gu Yixin Li
Yixin Li Baijuan Xia
Baijuan Xia Xiaolu Meng
Xiaolu Meng- 1Department of Histology and Embryology, School of Basic Medical Sciences, Guizhou Medical University, Guiyang, China
- 2Key Laboratory for Research on Autoimmune Diseases of Higher Education schools in Guizhou Province, Guiyang, China
- 3Department of Psychology, School of Medical Humanitarians, Guizhou Medical University, Guiyang, China
- 4Guizhou Health Development Research Center, Guiyang, China
Introduction: Previous studies have demonstrated a strong link between perceived stress and binge eating behavior, but the psychological mechanisms underlying such phenomenon are not fully understood. The present study further addressed this issue in a life history framework, focusing on life history strategy and distress tolerance.
Methods: Firstly, we investigated the mediation role of life history strategy on the relationship between perceived stress and binge eating behavior. Secondly, we examined the moderation role of distress tolerance on the effect of perceived stress on life history strategy, as well as on the direct effect of perceived stress on binge eating behavior. We analyzed data from 1342 Chinese university students.
Results: Results indicated that life history strategy mediates the relationship between perceived stress and binge eating behavior; distress tolerance has significant moderating effects on the direct effect of perceived stress on binge eating behavior and their indirect effect via life history strategy.
Discussion: Therefore, distress tolerance skills training and life history-based interventions might be potentially effective ways to reduce binge eating behavior triggered by perceived stress.
Introduction
Binge eating is characterized by rapid and excessive food consumption, often accompanied by a feeling of loss of control (1). From 2018 to 2020, the global prevalence of binge eating is estimated to be 0.6-1.8% among adult women and 0.3-0.7% among adult men (2). A study in China found 85 cases of binge eating behavior among 1,103 college students based on the scores of the binge eating scale (3). Binge eating often leads to poor personal quality of life, work, family (4), because of its negative consequences including non-suicidal self-injury (4), gastric perforation and acute gastric dilatation (5). Given its pervasiveness and serious negative consequences, binge eating has become a significant public health concern.
Laboratory, descriptive, and ecological momentary assessment studies have demonstrated that binge eating is preceded by negative affect accompanying perceived stress (6), and that perceived stress positively predicts binge eating behavior (7, 8). Further, individuals with binge eating behavior have higher level of perceived stress and negative emotional experience than healthy controls under the same stressful laboratory situation (9). However, the psychological mechanisms by which perceived stress leads to binge eating are still not fully understood.
Existing researches have mainly addressed this issue from the perspective of self-regulation or coping strategies. For example, higher level of psychological distress (including stress) and emotional eating was observed in individuals with emotional dysregulation, an important aspect of self-regulation (10). Meanwhile, more coping strategies (including both positive and negative coping strategies) to relieve stress and more catastrophizing were reported by individuals with binge eating in stressful tasks (11). The risk of binge eating was increased by distraction coping increases, while decreased by social support (7). More directly, the relationship between perceived stress and binge eating/emotional eating is mediated by eating self-regulation (12) and emotion-focused coping (13) and moderated by resilience (14), cognitive reappraisal, but not response inhibition (15). In this research perspective, binge eating behavior is regarded as maladaptive behavior because of its negative consequences in the long run.
On the other hand, binge eating also is proposed to be motivated by a desire to escape from self-awareness, it might be an emotion regulation strategy to avoid unpleasant emotional distress accompanying aversive self-perceptions (16). Specifically, binge eating is a concrete and palatable way to distract from concerns about emotional distress. It seems that the expectation that binge eating will help to alleviate negative affect leads to the occurrence of this behavior (17–19). Therefore, binge eating appears to be a proactive adaptation strategy effective at the moment. In this context, it may be an adaptive behavior for binge eaters under special circumstances where due to excessive pressure, they have to focus on the present and cannot take into consideration the future. That is a fast life history strategy according to life history theory in evolutionary psychology.
Life history theory has been developed as an explanation for differences in energy and time allocation patterns between and within species (20). Resources are limited for all living organisms. How to allocate their limited resources is critical to the survival and continued existence of the species. The strategies for allocating resources often change based on their assessment of environmental stress. In predictable environments, planning and working for higher future rewards is cost effective. Therefore, cognition and behavior of humans and animals tend to be more future oriented than present oriented. That is to say, they prefer to behave in ways that are likely to be rewarded in the future but little or no immediate benefit. This strategy is called the slow life history strategy. Conversely, when the future is uncertain and hard to be predicted, it is unlikely that investing will pay off in the future. Therefore, a fast strategy is more adaptive, with organisms focusing more on the present and discounting the future (21).
Environmental stress is key to inducing a fast life history strategy (22). In the human life history strategy, more emphasis is placed on individual’s subjective perception in term of environmental stress (23, 24). That is to say, perceived stress, rather than objective environmental stress, more accurately reflects an individual’s stress state and more effectively triggers a fast life history strategy. Individuals with binge eating behavior suffer from high standards and expectations, particularly an acute sensitivity to the difficult (perceived) demands of others (16); This psychological trait exacerbates the state of imbalance between environmental demands and the individual’s capacity to cope with these demands, resulting in more perceived stress. In fact, they have higher levels of perceived stress under the same stressful situation (9). Therefore, they are expected to have a faster life history strategy. Further, a number of reviews or studies have examined a variety of psychopathological symptoms within a life history strategy perspective (17, 25), including eating disorders (26, 27). In contrast, slow life history strategy has a function in protecting against disordered eating behaviors (28). Based on these evidences, it is reasonable to assume that fast life history strategy may mediate the relationship between perceived stress and binge eating (H1).
Distress tolerance (DT) refers to the perceived and actual capability to withstand aversive physical and psychological states (29, 30), including uncertainty, ambiguity, frustration, negative emotion, physical discomfort (31). Individuals with lower DT are thought to be more reactive to distress, more likely to experience stress overload (32) and more attempt to avoid these aversive states (29). That is to say, under the same perceived stressful situation, individuals with low distress tolerance are more likely to experience psychological overload followed by a stronger motivation to alleviate negative experiences, finally results in the initiation of the fast life history strategy and occurrence of binge eating behavior. Therefore, it seems reasonable to hypothesize that distress tolerance moderates the relationship between perceived stress and fast life history strategy (H2) and that distress tolerance moderates the relationship between perceived stress and binge eating (H3).
Together, the present study aimed to investigate the psychological mechanism underling the role of perceived stress in the occurrence of binge eating behavior in Chinese culture. First, we tested whether life history strategy independently mediates their relationship. Then, we investigated whether distress tolerance moderates the direct effect of perceived stress on binge eating behavior and/the life history strategies. The hypothetical model was shown in Figure 1.
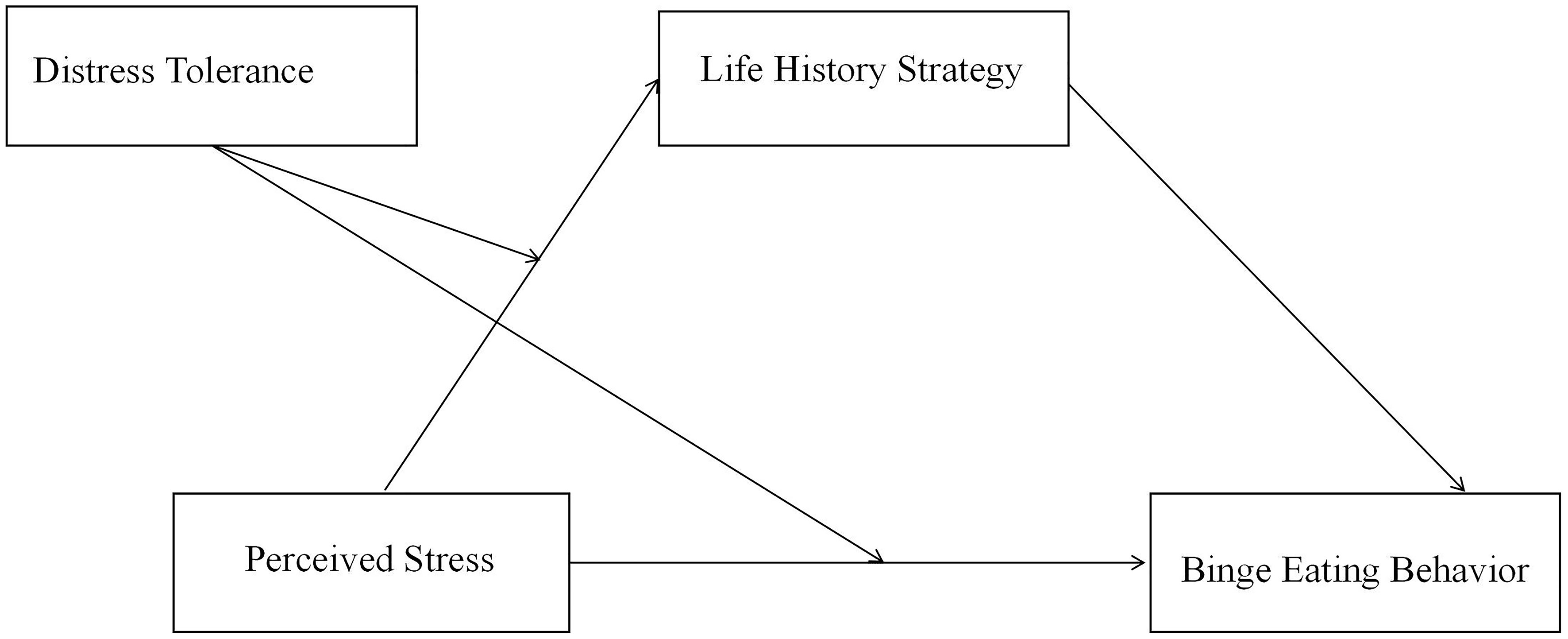
Figure 1 The moderated mediation model hypothesized in the present study. In this model, we hypothesized that fast life history strategy may mediate the relationship between perceived stress and binge eating (H1); and that distress tolerance may moderate both the relationship of perceived stress and fast life history strategies (H2) and that of perceived stress and binge eating (H3).
Materials and methods
Participants
This research was approved by the ethics committee of Guizhou Medical University. Chinese undergraduate students from a university in Guizhou province were recruited. Prior to participation, all students were asked to sign informed consent forms and informed that their responses would be anonymous with the option of withdrawal at any time. Data of the subjects who chose the same answer for more than half of the total scale were excluded (33). Finally,1342 students (519 males and 823 females) aged 18-24 (M = 19.03, SD = 1.02) were included in data analysis.
Measures
Binge eating behavior
To measure binge eating behavior, the Chinese version of Binge Eating Scale (BES) adapted by Wu Siyao, et al. (34) was adopted. The scale consists of 16 items, each with 3 to 4 options. The total score of the scale ranges from 0 to 46 points, higher total score indicates a more severe level of binge eating behavior. In this study, the Cronbach’s alpha was 0.79.
Perceived stress
To measure perceived Stress, the Chinese version of Perceived Stress Scale (PSS) revised by Tingzhong Yang (35) was adopted. PSS is developed by Cohen et al. (36) and includes two dimensions: tension (e.g, Can’t cope with all the tasks on your own.) and sense of loss of control (e.g., Things are going as hoped.). Each dimension contains 7 items, using a 5-Likert point scale. Items belonging to the sense of loss of control dimension were scored in reverse. The total score is from 0 to 56, with higher score indicating higher perceived stress. In this study, the Cronbach’s alpha was 0.77.
Life history strategy
To measure life history strategies, the life history strategy Scale revised by Sai Xueying et al. (37) was adopted. There are 20 items in the original scale and using a 7-Likert point scale. It’ s important to mention that item 20”I believe in religion and regularly participate in religious activities” has been removed in the Chinese version of the Life History Strategy Scale (37). The total score is derived from the summation of individual scores. Higher score suggests propensity towards slow life history strategy, whereas lower score indicates preference for fast life history strategy. In this study, the Cronbach’s alpha was 0.88.
Distress tolerance
To measure Distress tolerance, the Distress Tolerance Scale (DTS) the revised by You Jianing et al. (38) was adopted. The scale consists of 16 items, which was scored on a 5-Likert point scale. The scale has a total score range of 15-75, where higher DTS score indicates lower distress tolerance. In this study, the Cronbach’s alpha was 0.83.
Statistical analysis
The data gathered in this study were analyzed as outlined by Hayes (39) in his book. SPSS 26.0 was used to conduct common method bias test, descriptive statistical analysis and correlation analysis of the data. Then, the mediation effect of life history strategies was examined by PROCESS macro model 4 and the moderation role of distress tolerance was examined by model 1. Finally, all the study hypotheses were tested simultaneously by model 8. Data were calculated based on standardized scores. Bootstrapped confidence interval (CI; 5,000 bootstrap samples) for the indirect effect was obtained. If zero is not included in the confidence interval, effects are significant.
Results
Common method biases tests
To exclude common method bias, the Harman single factor method was used in this study (40). The results showed that there were 14 factors with feature roots greater than 1, among which the cumulative variance explained by the first factor was only 16.918%, less than the critical value of 40% (41). Therefore, common method biases are unlikely to confuse the interpretation of the data analysis.
Describe statistics and correlation analysis
Table 1 shows the descriptive statistics and correlations of the variables in this study. Perceived stress was negatively correlated with life history strategy (r = - 0.432, p < 0.001) and positively correlated with binge eating behavior (r = 0.362, p < 0.001). Life history strategy was negatively correlated with binge eating behavior (r = -0.253, p < 0.001). Distress tolerance was positively correlated with perceived stress (r = 0.565, p < 0.001) and negatively correlated with life history strategy (r = - 0.28, p < 0.001), while positively correlated with binge eating behavior (r = 0.368, p < 0.001).

Table 1 Descriptive statistics and correlation of variables.
Testing for mediation effect
To test hypothesis 1, PROCESS macro-Model 4 was used. The specifications of this model can be seen in Table 2. Since Gender and BMI are important variables that affect eating behavior and may confound the interpretation of our results (42–44), they were selected as covariates in the present study. After controlling for gender and BMI, the mediator and dependent variable models showed that perceived stress was negatively correlated with life history strategy (β = -0.73, p < 0.001. see Model 1 of Table 2), and life history strategy was negatively correlated with binge eating behavior (β = -0.06, p < 0.001. see Model 2 of Table 2). While, perceived stress was also positively associated with binge eating behavior (β = 0.25, p < 0.001. see Model 2 of Table 2). Therefore, life history strategy partly mediated the relationship between perceived stress and binge eating behavior, supporting Hypothesis 1.
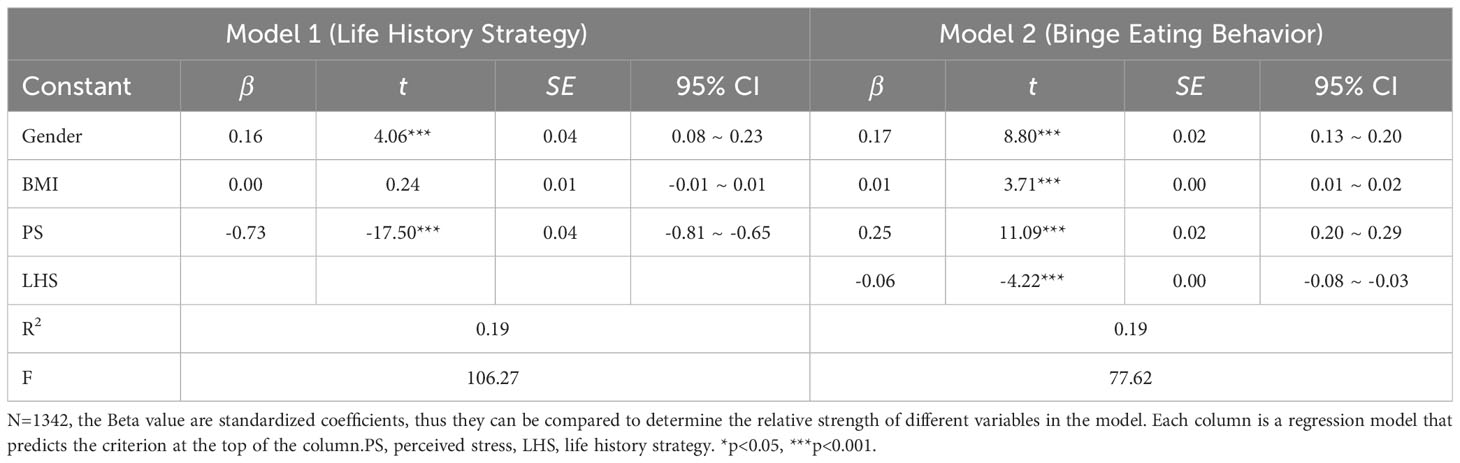
Table 2 Testing the mediation effect of Life History Strategy on binge eating behavior.
Testing for the moderation effect
To examine the moderation effect of distress tolerance on the relationship between perceived stress and life history strategy, the PROCESS macro model 1 was used. Results was shown in Table 3. The interaction between perceived stress and distress tolerance on life history strategy was significant (β = 0.14, p < 0.05; see Model 3 of Table 3). Thus, distress tolerance had a moderating role between perceived stress and life history strategy, supporting Hypothesis 2. Similarly, PROCESS macro model 1 was also ran to test the moderation effect of distress tolerance on the relationship between perceived stress and binge eating behavior. Results was also shown in Table 3. The interaction between perceived stress and distress tolerance on binge eating behavior was also significant (β = 0.06, p < 0.05. see Model 4 of Table 3), supporting Hypothesis 3.
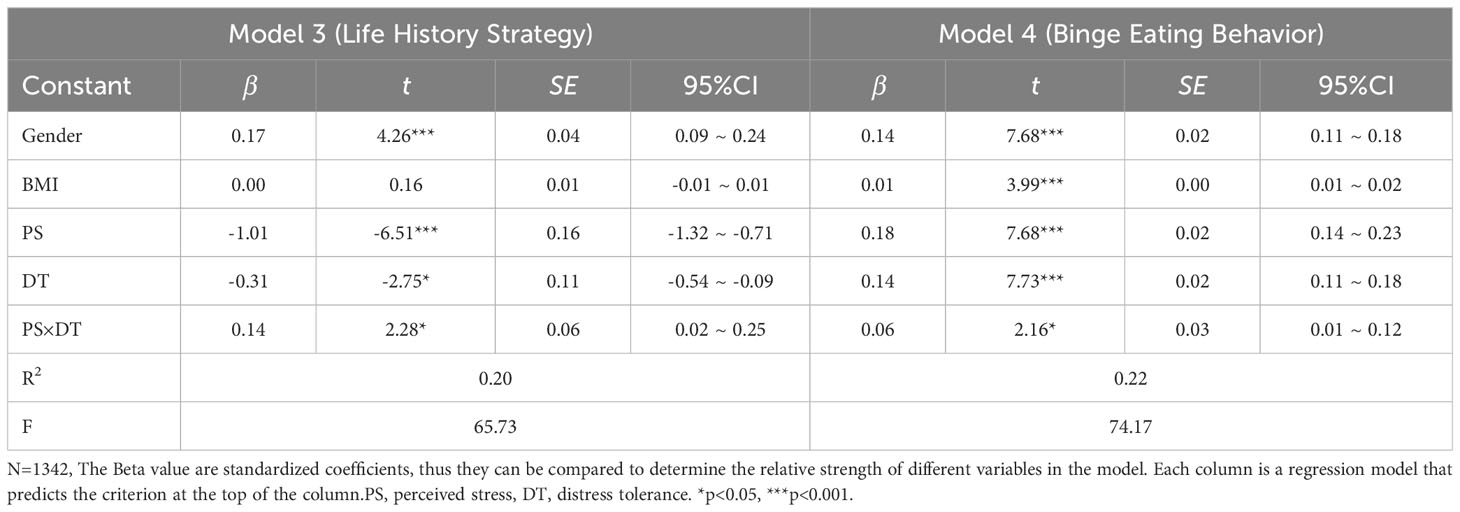
Table 3 Testing the moderation effect of distress tolerance.
To describe it more directly, figure of predicted perceived stress against life history strategy was plotted in Figure 2. Low and high level of distress tolerance score (1- SD below the mean and 1+ SD above the mean, respectively) were showed in the figure separately. The results showed that when perceived stress is high, both individuals with higher distress tolerance and those with lower distress tolerance tend to use the fast life history strategy; while perceived stress was low, individuals with low distress tolerance were more inclined to use faster life history strategy than those with high distress tolerance.
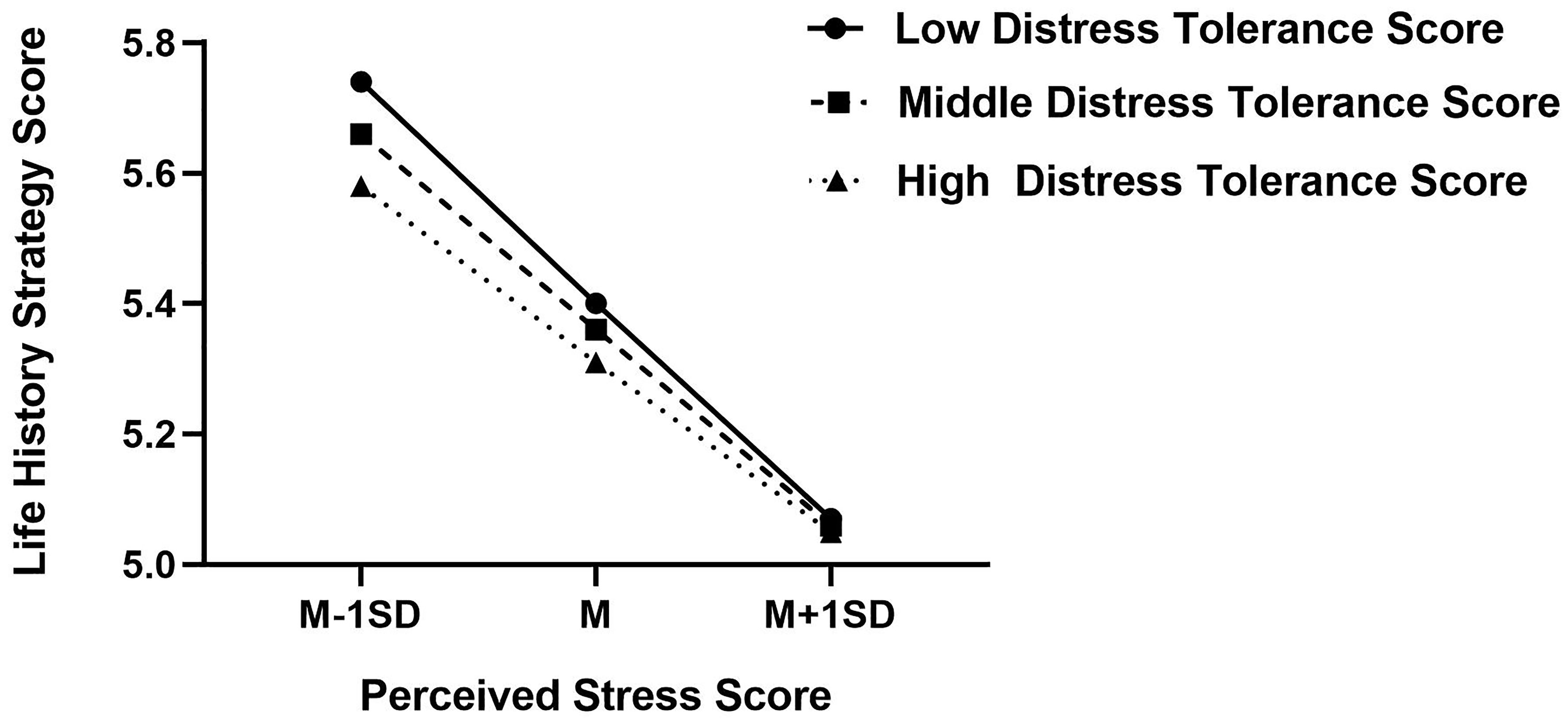
Figure 2 Interaction effect of distress tolerance and perceived stress on life history strategy. High and low levels of perceived stress and distress tolerance represent one standard deviation above and below the mean, respectively. Higher life history strategy score indicates a tendency to use slower life history strategy, and conversely, lower score indicates a tendency to use faster life history strategy. Higher distress tolerance score indicates lower distress tolerance; in contrast, lower distress tolerance score indicates higher distress tolerance.
Similarly, figure of predicted perceived stress against binge eating behavior was plotted. As shown in Figure 3, the higher distress tolerance score, the more prone to binge eating behavior score, regardless of the perceived stress. That is to say, individuals with lower distress tolerance are more likely to engage in binge eating behavior than those with higher distress tolerance.
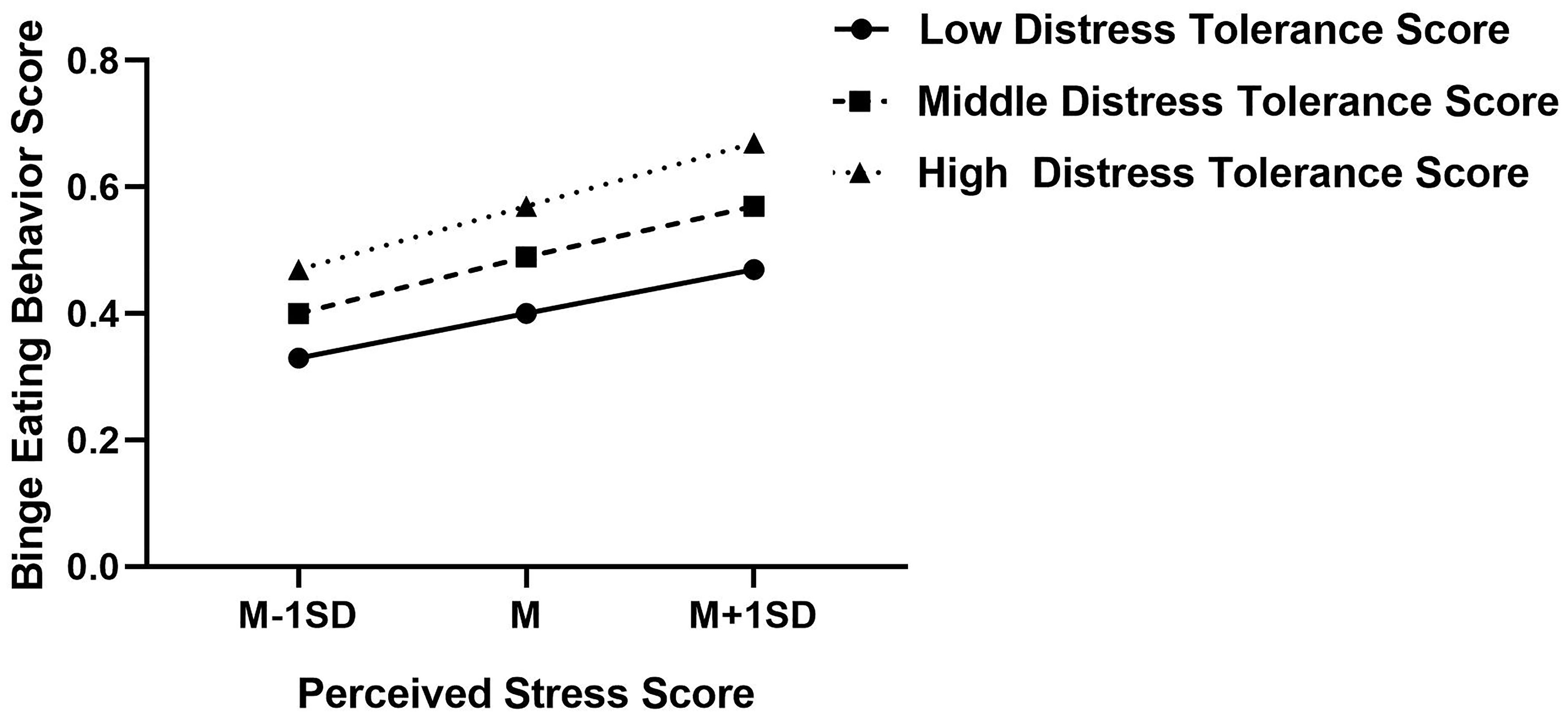
Figure 3 Interaction effect of distress tolerance and perceived stress on binge eating behavior. High and low level of perceived stress and distress tolerance represent one standard deviation above and below the mean, respectively. High distress tolerance score indicates lower distress tolerance, in contrast, lower distress tolerance score indicates higher distress tolerance.
Testing for the whole research model
Finally, all the study hypotheses were tested simultaneously using PROCESS macro model 8. The results showed that binge eating behavior was predicted by both perceived stress and life history strategy in Model 6, and life history strategy was predicted by perceived stress in Model 5. Therefore, the relationship between perceived stress and binge eating behavior was partly mediated by life history strategy. In addition, the indirect effect of perceived stress on binge eating behavior via life history strategies was also moderated by distress tolerance (β = 0.01, p < 0.05. see Model 5 of Table 4); meanwhile, the direct effect of perceived stress on binge eating behavior was also moderated by distress tolerance (β = 0.01, p < 0.05. see Model 6 of Table 4). The index of moderated mediation was -0.0006 with a 95% confidence interval (CI) of [-0.0012, -0.0001] (see Model 7 of Table 4), the zero value was not included. Therefore, the whole research model was supported.
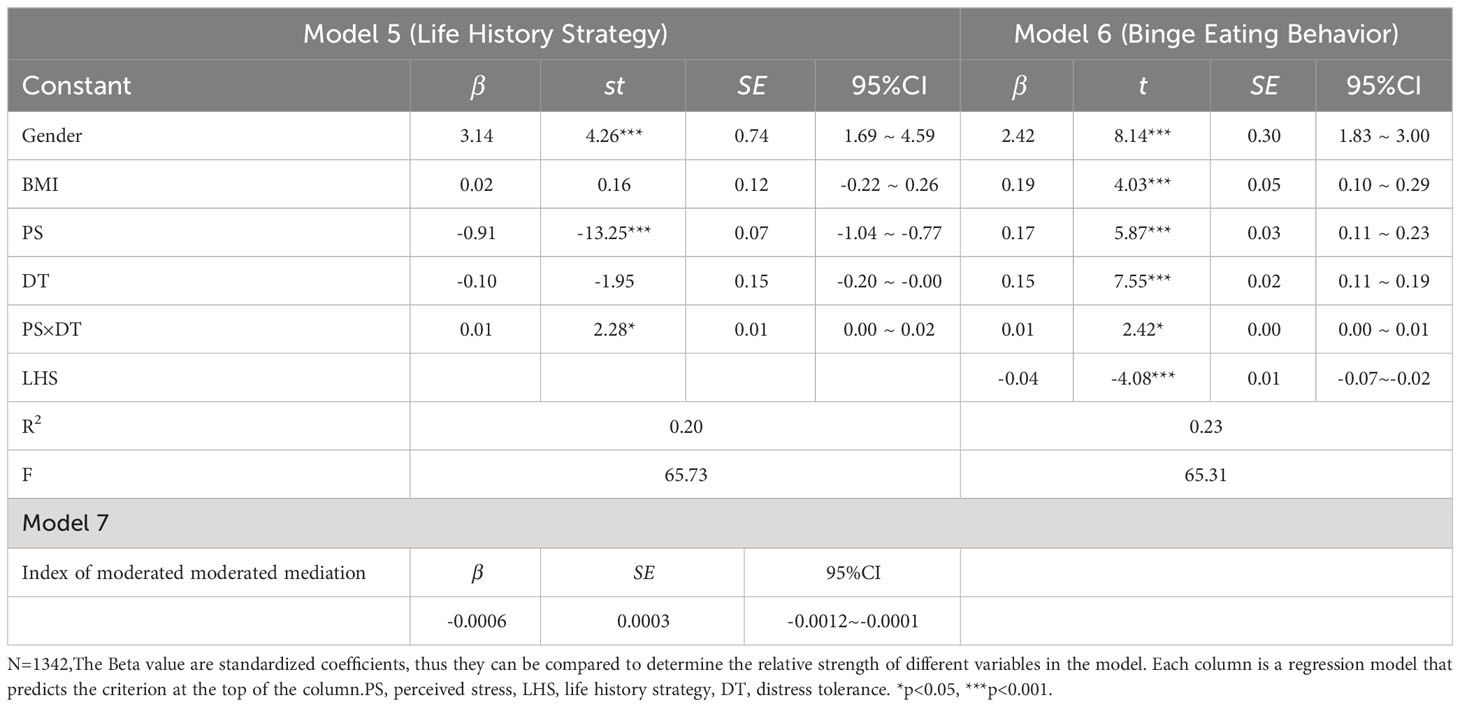
Table 4 Testing for the whole research model.
Discussion
Numerous studies have demonstrated perceived stress is an important trigger of binge eating behavior (6, 15, 45). However, the psychological mechanisms by which perceived stress triggers binge eating behavior are not fully understanded. In the present study, we further addressed this issue from the perspective of evolutionary psychology, focusing on life history strategy and distress tolerance. Firstly, we found a mediating role of life history strategy on the relationship between perceived stress and binge eating behavior. Secondly, when distress tolerance is introduced as a moderator for the perceived stress-life history strategy and perceived stress-binge eating in the model, main interactional effects were also been observed.
There are a number literatures have attempted to explain a variety of psychopathological symptoms within a life history strategy framework (17, 25, 28, 46), including eating disorders (26, 27). However, the evolutionary origin and function of binge eating remains unexplored, and binge eating may have adaptive implications from a life history strategy perspective, especially in situations of high perceived stress.
The term perceived stress refers to a perceived imbalance state between environmental demands and the individual’s capacity to cope with these demands (47). When a person perceives that his abilities are sufficient to cope with the demands of the environment, the perceived stress is low. On the contrary, when he perceives that his abilities are insufficient to cope with the demands of the environment, the perceived stress is high. It has been shown that individuals with binge eating behavior suffer from high standards and expectations, particularly an acute sensitivity to the difficult (perceived) demands of others (16). Therefore, the binge eater is expected to have higher perceived disparity between environmental demands and his capacity to cope with these demands. That is to say, they perceive that they are unable to cope with the demands of their environment and are more likely experience stress overload. In this context, the future is uncertain and hard to predict, it is unlikely that investing will pay off in the future. It is crucial for individuals with binge eating disorder to promptly address excessive psychological stress. Therefore, a fast strategy, focusing more on the present and discounting the future, is more adaptive, where binge eating was used to escape from such emotional distress, particularly when there is no alternative, adaptive emotion-regulation skills (48). The results of the present study supported this hypothesis, finding that life history strategy mediated the relationship between perceived stress and binge eating behavior.
Distress tolerance is another important psychological variable related to coping with stressors. It reflects the perceived and actual capability to withstand aversive physical and psychological states (29, 30). Individuals with low distress tolerance not only have a low threshold for experiencing negative emotions, but also lack emotion regulation skills (49). Previous researchers have found that distress tolerance alone negatively predicted binge eating behavior (50–52), although there are also studies that do not support this view (9, 53). This inconsistency might suggest that distress tolerance may interact with other factors in binge eating. In the present study, we expanded the mechanism of distress tolerance in binge eating. We found that distress tolerance regulates binge eating behavior by interacting with perceived stress through two pathways: (1) the direct effect of perceived stress on the binge eating; (2) the indirect effect of perceived stress on the binge eating through the life history strategy. Therefore, distress tolerance may be an important potential intervention target for binge eating. This was supported by the fact that Dialectical Behavior Therapy (DBT) skills training which include distress tolerance skills reduces binge eating (54).
At the theoretical level, the present study improves our understanding about how perceived stress leads to binge eating behavior in a life history framework. Perceived stress may affect binge eating by fast life history strategy; Distress tolerance moderates both the direct effect of perceived stress on binge eating and its indirect effect through life history strategy.
At the practical level, the present study results suggested that life history-based interventions might effectively relieve stress-induced binge eating behavior. Specifically, developing slow life history strategy could help individuals to reduce their binge eating behavior when encountering similar stressful situations in the future. This is consistent with the idea that understanding eating interventions through an evolutionary lens (55). Further, our results also suggested that distress tolerance skills training might be a potentially effective way to reduce binge eating behavior triggered by perceived stress directly or indirectly by developing slow life history strategy. In fact, previous researches have confirmed that DBT, which includes distress tolerance skills training, significantly reduces binge eating behavior (54, 56). Whether distress tolerance skills training alone also have a similar effect requires further studies in the future.
On the other hand, the present study cannot draw causal conclusions because of its cross-sectional design. Longitudinal studies are still needed to further confirm these conclusions in the future. In addition, although our sample size is relatively large, it is all from one university, which limits the representativeness of the sample. Future research should increase the sampling locations.
Conclusion
Perceived stress induced binge eating behavior may be mediated by fast life history strategy; Distress tolerance moderates both the direct effect of perceived stress on binge eating and its indirect effect through life history strategy. Therefore, distress tolerance skills training and life history-based interventions might be potentially effective ways to reduce binge eating behavior triggered by perceived stress.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by the ethics committee of Guizhou Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
XM: Conceptualization, Funding acquisition, Writing – review & editing. JG: Conceptualization, Formal analysis, Investigation, Writing – original draft. YL: Writing – review & editing. BX: Writing – review & editing. CL: Writing – review & editing, Conceptualization, Funding acquisition, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Guizhou Medical University start-up fund for doctoral talent (J-[2021]050; J-[2021]051), NSFC Cultivation Project (21NSFCP49; 22NSFCP40), the National Natural Science Foundation of China(32260199), Key Laboratory for Research on Autoimmune Diseases of Higher Education schools in Guizhou Province (Qianjiaoji[2023]016).
Acknowledgments
We acknowledge all participants involved in our research and those who helped in recruiting.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. American Psychiatric Association, Association. Diagnostic and statistical manual of mental disorders: DSM-5 Vol. 5. Washington, DC: American psychiatric association (2013). doi: 10.1176/appi.books.9780890425596
2. Giel KE, Bulik CM, Fernandez-Aranda F, Hay P, Keski-Rahkonen A, Schag K, et al. Binge eating disorder. Nat Rev Dis Primers. (2022) 8:16. doi: 10.1038/s41572-022-00344-y
3. Yan W-S, Zhang R-R, Lan Y, Li Z-M, Li Y-H. Questionnaire-based maladaptive decision-coping patterns involved in binge eating among 1013 college students. Front Psychol. (2018) 9:609. doi: 10.3389/fpsyg.2018.00609
4. Pak KN, Nelson J, Adams LM, Fischer S. Mixture modeling of nonsuicidal self-injury and binge eating: Behaviors and motives. Behav Ther. (2021) 52:1265–76. doi: 10.1016/j.beth.2021.02.00
5. Sato Y, Fukudo S. Gastrointestinal symptoms and disorders in patients with eating disorders. Clin J gastroenterol. (2015) 8:255–63. doi: 10.1007/s12328-015-0611-x
6. Nicholls W, Devonport T, Blake M. The association between emotions and eating behavior in an obese population with binge eating disorder. Obes Rev. (2016) 17:30–42. doi: 10.1111/obr.12329
7. Freeman LM, Gil KM. Daily stress, coping, and dietary restraint in binge eating. Int J Eat Disord. (2004) 36:204–12. doi: 10.1002/eat.20012
8. Mason TB, Lewis RJ. Minority stress and binge eating among lesbian and bisexual women. J Homosexuality. (2015) 62:971–92. doi: 10.1080/00918369.2015.1008285
9. Yiu A, Christensen K, Arlt JM, Chen EY. Distress tolerance across self-report, behavioral and psychophysiological domains in women with eating disorders, and healthy controls. J Behav Ther Exp Psychiatry. (2018) 61:24–31. doi: 10.1016/j.jbtep.2018.05.006
10. Guerrini-Usubini A, Cattivelli R, Scarpa A, Musetti A, Varallo G, Franceschini C, et al. The interplay between emotion dysregulation, psychological distress, emotional eating, and weight status: A path model. Int J Clin Health Psychol. (2023) 23:100338. doi: 10.1016/j.ijchp.2022.100338
11. Hansel SL, Wittrock DA. Appraisal and coping strategies in stressful situations: A comparison of individuals who binge eat and controls. Int J Eating Disord. (1997) 21:89–93. doi: 10.1002/(sici)1098-108x(199701)21:1<89::aid-eat11>3.0.co;2-j
12. Ling J, Zahry NR. Relationships among perceived stress, emotional eating, and dietary intake in college students: Eating self-regulation as a mediator. Appetite. (2021) 163:105215. doi: 10.1016/j.appet.2021.105215
13. Yilmazturk NH, Demir A, Celik-Orucu M. The mediator role of emotion-focused coping on the relationship between perceived stress and emotional eating. Trends Psychol. (2023) 31:383–99. doi: 10.1007/s43076-022-00142-1
14. Thurston IB, Hardin R, Kamody RC, Herbozo S, Kaufman C. The moderating role of resilience on the relationship between perceived stress and binge eating symptoms among young adult women. Eat Behav. (2018) 29:114–9. doi: 10.1016/j.eatbeh.2018.03.009
15. Yan J, Su H, Li C. Effect of body dissatisfaction on binge eating behavior of Chinese university students: A moderated mediation model. Front Psychol. (2022) 13:995301. doi: 10.3389/fpsyg.2022.995301
16. Heatherton TF, Baumeister RF. Binge eating as escape from self-awareness. psychol bulletin. (1991) 110:86. doi: 10.1037/0033-2909.110.1.86
17. Del Giudice M. An evolutionary life history framework for psychopathology. psychol Inquiry. (2014) 25:261–300. doi: 10.1080/1047840x.2014.884918
18. Fischer S, Wonderlich J, Breithaupt L, Byrne C, Engel S. Negative urgency and expectancies increase vulnerability to binge eating in bulimia nervosa. Eating Disord. (2018) 26:39–51. doi: 10.1080/10640266.2018.1418253
19. Smith KE, Mason TB, Juarascio A, Weinbach N, Dvorak R, Crosby RD, et al. The momentary interplay of affect, attention bias, and expectancies as predictors of binge eating in the natural environment. Int J Eating Disord. (2020) 53:586–94. doi: 10.1002/eat.23235
20. Sng O, Neuberg SL, Varnum ME, Kenrick DT. The crowded life is a slow life: Population density and life history strategy. J Pers Soc Psychol. (2017) 112:736. doi: 10.1037/pspi0000086
21. Chen B-B, Chang L. Procrastination as a fast life history strategy. Evolutionary Psychol. (2016) 14:1474704916630314. doi: 10.1177/1474704916630314
22. Sear R. Do human ‘life history strategies’ exist? Evol Hum Behavior. (2020) 41:513–26. doi: 10.1016/j.evolhumbehav.2020.09.004
23. Laran J, Salerno A. Life-history strategy, food choice, and caloric consumption. psychol sci. (2013) 24:167–73. doi: 10.1177/0956797612450033
24. Chua KJ, Lukaszewski AW, Grant DM, Sng O. Human life history strategies: Calibrated to external or internal cues? Evolutionary Psychol. (2016) 15:1474704916677342. doi: 10.1177/1474704916677342
25. Hurst JE, Kavanagh PS. Life history strategies and psychopathology: The faster the life strategies, the more symptoms of psychopathology. Evol Hum Behavior. (2017) 38:1–8. doi: 10.1016/j.evolhumbehav.2016.06.001
26. Hill SE, Prokosch ML, DelPriore DJ, Griskevicius V, Kramer A. Low childhood socioeconomic status promotes eating in the absence of energy need. Psychol Sci. (2016) 27:354–64. doi: 10.1177/0956797615621901
27. Nettersheim J, Gerlach G, Herpertz S, Abed R, Figueredo AJ, Brüne M. Evolutionary psychology of eating disorders: An explorative study in patients with anorexia nervosa and bulimia nervosa. Front Psychol. (2018) 9:2122. doi: 10.3389/fpsyg.2018.02122
28. Salmon C, Figueredo AJ, Woodburn L. Life history strategy and disordered eating behavior. Evolutionary Psychol. (2009) 7:147470490900700408. doi: 10.1177/147470490900700408
29. Leyro TM, Zvolensky MJ, Bernstein A. Distress tolerance and psychopathological symptoms and disorders: a review of the empirical literature among adults. psychol bulletin. (2010) 136:576. doi: 10.1037/a0019712
30. Kim HS, Hodgins DC. Component model of addiction treatment: A pragmatic transdiagnostic treatment model of behavioral and substance addictions. Front Psychiatry. (2018) 9:406. doi: 10.3389/fpsyt.2018.00406
31. Zvolensky MJ, Vujanovic AA, Bernstein A, Leyro T. Distress tolerance: Theory, measurement, and relations to psychopathology. Curr Dir psychol sci. (2010) 19:406–10. doi: 10.1177/0963721410388642
32. Jonker LC. Stress in a college workplace and its relationship with certain correlates and predictive variables. Stellenbosch: Stellenbosch University (2016).
33. Curran PG. Methods for the detection of carelessly invalid responses in survey data. J Exp Soc Psychol. (2016) 66:4–19. doi: 10.1016/j.jesp.2015.07.006
34. Wu S, He J, Cai T. Validation of the Binge Eating Scale in a sample of Chinese adolescents. Neurological Dis Ment Health. (2019) 19:273–6. doi: 10.3969/j.issn.1009-6574.2019.03.013
35. Tingzhong Y, Hanteng H. An epidemiological study on stress among urban residents in social transition period. Chin J Epidemiol. (2003) 24(9):760–4. doi: 10.3760/j.issn:0254-6450.2003.09.004
36. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
37. Xueying S, Yiran Z, Yaoguo G, Lei Z, Haijiao Z. Revision of the mini-K scale in Chinese college students. Chin J Clin Psychol. (2022) 30:1160–4. doi: 10.16128/j.cnki.1005-3611.2022.05.030
38. You J, Leung F. A Chinese adaptation of the Distress Tolerance Scale among adolescents: Factor structure and psychometric properties. J Psychopathol Behav Assessment. (2012) 34:136–44. doi: 10.1007/s10862-011-9256-3
39. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York:Guilford Publications (2017). doi: 10.1111/jedm.12050
41. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. (2003) 88:879–903. doi: 10.1037/0021-9010.88.5.879
42. Snoek HM, van Strien T, Janssens JM, Engels RC. Restrained eating and BMI: a longitudinal study among adolescents. Health Psychol. (2008) 27:753–9. doi: 10.1037/0278-6133.27.6.753
43. Cuzzocrea F, Larcan R, Lanzarone C. Gender differences, personality and eating behaviors in non-clinical adolescents. Eat Weight Disord. (2012) 17:e282–289. doi: 10.1007/bf03325139
44. Pace CS, Muzi S. Binge-eating symptoms, emotional-behavioral problems and gender differences among adolescents: a brief report. Mediterr J Clin Psychol. (2019) 7:2161. doi: 10.6092/2282-1619/2019.7.2161
45. Sims R, Gordon S, Garcia W, Clark E, Monye D, Callender C, et al. Perceived stress and eating behaviors in a community-based sample of African Americans. Eat Behav. (2008) 9:137–42. doi: 10.1016/j.eatbeh.2007.06.006
46. Kavanagh PS, Kahl BL. Are expectations the missing link between life history strategies and psychopathology? Front Psychol. (2018) 9:89. doi: 10.3389/fpsyg.2018.00089
47. Stokols D. A congruence analysis of human stress. Stress anxiety. (1979) 6:27–53. doi: 10.3109/01612848509009449
48. Wiser S, Telch CF. Dialectical behavior therapy for binge-eating disorder. J Clin Psychol. (1999) 55:755–68. doi: 10.1002/(sici)1097-4679(199906)55:6<755::aid-jclp8>3.0.co;2-r
49. Koball AM, Himes SM, Sim L, Clark MM, Collazo-Clavell ML, Mundi M, et al. Distress tolerance and psychological comorbidity in patients seeking bariatric surgery. Obes surg. (2016) 26:1559–64. doi: 10.1007/s11695-015-1926-x
50. Anestis MD, Selby EA, Fink EL, Joiner TE. The multifaceted role of distress tolerance in dysregulated eating behaviors. Int J Eating Disord. (2007) 40:718–26. doi: 10.1002/eat.20471
51. Anestis MD, Lavender JM, Marshall-Berenz EC, Gratz KL, Tull MT, Joiner TE. Evaluating distress tolerance measures: Interrelations and associations with impulsive behaviors. Cogn Ther Res. (2012) 36:593–602. doi: 10.1007/s10608-011-9377-8
52. Eichen DM, Chen E, Boutelle KN, McCloskey MS. Behavioral evidence of emotion dysregulation in binge eaters. Appetite. (2017) 111:1–6. doi: 10.1016/j.appet.2016.12.021
53. Kelly NR, Cotter EW, Mazzeo SE. Examining the role of distress tolerance and negative urgency in binge eating behavior among women. Eating behaviors. (2014) 15:483–9. doi: 10.1016/j.eatbeh.2014.06.012
54. Mushquash AR, McMahan M. Dialectical behavior therapy skills training reduces binge eating among patients seeking weight-management services: Preliminary evidence. Eating Weight Disorders-Studies Anorexia Bulimia Obes. (2015) 20:415–8. doi: 10.1007/s40519-015-0177-0
55. Ahlstrom B, Dinh T, Haselton MG, Tomiyama AJ. Understanding eating interventions through an evolutionary lens. Phys Rev. (2016) 47:777–80. doi: 10.1080/17437199.2016.1260489
Keywords: perceived stress, life history strategy, binge eating behavior, distress tolerance, Chinese university students
Citation: Li C, Gu J, Li Y, Xia B and Meng X (2024) The effect of perceived stress on binge eating behavior among Chinese university students: a moderated mediation model. Front. Psychiatry 15:1351116. doi: 10.3389/fpsyt.2024.1351116
Received: 06 December 2023; Accepted: 05 March 2024;
Published: 18 March 2024.
Edited by:
Cristina Segura-Garcia, University of Magna Graecia, ItalyCopyright © 2024 Li, Gu, Li, Xia and Meng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chunlu Li, bGlndWFuMTk4MEAxNjMuY29t; Xiaolu Meng, bXhsbXljQDEyNi5jb20=
†These authors have contributed equally to this work