 Shibo Shang
Shibo Shang Hongxing Li
Hongxing Li Li Wang1
Li Wang1- 1National Center for Rural Water Supply Technical Guidance, Chinese Center for Disease Control and Prevention, Beijing, China
- 2Office for Public Health Management, Chinese Center for Disease Control and Prevention, Beijing, China
Proper sanitation facilities promote health because they allow people to dispose of their waste appropriately. Since the founding of the People’s Republic of China, the Chinese government has been committed to improving water and sanitation. The coverage of sanitary latrines in rural China reached more than 70.0% in 2022. Using published literature, open data, and national statistics, this study evaluated the health effects of improved latrines in China. A search strategy aimed at collecting all latrine improvement-related community intervention research in China from 1990 to 2021 was designed and implemented. Incidences of three diseases—schistosomiasis, diarrheal disease, and soil-transmitted helminths (STH)—were used as indicators of health benefits. The relationship between adjusted relative risk (RR) and coverage of sanitary latrines in the study area was examined using a log-linear model. Overall, 411 incidences of the three diseases before and after community intervention were extracted from 74 qualified articles. The results demonstrated the importance of promoting access to sanitary latrines in disease prevention and control in China. The overall estimates revealed mean reductions of 60% for diarrhea risk, 42% for schistosomiasis risk, and 65% for STH risk compared to no intervention. In addition, increasing sanitary latrine coverage was negatively correlated with RR in China, indicating that populations with high sanitary latrine coverage were less likely to be affected with water, sanitation, and hygiene-related diseases.
1 Introduction
Poor excreta disposal is associated with cholera, typhoid, paratyphoid fevers, schistosomiasis, and hookworm disease, whereas proper sanitation facilities promote health because they allow people to dispose of their waste appropriately. Inadequate sanitation combined with contaminated water and poor hygiene is the leading cause of morbidity and mortality in low-income countries (WHO, 2021). In 2020, nearly half of the world’s population lacked safely managed sanitation and 494 million people still defecated in the open (WHO/UNIFC, 2021). Moreover, 80% of infectious diseases, such as children’s diarrhea and schistosomiasis, are caused by fecal pollution and unsafe drinking water, and environments with high fecal contamination put people at risk of long-term exposure to intestinal pathogens. Therefore, improvement of basic sanitation facilities is an important development goal in low- and middle-income countries (Deshpande et al., 2020).
Sanitation, especially sanitary latrines, can decrease the transmission of a variety of diseases (Reese et al., 2019). Indeed, improved latrines and sanitation can effectively stop most fecal–oral transmitted diseases (Pickering and Davis, 2012; Odagiri et al., 2016). Because human excreta may contain many types of pathogens and these pathogens can remain infectious for long periods when introduced into the environment, these pathogens can be transmitted to new victims in a number of ways and can therefore present a potential threat to human health (Wagner and Lanoix, 1958). Therefore, effective excreta management at the household and community levels plays important roles in protecting water resources and the food supply from fecal contamination (Fewtrell and Bartram, 2001). Related studies have shown that the popularization of sanitary latrines can directly and effectively prevent and control the incidence of some kinds of intestinal infectious diseases (Chen and Kallawicha, 2021). Moreover, increased sanitation latrine coverage can reduce the risk of exposure to fecal pathogens and can provide health benefits. Furthermore, associations between increased latrine coverage and reduced incidences of related diseases have been observed at the ecological level (Lin et al., 2020).
Improved sanitation facilities are defined as those that ensure hygienic separation of human excreta from human contact (UNICEF, 2018). For most countries, rural access to improved sanitation facilities typically lags behind urban areas (Hannah and Max, 2021; Wu et al., 2022). Goal 6 of the United Nations’ proposed 2030 Sustainable Development Goals (SDGs) is to achieve access to adequate and equitable sanitation and hygiene for all and to end open defecation (UN, 2016). For most countries, open defecation in urban areas is typically below 20% of the population, but in rural areas, this can range from 20 to 90% (Hannah and Max, 2021). Therefore, there is an urgent need to further reduce gaps in access to improved drinking water and sanitation between rural and urban areas. At the global level, a series of programs have been designed to improve sanitation and hygiene with a focus on the needs of rural residents, women, girls, and school students. These programs focus on latrine construction, sanitation science and technology, community-led health education, and policy advocacy (Tumwine et al., 2003; Fewtrell et al., 2005; Banke et al., 2006; Strunz et al., 2014; Du et al., 2019; Patel et al., 2019; Rheinländer et al., 2019; Als et al., 2020; Darmstadt et al., 2020; Morse et al., 2020).
As one of the largest developing agricultural countries in the world, China has been continuously implementing measures to improve sanitation coverage (Li et al., 2022). Latrines were regarded as obscure and dirty things in Chinese culture because of the association with human excreta, although human excrement had always been the most common fertilizer in China’s rural areas. After the establishment of the People’s Republic of China (PRC) in the 1950’s, the Patriotic Health Campaign (PHC) was launched to reduce disease and improve health conditions (Yang, 2004; Chen and Kallawicha, 2021). As one of the most important parts of the PHC, rural latrine improvement, which consists of measures aimed at providing sanitary latrines for households in China, has been continuously promoted by a series of policies, projects, and investments in the PHC. Now, “latrine improvement” has been updated to “latrine revolution,” with the additional goal of creating sanitation infrastructure and public services that work for everyone while turning waste into a value product (Cheng et al., 2018) (Tao, 2019).
In the 1990s, the Chinese government listed coverage of rural sanitary latrines as China’s primary health care index for measurement of attaining the goal of a minimum standard of health care for all residents by the year 2000 (WHO, 1981). In 2005, the government put forward the concept of “Building a New Socialist Countryside,” which emphasized improvement of water and latrines and used the construction of biogas digesters to promote changes in latrines in rural areas (Feng et al., 2012). The portion of the population with improved environmental sanitation facilities in China increased from 48% in 1990 to 76% in 2015 (WHO/UNIFC, 2021), and China achieved the water and sanitation goals outlined in the Millennium Development Goals (MDGs) by 2015. According to Health China 2030 Program Planning, the goal of China’s rural latrine revolution is to achieve 100% sanitary latrine coverage by 2030 (Dong et al., 2020).
Both latrine improvement and the latrine revolution have produced huge social, economic, and health benefits. In China, many epidemiological studies have focused on the health benefits of improved sanitation since the 1990’s, especially those from improved latrines. At the national level, such benefits could be summarized based on the reduction of specific diseases (Esrey, 1996; Clasen et al., 2010; Chen and Kallawicha, 2021). The mortality of WASH-related diseases varies in different countries, and significant differences in the burden of disease (BOD) have been observed between countries. For example, the mortality of children under 5 years old caused by diarrheal diseases in Chad (499 deaths per 100,000) was much higher than that in some areas such as the United States (4 deaths per 100,000) in 2016 (GBD, 2018). Moreover, it is likely that the health benefits of WASH intervention vary in different countries. For example, a study in Tanzania (Young et al., 2007) revealed that improved sanitation could reduce the risk of Ascaris lumbricoides infection by 67%, while only reducing the risk by 32% in Nigeria (Asaolu et al., 2002). No such assessments have been conducted in China, despite its long-term rural toilet improvement plan.
We designed this system review to evaluate the health benefits of latrine improvement in China and obtain evidence-based results. Because there are many sanitation-related diseases, we selected three typical diseases, namely, schistosomiasis, diarrhea, and STH. These diseases were selected for the following reasons: 1) they were widely prevalent in the early days in China; 2) there were sufficient research articles associated with these diseases in China to conduct reviews; and 3) they are related to poor sanitation, including the lack of a sanitary latrine in households.
2 Methods
2.1 Search Strategy
A search strategy was designed and implemented to collect all published and available literature on latrine improvement intervention and its effects on these three diseases in both Chinese and English. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Liberati et al., 2009) guidelines were followed when these systematic review and meta-analysis were conducted. A systematic database search of MEDLINE, Embase, and the Web of Science was conducted to identify potentially relevant English literature. At the same time, the China National Knowledge Infrastructure (CNKI), WanFang Data E-Resources, and VIP Journal Integration Platform were also searched for Chinese-language records. We defined two groups of key search terms: one including the three targeted diseases, “schistosomiasis,” “bilharziasis,” “diarrhea,” “soil-transmitted helminth” (STH, including ascariasis, trichuriasis, hookworm [Ancylostoma duodenale and Necator americanus], and Strongyloides stercoralis) and their synonyms, and another including intervention information such as “latrine,” “sanitation,” “intervene,” and their synonyms. Search terms and their synonyms were combined using the Boolean operator to capture as many documents as possible. The Boolean operator “or” was used to connect the keywords in the group, whereas “and” was used to connect the keywords between groups. The retrieved literature was limited to publication dates between 1990 and 2021.
2.2 Study Inclusion and Exclusion Criteria
We first filtered the articles according to title and abstract to ensure that they were not obviously beyond the scope of the review, after which we went to the next step of screening. We used the defined criteria to assess the eligibility of each retained article and extract data. The inclusion criteria were as follows: 1) the definition of the specific intervention measures and these measures, including the improved latrines. 2) The outcome indicators were measured by the occurrence of schistosomiasis, diarrhea, and STH. 3) The study design was required to consist of cross-sectional or community intervention experiments. The exclusion criteria were as follows: 1) latrine improvement was not included as an intervention measure; 2) studies were conducted in an outbreak background; and 3) control group data were not available.
Three researchers reviewed and screened all available titles and abstracts to identify potentially eligible records for full-text review. In the initial screening, only titles and abstracts were examined to avoid unintentional bias when looking at author names, publication types, and journal titles. On the basis of the content of the title and/or abstract, records of any latrine-related infection agent interventions that may have involved schistosomiasis, diarrhea, and STH were kept to exclude studies that did not meet the requirements of this step. In addition, two researchers reviewed all potentially eligible full-text records in accordance with the defined inclusion and exclusion criteria to determine eligibility for data extraction. If there was disagreement about the eligibility of the study at this stage, a third investigator was consulted and included in the discussion until a consensus was reached.
2.3 Data Extraction
Qualified studies were used for data extraction. A spreadsheet data entry table was designed to store data.
The major categories of the items coded included 1) study characteristics (such as author, year, language, and journal), 2) research object characteristics (such as age, quantity, crowd field, and region), 3) intervention characteristics (such as mode, starting year, ending year, and duration), and 4) outcome characteristics (such as disease types, diagnostic method, cases, and incidence).
All data were extracted from the original article independently by two researchers. Two researchers checked the completeness and accuracy of the extracted data, and if there was disagreement, another researcher participated in the discussion and made a decision. After the initial data extraction, one investigator performed a data cleanup and two researchers re-examined all of the final extracted data.
2.4 Data Processing
Relative risk (RR) was used to measure the effect size for each included study. RR, which was the incidence rate of the intervention group divided by the incidence rate of the control group (Eq. 1), indicated the relative risk of the intervention group and control group for a given disease. An RR value of less than 1 suggests that the intervention being considered is associated with a reduction in risk. Moreover, the lower the RR value is, the larger is the effect value (Massad et al., 2009). The Mantel–Haenszel method was then used to pool the effect sizes (Higgins et al., 2019). Inconsistency (i.e., heterogeneity) was assessed with Moran’s I-squared before calculating the pooling effect sizes (Als et al., 2020). When the I-squared statistic was below 50%, the data were considered to have good heterogeneity and a fixed-effects model (FEM) was used; otherwise, a random-effects model (REM) was used (Coory, 2010). The 95% CI was calculated using the natural logarithm of RR and SE of RR (Eq. 2), and the SE was calculated based on the incidence in the intervention group and control group, as well as the n of the two groups (Eq. 3).
In Eq. 3, a is the incidence in the intervention group, b is the incidence in the control group, n1 is the total number of the intervention group, and n2 is the total number of the control group. For this systematic review, latrine improvement was the primary sanitation exposure. This was defined as the use of any type of sanitary latrine, not a specific type. Moreover, because multiple intervention measures rather than individual measures such as latrine improvement were usually implemented to control schistosomiasis, our study compared the effects of different interventions. To accomplish this, the interventions were divided into five types from the perspective of ecology (Table 1). Latrine improvement and the combination of latrine improvement and these five types of interventions were compared using subgroup analysis. To reduce heterogeneity and avoid the impact of the already implemented interventions on the baseline, only studies from no intervention to the first year of intervention were included in the meta-analysis.

TABLE 1. Classification of interventions.
A linear model was used to examine the relationship between the sanitary latrine coverage rate and pooled RR. Because the coverage rate may change with the long duration of the included studies, this study focused on the incremental coverage, which was defined as the difference between the coverage rate at the end of the study and that at the beginning. Because not all coverage data of the included studies were available, provincial-level data were replaced when such coverage rates for the study area were not available (NHFPC, 2012; NHFPC, 2017). Egger’s test and the visual inspection of funnel plots were used to assess possible publication bias in this systematic review. A p > 0.05 for Egger’s test indicated that there was no significant publication bias; otherwise, publication bias existed. An inverted funnel that tends to be symmetrical indicates a smaller publication bias, and an asymmetrical funnel plot indicates a need to investigate the possible causes of the bias (Liu, 2011).
3 Results
3.1 Retrieved Studies
A total of 17,233 articles were retrieved from CNKI (n = 2,936), WanFang (n = 12,058), VIP (n = 2,200), Web of Science (n = 7), PubMed (n = 26), and Embase (n = 6). The detailed search results of each database are shown in Supplementary Tables S1–S8. After removing duplicates, 15,427 articles were identified. Following the review of the titles and abstracts, 15,225 articles were excluded according to the inclusion and exclusion criteria. A full-text review was then conducted to further screen the rest of the articles. On the basis of the exclusion criteria, there were no set control group in 69 articles, no latrine improvement interventions in 33 articles, and no specific disease incidence data in 24 articles. Furthermore, 76 articles met the criteria, including 64 on schistosomiasis, 6 on diarrhea, and 6 on STH. There were few intervention studies on diarrhea and STH possibly because most intervention studies focused on other measures, such as improved water supply, health education, and hygiene, rather than improved latrines. The PRISMA flow diagram is summarized in Figure 1.
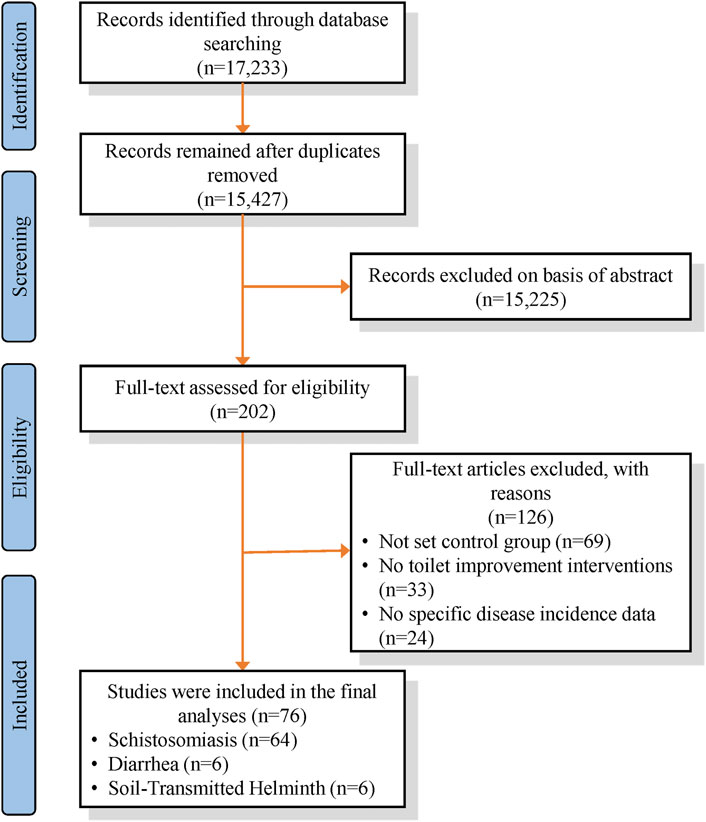
FIGURE 1. Overview of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses strategy used for the selection of articles.
3.2 Characteristics of Extracted Qualified Data
Of the 76 eligible articles, 411 reported results (i.e., potential sample sizes varied with data from different sources or duration of intervention). There were more studies on schistosomiasis than on diarrhea and STH. Overall, there were 376 (91.5%) reports of schistosomiasis, 8 (1.9%) reports of diarrhea, and 27 (6.6%) reports of STH. Among the qualified data, there were 376 (91.5%) community intervention studies that were frequently used for public health. Few were cross-sectional studies, and only 35 (8.5%) studies were conducted. Some other general features of the extracted data by study disease classification are shown in Table 2. When categorized by location, studies covered a total of 13 provinces and cities in the middle and lower reaches of the Yangtze River in China and areas south of the Yangtze River basin. A map of the frequency of eligible studies by province and city in China is provided in Figure 2. The extracted studies were mostly concentrated in the southern region of China and distributed along the Yangtze River valley. Most studies were conducted in Hubei province (n = 156), followed by Anhui (n = 90) and Jiangxi (n = 89). The distribution of the extracted studies was similar to that of schistosomiasis in China, which may have been due to the large proportion of studies of schistosomiasis in the extracted literature.
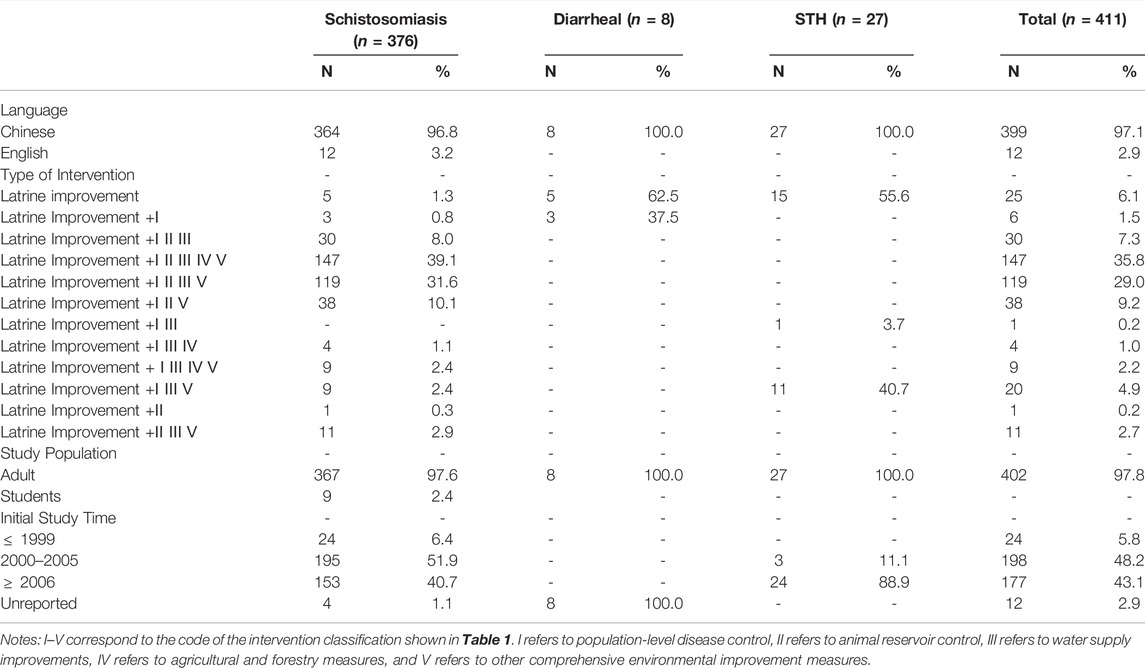
TABLE 2. Overview of eligible records with extractable data.
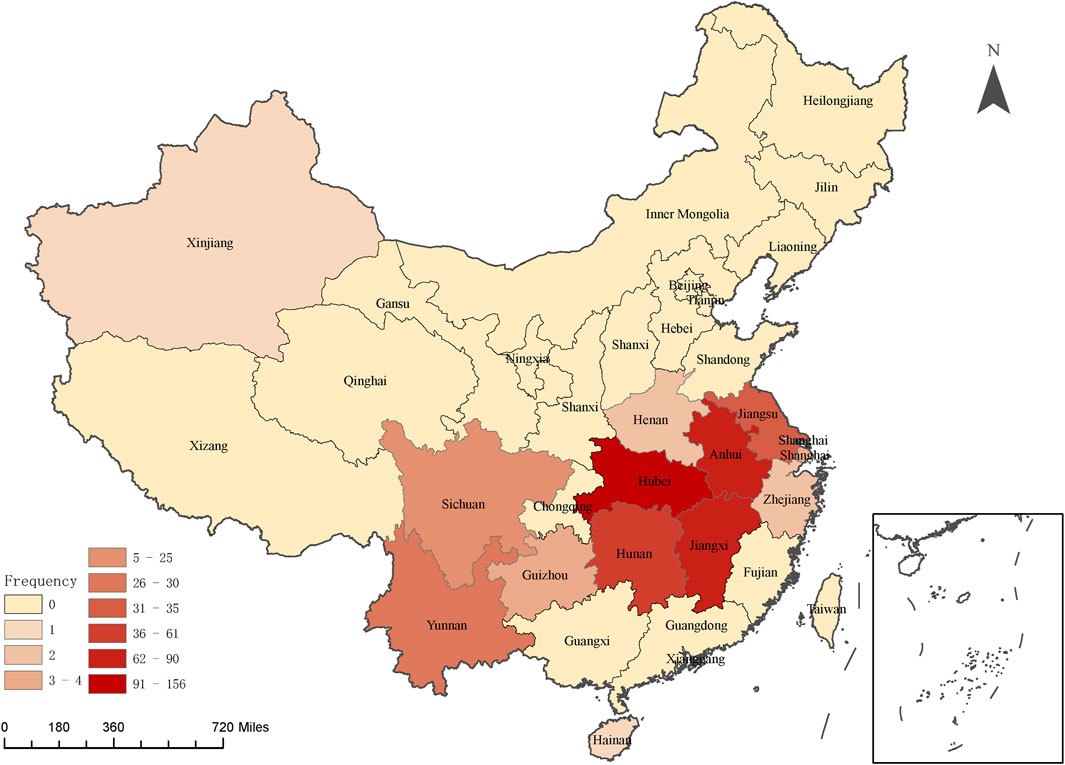
FIGURE 2. Map of China with the number of eligible studies with extractable data by province.
3.3 Latrine Improvement Effects on the Three Investigated Diseases
A total of 114 studies were included in the meta-analysis, among which 82 investigated schistosomiasis, 8 investigated diarrhea, and 24 investigated STH. Of the 82 studies investigating latrine improvement effects on schistosomiasis, 74 showed an infection rate in the intervention group that was significantly lower than that in the control group, 7 showed the opposite results, and 1 revealed no significant difference between groups. All eight diarrheal intervention studies revealed significantly fewer instances of diarrhea in the intervention group than in the control group. Among the 24 STH intervention studies, 20 showed a significantly lower infection rate in the intervention group than in the control group, 3 showed the opposite results, and 1 showed no significant difference.
High heterogeneity was observed for each of the three diseases with an I-squared value of 98% for schistosomiasis, 81% for diarrhea, and 97% for STH. Therefore, a random-effects model was used to pool the effect size. The results revealed that the pooled RR values were less than 1 for all three diseases, and the reduction of the infection rates of schistosomiasis (RR = 0.58, 95% CI: 0.54–0.62), diarrhea (RR = 0.40, 95% CI: 0.28–0.57), and STH (RR = 0.35, 95% CI: 0.25–0.50) was related to the studied interventions. The pooled relative risk for the latrine improvement group and 95% CI for controlling schistosomiasis, diarrheal disease, and STH are summarized in Figure 3.
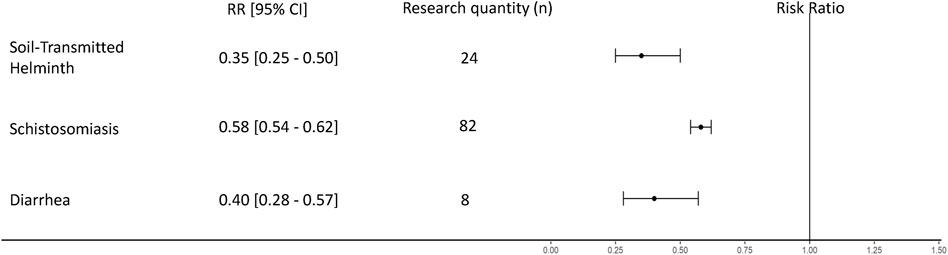
FIGURE 3. Forest plot for schistosomiasis, diarrhea, and soil-transmitted helminths.
The funnel plot of the schistosomiasis studies indicated that there was some potential publication bias (Supplementary Figure S1), as did Egger’s test (p = 0.001). Egger’s test of diarrheal studies did not show significant publication bias (p = 0.314), which is the funnel plot in Supplementary Figure S2. Egger’s test also did not indicate significant publication bias for STH articles (p = 0.398), which is the funnel plot in Supplementary Figure S3.
3.4 Subgroup Analysis of Different Intervention Combinations
Because latrine improvements are often combined with other interventions, the results of RR and 95% CI for these various combinations were consolidated (Figure 4). Based on the definition of intervention types in Table 3, a total of 10 combinations of intervention measures were obtained, and 6 combinations were obtained for schistosomiasis, 2 for diarrhea, and 2 for STH. The results confirmed that latrine improvement intervention alone could decrease the incidence of schistosomiasis (RR = 0.53, 95% CI: 0.50–0.55), diarrhea (RR = 0.46, 95% CI: 0.33–0.63), and STH (RR = 0.68, 95% CI: 0.53–0.87). For schistosomiasis, when combining latrine improvement interventions and other intervention measures, all combinations were associated with a reduction in the incidence rate of the disease, except the combination of latrine improvement and animal reservoir control and other comprehensive environmental improvement measures (II V) (RR = 0.98, 95% CI: 0.65–1.47). The lowest RR (0.63, 95% CI: 0.56–0.70) was observed in the group containing a combination of all interventions (I II III IV V), indicating that this had the best intervention effect. For diarrhea, when water improvement measures (III) were combined with latrine improvement measures, there was a lower RR value (RR = 0.28, 95% CI: 0.08–0.95), indicating a better intervention effect. For STH, when latrine improvement was combined with population-level disease control and water supply improvement measures (I III), there was a higher RR value (RR = 0.20, 95% CI: 0.13–0.29) than was observed for pure latrine improvement (RR = 0.68, 95% CI: 0.53–0.87).
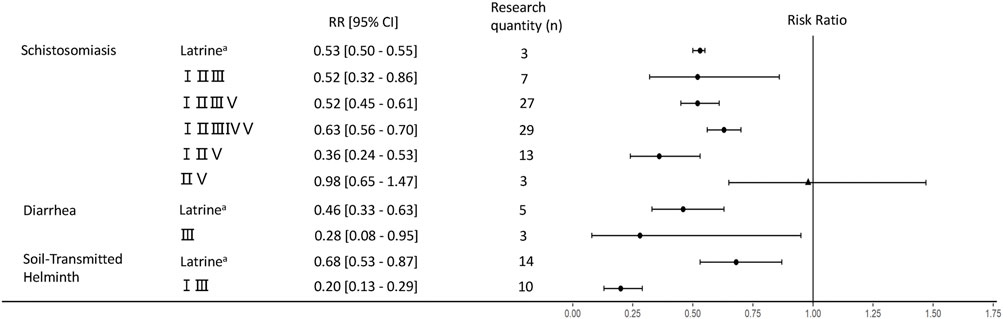
FIGURE 4. Forest plot for latrine improvement and other interventions. Note: a indicate measures of latrine improvement; I–V correspond to the code of the intervention classification shown in Table 1; the figure shows the RR value when these measures are combined with latrine improvement measures; I refers to population-level disease control, II refers to animal reservoir control, III refers to water supply improvements, IV refers to agricultural and forestry measures, and V refers to other comprehensive environmental improvement measures; round dots in the figure indicate that the measure is a protective factor, and triangles indicate that the statistical test of the measure is not significant.
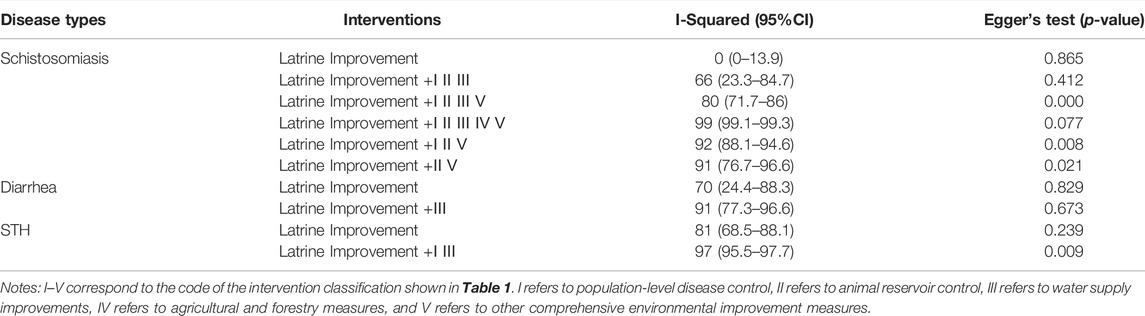
TABLE 3. Overview of eligible records with latrine improvement and other intervention.
The I-squared values of the heterogeneity tests and the Egger’s test information pertaining to publication bias are shown in Table 3. Owing to the limitations of the community intervention experiment, only the I-squared value of the latrine improvement interventions of the schistosomiasis group (I-squared: 0%, 95% CI: 0.0–13.9) was less than 50%. Therefore, the fixed-effects model was adopted. The remaining interventions had large heterogeneity and I-squared values greater than 50%. Therefore, the random-effects model was adopted. Heterogeneity may be caused by the introduction of many different interventions. Of the 10 interventions classified, 6 showed no significant publication bias based on Egger’s test (p > 0.05) and funnel plots (Supplementary Figures S4–S13). For the schistosomiasis group, the intervention group of latrine improvement combined with population-level disease control, animal reservoir control, water supply improvement, and other comprehensive environmental improvement measures (I II III V), as well as the intervention group of latrine improvement combined with population-level disease control, animal reservoir control, and other comprehensive environmental improvement measures (I II V), some small sample studies overestimated the effects of intervention (Deng et al., 2009; He et al., 2011), resulting in publication bias. For STH, the intervention group of latrine improvement combined with population-level disease control and water supply improvement (I III) had a large regional span and wide distribution of intervention starting years in several studies, which led to failure to concentrate the intervention effects (Zhang et al., 2011; Zhu et al., 2011; Deng et al., 2012). In addition, the implementation of intervention measures failed to achieve good results for this group (Chen et al., 2015), which may have led to the observed bias.
3.5 Relationship Between Coverage Increment and Relative Risk
A logarithmic linear equation was adopted to fit the relationship between the annual increase of latrine coverage and RR of annual incidence rate of all included studies. As shown in Figure 5, RR was lower when there was a larger coverage increase, indicating that a greater intervention intensity was associated with better disease prevention effects.
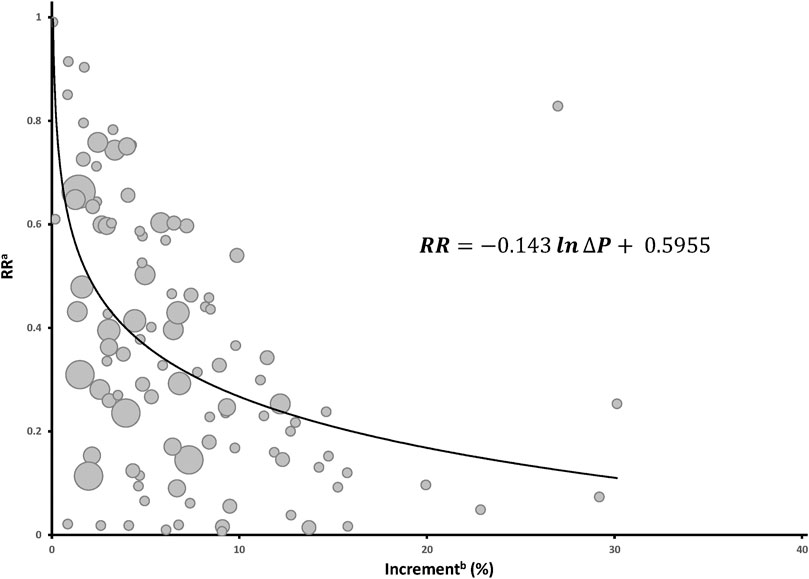
FIGURE 5. Logarithmic fitting diagram of the increase in latrine coverage and relative risk (RR) value. Note: the size of the bubbles represents the number of studies pooled. a RR. This value contains the effect size of the original study and the pooled effect size of several studies (for similar studies with a number less than 3, effect values were not pooled). b Increase represents the annual coverage increase. In the function,
3.6 Publication Bias
On the basis of the funnel plots and Egger’s test, there was no significant publication bias in 8 of the 13 groups of evidence combinations.
4 Discussion
Systematic review and meta-analysis were used to examine the relationship between latrine improvement in China and its health benefits. Our analysis revealed that latrine improvement measures, with or without other public health and nonpublic health interventions, were associated with lower risks of schistosomiasis, diarrhea, and STH infections. Both latrine improvement and the latrine revolution in rural China has had great social, economic, and health benefits, while also improving the environment of rural settlements. Moreover, the incidence of infectious diseases related to WASH has been decreasing annually. However, the incidences of diseases are related to many factors, such as society, the economy, the environment, and population health status. Therefore, more evidence-based data are needed to describe the health benefits of improved sanitation conditions. Nevertheless, this study revealed a correlation between China’s latrine improvement and the incidence of diseases for the first time.
On the basis of our general research objectives, this study included more population-based community intervention trials. Although well designed randomized controlled trials (RCTs) can provide powerful evidence (Melnikow et al., 2013), population intervention trials are more popular in public health studies, especially for population-based sanitation intervention research. Sanitation intervention, especially improved latrine facilities, has been shown to be associated with the reduction of certain diseases in many studies. For example, a study in California showed that the children in households with no sanitary latrines were twice as likely to be infected with Shigella as those in homes with sanitary latrines (Schliessmann, 1959). Moreover, living in an area without sanitary latrines is a risk factor for Hymenolepis nana infection (Al-Mekhlafi, 2020). A meta-analysis of the effects of increased access to sanitation studies revealed that there was at least a 33% reduction in the chance of infection associated with individual WASH practices or access (Strunz et al., 2014). The present study adds to the growing body of evidence that improved sanitation, especially with respect to household latrines in China, is significantly associated with decreased incidence of diseases.
Improved latrines can affect the health of populations through direct or indirect ways. Direct effects include stopping the transmission of certain diseases. During fermentation of excreta in septic tanks, biogas digesters, or other sanitary facilities, pathogenic microorganisms are destroyed and the proliferation of pathogenic microorganisms is prevented, resulting in the excreta becoming harmless. In addition, closed septic tanks prevent microorganisms from entering the environment. When compared with direct application of feces to farmland, use of treated feces is safer and prevents soil pollution. In addition to direct health benefits, improved latrine facilities have indirect effects on human health. For example, household latrine improvements are often combined with improvements in water supply, sanitation, and other basic public health services. Moreover, many studies showed that the effects of combined water and sanitation interventions were often greater than the sum effects of individual measures (Fewtrell et al., 2005; Schmidt, 2014; Luby et al., 2018; Null et al., 2018). Improved sanitary conditions were also found to be beneficial to the formation of personal hygienic behaviors for family members. In addition, health education regarding comprehensive WASH interventions promoted changes in health behavior. At last, the improvement of latrines in rural areas has reduced the BOD of related diseases (Cheng et al., 2018; Chen and Kallawicha, 2021) and promoted increased household incomes, which has brought about further improvements in health and medical levels.
The results of this study revealed that there were similar health effects on water, sanitation, and hygiene (WASH)-related diseases in response to latrine improvement. Overall, there was a mean decrease of 60% in diarrhea risk, 42% for schistosomiasis risk, and 65% for STH risk compared to no intervention. Diarrhea caused a substantial disease burden in China, especially in rural areas and west China, where sanitation conditions are relatively poor. However, a significant decrease in the prevalence of diarrheal disease since the founding of the People’s Republic of China was observed, which was a result of the implementation of many public and nonpublic health measures, including providing clean water supplies and improving latrines and sanitation in rural and poor areas (Cui et al., 2018; Lu, 2019; Cheng et al., 2022). STH was once a major parasitic disease that endangered the health of a large portion of the rural population in China. However, data collected during three national surveys revealed that the infection rate of STH decreased from 53.21% in the first survey (1988–1992) to 3.38% in the third survey (2014–2016). Intervention measures to control STH transmission in the population consisted of four improvement measures and one deworming event (drinking water improvement, latrine improvement, sanitation improvement, health behavior improvement, and mass deworming). In rural China, where there is a tradition of using compost to improve soil fertility, improved latrines have greatly reduced the risk of transmission of STH through the use of compost. Great achievements have also been made in the control of schistosomiasis in China, as indicated by the number of infected people decreasing from 9.49 million in 1957 to 30,000 in 2018 (Lv et al., 2019). Access to and the use of improved latrines will catch most Schistosoma eggs and will prevent miracidia from infecting intermediate host snails. This study confirmed that improvements in latrine facilities were associated with decreased likelihood of infection with schistosomiasis in China.
The most effective way of combatting diarrhea, STH, and schistosomiasis is improving access to water, sanitation, and hygiene. Moreover, WASH interventions are often not a single measure but multiple measures that are implemented at the same time. Therefore, this study evaluated the reduced risk of a disease associated with improved latrine facilities in combination with other improvements. In China, local governments coordinated health, agriculture, water, forestry, land, and other government resources to implement comprehensive measures for the prevention and control of WASH diseases, especially schistosomiasis (Yang et al., 2016). Our study revealed that the combination of various control and prevention measures had similar effects. The combination of these measures might be related to a specific local situation. Therefore, intervention study designers may develop personalized intervention strategies for specific public health problems in individual study areas.
Unlike previous systematic reviews, this study also focused on the relationship between increases in latrine coverage and RR value. Increasing sanitary latrine coverage was negatively correlated with RR, indicating that higher sanitary latrine coverage in a population results in a decreased likelihood of WASH-related diseases. This review provides more evidence linking latrine and sanitation interventions to human health. The results also indicate that latrine or sanitation improvement should not be based on individual household but should instead be promoted at the community level with the goal of improving the coverage of the entire population. Sanitary latrine coverage in rural China had reached more than 70.0% by 2022 (MARA, 2022). This rapid increase in coverage is due to a large amount of investment from local governments, as well as extensive social mobilization known as the latrine revolution.
It should be noted that this analysis may not have covered all WASH-related diseases. Moreover, the limited number of included diarrheal diseases and STH studies may affect the accuracy of the estimate of pooled effects.
5 Conclusion
This article provides evidence of the correlation between latrine improvement and reduced incidence of related diseases in rural China. The results of this study confirmed that latrine improvement in China played an important role in the prevention of many key infectious diseases. The overall estimates showed a mean reduction of 60% for diarrhea risk, 42% for schistosomiasis risk, and 65% for STH risk compared to no intervention.
Our research also confirmed that the intensity of health effects was positively correlated with the intensity of sanitation interventions (coverage of sanitary latrines) in China. The results presented herein suggest the important role of promoting access to sanitary latrines in disease prevention and control in China.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
SS managed data extraction and data cleaning, conducted the statistical analyses, created the tables and figures, and wrote the first draft of the manuscript. HL provided guidance on the study design and contributed to results interpretation and the final manuscript. SS, LW, WY, and LL conducted the search screening, full-text identification, review, and data extraction. RZ contributed to drafts and helped in writing the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fenvs.2022.914751/full#supplementary-material.
References
Al-Mekhlafi, H. M. (2020). The Neglected Cestode Infection: Epidemiology of Hymenolepis Nana Infection Among Children in Rural Yemen. Helminthologia 57 (4), 293–305. doi:10.2478/helm-2020-0038
Als, D., Meteke, S., Stefopulos, M., Gaffey, M. F., Kamali, M., Munyuzangabo, M., et al. (2020). Delivering Water, Sanitation and Hygiene Interventions to Women and Children in Conflict Settings: a Systematic Review. BMJ Glob. Health 5 (Suppl. 1), e002064. doi:10.1136/bmjgh-2019-002064
Asaolu, S. O., Ofoezie, I. E., Odumuyiwa, P. A., and Ogunniyi, T. A. B. (2002). Effect of Water Supply and Sanitation on the Prevalence and Intensity of Ascaris lumbricoides Among Pre-school-age Children in Ajebandele and Ifewara, Osun State, Nigeria. Trans. R. Soc. Trop. Med. Hyg. 96 (6), 600–604. doi:10.1016/S0035-9203(02)90323-8
Banke, R. O., Omudu, E. A., Ikenwa, D. A., and Feese, E. J. (2006). Prevalence of Gastro-Intestinal Parasites in Relation to Availability of Sanitary Facilities Among Schooling Children in Makurdi, Nigeria. Anim. Res. Int. 3 (2), 489–493. doi:10.4314/ari.v3i2.40777
Chen, M., Zhang, H., Hu, H., Liu, X., Liu, J., Zhang, X., et al. (2015). Analysis on the Measures and Effect Ofschistosomiasis Control at Pilot County Collaborated by Provinces and Ministry in Jiangling County,Hubei Province (2009-2013). J. Public Health. Prev. Med. 26 (01), 39–42.
Chen, T., and Kallawicha, K. (2021). Association between Sanitary Toilet Coverage Rate and Intestinal Infectious Disease in Jiangsu Province, China. Sci. Rep. 11 (1), 12805. doi:10.1038/s41598-021-92291-z
Cheng, S., Li, Z., Uddin, S. M. N., Mang, H.-P., Zhou, X., Zhang, J., et al. (2018). Toilet Revolution in China. J. Environ. Manag. 216, 347–356. doi:10.1016/j.jenvman.2017.09.043
Cheng, S., Long, J., Evans, B., Zhan, Z., Li, T., Chen, C., et al. (2022). Non-negligible Greenhouse Gas Emissions from Non-sewered Sanitation Systems: A Meta-Analysis. Environ. Res. 212, 113468. doi:10.1016/j.envres.2022.113468
Clasen, T. F., Bostoen, K., Schmidt, W.-P., Boisson, S., Fung, I. C.-H., Jenkins, M. W., et al. (2010). Interventions to Improve Disposal of Human Excreta for Preventing Diarrhoea. Cochrane. Database. Syst. Rev. 6 (6), CD007180. doi:10.1002/14651858.CD007180.pub2
Coory, M. D. (2010). Comment on: Heterogeneity in Meta-Analysis Should Be Expected and Appropriately Quantified. Int. J. Epidemiol. 39 (3), 932. doi:10.1093/ije/dyp157
Cui, P., Li, J., Liu, N., and Duan, Z.-j. (2018). Incidence of Acute Diarrheal Illness in Chinese Communities: a Meta-Analysis. BMC Gastroenterol. 18 (1), 114. doi:10.1186/s12876-018-0839-2
Darmstadt, G. L., Pepper, K. T., Ward, V. C., Srikantiah, S., Mahapatra, T., Tarigopula, U. K., et al. (2020). Improving Primary Health Care Delivery in Bihar, India: Learning from Piloting and Statewide Scale-Up of Ananya. J. Glob. Health. 10 (2), 021001. doi:10.7189/jogh.10.02100110.7189/jogh.10.0201001
Deng, Y., Qiang, G., Cai, Z., Li, X., and Zhang, Y. (2012). Effect of the Comprehensive Control Measures with Emphasis on Infection Source for Schistosomiasis in Inland Water Network Areas. J. Trop. Dis. Parasitol. 10 (01), 5–7. doi:10.3969/j.issn.1672-2302.2012.01.002
Deng, Y., Qiang, G., You, P., Ren, J., Zhao, J., and Yang, X. (2009). Effect on Schistosomiasis Control by Comprehensive Measuers with Enphasis on Infection Source Control. J. Trop. Dis. Parasitol. 7 (02), 89–90. doi:10.3969/j.issn.1672-2302.2009.02.010
Deshpande, A., Miller-Petrie, M. K., Lindstedt, P. A., Baumann, M. M., Johnson, K. B., Blacker, B. F., et al. (2020). Mapping Geographical Inequalities in Access to Drinking Water and Sanitation Facilities in Low-Income and Middle-Income Countries, 2000-17. Lancet Glob. Health. 8 (9), e1162–e1185. doi:10.1016/S2214-109X(20)30278-3
Dong, B., Zou, Z., Song, Y., Hu, P., Luo, D., Wen, B., et al. (2020). Adolescent Health and Healthy China 2030: a Review. J. Adolesc. Health 67 (5), S24–S31. doi:10.1016/j.jadohealth.2020.07.023
Du, P., Sun, B., Pan, L. J., Cheng, Y. B., Li, T. T., Wang, X. L., et al. (2019). Achievements and Prospects on Environmental Health and Sanitary Engineering in China. Zhonghua Yu Fang. Yi Xue Za Zhi 53 (9), 865–870. doi:10.3760/cma.j.issn.0253-9624.2019.09.001
Esrey, S. A. (1996). Water, Waste, and Well-Being: a Multicountry Study. Am. J. Epidemiol. 143 (6), 608–623. doi:10.1093/oxfordjournals.aje.a008791
Feng, Y., Guo, Y., Yang, G., Qin, X., and Song, Z. (2012). Household Biogas Development in Rural China: On Policy Support and Other Macro Sustainable Conditions. Renew. Sustain. Energy Rev. 16 (8), 5617–5624. doi:10.1016/j.rser.2012.06.019
Fewtrell, L., and Bartram, J. (2001). Water Quality: Guidelines, Standards and Health. London: IWA Publishing.
Fewtrell, L., Kaufmann, R. B., Kay, D., Enanoria, W., Haller, L., and Colford, J. M. (2005). Water, Sanitation, and Hygiene Interventions to Reduce Diarrhoea in Less Developed Countries: a Systematic Review and Meta-Analysis. Lancet Infect. Dis. 5 (1), 42–52. doi:10.1016/s1473-3099(04)01253-8
GBD (2018). Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Diarrhoea in 195 Countries: a Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 18 (11), 1211–1228. doi:10.1016/S1473-3099(18)30310-410.1016/S1473-3099(18)30362-1
Hannah, R., and Max, R. (2021). Clean Water and Sanitation. Available at: ourworldindata.org/clean-water-sanitation. (Accessed: 3 May 2022).
He, J., Zhang, S., Wang, T., Wu, H., Bao, J., Wang, Y., et al. (2011). Study on the Effectiveness of Schistosomiasis Control via Integrated Measure Emphasizing Infection Source Control. J. Pathog. Biol. 6 (10), 744–747+738. doi:10.13350/j.cjpb.2011.10.020
Higgins, J. P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2019). in Cochrane Handbook for Systematic Reviews of Interventions. Editor (Chichester (UK): John Wiley & Sons).
Li, Y., Cheng, S., Cui, J., Gao, M., Li, Z., Wang, L., et al. (2022). Mining of the Association Rules between Socio-Economic Development Indicators and Rural Harmless Sanitary Toilet Penetration Rate to Inform Sanitation Improvement in China. Front. Environ. Sci. 10, 817655. doi:10.3389/fenvs.2022.817655
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., et al. (2009). The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies that Evaluate Health Care Interventions: Explanation and Elaboration. J. Clin. Epidemiol. 62 (10), e1–e34. doi:10.1016/j.jclinepi.2009.06.006
Lin, L., Wei, Y., Yao, W., Li, H., Liu, D., and Zhang, R. (2020). Improving Sanitary Latrines in Rural Areas Correlated to Decreasing the Related Disease Burden - China, 2006−2017. Chin. CDC Wkly. 2 (46), 873–876. doi:10.46234/ccdcw2020.238
Liu, J. L. (2011). The Role of the Funnel Plot in Detecting Publication and Related Biases in Meta-Analysis. Evid. Based Dent. 12 (4), 121–122. doi:10.1038/sj.ebd.6400831
Lu, X. (2019). Changes of Village Appearance and Village Planning in China in the Past 70 Years. Chin. Dev. Obs. 22 (3), 36–38. doi:10.12140/j.issn.1000-7423.2019.05.002
Luby, S. P., Rahman, M., Arnold, B. F., Unicomb, L., Ashraf, S., Winch, P. J., et al. (2018). Effects of Water Quality, Sanitation, Handwashing, and Nutritional Interventions on Diarrhoea and Child Growth in Rural Bangladesh: a Cluster Randomised Controlled Trial. Lancet Glob. Health 6 (3), e302–e315. doi:10.1016/S2214-109X(18)30005-610.1016/s2214-109x(17)30490-4
Lv, S., Xv, J., Cao, C., Zhang, L., Li, S., and Zhou, X. (2019). China Fighting against Schistosomiasis for 70 Years: Progress and Experience. Chin. J. Parasitol. Parasit. Dis. 37 (05), 514–519. doi:10.12140/j.issn.1000-7423.2019.05.002
MARA. (2022). The Rural Centralized Water Supply Rate and Tap Water Penetration Rate Reached 89% and 84% Respectively, and the Living Environment Sanitation of Farmers Was Significantly Improved. Available at: www.moa.gov.cn/ztzl/ymksn/rmrbbd/202204/t20220415_6396443.htm. (Accessed: 12 May 2022)
Massad, E., Ortega, N. R. S., de Barros, L. C., and Struchiner, C. J. (2009). Fuzzy Logic in Action: Applications in Epidemiology and beyond. Berlin: Springer Science & Business Media.
Melnikow, J., Lefevre, M., Wilt, T. J., and Moyer, V. A. (2013). Counterpoint. Med. Care. 51 (4), 301–303. doi:10.1097/MLR.0b013e31828a67d3
Morse, T., Tilley, E., Chidziwisano, K., Malolo, R., and Musaya, J. (2020). Health Outcomes of an Integrated Behaviour-Centred Water, Sanitation, Hygiene and Food Safety Intervention-A Randomised before and after Trial. Ijerph 17 (8), 2648. doi:10.3390/ijerph17082648
NHFPC (2017). China Health and Family Planning Statistical Yearbook. Beijing: Peking Union Medical College Press.
Null, C., Stewart, C. P., Pickering, A. J., Dentz, H. N., Arnold, B. F., Arnold, C. D., et al. (2018). Effects of Water Quality, Sanitation, Handwashing, and Nutritional Interventions on Diarrhoea and Child Growth in Rural Kenya: a Cluster-Randomised Controlled Trial. Lancet Glob. Health 6 (3), e316–e329. doi:10.1016/S2214-109X(18)30005-6
Odagiri, M., Schriewer, A., Daniels, M. E., Wuertz, S., Smith, W. A., Clasen, T., et al. (2016). Human Fecal and Pathogen Exposure Pathways in Rural Indian Villages and the Effect of Increased Latrine Coverage. Water Res. 100, 232–244. doi:10.1016/j.watres.2016.05.015
Patel, K., Kalpana, P., Trivedi, P., Yasobant, S., and Saxena, D. (2019). Assessment of Water, Sanitation and Hygiene in HCFs: Which Tool to Follow? Rev. Environ. Health. 34 (4), 435–440. doi:10.1515/reveh-2019-0001
Pickering, A. J., and Davis, J. (2012). Freshwater Availability and Water Fetching Distance Affect Child Health in Sub-saharan Africa. Environ. Sci. Technol. 46 (4), 2391–2397. doi:10.1021/es203177v
Reese, H., Routray, P., Torondel, B., Sinharoy, S. S., Mishra, S., Freeman, M. C., et al. (2019). Assessing Longer-Term Effectiveness of a Combined Household-Level Piped Water and Sanitation Intervention on Child Diarrhoea, Acute Respiratory Infection, Soil-Transmitted Helminth Infection and Nutritional Status: a Matched Cohort Study in Rural Odisha, India. Int. J. Epidemiol. 48 (6), 1757–1767. doi:10.1093/ije/dyz157
Rheinländer, T., Gyapong, M., Akpakli, D. E., and Konradsen, F. (2019). Secrets, Shame and Discipline: School Girls' Experiences of Sanitation and Menstrual Hygiene Management in a Peri-Urban Community in Ghana. Health Care Women Int. 40 (1), 13–32. doi:10.1080/07399332.2018.1444041
Schliessmann, D. J. (1959). Diarrhoeal Disease and the Environment. B. World Health Organ. 21 (3), 381. doi:10.1021/ed069p346
Schmidt, W.-P. (2014). The Elusive Effect of Water and Sanitation on the Global Burden of Disease. Trop. Med. Int. Health. 19 (5), 522–527. doi:10.1111/tmi.12286
Strunz, E. C., Addiss, D. G., Stocks, M. E., Ogden, S., Utzinger, J., and Freeman, M. C. (2014). Water, Sanitation, Hygiene, and Soil-Transmitted Helminth Infection: a Systematic Review and Meta-Analysis. PLoS Med. 11 (3), e1001620. doi:10.1371/journal.pmed.1001620
Tao, Y. (2019). Development Course from "rural Toilet Changing" to "toilet Revolution. Chin. J. Public Health Eng. 18 (04), 481–484.
Tumwine, J., Thompson, J., Katui-Katua, M., Mujwahuzi, M., Johnstone, N., and Porras, I. (2003). Sanitation and Hygiene in Urban and Rural Households in East Africa. Int. J. Environ. Health Res. 13 (2), 107–115. doi:10.1080/0960312031000098035
UN (2016). Transforming Our World: The 2030 Agenda for Sustainable Development. Available at: https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf (Accessed May 3, 2022).
UNICEF (2018). Core Questions on Drinking Water, Sanitation and Hygiene for Household Surveys: 2018 Update. New York: United Nations Children’s Fund (UNICEF) and World Health Organization.
Wagner, E. G., and Lanoix, J. N. (1958). Excreta Disposal for Rural Areas and Small Communities. Geneva: World Health Organization.
WHO (2021). Drinking-water. Available at: www.who.int/news-room/fact-sheets/detail/drinking-water (Accessed May 3, 2022).
WHO/UNIFC. (2021). Progress on Household Drinking Water, Sanitation and Hygiene 2000-2020: Five Years into the SDGs. Available at: washdata.org/report/jmp-2021-wash-households.pdf (Accessed: 3 May 2022).
Wu, S., Zhang, Y., and He, B.-J. (2022). Public Willingness to Pay for and Participate in Sanitation Infrastructure Improvement in Western China's Rural Areas. Front. Public Health 9, 788922. doi:10.3389/fpubh.2021.788922
Yang, N. (2004). Disease Prevention, Social Mobilization and Spatial Politics: The Anti Germ-Warfare Incident of 1952 and the "Patriotic Health Campaign". Chin. Hist. Rev. 11 (2), 155–182. doi:10.1080/1547402X.2004.11827202
Yang, Y., Zhou, Y.-B., Song, X.-X., Li, S.-Z., Zhong, B., Wang, T.-P., et al. (2016). Integrated Control Strategy of Schistosomiasis in the People's Republic of China. Adv. Parasit. 92, 237–268. doi:10.1016/bs.apar.2016.02.004
Young, S. L., Goodman, D., Farag, T. H., Ali, S. M., Khatib, M. R., Khalfan, S. S., et al. (2007). Geophagia Is Not Associated with Trichuris or Hookworm Transmission in Zanzibar, Tanzania. Trans. R. Soc. Trop. Med. Hyg. 101 (8), 766–772. doi:10.1016/j.trstmh.2007.04.016
Zhang, Q., Chen, Y., Xv, L., Zheng, C., and Li, H. (2011). Effect of Control on Infections of Soil-Transmitted Helminthes in Demonstration Plots of China for 3 Years. Chin. J. Schistosomiasis Control 23 (05), 476–482. doi:10.16250/j.32.1374.2011.05.018
Keywords: latrine improvement, schistosomiasis, diarrheal, soil-transmitted helminth, meta-analysis
Citation: Shang S, Li H, Wang L, Yao W, Lin L and Zhang R (2022) Health Benefits of Improved Latrine in Rural China. Front. Environ. Sci. 10:914751. doi: 10.3389/fenvs.2022.914751
Received: 07 April 2022; Accepted: 01 June 2022;
Published: 15 August 2022.
Edited by:
Shikun Cheng, University of Science and Technology Beijing, ChinaReviewed by:
Yuming Sun, Institute of Botany (CAS), ChinaNeelam Rana, Indian Institute of Technology Bombay, India
Copyright © 2022 Shang, Li, Wang, Yao, Lin and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hongxing Li, bGloeEBuY3J3c3RnLmNoaW5hY2RjLmNu; Rong Zhang, emhhbmdyb25nQGNoaW5hY2RjLmNu