 Carmela de Lamas1†
Carmela de Lamas1† Paula Sánchez-Pintos1,2,3,4,5†
Paula Sánchez-Pintos1,2,3,4,5† María José de Castro1,2,3,4,5
María José de Castro1,2,3,4,5 Miguel Sáenz de Pipaon6
Miguel Sáenz de Pipaon6 María Luz Couce1,2,3,4,5*
María Luz Couce1,2,3,4,5*- 1Santiago de Compostela University, Santiago de Compostela, Spain
- 2Metabolic Unit, Neonatology Department, University Clinical Hospital of Santiago de Compostela, Santiago de Compostela, Spain
- 3IDIS-Health Research Institute of Santiago de Compostela, Santiago de Compostela, Spain
- 4European Reference Network for Rare Hereditary Metabolic Disorders (MetabERN), Madrid, Spain
- 5Rare Diseases Networking Biomedical Research Centre (CIBERER), Madrid, Spain
- 6Department of Pediatrics-Neonatology, Autonomous University of Madrid, La Paz University Hospital, Madrid, Spain
Introduction: Technological advances over the last 2 decades have led to an increase in the time spent by children and youth engaged in screen-based activities, and growing recognition of deleterious effects on health. In this systematic review of cohort and cross-sectional studies, we assess current data on the relationship between screen time and bone status in children and teenagers.
Methods: We searched PUBMED and SCOPUS databases for studies of children and adolescents that assessed screen time and bone status, determined by measuring bone mineral content or density, bone stiffness index, bone speed of sound, bone broadband ultrasound attenuation, or frame index. Searches were limited to studies published between 1900 and 2020, and performed in accordance with Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. The studies included were evaluated using the Newcastle-Ottawa quality assessment scale.
Results: Ten cohort and cross-sectional studies including pediatric population were selected. The combined study population was 20,420 children/adolescents, of whom 18,444 participated in cross-sectional studies. Four studies assessed the effects of total screen time, seven the consequences of TV viewing time, and six the effects of recreational computer use on bone health. Our findings indicate an inverse association between total and weekly screen time and bone health in children and adolescents. In 57% of the studies included also a negative correlation between television viewing time and bone status was observed, while recreational computer time did not have a significant impact on bone health. According to the only four studies that included dietetic factors, no relevant differences were found between calcium intake and screen time or bone broadband ultrasound attenuation and bone speed of sound.
Conclusions: Review of the literature of the past three decades provides strong support for comprehensive education of screen time on bone status. The findings of this systematic review support a negative association between screen time and bone status in children and adolescents, with a different impact when considering the different technological devices. As peak bone mass in adolescents is the strongest predictor of osteoporosis risk, strategies aimed at improving bone health should incorporate conscious use of digital technology.
Introduction
In recent years screen use has expanded to include a wide variety of electronic media devices available throughout the world. Although television (TV) remains the predominant screen-based activity among children (1), use of computers, video games, tablets, and smart phones begins at increasingly younger ages (2–4). The popularity and widespread use of screen-based activities among children and young people and the accompanying rapid change in technology and patterns of use, has turned the detrimental effects of excessive screen time and its prevalence into a global health problem. A recent study that compared screen time exposure in young children before and after mobile devices became widely available found that between 1997 and 2014 total screen time in children aged 0–2 years increased from 1.32 h to 3.05 h per day, and that most of this time was spent watching TV (5). Since the invention of television, parents, educators, and health care providers have raised concerns about the immediate and long-term deleterious effects of excessive screen-based activity, especially TV viewing (6–9). Several studies have reported negative associations between screen time and physical and cognitive abilities (10), and positive associations with obesity (11), sleep problems, attention disorders, depression, and anxiety (12–14). Excessive screen exposure can also cause visual discomfort (15, 16), myopia, or squinting due to a lack of outdoor activities (17), and video games and TV viewing in particular are associated with unhealthy diets (18). Other concerns relate to the exposure of children to potentially deleterious content, including violence, sex, and fast food advertising (19).
The American Academy of Pediatrics (AAP) has recommended limiting children's total media time (with entertainment media) to no more than 1–2 h of quality programming per day (20), no screen time for children under 2 years of age, and removal of TV sets from children's bedrooms. Several studies have investigated the individual, familial, and sociocultural forces that shape children's screen habits to identify simple and incremental approaches that may help reduce TV viewing time (21–23). Although most parents report that they adhere to TV viewing guidelines, few establish rules that limit the time their children spend watching TV (24, 25). Moreover, while parents tend to agree with a 2-h limit in principle, many feel that it does not apply to their child in the absence of academic difficulties or behavioral problems, and perceive numerous barriers to implementing the recommendations (26).
It is increasingly acknowledged that screen-based activity may also negatively affect bone status, resulting in low bone mineral content (BMC), low bone mineral density (BMD), and osteoporosis (27), since nutrition (including adequate intake of protein, Calcium (Ca), Phosphorus (P), and vitamin D) (28, 29) and physical activity are major factors implicated in bone growth and health. In general, dual energy X-ray absorptiometry (DEXA) of the lumbar spine and hip is the preferred method of measuring BMD. The International Society for Clinical Densitometry (ISCD) recommends using DEXA BMD Z-scores rather than T-scores in children, since diagnosis of osteoporosis in these groups should not be based on densitometry criteria alone and should include the presence of a clinically significant fracture history (30). While the current gold standard for measuring BMD is DEXA, this method is costly, involves ionizing radiation, and requires a highly trained operator (31). Another method developed to assess osteoporosis risk is quantitative ultrasound (QUS) (17). QUS assesses bone quality by measuring the attenuation and velocity of ultrasound waves passing through the bone, and has become a popular low-cost, readily accessible, and radiation-free alternative to DEXA for osteoporosis screening (32, 33).
The incidence, severity, underlying mechanisms, and clinical implications of bone disease associated with screen use in children remain a matter of discussion. In this systematic review we present a comprehensive overview of evidence from cohort and cross-sectional studies assessing the association between screen-based activity and bone status in children and adolescents, including BMC, BMD, bone stiffness index (BSI), bone speed of sound (SOS), bone broadband ultrasound attenuation (BUA), and frame index (FI).
Methods
The review question on which this work was based was as follows: “Does screen time in children and adolescents correlate with bone status?”. This systematic review was carried out following PRISMA (Preferred Reporting Items for Systematic reviews and Meta-analyses) guidelines (34, 35) and was registered in the International Prospective Register of Systematic Reviews (PROSPERO Code: CRD42020217924. Data registry: Nov 28, 2020).
Once the review question was formulated, we performed searches of PUBMED and SCOPUS databases in December 2020. The PUBMED search was carried out using the following search terms: (“Bone and Bones”[Mesh] OR “Calcification, Physiologic”[Mesh]) AND (“Life Style”[Mesh] OR “Sedentary Behavior”[Mesh] OR “television”[Mesh] OR “screen time”[Mesh]). The search was limited to the pediatric population through the filter: Child: birth-18 years. The SCOPUS search was conducted using the search terms “(Television OR screen time) AND Bone”. In addition, the bibliographies of the articles returned by searches and other previously published reviews on the topic were manually reviewed.
Based on the PICOS criteria (Population, Intervention, Comparison, Outcome and, Settings) (34) the inclusion criteria were: children and adolescents, assessing screen time (TV, computer, mobile devices) and bone status observational studies published between January 1, 1900 and December 31, 2020. Studies that did not include screen time or bone status data or were carried out in patients with chronic pathologies including obesity, single case review studies or studies written in languages other than Spanish and Englis were excluded from our review.
The time dedicated to screen-based activities was the exposure studied. The purpose of the study was to assess how this variable influences bone health in children and adolescents. Studies that fulfilled the inclusion criteria, regardless of the number (although always >1) and ethnicity of participants and the duration of exposure, were eligible for inclusion in the review process. Potential confounding factors related to diet such as calcium and protein intake, soft drinks and dairy consumption were also included when data were available.
Two types of outcome measures were considered useful for evaluating bone status: BMC and BMD.
Results considered valid were those that included BMC or BMD measurements taken using DEXA and reported as absolute values or z-scores for the whole body, lumbar spine, femoral neck, or extremities; skeletal robustness (BSI measured in the calcaneus bone); SOS measured in the radius, tibia, or calcaneus; BUA measured in the calcaneus by quantitative ultrasound; and the anthropometric index FI [(elbow breadth in mm/ (height in cm) × 100]. Non measurable-data, such as evaluation of deformities on radiographs, were excluded.
The 10 studies finally included were selected independently by two authors from the 414 articles identified during the bibliographic search. In cases in which there was a lack of consensus the remaining authors acted as arbitrators.
Two authors independently collected data from the articles considered for review. The following data were extracted from each study: number, age and sex of participants, type of study, outcome measures, results, and conclusions. The remaining authors arbitrated in cases in which any discrepancies arose.
The risk of bias assessment was performed using the Newcastle-Ottawa quality assessment scale (36). This scale studies the risk of bias during participant selection, comparison between individuals, and exposure assessment. Based on the analysis of each of these risks each article is awarded a maximum of 9 stars, corresponding to the selection process (maximum, 4 stars), comparability between groups (maximum, 2 stars); and exposure assessment (maximum, 3 stars). Seven or more stars are considered indicative of a good quality study.
Results
The process by which articles were selected for this systematic review is summarized in Figure 1. The SCOPUS search returned 164 articles, while the PUBMED search identified a further 249 studies. One other article, identified in the manual review of the bibliography of the aforementioned articles, was also included. Of the 414 articles found in database searches, 6 duplicate articles were excluded, and 349 were excluded due to a lack of relevance of the abstract (129 lacked screen time data, 106 lacked bone health data, 65 were studies of adult populations, 27 recruited unhealthy individuals, 21 were narrative reviews, and 1 was a preclinical study). Of the 59 full-text articles reviewed, 45 were excluded due to a lack of screen time data; 2 due to unsuitable study characteristics; 1 due to the absence of bone health data; and 1 because the study population was exclusively adult (Supplementary Table 1). Ultimately, 10 articles (37–46) were selected for inclusion in this systematic review.
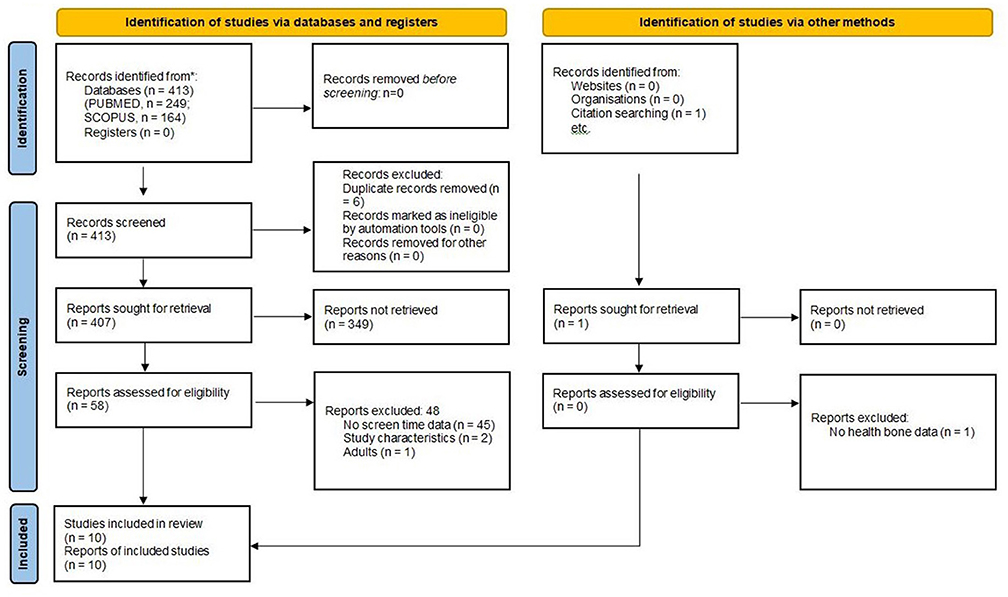
Figure 1. PRISMA 2020 flow diagram for systematic reviews which included searches of databases, registers, and other sources.
Study Characteristics
Tables 1–3 summarize the main characteristics of the 10 selected cohort and cross-sectional studies, which are ordered according to the age of the study population. Three cohort studies were included (40, 45, 46). All studies were published after 2004, and 4 in the last 5 years (37, 38, 41, 42). The combined study population of the 10 studies was 20,420 children and adolescents, of whom 18,444 participated in cross-sectional studies. The age of the study populations ranged from 2–22 years. All studies involved a pediatric population (range, 2–18 years) and 1 also included young adults up to 22 years of age (37). Four studies assessed the effects of total screen time on bone health (37–40), 7 the effects of TV viewing time on bone health (37, 39–44), and 6 the effects of recreational computer use on bone health (39, 41, 42, 44–46). Four studies used DEXA to evaluate bone health (38, 39, 42, 44), of which 2 measured BMC (39, 44) and the other 2 measured BMD (38, 42). Six studies used QUS (37, 40, 41, 43, 45, 46) to measure BSI (2 studies) (37, 41), SOS (3 studies) (40, 45, 46), FI (1 study) (43), or BUA (2 studies) (45, 46). In the selected studies screen time was measured as TV and/or computer time in hours/week in 4 studies (37, 41, 45, 46) and in minutes or hours/day in 6 studies (38–40, 42–44). One study (42) also analyzed videogame time in minutes/day and internet use for non-school purposes in minutes/day.
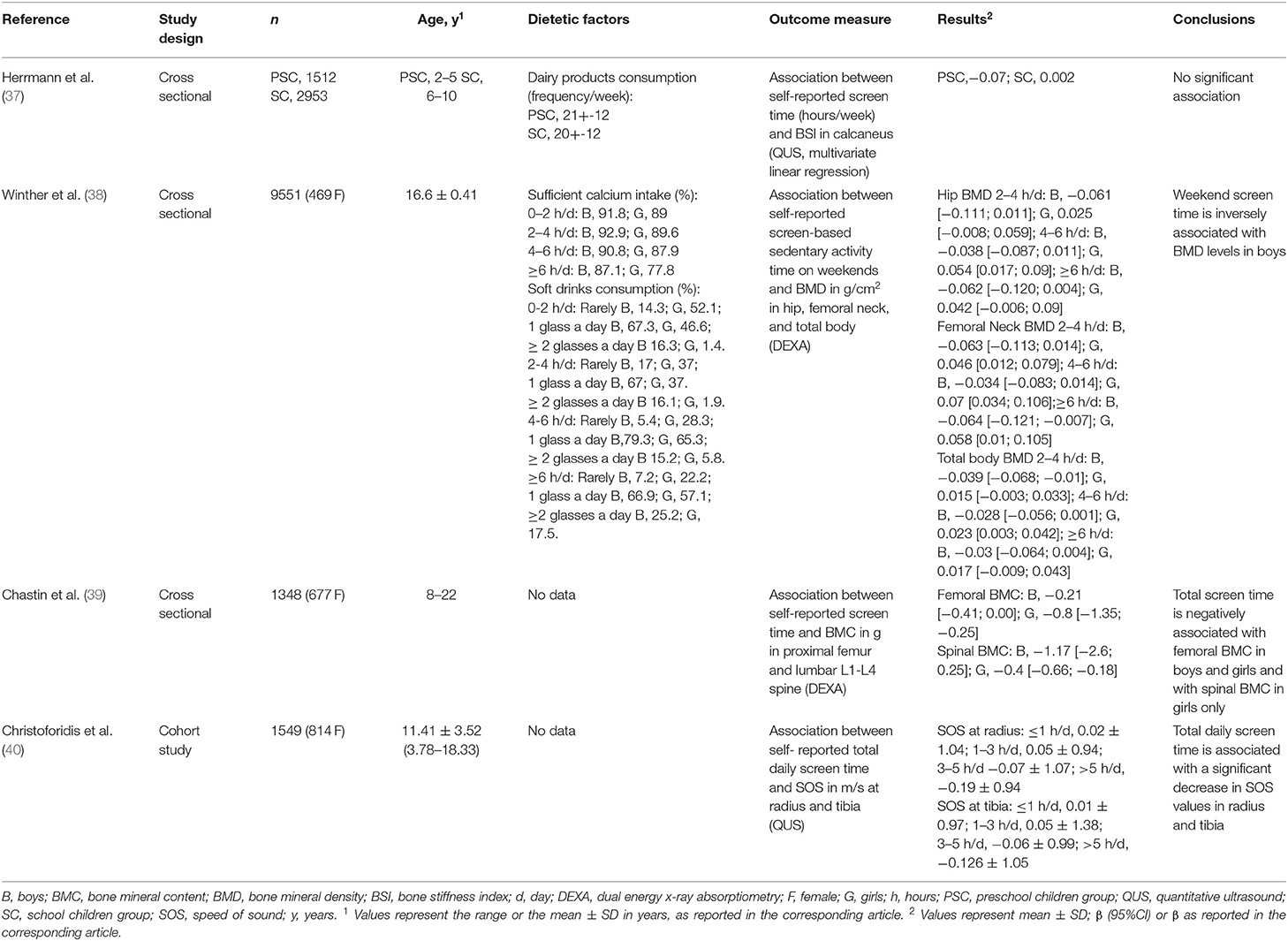
Table 1. Effects of total screen time on bone health.
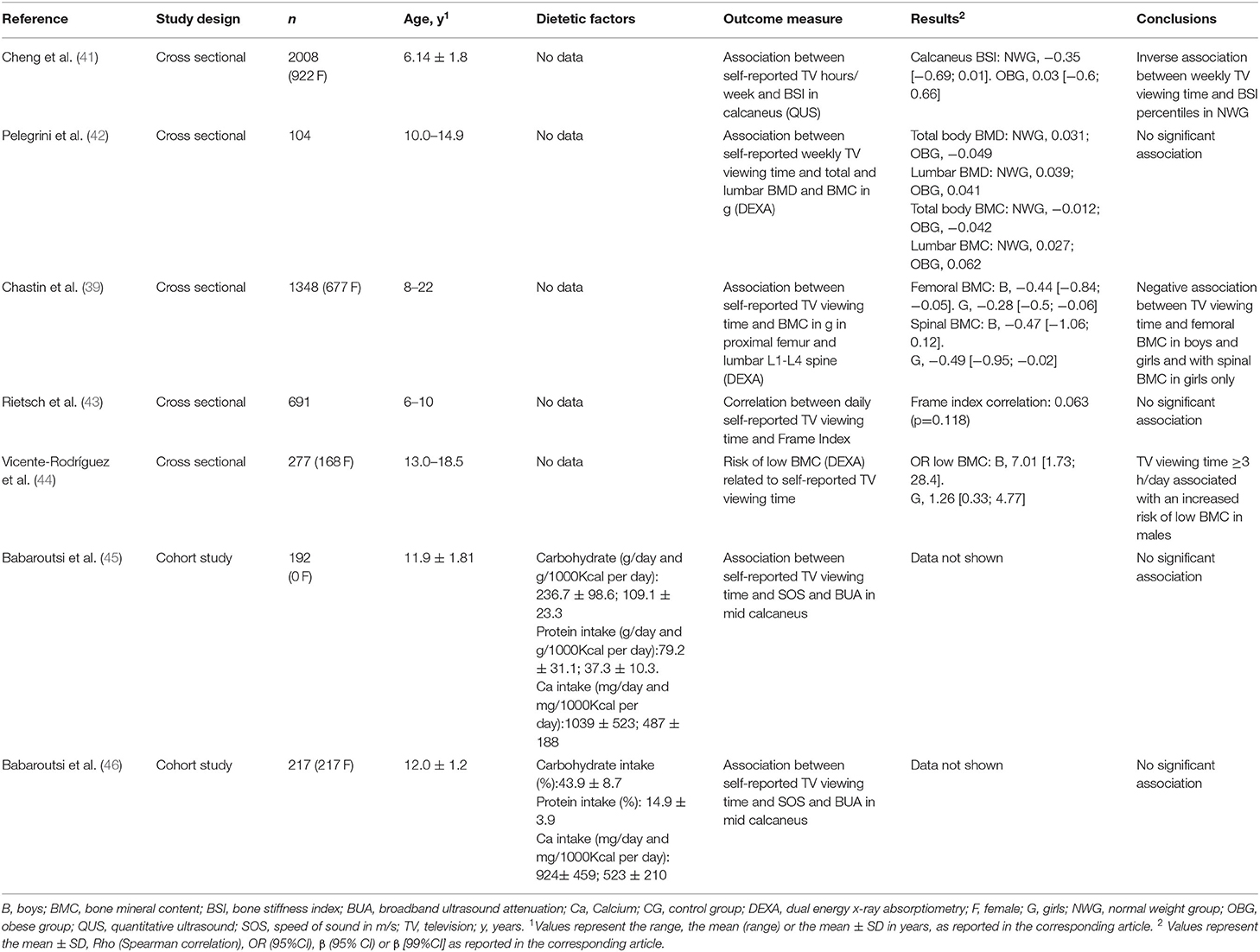
Table 2. Effects of television viewing time on bone health.
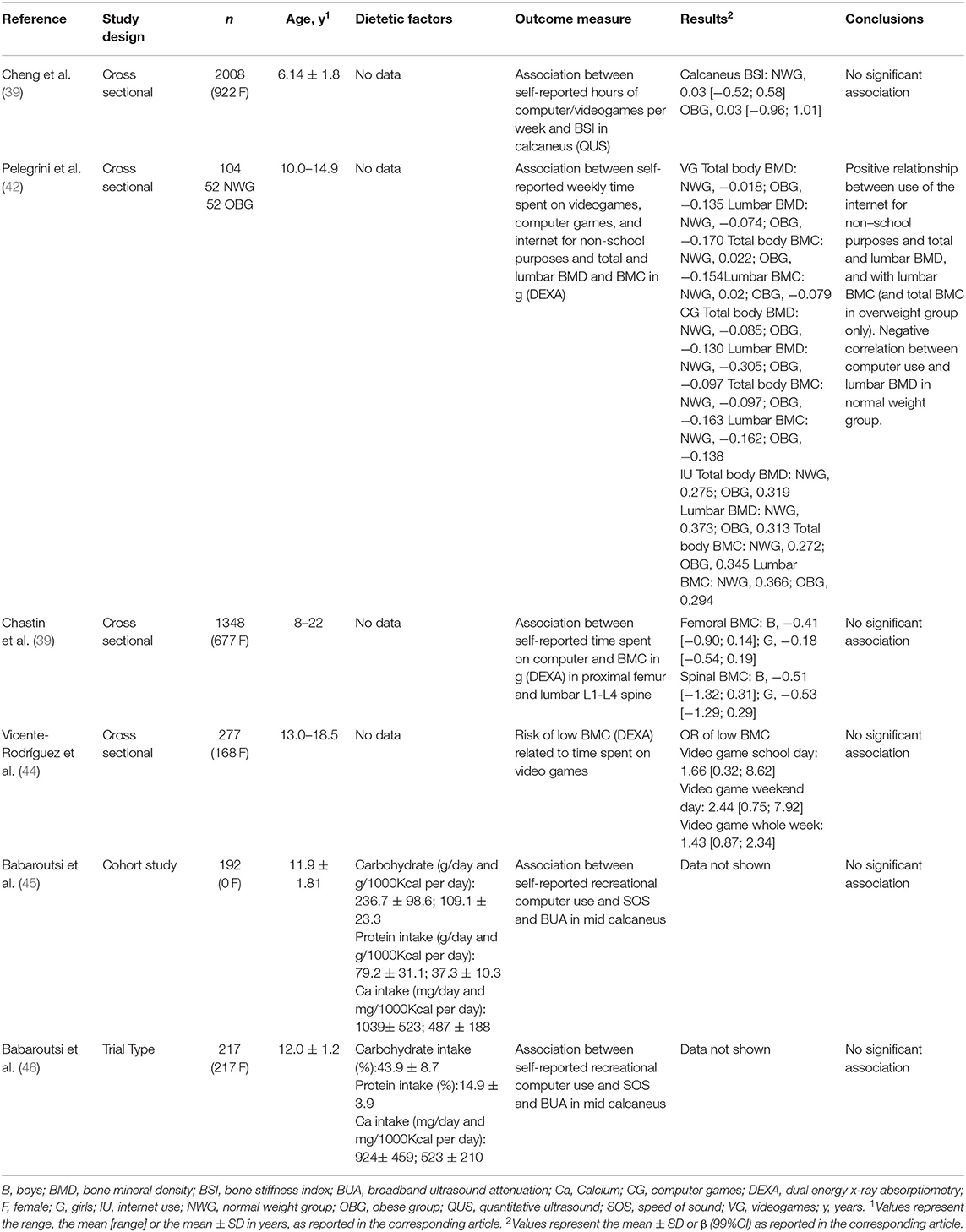
Table 3. Effects of recreational computer usage time on bone health.
Dietetic Factors
Only four studies (40%) (37, 38, 45, 46) included dietetic factors. Three of them assessed calcium intake (38, 45, 46) as sufficient calcium intake (%) (38) or absolute calcium intake (mg/day and mg/1000Kcal/day) (45, 46). No significant difference between calcium intake and screen time (38) or BUA and SOS (45, 46) was found in any of them. One included dairy products consumption (frequency/week) (37) and did not find any significant difference between preschool and school children and adolescent group but they did not assess its relation with bone status. One assessed soft drinks consumption (38) in glasses/day according to screen time during weekends, founding a significant positive relation in both sexes. Protein and carbohydrate intake (% and g/day) was assessed in males and females by Babaroutsi et al. (45, 46), and they did not found a significant difference when correlated with BUA and SOS.
Total Screen Time and Bone Health
Four articles included in this systematic review assessed the effects of total screen time on bone health (37–40). Three of the studies were cross-sectional (37–39) and 1 was a cohort study (40). Three articles (38–40) found a significant inverse association between screen time and bone health, as evidenced by decreased BMC (measured by DEXA in the proximal femur and the lumbar L1–L4 spine), BMD (measured by DEXA in the hip, femoral neck, and total body), and SOS (measured by QUS at radius and tibia), respectively. One study (37) found no significant association between screen time and bone health (BSI measured in the calcaneus by QUS). That study included the youngest population (preschool and school children aged 2–10 years).
TV Viewing Time and Bone Health
Seven studies included in this review evaluated the effects of TV viewing time on bone health (39, 41–46). Two of the 7 studies were cohort studies (45, 46) and 5 were cross-sectional studies (39, 41–44). Three reported a significant inverse association between bone health and TV viewing time (39, 41, 44): 2 described a decrease in BMC (measured by DEXA in the proximal femur and the lumbar L1-L4 spine) and 1 a decrease in BSI (measured in the calcaneus by QUS). The participants in the 2 studies that reported a negative association between TV viewing time and BMC were the oldest (18.5–22 years) of all the studies included in this review. Four studies (42, 43, 45, 46) reported no significant effect of TV viewing time on bone health, as determined by total and lumbar BMD and BMC, measured by DEXA (1 study) (42); FI (1 study) (43); and SOS and BUA measured at the mid calcaneus by QUS (2 studies) (45, 46).
Recreational Computer Time and Bone Health
Six studies included in this review evaluated the effects of recreational computer use on bone health (39, 41, 42, 44–46). Two of the 6 studies were cohort studies (45, 46) and 4 were cross-sectional studies (39, 41, 42, 44). Five articles reported no significant association between bone health and recreational computer use (39, 41, 44–46). Two measured BMC (proximal femur and lumbar L1-L4 spine) by DEXA (39, 44), 2 measured SOS and BUA in the mid-calcaneus by QUS (45, 46), and 1 measured BSI in the calcaneus by QUS (41). Only one study (40) found a negative correlation between computer use and lumbar BMD measured by DEXA in a group of children of normal weight (and between computer use and lumbar total BMC in the overweight group only). However, those authors reported a positive relationship between internet use for non-school purposes and total and lumbar BMD and lumbar BMC.
Risk-of-Bias Assessment
All the articles included in our review received at least 7 stars in the risk of bias assessment performed using the Newcastle-Ottawa scale, indicating that they were suitable for inclusion in the narrative analysis of the results. Four of these papers (38, 39, 42, 43) received 7 stars, while the remaining 6 (37, 40, 41, 44–46) received 8 stars.
All 10 articles included in the review received 2 stars for comparability between individuals. Following assessment of the risk of bias during the individual selection process, 6 of the 10 articles (37, 40, 41, 44–46) received 4 stars. The other 4 articles (38, 39, 42, 43) received 3 stars: in 3 cases (38, 39, 43) due to the absence of any description of measures taken to mitigate the risk of bias and in 1 case (42) because the study did not exclude individuals with chronic diseases that could interfere with the final result. Regarding screen exposure, all studies received 2 stars, as in all cases screen time was measured based on self-reporting or medical records (Supplementary Table 2).
Discussion
Recent technological advances have led to an increase in the use of screen-based technologies (screen time) by children and youth. This systematic review of observational studies assesses current evidence on the relationship between screen time and bone status in children and teenagers. The results suggest that total screen time is inversely associated with bone health in both groups. This effect persisted when only weekend screen time was considered. Moreover, we observed a negative correlation between TV viewing time and BMC and BSI, but no significant correlation between recreational computer usage time and bone health.
Environmental and lifestyle factors may markedly influence the achievement of genetic potential peak bone mass. Sedentary time, defined as time spent sitting or lying for extended periods of time, has become a global health concern in recent years (6–11). It is estimated that roughly half of children and youth (47) exceed the maximum screen time of 2 hours per day recommended by public health bodies (20), and even adolescents in the USA exceed 5 hours per day (18). A growing body of evidence associates excessive screen time with numerous deleterious outcomes, including obesity (11, 48), cardiometabolic risk (49), adverse sleep outcomes (13), visual (15) and psychological effects (50) with negative behavioral impacts, and lower self-esteem (51).
The ongoing worldwide coronavirus disease 2019 (COVID-19) pandemic and lockdown have markedly accentuated the trend toward increasing screen time, a consequence of a shift toward online working, educating, and socializing that will likely persist for the foreseeable future (52). This shift has coincided with a concomitant decrease in physical activity resulting from the epidemiological situation and temporary home confinement (53–56). Thus, in the short and medium term we can expect a potential global outbreak of adverse effects linked to excessive screen time. In this context, evaluation of the influence of screen time on bone health is particularly important.
Peak bone mass achieved during youth is the strongest predictor of osteoporosis risk in later life (57). Increased bone mass in childhood and youth is associated with the frequency and intensity of physical activity (58–60) due to the osteogenic effect of exercise. Physical activity mediates different changes beneficial to improve bone mass and promote bone formation (61). Exercise-mechanical loadings are essential stimuli for osteoblast differentiation and mineralization, regulate hormones and cytokines secretion that could play a role in bone metabolism (62), and promote bone angiogenic-osteogenic responses via the modulation of angiogenic mediators and signaling pathways (63, 64). Therefore, the progressive increase in the use of screens in recent years (65), as it increases the inactive time, is expected to have a negative influence on bone status, especially in late childhood and peripubertal years, a critical period for bone accretion.
Total and weekly screen time was negatively correlated with bone mass in 3 (38–40) of the 4 studies that evaluated these parameters. When analyzing TV viewing time this negative correlation was only observed in 50% of the studies included (39, 41, 44), and in 1 study that included males only (45). Only the study published by Vicente-Rodríguez et al. (44) offers data on the relative risk increase of low bone mineral content in relation to the time spent watching television in males, allowing us to calculate the fraction of risk attributable to television time, which corresponds to 85.7%. A notable finding was the absence of a negative association between recreational computer usage time and bone mass (39, 41, 44–46). One possible explanation for this observation is that playing videogames may involve greater energy expenditure, equating to mild-intensity exercise (66, 67), compared with watching TV, which does not increase the resting metabolic rate (68). However, this hypothesis does not explain the positive correlation observed in one study of adolescents between internet use for non-school purposes and BMD (42) unless, as the authors suggest, this use, which probably involves mobile devices, occurs while engaging in active behaviors.
An important aspect to consider is the added physical activity rate in this group of age. It should be noted that although screen time is traditionally associated with sedentary activities, it does not always preclude physical exercise. For example, in the study by Winther et al. (38) 20% of girls and 26% of boys for whom screen time exceeded 4 hours per day also spent more than 4 hours per week playing sports or engaged in high intensity physical activities. Moreover, screen time can also promote physical activity through platforms such as online physical activity classes, exercise applications on mobile devices, and video games with a physical activity component (69, 70). Therefore the individual contributions of sedentarism and physical activity should be distinguished (71). After adjustment by physical activity, some of the studies failed to detect an association between sedentary time and BMC (37, 44). There appears to be a positive association between bone health and a pattern of intermittent periods of sitting punctuated by moderate to vigorous activity (39).
In addition, screen time has been also linked to obesity (11), adiposity (72) and alterations in food and drink consumption, including increased consumption of carbonated drinks (38), sweets, and salty snacks (73–75) that could also influence bone health. Accordingly, Winther et al. found an association between soft drinks consumption and screen time in both sexes (38). However no significant differences between calcium, protein and carbohydrate intake with BUA and SOS were observed (45, 46). Another aspect essential for normal bone development and maintenance is vitamin D whose active form, 1α,25(OH)2D3, is involved in calcium regulation and bone homeostasis. The study in which a multivariate analysis of the relation between sedentary time, nutritional markers, and bone mass was performed, found that the risk of poor bone stiffness was highest in individuals who engaged in low levels of physical activity and had lower serum calcium or 25-OH vitamin D levels (37).
There are well recognized sex differences in bone accrual in terms of the timing of growth and maturation (76). An increased bone turnover was described in males compared to females across adolescence suggesting higher metabolic activity (77). Although screen time was globally higher in males in the reviewed studies (38, 39, 43), a sex-related trend in correlation between bone mass and screen time was observed in only 2 studies: Chastin et al. (39) reported a negative correlation between TV viewing time and femoral BMC in boys and girls and spinal BMC in girls only; and Vicente-Rodriguez et al. (44) reported that TV viewing time was positively associated with the risk of low BMC in males.
The cross-sectional and cohort studies included in this review differ in terms of the method employed to evaluate bone mass, the age range of the children and youth included, and the type of screen time considered (daily or weekly). Four of the studies (38, 39, 42, 44) evaluated BMC by DEXA in the lumbar spine and the neck of the femur, and Winther et al. (38) also evaluated total body BMC by DEXA; 2 studies (37, 41) analyzed BSI by QUS in the calcaneus or the radius and tibia; and the remaining studies analyzed BSI by SOS and BUA in the mid calcaneus (40, 45, 46) and FI (43).
Limitations of this systematic review that should be noted include those inherent to the observational nature of the evaluated studies, as well as the methodological differences in bone measurement and screen time quantification across studies. Likewise, it should be noted the limitations derived from having used only two databases, not having included articles published in languages other than English and Spanish, and not being able to perform meta-analysis due to the heterogeneity of the articles included in the revision. It is possible that negative effects on bone health are progressively accentuated with age, as suggested by the greater negative association between TV viewing time and bone health reported in studies that included older participants. Our findings underscore the need for further studies to assess the long-term effects of screen time on bone status.
Conclusions
The findings of this systematic review support a negative association between screen time and bone status in children and adolescents, with a different impact of the exposure of the considered technological devices. The studies reviewed revealed a negative correlation between TV viewing time and bone status, but no correlation between recreational computer usage time and bone health.
Osteoporosis is a major public health problem. Bone accretion during childhood and adolescence is a key factor to prevent it. The marked increased in screen time in recent years and its negative association with bone health may lead to an outbreak of this burden worldwide. Strategies promoting lifestyle modifications to achieve peak bone mass and strength should incorporate a multifactorial approach, including promotion of active and conscious use of digital technology.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
CL, MJ, and MC conceived the study and contributed to the design, methodology, and supervision of the study. PS-P wrote the first draft of the manuscript. MS and MC edited and reviewed the manuscript, and made important intellectual contributions. CL, MJ, and PS-P contributed to data selection and extraction, and the presentation of the results. All authors discussed, revised, and approved the final manuscript.
Funding
Fundación Instituto de Investigación Sanitaria de Santiago de Compostela.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2021.675214/full#supplementary-material
References
1. Rodrigues D, Gama A, Machado-Rodrigues AM, Nogueira H, Silva MG, Rosado-Marques V, et al. Social inequalities in traditional and emerging screen devices among Portuguese children: a cross-sectional study. BMC Public Health. (2020) 20:902. doi: 10.1186/s12889-020-09026-4
2. Munzer TG, Miller AL, Wang Y, Kaciroti N, Radesky JS. Tablets, toddlers and tantrums: the immediate effects of tablet device play. Acta Paediatr. (2021) 110:255–6. doi: 10.1111/apa.15509
3. Radesky J S, Weeks HM, Ball R, Schaller A, Yeo S, Durnez J, et al. Young children's use of smartphones and tablets. Pediatrics. (2020) 146:e20193518. doi: 10.1542/peds.2019-3518
4. Paudel S, Jancey J, Subedi N, Leavy J. Correlates of mobile screen media use among children aged 0-8: a systematic review. BMJ Open. (2017) 7:e014585. doi: 10.1136/bmjopen-2016-014585
5. Chen W, Adler JL. Assessment of screen exposure in young children, 1997 to 2014. JAMA Pediatr. (2019) 173:391–3. doi: 10.1001/jamapediatrics.2018.5546
6. Grontved A, Hu F B. Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: a meta-analysis. JAMA. (2011) 305:2448–55. doi: 10.1001/jama.2011.812
7. Lapierre MA, Rozendaal EA. Cross-national study examining the role of executive function and emotion regulation in the relationship between children's television exposure and consumer behavior. J Youth Adolesc. (2019) 48:1980–2004. doi: 10.1007/s10964-019-01119-7
8. Scarf D, Hinten AE. Television format and children's executive function. Pediatrics. (2018) 141:e20172674. doi: 10.1542/peds.2017-2674
9. Biddle SJH, García Bengoechea E, Pedisic Z, Bennie J, Vergeer I, Wiesner G. Screen time, other sedentary behaviours, and obesity risk in adults: a review of reviews. Curr Obes Rep. (2017) 6:134–47. doi: 10.1007/s13679-017-0256-9
10. Anderson DR, Subrahmanyam K. Cognitive impacts of digital media, W. Digital screen media and cognitive development. Pediatrics. (2017) 140:S57–61. doi: 10.1542/peds.2016-1758C
11. Gortmaker S L, Must A, Sobol AM, Colditz GA, Dietz WH. Television viewing as a cause of increasing obesity among children in the United States, 1986-1990. Arch Pediatr Adolesc Med. (1996) 150:356–62. doi: 10.1001/archpedi.1996.02170290022003
12. Domingues-Montanari S. Clinical and psychological effects of excessive screen time on children. J Paediatr Child Health. (2017) 53:333–8. doi: 10.1111/jpc.13462
13. Hale L, Guan S. Screen time and sleep among school-aged children and adolescents: a systematic literature review. Sleep Med Rev. (2015) 21:50–8. doi: 10.1016/j.smrv.2014.07.007
14. Li X, Buxton OM, Lee S, Chang AM, Berger LM, Hale L. Sleep mediates the association between adolescent screen time and depressive symptoms. Sleep Med. (2019) 57:51–60. doi: 10.1016/j.sleep.2019.01.029
15. Kim J, Hwang Y, Kang S, Kim M, Kim TS, Kim J. Association between exposure to smartphones and ocular health in adolescents. Ophthalmic Epidemiol. (2016) 23:269–76. doi: 10.3109/09286586.2015.1136652
16. Li SM, Li SY, Kang MT, Zhou Y, Liu LR, Li H, et al. Near work related parameters and myopia in Chinese children: the anyang childhood eye study. PLoS ONE. (2015) 10:e0134514. doi: 10.1371/journal.pone.0134514
17. Delfino LD, Tebar WR, Silva DAS, Gil FCS, Mota J, Christofaro DGD. Food advertisements on television and eating habits in adolescents: a school-based study. Rev Saude Publica. (2020) 54:55. doi: 10.11606/s1518-8787.2020054001558
18. Kenney E L, Gortmaker SL. United States adolescents' television, computer, videogame, smartphone, and tablet use: associations with sugary drinks, sleep, physical activity, and obesity. J Pediatr. (2017) 182:144–9. doi: 10.1016/j.jpeds.2016.11.015
19. Nucci D, Rabica F, Dallagiacoma G, Fatigoni C, Gianfredi V. Are the Italian children exposed to advertisements of nutritionally appropriate foods? Foods. (2020) 9:1632. doi: 10.3390/foods9111632
20. Guram S, Heinz P. Media use in children: American Academy of Pediatrics recommendations 2016. Arch Dis Child Educ Pract Ed. (2018) 103:99–101. doi: 10.1136/archdischild-2017-312969
21. O'Connor TM, Chen TA, del Rio Rodriguez B, Hughes SO. Psychometric validity of the parent's outcome expectations for children's television viewing (POETV) scale. BMC Public Health. (2014) 14:894. doi: 10.1186/1471-2458-14-894
22. Jago R, Edwards M J, Urbanski CR, Sebire S J. General and specific approaches to media parenting: a systematic review of current measures, associations with screen-viewing, and measurement implications. Child Obes. (2013) 9:S51–72. doi: 10.1089/chi.2013.0031
23. Jago R, Wood L, Zahra J, Thompson JL, Sebire SJ. Parental control, nurturance, self-efficacy, and screen viewing among 5- to 6-year-old children: a cross-sectional mediation analysis to inform potential behavior change strategies. Child Obes. (2015) 11:139–47. doi: 10.1089/chi.2014.0110
24. Xu H, Wen LM, Rissel C. Associations of parental influences with physical activity and screen time among young children: a systematic review. J Obes. (2015) 2015:546925. doi: 10.1155/2015/546925
25. Kubik MY, Gurvich OV, Fulkerson JA. Association between parent television-viewing practices and setting rules to limit the television-viewing time of their 8- to 12-year-old children, Minnesota, 2011-2015. Prev Chronic Dis. (2017) 14:E06. doi: 10.5888/pcd14.160235
26. McVeigh JA, Zhu K, Mountain J, Pennell CE, Lye SJ, Walsh JP, et al. Longitudinal trajectories of television watching across childhood and adolescence predict bone mass at age 20 years in the raine study. J Bone Miner Res. (2016) 31:2032–40. doi: 10.1002/jbmr.2890
27. Ye S, Song A, Yang M, Ma X, Fu X, Zhu S. Duration of television viewing and bone mineral density in Chinese women. J Bone Miner Metab. (2014) 32:324–30. doi: 10.1007/s00774-013-0504-3
28. Rizzoli R, Biver E, Bonjour JP, Coxam V, Goltzman D, Kanis JA, et al. Benefits and safety of dietary protein for bone health-an expert consensus paper endorsed by the European Society for Clinical and Economical Aspects of Osteopororosis, Osteoarthritis, and Musculoskeletal Diseases and by the International Osteoporosis Foundation. Osteoporos Int. (2018) 29:1933–48. doi: 10.1007/s00198-018-4534-5
29. Weaver CM, Gordon CM, Janz KF, Kalkwarf HJ, Lappe JM, Lewis R, et al. The National Osteoporosis Foundation's position statement on peak bone mass development and lifestyle factors: a systematic review and implementation recommendations. Osteoporos Int. (2016) 27:1281–386. doi: 10.1007/s00198-015-3440-3
30. Ward LM, Weber D R, Munns CF, Högler W, Zemel BS. A contemporary view of the definition and diagnosis of osteoporosis in children and adolescents. J Clin Endocrinol Metab. (2020) 105:e2088–97. doi: 10.1210/clinem/dgz294
31. Moayyeri A, Adams JE, Adler RA, Krieg MA, Hans D, Compston J, et al. Quantitative ultrasound of the heel and fracture risk assessment: an updated meta-analysis. Osteoporos Int. (2012) 23:143–53. doi: 10.1007/s00198-011-1817-5
32. Steiner B, Dimai H P, Steiner H, Cirar S, Fahrleitner-Pammer A. Prescreening for osteoporosis with quantitative ultrasound in postmenopausal white women. J Ultrasound Med. (2019) 38:1553–9. doi: 10.1002/jum.14844
33. Schraders K, Zatta G, Kruger M, Coad J, Weber J, Brough L, et al. Quantitative ultrasound and dual X-ray absorptiometry as indicators of bone mineral density in young women and nutritional factors affecting it. Nutrients. (2019) 11:2336. doi: 10.3390/nu11102336
34. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. (2016) 354:i4086. doi: 10.1136/bmj.i4086
35. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
36. Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hosp Resea Insti. (2014). Available online at: www.ohri.ca/programs/clinical_epidemiology/oxford.asp
37. Herrmann D, Buck C, Sioen I, Kouride Y, Marild S, Molnár D, et al. Impact of physical activity, sedentary behaviour and muscle strength on bone stiffness in 2-10-year-old children-cross-sectional results from the IDEFICS study. Int J Behav Nutr Phys Act. (2015) 12:112. doi: 10.1186/s12966-015-0273-6
38. Winther A, Ahmed LA, Furberg AS, Grimnes G, Jorde R, Nilsen OA, et al. Leisure time computer use and adolescent bone health–findings from the Tromso Study, Fit Futures: a cross-sectional study. BMJ Open. (2015) 5:e006665. doi: 10.1136/bmjopen-2014-006665
39. Chastin S F, Mandrichenko O, Skelton DA. The frequency of osteogenic activities and the pattern of intermittence between periods of physical activity and sedentary behaviour affects bone mineral content: the cross-sectional NHANES study. BMC Public Health. (2014) 14:4. doi: 10.1186/1471-2458-14-4
40. Christoforidis A, Papadopoulou E, Dimitriadou M, Stilpnopoulou D, Gkogka C, Katzos G, et al. Reference values for quantitative ultrasonography (QUS) of radius and tibia in healthy greek pediatric population: clinical correlations. J Clin Densitom. (2009) 12:360–8. doi: 10.1016/j.jocd.2009.03.097
41. Cheng L, Pohlabeln H, Ahrens W, Lauria F, Veidebaum T, Chadjigeorgiou C, et al. Cross-sectional and longitudinal associations between physical activity, sedentary behaviour and bone stiffness index across weight status in European children and adolescents. Int J Behav Nutr Phys Act. (2020) 17:54. doi: 10.1186/s12966-020-00956-1
42. Pelegrini A, Klen JA, Costa AM, Bim MA, Claumann GS, De Angelo HCC, et al. Association between sedentary behavior and bone mass in adolescents. Osteoporos Int. (2020) 31:733–1740. doi: 10.1007/s00198-020-05412-1
43. Rietsch K, Eccard JA, Scheffler C. Decreased external skeletal robustness due to reduced physical activity? Am J Hum Biol. (2013) 25:404–10. doi: 10.1002/ajhb.22389
44. Vicente-Rodriguez G, Ortega FB, Rey-López JP, et al. Extracurricular physical activity participation modifies the association between high TV watching and low bone mass. Bone. (2009) 45:925–30. doi: 10.1016/j.bone.2009.07.084
45. Babaroutsi E, Magkos F, Manios Y, Sidossis LS. Body mass index, calcium intake, and physical activity affect calcaneal ultrasound in healthy Greek males in an age-dependent and parameter-specific manner. J Bone Miner Metab. (2005) 23:157–66. doi: 10.1007/s00774-004-0555-6
46. Babaroutsi E, Magkos F, Manios Y, Sidossis LS. Lifestyle factors affecting heel ultrasound in Greek females across different life stages. Osteoporos Int. (2005) 16:552–61. doi: 10.1007/s00198-004-1720-4
47. Saunders TJ, Vallance JK. Screen Time and Health Indicators Among Children and Youth: Current Evidence, Limitations and Future Directions. Appl Health Econ Health Policy. (2017) 15:323–31. doi: 10.1007/s40258-016-0289-3
48. Viner RM, Cole TJ. Television viewing in early childhood predicts adult body mass index. J Pediatr. (2005) 147:429–35. doi: 10.1016/j.jpeds.2005.05.005
49. Kang HT, Lee HR, Shim JY, Shin YH, Park BJ, Lee YJ. Association between screen time and metabolic syndrome in children and adolescents in Korea: the 2005 Korean National Health and Nutrition Examination Survey. Diabetes Res Clin Pract. (2010) 89:72–8. doi: 10.1016/j.diabres.2010.02.016
50. Lissak G. Adverse physiological and psychological effects of screen time on children and adolescents: Literature review and case study. Environ Res. (2018) 164:149–57. doi: 10.1016/j.envres.2018.01.015
51. Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput JP, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. (2016) 41:S240–265. doi: 10.1139/apnm-2015-0630
52. Hoehe MR, Thibaut F. Going digital: how technology use may influence human brains and behavior. Dialogues Clin Neurosci. (2020) 22:93–7. doi: 10.31887/DCNS.2020.22.2/mhoehe
53. Xiang M, Zhang Z, Kuwahara K. Impact of COVID-19 pandemic on children and adolescents' lifestyle behavior larger than expected. Prog Cardiovasc Dis. (2020) 63:531–2. doi: 10.1016/j.pcad.2020.04.013
54. Lopez-Bueno R, Calatayud J, Casaña J, Casajús JA, Smith L, Tully MA, et al. COVID-19 Confinement and Health Risk Behaviors in Spain. Front Psychol. (2020) 11:1426. doi: 10.3389/fpsyg.2020.01426
55. Pietrobelli A, Pecoraro L, Ferruzzi A. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: a longitudinal study. Obesity (Silver Spring). (2020) 28:1382–5. doi: 10.1002/oby.22861
56. Carroll N, Sadowski A, Laila A, Hruska V, Nixon M, Ma DWL, et al. The impact of COVID-19 on health behavior, stress, financial and food security among middle to high income Canadian families with young children. Nutrients. (2020) 12:2352. doi: 10.3390/nu12082352
57. Hernandez C J, Beaupre G S, Carter DR. A theoretical analysis of the relative influences of peak BMD, age-related bone loss and menopause on the development of osteoporosis. Osteoporos Int. (2003) 14:843–7. doi: 10.1007/s00198-003-1454-8
58. Linden C, Ahlborg HG, Besjakov J, Gardsell P, Karlsson MK. A school curriculum-based exercise program increases bone mineral accrual and bone size in prepubertal girls: two-year data from the pediatric osteoporosis prevention (POP) study. J Bone Miner Res. (2006) 21:829–35. doi: 10.1359/jbmr.060304
59. Gracia-Marco L, Moreno LA, Ortega FB, León F, Sioen I, Kafatos A, et al. Levels of physical activity that predict optimal bone mass in adolescents: the HELENA study. Am J Prev Med. (2011) 40:599–607. doi: 10.1016/j.amepre.2011.03.001
60. Ronne MS, Heidemann M, Lylloff L, Schou AJ, Tarp J, Laursen JO, et al. Bone mass development in childhood and its association with physical activity and vitamin D levels the CHAMPS-study. DK Calcif Tissue Int. (2019) 104:1–13. doi: 10.1007/s00223-018-0466-5
61. Tong X, Chen X, Zhang S, Huang M, Shen X, Xu J, et al. The effect of exercise on the prevention of osteoporosis and bone angiogenesis. Biomed Res Int. (2019) 2019:8171897. doi: 10.1155/2019/8171897
62. Prisby RD. Mechanical, hormonal and metabolic influences on blood vessels, blood flow and bone. J Endocrinol. (2017) 235:R77–R100. doi: 10.1530/JOE-16-0666
63. Yao Z, Lafage-Proust MH, Plouët J, Bloomfield S, Alexandre C, Vico L. Increase of both angiogenesis and bone mass in response to exercise depends on VEGF. J Bone Miner Res. (2004) 19:1471–80. doi: 10.1359/JBMR.040517
64. MacKenzie MG, Hamilton DL, Pepin M, Patton A, Baar K. Inhibition of myostatin signaling through Notch activation following acute resistance exercise. PLoS ONE. (2013) 8:e68743. doi: 10.1371/journal.pone.0068743
65. Garcia-Soidan J L, Leiros-Rodriguez R, Romo-Perez V, Arufe-Giraldez V. Evolution of the habits of physical activity and television viewing in Spanish children and pre-adolescents between 1997 and 2017. Int J Environ Res Public Health. (2020) 17:6836. doi: 10.3390/ijerph17186836
66. Segal KR, Dietz WH. Physiologic responses to playing a video game. Am J Dis Child. (1991) 145:1034–6. doi: 10.1001/archpedi.1991.02160090086030
67. Gomez DH, Bagley JR, Bolter N, Kern M, Lee CM. Metabolic cost and exercise intensity during active virtual reality gaming. Games Health J. (2018) 7:310–6. doi: 10.1089/g4h.2018.0012
68. Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. (2000) 32:S498–504. doi: 10.1097/00005768-200009001-00009
69. Bock BC, Dunsiger SI, Ciccolo JT, Serber ER, Wu WC, Tilkemeier P, et al. Exercise videogames, physical activity, and health: wii heart fitness: a randomized clinical trial. Am J Prev Med. (2019) 56:501–11. doi: 10.1016/j.amepre.2018.11.026
70. Nagata JM, Abdel Magid H S, Pettee Gabriel K. Screen time for children and adolescents during the coronavirus disease 2019 pandemic. Obesity (Silver Spring). (2020) 28:1582–3. doi: 10.1002/oby.22917
71. Gabel L, McKay H A, Nettlefold L, Race D, Macdonald HM. Bone architecture and strength in the growing skeleton: the role of sedentary time. Med Sci Sports Exerc. (2015) 47:363–72. doi: 10.1249/MSS.0000000000000418
72. Gállego Suárez C, Singer BH, Gebremariam A, Lee JM, Singer K. The relationship between adiposity and bone density in US children and adolescents. PLoS ONE. (2017) 12:e0181587. doi: 10.1371/journal.pone.0181587
73. Bornhorst C, Wijnhoven TM, Kunešová M, Yngve A, Rito AI, Lissner L, et al. WHO European Childhood Obesity Surveillance Initiative: associations between sleep duration, screen time and food consumption frequencies. BMC Public Health. (2015) 15:442. doi: 10.1186/s12889-015-1793-3
74. Kelishadi R, Mozafarian N, Qorbani M, Maracy MR, Motlagh ME, Safiri S, et al. Association between screen time and snack consumption in children and adolescents: the CASPIAN-IV study. J Pediatr Endocrinol Metab. (2017) 30:211–9. doi: 10.1515/jpem-2016-0312
75. Boylan S, Hardy LL, Drayton BA, Grunseit A, Mihrshahi S. Assessing junk food consumption among Australian children: trends and associated characteristics from a cross-sectional study. BMC Public Health. (2017) 17:299. doi: 10.1186/s12889-017-4207-x
76. McCormack SE, Cousminer DL, Chesi A, Mitchell JA, Roy SM, Kalkwarf HJ, et al. Association between linear growth and bone accrual in a diverse cohort of children and adolescents. JAMA Pediatr. (2017) 171:e171769. doi: 10.1001/jamapediatrics.2017.1769
Keywords: bone mineral density, computer, mobile phone, screen, tablets, bone turnover
Citation: de Lamas C, Sánchez-Pintos P, José de Castro M, Sáenz de Pipaon M and Couce ML (2021) Screen Time and Bone Status in Children and Adolescents: A Systematic Review. Front. Pediatr. 9:675214. doi: 10.3389/fped.2021.675214
Received: 02 March 2021; Accepted: 11 November 2021;
Published: 01 December 2021.
Edited by:
Andrea Deregibus, Politecnico di Torino, ItalyReviewed by:
Vincenza Gianfredi, Vita-Salute San Raffaele University, ItalyWalter A. Mihatsch, Ulm University Medical Center, Germany
Copyright © 2021 de Lamas, Sánchez-Pintos, José de Castro, Sáenz de Pipaon and Couce. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Luz Couce, bWFyaWEubHV6LmNvdWNlLnBpY29Ac2VyZ2FzLmVz
†These authors have contributed equally to this work and share first authorship