 Omar Sepúlveda-Robles1
Omar Sepúlveda-Robles1 Elva Jiménez-Hernández2
Elva Jiménez-Hernández2 Victoria Domínguez-Catzín3Eber Gómez-Flores3Jorge Alfonso Martín-Trejo4
Victoria Domínguez-Catzín3Eber Gómez-Flores3Jorge Alfonso Martín-Trejo4 Janet Flores-Lujano5
Janet Flores-Lujano5 José Refugio Torres-Nava6
José Refugio Torres-Nava6 Juan Carlos Núñez-Enríquez5
Juan Carlos Núñez-Enríquez5 Marlon De Ita1Aurora Medina-Sanson7
Marlon De Ita1Aurora Medina-Sanson7 Minerva Mata-Rocha1Blanca Angelica Morales-Castillo1
Minerva Mata-Rocha1Blanca Angelica Morales-Castillo1 Juan Carlos Bravata-Alcántara8
Juan Carlos Bravata-Alcántara8 Alan Steve Nájera-Cortés8
Alan Steve Nájera-Cortés8 Norberto Sánchez-Escobar9
Norberto Sánchez-Escobar9 José Gabriel Peñaloza-Gonzalez10
José Gabriel Peñaloza-Gonzalez10 Rosa Martha Espinosa-Elizondo11Luz Victoria Flores-Villegas12Raquel Amador-Sanchez13Darío Orozco-Ruiz6
Rosa Martha Espinosa-Elizondo11Luz Victoria Flores-Villegas12Raquel Amador-Sanchez13Darío Orozco-Ruiz6 Maria Luisa Pérez-Saldívar5Martha Margarita Velázquez-Aviña10Laura Elizabeth Merino-Pasaye12Karina Anastacia Solís-Labastida4Ana Itamar González-Ávila13Jessica Denisse Santillán-Juárez14
Maria Luisa Pérez-Saldívar5Martha Margarita Velázquez-Aviña10Laura Elizabeth Merino-Pasaye12Karina Anastacia Solís-Labastida4Ana Itamar González-Ávila13Jessica Denisse Santillán-Juárez14 Vilma Carolina Bekker-Méndez15
Vilma Carolina Bekker-Méndez15 Silvia Jiménez-Morales16
Silvia Jiménez-Morales16 Angélica Rangel-López17
Angélica Rangel-López17 Haydeé Rosas-Vargas1*
Haydeé Rosas-Vargas1* Juan Manuel Mejía-Aranguré16,17,18*
Juan Manuel Mejía-Aranguré16,17,18*
- 1Unidad de Investigación Médica en Genética Humana, UMAE Hospital de Pediatría, Centro Médico Nacional “Siglo XXI”, Instituto Mexicano del Seguro Social (IMSS), Mexico City, Mexico
- 2Servicio de Hematología Pediátrica, Hospital General “Gaudencio González Garza”, Centro Médico Nacional “La Raza”, Instituto Mexicano del Seguro Social (IMSS), Mexico City, Mexico
- 3Genes & Care, Centro de Diagnóstico Molecular, Mexico City, Mexico
- 4Servicio de Hematología Pediátrica, UMAE Hospital de Pediatría, Centro Médico Nacional “Siglo XXI”, Instituto Mexicano del Seguro Social (IMSS), Mexico City, Mexico
- 5Unidad de Investigación Médica en Epidemiología Clínica, UMAE Hospital de Pediatría, Centro Médico Nacional “Siglo XXI”, Instituto Mexicano del Seguro Social (IMSS), Mexico City, Mexico
- 6Servicio de Oncología, Hospital Pediátrico de Moctezuma, Secretaría de Salud de la Ciudad de México, Mexico City, Mexico
- 7Servicio de Hemato-Oncología, Hospital Infantil de México Federico Gómez, Secretaría de Salud (SSa), Mexico City, Mexico
- 8Laboratorio de Genética y Diagnóstico Molecular, Hospital Juárez de México, Secretaría de Salud (SSa), Mexico City, Mexico
- 9Facultad de Medicina y Cirugía, Universidad Autónoma “Benito Juárez” de Oaxaca, Oaxaca City, Mexico
- 10Servicio de Onco-Pediatría, Hospital Juárez de México, Secretaría de Salud (SSa), Mexico City, Mexico
- 11Servicio de Hematología Pediátrica, Hospital General de México, Secretaría de Salud (SSa), Mexico City, Mexico
- 12Servicio de Hematología Pediátrica, Centro Médico Nacional “20 de Noviembre”, Instituto de Seguridad Social al Servicio de los Trabajadores del Estado (ISSSTE), Mexico City, Mexico
- 13Hospital General Regional No. 1 “Carlos McGregor Sánchez Navarro”, Instituto Mexicano del Seguro Social (IMSS), Mexico City, Mexico
- 14Servicio de Hemato-Oncología Pediatrica, Hospital Regional 1° de Octubre, Instituto de Seguridad Social al Servicio de los Trabajadores del Estado (ISSSTE), Mexico City, Mexico
- 15Unidad de Investigación Médica en Inmunología e Infectología, Hospital de Infectología “Dr. Daniel Méndez Hernández”, Centro Médico Nacional “La Raza”, Instituto Mexicano del Seguro Social (IMSS), Mexico City, Mexico
- 16Laboratorio de Genómica del Cáncer, Instituto Nacional de Medicina Genómica, Mexico City, Mexico
- 17Coordinación de Investigación en Salud, Instituto Mexicano del Seguro Social (IMSS), Mexico City, Mexico
- 18Facultad de Medicina, Universidad Nacional Autónoma de México (UNAM), Mexico City, Mexico
Background: The distribution of RUNX1-RUNXT1, PML-RARA, CBFB-MYH11, BCR-ABL1p210, and KMT2A-MLLT3 in the pediatric population with acute myeloid leukemia (AML) in many countries of Latin America is largely unknown. Therefore, we aimed to investigate the frequency of these fusion genes in children with de novo AML from Mexico City, which has one of the highest incidence rates of acute leukemia in the world. Additionally, we explored their impact in mortality during the first year of treatment.
Methods: We retrospectively analyzed the presence of RUNX1-RUNXT1, PML-RARA, CBFB-MYH11, BCR-ABL1p210, and KMT2A-MLLT3 by RT-PCR among 77 patients (<18 years) diagnosed with de novo AML between 2019 and 2021 in nine Mexico City hospitals.
Results: The overall frequency of the fusion genes was 50.7%; RUNX1-RUNXT1 (22.1%) and PML-RARA (20.8%) were the most prevalent, followed by CBFB-MYH11 (5.2%) and BCR-ABL1p210 (2.4%). KMT2A-MLLT3 was not detected. Patients with PML-RARA showed the lowest survival with high early mortality events. However, more studies are required to evaluate the impact of analyzed fusion genes on the overall survival of the Mexican child population with AML.
Conclusion: The pediatric population of Mexico City with AML had frequencies of AML1-ETO, PML-RARA, CBFB-MYH11, and BCR-ABL1p210 similar to those of other populations around the world. Patients with BCR-ABL1p210and CBFB-MYH11 were few or did not die, while those with MLL-AF9 was not detected. Although patients with PML-RARA had a low survival and a high early mortality rate, further studies are needed to determine the long-term impacts of these fusion genes on this Latino population.
Introduction
The Acute myeloid leukemia (AML) represents ∼20% of acute leukemia cases in children and 80% in adults (1). Although AML in children and adolescents does not affect a great number of patients, its lethality is the highest amongst those of acute leukemias, with a global 5-year net survival of ∼42.9% and a maximum achievable survival of 73.1% (2). Among Hispanics, the population of Mexico City has one of the highest incidence rates, with an adjusted average annual incidence rate of 8.18 per million for children under the age of 15 years, which has been increasing for the last 10 years (3, 4).
The five most common chromosomal translocations in patients with AML are t(8;21), t(15;17), inv(16), der(11), and t(9;22), which encode the fusion genes RUNX1-RUNXT1 (AML1-ETO), PML-RARA, CBFB-MYH11, MLL-fusions, and BCR-ABL1, respectively (5). The identification of which is useful for stratifying patients, revealing prognoses, and making decisions regarding treatment protocols (5). The frequency of this fusion genes in pediatric patients is ∼50%, which is much higher than that in adults (6–9), and their individual frequencies range from 3 to 20% (5). Patients with AML1-ETO, PML-RARA, and CBFB-MYH11 tend to have favorable outcomes; therefore, they are not recommended for stem cell transplantation at first complete remission (5). By contrast, patients who harbor MLL fusion genes tend to have intermediate to poor prognoses (10). Importantly, the WHO classification categorizes the specific fusion gene MLL-AF9 as an entity and recommends that the partners in the variant MLL fusion genes should be identified; however, MLL-AF9 is one of the most common fusion gene presented in patients with AML (10, 11). The presence of BCR-ABL1 in de novo AML cases appears to be a rare disease subtype (0.5%–3%) that is apparently related to induction failures and relapses (12).
Despite its manifest clinical relevance, the distribution of these fusion genes in the pediatric population in Mexico with AML is largely unknown. Studies performed in Mexican patients have been conducted with small population sizes or have been limited to specific fusion genes, such as AML1-ETO or PML-RARA (13–15). Regarding CBFB-MYH11, MLL fusions, or BCR-ABL1, there are no data, or the few studies performed have considered patients from individual hospitals without population-level information (13–16). Given the high incidence of AML in Mexican children, as well as the importance of knowing the epidemiological behavior of AML1-ETO, PML-RARA, CBFB-MYH11, MLL-AF9, and BCR-ABL1p210 for diagnosis and best treatment selection, the aims of this multicenter study performed by the Mexican Interinstitutional Group for the Identification of the Causes of Childhood Leukemia (MIGICCL) were to determine the frequencies of these five common fusion genes in children with AML from Mexico City. Additionally, we explored their impact in mortality during the first year of treatment.
Materials and methods
Patients, hospitals, and clinical data
A total of 77 children under 18 years old newly diagnosed with AML were recruited between January 2019 and June 2021, from nine hospitals belonged to four Mexican Health Institutions: (1) Secretaría de Salud del Distrito Federal (Hospital Pediátrico de Moctezuma), (2) Instituto de Seguridad Social al Servicio de los Trabajadores del Estado (Hospital Regional No. 1 de Octubre and Centro Médico Nacional 20 de Noviembre), (3) Secretaría de Salud (Hospital General de México Dr. Eduardo Liceaga, Hospital Infantil de México Federico Gómez, and Hospital Juárez de México), and (4) Instituto Mexicano del Seguro Social (Hospital de Pediatría, Centro Médico Nacional Siglo XXI, Centro Médico Nacional La Raza, and Hospital General Regional No. 1 Carlos Mac Gregor Sánchez Navarro). Information regarding sex, age, white blood cell (WBC) count at diagnosis, morphological subtype, and immunophenotype was collected from the patients' clinical records. Patients were treated with protocols PETHEMA-APL05 (n = 13), NOPHO-AML93 (n = 18), BFM-2001 (n = 20), or BFM-1998 (n = 26), were categorized into the age groups: infants <2 years; children: 2 to <13 years; and adolescents: 13 to <18 years (17).
RNA isolation, cDNA synthesis, and fusion gene detection by PCR
Total RNA was isolated from mononuclear cells using Direct-zol RNA MiniPrep kit (Zymo Research), and its quality was confirmed by visualization of intact 28S and 18S bands in agarose gels. Reverse transcription reaction was carried out using 500 ng of total RNA and the iScript Reverse Transcription Supermix (Bio-Rad). All PCR reactions were performed using Multiplex TEMPase 2× Master Mix (Ampliqon), using a start incubation step at 95°C for 15 min, and 35 cycles. Then, reactions for AML1-ETO, PML-RARA(bcr1, bcr2), and CBFB-MYH11 were incubated at 94°C/45 s, 63°C/1 min, 72°C/1:30 min, 72°C/5 min; BCR-ABL1p210 was incubated at 96°C/30 s, 60°C/45 s, 72°C/1 min, 72°C/5 min; MLL-AF9 was incubated at 94°C/1 min, 60°C/1 min, 72°C/1 min, 72°C/5 min. PML-RARA(bcr3) was detected in a separately reaction with incubation at 94°C/30 s, 65°C/1 min, 72°C/1 min, 72°C/5 min. Oligonucleotide sequences described previously were used for detection of AML1-ETO (Fw-ctaccgcagccatgaagaacc, Rv-agaggaaggcccattgctgaa), CBFB-MYH11 (Fw-gcaggcaaggtatatttgaagg, Rv-tcctcttctcctcattctgctc), BCR-ABL1p210 (Fw-acagaattccgctgaccatcaataag, Fv-tgttgactggcgtgatgtagttgcttgg), MLL-AF9 (Fw-ctcagccacctactacaggac, Fv-agcgagcaaagatcaaaatc), PML-RARA(bcr1, bcr2) (Fw-cagtgtacgccttctccatca, Rv-gcttgtagatgcggggtaga) (18–20), and PML-RARA(bcr3) (Fw-ctgctggaggctgtggac, Rv-gcttgtagatgcggggtaga) (21). The PCR products were analyzed by agarose gel electrophoresis: AML1-ETO (395 bp), PML-RARA(bcr1, bcr2, bcr3) (381, 345 and 376 bp), CBFB-MYH11 (418 bp), BCR-ABL1P210 (310 bp), and MLL-AF9 (314 bp) (Supplementary Figure S1); and sequenced for validation using a 3500 Genetic Analyzer from Applied Biosystems (Supplementary Figure S2). Cell lines or validated positive patient samples were used as positive controls. A blank control without cDNA was used in each PCR.
Statistical analysis and ethical statement
The frequencies of the fusion genes were calculated using SPSS IBM V.21. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Research and Ethics Committee of the Centro Médico Nacional Siglo XXI (project number: R-2015-785-121). The patients/participants provided their written informed consent to participate in this study.
Results
Demographic and biological characteristics of studied population
We registered 77 patients (<18 years) with confirmed diagnoses of AML in nine public hospitals between January 2019 and June 2021. We found that 64.9% of the patients were male and 35.1% were female, with a median age of 9.4 years (Table 1). The largest age group was children, representing 55.8%, followed by adolescents (35.1%) and infants (9.1%) (Table 1). The mean WBC was 67.96 × 109/L, with a range of 0.76–500 × 109/L. According to the French–American–British (FAB) classification, 29.9% of the patients had the M2 or M4 subtype and 18.2% had M3; together, these three subtypes accounted for 78% of the patients (Table 1). The remaining few patients (n = 11, 14.28%) were classified as M0, M1, M5, and M6 (Table 1).
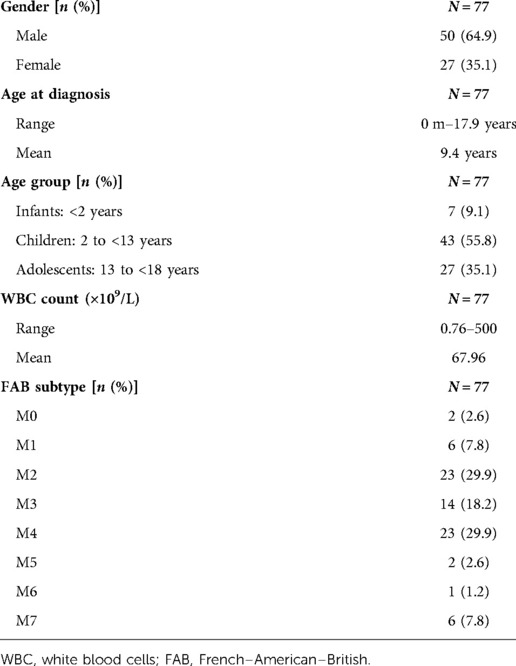
Table 1. Characteristics of pediatric patients diagnosed with AML and registered by the MIGICCL between 2019 and 2021.
Frequencies of fusion genes in child population with AML
The analyzed fusion genes showed a prevalence of 50.7% in our pediatric population (Table 2). AML1-ETO was the most frequent, with 22.1%, and was prevalent in the M2 subtype (39.2%) (Table 2). PML-RARA and CBFB-MYH11 had the second and third frequency positions, with 20.8% and 5.2%, respectively (Table 2). PML-RARA showed the highest prevalence in M3 (85.7%) and CBFB-MYH11 in M4 (8.7%) (Table 2). BCR-ABL1p210 was detected with a frequency of 2.6% and was prevalent in M2 (4.3%) and M4 (4.3%), while MLL-AF9 was not detected (Table 2). We did not detect the coexistence of fusion genes.
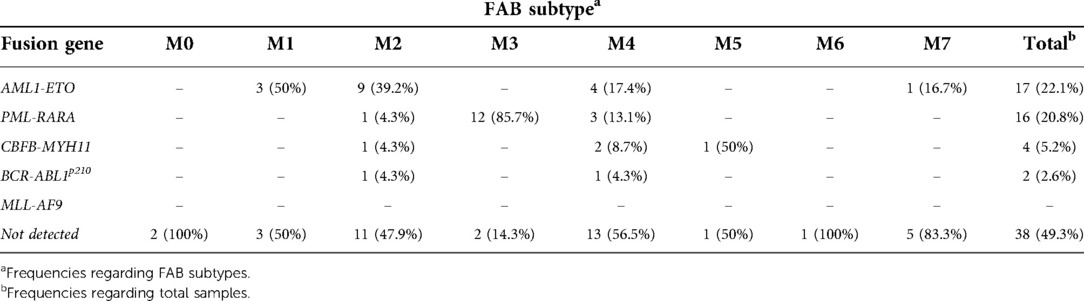
Table 2. Fusion gene frequencies and FAB subtypes of pediatric patients with AML.
Fusion gene frequencies according to patients' age groups and FAB subtypes
The prevalence of fusion genes with respect to the three groups of age (see Methods) and FAB subtype was analyzed. As shown in Table 3, the children and adolescents were positive for four of the five fusion genes analyzed, while the infants did not show the presence of fusion genes. The children and adolescents had similar overall fusion gene frequencies of ∼55.7%; however, AML1-ETO showed a prevalence in children (27.9%), and PML-RARA was prevalent in adolescents (22.3%) (Table 3). The most common FAB subtypes in infants, children, and adolescents were M7, M2, and M4, respectively (Table 3). The FAB subtype M3 showed a similar distribution in children and adolescents, but it was not present in infants (Table 3).
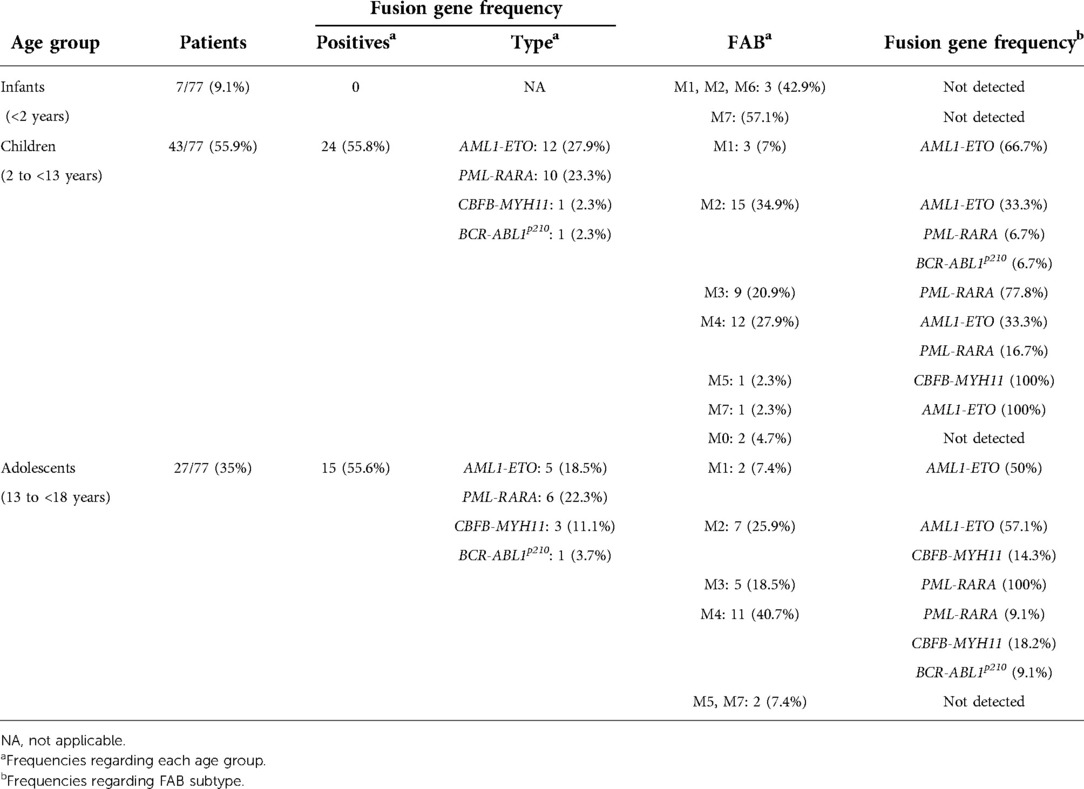
Table 3. Fusion gene frequencies in pediatric patients with acute myeloid leukemia according to age group and FAB subtype.
Children constituted the largest group, with 55.9% of the patients and a fusion gene frequency of 55.8%, being positive for AML1-ETO, PML-RARA, CBFB-MYH11, and BCR-ABL1p210 (Table 3). This group comprised patients with diverse subtypes, with M2 being the most prevalent (34.9%), followed by M4 (27.9%), and M3 (20.9%) (Table 3). AML1-ETO was the most prevalent in children, detected in M1 (66.7%), M2 (33.3%), M4 (33.3%), and M7 (Table 3). PML-RARA was the second most prevalent, which was detected in M2 (6.7%), M3 (77.8%), and M4 (16.7%) (Table 3). Finally, CBFB-MYH11 and BCR-ABL1p210 were the least frequent in children; CBFB-MYH11 was solely detected in the sample of M5, while BCR-ABL1p210 was detected in M2 with a frequency of 6.7% (Table 3). Adolescents constituted the second largest group, with 35% of the patients and a frequency of fusion genes of 55.6%, being positive for AML1-ETO, PML-RARA, CBFB-MYH11, and BCR-ABL1p210 (Table 3). This group comprised subtypes M1–M5 and M7, where M4 was the most prevalent, with 40.7%, followed by M2 (25.9%) and M3 (18.5%) (Table 3). PML-RARA was the most prevalent in adolescents, which was detected in M3 (100%) and M4 (9.1%) (Table 3). AML1-ETO was the second most prevalent and was detected in M1 (50%) and M2 (57.1%) (Table 3). CBFB-MYH11 was the third most prevalent in adolescents, and was present in M2 (14.3%) and M4 (18.2%) (Table 3). Finally, infants were the smallest group, with 9.1% of the patients, and they did not show the presence of fusion genes. This group comprised M1 (14.3%), M2 (14.3%), M6 (14.3%), and M7 (57.1%) sub-types (Table 3).
Discussion
We report the prevalence of AML1-ETO, PML-RARA, CBFB-MYH11, BCR-ABL1p210 and MLL-AF9 in a Mexican pediatric population with newly diagnosed AML recruited between January 2019 and June 2021. This constitutes an effort of the MIGICCL to increase the knowledge and comprehension of the epidemiological behavior of these fusion genes within the childhood population of Mexico City, which has one of the highest incidence rates of acute leukemia in the world (3, 4).
Previous studies have reported a prevalence of the M2 (avg = 19.8%), M3 (avg = 21.4%), and M4 (avg = 16.6%) subtypes in certain Latin American populations, with a major susceptibility to M3 (4, 22). In agreement with these reports, we identified these three subtypes as prevalent in our population (M2 = 29.9%, M4 = 29.9%, and M3 = 18.2%); however, M3 was not the most common in this study.
The most frequent fusion genes detected were AML1-ETO, PML-RARA, and CBFB-MYH11, although BCR-ABL1p210 was also detected at a lower frequency (Table 2). Altogether, these fusion genes account for a frequency of 50.7%, a percentage similar to that reported for pediatric patients around the world (6–9, 23). AML1-ETO was the most prevalent, which is consistent with previous reports that denote its ubiquity in patients with AML (23). However, our results showed a frequency that was ∼9% higher than that found in studies from the United States, Europe, Asia, and Australia, but it was 2.5% lower than that reported for the Japanese population (Supplementary Table S2). This fusion gene was prevalent in M2, but it was also detected in M1, M3, M4, and M7, in agreement with other studies, but there are no studies about their clinical impact (7–9, 24–27). PML-RARA had a prevalence that was ∼10% higher than that found in studies from the United Kingdom, Germany, Japan, and Austria, but not for Brazil, whose population has a 1.5% lower frequency (Supplementary Table S2). We found that this fusion gene was prevalent in M3, but it was also detected in M2 and M4 (Table 2), which has been reported as a rare event (28, 29). CBFB-MYH11 showed a similar frequency to that found in studies from the United Kingdom, Brazil, and Japan (7), although studies from the United States, Germany, Austria, and Switzerland have reported frequencies as high as 11.3% (Supplementary Table S2). This fusion gene has been associated with the M4 subtype with abnormal eosinophils (M4Eo) (30), but it could also be detected in M4 without eosinophilic abnormalities, M2, and M5, as we observed in this study (Table 2). BCR-ABL1 or the Philadelphia chromosome (Ph+) has been listed in the 2016 revised WHO classification of myeloid malignancies as a provisional entity (31). The incidence of Ph + in AML is approximately 0.5%–3%, however, an incidence of <1% was reported in studies with only purely de novo cases (12). Most of the patients with Ph+ express the BCR-ABL1p210 transcript, while few cases express BCR-ABL1p190 (12, 31). Although we analyzed these two transcript types, we only detected BCR-ABL1p210, which was four times more prevalent than reported for the population of the United Kingdom, but it was not detected in the Brazilian population (Supplementary Table S2). Due to the lack of studies with a pediatric population and the low prevalence of this fusion gene (12, 32), large-scale studies are needed to achieve better epidemiological/molecular characterization. Finally, although MLL-AF9 is one of the most common types of MLL fusions in AML (11, 26) we did not detect it in our population (Table 2), probably due to the small number of infant samples analyzed. However, it has been reported that MLL can translocate with other genes, such as AF10 and ENL, but we did not analyze it in this study. It is important to mention that, in a previous study on this same population, it was identified that children with acute leukemias treated in public hospitals are not genetically predominantly European, African, or Amerindian, but are a mixture of the three, so there are arguments that suggest that the population included in this study was a mixed-ethnicity population (33).
We performed a follow-up of patients to explore the relationship of fusion genes with mortality rates during the first year of treatment (Supplementary Figure S3). Several studies associate AML1-ETO, PML-RARA, and CBFB-MYH11 with favorable prognosis and long survival; BCR-ABL1p210 is associated with adverse prognosis, while MLL-AF9 has been associated with intermediate to poor prognosis (23). Patients with CBFB-MYH11 and AML1-ETO showed the highest rates of overall survival (Supplementary Figure S3), which is consistent with many previous reports indicating long survival and low mortality rates for these patients (23). In this study, patients with CBFB-MYH11 did not die, and only one of the AML1-ETO patients died (Supplementary Table S1). One of the two patients with BCR-ABL1p210 died, which was an expected outcome due to the association of these fusion genes with adverse prognosis (34). Although this is most likely not because of BCR-ABL1 itself but rather due to other high-risk cytogenetic/molecular features that are present in the majority of cases (35), it is important to note that we only had two positive patients, which makes it difficult to draw conclusions about the impact of this fusion gene in our population (Table 2). It has been reported that 70%–80% of patients with newly diagnosed M3 carrying PML-RARA achieve long-term remission. However, mortality in the first 30 days following therapy remains a major contribution to treatment failures, which is mainly attributable to thrombotic or hemorrhagic complications, reporting early mortality rates of 3%–20% (36–38). In this study, patients with PML-RARA had an early mortality rate of 18.75% due to intracranial hemorrhages (3/16 patients), showed that all of the deceased patients died within the first months after diagnosis (Supplementary Table S1). This early mortality rate shown in our population could be an overestimate due to the number of patients analyzed in comparison with other studies, or an indication of aspects related to local protocols that need improvement (36–39). Further studies are needed to establish an association.
A limitation of this study was the use of conventional PCR to detect AML1-ETO, PML-RARA, CBFB-MYH11, BCR-ABL1p210 and MLL-AF9. However, we are performing a prospective study using Real-Time Quantitative PCR to increase the power detection of these fusion genes, as well as the incorporation of primers and probes to detect the main variants of CBFB-MYH11, the BCR-ABLp190 and MLL-ENL fusion gen.
The use of molecular diagnostics to detect fusion genes with an impact on therapy has contributed to improved survival rates for pediatric patients with AML in developed countries (2). However, fusion gene screening by molecular approaches is not a routine activity in most public hospitals in Mexico City; nevertheless, it may be available through research projects such as this study. Besides, it is very important that fusion gene screening can be implemented with standard criteria in all public hospitals where children with AML are cared for. In this way, it may be possible to improve the survival rates in our pediatric population. Finally, we believe that long-term follow-up studies are needed to support solid conclusions about the impact of fusion genes on the survival of Mexican pediatric patients with AML.
Conclusions
The pediatric population of Mexico City with de novo AML had frequencies of AML1-ETO, PML-RARA, CBFB-MYH11, and BCR-ABL1p210 similar to those of other populations around the world. The patients with BCR-ABL1p210 and CBFB-MYH11 were few or did not die, while those with MLL-AF9 was not detected in this study. Although patients with PML-RARA had a low survival and a high early mortality rate, further studies are needed to determine the long-term impacts of these fusion genes on this Latino population.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were review and approved by the Institutional Research and Ethics Committee of the Centro Médico Nacional Siglo XXI (project number: R-2015-785-121). The patients/participants provided their written informed consent to participate in this study.
Author contributions
OS-R: investigation, formal analysis, and writing—original draft. EJ-H, JF-L, JCN-E, MLP-S, MMV-A, LEM-P, VCB-M, and AR-L: data curation. MD, MM-R, BAM-C, JCB-A, ASN-C, and NS-E: formal analysis. JAM-T, JRT-N, AM-S, JGP-G, RME-E, LVF-V, RA-S, DO-R, KAS-L, AIG-A, JDS-J, and SJ-M: resources. JMM-A, HR-V, VD-C, and EG-F: funding acquisition. HR-V, and JMM-A: writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by the Consejo Nacional de Ciencia y Tecnología (grant numbers: PDCPN2013–01-215726; FIS/IMSS/PROT/1364; SALUD 2015–1-262190; FIS/IMSS/PROT/1533; CB-2015-1-258042; FIS/IMSS/PROT/1548; FONCICYT/37/2018, FIS/IMSS/PROT/1782) by the Instituto Mexicano del Seguro Social (grant numbers: FIS/IMSS/PROT/PRIO/14/031; FIS/IMSS/PROT/PRIO/15/048; FIS/IMSS/PROT/G15/1477; FIS/IMSS/PROT/PRIO/18/080) and by Internal Funds of the Instituto Nacional de Medicina Genómica (INMEGEN).
Acknowledgments
We thank Alicia Estrada and Carmen Luttrell for their diligent proofreading of this paper.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.946690/full#supplementary-material.
References
1. Linabery AM, Ross JA. Trends in childhood cancer incidence in the U.S. (1992–2004). Cancer. (2008) 112(2):416–32. doi: 10.1002/cncr.23169
2. Ward ZJ, Yeh JM, Bhakta N, Frazier AL, Girardi F, Atun R. Global childhood cancer survival estimates and priority-setting: a simulation-based analysis. Lancet Oncol. (2019) 20(7):972–83. doi: 10.1016/S1470-2045(19)30273-6
3. Mejia-Arangure JM, Fajardo-Gutierrez A, Bernaldez-Rios R, Farfan-Canto JM, Ortiz-Fernandez A, Martinez-Garcia MD. Incidence trends of acute leukemia among the children of Mexico city: 1982–1991. Arch Med Res. (1996) 27(2):223–7.8696068
4. Perez-Saldivar ML, Fajardo-Gutierrez A, Bernaldez-Rios R, Martinez-Avalos A, Medina-Sanson A, Espinosa-Hernandez L, et al. Childhood acute leukemias are frequent in Mexico city: descriptive epidemiology. BMC Cancer. (2011) 11:355. doi: 10.1186/1471-2407-11-355
5. Martens JH, Stunnenberg HG. The molecular signature of oncofusion proteins in acute myeloid leukemia. FEBS Lett. (2010) 584(12):2662–9. doi: 10.1016/j.febslet.2010.04.002
6. Betts DR, Ammann RA, Hirt A, Hengartner H, Beck-Popovic M, Kuhne T, et al. The prognostic significance of cytogenetic aberrations in childhood acute myeloid leukaemia. A study of the Swiss paediatric oncology group (SPOG). Eur J Haematol. (2007) 78(6):468–76. doi: 10.1111/j.1600-0609.2007.00854.x
7. Grimwade D. The clinical significance of cytogenetic abnormalities in acute myeloid leukaemia. Best Pract Res Clin Haematol. (2001) 14(3):497–529. doi: 10.1053/beha.2001.0152
8. Harrison CJ, Hills RK, Moorman AV, Grimwade DJ, Hann I, Webb DK, et al. Cytogenetics of childhood acute myeloid leukemia: United Kingdom medical research council treatment trials AML 10 and 12. J Clin Oncol. (2010) 28(16):2674–81. doi: 10.1200/JCO.2009.24.8997
9. von Neuhoff C, Reinhardt D, Sander A, Zimmermann M, Bradtke J, Betts DR, et al. Prognostic impact of specific chromosomal aberrations in a large group of pediatric patients with acute myeloid leukemia treated uniformly according to trial AML-BFM 98. J Clin Oncol. (2010) 28(16):2682–9. doi: 10.1200/JCO.2009.25.6321
10. Meyer C, Burmeister T, Groger D, Tsaur G, Fechina L, Renneville A, et al. The MLL recombinome of acute leukemias in 2017. Leukemia. (2018) 32(2):273–84. doi: 10.1038/leu.2017.213
11. Bolouri H, Farrar JE, Triche T Jr., Ries RE, Lim EL, Alonzo TA, et al. The molecular landscape of pediatric acute myeloid leukemia reveals recurrent structural alterations and age-specific mutational interactions. Nat Med. (2018) 24(1):103–12. doi: 10.1038/nm.4439
12. Neuendorff NR, Burmeister T, Dorken B, Westermann J. BCR-ABL-positive acute myeloid leukemia: a new entity? Analysis of clinical and molecular features. Ann Hematol. (2016) 95(8):1211–21. doi: 10.1007/s00277-016-2721-z
13. Ruiz-Arguelles GJ, Garces-Eisele J, Reyes-Nunez V, Gomez-Rangel JD, Ruiz-Delgado GJ. More on geographic hematology: the breakpoint cluster regions of the PML/RARalpha fusion gene in Mexican mestizo patients with promyelocytic leukemia are different from those in caucasians. Leuk Lymphoma. (2004) 45(7):1365–8. doi: 10.1080/10428190310001657344
14. Ruiz-Arguelles GJ, Morales-Toquero A, Manzano C, Ruiz-Delgado GJ, Jaramillo P, Gonzalez-Carrillo ML, et al.. t(8;21) (q22;q22) acute myelogenous leukemia in Mexico: a single institution experience. Hematology. (2006) 11(4):235–8. doi: 10.1080/10245330600702893
15. Zapata-Tarres M, Sánchez-Huerta J, Angeles-Floriano T, Parra-Ortega I, Klunder-Klunder M, Vilchis-Ordoñez A, et al. Identificación de alteraciones moleculares en pacientes pediátricos con diagnóstico de leucemia aguda. Rev Hematol Mex. (2017) 18(2):47–57.
16. Ruiz-Delgado GJ, Macías-Gallardo J, Lutz-Presno J, Garcés-Eisele J, Hernández-Arizpe A, Montes-Montiel M, et al. Core binding factor acute myeloid leukemia (CBF-AML) in México: a single institution experience. Rev Invest Clin. (2011) 63(1):25–30.21574542
17. Creutzig U, Buchner T, Sauerland MC, Zimmermann M, Reinhardt D, Dohner H, et al. Significance of age in acute myeloid leukemia patients younger than 30 years: a common analysis of the pediatric trials AML-BFM 93/98 and the adult trials AMLCG 92/99 and AMLSG HD93/98A. Cancer. (2008) 112(3):562–71. doi: 10.1002/cncr.23220
18. Amanollahi Kamaneh E, Shams Asenjan K, Movassaghpour Akbari A, Akbarzadeh Laleh P, Chavoshi H, Eivazi Ziaei J, et al. Characterization of common chromosomal translocations and their frequencies in acute myeloid leukemia patients of northwest Iran. Cell J. (2016) 18(1):37–45. doi: 10.22074/cellj.2016.3985
19. Pakakasama S, Kajanachumpol S, Kanjanapongkul S, Sirachainan N, Meekaewkunchorn A, Ningsanond V, et al. Simple multiplex RT-PCR for identifying common fusion transcripts in childhood acute leukemia. Int J Lab Hematol. (2008) 30(4):286–91. doi: 10.1111/j.1751-553X.2007.00954.x
20. Wilson G, Frost L, Goodeve A, Vandenberghe E, Peake I, Reilly J. BCR-ABL transcript with an e19a2 (c3a2) junction in classical chronic myeloid leukemia. Blood. (1997) 89(8):3064. doi: 10.1182/blood.V89.8.3064
21. van Dongen JJ, Macintyre EA, Gabert JA, Delabesse E, Rossi V, Saglio G, et al. Standardized RT-PCR analysis of fusion gene transcripts from chromosome aberrations in acute leukemia for detection of minimal residual disease. Report of the BIOMED-1 concerted action: investigation of minimal residual disease in acute leukemia. Leukemia. (1999) 13(12):1901–28. doi: 10.1038/sj.leu.2401592
22. Gomez-Almaguer D, Marcos-Ramirez ER, Montano-Figueroa EH, Ruiz-Arguelles GJ, Best-Aguilera CR, Lopez-Sanchez MD, et al. Acute leukemia characteristics are different around the world: the Mexican perspective. Clin Lymphoma Myeloma Leuk. (2017) 17(1):46–51. doi: 10.1016/j.clml.2016.09.003
23. Creutzig U, van den Heuvel-Eibrink MM, Gibson B, Dworzak MN, Adachi S, de Bont E, et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood. (2012) 120(16):3187–205. doi: 10.1182/blood-2012-03-362608
24. Andrade FG, Noronha EP, Brisson GD, Dos Santos Vicente Bueno F, Cezar IS, Terra-Granado E, et al. Molecular characterization of pediatric acute myeloid leukemia: results of a multicentric study in Brazil. Arch Med Res. (2016) 47(8):656–67. doi: 10.1016/j.arcmed.2016.11.015
25. Iijima-Yamashita Y, Matsuo H, Yamada M, Deguchi T, Kiyokawa N, Shimada A, et al. Multiplex fusion gene testing in pediatric acute myeloid leukemia. Pediatr Int. (2018) 60(1):47–51. doi: 10.1111/ped.13451
26. Rubnitz JE, Inaba H, Dahl G, Ribeiro RC, Bowman WP, Taub J, et al. Minimal residual disease-directed therapy for childhood acute myeloid leukaemia: results of the AML02 multicentre trial. Lancet Oncol. (2010) 11(6):543–52. doi: 10.1016/S1470-2045(10)70090-5
27. Uz B, Eliacik E, Isik A, Aksu S, Buyukasik Y, Haznedaroglu IC, et al. Co-expression of t(15;17) and t(8;21) in a case of acute promyelocytic leukemia: review of the literature. Turk J Haematol. (2013) 30(4):400–4. doi: 10.4274/Tjh.2012.0180
28. Allford S, Grimwade D, Langabeer S, Duprez E, Saurin A, Chatters S, et al. Identification of the t(15;17) in AML FAB types other than M3: evaluation of the role of molecular screening for the PML/RARalpha rearrangement in newly diagnosed AML. The medical research council (MRC) adult leukaemia working party. Br J Haematol. (1999) 105(1):198–207. doi: 10.1111/j.1365-2141.1999.01312.x
29. Braham Jmili N, Omri H, Senana Sendi H, Fekih S, Hizem S, Sriha B, et al. Identification of the translocation t(15;17) in acute myeloid leukemia (AML) initially classified as FAB M1: case report and review of the literature. Clin Lab. (2006) 52(3–4):125–30.16584058
30. Poirel H, Radford-Weiss I, Rack K, Troussard X, Veil A, Valensi F, et al. Detection of the chromosome 16 CBF beta-MYH11 fusion transcript in myelomonocytic leukemias. Blood. (1995) 85(5):1313–22. doi: 10.1182/blood.V85.5.1313.bloodjournal8551313
31. Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the world health organization classification of lymphoid neoplasms. Blood. (2016) 127(20):2375–90. doi: 10.1182/blood-2016-01-643569
32. Grimwade D, Hills RK, Moorman AV, Walker H, Chatters S, Goldstone AH, et al. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom medical research council trials. Blood. (2010) 116(3):354–65. doi: 10.1182/blood-2009-11-254441
33. Medina-Sanson A, Nunez-Enriquez JC, Hurtado-Cordova E, Perez-Saldivar ML, Martinez-Garcia A, Jimenez-Hernandez E, et al. Genotype-Environment interaction analysis of NQO1, CYP2E1, and NAT2 polymorphisms and the risk of childhood acute lymphoblastic leukemia: a report from the Mexican interinstitutional group for the identification of the causes of childhood leukemia. Front Oncol. (2020) 10:571869. doi: 10.3389/fonc.2020.571869
34. Soupir CP, Vergilio JA, Dal Cin P, Muzikansky A, Kantarjian H, Jones D, et al. Philadelphia chromosome-positive acute myeloid leukemia: a rare aggressive leukemia with clinicopathologic features distinct from chronic myeloid leukemia in myeloid blast crisis. Am J Clin Pathol. (2007) 127(4):642–50. doi: 10.1309/B4NVER1AJJ84CTUU
35. Neuendorff NR, Hemmati P, Arnold R, Ihlow J, Dorken B, Muller-Tidow C, et al. BCR-ABL(+) acute myeloid leukemia: are we always dealing with a high-risk disease? Blood Adv. (2018) 2(12):1409–11. doi: 10.1182/bloodadvances.2018015594
36. Bally C, Fadlallah J, Leverger G, Bertrand Y, Robert A, Baruchel A, et al. Outcome of acute promyelocytic leukemia (APL) in children and adolescents: an analysis in two consecutive trials of the European APL group. J Clin Oncol. (2012) 30(14):1641–6. doi: 10.1200/JCO.2011.38.4560
37. Ortega JJ, Madero L, Martin G, Verdeguer A, Garcia P, Parody R, et al. Treatment with all-trans retinoic acid and anthracycline monochemotherapy for children with acute promyelocytic leukemia: a multicenter study by the PETHEMA group. J Clin Oncol. (2005) 23(30):7632–40. doi: 10.1200/JCO.2005.01.3359
38. Testi AM, Biondi A, Lo Coco F, Moleti ML, Giona F, Vignetti M, et al. GIMEMA-AIEOPAIDA protocol for the treatment of newly diagnosed acute promyelocytic leukemia (APL) in children. Blood. (2005) 106(2):447–53. doi: 10.1182/blood-2004-05-1971
Keywords: AML – acute myeloid leukaemia, fusion genes, translocation, pediatric population, Mexican population
Citation: Sepúlveda-Robles O, Jiménez-Hernández E, Domínguez-Catzín V, Gómez-Flores E, Martín-Trejo JA, Flores-Lujano J, Torres-Nava JR, Núñez-Enríquez JC, De Ita M, Medina-Sanson A, Mata-Rocha M, Morales-Castillo BA, Bravata-Alcántara JC, Nájera-Cortés AS, Sánchez-Escobar N, Peñaloza-Gonzalez JG, Espinosa-Elizondo RM, Flores-Villegas LV, Amador-Sanchez R, Orozco-Ruiz D, Pérez-Saldívar ML, Velázquez-Aviña MM, Merino-Pasaye LE, Solís-Labastida KA, González-Ávila AI, Santillán-Juárez JD, Bekker-Méndez VC, Jiménez-Morales S, Rangel-López A, Rosas-Vargas H and Mejía-Aranguré JM (2022) Analytical study of RUNX1-RUNXT1, PML-RARA, CBFB-MYH11, BCR-ABL1p210, and KMT2-MLLT3 in Mexican children with acute myeloid leukemia: A multicenter study of the Mexican interinstitutional group for the identification of the causes of childhood leukemia (MIGICCL). Front. Pediatr. 10:946690. doi: 10.3389/fped.2022.946690
Received: 17 May 2022; Accepted: 13 October 2022;
Published: 14 November 2022.
Edited by:
Tim S. Nawrot, University of Hasselt, BelgiumReviewed by:
Anca M. Colita, Carol Davila University of Medicine and Pharmacy, RomaniaLi Yao, First Affiliated Hospital of Soochow University, China
© 2022 Sepúlveda-Robles, Jiménez-Hernández, Domínguez-Catzín, Gómez-Flores, Martín-Trejo, Flores-Lujano, Torres-Nava, Núñez-Enríquez, De Ita, Medina Sanson, Mata-Rocha, Morales-Castillo, Bravata-Alcántara, Nájera-Cortés, Sánchez-Escobar, Peñaloza-Gonzalez, Espinosa-Elizondo, Flores-Villegas, Amador-Sánchez, Orozco-Ruiz, Pérez-Saldívar, Velázquez-Aviña, Merino-Pasaye, Solís-Labastida, González-Ávila, Santillán-Juárez, Bekker-Méndez, Jiménez-Morales, Rangel-López, Rosas-Vargas and Mejía-Aranguré. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Manuel Mejía-Aranguré am1lamlhQGlubWVnZW4uZ29iLm14 Haydeé Rosas-Vargas aGF5cm92QGdtYWlsLmNvbQ==
Specialty Section: This article was submitted to Children and Health, a section of the journal Frontiers in Pediatrics