 Moa Wahlqvist
Moa Wahlqvist Maria Björk2
Maria Björk2 Agneta Anderzén-Carlsson
Agneta Anderzén-Carlsson Karina Huus
Karina Huus- 1Faculty of Medicine and Health, Audiological Reserach Center and Swedish Institute for Disability Research, The Swedish National Resource Center for Deafblindness, Örebro University, Örebro, Sweden
- 2CHILD Research Group, Department of Nursing Science, School of Health Sciences, Swedish Institute for Disability Research, Jönköping University, Jönköping, Sweden
- 3Faculty of Medicine and Health, University Health Care Research Center and Swedish Institute for Disability Research, Örebro University, Örebro, Sweden
Introduction: The consequences of living with deafblindness can be vast and have been described as concerning difficulties with communication, restrictions in the activities of daily living and a lack of independence. Deafblindness has also been associated with poor health-related quality of life. Little is known about parenting when having deafblindness or how the health and family climate of families in which a parent has deafblindness are affected.
Aim: The aim of the study was to describe the health-related quality of life, sense of coherence and family climate in families where a parent has a deafblindness.
Methods: A total of 38 individuals, of which 14 were parents with deafblindness and 6 were partners to the parent with deafblindness, and 18 children, were included. The participants answered questionnaires about their health-related quality of life, family climate and sense of coherence (comprehensibility, manageability, and meaningfulness). The Swedish age-relevant versions of the questionnaires were used. Due to the small number of participants, descriptive statistics were used to explore the results from the questionnaires.
Results: The results revealed a pattern indicating that the health-related quality of life was affected, parents with deafblindness reported the poorest health-related quality of life. Sense of coherence was reported by all the family members as either moderate or low. The Family climate questionnaire revealed the positive aspect of closeness across family members, however negative aspects of chaos and expressiveness in the families were reported, mainly by, but not restricted to, the parents with deafblindness.
Discussion: This study includes a small sample, too small to draw far-reaching conclusions. However, some interesting results need to be highlighted and discussed. When considering the family as a system, it is reasonable to assume that the family members contribute in different ways to how health and wellbeing is experienced in the family. Deafblindness is a unique disability that affects not only the individual but also the whole family. This fact needs to be considered when support is offered to individuals with deafblindness. All members of families where a parent has deafblindness have to be asked about their needs and about how they experience the situation.
Introduction
This study describes the perspectives of all family members when a parent has a specific impairment, i.e., deafblindness. When a parent has a chronic illness, the whole family is affected (Payne and McPherson, 2010; Bergström et al., 2014). Family members can feel neglected and that their problems and needs are underestimated. Individuals can experience feelings of detachment from their partner when that partner has an impairment (Eriksson and Svedlund, 2006), and children might experience shame or guilt when their parent appears different from others (Willems et al., 2007; Dam and Hall, 2016). There are studies that have described that the mental health of children is associated with their parents’ own feelings about the family’s health, social and economic situations (Bergström et al., 2014), and other studies have described positive aspects of good self-esteem and an overall positive experience of growing up with a parent with a disability (Jacob et al., 2019). However, what it is like to grow up with a parent with deafblindness has not yet been studied.
Deafblindness
In the Nordic definition, deafblindness is defined as “a distinct disability. Deafblindness is a combined vision and hearing impairment. It limits the activities of a person and restricts full participation in society to such a degree that society is required to facilitate specific services, environmental alterations and/or technology” (Nordens Välfärdscenter, 2016). Some of the consequences of living with deafblindness are shared regardless of the cause. This mainly has to do with difficulties with communication, restrictions in the activities of daily living, a lack of independence and a risk for isolation, as well as difficulties concerning mobility (Fletcher and Guthrie, 2013; Hersh, 2013; Simcock, 2017). Deafblindness can be present from birth or acquired later in life, and there is great variation in the degree of vision and hearing loss between individuals’ deafblindness, as well as in the etiology (Dalby et al., 2009; Ask Larsen and Damen, 2014). The number of individuals under the age of 65 with deafblindness in Sweden is approximately 20001.
Health-Related Quality of Life and Wellbeing
Research has shown that health and wellbeing can be affected when living with deafblindness (Ellis and Hodges, 2013; Fletcher and Guthrie, 2013). Significantly poorer health has been reported, especially in regard to headache, fatigue, depression and suicide ideation for adults with Usher syndrome (USH), who represent the largest group of individuals under the umbrella of deafblindness. The lack of general trust in others and having no one to share one’s innermost feelings and thoughts with have also been reported, as well as strained financial situations (Wahlqvist et al., 2013, 2016a,b). However, there have also been reports of good health, positive outlooks and the positive meaning of everyday living (Dalby et al., 2009; Ellis and Hodges, 2013). A review of existing research on determinants that are associated with the quality of life of people with deafblindness due to Usher syndrome has found that the adjustment of living habits, maintaining hope for the future and a belief in one’s own capacity to accomplish goals are important in maintaining a good quality of life (Arcous et al., 2019). Being an active agent in one’s own life has also been identified when having to adopt to new situations due to a USH, which is a disease with a progressive course (Ehn et al., 2019). Furthermore, social participation and inclusion have been reported as having a positive impact on the health-related quality of life for persons with deafblindness (Dean et al., 2017).
Sense of Coherence
Antonovsky has formulated a theoretical model of salutogenesis to increase the understanding of the relationship between stress factors, coping and health (Antonovsky, 1987b) to understand why some people cope with life crises better than others. The core concept of salutogenesis is a sense of coherence (SOC), which can be further operationalized into three components: comprehensibility, manageability and meaningfulness (Antonovsky, 1987b). Comprehensibility has to do with to what extent the individual perceives the world as predictable, ordered and explicable. Manageability refers to the individuals personal and social resources to deal with demands posed. Finally, meaningfulness, has to do with the individuals believes that challenges are worth commitment and investment. The last component is seen as the most important dealing with emotional motivation to create order in the world and to use resources available as well as finding new strategies to manage demands (Antonovsky, 1987b). Research on sense of coherence and quality of life has shown positive outcomes in that a strong sense of coherence (i.e., higher scores on the SOC questionnaire) positively relates to a good quality of life (Eriksson and Lindström, 2007). Antonovsky (1987b) describes the development of a sense of coherence as a process that starts in early life through a child’s experiences with his or her parents’ predictability and demands, but the process is not restricted to development during childhood. The experiences from family life in early childhood have also been studied and have indicated that the level of education and gender are related to one’s sense of coherence (Sagy and Antonovsky, 2000).
Research about sense of coherence in relation to disability has had different focus, for example a study where the degree of sense of coherence of parents was studied to understand individual differences in adjustment of family life when living with children with developmental disabilities. A stronger sense of coherence was related to a better psychosocial adjustment of being a parent with a child with developmental disabilities (Olsson and Hwang, 2002). Another study examined the sense of coherence and its effect on thoughts on career for individuals with different disabilities (cognitive, physical and psychological) who were studying at university. The results indicated that the individuals with disabilities had more negative thought of their careers and lower sense of coherence than students without disabilities (Lustig and Strauser, 2008). In relation to adjustment to disability, a sense of coherence has been described not only as a positive predictor of the adjustment process (Lustig et al., 2000) but also as an important factor for a spouse’s ability to adjust to the acquired disability of his or her partner (Rena et al., 1996). It is reasonable to believe that comprehensibility, manageability and meaningfulness can be affected in persons with deafblindness, but this has not been studied. We have also not found any research about the sense of coherence in other family members who share a household with a parent with deafblindness.
Family Life
Fragmented descriptions about family life can be found in previous research that has focused on individuals with deafblindness, in which they describe their perspectives of how their family members can either meet the needs of everyday living or not (Miner, 1995, 1997). Both the emotional and practical support given by family members to the person with deafblindness and the efforts required from the family members, especially from the partner, have been addressed by Ellis and Hodges (2013). However, the authors do not report on the partner’s perspective or the perspective from the children. To our knowledge, the perspective of being a parent with deafblindness has never been addressed as the main focus in any study. Reports from parents having deafblindness can, however, be identified. In such cases, the fear of passing on a genetic illness to a child has been described. Furthermore, these individuals have also described the challenges that they meet in terms of communication and feelings of not being a source of support for the other parent to the extent that they wanted (Ellis and Hodges, 2013).
A few recent articles have described the experiences of being the partner of someone who has dual sensory loss (i.e., concurrent hearing and vision loss) (Lehane et al., 2017a, b, 2018). These studies have focused mainly on members of the aging population and the challenges they face due to the changed way of communication and the effects on their wellbeing or sexuality.
The consequences of the lack of research focusing on the family climate (i.e., emotional aspects of family life), sense of coherence and health-related quality of life of the whole family means that there is no knowledge basis for how support should be formed for these family members. The data presented in this article constitute one of four articles in a research project that addresses health and quality of life, family climate and the need for support for families in which a parent has deafblindness from a family perspective.
Aim
The aim of this study was to describe the health-related quality of life, sense of coherence and family climate in families where a parent has deafblindness.
Materials and Methods
The study presented in this article is a descriptive cross-sectional study of the health-related quality of life, sense of coherence and family climate between family members in families where a parent has deafblindness.
Participants
A major challenge for people with deafblindness is the ability to access information. Therefore, the research group tried to spread information about the project through several different channels. Contact with the family section of the Association of the Swedish Deafblind and the Swedish National Resource Center for Deafblindness was established, as well as contact with some existing deafblind teams within health care services. Information about the project was further spread through Facebook, the journal for members of the Association of the Swedish Deafblind and at a meeting for members of the Association of the Swedish Deafblind. The researchers also sent information letters to known individuals with deafblindness who also have families to inform them about the project and invite them to participate.
The inclusion criteria were as follows: at least one of the parents should have deafblindness regardless of the cause, the families should live together at least 50% of the time and have children between 6 and 18 years of age. An additional inclusion criterion was that the participants had to be able to communicate with the researchers either directly or through professional interpreters from Swedish sign language to spoken Swedish. Those who were interested in participation were called upon to contact the researchers to obtain more information and make appointments for interviews (reported elsewhere) and to answer the questionnaires.
In all, 38 individuals were included in the study, i.e., 20 adults, of which 14 had deafblindness and 6 were partners to the parent with deafblindness, and 18 children (aged 5–19 years). However, not all of the participants answered the questionnaires and some gave incomplete answers; therefore, the number of participants varied between the analyses. The number of participants who answered each questionnaire is indicated in the results.
The characteristics of the families and the individuals in the families will be further described in the results.
Ethical Considerations
The project in which the present study is housed is one of four that have been approved by the Regional Ethics Committee of Uppsala (DNR 2016/124). After receiving written and spoken information, all the participants were given the opportunity to ask questions, and then they all signed a written informed consent form.
Individuals with deafblindness constitute a small and rare group in society, and by adding the requirement of having a family and children, the possible number of participants in Sweden becomes even smaller. To prevent the exposure of the participants, caution must be taken when presenting background data and results.
Questionnaires
The participants answered questionnaires about their health-related quality of life, family climate and sense of coherence. The Swedish age-relevant versions of the questionnaires have been used (see Table 1).
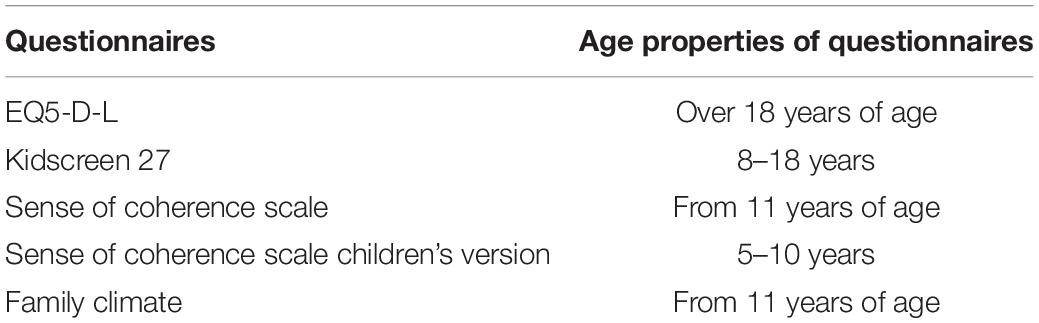
Table 1. Questionnaires and age properties used in the study.
EQ5-D-L
The EQ5 is a standardized measure of health status developed by the EuroQoL Group to provide a generic measure of health (EuroQol Group, 1990). The questionnaire was further developed in 2005 and resulted in the EQ5-D-L, which is the instrument that was used in the present study. The EQ5-D-L consists of two parts. The first part measures health status within five different dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression). Each dimension can be answered on a five-level graded scale from “no problems” to “extreme problems.” The second part consists of a Visual Analogue Scale (VAS-scale) for self-rated health based on a 20-cm vertical, visual analog scale with the endpoints of “the best health you can imagine” and “the worst health you can imagine;” there is also a box in which the figure marked in the VAS-scale should be written. The mark and the written figure should represent the current health of the respondent. The EQ5-D-L has not previously been used when asking people with deafblindness about their health-related quality of life. However, the questionnaire has been used in different groups of people experiencing chronic diseases (for example, Petersson et al., 2013). The Cronbach’s alpha value for the EQ5-D-L questionnaire in the present study was 0.74, while previous studies have shown a range of 0.73–0.85 (Savoia et al., 2006; Tran et al., 2012).
Kidscreen-27
The Kidscreen questionnaire is a generic health-related quality of life instrument for children and adolescents between 8 and 18 years of age (The Kidscreen Group Europe, 2006; Ravens-Sieberer et al., 2014). Different versions exist, and in the present study, Kidscreen-27 has been used. Children are asked to self-report their subjective health and wellbeing within five dimensions (physical activity and health, feelings, family and free time, friends, school and learning). Questions posed are for example within the domain of physical activity and health; “In general, how would you say your health is?” or within the domain of family and free time; “Have you been able to talk to your parent(s) when you wanted to?” The overall aim of the questionnaire is to identify children who are at risk in terms of their subjective health-related quality of life. The children give their response on a five-level graded scale from “not at all” to “a lot” or “never” to “always.” Psychometric testing to validate the construction and consistency of the questionnaire has been performed in children and adolescents in thirteen European countries as well as in a Swedish context (Ravens-Sieberer et al., 2007; Berman et al., 2016). The Cronbach’s alpha value for the Kidscreen-27 questionnaire in the present study was 0.78, while previous studies have shown a range of 0.78–0.84 (Robitail et al., 2007). The Kidscreen-27 has, to the best of our knowledge, not been previously answered by children from families in which a parent has deafblindness.
Sense of Coherence
Deafblindness means that information received from the surrounding environment can be fragmented, and this could have an impact on how the individual experiences the sense of coherence (SOC). Information about the sense of coherence of individuals with deafblindness as well as their partners is sparse; therefore, this aspect was included in the current study. The SOC questionnaire consists of thirteen questions. An example of a question related to comprehensibility is “Has it happened in the past that you were surprised by the behavior of people whom you thought you knew well?” An example of a question related to manageability is “Has it happened that people whom you counted on disappointed you?” Finally an example of a question with regards to meaningfulness “Do you have a feeling that you don’t really care about what is going on around you?” The maximum score is 91, and the minimum score is 13. The cut-off values are set to 13–57 for low SOC, 58–74 for medium SOC and 75–91 for high SOC (Holmefur et al., 2015). Psychometric testing has been conducted by Holmefur et al. (2015) in a total sample of 623 individuals divided into two groups, one consisting of women from a breast clinic and the other consisting of a random sample from a population register. The Cronbach’s alpha value for the sense of coherence scale in the present study was 0.73, while previous studies have shown a range of 0.70–0.95 (Lindström and Eriksson, 2006).
Sense of Coherence, Children’s Version
Based on the work of Antonvsky, a test measuring children’s sense of coherence has been developed (Margalit, 1998; Margalit et al., 1999). In this study, a translation into Swedish of the instrument made by Familjeforum in Lund has been used (Nagy, 2004). This form consists of 19 statements, three of which are complementary questions that should be easy for the child to answer, e.g., “I like ice cream.” These three statements are not included in the score. The other 16 statements measure how the child perceives the world, as expressed by a sense of comprehensibility, e.g., “When someone gets angry with me, I understand why;” a sense of manageability, e.g., “There is someone who can help me when I need help”; and a sense of meaningfulness, e.g., “Things I do every day are fun and make me happy.” The children respond by using a four-digit scale ranging from (1) never to (4) always. The total score of the test, i.e., the sum of the 16 statements, may vary between 16 and 64, no cut-off values have been identified. However, higher scores indicate a higher sense of coherence. The SOC questionnaire is intended for use in children between the ages of 5 and 10 years. Children aged 11 years or older have answered the adult version of the sense of coherence scale.
The Cronbach’s alpha value for the sense of coherence scale for children in the present study was 0.88, while previous studies, not considering children in families where a parent has deafblindness, have shown a range of 0.72 (Margalit, 1998) to 0.83 (Berntsson, 2003). To the best of our knowledge, the SOC for children has not previously been used for children in families where a parent has deafblindness.
Family Climate Scale
The Family Climate Scale is a Swedish instrument with 85 adjectives measuring four different factors in families, namely, closeness (18 adjectives), distance (11 adjectives), expressiveness (6 adjectives), and chaos (6 adjectives) (Hansson, 1989). The scale is to be used from the age of 11. The respondent is asked to read the words and mark at least 15 words that describe the climate in his or her family. The words are then organized within the factor where it belongs, and an index is created for each of the four dimensions as well as for the total scale. The index is created by dividing the total number of reported words in each dimension by the total sum in each dimension. The index for the total scale is given by dividing the total number of affirmed words by the total number of words in the scale. Closeness is positive and concerns safety, harmony and warmth in the family, a high value indicates closeness in the family. Distance is negative and represents cold separation between family members, a high value indicates a distance in the family. Expressiveness can be both positive and negative and is concerned with significance in the family, both a high and a low value can indicate a good family climate. Chaos describes that the family life is unstable and has many worries, a high value indicates chaos in the family (Hansson, 1989). According to Hansson (1989) a well-functioning family generally has high values on closeness and low values on distance and chaos, while a dysfunctional family has low values on closeness and high values of distance and chaos. The response profiles can be used to interpret how well the family members are consistent in how they experience the climate in the family.
Data Collection
This project includes different methods of data collection, e.g., questionnaires and interviews (presented elsewhere). The participants answered the questionnaires in conjunction with an interview. The participants were also asked to fill out background information. Some participants needed, due to their visual impairment, additional help to be able to answer the questionnaires. This help was administered by a professional interpreter or by one of the researchers (MW) (bilingual in Swedish and Swedish sign language), who signed or read the question out loud, including the alternative possibility answers, and then marked the answer given by the participant. Children who could read filled out the questionnaires by themselves and had the ability to ask questions to the researchers (AAC, MB, and KH) if needed. Those children who were not able to read had the questions read out loud to them by the researchers Most of the children answered the questionnaires without their parents; however, one child had a parent present when answering the questionnaire.
Analysis
The questionnaires that were completed by the participants were imputed into IBM® SPSS Software version 22. The instructions for how to summarize each questionnaire have been followed, and descriptive statistics such as frequencies, mean values, median values and cross tables have been used to analyze the empirical data.
Results
Due to the small number of participants in this study, the results reported will be descriptive.
Characteristics of the Participants
In all, the 16 families included comprised 14 parents with deafblindness, 6 partners and 18 children. Their background characteristics are presented in Table 2.
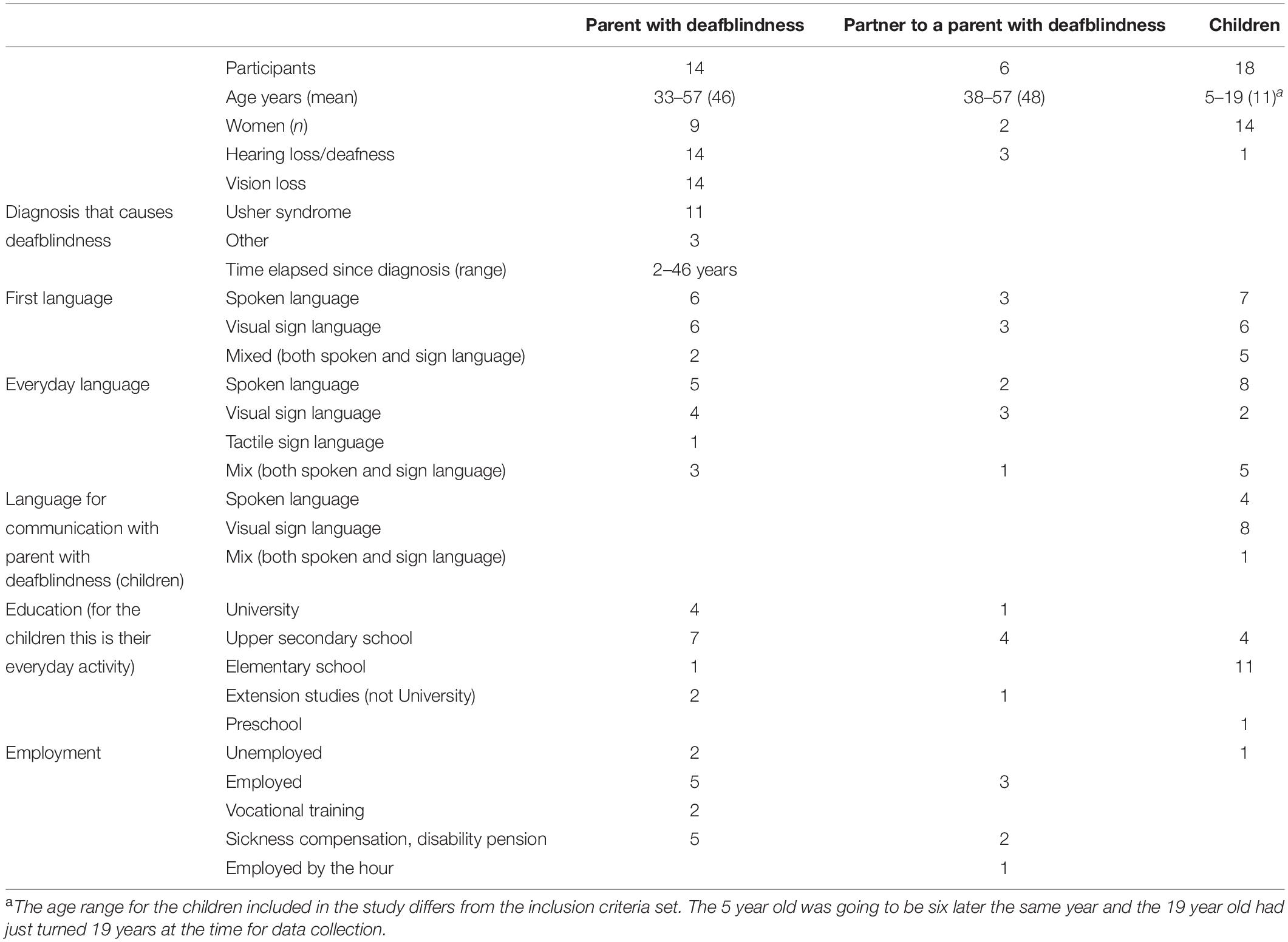
Table 2. Characteristics of participants in study.
Health-Related Quality of Life
Both the parents and children were asked about their health-related quality of life using different questionnaires, the EQ5-D-L and the Kidscreen-27, respectively. In total, 16 adults (12 parents with deafblindness and 4 partners) answered the EQ5-D-L, and their results are shown in the diagrams below (Figures 1, 2). The most frequently reported problems were in the dimensions of mobility, usual activities and anxiety or depression. When dividing the respondents into the parents with deafblindness or the other parents, a pattern emerged in which it was the parent with deafblindness who reported the most frequent problems (Figure 2).
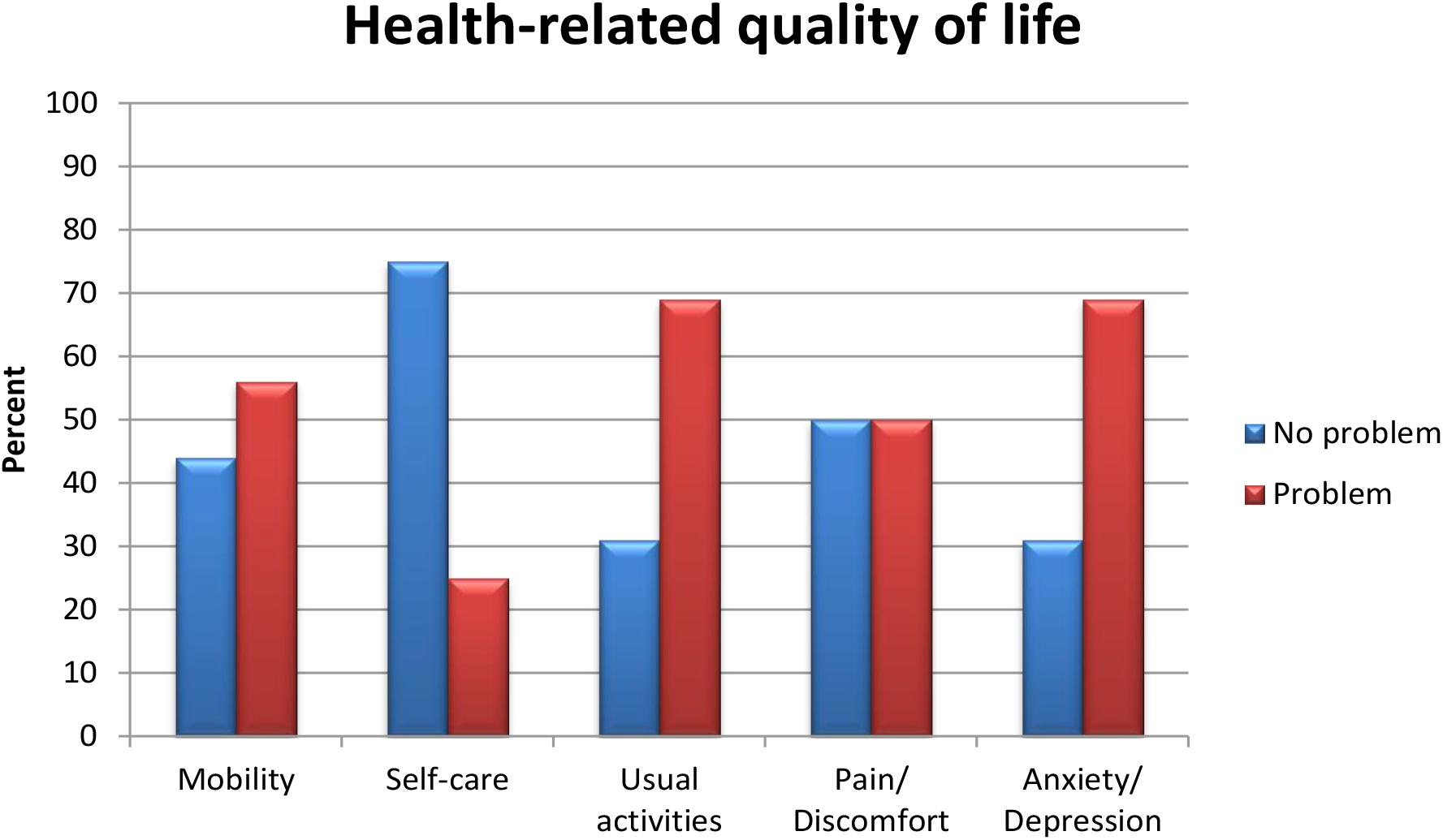
Figure 1. Health-related quality of life, problem or no problem reported, parents with deafblindness and partner, n = 16.
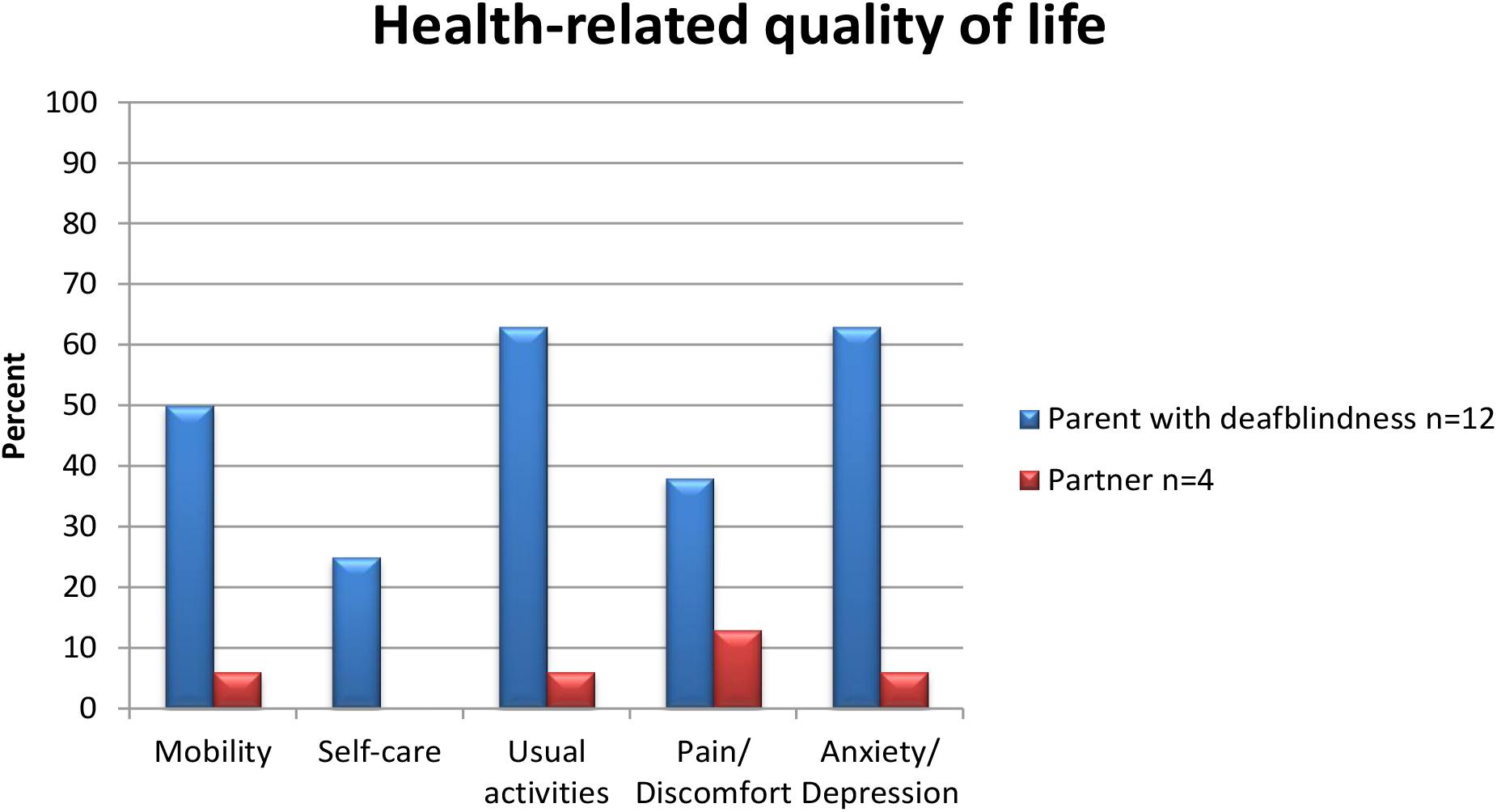
Figure 2. Health-related quality of life problems reported, parents with deafblindness and partner.
VAS-Scale EQ5-DL
Both parents with and without deafblindness were asked to rate their health. The mean value for their current health was 68 (range 25–100). Parents with deafblindness rated their current health with a mean value of 64 (SD = 23.98). For partners, the mean figure for their current health was 79 (SD = 21.75).
Kidscreen-27
Descriptive data (mean values and St. D.) from Kidscreen-27 are presented for each of the dimensions (Table 3). The total number of children included in the project was 18. Not all children completed the Kidscreen-27 due to age. In all 12 children completed the Kidscreen-27. However, internal missing for the dimensions in the Kidscree-27 exists, the included n is given for each dimension in Table 3.
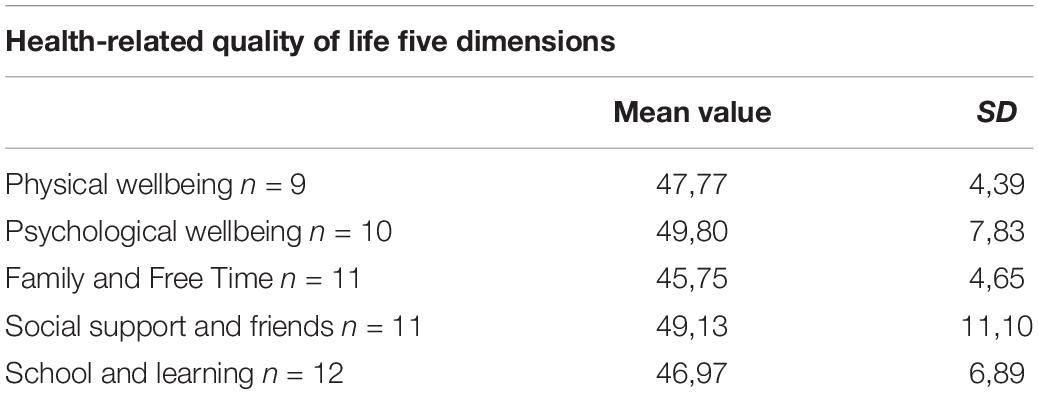
Table 3. The health-related quality of life in children, presented in five dimensions, Mean value and SD.
The interpretation of the results from the children and adolescents included in this study has to be undertaken with caution. However, the patterns identified do not differ significantly when compared with the findings of Ravens-Sieberer et al. (2007) or with the norm material included in the Kidscreen questionnaires handbook (The Kidscreen Group Europe, 2006). A mean T-value of 50 is considered a good health-related quality of life, and the results of the health-related quality of life in the present study are slightly decreased (see Table 3).
Sense of Coherence
The results revealed that none of the groups reported a high sense of coherence (SOC). The reported SOC mean values were found to be either low or moderate. Parents with deafblindness (n = 13) mean score 51.7, partner (n = 4) 68.7, children 5–10 years (n = 10), 45.5, and children ≥ 11 years (n = 7), presented with a mean score of 47.4.
Family Climate
The family members were asked to describe how they experienced the family climate. Twelve parents with deafblindness, four partners and nine children completed the family climate scale (Figure 3). A similar pattern was revealed for the different perspectives, where all groups reported the positively loaded factor of closeness. Distance was not an apparent factor in the families. The factor with words related to expressiveness was more diverse between the different family members. Parents with deafblindness had a higher degree of marked words that related to the factor of expressiveness than did their partners or children. The fourth factor in the family climate scale deals with chaos, which is a factor that has a negative meaning. Chaos was reported by the parents with deafblindness and was similarly described by some of the children. No experiences of chaos were reported by the partners (Figure 3).
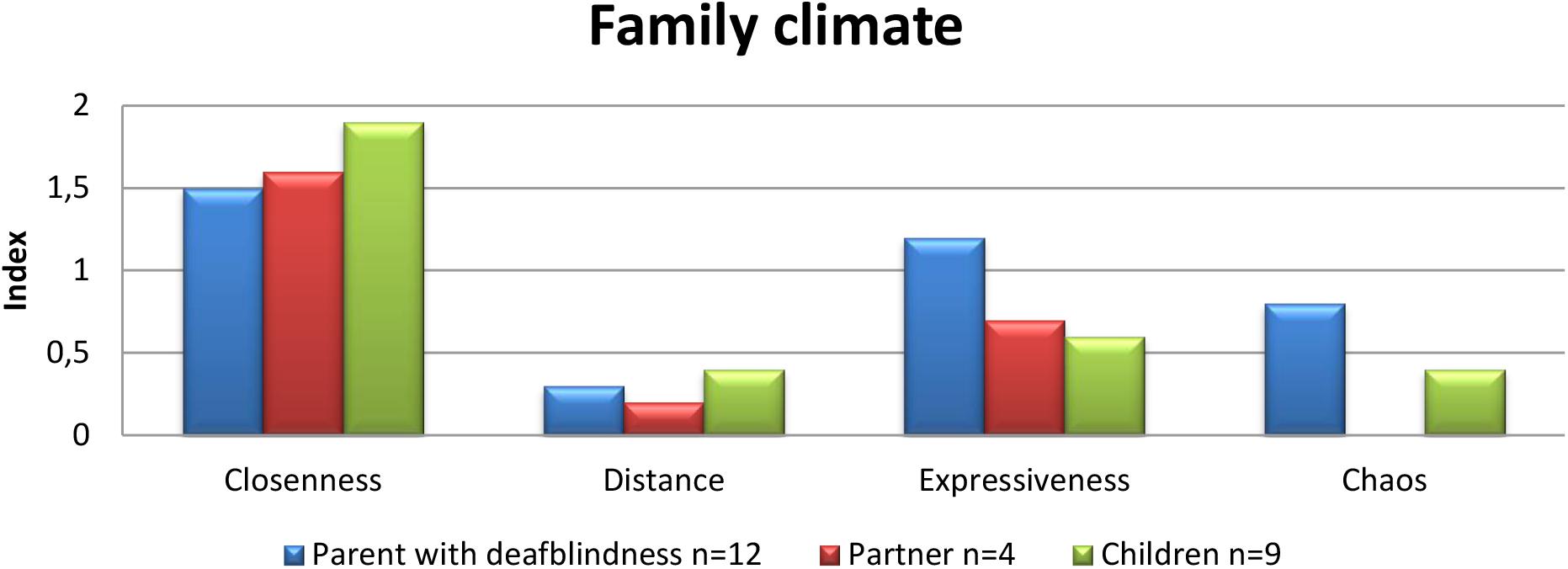
Figure 3. Family climate index. Closeness: a high value indicates closeness in the family. Distance: a high value indicates distance in the family. Expressiveness: includes both positive and negative aspects of emotional expressiveness. Chaos: a high value indicates chaos in the family.
Discussion
The main findings in the present study indicate that family members share a positive feeling of being close to each other. The findings also indicate that in regard to problems reported, parents with deafblindness report the greatest challenges related to health-related quality of life (including mental health issues of anxiety and depression), sense of coherence, expressiveness and chaos. These findings might be understood in light of the consequences of living with deafblindness, such as restrictions in access to information, communication, activities of daily living and mobility (Fletcher and Guthrie, 2013; Hersh, 2013). Furthermore, these outcomes are in conjunction with those of previous research, which have described a compromised health situation for adults with deafblindness (Wahlqvist et al., 2013, 2016a,b; Dean et al., 2017). However, the other members of the families do not report an overall positive experience of their health, quality of life or sense of coherence. For the partner, a lacking sense of coherence was reported, and some problems with health-related quality of life were within the dimensions of pain/discomfort and depression/anxiety. The children in the families also reported a moderate or low sense of coherence and a slightly decreased health-related quality of life. To summarize, in this small-scale study, the findings indicate a risk that health and wellbeing could be affected in the family members of families in which a parent has deafblindness.
All members of a family are affected by how well the family system works. The results of the current study indicate that it is important to consider the whole family’s perspective and their individual needs of support. This issue has not previously been addressed for families in which one parent has deafblindness. Support has instead been offered to the deafblind individuals in these families (Miner, 1995, 1997; Ellis and Hodges, 2013). However, families are heterogeneous, and a family where a parent has deafblindness is assumingly no exception.
According to Antonovsky, a sense of coherence is of great importance for individuals in maintaining their health and meeting challenges in life (Antonovsky, 1987a). Some of the consequences of living with deafblindness could have an impact on the possibility of maintaining a high sense of coherence. It is plausible to assume that when one’s possibility of communicating and accessing information from the surrounding environment is fragmented, then one’s inner consistency in terms of being able to find things meaningful and comprehensible as well as manageable might be affected. However, how should we understand the findings of a moderate or low sense of coherence for the partners and children in such families? With regard to the family as a system (Eriksson et al., 2018), could it be that the insecurity of living with deafblindness has consequences for the other family members as well? Further studies with larger populations from more than one country are needed to determine the mechanism behind this pattern.
Restrictions regarding everyday activities are presented as a consequence of deafblindness (Ellis and Hodges, 2013; Fletcher and Guthrie, 2013; Hersh, 2013), whereas this could be a way to understand the differences in the expressiveness that is reported in the families in the present study. Deafblindness implies a need for structure and the planning of everyday life, leaving little room for doing things spontaneously. For some persons with deafblindness, a guide or interpreter is needed to be able to participate in activities, and if such support is not provided externally, it has to be provided by a family member (Ellis and Hodges, 2013; Hersh, 2013). The chaos that parents with deafblindness express could be interpreted as a deafblind-specific problem. When one lacks information, things can seem random or inconsistent when they occur. In the family system, the partner might be the one who manages different activities and has control of the family life and therefore does not experience the chaos reported by the parent with deafblindness. The children also reported chaos, but not to the extent of the parents who has deafblindness. It is plausible to assume that the children in these families are affected by the chaos that the parents with deafblindness experience, because they are, depending on their age and to various degrees, dependent on their parents. Here, the partner or other parent can act as a buffer for the children, making everyday life more predictable.
Methodological Challenges
Although there were limited numbers of participants in the present study, it is the largest study with a family approach that has been conducted within the field of deafblindness, as far as we know. Despite a comprehensive recruitment strategy, we could not recruit any more participants than we did. As mentioned above, the number of people with deafblindness is limited, and those who are parents comprise an even smaller group. Nevertheless, they and their families have the right to make their voices heard within research similar to that of any other group. However, when conducting research with this group, there are challenges that need to be taken into account. First, the participants must be offered time enough to access information about the aim and participation in the study. Second, the questionnaires should be assessable for the participants. None of the questionnaires used in this study were adapted for people with deafblindness or had been used in this population before, which could be regarded as a limitation (c.f. Wahlqvist et al., 2016b). The authors do acknowledge the use of the Likert scale as interval rather than ordinal (c.f. Bishop and Herron, 2015), and that the scale steps in the Likert scale are not equal. The results are, however, presented in line with how other authors have reported results based on the same questionnaires (c.f. Lustig et al., 2000; The Kidscreen Group Europe, 2006; Holmefur et al., 2015).
This study is one of four housed within a project concerning families where at least one parent has deafblindness. The studies are to be seen as complementary in research methodology, and they describe different perspectives and experiences of living in this type of family.
Conclusion and Implications for Professionals
The aim of this study was to describe the health-related quality of life, sense of coherence and family climate in families where a parent has deafblindness. We identified a positive family climate characterized by a feeling of closeness but also a risk of poor health-related quality of life and a decreased sense of coherence among the family members.
Since this is the first study focusing on this perspective and the number of participants is low from a quantitative study perspective, this area of study calls for further research.
For professionals who are to provide support to persons with deafblindness, the findings of the current study indicate that the whole family needs to be asked about their situation and about their need for support. How this support should be organized and what should be included in this support should be further studied. Until then, we suggest that the risk for poor health-related quality of life in the family members of a parent with deafblindness should always be considered when encountering them both as individuals and as a family.
Data Availability Statement
Due to privacy concerns, the data will not be made publicly available.
Ethics Statement
The studies involving human participants were reviewed and approved by the Regional Ethics Committee of Uppsala (DNR 2016/124). Written informed consent to participate was given by the parents with deafblindness and the partners. From the children informed consent to participate in this study was provided by the legal guardian/next of kin.
Author Contributions
KH and MW were responsible researchers in the analysis and writing of the manuscript. MB and AA-C took an active part in the discussion of the results of the analysis and in the process of writing, reading and commenting in all parts of the manuscript. AA-C, KH, and MB were responsible for the design of the study. AA-C was the PI of the project. All authors took part in the data collection process.
Funding
This study was part of a project called “Health and family life in families where a parent has deafblindness” and has been funded by the research fund of Stiftelsen MoGård, Nyckelfonden and the Region Örebro County, Sweden. Funding includes open access publication fees and funding for language editing, Region Örebro County.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We wish to thank the families who have contributed by offering their time and sharing their stories about their experiences of family life when a parent has deafblindness. Furthermore, we wish to thank the family section of the Association of the Swedish Deafblind and the Swedish National Resource Center for Deafblindness for their contributions to the design and carrying through of the project.
Footnotes
References
Antonovsky, A. (1987a). The salutogenic perspective: toward a new view of health and illness. Advances 4, 47–55.
Antonovsky, A. (1987b). Unraveling the Mystery of Health: How People Manage Stress and Stay Well. San Francisco, CA: Jossey-Bass.
Arcous, M., Putois, O., Dalle-Nazebi, S., Kerbourch, S., Cariou, A., Ben Aissa, I., et al. (2019). Psychosocial determinants associated with quality of life in people with usher syndrome. A scoping review. Disabil. Rehabil. 12, 1–12. doi: 10.1080/09638288.2019.1571637
Ask Larsen, F., and Damen, S. (2014). Definitions of deafblindness and congenital deafblindness. Res. Dev. Disabil. 35, 2568–2576.
Bergström, M., Fransson, E., Hjern, A., Köhler, L., and Wallby, T. (2014). Mental health in Swedish children living in joint physical custody and their parents’ life satisfaction: a cross-sectional study. Scand. J. Psychol. 55, 433–439. doi: 10.1111/sjop.12148
Berman, A. H., Liu, B., Ullman, S., Jadbäck, I., and Engström, K. (2016). Children’s quality of life based on the KIDSCREEN-27: child self-report, parent ratings and child-parent agreement in a Swedish random population sample. PLoS One 11:e0150545. doi: 10.1371/journal.pone.0150545
Berntsson, T. (2003). BARNKASAM. En Första Valideringsstudie (Sense of Coherence for Children. A Validation Study). Lund: Lund University.
Bishop, P. A., and Herron, R. L. (2015). Use and misuse of the likert item responses and other ordinal measures. Int. J. Exerc. Sci. 8, 297–302.
Dalby, D. M., Hirdes, J. P., Stolee, P., Strong, J. G., Poss, J., Tjam, E. Y., et al. (2009). Characteristics of individuals with congenital and acquired deaf-blindness. J. Vis. Impairment Blind. 103, 93–102.
Dam, K., and Hall, E. O. C. (2016). Navigating in an unpredictable daily life: a metasynthesis on children’s experiences living with a parent with severe mental illness. Scand. J. Caring Sci. 30, 442–457. doi: 10.1111/scs.12285
Dean, G., Orford, A., Staines, R., McGee, A., and Smith, K. J. (2017). Psychosocial well-being and health-related quality of life in a UK population with Usher syndrome. BMJ Open 7:e013261.
Ehn, M., Anderzén-Carlsson, A., Möller, C., and Wahlqvist, M. (2019). Life strategies of people with deafblindness due to Usher syndrome type 2a - a qualitative study. Int. J. Qual. Stud. Health Well Being 14:1656790. doi: 10.1080/17482631.2019.1656790
Ellis, L., and Hodges, L. (2013). Life and Change with Usher: The Experiences of Diagnosis for People with Usher Syndrome. Birmingham: University of Birmingham.
Eriksson, M., Ghazinour, M., and Hammarström, A. (2018). Different uses of Bronfenbrenner’s ecological theory in public mental health research: what is their value for guiding public mental health policy and practice? Soc. Theory Health 16, 414–433. doi: 10.1057/s41285-018-0065-6
Eriksson, M., and Lindström, B. (2007). Antonovsky’s sense of coherence scale and its relation with quality of life: a systematic review. J. Epidemiol. Community Health 61, 938–944.
Eriksson, M., and Svedlund, M. (2006). ‘The intruder’: spouses’ narratives about life with a chronically ill partner. J. Clin. Nurs. 15, 324–333.
EuroQol Group (1990). EuroQol- a new facility for the measuremnet of health-related quality of life. Health Policy 16, 199–208.
Fletcher, P. C., and Guthrie, D. M. (2013). The lived experiences of individuals with acquired deafblindness: challenges and the future. Int. J. Disabil. Commun. Rehabilitat. 12:1.
Hersh, M. (2013). Deafblind people, communication, independence, and isolation. J. Deaf Stud. Deaf Educ. 18, 446–463. doi: 10.1093/deafed/ent022
Holmefur, M., Sundberg, K., Wettergren, L., and Langius-Eklöf, A. (2015). Measurement properties of the 13-item sense of coherence scale using Rasch analysis. Qual. Life Res. 24, 1455–1463. doi: 10.1007/s11136-014-0866-6
Jacob, J., Canchola, J. A., and Preston, P. (2019). Young adult children of parents with disabilities: self-esteem, stigma, and overall experience. Stigma Health 4, 310–319. doi: 10.1037/sah0000145
Lehane, C. M., Dammeyer, J., and Elsass, P. (2017a). Sensory loss and its consequences for couples’ psychosocial and relational wellbeing: an integrative review. Aging Ment. Health 21, 337–347. doi: 10.1080/13607863.2015.1132675
Lehane, C. M., Dammeyer, J., Hovaldt, H. B., and Elsass, P. (2017b). Sexuality and well-being among couples living with acquired deafblindness. Sex. Disabil. 35, 135–146. doi: 10.1007/s11195-016-9470-8
Lehane, C. M., Elsass, P., Hovaldt, H. B., and Dammeyer, J. (2018). A relationship-focused investigation of spousal psychological adjustment to dual-sensory loss. Aging Ment. Health 22, 397–404. doi: 10.1080/13607863.2016.1268091
Lindström, B., and Eriksson, M. (2006). Contextualizing salutogenesis and Antonovsky in public health development. Health Promot. Int. 21, 238–244. doi: 10.1093/heapro/dal016
Lustig, D. C., Rosenthal, D. A., Strauser, D. R., and Haynes, K. (2000). The relationship between sense of coherence and adjustment in persons with disabilities. Rehabil. Counsel. Bull. 43, 134–141. doi: 10.1177/003435520004300302
Lustig, D. C., and Strauser, D. R. (2008). The impact of sense of coherence on career thoughts for individuals with disabilities. Rehabil. Counsel. Bull. 51, 139–147. doi: 10.1177/0034355207311313
Margalit, M. (1998). Loneliness and coherence among preschool children with learning disabilities. J. Learn. Disabil. 31, 173–180. doi: 10.1177/002221949803100207
Margalit, M., Tur-Kaspa, H., and Most, T. (1999). Reciprocal nominations, reciprocal rejections and loneliness among students with learning disorders. Educ. Psychol. 19, 79–90. doi: 10.1080/0144341990190106
Miner, I. D. (1995). Psychosocial implications of Usher Syndrome, Type-I, throughout the life-cycle. J. Vis. Impairment Blind. 89, 287–296.
Miner, I. D. (1997). People with Usher syndrome Type II: issues and adaptations. J. Vis. Impairment Blind. 91, 579–589.
Nagy, E. (2004). Barns Känsla av Sammanhang - En Valideringsstudie av BarnKASAM i årskurserna 1-6 (7-12 år). Master thesis, Lunds Universitet, Lund.
Nordens Välfärdscenter (2016). Dövblindverksamhet. Available online at: https://nordicwelfare.org/funktionshinder/dovblindverksamheten/ (accessed June 15, 2020).
Olsson, M. B., and Hwang, C. P. (2002). Sense of coherence in parents of children with different developmental disabilities. J. Intellect. Disabil. Res. 46, 548–559.
Payne, D., and McPherson, K. M. (2010). Becoming mothers. Multiple sclerosis and motherhood: a qualitative study. Disabil. Rehabil. 32, 629–638. doi: 10.3109/09638280903204708
Petersson, C., Simeonsson, R. J., Enskar, K., and Huus, K. (2013). Comparing children’s self-report instruments for health-related quality of life using the international classification of functioning, disability and health for children and youth (ICF-CY). Health Qual. Life Outcomes 11:75. doi: 10.1186/1477-7525-11-75
Ravens-Sieberer, U., Auquier, P., Erhart, M., Gosch, A., Rajmil, L., Bruil, J., et al. (2007). The KIDSCREEN-27 quality of life measure for children and adolescents: psychometric results from a cross-cultural survey in 13 European countries. Qual. Life Res. 16, 1347–1356. doi: 10.1007/s11136-007-9240-2
Ravens-Sieberer, U., Herdman, M., Devine, J., Otto, C., Bullinger, M., Rose, M., et al. (2014). The European KIDSCREEN approach to measure quality of life and well-being in children: development, current application, and future advances. Qual. Life Res. 23, 791–803. doi: 10.1007/s11136-013-0428-3
Rena, F., Moshe, S., and Abraham, O. (1996). Couples’ adjustment to one partner’s disability: the relationship between sense of coherence and adjustment. Soc. Sci. Med. 43, 163–171. doi: 10.1016/0277-9536(95)00358-4
Robitail, S., Ravens-Sieberer, U., Simeoni, M.-C., Rajmil, L., Bruil, J., Power, M., et al. (2007). Testing the structural and cross-cultural validity of the KIDSCREEN-27 quality of life questionnaire. Qual. Life Res. 16, 1335–1345. doi: 10.1007/s11136-007-9241-1
Sagy, S., and Antonovsky, H. (2000). The development of the sense of coherence: a retrospective study of early life experiences in the family. Int. J. Aging Hum. De. 51, 155–166. doi: 10.2190/765l-k6nv-jk52-ufkt
Savoia, E., Fantini, M. P., Pandolfi, P. P., Dallolio, L., and Collina, N. (2006). Assessing the construct validity of the Italian version of the EQ-5D: preliminary results from a cross-sectional study in North Italy. Health Qual. Life Outcomes 4:47. doi: 10.1186/1477-7525-4-47
Simcock, P. (2017). One of society’s most vulnerable groups? A systematically conducted literature review exploring the vulnerability of deafblind people. Health Soc. Commun. 25, 813–839. doi: 10.1111/hsc.12317
The Kidscreen Group Europe (2006). The KIDSCREEN Questionnaries, Quality of Life Questionnaires for Children and Adolecents. Lengerisch: Pabst Science Publishers.
Tran, B. X., Ohinmaa, A., and Nguyen, L. T. (2012). Quality of life profile and psychometric properties of the EQ-5D-5L in HIV/AIDS patients. Health Qual. Life Outcomes 10:132. doi: 10.1186/1477-7525-10-132
Wahlqvist, M., Möller, C., Möller, K., and Danermark, B. (2013). Physical and psychological health in persons with deafblindness that is due to Usher Syndrome Type II. J. Vis. Impairment Blind. 107, 207–220.
Wahlqvist, M., Möller, C., Möller, K., and Danermark, B. (2016a). Implications of deafblindness: the physical and mental health and social trust of persons with Usher Syndrome Type 3. J. Vis. Impairment Blind. 110, 245–256.
Wahlqvist, M., Möller, K., Möller, C., and Danermark, B. (2016b). Physical and psychological health, social trust, and financial situation for persons with Usher syndrome type 1. Br. J. Vis. Impairment 34, 15–25. doi: 10.1177/0264619615610158
Keywords: deafblindness, family climate, family life, health, sense of coherence
Citation: Wahlqvist M, Björk M, Anderzén-Carlsson A and Huus K (2020) Health-Related Quality of Life, Family Climate and Sense of Coherence of Families in Which a Parent Has Deafblindness. Front. Educ. 5:143. doi: 10.3389/feduc.2020.00143
Received: 03 March 2020; Accepted: 16 July 2020;
Published: 18 August 2020.
Edited by:
Timothy Scotford Hartshorne, Central Michigan University, United StatesReviewed by:
John Ravenscroft, University of Edinburgh, United KingdomSarah Anne Fraser, University of Ottawa, Canada
Copyright © 2020 Wahlqvist, Björk, Anderzén-Carlsson and Huus. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Moa Wahlqvist, bW9hLndhaGxxdmlzdEByZWdpb25vcmVicm9sYW4uc2U=; bW9hLndhaGxxdmlzdEBua2NkYi5zZQ==
†ORCID: Moa Wahlqvist, orcid.org/0000-0002-6965-6820; Agneta Anderzén-Carlsson, orcid.org/0000-0001-7352-8234