 Wendy Ng
Wendy Ng Darren Beales1,2
Darren Beales1,2 Daniel F. Gucciardi
Daniel F. Gucciardi- 1Curtin School of Allied Health, Curtin University, Perth, WA, Australia
- 2Curtin enAble Institute, Curtin University, Perth, WA, Australia
Achieving high value, biopsychosocial pain care can be complex, involving multiple stakeholders working synergistically to support the implementation of quality care. In order to empower healthcare professionals to assess, identify and analyse biopsychosocial factors contributing to musculoskeletal pain, and describe what changes are needed in the whole-of-system to navigate this complexity, we aimed to: (1) map established barriers and enablers influencing healthcare professionals' adoption of a biopsychosocial approach to musculoskeletal pain against behaviour change frameworks; and (2) identify behaviour change techniques to facilitate and support the adoption and improve pain education. A five-step process informed by the Behaviour Change Wheel (BCW) was undertaken: (i) from a recently published qualitative evidence synthesis, barriers and enablers were mapped onto the Capability Opportunity Motivation-Behaviour (COM-B) model and Theoretical Domains Framework (TDF) using “best fit” framework synthesis; (ii) relevant stakeholder groups involved in the whole-of-health were identified as audiences for potential interventions; (iii) possible intervention functions were considered based on the Affordability, Practicability, Effectiveness and Cost-effectiveness, Acceptability, Side-effects/safety, Equity criteria; (iv) a conceptual model was synthesised to understand the behavioural determinants underpinning biopsychosocial pain care; (v) behaviour change techniques (BCTs) to improve adoption were identified. Barriers and enablers mapped onto 5/6 components of the COM-B model and 12/15 domains on the TDF. Multi-stakeholder groups including healthcare professionals, educators, workplace managers, guideline developers and policymakers were identified as target audiences for behavioural interventions, specifically education, training, environmental restructuring, modelling and enablement. A framework was derived with six BCTs identified from the Behaviour Change Technique Taxonomy (version 1). Adoption of a biopsychosocial approach to musculoskeletal pain involves a complex set of behavioural determinants, relevant across multiple audiences, reflecting the importance of a whole-of-system approach to musculoskeletal health. We proposed a worked example on how to operationalise the framework and apply the BCTs. Evidence-informed strategies are recommended to empower healthcare professionals to assess, identify and analyse biopsychosocial factors, as well as targeted interventions relevant to various stakeholders. These strategies can help to strengthen a whole-of-system adoption of a biopsychosocial approach to pain care.
Introduction
Engel's biopsychosocial model (1), has provided a blueprint for contemporary care of chronic pain disorders (2–10). However, there are significant challenges putting this model into clinical practice (11, 12). Pain is complex with multidimensional (biological, psychological and social) factors interacting to influence the lived experience (3, 13), often with multimorbidity (chronic lifestyle illnesses and mental health illnesses) (14). This complexity makes comprehending and caring for each individual's needs as a whole person challenging for healthcare professionals.
Against this background, we previously systematically reviewed evidence and generated insights on the barriers and enablers to the adoption of the biopsychosocial model in musculoskeletal pain, spanning the whole-of-health. Our recent qualitative review included 25 studies and the perspectives of 413 healthcare professionals (15). There are multiple factors influencing healthcare professionals' adoption of the biopsychosocial model. At the micro-level (clinical interface), healthcare professionals' knowledge and skills, personal factors, their misconceptions of clinical practice guidelines, perception of patients' factors, and time can influence adoption of a biopsychosocial approach. At the meso-level (health service provision), clinical practice guideline formulation, the availability and alignment of the clinical community, funding models, health service provision, resourcing, and workforce training issues may or may not adequately support the care. At the macro-level (health system), health policy, organizational, and social factors can significantly affect and shape how care for musculoskeletal disorders is delivered. Further evidence for challenges to adoption come from another review that included 12 qualitative studies and the views of 113 physiotherapists showing that despite the positive changes with education, physiotherapists lack confidence to implement biopsychosocial pain care (16). These findings are supported by the modest effect of educational meetings on changing clinical practice behaviours and clinical outcomes (17–21). Re-design of educational efforts to address the micro-level barriers might facilitate healthcare professionals in adopting the model in pain care, while also leveraging the meso- and macro-level enablers.
Using behavioural science frameworks to understand human behaviour may provide insights into how to drive translation efforts to support effective design of behavioural interventions that target relevant audiences involved in pain care (22). Inferring from Engel's original frame of reference of the Biopsychosocial Model (1), our specification of the target behaviour is: Healthcare professionals (who) assessing, identifying and analysing biopsychosocial factors contributing to musculoskeletal pain (what), using authentic communication upon patient interview within a strong therapeutic alliance and critical clinical reasoning (how, with whom), during consultation in clinical practice (when, where). We are also interested in what the critical stakeholder groups within healthcare services and systems (meso- and macro-level) can do, to assist healthcare professionals to achieve specified target behaviours.
The Behaviour Change Wheel (BCW) is derived from 19 frameworks of behaviour change, and is a systematic process used for designing behavioural interventions (23, 24). Broadly, the process covers understanding the behaviour, identifying intervention options, and identifying content and implementation options (23, 24). At the hub of the wheel is the Capability Opportunity Motivation-Behaviour (COM- B) model, surrounded by nine intervention functions and seven policy categories (24). The Theoretical Domains Framework (TDF) expands on the COM-B components and provides a more detailed understanding of the cognitive, affective, social and environmental influences on behaviour (25). The COM-B and TDF can be used to understand behaviour at the individual, community and organizational levels (23), i.e., allows us to analyse necessary conditions internal to individuals, and the social and physical environment to achieve a specified target behaviour (24). This is well-aligned to investigating what can empower healthcare professionals to assess, identify and analyse biopsychosocial factors at the clinical-level, what can support them at the health service and policy levels (across multi-levels) (26). It is also worth noting the COM-B model and TDF have been used in the implementation of evidence-based recommendations of musculoskeletal conditions (27–30). The hypothesized relationship between the COM-B model components and intervention functions in the BCW allows a precise analysis of how to make the selection of interventions and policies (24), after which can then be linked to specific behaviour change techniques (BCTs) (24, 31). The BCW offered a comprehensive and solid theoretical foundation for the synthesis.
Thus, the aims of this study are:
(i) to map established barriers and enablers influencing healthcare professionals' adoption of a biopsychosocial approach to musculoskeletal pain (15) using theoretical frameworks of behaviour change (23–25, 27, 31), and in the process, identify the behavioural determinants that can support the adoption,
(ii) formulate a novel conceptual model (using concepts from the COM-B model and TDF) to outline the behavioural determinants, as an overview to a whole-of-health perspective to healthcare professionals' adoption of the biopsychosocial model, and
(iii) derive a framework of BCTs that characterise how various stakeholder groups can help improve current pain education training efforts to support healthcare professionals' adoption of biopsychosocial musculoskeletal pain care.
Methods
We adopted a five-step process informed by the BCW (23, 24) (Figure 1) to synthesize the 46 subthemes and 14 main themes derived from our systematic review of the barriers and enablers influencing healthcare professionals' adoption of a biopsychosocial approach to musculoskeletal pain (15). These subthemes and main themes were therefore our data set used to apply the behavioural analysis. In each step, when discussion was necessary, iterative consensus was used to reach agreement within the research team (32). The characteristics and reflexivity of the research team members are described in Table 1. The team adopted our epistemological position as constructivist (33). Overall, the team has expertise that cuts across the micro-, meso- and macro-levels of healthcare, and proficiency with the biopsychosocial model, musculoskeletal pain, and the BCW process. Please note that all definitions and detailed description of terminologies related to the BCW are provided in the Supplementary Tables S1–S4.
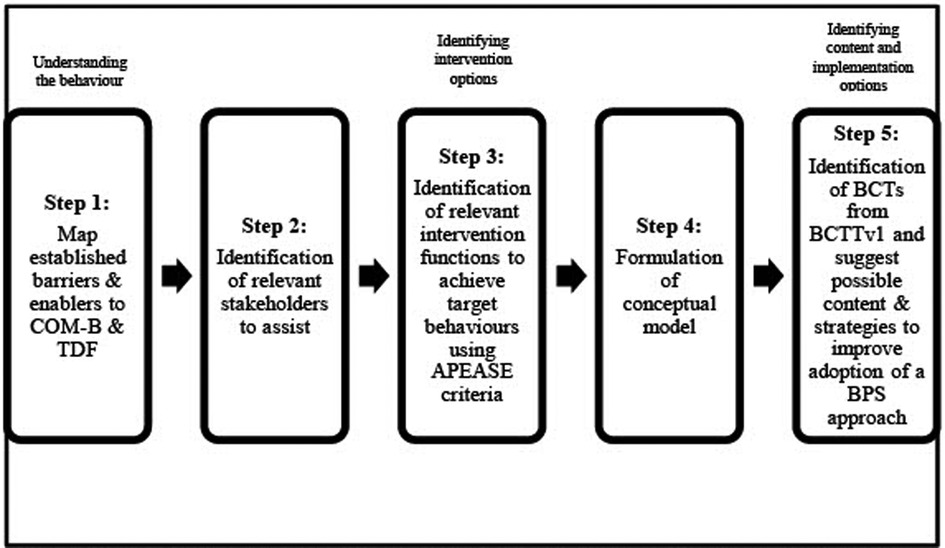
Figure 1. An Overview of the five-step process, informed by the behavioural change wheel (BCW). APEASE, affordability, practicability, effectiveness/cost-effectiveness, acceptability, side-effects/safety, equity; BCTs, behaviour change techniques; BCTTv1, behaviour change techniques taxonomy version 1; BPS, biopsychosocial; COM-B, capability opportunity motivation-behaviour model; TDF, theoretical domains framework.
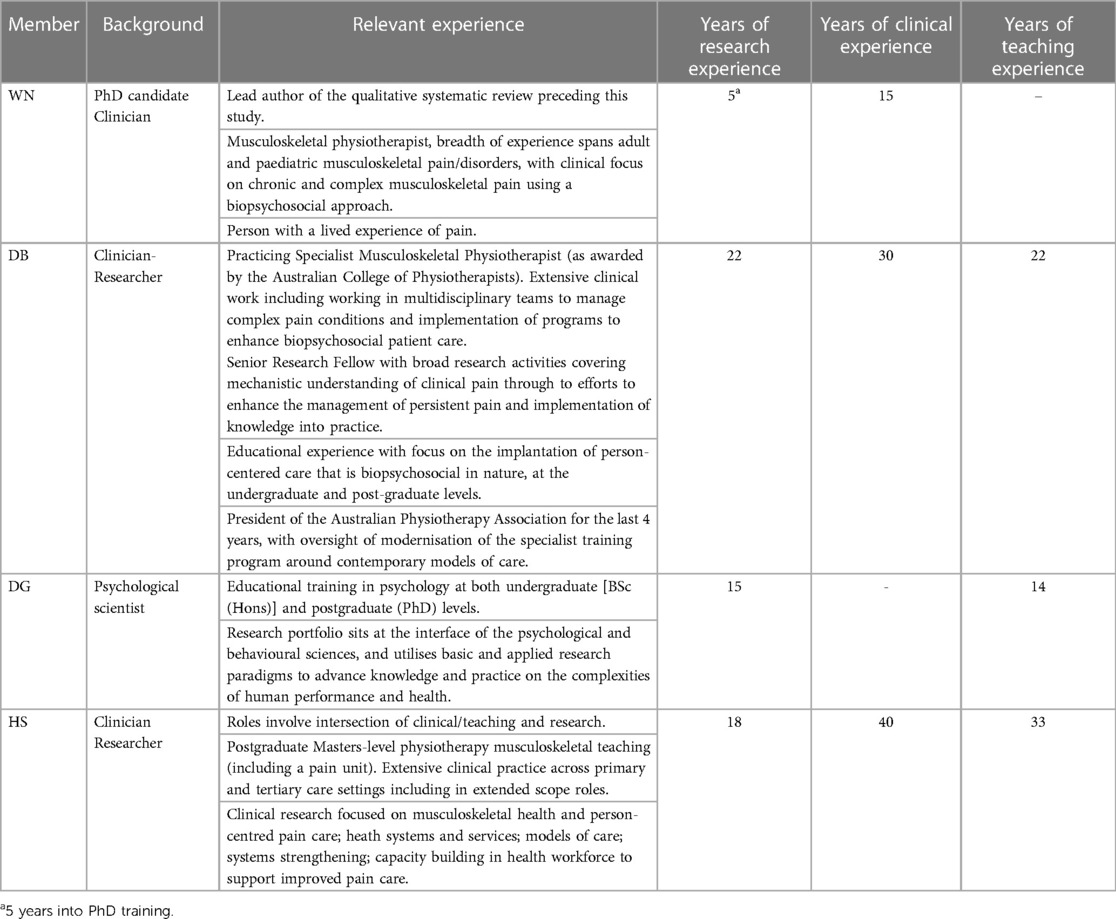
Table 1. Characteristics & reflexivity of the research team.
We utilised a “best fit” framework synthesis (34–36) approach to analyse and develop new insights on the behavioural determinants to the adoption of biopsychosocial musculoskeletal pain care (hereafter, referred to as “adoption”). Framework synthesis offered a theory-based synthesis method, and utility and value have already been demonstrated in areas of healthcare with policy relevance (35). This approach allowed the application of a primarily deductive approach (34, 36) to the data, yet also permitted inductive revision and supplementation of the “a priori” theory (35). The components of the COM-B model, “capability”, “opportunity”, “motivation” and “behaviour”, and the 14 domains of the TDF (23), formed the “a priori” framework for the synthesis. The approach enabled us to further interrogate from a behavioural perspective, previously established themes from our qualitative review and identify gaps in the knowledge. The definition of each COM-B component and TDF domain (Supplementary Material) were provided to research team members to facilitate consistent interpretation and mapping of the data to the framework. The following steps demonstrate our phased methodologic approach:
Step 1 Mapping previously derived subthemes to the COM-B model and TDF
Three team members (WN, DB, DG) were provided with a Microsoft Excel spreadsheet consisting of the 46 subthemes drawn from our previous qualitative synthesis (15). They independently mapped these subthemes against the COM-B model and TDF. Conflicts or discrepancy in the mapping results were resolved through discussion and consensus with the mapping team and an additional independent team member (HS).
Step 2 Identifying stakeholders who may potentially influence healthcare professionals' adoption of a biopsychosocial model in musculoskeletal pain care
All team members studied the overall outcomes from Step 1. Based on the extracted data from the studies included in our previous review (15), the team derived a minimum list of stakeholders. This included stakeholders from across the whole-of-health from the micro-level (clinical interface), meso-level (health service provision and workforce training), and macro-level (health system).
In this step, a list of stakeholders and the previously derived 14 main themes were presented as a word document to the team. Members were tasked with independently answering the question “Is the theme critical for this stakeholder group to intervene on to improve biopsychosocial adoption?” We defined “intervene” as “to become intentionally involved in influencing and improving adoption”. More than one stakeholder group could be selected to intervene for each theme, and team members could nominate any other relevant stakeholder group not otherwise mentioned but considered important potential contributors to adoption. Consensus on the most appropriate “proposed stakeholders” to potentially intervene on each of the 14 themes was achieved through a meeting.
Step 3 Deciding what intervention functions were important in supporting healthcare professionals' adoption of a biopsychosocial model
To establish which category of interventions could potentially shift the behaviour of healthcare professionals to improve adoption, team members were asked to independently respond to this question “From the nine BCW intervention functions (education, persuasion, incentivisation, coercion, training, restriction, environmental restructuring, modelling, enablement), which function(s) meet the affordability, practicability, effectiveness/cost-effectiveness, acceptability, side-effects/safety, equity (APEASE) criteria to improving adoption?” (Definition of these intervention functions are shown later under results). We applied the APEASE criteria (23) to make strategic judgments on what might be the most appropriate intervention(s), with real world applicability. The description of the APEASE criteria can be found in Supplementary Material. Responses were collated and recorded on a Word document.
Step 4 Interpreting and conceptualising: Formulation of a conceptual model to understand the behavioural determinants and reach consensus on who may potentially influence healthcare professionals' adoption of the biopsychosocial model
A conceptual model, comprised of the pre-determined concepts (from the COM-B model and TDF) and newly-derived concepts integrated together, was developed to describe the behavioural determinants and explained how alignment of the various stakeholder groups could help achieve the goal of biopsychosocial musculoskeletal pain care.
The combination of the “a priori” concepts from the COM-B and TDF, and the research team members' newly-derived concepts from the interpretation of the data, highlighted the use of both deductive and inductive analyses in this step. The resultant synthesis of the conceptual model was built on the COM-B model and TDF, and was further enhanced with additional concepts from our qualitative review (15). This moved the description of the data used for the analysis to a higher level of abstraction and created an integrative conceptual framework. WN conceptualized and drew the conceptual model, the rest of the team commented on and refined the model to accurately reflect a visual representation of the behavioural determinants.
Step 5 Derivation of a pragmatic framework of behaviour change techniques to improve adoption
A behaviour change technique (BCT) is defined as “an active component of an intervention designed to change behaviour” (23). Here, we were interested to identify the observable, replicable, and irreducible components (i.e., active ingredients) of an intervention (31) that could facilitate behaviour change in healthcare professionals towards improved adoption. To approach this step, we gave thoughtful consideration to a principle used to achieve rigor in qualitative research analysis (37)—a hybrid approach of inductive and deductive analysis (38). Using both inductive and deductive analyses enabled us to collate a more comprehensive list of BCTs, grounded in the evidence-base, that would not have been achieved using either approach alone.
Figure 2 shows a graphic summary of the applied processes of deductive and inductive analyses.
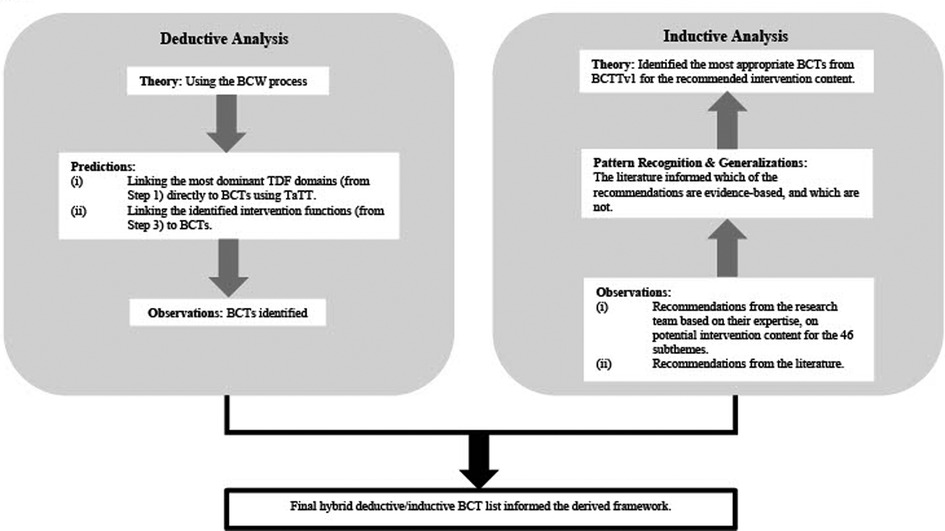
Figure 2. A graphic summary of the process of deductive and inductive analyses applied to derive a hybrid list of BCTs. Deductive analysis involves applying a theory (in this case, the Behaviour Change Wheel) to make predictions to our observed data. Inductive analysis involves observing our data thoroughly using researches’ reflexivity and the evidence-base, to look for patterns, trends and generalizations in the data, to see if the data fits into a suggested theory (i.e., behavioural change techniques). BCTs, behaviour change techniques; BCTTv1, behaviour change techniques taxonomy version 1; BCW, behavioural change wheel; TDF, theoretical domains framework; TaTT, theory and technique tool.
Deductive analysis
(i) Linking TDF domains directly to BCTs using the Theory and Technique Tool (TaTT).
Based on the overall mapping results in Step 1, in order to identify priority areas for focusing intervention efforts to improve training and support for healthcare professionals' pain education, the most dominant TDF domains (as defined by count of the number of subthemes, at the micro-level, meso- and macro-level) populated by the mapping data were identified (WN). The most dominant TDF domains were linked directly to BCTs using the Theory and Technique Tool (TaTT) (39) via the Theory and Technique Tool website (40) through deductive inference. On the TaTT, the strength of a particular link between a mechanism of action/TDF domain and a BCT is denoted by four different coloured cells—white (“no evidence”), yellow (“inconclusive”), blue (“non-links”) or green (“links”) (39, 41, 42). For the purpose of this study, we wanted to identify the most effective BCTs to target on the most dominant TDF domains, hence only the green cells (“links”) were considered.
(ii) Linking intervention functions to BCTs.
From Step 3, the identified intervention functions were then linked to the BCTs on Behavioural Change Techniques Taxonomy v1 (BCTTv1) (Supplementary Material) deductively by the BCW (23, 31). The links between intervention functions and BCTs had been established by expert consensus (23). To narrow down the list of BCTs for selection, for each intervention function, we only considered the most frequently used BCTs (43).
Using both deductive methods of linking, we were able to make predictions and identify which BCTs could potentially be adopted to target specific behavioural change. At this point, we assessed whether the BCTs selected would fit into proposed intervention(s) that also met the APEASE criteria i.e., were affordable, practical, cost-effective, acceptable, safe and equitable in the real world. One researcher (WN) collated, observed, and compared the two list of BCTs derived from both deductive methods of linking.
Inductive analysis
Based on their areas of expertise, the research team discussed their recommendations on how to address the target behaviour (Table 2) and suggested potential intervention content. These data were recorded in an Excel spreadsheet and interrogated against the 46 subthemes (the dataset) to ensure recommendations targeted specific areas relevant to healthcare professionals assessing, identifying and analysing biopsychosocial factors contributing to musculoskeletal pain. Recommendations from the team were collaboratively discussed and synthesized inductively and iteratively. The literature was then reviewed to examine if these recommendations were reflected in the evidence-base. The entire inductive analysis process was both iterative and reflexive. The most appropriate BCTs were identified by coding the intervention content to the most relevant grouping and definition of the BCT on the BCTTv1.
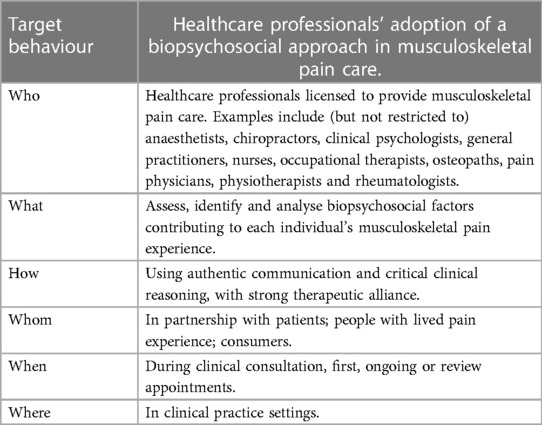
Table 2. Specifications of the target behaviour.
Derivation of a final framework of BCTs
Based on what is in common between the BCTs derived from deductive linking, and the BCTs derived from inductive analysis of recommendations from the research team (that is also evidence-based), a hybrid list of BCTs (required at the bare minimal) to facilitate change towards improved adoption were identified.
The recommended strategies that could potentially empower healthcare professionals to assess, identify and analyse biopsychosocial factors contributing to musculoskeletal pain were collated and reported under “discussion”. The research team also derived a worked example of how to use BCTs to improve healthcare professionals' adoption of a biopsychosocial approach across the whole-of-health.
Results
Step 1 Mapping previously derived subthemes to the COM-B model and TDF
Table 3 provides a detailed breakdown of how the subthemes from our previous qualitative evidence synthesis (15) mapped onto the COM-B model and TDF. A subtheme could be mapped onto more than one component on the COM-B and more than one domain on the TDF. An overview of the number of subthemes mapped to each COM-B component and TDF domain is provided in Supplementary Table S5. Overall, the 46 subthemes (barriers and enablers to the adoption of a biopsychosocial approach) mapped on 5/6 components on the COM-B model (with the exception of physical capability), and 12/15 domains on the TDF (with the exception of physical skills, optimism and goals), reflecting that the adoption of a biopsychosocial approach involved a complex set of behavioural determinants across multi-levels of healthcare.
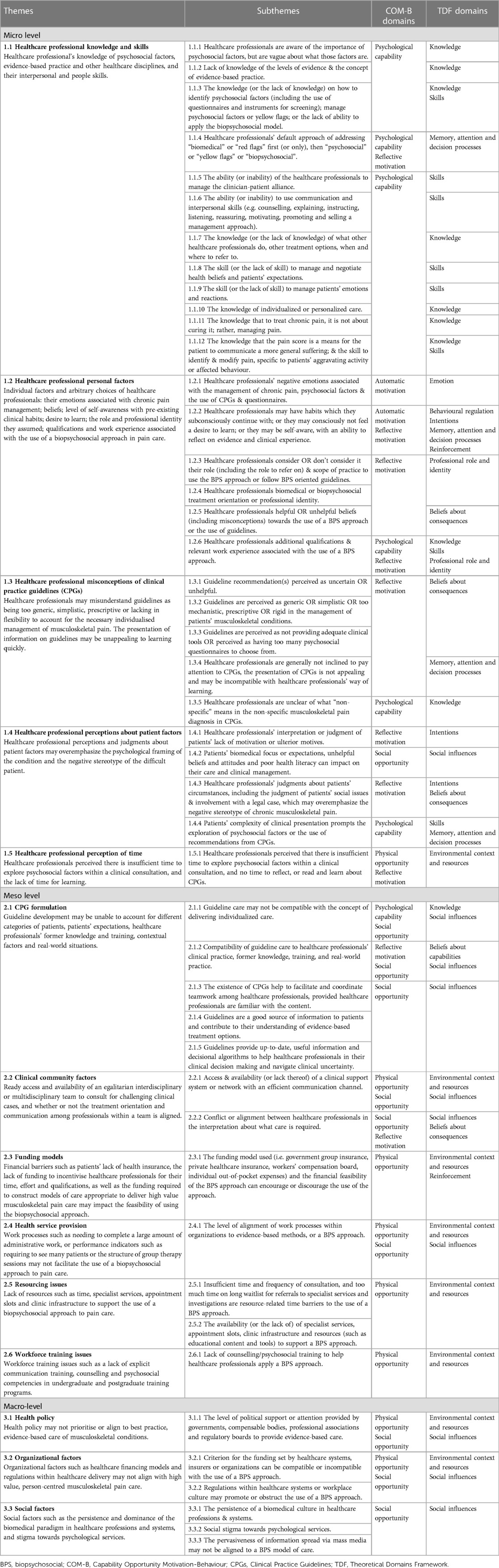
Table 3. Healthcare professionals’ barriers and enablers to the biopsychosocial approach mapped onto the COM-B model and TDF.
Step 2 Identifying stakeholders who may potentially influence healthcare professionals’ adoption of a biopsychosocial model in musculoskeletal pain care
Table 4 shows the tabulation of the identified key stakeholder groups. Healthcare professionals, educators, guideline developers, workplace managers, and policymakers were the stakeholder groups identified as target audiences for potential interventions. Researchers were considered as relevant to all five stakeholder groups. Researchers' roles may involve an investigation into healthcare professionals' behaviour, educators' behaviour, evaluation of clinical practice guideline implementation, workplace programs or policy implementation.
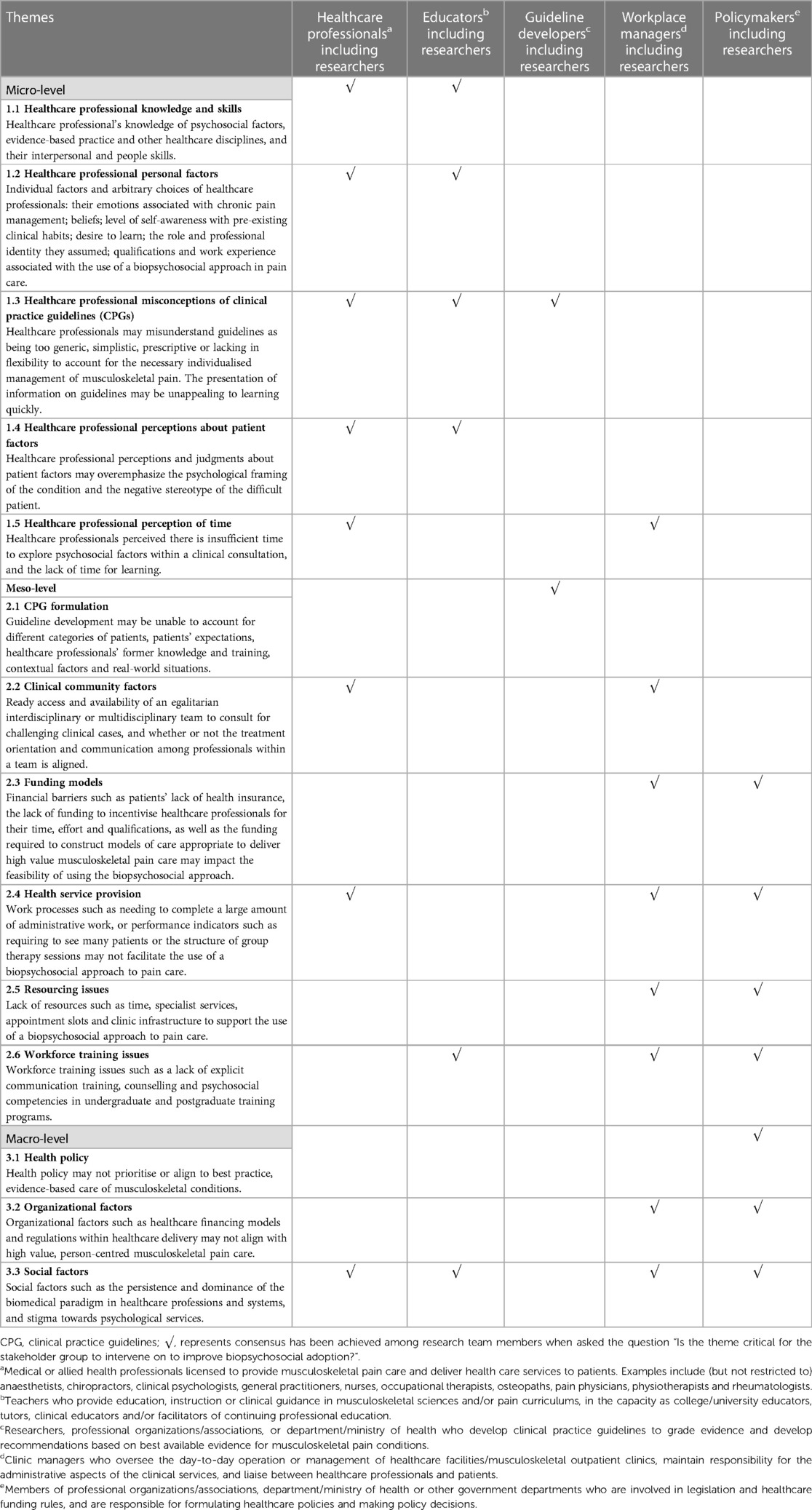
Table 4. The key stakeholder groups to target behavioural interventions for the respective barriers and enablers to the adoption of the biopsychosocial approach.
Step 3 Deciding what intervention functions were important in supporting healthcare professionals’ adoption of a biopsychosocial model
Table 5 provides a list of targeted intervention functions that could help to address specific barriers to healthcare professionals' adoption of a biopsychosocial approach to musculoskeletal pain care. A supporting rationale is shown. This is based upon considering criteria such as affordability, practicability, effectiveness/cost-effectiveness, acceptability, side-effects/safety, and equity (APEASE). Team members discussed and reached consensus that the essential intervention functions important in supporting healthcare professionals' adoption of a biopsychosocial model were education, training, environmental restructuring, modelling and enablement.
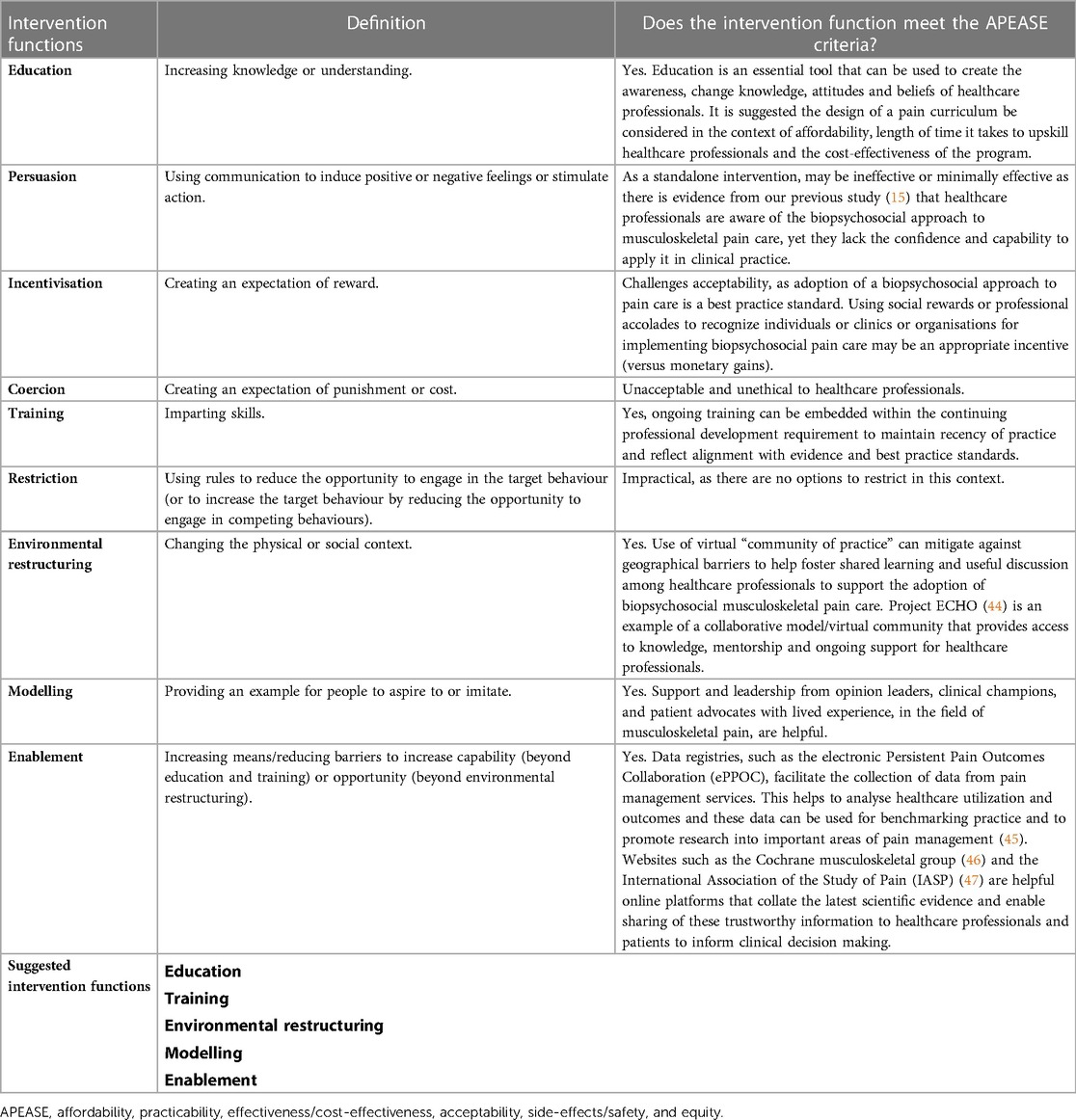
Table 5. Selection of the intervention functions and rationale based on the APEASE criteria.
It is important to note that in this step, applying the APEASE criteria to decide on the intervention functions is essentially a judgment call by the research team, based on our researchers' reflexivity and positionality (Table 1). Our assessment using the APEASE criteria may or may not accurately represent the views of stakeholder groups such as the workplace manager and policymaker, as there is no such representation within the research team. However, it is noteworthy that two of the team members (DB, HS) have relevant experience in collaborating with service providers, workplace managers and policymakers in their clinical and research scope of work. Whether the selected intervention functions will result in improved adoption of biopsychosocial musculoskeletal pain care remains to be tested.
Step 4 Interpreting and conceptualising: formulation of a conceptual model to understand the behavioural determinants, and reach consensus on who may potentially influence healthcare professionals’ adoption of the biopsychosocial model
A conceptual model is shown to simplify the behavioural determinants of healthcare professionals adopting biopsychosocial pain care. The model aligns stakeholders towards enacting emergent, novel behaviours supporting biopsychosocial pain care. Figure 3 provides readers with a summary at one glance to understand the behavioural determinants and the major stakeholder groups that need to be involved, to help support healthcare professionals to achieve biopsychosocial pain care.
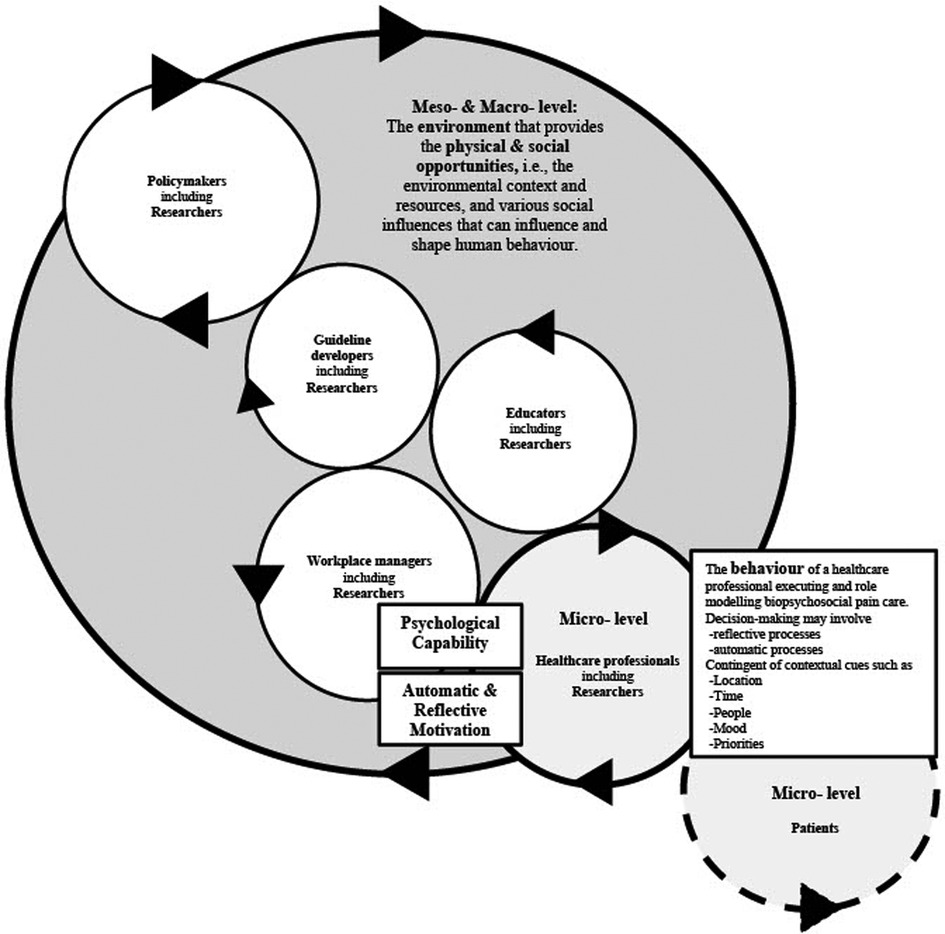
Figure 3. A conceptual cogwheel model outlinning the behavioural determinates of healthcare professionals adopting biopsychosocial pain care, and aligning stakeholders towards enacting emergent, novel behaviours supporting pain care. The terms “psychological capability”, “automatic & reflective motivation”, “behaviour”, “physical & social opportunity” are concepts from the COM-B model. The terms “enviromental context and resources” “social influences” are concepts from the TDF. COM-B, capability opportunity motivation-behaviour model; TDF, theoretical domains framework.
A new conceptual model differentiated from the original COM-B model (23) was developed (Figure 3) and demonstrates the relationship between “capability”, “motivation”, “behaviour”, and “opportunity”. Unlike the original COM-B model that does not give dominance to either factor “capability”, “opportunity”, or “motivation” influencing behaviour, this graphic proposes the environment (i.e., physical and social opportunity) in which healthcare professionals practise is crucial to adoption (illustrated as the big shaded circle, comprising of other stakeholder groups). Healthcare professionals (illustrated as the smaller circle) are surrounded by environmental context and social influences (physical and social opportunities) of the healthcare system, which will influence and shape how they behave. However, behaviours may sometimes be “out of context”- that is why the smaller circle representing the healthcare professional is drawn slightly out of the big circle representing the environmental context. Healthcare professionals' behaviours require psychological capability in decision-making in complex and varied clinical scenarios and may involve both reflective and automatic processes (or motivation) (48). Reflective processes refer to the cognitive ability, awareness and conscious deliberation to make complex clinical decisions before enacting behaviour; whereas automatic processes are learnt predispositions/proclivity to think or act in a given way or habits. These processes are cued by external factors (location, time, or people) or internal reactions and factors (mood or priorities) of the healthcare professional (48, 49).
A hypothetical patient cogwheel (illustrated as the circle with dotted line) is interacting with and influencing the behaviour of the healthcare professional, and vice versa. Every stakeholder, illustrated as interconnected individual circles, plays a role in the whole healthcare landscape (illustrated as the big shaded circle, i.e., representing the environmental context and social influences). The behaviour of a complex system emerges from the interaction of the six stakeholder groups (patients, healthcare professionals, educators, workplace managers, guideline developers and policymakers) (50), and will potentially influence and change the environmental and social context towards supporting the goal of biopsychosocial pain care, with the whole being greater than the sum of its parts. In other words, these emergent, novel behaviours extend beyond the clinician-patient system to the remainder of the healthcare system, encouraging communication and relationship-centered care among stakeholders across all levels of healthcare (51, 52). A circle coming in contact with another circle here represents the interdependency of the stakeholders to one another, though alignment of the stakeholders is not necessarily mutually exclusive (e.g., workplace managers may come directly in contact with policymakers). Arrows are used to denote the dynamicity of the system, i.e., moving one cogwheel can potentially influence and impact the adjacent aligning cogwheel. Subsequently, the interdependencies can set the whole cogwheel system in motion (synonymous to cooperation and collaboration between stakeholders). However, if one cogwheel moves in a direction that does not align with the rest of the cogwheels, it may potentially create a barrier or “logjam” in the system.
Step 5 Derivation of a pragmatic framework of behaviour change techniques to improve adoption
As shown in Table 3 (and Supplementary Table S5), the majority of the micro-level subthemes mapped to the “knowledge” and “cognitive and interpersonal skills” domain on the TDF, whereas the majority of the meso-level and macro-level subthemes mapped to the “environmental context and resources” and “social influences” domain on the TDF.
Table 6 shows the list of BCTs identified via two deductive methods of linking, inductive analysis and the final hybrid list of BCTs identified by both deductive linking and inductive analysis. The full BCT taxonomy v1 and the definition of each BCT are provided in Supplementary Table S4.
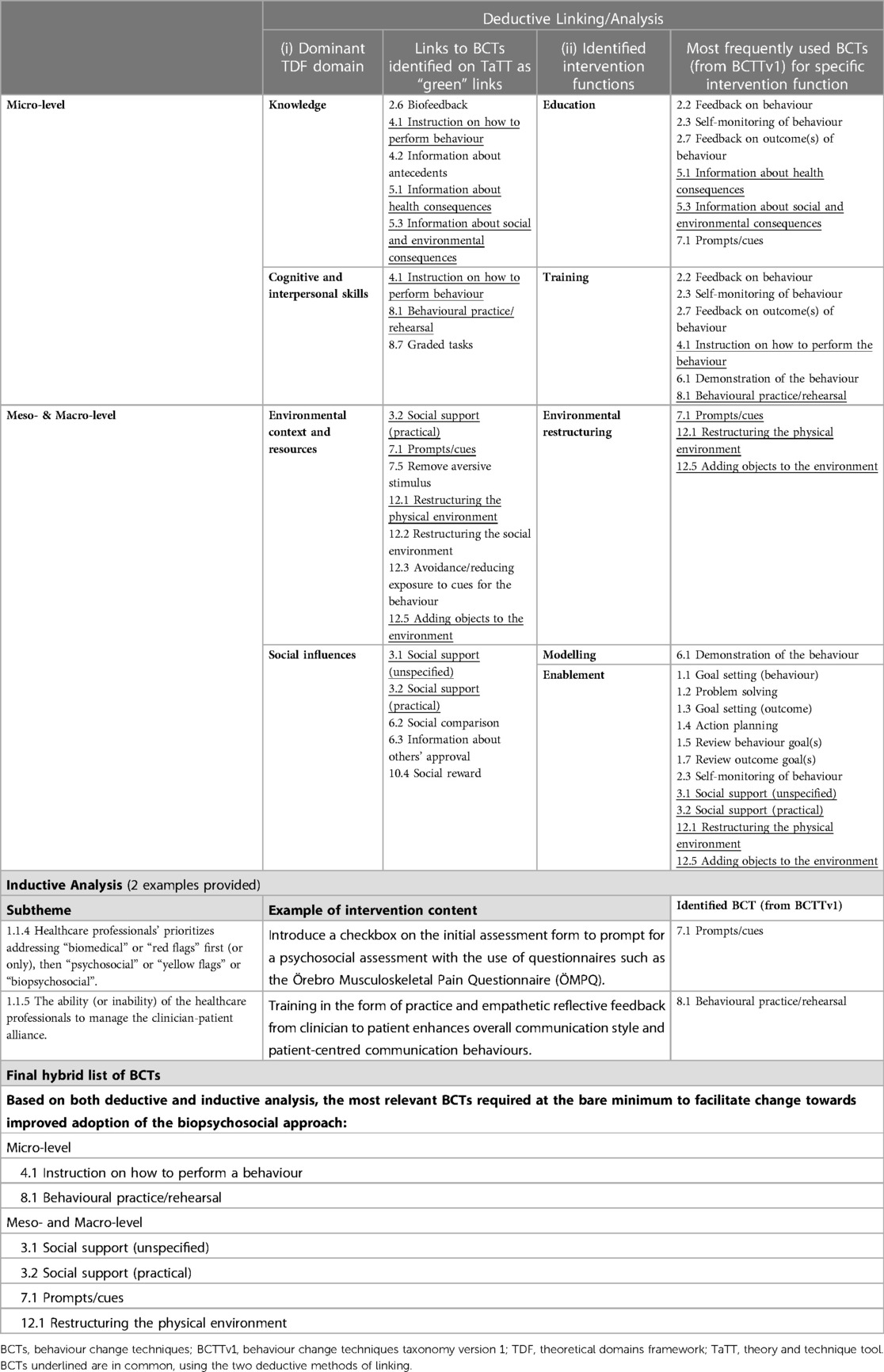
Table 6. Identified behaviour change techniques derived from deductive linking, inductive analysis resulting in the final hybrid list.
Overall, six BCTs from BCTTv1 were identified as relevant and the minimum required to facilitate healthcare professionals' behaviour change towards improved adoption. At the micro-level, BCTs “4.1 instruction on how to perform a behaviour” and “8.1 behavioural practice/rehearsal” were relevant. At the meso- and macro-level, BCTs “3.1 social support (unspecified)”, “3.2 social support (practical)”, “7.1 prompts/cues”, and “12.1 restructuring the physical environment” were relevant.
A template of our synthesized framework of BCTs, with the links between the dominant COM-B components and TDF domains, intervention functions and the selected BCTs as informed by the BCW process (23, 24, 31, 40–43) can be found in Supplementary Table S6.
Discussion
This study describes a novel systematic approach in which we leveraged principles from the BCW process to (i) identify behavioural determinants that can support the adoption of a biopsychosocial approach, (ii) formulate a novel conceptual model outlining these behavioural determinants, and (iii) derive a framework of BCTs that have the potential to facilitate and improve healthcare professionals' adoption of a biopsychosocial approach to musculoskeletal pain care. This approach provides a blueprint to road test how target interventions can help improve healthcare professionals' understanding of pain by addressing important target behaviours that underpin quality pain care.
In line with the aim of our work, a recent review (26) also investigated and mapped the barriers and facilitators to a biopsychosocial approach against the TDF and subsequently to the TaTT. These colleagues identified 10 TDF domains and 33 BCTs that could foster implementation. Consistent with our findings, the authors highlighted that implementation of a biopsychosocial approach is complex (26). That study also used deductive coding and analysis, and their results were specific to physiotherapy practice. In contrast, by taking a more in-depth and broader whole-of-system approach to driving adoption, our study value-adds to the evidence base by (i) amalgamating the determinants to derive a cogwheel model to enhance understanding of the subject matter from a behavioural perspective, (ii) identifying relevant stakeholder groups to intervene, (iii) suggesting targeted intervention functions and content, and (iv) identifying core BCTs to improve adoption.
The use of both deductive and inductive analysis in our study is a strength of this study as we combined the use of theory with clinical and research expertise. It is important to note the BCW process is not a panacea for behaviour change but a system of using best available evidence, informed judgment and resources to arrive at a strategy to address a specified behaviour (23). Hence, this discussion is structured to elucidate our reasoning processes. Stakeholders working within the health services and systems level may derive practical, useful and actionable insights from our findings.
Strengths
The conceptual model developed in our study capture a broad system overview on factors and key stakeholders who can potentially influence the adoption of a biopsychosocial approach to musculoskeletal pain care. This cogwheel model reflects a whole-of-system approach and highlight opportunities for behavioural intervention designers and policymakers to target specific initiatives to promote and support and strengthen a system-wide approach to biopsychosocial musculoskeletal pain care. Developing the model from existing evidence-based behaviour change theoretical foundations (23, 24, 27, 31) is also a strength. Our method of conceptual model development is explicit and transparent, allowing readers to see clearly how data from our previous review (15) mapped to the COM-B model and TDF, and how these data are then translated back to the COM-B model to derive the new conceptual model (53). Our constructivist epistemological position towards knowledge construction and the hybrid approach of using both deductive and inductive analysis demonstrate theoretical rigor by accounting for sound and logical reasoning in the analysis process. We incorporated team members' subjective interpretation of the data from various experiential levels of the health system and ensured knowledge generated by this research is usable in real-world healthcare settings (37).
Limitations
The consensus reached in the team was driven by the knowledge and experience of a small group of clinicians and researchers working in musculoskeletal pain, the majority of whom are clinical and research physiotherapists (Table 1). Physiotherapists develop, maintain and restore maximum movement and functional ability in people and maximise their quality of life by looking at physical, psychological, emotional and social wellbeing, mainly using non-invasive, physical treatments or modalities such as exercises, manual therapy and education (54). High-value, biopsychosocial musculoskeletal pain care encompasses a mixture of conservative, non-invasive treatment methods, education, psychological therapies, pharmacological treatment and only in relevant cases, surgical treatment (55, 56). As such, the research team was unable to offer comprehensive representation of the views of all other healthcare professionals utilising assessment and treatment methods that were also evidence-based, when we came up with the recommendations to address the target behaviour during the inductive analysis at Step 5. The BCTs framework and worked example (see below) have been designed with the purpose of offering some proposed interventions with universal applicability across implementation contexts. However, the BCTs suggested are by no means exhaustive. This does not mean other BCTs are unimportant or ineffective, rather our selection of the BCTs is targeted at addressing the specified healthcare professionals' behaviours at the micro-level, and supporting these behaviours at the meso- and macro-level. We acknowledge the need to externally test and validate the conceptual model and synthesized framework of BCTs we have derived, to assess readiness to change, and to mindfully consider cultural factors influencing clinical community collaboration in different jurisdictions. We also speculate that the barriers to the adoption of a biopsychosocial approach may be “musculoskeletal pain”-agnostic, but since our search criterion for the initial review (15) is limited to musculoskeletal pain conditions, we could not generalise the findings beyond musculoskeletal pain.
Context is key in influencing healthcare professionals' behaviour towards improved adoption of a biopsychosocial approach to pain care
Data from our previous qualitative review (15) were found to support almost all the constructs in the COM-B model and TDF, with no data not fitting within the “a priori” framework. Consequently, no secondary thematic analysis was required in the “best fit” framework synthesis. It was worth highlighting that none of the coding undertaken in the meta-synthesis process for the previous review (15) was structured explicitly around concepts in the COM-B model and TDF. This implied that our chosen theory was sufficiently broad and a good fit to capture the data. In this current synthesis, the “best fit” method not only tested the theory, i.e., alignment with the COM-B model and TDF, but also supplemented the foundational theory of the COM-B model. The original COM-B model accorded equal value and importance to “capability”, “opportunity” and “motivation” as influencing behaviours (23). The focal point of our novel synthesized conceptual model was “opportunity” (also known as the “environmental context”), appearing as a key target in influencing, shaping and regulating healthcare professionals' behaviour towards improved adoption. Consistent with previous studies (16, 57), context was key in the acquisition of professional knowledge and clinical skills in the learning of the biopsychosocial approach to pain, and it could either enable or hinder learning and practice behaviours.
Rationale for the selection of BCTs at the micro-level
In order to improve healthcare professionals' pain education training, our findings suggest that we need to prioritize intervention efforts at “knowledge” and “cognitive and interpersonal skills” and target the micro-level (clinical interface). Review-level evidence indicates that existing healthcare professionals' communication skills training uses a combination of information (delivered in the form of written instructions, didactic lectures, on-line learning or clinical tools), verbal or video feedback, modelling, problem-based learning, and practice (58, 59). More broadly, Cochrane reviews have stated that interventions such as education meetings (60), as well as printed educational materials (61), when used alone or combined with other interventions, can be effective to improve healthcare professionals' practice behaviours, but with small effect sizes. Educational meetings alone do not necessarily translate to changing healthcare professionals' ingrained practice behaviour and improved patients' outcomes (17, 20). To increase effectiveness, considerations are therefore needed in the design of education to use interactive, combined with didactic formats (60). To improve the fidelity of education/training interventions, incorporating the following BCTs; “4.1 instruction on how to perform the behaviour”, and “8.1 behavioural practice/rehearsal” into training may be beneficial.
Rationale for the selection of BCTs at the meso- and macro-level
In order to adequately support pain education for healthcare professionals, our findings suggest a crucial need for targeted intervention efforts at the meso- (health services and workforce training) and macro-level (systems/policy), specifically for TDF domains “environmental context and resources” and “social influences”. Here, aligning implementation efforts of biopsychosocial pain care to the health services and system levels is paramount. As a first step, addressing how clinical communities and the lived environment is structured to modify or create new knowledge, clinical practice guidelines, health services and policy is key. Target levers to support implementation include: establishing strong multi-sectoral partnerships and advocacy across clinical communities, people with lived experience of pain, work and professional organisations, universities, funding and insurance agencies and governments. This can strengthen health systems to support high value musculoskeletal pain care (62). Examples of existing partnerships and collaboration may include: partnering with patient advocates from the Global Alliance of Partners for Pain Advocacy (GAPPA) task force (63) or people with lived experience of pain to create better outcomes in the understanding, research, teaching and management of musculoskeletal pain (64–66); partnering with consumer representatives from Cochrane musculoskeletal review group to develop meaningful and person-centred clinical practice guidelines (46); delivering biopsychosocial-informed education to promote improvements in insurance workers’ pain beliefs and helpful claims management behaviour (67); aligning country-level strategies to address the burden of pain to the newly developed global blueprint/framework for musculoskeletal health (68, 69). Additionally, as highlighted by our previous qualitative review (15), there is a critical need within health systems to support interdisciplinary or multidisciplinary care, especially for complex and chronic pain presentations. Appropriate funding or a reorientation of funding to develop models of care to deliver high value musculoskeletal pain care is required (68). There is an urgent need for governments, insurers, and health services to support and invest in high-value pain care, while concurrently disinvesting in low-value or no-value pain care (62). A change in the funding criterion and regulations within health systems for multidisciplinary services that aligns with and supports the use of a biopsychosocial approach will facilitate a change in the environmental context in which biopsychosocial pain care can be optimized. Hence, we incorporated the BCTs “3.1 Social support (unspecified)” and “3.2 Social support (practical)” into the synthesized framework because high value, biopsychosocial musculoskeletal pain care is the result of relationships, collaboration, coordination and authentic communication across the whole-of-health.
The availability of courses, and the re-design of curricula and capabilities/competencies across health disciplines is required to mobilise the knowledge and interpersonal skills required to support quality person-centred biopsychosocial musculoskeletal pain care. The design of value-add clinical systems learning roles as entrustable professional activities can enable healthcare students to learn tacit and contextualized knowledge. This could help bridge the gap between fulfilling a checklist of competencies and applying the knowledge and skills in dynamic, complex real-life situations (70). Here, the BCT “12.1 Restructuring the physical (learning) environment” is suggested.
Finally, the work spaces in which healthcare professionals practise is important. To implement behaviour change, introducing an environmental stimulus such as allocating a designated waiting room (with soundproof walls and a door), allows for a safe space for screening of psychosocial factors and can facilitate sensitive disclosure about patients' pain experience (64). The same contextual cues may help strengthen the context-behaviour association (71, 72) of the healthcare professional practising using a biopsychosocial approach in a safe space. Here, the BCT “7.1 Prompts/Cues” is suggested.
A worked example of how the derived framework of BCTs could be operationalised to improve adoption of biopsychosocial musculoskeletal pain care across the whole-of-health can be found in Supplementary Table S7. Supplementary Table S7 has specific examples on how to use our identified BCTs to target on healthcare professionals, educators, guideline developers, workplace managers and policymaker, in order to facilitate the implementation of biopsychosocial pain care.
Potential strategies to empower healthcare professionals to assess, identify and analyse biopsychosocial factors
Though not an explicit aim of the study to answer what “knowledge” and “cognitive and interpersonal skills” are needed, and how to empower healthcare professionals to assess, identify and analyse biopsychosocial factors, the team was able to map potential strategies from best-level evidence during the inductive analysis process to derive the framework of BCTs. These suggestions are by no means comprehensive in scope but may serve as useful insights to implementation interventionists.
Review-level evidence highlights that a strong therapeutic alliance underpinned by trust, rapport, an affective bond demonstrating emotional sensitivity to patients; patient-centred empathic communication; and agreement on tasks and treatment goals can affect pain outcomes and physical functioning (78–80). Specific to patient-centred communication, strategies such as asking open-ended questions, discussing options, encouraging questions, expressing empathy and providing reassurance, explaining and providing information (59, 79), and validating the disclosure of patients (81, 82) are all important. This means biopsychosocial musculoskeletal pain care involves establishing meaningful connections with patients, shared-decision making, and supportive self-management (64, 83, 84). This will require communication behaviours synonymous to health coaching and/or motivational interviewing to navigate and optimise the clinical consultation (64, 84).
The communication behaviour in health coaching closely aligns with a recently developed classification of motivation and behaviour change techniques (MBCTs) derived from self-determination theory (73). Of note, self-determination theory is not part of the 19 theories used to formulate the BCW (23, 24) and MBCTs belong to a different taxonomy (not part of BCTTv1) (73). MBCTs offer unique insights into the specific behaviour change techniques that respond to human primacy needs of autonomy, competence and relatedness (73). Especially in persistent pain or centrally maintained pain states, there are more than biological factors driving a human pain experience (85). Restoring health and well-being requires healthcare professionals to consider these needs. Using MBCTs as a tool, or as “instructions on how to perform the communication behaviour” may support and enable healthcare professionals to better assess biopsychosocial factors. Behavioural counselling skills can help enable persons with chronic musculoskeletal pain to make positive lifestyle changes and encourage adherence to self-management (77). Here, the use of MBCTs may help motivate health behaviour change in patients with musculoskeletal pain. See Supplementary Table S8 for list of MBCTs.
To empower healthcare professionals to learn to identify and analyse biopsychosocial factors, a focus of intervention might consider designing educational training programs. Here the aim would be to illustrate the multidimensional interacting biopsychosocial factors associated with musculoskeletal pain and identify how, for each person, these interacting factors create a unique multidimensional experience of pain. Our previous qualitative evidence synthesis highlighted that healthcare professionals, while aware of the importance of psychosocial factors, were unclear about what those specific factors were (15). While addressing biological factors remains important, a broader view that captures the impact of psychological and social dimensions, reflects the multidimensionality of each individual's unique pain experience. During the inductive analysis process, we developed a list of recommendations to address healthcare professionals' training (see Box 1 below). This list can be further strategized, contextualized and incorporated into training curricula to enhance healthcare professionals' understanding of the common psychosocial factors associated with musculoskeletal pain presentations.
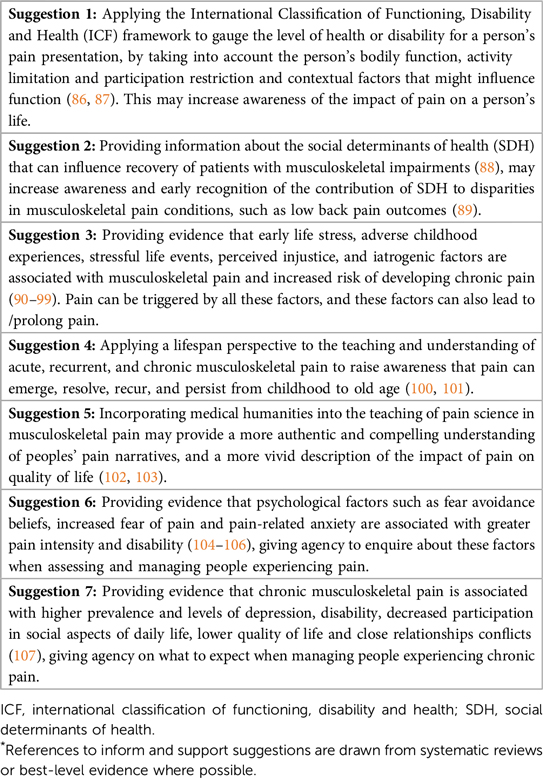
Box 1. A suggested list of evidence-informed strategies* to help promote and enhance healthcare professionals’ awareness of psychosocial factors associated with musculoskeletal pain.
Practicing biopsychosocial pain care requires healthcare professionals to believe their patients about their report of pain, i.e., validation is critical. From a person-centred frame, this involves doing what is right for each person (aligned to their priorities and goals) at the right time, and taking into account relevant biological factors, their psychological wellbeing and social and environmental circumstances. It is important to educate healthcare students' and health professionals to be listen carefully to each person's pain narrative/story and work in partnership to address various contextual life events within a person-centred evidence-based framework. This approach flips the lens towards the person rather than their condition. Such an inversion that is required of the healthcare professional is not easy but can be trained (64). Here, the focus becomes training healthcare professionals to empathise with their patients, to create more authentic communication and emotional connection that builds therapeutic alliance and supports recovery.
The biopsychosocial model of pain 40 years on: How this work improves what may be limiting implementation
Most research focus on improving the adoption of the biopsychosocial model at the micro-level, i.e., the clinical interface (11, 83, 84, 108). In this regard, we highlighted and proposed how the training of communication strategies and empathic listening (64, 81, 82) and insights from behavioural change techniques (31, 73) can help to enhance training efforts to support implementation and improve the quality of musculoskeletal pain care. At the meso- and macro-level, contextual factors and the interdependencies between various stakeholder groups in the whole-of-health within modern healthcare systems have not been adequately addressed and have not been addressed well in health systems strengthening strategies (68, 109). This may be one key to limiting effective implementation. Our work gives a refreshing whole-of-health perspective to a more-than-four-decade old biopsychosocial model of pain care.
Implications for research and practice
Further research and road testing is required to check the validity, credibility and transferability of our derived BCT framework, including through relevant stakeholder engagement or an interdisciplinary partnership model. In this context, the evaluation of contemporary musculoskeletal models of care and policy-into-practice initiatives that incorporate a biopsychosocial approach, will be useful (109–112).
Conclusion
From a behavioural perspective, implementation of a biopsychosocial approach to musculoskeletal pain care is a highly complex task. We have derived a conceptual model and a framework of BCTs to support future implementation efforts. Other than healthcare professionals, this requires a system-wide initiative from multi-stakeholders such as educators, to workplace managers and non-medical professions involved in healthcare (e.g., insurance workers, vocational rehabilitation providers), to guideline developers and policymakers. At the micro-level, prioritizing intervention efforts aimed at educational upskilling in a biopsychosocial approach, critical clinical reasoning and effective communication behaviours to strengthen therapeutic alliance are proposed. At the meso- and macro-level, encouraging multi-sectoral partnerships across the whole-of-health, increasing the availability of health workforce pain training programs and the re-design of curricula to strengthen interdisciplinary pain competency are crucial.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s. The data analyzed in this study was obtained from https://journals.lww.com/pain/Abstract/2021/08000/Barriers_and_enablers_influencing_healthcare.2.aspx, the following licenses/restrictions apply [Copyright © 2021 International Association for the Study of Pain]. Requests to access these datasets should be directed to PAIN or Wendy Ng,dy5uZzIxQHBvc3RncmFkLmN1cnRpbi5lZHUuYXU=.
Author contributions
WN conceived and designed the study, mapped the data, collated the results at every step of the BCW process, conducted the analysis, interpreted the data, formulated the conceptual model and framework of BCTs, participated in discussions and drafted the manuscript. HS participated in research team discussions as an independent team member/subject matter expert not privy to the BCW process, and contributed to interpretation of primary data, discussions and conceptual framing of the study outcomes, drafting and revising the manuscript. DB and DFG contributed to the initial conception of the study design and data mapping, participated in group discussions, advised as subject matter experts, interpreted the results, and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
WN is supported by an Australian Government Research Training Program Scholarship for her PhD studies. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
WN will like to acknowledge and express her deepest thanks to Rena Sivadas for her support, invaluable insights on healing chronic pain from a psychotherapeutic perspective and the discussion on humanistic psychology. WN will also like to thank Adele Ang, a musculoskeletal physiotherapist skilled in health coaching, motivational interviewing and Acceptance and Commitment Therapy, for the collegial conversations on how physiotherapists (or non-psychologists) can change and adapt clinical communication to treat persons with chronic pain.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2023.1169178/full#supplementary-material.
Abbreviations
APEASE, affordability, practicability, effectiveness/cost-effectiveness, acceptability, side-effects/safety, equity; BCTs, behaviour change techniques; BCTTv1, behaviour change techniques taxonomy version 1; BCW, behavioural change wheel; BPS, biopsychosocial; COM-B, capability opportunity motivation-behaviour model; CPGs, clinical practice guidelines; DASS-21, depression, anxiety and stress scale; ePPOC, electronic persistent pain outcomes collaboration; GAPPA, global alliance of partners for pain advocacy; IASP, international association of the study of pain; ICF, international classification of functioning, disability and health; MBCTs, motivation and behaviour change techniques; ÖMPQ, örebro musculoskeletal pain questionnaire; SDH, social determinants of health; TaTT, theory and technique tool; TDF: theoretical domains framework.
References
1. Engel G. The need for a new medical model: a challenge for biomedicine. Science. (1977) 196(4286):129–36. doi: 10.1126/science.847460
2. Wade DT, Halligan PW. The biopsychosocial model of illness: a model whose time has come. Clin Rehabil. (2017) 31(8):995–1004. doi: 10.1177/0269215517709890
3. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. (2021) 397(10289):2082–97. doi: 10.1016/S0140-6736(21)00393-7
4. Clark S, Horton R. Low back pain: a major global challenge. Lancet. (2018) 391(10137):2302. doi: 10.1016/S0140-6736(18)30725-6
5. Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. (2018) 391(10137):2356–67. doi: 10.1016/S0140-6736(18)30480-X
6. Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. (2018) 391(10137):2368–83. doi: 10.1016/S0140-6736(18)30489-6
7. Buchbinder R, van Tulder M, Öberg B, Costa LM, Woolf A, Schoene M, et al. Low back pain: a call for action. Lancet. (2018) 391(10137):2384–8. doi: 10.1016/S0140-6736(18)30488-4
8. Fitzcharles M-A, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet. (2021) 397(10289):2098–110. doi: 10.1016/S0140-6736(21)00392-5
9. Knotkova H, Hamani C, Sivanesan E, Le Beuffe MFE, Moon JY, Cohen SP, et al. Neuromodulation for chronic pain. Lancet. (2021) 397(10289):2111–24. doi: 10.1016/S0140-6736(21)00794-7
10. Lancet T. Rethinking chronic pain. Lancet. (2021) 397(10289):2023. doi: 10.1016/S0140-6736(21)01194-6
11. Jull G. Biopsychosocial model of disease: 40 years on. Which way is the pendulum swinging? Br J Sports Med. (2017) 51(16):1187–8. doi: 10.1136/bjsports-2016-097362
12. Nicholas MK. The biopsychosocial model of pain 40 years on: time for a reappraisal? Pain. (2022):163(S1):S3–S14. doi: 10.1097/j.pain.0000000000002654
13. Pourbordbari N, Riis A, Jensen MB, Olesen JL, Rathleff MS. Poor prognosis of child and adolescent musculoskeletal pain: a systematic literature review. BMJ Open. (2019) 9(7):e024921. doi: 10.1136/bmjopen-2018-024921
14. Duffield SJ, Ellis BM, Goodson N, Walker-Bone K, Conaghan PG, Margham T, et al. The contribution of musculoskeletal disorders in multimorbidity: implications for practice and policy. Best Pract Res Clin Rheumatol. (2017) 31(2):129–44. doi: 10.1016/j.berh.2017.09.004
15. Ng W, Slater H, Starcevich C, Wright A, Mitchell T, Beales D. Barriers and enablers influencing healthcare professionals’ adoption of a biopsychosocial approach to musculoskeletal pain: a systematic review and qualitative evidence synthesis. Pain. (2021) 162(8):2154–85. doi: 10.1097/J.PAIN.0000000000002217
16. Holopainen R, Simpson P, Piirainen A, Karppinen J, Schütze R, Smith A, et al. Physiotherapists’ perceptions of learning and implementing a biopsychosocial intervention to treat musculoskeletal pain conditions: a systematic review and metasynthesis of qualitative studies. Pain. (2020) 161(6):1150–68. doi: 10.1097/j.pain.0000000000001809
17. Bérubé M-È, Poitras S, Bastien M, Laliberté L-A, Lacharité A, Gross DP. Strategies to translate knowledge related to common musculoskeletal conditions into physiotherapy practice: a systematic review. Physiotherapy. (2018) 104(1):1–8. doi: 10.1016/j.physio.2017.05.002
18. Mesner SA, Foster NE, French SD. Implementation interventions to improve the management of non-specific low back pain: a systematic review. BMC Musculoskelet Disord. (2016) 17(1):258. doi: 10.1186/s12891-016-1110-z
19. Suman A, Dikkers MF, Schaafsma FG, van Tulder MW, Anema JR. Effectiveness of multifaceted implementation strategies for the implementation of back and neck pain guidelines in health care: a systematic review. Implement Sci. (2015) 11(1):126. doi: 10.1186/s13012-016-0482-7
20. Zoubi FMA, Menon A, Mayo NE, Bussières AE. The effectiveness of interventions designed to increase the uptake of clinical practice guidelines and best practices among musculoskeletal professionals: a systematic review. BMC Health Serv Res. (2018) 18(1):435. doi: 10.1186/s12913-018-3253-0
21. Overmeer T, Boersma K, Denison E, Linton SJ. Does teaching physical therapists to deliver a biopsychosocial treatment program result in better patient outcomes? A randomized controlled trial. Phys Ther. (2011) 91(5):804–19. doi: 10.2522/ptj.20100079
22. World Health Organization Technical Advisory Group. Technical note from the WHO Technical Advisory Group on behavioural insights and science for health (2022). Available at: https://www.who.int/publications/m/item/technical-note-from-the-who-technical-advisory-group-on-behavioural-insights-and-science-for-health (Cited October 17, 2022).
23. Michie S, Atkins L, West R. The behaviour change wheel: A guide to designing interventions. Great Britain: Silverback Publishing (2014).
24. Michie S, Van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. (2011) 6(1):42. doi: 10.1186/1748-5908-6-42
25. Atkins L, Francis J, Islam R, O’Connor D, Patey A, Ivers N, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. (2017) 12(1):77. doi: 10.1186/s13012-017-0605-9
26. Gervais-Hupé J, Filleul A, Perreault K, Hudon A. Implementation of a biopsychosocial approach into physiotherapists’ practice: a review of systematic reviews to map barriers and facilitators and identify specific behavior change techniques. Disabil Rehabil. (2022):1–10. doi: 10.1080/09638288.2022.2094479. [Epub ahead of print]
27. French SD, Green SE, O’Connor DA, McKenzie JE, Francis JJ, Michie S, et al. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the theoretical domains framework. Implement Sci. (2012) 7(1):38. doi: 10.1186/1748-5908-7-38
28. Egerton T, Nelligan RK, Setchell J, Atkins L, Bennell KL. General practitioners’ views on managing knee osteoarthritis: a thematic analysis of factors influencing clinical practice guideline implementation in primary care. BMC Rheumatol. (2018) 2(1):1–11. doi: 10.1186/s41927-018-0037-4
29. Bussières AE, Al Zoubi F, Quon JA, Ahmed S, Thomas A, Stuber K, et al. Fast tracking the design of theory-based KT interventions through a consensus process. Implement Sci. (2015) 10(1):18. doi: 10.1186/s13012-015-0213-5
30. Saunders B, Hill JC, Foster NE, Cooper V, Protheroe J, Chudyk A, et al. Stratified primary care versus non-stratified care for musculoskeletal pain: qualitative findings from the STarT MSK feasibility and pilot cluster randomized controlled trial. BMC Fam Pract. (2020) 21(1):31. doi: 10.1186/s12875-020-1098-1
31. Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. (2013) 46:81–95. doi: 10.1007/s12160-013-9486-6
32. Schielke HJ, Fishman JL, Osatuke K, Stiles WB. Creative consensus on interpretations of qualitative data: the ward method. Psychother Res. (2009) 19(4–5):558–65. doi: 10.1080/10503300802621180
33. Charmaz K. The power of constructivist grounded theory for critical inquiry. Qual Inq. (2017) 23(1):34–45. doi: 10.1177/1077800416657105
34. Carroll C, Booth A, Cooper K. A worked example of “best fit” framework synthesis: a systematic review of views concerning the taking of some potential chemopreventive agents. BMC Med Res Methodol. (2011) 11(1):29. doi: 10.1186/1471-2288-11-29
35. Carroll C, Booth A, Leaviss J, Rick J. “Best fit” framework synthesis: refining the method. BMC Med Res Methodol. (2013) 13(1):37. doi: 10.1186/1471-2288-13-37
36. Dixon-Woods M. Using framework-based synthesis for conducting reviews of qualitative studies. BMC Med. (2011) 9(1):39. doi: 10.1186/1741-7015-9-39
37. Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. (2006) 5(1):80–92. doi: 10.1177/160940690600500107
38. Bonner C, Tuckerman J, Kaufman J, Costa D, Durrheim DN, Trevena L, et al. Comparing inductive and deductive analysis techniques to understand health service implementation problems: a case study of childhood vaccination barriers. Implement Sci Commun. (2021) 2(1):100. doi: 10.1186/s43058-021-00202-0
39. Johnston M, Carey RN, Connell Bohlen LE, Johnston DW, Rothman AJ, de Bruin M, et al. Development of an online tool for linking behavior change techniques and mechanisms of action based on triangulation of findings from literature synthesis and expert consensus. Transl Behav Med. (2021) 11(5):1049–65. doi: 10.1093/tbm/ibaa050
40. Theory and Technique Tool. (2022). Available at: https://theoryandtechniquetool.humanbehaviourchange.org (Cited September 20, 2022).
41. Carey RN, Connell LE, Johnston M, Rothman AJ, Bruin M, Kelly MP, et al. Behavior change techniques and their mechanisms of action: a synthesis of links described in published intervention literature. Ann Behav Med. (2019) 53(8):693–707. doi: 10.1093/abm/kay078
42. Connell LE, Carey RN, Md B, Rothman AJ, Johnston M, Kelly MP, et al. Links between behavior change techniques and mechanisms of action: an expert consensus study. Ann Behav Med. (2019) 53(8):708–20. doi: 10.1093/abm/kay082
43. Abraham C, Wood CE, Johnston M, Francis J, Hardeman W, Richardson M, et al. Reliability of identification of behavior change techniques in intervention descriptions. Ann Behav Med. (2015) 49(6):885–900. doi: 10.1007/s12160-015-9727-y
44. University of New Mexico School of Medicine. Project ECHO (2022). Available at https://hsc.unm.edu/echo/ (Cited October 17, 2022).
45. University Of Wollongong Australia. Electronic persistent pain outcomes collaboration (2022). Available at: https://www.uow.edu.au/ahsri/eppoc/ (Cited October, 2022).
46. Cochrane. Cochrane Musculoskeletal (2022). Available at: https://musculoskeletal.cochrane.org (Cited October 17, 2022).
47. IASP. International Association for the Study of Pain (2022). Available ar: https://www.iasp-pain.org (Cited October 17, 2022).
48. Presseau J, Johnston M, Heponiemi T, Elovainio M, Francis JJ, Eccles MP, et al. Reflective and automatic processes in health care professional behaviour: a dual process model tested across multiple behaviours. Ann Behav Med. (2014) 48(3):347–58. doi: 10.1007/s12160-014-9609-8
49. Gardner B, Tang V. Reflecting on non-reflective action: an exploratory think-aloud study of self-report habit measures. Br J Health Psychol. (2014) 19(2):258–73. doi: 10.1111/bjhp.12060
50. Plsek PE, Greenhalgh T. The challenge of complexity in health care. Br Med J. (2001) 323(7313):625–8. doi: 10.1136/bmj.323.7313.625
51. Smith RC. The biopsychosocial revolution. J Gen Intern Med. (2002) 17(4):309–10. doi: 10.1046/j.1525-1497.2002.20210.x
52. Inui TS. What are the sciences of relationship-centered primary care? J Fam Pract. (1996) 42(2):171–7. PMID: 8606307
53. Brunton G, Oliver S, Thomas J. Innovations in framework synthesis as a systematic review method. Res Synth Methods. (2020) 11(3):316–30. doi: 10.1002/jrsm.1399
54. World Physiotherapy (2023). Available at: https://world.physio/resources/what-is-physiotherapy (Cited April 20, 2023).
55. Lin I, Wiles L, Waller R, Caneiro JP, Nagree Y, Straker L, et al. Patient-centred care: the cornerstone for high-value musculoskeletal pain management. Br J Sports Med. (2020) 54(21):1240–2. doi: 10.1136/bjsports-2019-101918
56. Lin I, Wiles L, Waller R, Goucke R, Nagree Y, Gibberd M, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. (2020) 54:79–86. doi: 10.1136/bjsports-2018-099878
57. Simpson P, Holopainen R, Schütze R, O'Sullivan P, Smith A, Linton SJ, et al. Training of physical therapists to deliver individualized biopsychosocial interventions to treat musculoskeletal pain conditions: a scoping review. Phys Ther. (2021) 101(10):1–12. doi: 10.1093/ptj/pzab188
58. Muddle L, O'Malley CJ, Stupans I. Learning and teaching of patient-centred communication skills in allied healthcare manual therapy students: a systematic review. Int J Osteopath Med. (2019) 32:21–7. doi: 10.1016/j.ijosm.2019.04.002
59. Rao JK, Anderson LA, Inui TS, Frankel RM. Communication interventions make a difference in conversations between physicians and patients: a systematic review of the evidence. Med Care. (2007) 45(4):340–9. doi: 10.1097/01.mlr.0000254516.04961.d5
60. Forsetlund L, Bjørndal A, Rashidian A, Jamtvedt G, O'Brien MA, Wolf FM, et al. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. (2009) 2009(2):CD003030. doi: 10.1002/14651858.CD003030.pub2
61. Giguère A, Zomahoun HTV, Carmichael P-H, Uwizeye CB, Légaré F, Grimshaw JM, et al. Printed educational materials: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. (2020) 8(8):CD004398. doi: 10.1002/14651858.CD004398.pub4
62. Briggs AM, Slater H, Hsieh E, Kopansky-Giles D, Åkesson KE, Dreinhöfer KE, et al. System strengthening to support value-based care and healthy ageing for people with chronic pain. Pain. (2019) 160(6):1240–4. doi: 10.1097/j.pain.0000000000001526
63. IASP. Global Alliance of Partners for Pain Advocacy (GAPPA) Task Force (2022). Available at: https://www.iasp-pain.org/group/global-alliance-of-partners-for-pain-advocacy-gappa-task-force/m (Cited September 9, 2022).
64. Slater H, Jordan JE, O'Sullivan PB, Schütze R, Goucke R, Chua J, Browne A, Horgan B, De Morgan S, Briggs AM. ‘Listen to me, learn from me': a priority setting partnership for shaping interdisciplinary pain training to strengthen chronic pain care. Pain. (2022) 163(11):e1145–63. doi: 10.1097/j.pain.0000000000002647
65. Partnering for Pain. Shaping pain research and care for kids, together (2022). Available at: https://partneringforpain.com (Cited September 9, 2022).
66. Belton JL, Slater H, Ravindran TS, Briggs AM. Harnessing people’s lived experience to strengthen health systems and support equitable musculoskeletal health care. J Orthop Sports Phys Ther. (2023) 53(4):162–71. doi: 10.2519/jospt.2022.11427
67. Beales D, Mitchell T, Pole N, Weir J. Brief biopsychosocially informed education can improve insurance workers’ back pain beliefs: implications for improving claims management behaviours. Work. (2016) 55(3):625–33. doi: 10.3233/WOR-162428
68. Briggs AM, Huckel Schneider C, Slater H, Jordan JE, Parambath S, Young JJ, et al. Health systems strengthening to arrest the global disability burden: empirical development of prioritised components for a global strategy for improving musculoskeletal health. BMJ Glob Health. (2021) 6(6):e006045. doi: 10.1136/bmjgh-2021-006045
69. Briggs AM, Jordan JE, Sharma S, Young JJ, Chua J, Foster HE, et al. Context and priorities for health systems strengthening for pain and disability in low- and middle-income countries: a secondary qualitative study and content analysis of health policies. Health Policy Plan. (2022) 38(2):129–49. doi: 10.1093/heapol/czac061
70. Gonzalo JD, Thompson BM, Haidet P, Mann K, Wolpaw DR. A constructive reframing of student roles and systems learning in medical education using a communities of practice lens. Acad Med. (2017) 92(12):1687–94. doi: 10.1097/ACM.0000000000001778
71. Gardner B, Lally P, Wardle J. Making health habitual: the psychology of ‘habit-formation’ and general practice. Br J Gen Pract. (2012) 62(605):664–6. doi: 10.3399/bjgp12X659466
72. Nilsen P, Roback K, Broström A, Ellström P-E. Creatures of habit: accounting for the role of habit in implementation research on clinical behaviour change. Implement Sci. (2012) 7(1):53. doi: 10.1186/1748-5908-7-53
73. Teixeira PJ, Marques MM, Silva MN, Brunet J, Duda JL, Haerens L, et al. A classification of motivation and behavior change techniques used in self-determination theory-based interventions in health contexts. Motiv Sci. (2020) 6(4):438–55. doi: 10.1037/mot0000172
74. Ernstzen DV, Louw QA, Hillier SL. Clinical practice guidelines for the management of chronic musculoskeletal pain in primary healthcare: a systematic review. Implement Sci. (2017) 12(1):1. doi: 10.1186/s13012-016-0533-0
75. Hockings RL, McAuley JH, Maher CG. A systematic review of the predictive ability of the orebro musculoskeletal pain questionnaire. Spine. (2008) 33(15):E494–E500. doi: 10.1097/BRS.0b013e31817ba3bb
76. Henry JD, Crawford JR. The short-form version of the depression anxiety stress scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. (2005) 44(2):227–39. doi: 10.1348/014466505X29657
77. Martin ES, Dobson F, Hall M, Marshall C, Egerton T. The effects of behavioural counselling on the determinants of health behaviour change in adults with chronic musculoskeletal conditions making lifestyle changes: a systematic review and meta-analysis. Musculoskelet Care. (2019) 17(3):170–97. doi: 10.1002/msc.1410
78. Kinney M, Seider J, Beaty AF, Coughlin K, Dyal M, Clewley D. The impact of therapeutic alliance in physical therapy for chronic musculoskeletal pain: a systematic review of the literature. Physiother Theory Pract. (2020) 36(8):886–98. doi: 10.1080/09593985.2018.1516015
79. Pinto RZ, Ferreira ML, Oliveira VC, Franco MR, Adams R, Maher CG, et al. Patient-centred communication is associated with positive therapeutic alliance: a systematic review. J Physiother. (2012) 58(2):77–87. doi: 10.1016/S1836-9553(12)70087-5
80. Jorna-Lakke S, Meerman S. Does working alliance have an influence on pain and physical functioning in patients with chronic musculoskeletal pain; a systematic review. J Compassionate Health Care. (2016) 3(1):1–10. doi: 10.1186/s40639-016-0018-7
81. Cowell I, McGregor A, O’Sullivan P, O’Sullivan K, Poyton R, Schoeb V, et al. Physiotherapists’ approaches to patients’ concerns in back pain consultations following a psychologically informed training program. Qual Health Res. (2021) 31(13):2486–501. doi: 10.1177/10497323211037651
82. Holopainen R, Lausmaa M, Edlund S, Carstens-Söderstrand J, Karppinen J, O'Sullivan P, et al. Physiotherapists’ validating and invalidating communication before and after participating in brief cognitive functional therapy training. Test of concept study. Eur J Physiother. (2023) 25(2):73–9. doi: 10.1080/21679169.2021.1967446
83. Hutting N, Caneiro JP, Ong'wen OM, Miciak M, Roberts L. Patient-centered care in musculoskeletal practice: key elements to support clinicians to focus on the person. Musculoskelet Sci Pract. (2022) 57(2022):102434. doi: 10.1016/j.msksp.2021.102434:102434
84. Hutting N, Caneiro J, Ong'wen OM, Miciak M, Roberts L. Person-centered care for musculoskeletal pain: putting principles into practice. Musculoskelet Sci Pract. (2022) 62(2022):102663. doi: 10.1016/j.msksp.2022.102663
85. Loeser JD. A new way of thinking about pains. Pain. (2022) 163(9):1670–4. doi: 10.1097/j.pain.0000000000002583
86. Üstun TB, Chatterji S, Bickenbach J, Kostanjsek N, Schneider M. The international classification of functioning, disability and health: a new tool for understanding disability and health. Disabil Rehabil. (2003) 25(11–12):565–71. doi: 10.1080/0963828031000137063
87. Imrie R. Demystifying disability: a review of the international classification of functioning, disability and health. Sociol Health Illn. (2004) 26(3):287–305. doi: 10.1111/j.1467-9566.2004.00391.x
88. Rethorn ZD, Cook C, Reneker JC. Social determinants of health: if you aren't measuring them, you aren't seeing the big picture. J Orthop Sports Phys Ther. (2019) 49(12):872–4. doi: 10.2519/jospt.2019.0613
89. Karran EL, Grant AR, Moseley GL. Low back pain and the social determinants of health: a systematic review and narrative synthesis. Pain. (2020) 161(11):2476–93. doi: 10.1097/j.pain.0000000000001944
90. Craner JR, Lake ES. Adverse childhood experiences and chronic pain rehabilitation treatment outcomes in adults. Clin J Pain. (2021) 37(5):321–9. doi: 10.1097/AJP.0000000000000924
91. Nelson S, Simons LE, Logan D. The incidence of adverse childhood experiences (ACEs) and their association with pain-related and psychosocial impairment in youth with chronic pain. Clin J Pain. (2018) 34(5):402–8. doi: 10.1097/AJP.0000000000000549
92. Petruccelli K, Davis J, Berman T. Adverse childhood experiences and associated health outcomes: a systematic review and meta-analysis. Child Abuse Negl. (2019) 97:104127. doi: 10.1016/j.chiabu.2019.104127
93. Häuser W, Kosseva M, Üceyler N, Klose P, Sommer C. Emotional, physical, and sexual abuse in fibromyalgia syndrome: a systematic review with meta-analysis. Arthritis Care Res (Hoboken). (2011) 63(6):808–20. doi: 10.1002/acr.20328
94. Beerthuizen A, van ‘t Spijker A, Huygen FJPM, Klein J, de Wit R. Is there an association between psychological factors and the complex regional pain syndrome type 1 (CRPS1) in adults? A systematic review. Pain. (2009) 145(1–2):52–9. doi: 10.1016/j.pain.2009.05.003
95. Buscemi V, Chang W-J, Liston MB, McAuley JH, Schabrun SM. The role of perceived stress and life stressors in the development of chronic musculoskeletal pain disorders: a systematic review. J Pain. (2019) 20(10):1127–39. doi: 10.1016/j.jpain.2019.02.008
96. Carriere JS, Donayre Pimentel S, Yakobov E, Edwards RR. A systematic review of the association between perceived injustice and pain-related outcomes in individuals with musculoskeletal pain. Pain Med. (2020) 21(7):1449–63. doi: 10.1093/pm/pnaa088
97. Williams CM, Kamper SJ. A broader perspective of musculoskeletal conditions in children. J Orthop Sports Phys Ther. (2017) 47(10):699–701. doi: 10.2519/jospt.2017.0108
98. van Rijswijk SM, van Beek MHCT, Schoof GM, Schene AH, Steegers M, Schellekens AF. Iatrogenic opioid use disorder, chronic pain and psychiatric comorbidity: a systematic review. Gen Hosp Psychiatry. (2019) 59:37–50. doi: 10.1016/j.genhosppsych.2019.04.008
99. Kouyanou K, Pither CE, Wessely S. Iatrogenic factors and chronic pain. Psychosom Med. (1997) 59(6):597–604. doi: 10.1097/00006842-199711000-00007
100. Walco GA, Krane EJ, Schmader KE, Weiner DK. Applying a lifespan developmental perspective to chronic pain: pediatrics to geriatrics. J Pain. (2016) 17(9):T108–17. doi: 10.1016/j.jpain.2015.11.003
101. Dario AB, Kamper SJ, O'Keeffe M, Zadro J, Lee H, Wolfenden L, et al. Family history of pain and risk of musculoskeletal pain in children and adolescents: a systematic review and meta-analysis. Pain. (2019) 160(11):2430–9. doi: 10.1097/j.pain.0000000000001639
102. Macnaughton J. Medical humanities’ challenge to medicine: medical humanities’ challenge. J Eval Clin Pract. (2011) 17(5):927–32. doi: 10.1111/j.1365-2753.2011.01728.x
103. Ousager J, Johannessen H. Humanities in undergraduate medical education: a literature review. Acad Med. (2010) 85(6):988–98. doi: 10.1097/ACM.0b013e3181dd226b
104. Wertli MM, Rasmussen-Barr E, Held U, Weiser S, Bachmann LM, Brunner F. Fear-avoidance beliefs—a moderator of treatment efficacy in patients with low back pain: a systematic review. Spine J. (2014) 14(11):2658–78. doi: 10.1016/j.spinee.2014.02.033
105. Wertli MM, Rasmussen-Barr E, Weiser S, Bachmann LM, Brunner F. The role of fear avoidance beliefs as a prognostic factor for outcome in patients with nonspecific low back pain: a systematic review. Spine J. (2014) 14(5):816–36. doi: 10.1016/j.spinee.2013.09.036
106. Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, Luque-Suarez A. Pain-related fear, pain intensity and function in individuals with chronic musculoskeletal pain: a systematic review and meta-analysis. J Pain. (2019) 20(12):1394–415. doi: 10.1016/j.jpain.2019.04.009
107. Andersen LN, Kohberg M, Juul-Kristensen B, Herborg LG, Søgaard K, Roessler KK. Psychosocial aspects of everyday life with chronic musculoskeletal pain: a systematic review. Scand J Pain. (2014) 5(2):131–48. doi: 10.1016/j.sjpain.2014.01.001
108. Cormack B, Stilwell P, Coninx S, Gibson J. The biopsychosocial model is lost in translation: from misrepresentation to an enactive modernization. Physiother Theory Pract. (2022):1–16. doi: 10.1080/09593985.2022.2080130. [Epub ahead of print]35645164
109. Briggs AM, Jordan JE, Kopansky-Giles D, Sharma S, March L, Schneider CH, et al. The need for adaptable global guidance in health systems strengthening for musculoskeletal health: a qualitative study of international key informants. Glob Health Res Policy. (2021) 6(24):1–22. doi: 10.1186/s41256-021-00201-7
110. Briggs AM, Bragge P, Slater H, Chan M, Towler SC. Applying a health network approach to translate evidence-informed policy into practice: a review and case study on musculoskeletal health. BMC Health Serv Res. (2012) 12(394):1–12. doi: 10.1186/1472-6963-12-394
111. Briggs AM, Chan M, Slater H. Models of care for musculoskeletal health: moving towards meaningful implementation and evaluation across conditions and care settings. Best Pract Res Clin Rheumatol. (2016) 30(3):359–74. doi: 10.1016/j.berh.2016.09.009
Keywords: biopsychosocial, behaviour change techniques, behaviour change techniques taxonomy version 1, capability opportunity motivation-Behaviour, healthcare professionals, musculoskeletal pain, theoretical domains framework
Citation: Ng W, Beales D, Gucciardi DF and Slater H (2023) Applying the behavioural change wheel to guide the implementation of a biopsychosocial approach to musculoskeletal pain care. Front. Pain Res. 4:1169178. doi: 10.3389/fpain.2023.1169178
Received: 28 February 2023; Accepted: 21 April 2023;
Published: 9 May 2023.
Edited by:
Mark I. Johnson, Leeds Beckett University, United KingdomReviewed by:
Anne Thackeray, The University of Utah, United StatesCarol Vance, The University of Iowa, United States
© 2023 Ng, Beales, Gucciardi and Slater. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wendy Ng dy5uZzIxQHBvc3RncmFkLmN1cnRpbi5lZHUuYXU=