 Saad M. AlRabeeah1†
Saad M. AlRabeeah1† Eidan M. Alzahrani2†
Eidan M. Alzahrani2† Abdulelah M. Aldhahir3
Abdulelah M. Aldhahir3 Rayan A. Siraj4
Rayan A. Siraj4 Abdullah A. Alqarni5Ibrahim A. AlDraiwiesh1
Abdullah A. Alqarni5Ibrahim A. AlDraiwiesh1 Abdullah S. Alqahtani1Badr S. Almqati1Turki G. Alharbi1Abdulraheem A. Almuntashiri1Saeed M. Alghamdi6Fahad E. Aljohani7Mohammed A. Almulhim8Ali F. Alshehri9
Abdullah S. Alqahtani1Badr S. Almqati1Turki G. Alharbi1Abdulraheem A. Almuntashiri1Saeed M. Alghamdi6Fahad E. Aljohani7Mohammed A. Almulhim8Ali F. Alshehri9 Abdallah Y. Naser10
Abdallah Y. Naser10 Hassan Alwafi11Nowaf Y. Alobaidi12,13Ahmed M. Hjazi14Mujahid A. Alsulaimani15
Hassan Alwafi11Nowaf Y. Alobaidi12,13Ahmed M. Hjazi14Mujahid A. Alsulaimani15 Tope Oyelade16
Tope Oyelade16 Mushabbab Alahmari17
Mushabbab Alahmari17 Turki M. Alanazi12,13Mohammed A. Almeshari18,19
Turki M. Alanazi12,13Mohammed A. Almeshari18,19 Jaber S. Alqahtani1*
Jaber S. Alqahtani1*- 1Department of Respiratory Care, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia
- 2Department of Physical Therapy, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia
- 3Respiratory Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia
- 4Respiratory Therapy Department, King Faisal University, Al-Ahsa, Saudi Arabia
- 5Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia
- 6Respiratory Care Program, College of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia
- 7Pediatric Department, Khobar Governmental Hospital, Khobar, Saudi Arabia
- 8Anesthesia Section, Security Forces Hospital Dammam, Dammam, Saudi Arabia
- 9Preventive Medicine Department, Khobar Primary Health Care Centers, Khobar, Saudi Arabia
- 10Department of Applied Pharmaceutical Sciences and Clinical Pharmacy, Faculty of Pharmacy, Isra University, Amman, Jordan
- 11Faculty of Medicine, Umm Al Qura University, Mecca, Saudi Arabia
- 12Respiratory Therapy Department, King Saud bin Abdulaziz University for Health Sciences, Alahsa, Saudi Arabia
- 13King Abdullah International Medical Research Center, Alahsa, Saudi Arabia
- 14Department of Medical Laboratory Sciences, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia
- 15Basic Medical Unit, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia
- 16University College London (UCL) Division of Medicine, London, United Kingdom
- 17Department of Respiratory Therapy, University of Bisha, Bisha, Saudi Arabia
- 18Rehabilitation Health Sciences Department, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
- 19Institute of Inflammation and Ageing, University of Birmingham, Birmingham, United Kingdom
Background: Lung cancer is currently the most fatal form of cancer worldwide, ranking as the fourth most prevalent type in Saudi Arabia, particularly among males. This trend is expected to increase with growing population, lifestyle changes, and aging population. Understanding the awareness of the Saudi population regarding the risk factors and symptoms of lung cancer is necessary to attenuate the predicted increase in cases.
Method: A cross-sectional, population-based survey was performed using a previously validated questionnaire (Lung CAM). Multiple linear regression analysis was used to assess variables associated with deficiency in knowledge and awareness of risk factors and symptoms of lung cancer.
Results: Majority of the 15,099 respondents were male (65%), aged between 18 and 30 years (53%), 50% of which were educated up to a bachelor’s degree level. Overall awareness of lung cancer signs and symptoms was 53%, with painful cough and coughing up blood being the best-known symptoms. Conversely, persistent shoulder pain (44%) and clubbing fingers (47%) were the least known lung cancer symptoms. Also, 60% of the respondents showed low confidence in identifying the signs and symptoms of lung cancer. The overall awareness of the risk factors for lung cancer development was 74%, with first-hand (74%) and second-hand (68%) smoking being the most known risk factors. However, only ≤ 62% know the other non-smoking risk factors. Awareness of the risk factors and symptoms of lung cancer depended on age, gender, education, marital and employment status (p < 0.001).
Conclusion: Public awareness of the risk factors and symptoms of lung cancer in Saudi Arabia is inadequate and heavily dependent on education and socio-economic status. Awareness can be improved through campaigns to raise awareness about other lesser-known lung cancer risk factors and symptoms.
Introduction
Lung cancer is the most commonly diagnosed cancer worldwide (1). In 2020, the number of new cases of lung cancer worldwide was estimated to be around 2.21 million (2). Additionally, there were approximately 1.8 million deaths attributed to this disease with around two-third of the global burden attributed to males (1–3). In Saudi Arabia, lung cancer in 2018 was ranked as the fifth most prevalent cancer among males and 12th among females (4). Unfortunately, it is anticipated that the incidence rate will rise as a result of population growth, including a projected seven-fold increase in the older adult population due to increased tobacco smoking in the Saudi population (5–8). Furthermore, in Saudi Arabia, there were 504 reported lung cancer cases in 2018, accounting for 3.2% of all newly diagnosed cases among Saudis (9). Accordingly, the death rate of lung cancer in Saudi Arabia from 2009 to 2012 was 52.75% (10).
Modifiable risk factors, such as cigarette smoking, lack of physical exercise, obesity, as well as exposure to second-hand smoke, minerals, metal particles, radon, and asbestos contributes to more than half of cancer cases, including lung cancer (4, 11). Specifically, tobacco use is one of these modifiable risk factors, accounting for 80%–90% of all cases of lung cancer (12). Thus, it is crucial to have an in-depth knowledge of risk factors if the projected trend is to be attenuated. Importantly, smoking cessation has been shown by several community-based studies to substantially reduce the risk of lung cancer (13, 14). Further, the implementation of annual lung cancer screening among high-risk individuals has been strongly advised by several authoritative sources (10, 15), as it has been shown to potentially reduce the death rate by up to 20% (15).
Most patients in the Middle Eastern and Northern African regions are diagnosed with lung cancer at an advanced stage (16). Specifically, early diagnosis of lung cancer in Saudi Arabia has been achieved only in 14% of all cases (1, 17) with most cases diagnosed at a later and metastatic stage (10). This may be partly due to the lack of public awareness regarding the risk factors, early signs, and prognosis of lung cancer (18). Moreover, lung cancer can be effectively treated when diagnosed early, making awareness of its early signs extremely crucial (19). Therefore, promoting community knowledge of lung cancer, including how to identify early signs and symptoms as well as risk factors, has the potential to facilitate timely detection, mitigate the incidence of new cases, and subsequently have a favorable influence on the overall trajectory and prognosis of the illness. Therefore, the present research evaluates lung cancer awareness across the Saudi community, including knowledge of the associated risk factors and symptoms.
Methods
Study design and study population
This cross-sectional study aimed to evaluate the level of public knowledge and awareness of the symptoms and risk factors associated with lung cancer in Saudi Arabia. The data was collected between January 2023 and July 2023. The recruitment of participants for this study was conducted using convenience sampling method, with careful consideration of their suitability, and population distribution across the five major regions of the kingdom. Before answering the questionnaire, all participants willingly and voluntarily provided their informed consent. The purpose and goals of this study were explicitly described prior to the commencement of the survey. The inclusion criteria include being an adult individual (aged ≥ 18 years) of Saudi Arabian nationality currently residing in Saudi Arabia.
The Prince Sultan Military College of Health Sciences Institutional Review Board (IRB) approved this study (IRB-2023-RC-003). Confidential data were de-identified and removed before processing. The study followed the guidelines of the Declaration of Helsinki.
Survey tool and distribution
We used a validated lung cancer awareness measure (17), derived from a pre-existing generic cancer awareness model. The survey instrument comprised four main sections (see Supplementary File). The first section collects participants’ demographic information. The second section obtains responses regarding the signs and symptoms of lung cancer. The third section asks questions about the various risk factors for lung cancer. The fourth section gauges the respondents’ level of confidence in their ability to recognize symptoms of lung cancer. The Arabic language is the official language and the predominant means of communication for most individuals residing in Saudi Arabia. Thereby, while the survey was initially designed in English language, it was subsequently forwarded to the Professional Translation Unit of Prince Sultan Military College of Health Sciences for translation into Arabic. A proficient translator specialized in the Arabic language undertook the task of retranslating the responses back into English. The translation unit used the forward–backward translation method, as recommended by the World Health Organization, to assess the two English versions (20). A subsequent pilot study was conducted on the Arabic version, in which a sample of 10 individuals from the general population was randomly recruited. The purpose of this pilot study was to evaluate the readability and suitability of the questionnaire items (21). A cut-off of ≥70% for responses was chosen in advance as an indicator of good awareness, while awareness level below 70% was deemed to be poor. The survey used a multi-channel methodology to effectively engage participants, encompassing online platforms, such as social media and WhatsApp groups, and offline distribution in public venues, such as shopping centers, cafes, and restaurants. This approach was specifically designed to ensure inclusivity by targeting individuals who could be at risk of digital exclusion.
Power calculation
To obtain the minimum sample size, we considered a confidence interval of 98%, a margin of error of 1%, and the adult population of Saudi Arabia in 2023 of approximately 27.58 million. We also assumed a response distribution of 50%. Thus, the minimum sample size required for this study to be widely generalized was 13,523 respondents.
Statistical analysis
To clearly represent the characteristics of the participants, a comprehensive descriptive analysis was conducted. Normality was assessed using Kolmogorov–Smirnov test. If normally distributed (parametric), data were presented as mean and SD; otherwise, median and inter-quartile range (IQR) were used. The comparisons among the various groups were evaluated using the chi-square and Fisher’s exact tests. Pearson’s correlation coefficient measure was used to examine the correlation between lung cancer risk and symptom awareness and the participants’ confidence level. Multiple linear regression analysis was used to assess variables associated with a deficiency in knowledge and awareness of lung cancer. The co-variates included in the multiple linear models were age, gender, religion, marital status, education and job status and smoking. This was done using the total score of the lung awareness measure scale for recognizing signs and symptoms and the total score of the Likert scale concerning the awareness of risk factors as dependent variables in this model. The data analysis was performed using SPSS Statistics 28 (IBM Corp., Armonk, NY), with statistical significance set to p-values less than 0.05.
Results
Demographic data
A total of 15,099 participants completed the survey. More than half of the responders were male (66%), aged 18–30 years old (52.5%), and had a bachelor’s degree (52%). The distribution of participants across the different provinces is as follows – eastern region: 2,702 (17.9%), western region: 3,188 (21.1%), central region: 3,200 (21.2%), northern region: 2,140 (14.2%), and southern region: 3,869 (25.6%). Nearly half of those who completed the survey were employed (46.3%). Most of the participants did not have cancer (98%), and neither did their partners (99%), close family members (96%), other family members (92%), or friends (97%). Among the respondents, 88% were non-smokers, 9% were current smokers, with a mean of 13.75 packs per year, and 3.5% had a smoking history (Table 1). Females accounted for 239 (18%) of the 1,317 current smokers.
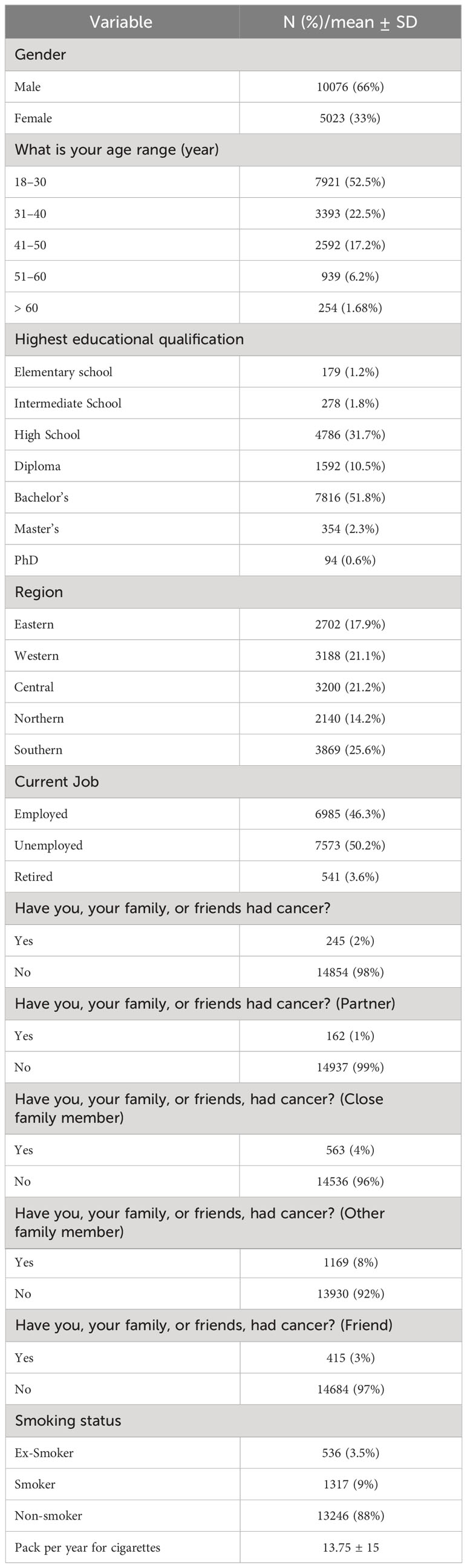
Table 1 Demographic data and characteristics of the respondents (n = 15,099).
Knowledge, awareness, and confidence in recognizing lung cancer signs and symptoms
The overall level of knowledge and awareness of lung cancer signs and symptoms was 53%, which suggests poor public awareness. The least recognizable signs and symptoms were persistent shoulder pain (44%) and changes in the shape of the fingers (47%), whereas the most obvious signs were coughing up blood (65%) and painful cough (59%). Among the main lung cancer signs and symptoms, persistent cough was recognized by 55%, persistent shortness of breath by 51.5%, unexplained weight loss by 55.4%, persistent tiredness by 57%, and loss of appetite by 53% (Table 2). In addition, 60% of the respondents showed low confidence in identifying signs and symptoms of lung cancer (Figure 1).
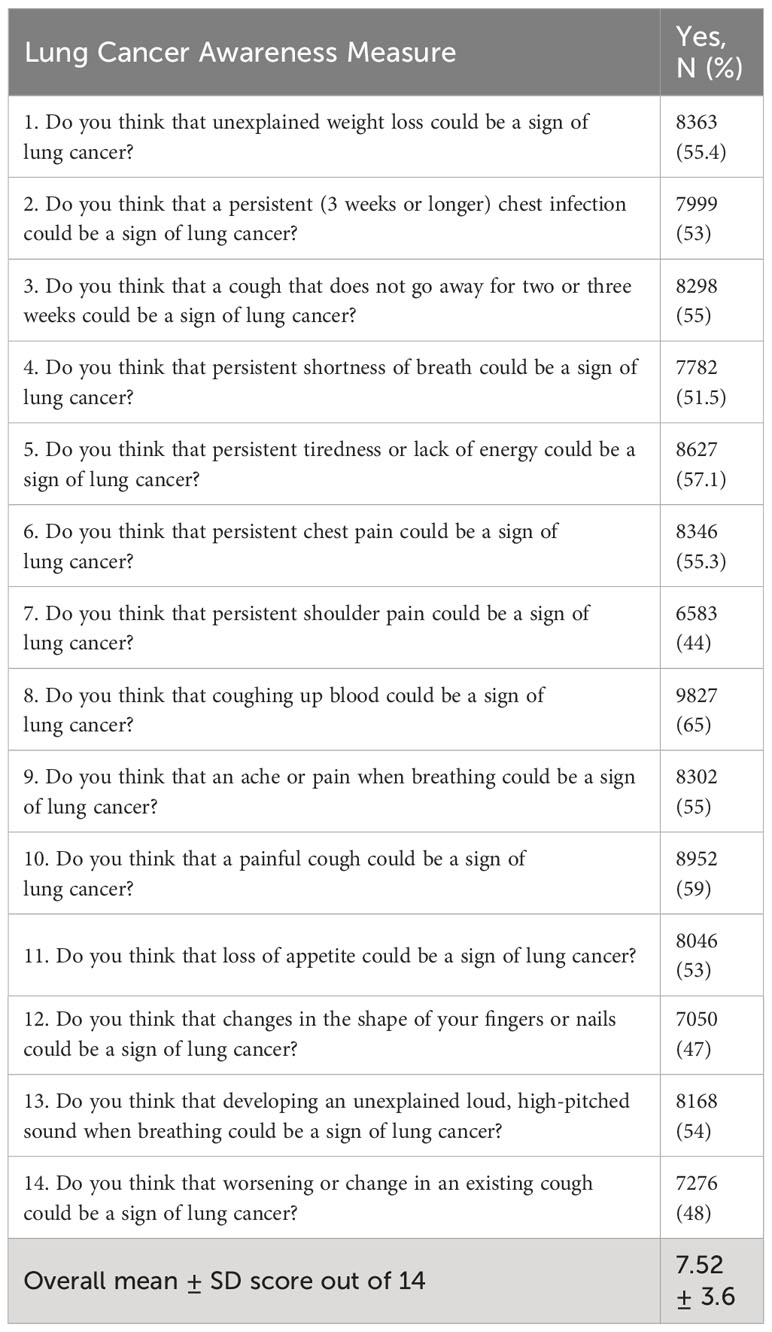
Table 2 Knowledge and awareness of recognizing lung cancer signs and symptoms (n = 15,099).
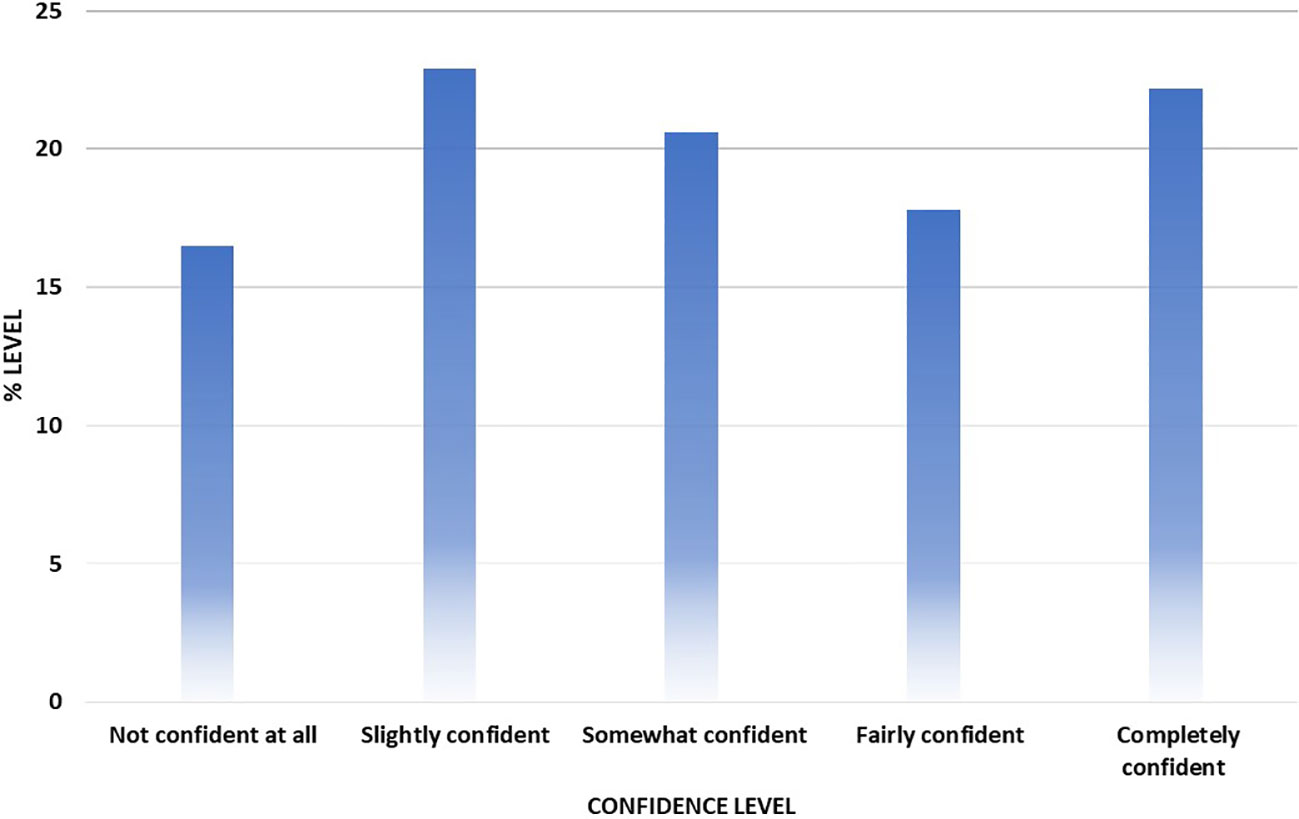
Figure 1 Confidence level of participants in noticing symptoms of lung cancer.
Awareness of risk factors for developing lung cancer
Table 3 shows the awareness of the various risk factors for lung cancer among the respondents. The overall awareness level for recognizing the risk factors for lung cancer was 74%. The proportion of agreement is as follows: smoking (74%) and second-hand smoking (68%), exposure to air pollution (62%) and radon gas and chemicals (58%), having a medical history of chronic obstructive pulmonary disease (COPD) (56%), previously diagnosis with cancer (55%), having family history of lung cancer (54%), and having had treatment for any cancer in the past (49%).
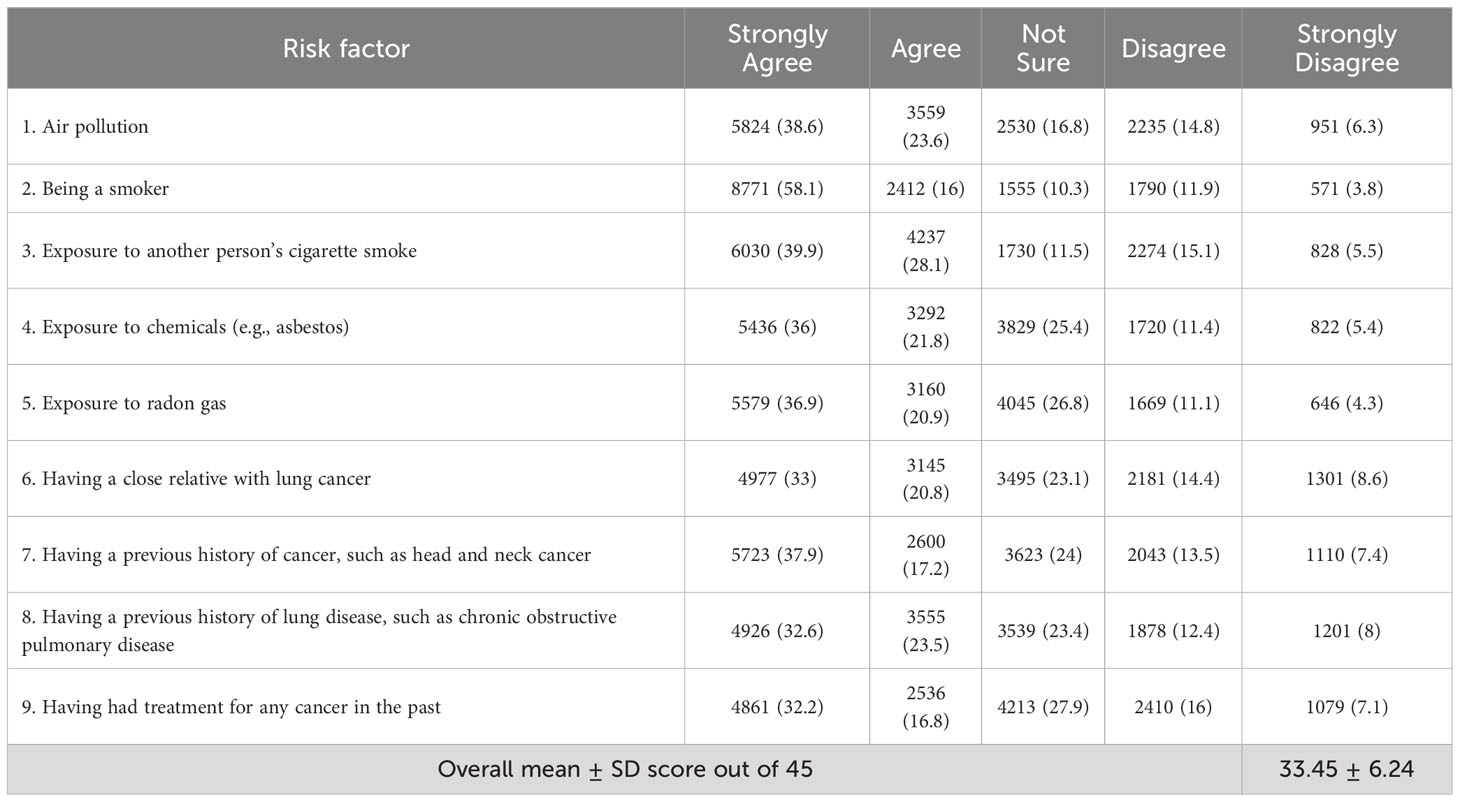
Table 3 Awareness of the risk factors for developing lung cancer (n = 15,099).
Determinants of lung cancer risk factors and signs/symptoms awareness
Table 4 shows the associations between knowledge and awareness of lung cancer signs/symptoms and demographics. Being 18–30 years of age, male, living in the central and southern regions, married, employed, or having a bachelor’s degree were significantly associated with higher knowledge of the signs/symptoms of lung cancer (p < 0.001). Similarly, awareness of the risk factors of lung cancer was significantly associated with age group, gender, marital status, educational status, and smoking status (p < 0.001) (Table 5).
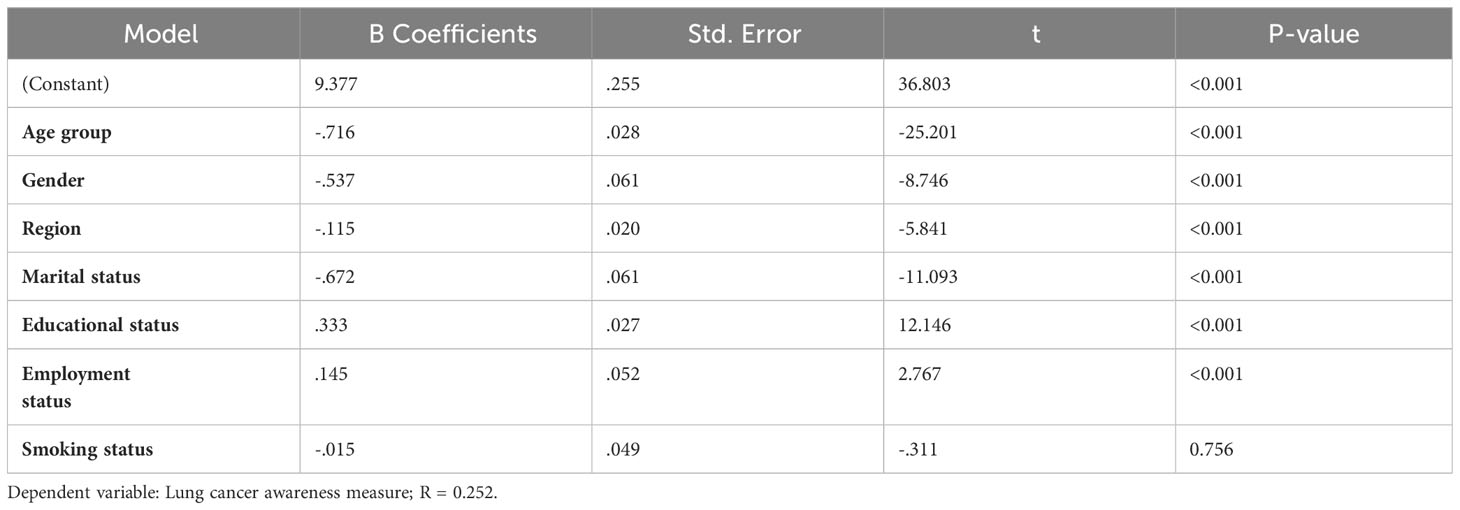
Table 4 Linear regression between lung cancer awareness measures and demography.
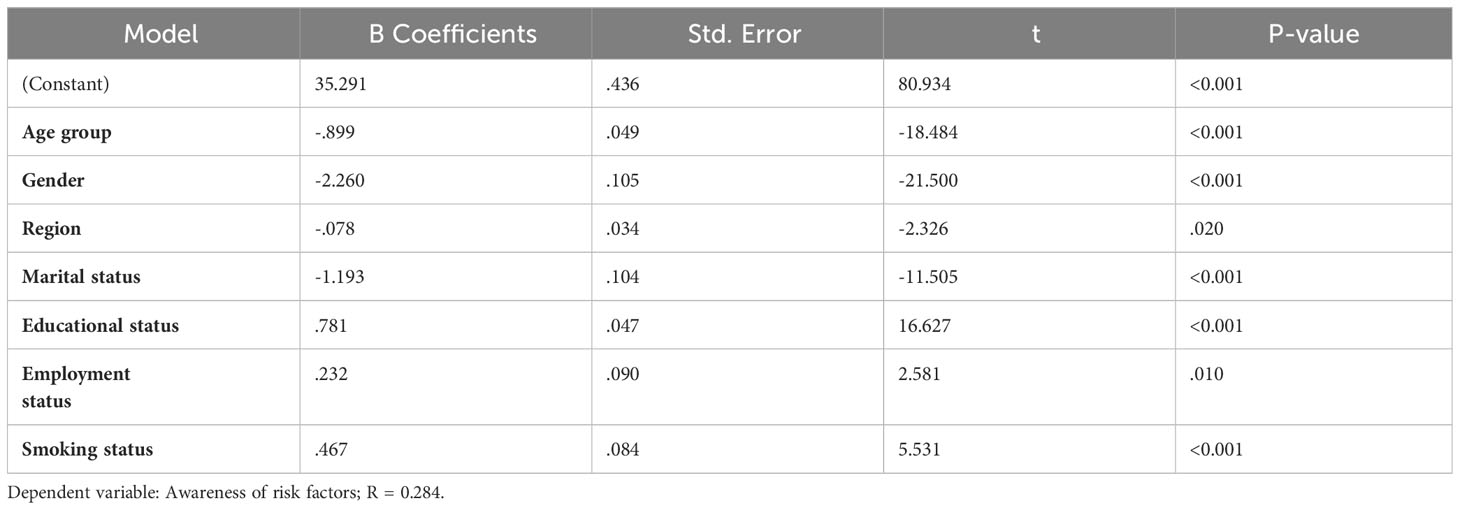
Table 5 Linear regression between risk factors awareness and demography.
Correlation between lung cancer risk and symptom awareness and participants’ confidence level
Table 6 shows the significant positive correlation between the lung cancer awareness measure, awareness of risk factors, and level of confidence in recognizing the symptoms of lung cancer. Respondents with greater awareness of the signs and symptoms of lung cancer concurrently had better awareness of the risk factors as well as higher confidence in identifying the symptoms of lung cancer. Figure 2 shows a statistically significant negative correlation between pack per year and lung cancer awareness of risk factors (R = −.058, p-value = 0.035).
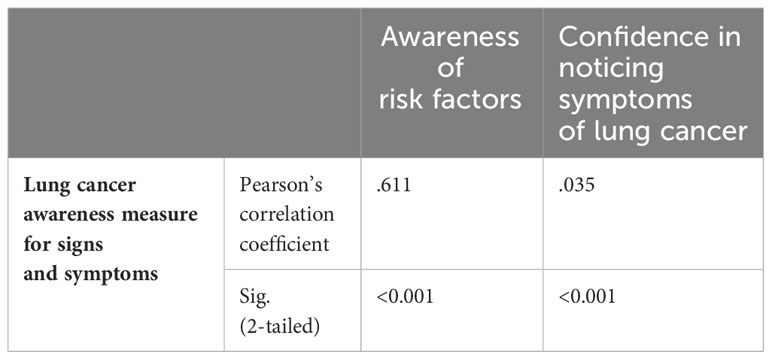
Table 6 Correlation between lung cancer risk and symptom awareness and the participants’ confidence level (n = 15,099).
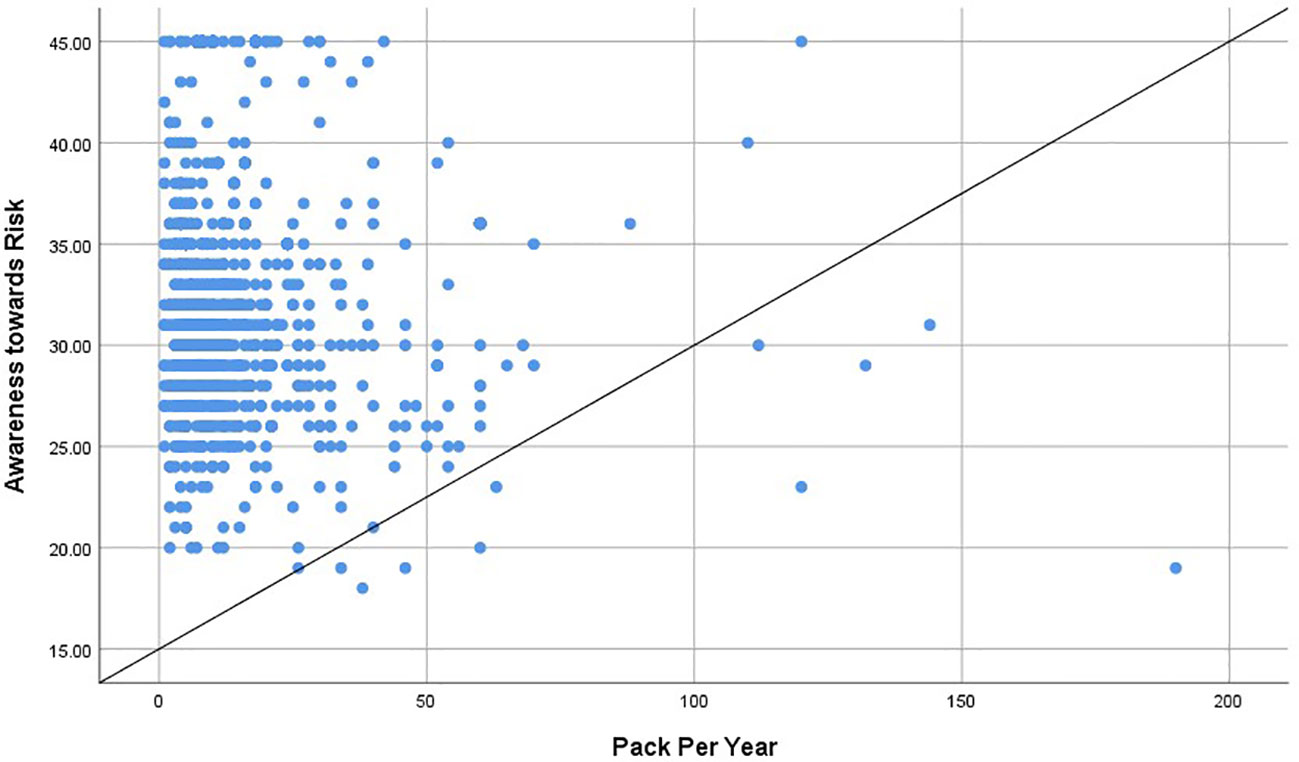
Figure 2 Correlation between pack per year and lung cancer awareness of risk factors (R = -.058, p-value = 0.035).
Discussion
In this first-of-its-kind national survey of over 15,000 participants, we assessed the public’s awareness of the risk factors and symptoms of lung cancer in the Kingdom of Saudi Arabia. Our main results show that, while more than half of the respondents recognized the main symptoms of lung cancer, such as persistent cough, shortness of breath, coughing up blood, and unexplained weight loss, they were less familiar with other symptoms such as persistent shoulder pain and finger clubbing, with around two-thirds admitting their lack of certainty (confidence) in making an association between the symptoms and lung cancer.
The finding that some of these symptoms of lung cancer are less recognized by our study population is similar to a previous report in Ireland in which morphological changes to the fingers and persistent shoulder pain were symptoms that the populace were least likely to associate with lung cancer (22). In a similar population survey performed in the United Kingdom, it was reported that only approximately 30% and 20% of the sampled population recognized persistent shoulder pain and clubbing fingers, respectively, as signs of potential lung cancer (17). This is interesting as most lung cancer patients often present to the clinic with advanced stages of the disease, usually when curative treatment is no longer applicable (23). In other studies from a neighboring country, Palestine, authors have also reported suboptimal levels of knowledge regarding symptoms of lung cancer among general population (24, 25). In a study of Saudi patients with lung cancer, the stage at diagnosis was emphasized as the single most important predictor of mortality in patients (10). This further validates how early detection through timely identification of symptoms is essential for better clinical management and prognosis of lung cancer. Indeed, the survival rate of various cancers has been shown to increase with the application of population-based screening techniques and early detection (26).
In terms of the risk factors for the development of lung cancer, most respondents showed a good level of awareness, with over 70% agreeing that smoking is a significantly increases the risk of the disease. Only 9% of the respondents in our sample were smokers, which is less than the 14% described by Qattan et al. research (27). This difference can be explained by the fact that our study had 15,099 subjects, while their study only had 8813. Indeed, more population-level education is needed to reduce or avoid the health and non-health impacts of smoking (28). Exposure to pollution, radon gas, and chemicals, as well as being diagnosed previously with COPD or other cancer types, and familial history were recognized by more than 50% of the respondents as risk factors. However, less than 50% were aware that relapse from any previously treated cancer type is a risk factor for lung cancer. This finding corroborates previous studies that found that smoking remains the most popularly known risk factor for lung cancer, with a relatively lower awareness of other risk factors (17). Our finding also supports Palestinian research that indicated smoking-related lung cancer risk factors were more generally recognized than non-smoke-related factors (25). There has also been discussions about the need to improve the awareness of non-smoking-related cancer risk factors in the general population, as most people already associate smoking with cancer. For example, Redeker et al. showed a similarly low awareness of risk factors for cancer that are not smoking-related, thereby suggesting a change in campaign focus (29). A substantial proportion of lung cancer patients has been shown to be non-smokers, and other factors, such as exposure to radon and domestic fuel smokes, have been implicated as factors that increases the risk of the disease (30, 31).
It is interesting to observe that the limited or inadequate understanding of risk factors is not exclusive to lung cancer. A recent comprehensive study conducted on a national scale examined the general population’s awareness of the risk factors associated with COPD (32). The authors revealed a generally low awareness among the studied population (32), despite high prevalence and incidence of COPD in Saudi Arabia (33). This is especially interesting as the survey was conducted in the post-COVID-19 era, with the expectation that knowledge and awareness of the risk factors for lung diseases would generally be better than before the COVID-19 pandemic.
Furthermore, we assessed the factors associated with awareness of the risk factors for lung cancer and the ability to recognize the symptoms of the disease using a linear regression model. Our results show that sufficient knowledge or awareness of the signs and symptoms of lung cancer was significantly determined by age, gender, geographical location, marital status, level of education, and employment status. Specifically, we found that being male, young (18–30 years old), living in central or southern region, being married, employed, or educated up to bachelor’s degree level increases the possibility of being aware of lung cancer signs and symptoms. Similarly, age, gender, marital status, educational level, and smoking status were found to be strong determinants of the awareness of lung cancer risk factors. These findings corroborate previous studies regarding the factors that determine awareness of lung cancer risk factors. For example, Chawla et al. found that socio-economic status and education level determined the level of awareness of the risk factors for lung cancer in a population of Nepalese residents (34). In the same study, the authors observed that while most respondents knew smoking is a risk factor, their knowledge did not influence their intention to quit smoking. This was further substantiated by another study that found that socio-economic status determined the level of awareness of the risk factors of cancer in a sample of UK residents (29). As expected, we also found that respondents with greater awareness of the risk factors for the development of lung cancer were also more aware of the predisposing symptoms and had a higher level of confidence in identifying the symptoms.
This survey has some limitations. First, there is risk of recall and self-reporting bias inherent to surveys, which may limit the interpretations of our findings (35). Second, the survey questionnaire was mainly distributed online, but we offered Offline distribution at shopping malls, cafés, and restaurants that targeted people at high risk of being digitally. Third, we lack data about household income and the results may not be applicable to a wider population due to the use of convenience sampling. Nevertheless, the study population included randomly sampled group of over 15,000 Saudi Arabians, the largest survey of its kind, to the best of our knowledge.
In sum, there is relatively low awareness of the risk factors and symptoms of lung cancer in the general population in the Kingdom of Saudi Arabia, with socio-economic status playing an influential role in this observation. The incidence and mortality due to lung and other types of cancer in Saudi Arabia are expected to increase, mostly due to social and economic development. Thus, more people are now exposed to various risk factors of cancer, including higher caloric intake, sedentary lifestyle, and smoking (28, 36). There is indeed, need to improve public awareness to change this outlook. The recent launch of Vison 2030 in the Kingdom of Saudi Arabia (37), which relates to the transformation of healthcare in the country, means that to achieve the lofty aims of reducing the national burden of diseases, more attention will need to be paid to public awareness of the various risk factors for common diseases, including lung cancer. Specifically, other significant risk factors aside from smoking should be the main target of the public health campaign, and this combined with a targeted, age-specific, sex-specific, public health screening, could help achieve a healthier Saudi Arabia. Implementing extensive public education initiatives and enhancing school curriculums to highlights the commonly known and unknown symptoms and risk factors of lung cancer may also help improve awareness.
Conclusion
Insufficient public awareness of the risk factors and symptoms of lung cancer in Saudi Arabia was observed, with a notable dependency on educational attainment and socio-economic status as the determining factors. One potential avenue for improvement involves the implementation of targeted campaigns aimed at enhancing public awareness of the obscure risk factors for and symptoms of lung cancer.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Prince Sultan Military College of Health Sciences Institutional Review Board (IRB-2023-RC-003). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants in accordance with the national legislation and the institutional requirements.
Author contributions
SAr: Investigation, Methodology, Writing – original draft, Writing – review & editing. JA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Writing – original draft, Writing – review & editing. AMA: Conceptualization, Data curation, Formal analysis, Methodology, Validation, Writing – review & editing. RS: Data curation, Formal analysis, Investigation, Writing – review & editing. AAAl: Data curation, Formal analysis, Investigation, Validation, Writing – review & editing. IA: Data curation, Investigation, Validation, Visualization, Writing – review & editing. ASA: Data curation, Investigation, Visualization, Writing – review & editing. BA: Conceptualization, Data curation, Formal analysis, Resources, Writing – review & editing. TGA: Data curation, Investigation, Resources, Writing – review & editing. AAAm: Data curation, Investigation, Methodology, Project administration, Writing – review & editing. SAg: Data curation, Methodology, Validation, Visualization, Writing – review & editing. FA: Data curation, Investigation, Resources, Writing – review & editing. MAl: Data curation, Investigation, Project administration, Resources, Validation, Visualization, Writing – review & editing. AFA: Data curation, Investigation, Resources, Writing – review & editing. AN: Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – review & editing. HA: Data curation, Formal analysis, Investigation, Validation, Visualization, Writing – review & editing. NA: Data curation, Investigation, Validation, Visualization, Writing – review & editing. AH: Data curation, Investigation, Project administration, Validation, Visualization, Writing – review & editing. MAs: Data curation, Investigation, Project administration, Resources, Visualization, Writing – review & editing. TO: Investigation, Methodology, Resources, Validation, Visualization, Writing – review & editing. MAa: Data curation, Investigation, Project administration, Validation, Visualization, Writing – review & editing. TMA: Data curation, Investigation, Project administration, Resources, Validation, Visualization, Writing – review & editing. MAm: Data curation, Investigation, Validation, Visualization, Writing – review & editing. EA: Data curation, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1295847/full#supplementary-material
References
1. Yuan J, Sun Y, Bu X, Ren H, Chen M. Global, regional and national burden of lung cancer and its attributable risk factors in 204 countries and territories, 1990–2019. Eur J Cancer Prev (2022) 31(3):253–9. doi: 10.1097/CEJ.0000000000000687
2. Sharma R. Mapping of global, regional and national incidence, mortality and mortality-to-incidence ratio of lung cancer in 2020 and 2050. Int J Clin Oncol (2022) 27(4):665–75. doi: 10.1007/s10147-021-02108-2
3. Thandra KC, Barsouk A, Saginala K, Aluru JS, Barsouk A. Epidemiology of lung cancer. Contemp Oncol (Pozn) (2021) 25(1):45–52. doi: 10.5114/wo.2021.103829
4. Colditz GA, Wolin KY, Gehlert S. Applying what we know to accelerate cancer prevention. Sci Transl Med (2012) 4(127):127rv4. doi: 10.1126/scitranslmed.3003218
5. Roudi F. Population trends and challenges in the Middle East and North Africa. Washington, DC, USA: Population Reference Bureau (2001).
6. WHO. WHO report on the global tobacco epidemic 2015: raising taxes on tobacco. Geneva, Switzerland: World Health Organization (2015).
7. Youlden DR, Cramb SM, Baade PD. The International Epidemiology of Lung Cancer: geographical distribution and secular trends. J Thorac Oncol (2008) 3(8):819–31. doi: 10.1097/JTO.0b013e31818020eb
8. Gibson GJ, Loddenkemper R, Lundbäck B, Sibille Y. Respiratory health and disease in Europe: the new European Lung White Book. Eur Respir J (2013) 42(3):559–63. doi: 10.1183/09031936.00105513
9. Council SH, Center NC, Registry SC. Cancer Incidence Report In Kingdom of Saudi Arabia. Riyadh: Saudi Health Council, Vol. 2018. (2018).
10. Alghamdi HI, Alshehri AF, Farhat GN. An overview of mortality & predictors of small-cell and non-small cell lung cancer among Saudi patients. J Epidemiol Glob Health (2018) 7 Suppl 1(Suppl 1):S1–s6. doi: 10.1016/j.jegh.2017.09.004
11. de Groot PM, Wu CC, Carter BW, Munden RF. The epidemiology of lung cancer. Trans Lung Cancer Res (2018) 7(3):220–33. doi: 10.21037/tlcr.2018.05.06
12. Pesch B, Kendzia B, Gustavsson P, Jöckel KH, Johnen G, Pohlabeln H, et al. Cigarette smoking and lung cancer–relative risk estimates for the major histological types from a pooled analysis of case-control studies. Int J Cancer (2012) 131(5):1210–9. doi: 10.1002/ijc.27339
13. Godtfredsen NS, Prescott E, Osler M. Effect of smoking reduction on lung cancer risk. Jama (2005) 294(12):1505–10. doi: 10.1001/jama.294.12.1505
14. Tse LA, Yu IT-s, Qiu H, Au J-k, Wang XR, Tam W, et al. Lung cancer decreased sharply in first 5 years after smoking cessation in Chinese men. J Thorac Oncol (2011) 6(10):1670–6. doi: 10.1097/JTO.0b013e3182217bd4
15. Moyer VA. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med (2014) 160(5):330–8. doi: 10.7326/M13-2771
16. Jazieh AR, Algwaiz G, Errihani H, Elghissassi I, Mula-Hussain L, Bawazir AA, et al. Lung cancer in the middle East and North Africa region. J Thorac Oncol (2019) 14(11):1884–91. doi: 10.1016/j.jtho.2019.02.016
17. Simon AE, Juszczyk D, Smyth N, Power E, Hiom S, Peake MD, et al. Knowledge of lung cancer symptoms and risk factors in the U.K.: development of a measure and results from a population-based survey. Thorax (2012) 67(5):426–32. doi: 10.1136/thoraxjnl-2011-200898
18. Hanson HM, Raag M, Adrat M, Laisaar T. Awareness of lung cancer symptoms and risk factors in general population. Open J Respir Dis (2016) 7(1):1–11. doi: 10.4236/ojrd.2017.71001
19. Robb K, Stubbings S, Ramirez A, Macleod U, Austoker J, Waller J, et al. Public awareness of cancer in Britain: a population-based survey of adults. Br J Cancer (2009) 101 Suppl 2(Suppl 2):S18–23. doi: 10.1038/sj.bjc.6605386
20. Group W. Development of the World Health Organization WHOQOL-BREF quality of life assessment. psychol Med (1998) 28(3):551–8. doi: 10.1017/S0033291798006667
21. Jain S, Dubey S, Jain S. Designing and validation of questionnaire. Int Dental Med J advanced Res (2016) 2(1):1–3. doi: 10.15713/ins.idmjar.39
23. Midthun DE. Early detection of lung cancer. F1000Res (2016) 5. doi: 10.12688/f1000research.7313.1
24. Elshami M, Abukmail H, Aqel W, Alser M, Al-Slaibi I, Shurrab H, et al. Awareness of Palestinians about lung cancer symptoms: a national cross-sectional study. BMC Pulm Med (2022) 22(1):135. doi: 10.1186/s12890-022-01923-1
25. Elshami M, Mansour A, Alser M, Al-Slaibi I, Abukmail H, Shurrab H, et al. Current situation and future directions of lung cancer risk factor awareness in Palestine: a cross-sectional study. BMJ Open (2023) 13(1):e061110. doi: 10.1136/bmjopen-2022-061110
26. Fontana RS, Sanderson DR, Woolner LB, Taylor WF, Eugene Miller W, Muhm JR, et al. Screening for lung cancer. A critique of the Mayo Lung Project. Cancer (1991) 67(S4):1155–64. doi: 10.1002/1097-0142(19910215)67:4+<1155::aid-cncr2820671509>3.0.co;2-0
27. Qattan AMN, Boachie MK, Immurana M, Al-Hanawi MK. Socioeconomic determinants of smoking in the Kingdom of Saudi Arabia. Int J Environ Res Public Health (2021) 18(11). doi: 10.3390/ijerph18115665
28. Alqahtani JS, Aldhahir AM, Alanazi Z, Alsulami EZ, Alsulaimani MA, Alqarni AA, et al. Impact of smoking status and nicotine dependence on academic performance of health sciences students. Subst Abuse Rehabil (2023) 14:13–24. doi: 10.2147/SAR.S393062
29. Redeker C, Wardle J, Wilder D, Hiom S, Miles A. The launch of Cancer Research UK's 'Reduce the Risk' campaign: baseline measurements of public awareness of cancer risk factors in 2004. Eur J Cancer (2009) 45(5):827–36. doi: 10.1016/j.ejca.2008.10.018
30. Gaskin J, Coyle D, Whyte J, Krewksi D. Global estimate of lung cancer mortality attributable to residential radon. Environ Health Perspect (2018) 126(5):057009. doi: 10.1289/EHP2503
31. Hosgood HD III, Boffetta P, Greenland S, Lee Y-CA, McLaughlin J, Seow A, et al. In-home coal and wood use and lung cancer risk: a pooled analysis of the International Lung Cancer Consortium. Environ Health Perspect (2010) 118(12):1743–7. doi: 10.1289/ehp.1002217
32. Alqahtani JS, Aldhahir AM, Siraj RA, Alqarni AA, AlDraiwiesh IA, AlAnazi AF, et al. A nationwide survey of public COPD knowledge and awareness in Saudi Arabia: A population-based survey of 15,000 adults. PloS One (2023) 18(7):e0287565. doi: 10.1371/journal.pone.0287565
33. Alqahtani JS. Prevalence, incidence, morbidity and mortality rates of COPD in Saudi Arabia: Trends in burden of COPD from 1990 to 2019. PloS One (2022) 17(5):e0268772. doi: 10.1371/journal.pone.0268772
34. Chawla R, Sathian B, Mehra A, Kiyawat V, Garg A, Sharma K. Awareness and assessment of risk factors for lung cancer in residents of Pokhara Valley. Asian Pac J Cancer Prev (2010) 11(6):1789.
35. Coughlin SS. Recall bias in epidemiologic studies. J Clin Epidemiol (1990) 43(1):87–91. doi: 10.1016/0895-4356(90)90060-3
36. Althubiti MA, Nour Eldein MM. Trends in the incidence and mortality of cancer in Saudi Arabia. Saudi Med J (2018) 39(12):1259–62. doi: 10.15537/smj.2018.12.23348
Keywords: lung cancer, Saudi Arabia, public awareness, survey, smoking
Citation: AlRabeeah SM, Alzahrani EM, Aldhahir AM, Siraj RA, Alqarni AA, AlDraiwiesh IA, Alqahtani AS, Almqati BS, Alharbi TG, Almuntashiri AA, Alghamdi SM, Aljohani FE, Almulhim MA, Alshehri AF, Naser AY, Alwafi H, Alobaidi NY, Hjazi AM, Alsulaimani MA, Oyelade T, Alahmari M, Alanazi TM, Almeshari MA and Alqahtani JS (2024) A population-based study of 15,000 people on Knowledge and awareness of lung cancer symptoms and risk factors in Saudi Arabia. Front. Oncol. 14:1295847. doi: 10.3389/fonc.2024.1295847
Received: 17 October 2023; Accepted: 29 January 2024;
Published: 20 February 2024.
Edited by:
Seyed Aria Nejadghaderi, Shahid Beheshti University of Medical Sciences, IranReviewed by:
Mohamedraed Elshami, University Hospitals Cleveland Medical Center, United StatesFouad M. Fouad, American University of Beirut, Lebanon
Copyright © 2024 AlRabeeah, Alzahrani, Aldhahir, Siraj, Alqarni, AlDraiwiesh, Alqahtani, Almqati, Alharbi, Almuntashiri, Alghamdi, Aljohani, Almulhim, Alshehri, Naser, Alwafi, Alobaidi, Hjazi, Alsulaimani, Oyelade, Alahmari, Alanazi, Almeshari and Alqahtani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jaber S. Alqahtani, QWxxYWh0YW5pLUphYmVyQGhvdG1haWwuY29t
†These authors have contributed equally to this work and share first authorship