 Fabien Beaufils
Fabien Beaufils Aiham Ghazali4,5
Aiham Ghazali4,5 Bettyna Boudier
Bettyna Boudier- 1Univ-Bordeaux, Centre de Recherche Cardio-thoracique de Bordeaux, Département de Pharmacologie, CIC 1401, Bordeaux, France
- 2INSERM, Centre de Recherche Cardio-thoracique de Bordeaux, U1045, CIC 1401, Bordeaux, France
- 3CHU de Bordeaux, Service d'Exploration Fonctionnelle Respiratoire, Service de Pharmacologie, CIC 1401, Pessac, France
- 4ABS Lab, Simulation Center, Faculty of Medicine, University of Poitiers, Poitiers, France
- 5Emergency Department and Emergency Medical Service, University Hospital of Bichat, Paris, France
- 6Early Childhood Department of the Cityhall Social Action Center of Poitiers, Poitiers, France
- 7Pediatric Emergency Department, University Hospital of Poitiers, Poitiers, France
Background: Child cardiac arrest is rare, but more frequent among infants, requiring immediate cardiopulmonary resuscitation (CPR). Many studies have reported that simulation-based training (SBT) increased CPR performance of healthcare providers. However, the CPR performance of laypeople using basic life support remains poorly known. The aim of this study was to assess nursery assistants' (non-healthcare providers) CPR performance and knowledge, before and after SBT.
Methods: The study was carried out from January to June 2018 in the city of Poitiers, France. Two teaching sessions (T1 and T2) and two evaluation sessions (E1 and E2) were performed. Performance in infant CPR on a manikin at E1 and E2 were videotaped and assessed automatically with Resusci Baby QCPR® and a SimPad PLUS SkillReporter (QCPR Global Score and skills) and by an observer using an original CPR performance checklist (MCPR Global-Score and skills). Nursery assistant's CPR knowledge was assessed by a questionnaire at the beginning and the end of the session T1, E1, and E2.
Results: Twenty-Seven nursery assistants over 30 contacted were included. There was an improvement between E1 and E2 in QCPR Global-Score (E1: 42.4 ± 23.6 vs. E2: 55.1 ± 23.7%, p = 0.032), MCPR Global-Score (E1: 50.0+11.9 vs. E2: 72.3+8.5%; p < 0.001) and theoretical knowledge with score (over 45) of 16.9+5.4 before T1 and 35.2+2.7 after E2, respectively (p < 0.001). The improvement mainly concerned QCPR and MCPR compression steps scores. MCPR Global-Score was strongly correlated to QCPR Global-Score (r = 0.61; p < 0.01) and predictive to CPR quality determined by QCPR Global-Score (AUC = 0.77; p < 0.01) with a high sensitivity and negative predictive values. Moreover, these improvements were maintained 2 months after training with no difference between scores obtained by the three groups 15, 30, or 60 days after simulation-based training session T2.
Conclusion: SBT could significantly improve knowledge and skills in infant CPR management by nursery assistants especially for chest compression. CPR performance checklist appeared as an interesting tool to assess CPR performance quality.
Introduction
Pediatric prehospital cardiac arrest are rare, with an overall incidence of 8 to 10 per 100,000 persons (1–3) but occurs mostly non-public location such as the residence (96% for infants) (4). The survival is low by about 10% (5). Survival can be improved by quality cardiopulmonary resuscitation (CPR) performed immediately (3, 6, 7). However, CPR performed by laypeople is regularly suboptimal (8, 9), initiated in only half of OHCA (10) and more frequently when bystanders were previously trained in CPR (10).
To improve quality CPR of rescuers, the use of simulation-based training (SBT) increased these last years and has proven its efficiency to improve CPR skills and maintain them over time (11–13). Moreover, development of specific devices (QCPR devices) on the top of manikins (14–16) coupled with SBT allowed to easily and objectively assess CPR quality, giving details on CPR performance. However, these devices and most of the interventions trying to improve CPR performance with SBT focused on healthcare providers but not on laypeople (17, 18) while they could represent the first possible rescuers in OHCA.
Because infant OHCA are more frequent than in children (1), occur more frequently at home and have a lower survival rate than in adults (19), in France, an initial CPR training including infant CPR is mandatory for nursery assistants certification (20) and then regular CPR training is recommended. However, effectiveness of CPR training to improve infant CPR performed by nursery assistant has not been regularly assessed. While previous study had demonstrated that after traditional basic life support courses, skills retention gradually decreased (21) and that could contribute to the low rate of survival after OHCA (22).
We hypothesized that SBT with mastery training would increase infant CPR performance of nursery assistants.
The aim of this study was to assess infant CPR performance among a population of nursery assistants working alone at home, before and after mastery training including didactics and SBT. The primary objective was to improve nursery assistants' infant CPR performance quality. Secondary objectives were: (1) To assess CPR specific steps quality; (2) To measure theoretical test scores at different times of the study; (3) To compare theoretical scores to CPR performance scores; (4) To assess maintaining of skills and knowledge over time.
Methods
Population
This monocentric prospective pilot study with assessment before and after intervention took place in Poitiers, France, from January to June 2018 and involved nursery assistant (NA), managed by the “Early Childhood department” of the City hall of Poitiers, working alone at home. After the agreement of the “Early childhood department,” the 30 nursery assistants were contacted for the study. Inclusion criteria were: being a certified NA (involving previous participation in certified CPR training), having participated in CPR training within the last 2 years and giving a written informed consent to participate. Participants who did not completed all the study procedure were excluded. The study received the approval of the simulation center and the local ethics committee of the Faculty of Medicine of Poitiers.
Protocol
The study design is represented in Figure 1. Briefly, nursery assistants participated to two teaching sessions (T1 and T2) and two evaluation session (E1 and E2). T1 consisted in a 1-h didactic reminder about infant CPR (T1) performed by CPR-certified physician instructors (FB, AG, DO) explaining the epidemiology of cardiac arrest in infant and detailing the steps of CPR according to the European Resuscitation Council recommendation (23). T2 consisted in SBT focus on infant CPR training using mannikin (BabyBen®, Laerdal, Norway) under supervision of CPR-certified physician instructors (FB, AG, DO). The duration of T2 was 2 h allowing participants to rehearse and correct their performance. Each participant repeated the CPR sequence on the manikin a minimum of three times. For evaluation sessions, the participant had to perform an infant CPR on manekin. The performance was assessed automatically and with a checklist as described below. E1 was performed before SBT and E2 after SBT training performed at T2. For E2, participants were randomly divided into three equal groups and the session was performed 15 (Group 1 – D15), 30 (Group 2 – D30), or 60 days after T2 (Group 3 – D60).
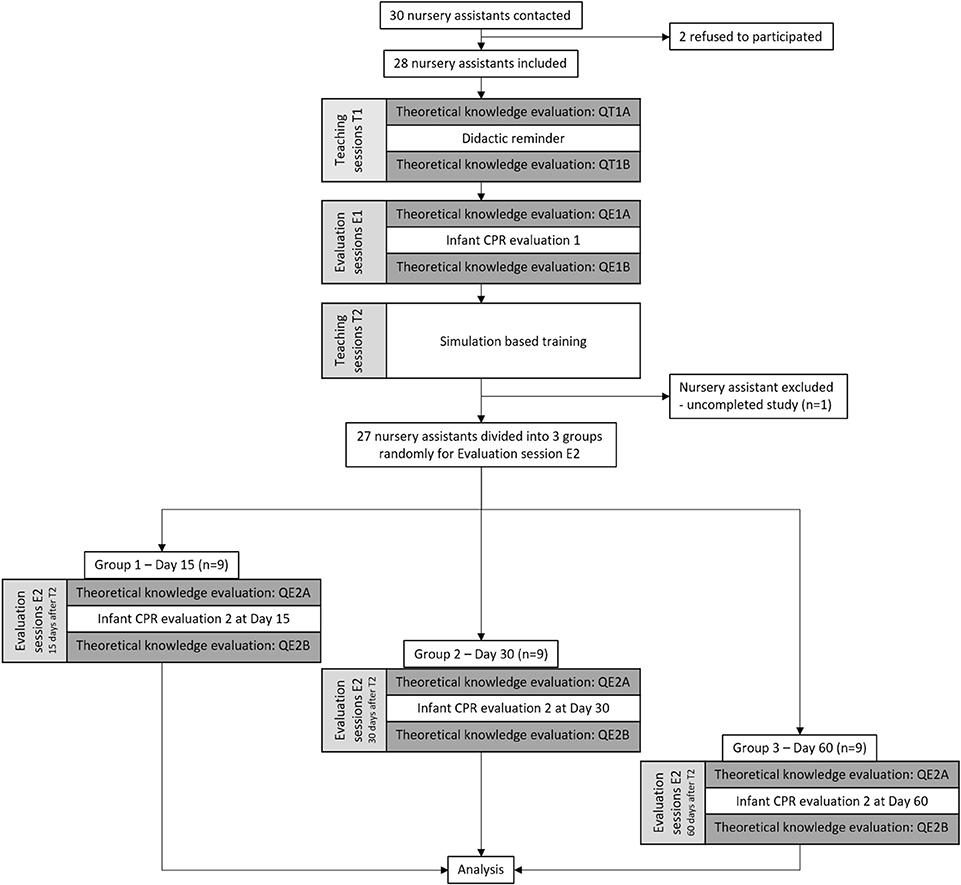
Figure 1. Study design and flow chart.
Except for T2, knowledge test was performed at the beginning and the end of each session. Content of the scenario was explained out to participants during briefing just before simulation and of the simulation room. The same scenario (Appendix A1) was used for evaluation session to allow comparison between scores. To improve the realism of the situation, the evaluation room has been converted into a baby's room and contained the manikin (dressed like a baby and lying in a crib), towels, table and phone (to simulated the call for help to the emergency medical system. For each evaluation, the performance starts immediately after entering the room where the manikin is located and duration was limited at 4 min. All performances were videotaped and followed by a good-judgment debriefing (19) run by a trained facilitator (FB, DO) including a short feedback on participant's performance to improve further CPR practice. The study was performed in addition of the usual CPR training. However, to limit bias, all of the study was performed between two session of the usual CPR training.
Performance Measure
Basic life support (BLS) competencies were measured using Resusci Baby QCPR® (ref: 161-01250, Laerdal Medical) and a SimPad PLUS SkillReporter (ref: 206-30033, Laerdal Medical) connected defining a QCPR Score, a QCPR Breathing Score (based on the time of the first recue breath, tidal volume, and respiratory rate) and a QCPR Compression Score (based on time of the first compression, compression rate, compression depth, chest recoil, finger position, and no flow duration). Scores were expressed by the device as percentage of success. According to manufacturer instructions, the CPR performance quality was determined by the QCPR scores which reflect a basic (<50%), intermediate (≥50 and <75%), or advanced (≥75%) CPR performance quality. A CPR performance checklist created for the study based on the European Resuscitation Council recommendations (Appendix A2), was also used to measure basic life support competences not recorded with the skill reporter. The checklist was composed by 18 items (e.g., check breath, start rescue breaths, start chest compression) and were associated to a 2-point (0 or 1 point) or 3-point (0, 1 or 2 points) scale. The sum of all items scores defined the MCPR Global-Score. Two independent evaluations, spaced by 6 months, were performed by the referring observer (FB) for each CPR performance (one during evaluation sessions and the other, blinded of the first results, using anonymized participants' performance videotapes) and intra-class correlation was calculated.
The same QCPR Global-Scores thresholds were used for MCPR scores to determine CPR quality.
Theoretical Knowledge Evaluation
A written theoretical knowledge test based on questionnaire created for the study was used to measure infant CPR knowledge and included 36 items (Appendix A3) for a maximum score of 45. The questionnaire was composed by 7 sections: Infant ALTE signs (/7 points), Cardiac arrest generalities (/6 points), Infant cardiac arrest management (/6 points), Alone rescuer CPR (/6 points), Ventilation management score (/4 points), chest compression management (/5 points) and Emergency call section (/11 points). Each correct answer per item corresponds to 1 point except for 2 items scored out of 2 points and 1 out of 3 points (3 answers expected). For the Alone rescuer CPR section, corresponding to one item, participant had to order CPR step for a maximum of 6 points. Throughout the study, each participant had to complete 6 questionnaires (QT1A, QT1B, QE1A, QE1B, Q2EA, QE2B) (Figure 1). Before analysis participant's answers were double check by investigator (FB, DO).
Statistical Analysis
Statistical analysis was performed with SPSS 26.0 (SPSS Inc., Chicago, IL). Results are presented as mean + standard deviation (SD) or median with interquartile range [IQR25-IQR75]. Comparisons of continuous variables were made with paired t-test or ANOVA for paired and parametric values, Wilcoxon or Friedman tests for non-parametric paired values and Mann–Whitney or ANOVA test for non-parametric and unpaired values. Categorial variables were analyzed with Chi square test or Fisher's test. Pearson test was used to assessed correlation for parametric values or Spearman test for non-parametric values. Bland and Altman test was used to assess intra-observers reproducibility. A p-value < 0.05 was considered significant.
Results
Population
Out of the thirty contacted nursery assistants, two refused to participate, and one was excluded because she did not complete the study protocol (Figure 1). Characteristics of the population are presented in Table 1. The three groups obtained for E2 did not present significant difference.
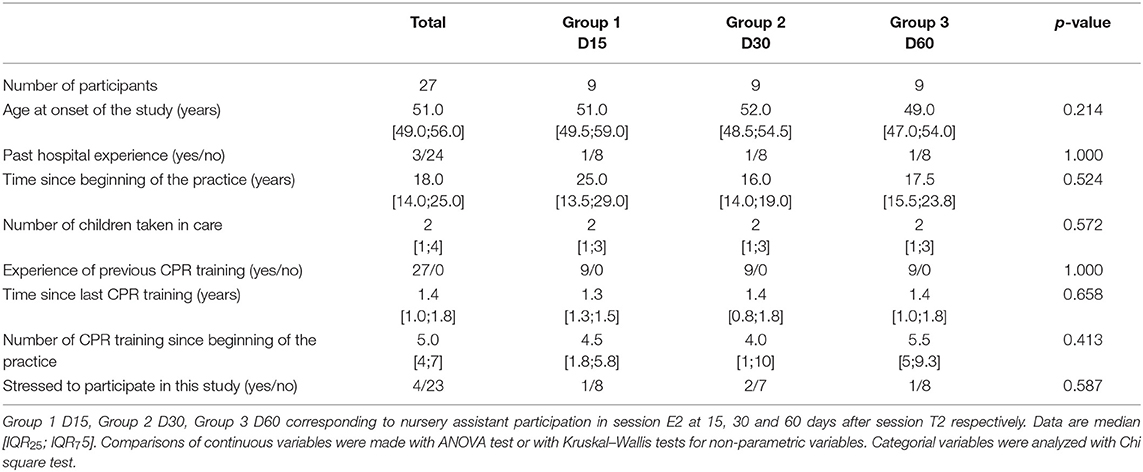
Table 1. Characteristics of the population.
Practical Evaluation
Improvement in CPR Performance: Global-Scores
While the QCPR Global-Score was significantly improved between E1 and E2, the increase in the number of participants with a QCPR Global-Score between 50 and 75% or over 75% was not significant (Table 2).
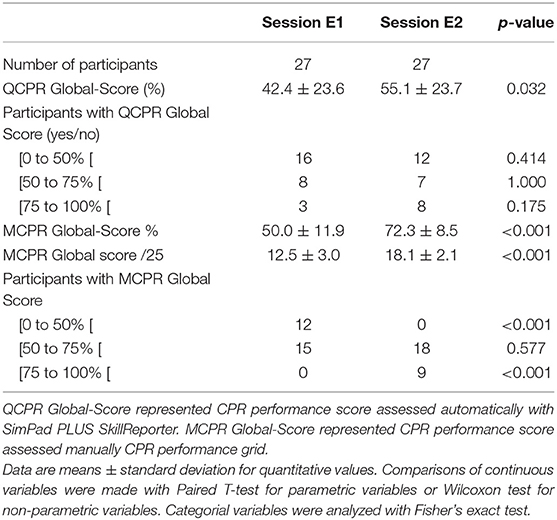
Table 2. CPR performance global scores.
Considering MCPR scores, intra-observer agreement and intra-class correlation over time were high and lack of intra-observer agreement over time was low at E1, E2 or for all observations together (Figures E1A,B). MCPR Global-Scores and the number of participants with a score between 50 and 75% or over 75% were increased significantly between E1 and E2 (Table 2). QCPR and MCPR Global-Scores appeared strongly correlated at E1 and E2 or with all values together (Figures E2A–C). In addition, ROC curves analysis performed to determine the ability of MCPR Scores to predict a QCPR Global-Score had significant AUCs and >0.5 with a high sensitivity and a high negative predictive value (NPV) to predict QCPR Global-Score ≥50% and a high specificity and a high negative predictive value (NPV) to predict QCPR Global-Score ≥75% (Table E1).
Changes in Specific BLS Step of CPR (Table 3)
Airways and communication
There was a significant improvement in participants positioning the manikin in neutral position, opening airways, inspecting airways and performing CPR during the call to emergency medical system. There was no significant change for stimulating the manikin, putting it on hard surface and calling emergency medical system item performed by most of participant at E1.
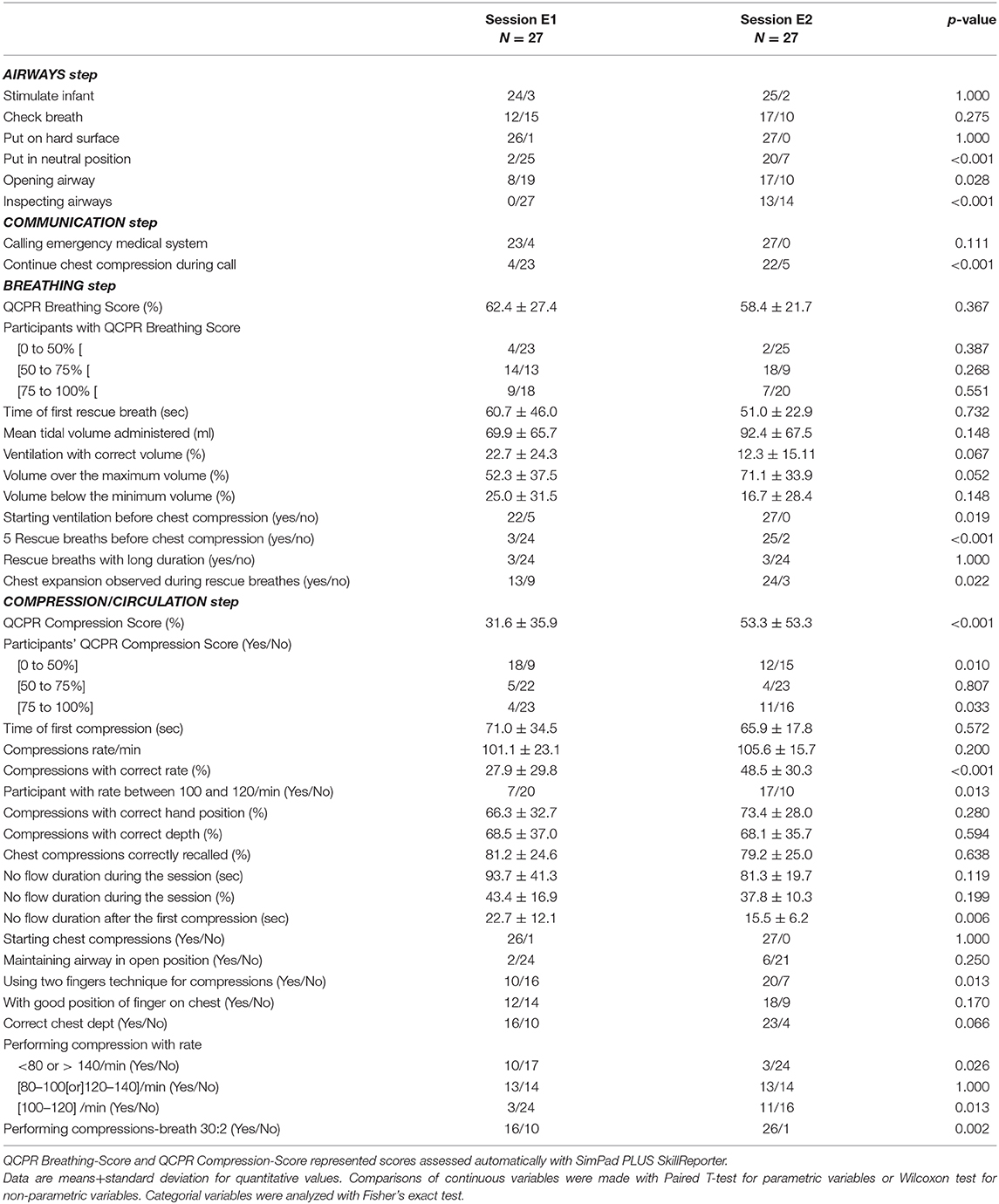
Table 3. BLS steps.
Breathing
There was no significant difference of QCPR B-Score between E1 and E2, however the number of participants starting and performing 5 rescue breathes before chest compressions and with chest expansion observed during rescue breathes. The time of the first rescue breath after the discovery of the manikin was decreased at E2 compared to E1 but the difference was not significant. The percentage of ventilation administering the correct volume remained very low at E2, with most of the volumes administered exceeding the maximum expected volume.
Circulation/compression
QCPR C-Score and number of participants with a QCPR C-score over 75% increased significantly between E1 and E2. Moreover, the percentage of compressions performed at a correct rate, the number of participants with an average compression rate of 100–120 per minute, and the use of the two fingers technique for chest compression and performing 2 rescue breathes each 30 chest compressions increased significantly between E1 and E2. The time to first compression and the percentage of no flow duration were decreased between E1 and E2 but the difference was not significant. However, the no flow duration after the first compression decrease significantly between the session. Chest compression depth and recoil, or correct hand position were not different between E1 and E2.
Theoretical Knowledge Evaluation
Score obtained before any intervention at the beginning of T1 (QT1A) increased significantly after didactic intervention (QT1B) with an improvement of knowledge in infant cardiac arrest management, order of CPR steps of management, chest compression, ventilation, and emergency call (Figures 2A–F) and after E1 for infant ALTE signs and cardiac arrest score (Figures 2G,H). Then scores were not significantly different. Interestingly, there was a correlation between theoretical knowledge score at the beginning of E1 (QE1A) with QCPR or MCPR Global-Score at E1 (Figures E3A,B) but not between theoretical knowledge score at the beginning of E2 (QE2A) with QCPR or MCPR Global-Score at E2 (Figures E3C,D).
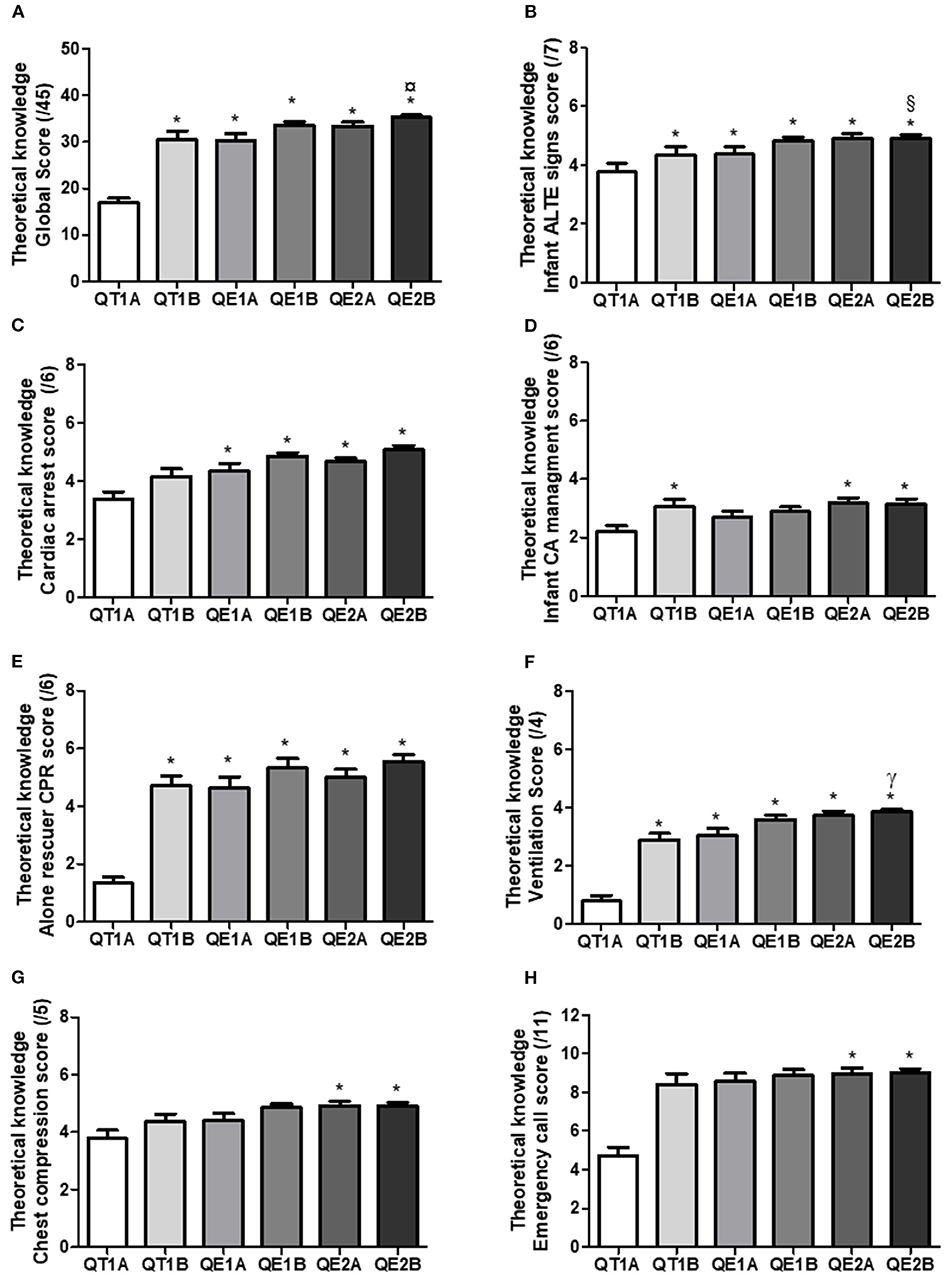
Figure 2. Theoretical knowledge score. Theoretical knowledge was assessed with questionnaire at the beginning and the end of T1, E1, and E2 defining qussssestionnaire T1A, T1B, E1A, E1B, E2A, and E2B respectively to determine the evolution of (A) the theoretical knowledge global score composed by (B) infant ALTE signs score, (C) cardiac arrest generalities score, (D) infant cardiac arrest management score, (E) alone rescuer CPR score, (F) ventilation management score, (G) chest compression management score and (H) Emergency call score and. P < 0.05 * vs. T1B, ¤ vs. E1A, § vs. E2A, γ vs. T1A.
Evaluation of Persistence of Performance Over Time
BLS competencies assessed with Skill Reporter or with BLS checklist and QE2A questionnaire score were not significantly different between the three groups performing E2 15, 30, or 60 days after SBT training session T2 (Table E2).
Discussion
Main Results
This simulation-based study demonstrated an improvement in infant CPR performance, skills and knowledge—especially concerning Chest compression steps—with a satisfactory retention at 15, 30, or 60 days in a population of nursery assistants. Scores assessed with checklist were strongly correlated to automatically assessment and predictive of the of CPR performance quality determined by skill recorder.
Discussion of Primary Outcomes
In this study, most of participants had CPR performance scores and Compression scores above 50% at baseline while they were previously trained to CPR, suggesting that first aid management of cardiac arrest training was insufficient and that scores of untrained laypeople would be similar or worse (24). Most simulation studies included healthcare providers and did not address the infant OHCA cardiac arrest. However, some studies have shown that knowledge of first aid management was a predictor of parents' self-efficacy in infant CPR skills (25, 26). The present study showed the benefits of SBT combined with didactics corresponding to mastery training as previously reported (27) and demonstrated the ability of SBT to improve CPR performance even in lay people such as nursery assistants (13, 21, 28–30). This improvement can be observed both with automatically assessment using QCPR device or by observer assessment using CPR checklist. However, a QCPR Global-Score over 75%—corresponding to advanced CPR quality—was not obtained by all the performers. Nevertheless, a study performed with healthcare providers (31) or with laypeople reported similar results (32). We could imagine that a single practical training course would be sufficient to improve a low starting CPR quality to an intermediate one, and only a repeated training would be necessary to achieve an advance CPR quality. Another explanation from this lack of results could be related to the difficulty for some participants to maintain the same CPR quality for 4 min of simulation because of exhaustion since it was a population close to 50 years old.
Discussion of Secondary Outcomes
As previously demonstrated, mastery training, led to an improvement in participants' skills and knowledge in different steps of infant CPR management (13, 16, 17). In this study, participants improved their skill in each step of infant CPR.
Surprisingly QCPR B-Score was not increased after SBT. This lack of result could be explained by difficulties for participants to administrate a correct volume during rescue breathes. Previous studies highlighted that rescue breathes in CPR did not improve survival or morbidity (33–35) except for infants (up to 1 year) because of hypoxic high frequency of CA. However, to improve survival or morbidity, these studies concluded that ventilation must be optimal—that was not the case even after CPR training. Moreover, the first chest compression was delayed over 1 min representing a considerable no flow duration even if after the first compression the no flow duration was low. This encourages, for laypeople, to perform infant CPR with a C-A-B sequence to initiate sooner chest compressions and reduce no flow duration as mentioned by the American Heart Association guidelines or European Resuscitation Council Guidelines for adults (23, 34, 36). Moreover, as reported, in infants, to not perform rescue breath would not be associated with several outcomes 1 month after CPR (35, 37).
As described previously, an optimal CPR could improve survival after CA (3, 6, 7), however it could be harder to determine laypeople's CPR quality during CPR training without QCPR device. In this study, performance score obtained automatically and with the checklist were correlated, and MCPR scores appeared predictive of CPR quality defined by QCPR global-Scores over 50 or 75%. This result was consistent with the literature that objective and detailed checklist were sufficient to assess CPR quality (38).
This study showed that CPR performance was correlated to laypeople's CPR theoretical knowledge after didactic reminder but not after practice training. However, after the didactic reminder, performance scores remained low. This result highlighted that improved theoretical knowledge in CPR was not enough to obtain a satisfactory CPR quality and the interest of practical training (39, 40). Moreover, as presented in this study, the association of didactic intervention and SBT—mastery training—could maintain knowledge and skills up to 2 months as for healthcare providers (13, 14, 29, 32, 41) which correspond to an adequate which corresponds to an adequate amount of time to repeat the training or assessment of the performance (42, 43).
Limitations
This study had some limitations. First, while the inclusion rate was high number of participants included was small leading to little group to assess retention over time. However, the results obtained by the three groups were very similar and it seems unlikely that the lack of difference is related to a lack of statistical power.
Secondary, the equipment used for simulation was only presented during briefing before CPR performance while most of participant had never used QCPR devices or manikin Resusci Baby QCPR before the study. The lack of awareness of the possibilities of these elements by the participants may had influenced results of E1 and artificially increased those of E2. However, the influence of equipment on score may be low because all participants were previously trained to CPR on different types of manikin. The use of the same scenario for E1 and E2 may have contributed to artificially increasing the results on E2. However, before E2 and until the briefing, participants were not informed that scenario used for E2 would be the same as for E1 to prevent external training. Moreover, using the same scenario was necessary to compare performance.
Another limitation of the study was the absence of evaluation before any intervention to know CPR performance at baseline and to correlate it to theoretical knowledge. However, score and skills at E1 were low and were probably not or only slightly modified by the didactic intervention. Moreover, previous studies have demonstrated the low quality of CPR performance of laypeople at baseline (8, 9). The CPR sequence used was A-B-C and not C-A-B because it dealt with infants. Comparison of performance between groups using a different sequence may be interesting but the small number of participants limited this possibility but could be the purpose of a future study.
The used of non-standardized checklist was a limitation of the study however the checklist was developed from ERC recommendations and allowed to assess skills unrecorded by the QCPR device. Moreover, MCPR score determined with the checklist was strongly correlated to the CPR quality assess automatically with the QCPR device. The knowledge questionnaire was also non-standardized however no standardized questionnaire was previously available. In addition, each answer can be deduced from the didactic reminder performed at T1 and ensured that the participant had sufficient knowledge to perform a CPR. In addition,
External Validity
To our knowledge, this is the first simulation-based study about infant CPR performance of nursery assistants working alone at home proposing an easy and accessible method to assess infant CPR quality. The chosen population included motivated and very engaged nursery assistant women previously trained once every 2 years in infant CPR. In addition to the small number of participants, it would be difficult to generalize these results to all of the nursery assistant, other caregivers or laypeople and further study with a larger number of participants would be necessary.
Conclusion
Mastery training including didactics and SBT could improve performance, skills, knowledge with satisfactory retention over time in infant CPR management performed by nursery assistants especially for chest compression step. CPR performance quality could be assessed with detailed CPR checklist. This training represents an interesting method to train laypeople in charge of infants in management of different emergencies requiring immediate support while waiting for help. However, further study would be useful in determining the number of SBT training sessions required for each participant to achieve advanced quality. The repetition of simulation sessions would be mandatory for long-term memory retention as infant cardiac arrest represents a low volume-high stakes situation. Further studies should include larger area-based populations and measure critical events management in infants taken care of by nursery assistants.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
Conception and design of the study, or acquisition of data, or analysis and interpretation of data: FB, BB, VG-M, and DO. Drafting the article or revising it critically for important intellectual content: FB, AG, and DO. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are very grateful to the staff of the Early Childhood Department of the Social Action Center of the City Hall of Poitiers who allowed this study and to all the nursery assistants who participated.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.00356/full#supplementary-material
Abbreviations
AHA, American Heart Association; ALTE, Apparent life-threatening event; BLS, Basic life support; CA, Cardiac arrest; CPR, Cardiopulmonary resuscitation; OHCA, Out-of-hospital cardiac arrest; ROC, Receiver operating characteristic; SBT, Simulation-based training; SD, standard deviation.
References
1. Luc G, Baert V, Escutnaire J, Genin M, Vilhelm C, Di Pompéo C, et al. Epidemiology of out-of-hospital cardiac arrest: a French national incidence and mid-term survival rate study. Anaesth Crit Care Pain Med. (2019) 38:131–5. doi: 10.1016/j.accpm.2018.04.006
2. Tursz A, Crost M, Gerbouin-Rérolle P. La maltraitance dans l'enfance en France: quels chiffres, quelle fiabilité? [Child abuse in France: how much, how reliable are the numbers?]. Rev Epidemiol Sante Publique. (2003) 51:439–44.
3. Kämäräinen A. Out-of-hospital cardiac arrests in children. J Emerg Trauma Shock. (2010) 3:273–6. doi: 10.4103/0974-2700.66531
4. Atkins DL, Everson-Stewart S, Sears GK, Daya M, Osmond MH, Warden CR, et al. Epidemiology and outcomes from out-of-hospital cardiac arrest in children: the roc epistry-cardiac arrest. Circulation. (2009) 119:1484–91. doi: 10.1161/CIRCULATIONAHA.108.802678
5. Bougouin W, Lamhaut L, Marijon E, Jost D, Dumas F, Deye N, et al. Characteristics and prognosis of sudden cardiac death in greater Paris: population-based approach from the paris sudden death expertise center (Paris—SDEC). Intensive Care Med. (2014) 40:846–54. doi: 10.1007/s00134-014-3252-5
6. Meert KL, Telford R, Holubkov R, Slomine BS, Christensen JR, Dean JM, et al. Pediatric out-of-hospital cardiac arrest characteristics and their association with survival and neurobehavioral outcome. Pediatr Crit Care Med. (2016) 17:e543–50. doi: 10.1097/PCC.0000000000000969
7. Wellens HJJ. Cardiac arrest outside of a hospital: how can we improve results of resuscitation? Circulation. (2003) 107:1948–50. doi: 10.1161/01.CIR.0000067880.57844.62
8. Handley JA, Handley AJ. Four-step CPR—improving skill retention. Resuscitation. (1998) 36:3–8. doi: 10.1016/S0300-9572(97)00095-6
9. Cho GC, Sohn YD, Kang KH, Lee WW, Lim KS, Kim W, et al. The effect of basic life support education on laypersons' willingness in performing bystander hands only cardiopulmonary resuscitation. Resuscitation. (2010) 81:691–4. doi: 10.1016/j.resuscitation.2010.02.021
10. Hasselqvist-Ax I, Riva G, Herlitz J, Rosenqvist M, Hollenberg J, Nordberg P, et al. Early cardiopulmonary resuscitation in out-of-hospital cardiac arrest. N Engl J Med. (2015) 372:2307–15. doi: 10.1056/NEJMoa1405796
11. Austin AL, Spalding CN, Landa KN, Myer BR, Donald C, Smith JE, et al. A randomized control trial of cardiopulmonary feedback devices and their impact on infant chest compression quality: a simulation study. Pediatr Emerg Care. (2017) 36:e79–84. doi: 10.1097/PEC.0000000000001312
12. Bragard I, Farhat N, Seghaye M, Karam O, Neuschwander A, Shayan Y, et al. Effectiveness of a high-fidelity simulation-based training program in managing cardiac arrhythmias in children: a randomized pilot study. Pediatr Emerg Care. (2019) 35:412–8. doi: 10.1097/PEC.0000000000000931
13. Aqel AA, Ahmad MM. High-fidelity simulation effects on cpr knowledge, skills, acquisition, and retention in nursing students. Worldviews Evid Based Nurs. (2014) 11:394–400. doi: 10.1111/wvn.12063
14. Lateef F. Simulation-based learning: Just like the real thing. J Emerg Trauma Shock. (2010) 3:348–52. doi: 10.4103/0974-2700.70743
15. Bradley P. The history of simulation in medical education and possible future directions. Med Educ. (2006) 40:254–62. doi: 10.1111/j.1365-2929.2006.02394.x
16. Datta R, Upadhyay K, Jaideep C. Simulation and its role in medical education. Med J Armed Forces India. (2012) 68:167–72. doi: 10.1016/S0377-1237(12)60040-9
17. Armenia S, Thangamathesvaran L, Caine A, King N, Kunac A, Merchant A. The role of high-fidelity team-based simulation in acute care settings: a systematic review. Surg J. (2018) 04:e136–51. doi: 10.1055/s-0038-1667315
18. Aggarwal R, Mytton OT, Derbrew M, Hananel D, Heydenburg M, Issenberg B, et al. Training and simulation for patient safety. Qual Saf Health Care. (2010) 19:i34–43. doi: 10.1136/qshc.2009.038562
19. Fink EL, Prince DK, Kaltman JR, Atkins DL, Austin M, Warden C, et al. Unchanged pediatric out-of-hospital cardiac arrest incidence and survival rates with regional variation in north America. Resuscitation. (2016) 107:121–8. doi: 10.1016/j.resuscitation.2016.07.244
20. PSC 1 version septembre 2018 VF,.pdf. (2018). Available online at: https://www.interieur.gouv.fr/Le-ministere/Securite-civile/Documentation-technique/Secourisme-et-associations/Les-recommandations-et-les-referentiels (accessed September 15, 2019).
21. Sankar J, Vijayakanthi N, Sankar MJ, Dubey N. Knowledge and skill retention of in-service versus preservice nursing professionals following an informal training program in pediatric cardiopulmonary resuscitation: a repeated-measures quasiexperimental study. BioMed Res Int. (2013) 2013:403415. doi: 10.1155/2013/403415
22. Miller DR, Kalinowski EJ, Wood D. Pediatric continuing education for EMTs: recommendations for content, method, and frequency. Pediatr Emerg Care. (2004) 20:269–72. doi: 10.1097/01.pec.0000121249.99242.11
23. Maconochie IK, Bingham R, Eich C, López-Herce J, Rodríguez-Núñez A, Rajka T, et al. European resuscitation council guidelines for resuscitation 2015. Resuscitation. (2015) 95:223–48. doi: 10.1016/j.resuscitation.2015.07.028
24. Lerjestam K, Willman A, Andersson I, Abelsson A. Enhancing the quality of CPR performed by laypeople. Australas J Paramed. (2018) 15:1–5. doi: 10.33151/ajp.15.4.594
25. Wei Y-L, Chen L-L, Li T-C, Ma W-F, Peng N-H, Huang L-C. Self-efficacy of first aid for home accidents among parents with 0- to 4-year-old children at a metropolitan community health center in Taiwan. Accid Anal Prev. (2013) 52:182–7. doi: 10.1016/j.aap.2012.12.002
26. Bánfai B, Deutsch K, Pék E, Radnai B, Betlehem J. Accident prevention and first aid knowledge among preschool children's parents. Kontakt. (2015) 17:e42–7. doi: 10.1016/j.kontakt.2015.01.001
27. Kim IO, Shin SH. The CPR educational program effect of infant cpr immediate remediation for child care teachers. J Korean Acad Soc Nurs Educ. (2013) 19:508–17. doi: 10.5977/jkasne.2013.19.4.508
28. Brennan RT, Braslow A. Skill mastery in public CPR classes. Am J Emerg Med. (1998) 16:653–7. doi: 10.1016/S0735-6757(98)90167-X
29. Barsuk JH, Cohen ER, McGaghie WC, Wayne DB. Long-term retention of central venous catheter insertion skills after simulation-based mastery learning. Acad Med. (2010) 85:S9–12. doi: 10.1097/ACM.0b013e3181ed436c
30. Roh YS, Lee WS, Chung HS, Park YM. The effects of simulation-based resuscitation training on nurses' self-efficacy and satisfaction. Nurse Educ Today. (2013) 33:123–8. doi: 10.1016/j.nedt.2011.11.008
31. Owen H, Mugford B, Follows V, Plummer JL. Comparison of three simulation-based training methods for management of medical emergencies. Resuscitation. (2006) 71:204–11. doi: 10.1016/j.resuscitation.2006.04.007
32. Boet S, Bould MD, Pigford A-A, Rössler B, Nambyiah P, Li Q, et al. Retention of basic life support in laypeople: mastery learning vs. Time-based Education. Prehosp Emerg Care. (2017) 21:362–77. doi: 10.1080/10903127.2016.1258096
33. Atkins DL, de Caen AR, Berger S, Samson RA, Schexnayder SM, Joyner BL, et al. American heart association focused update on pediatric basic life support and cardiopulmonary resuscitation quality: an update to the American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. (2018) 137:e1–6. doi: 10.1161/CIR.0000000000000540
34. Powers WJ, Derdeyn CP, Biller J, Coffey CS, Hoh BL, Jauch EC, et al. AHA/ASA focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment. Stroke. (2015) 46:3020–35. doi: 10.1161/STR.0000000000000074
35. Fukuda T, Ohashi-Fukuda N, Kobayashi H, Gunshin M, Sera T, Kondo Y, et al. Conventional versus compression-only versus no-bystander cardiopulmonary resuscitation for pediatric out-of-hospital cardiac arrest. Circulation. (2016) 134:2060–70. doi: 10.1161/CIRCULATIONAHA.116.023831
36. Marsch S, Tschan F, Semmer N, Zobrist R, Hunziker P, Hunziker S. ABC versus CAB for cardiopulmonary resuscitation: a prospective, randomized simulator-based trial. Swiss Med Wkly. (2013) 143:w13856. doi: 10.4414/smw.2013.13856
37. Naim MY, Burke RV, McNally BF, Song L, Griffis HM, Berg RA, et al. Association of bystander cardiopulmonary resuscitation with overall and neurologically favorable survival after pediatric out-of-hospital cardiac arrest in the United States: a report from the cardiac arrest registry to enhance survival surveillance registry association of bystander CPR with survival after pediatric cardiac arrest association of bystander CPR with survival after pediatric cardiac arrest. JAMA Pediatr. (2017) 171:133–41. doi: 10.1001/jamapediatrics.2016.3643
38. Morgan PJ, Cleave-Hogg D, DeSousa S, Tarshis J. High-fidelity patient simulation: validation of performance checklists. Br J Anaesth. (2004) 92:388–92. doi: 10.1093/bja/aeh081
39. Sanri E, Karacabey S, Eroglu SE, Akoglu H, Denizbasi A. The additional impact of simulation based medical training to traditional medical training alone in advanced cardiac life support: a scenario based evaluation. Signa Vitae - J Intensive Care Emerg Med. (2018) 14:68–72. doi: 10.22514/SV142.102018.10
40. Ruesseler M, Weinlich M, Müller MP, Byhahn C, Marzi I, Walcher F. Simulation training improves ability to manage medical emergencies. Emerg Med J. (2010) 27:734. doi: 10.1136/emj.2009.074518
41. Lammers RL, Byrwa MJ, Fales WD, Hale RA. Simulation-based assessment of paramedic pediatric resuscitation skills. Prehosp Emerg Care. (2009) 13:345–56. doi: 10.1080/10903120802706161
42. Ghazali DA, Fournier E, Breque C, Ragot SP, Oriot D. Immersive simulation training at 6-week intervals for 1 year and multidisciplinary team performance scores: a randomized controlled trial of simulation training for life-threatening pediatric emergencies. El efecto de las simulaciones inmersivas repetidas cada 6 semanas en la evolución del rendimiento de un equipo multidisciplinar durante un año: un ensayo controlado aleatorizado en situaciones pediátricas de riesgo vital. Emergencias. (2019) 31:391–8.
Keywords: infant, CPR, simulation-based training, nursery assistants, assessment, performance
Citation: Beaufils F, Ghazali A, Boudier B, Gustin-Moinier V and Oriot D (2020) Nursery Assistants' Performance and Knowledge on Cardiopulmonary Resuscitation: Impact of Simulation-Based Training. Front. Pediatr. 8:356. doi: 10.3389/fped.2020.00356
Received: 26 October 2019; Accepted: 28 May 2020;
Published: 30 June 2020.
Edited by:
Martin Chalumeau, Université Paris Descartes, FranceReviewed by:
Romain Basmaci, Hôpital Louis-Mourier, Assistance Publique Hopitaux De Paris, FranceEdward Purssell, City University of London, United Kingdom
Copyright © 2020 Beaufils, Ghazali, Boudier, Gustin-Moinier and Oriot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabien Beaufils, ZmFiaWVuLmJlYXVmaWxzQGNodS1ib3JkZWF1eC5mcg==