 Marco Antonio Yamazaki-Nakashimada1
Marco Antonio Yamazaki-Nakashimada1 Horacio Márquez-González2
Horacio Márquez-González2 Guadalupe Miranda-Novales3
Guadalupe Miranda-Novales3 Gonzalo Antonio Neme Díaz4Sandhi Anel Prado Duran5
Gonzalo Antonio Neme Díaz4Sandhi Anel Prado Duran5 Antonio Luévanos Velázquez6
Antonio Luévanos Velázquez6 Maria F. Castilla-Peon7*
Maria F. Castilla-Peon7* Nadia González-García2*
Nadia González-García2* Miguel Alejandro Sánchez Duran1Martha Patricia Márquez Aguirre1
Miguel Alejandro Sánchez Duran1Martha Patricia Márquez Aguirre1 Miguel Angel Villasis-Keever3
Miguel Angel Villasis-Keever3 Ranferi Aragón Nogales3
Ranferi Aragón Nogales3 Juan Carlos Núñez-Enríquez3Maria Elena Martinez Bustamante8
Juan Carlos Núñez-Enríquez3Maria Elena Martinez Bustamante8 Carlos Aguilar Argüello4Jesús Ramírez de los Santos4Alejandra Pérez Barrera4
Carlos Aguilar Argüello4Jesús Ramírez de los Santos4Alejandra Pérez Barrera4 Lourdes Anais Palacios Cantú5
Lourdes Anais Palacios Cantú5 Jesús Membrila Mondragón5
Jesús Membrila Mondragón5 Paloma Vizcarra Alvarado6
Paloma Vizcarra Alvarado6 Rodolfo Norberto Jiménez Juárez2
Rodolfo Norberto Jiménez Juárez2 Víctor Olivar López2Roberto Velasco-Segura9Adrián López Chávez2
Víctor Olivar López2Roberto Velasco-Segura9Adrián López Chávez2
- 1National Institute of Pediatrics, Mexico City, Mexico
- 2Department of Rheumatology, Hospital Infantil de Mexico Federico Gomez, Mexico City, Mexico
- 3XXI Century National Medical Center, Mexican Social Security Institute, Mexico City, Mexico
- 4Hospital del Niño Dr. Rodolfo Nieto Padrón, Villahermosa, Mexico
- 5Mexican Social Security Institute (IMSS), Mexico City, Mexico
- 6Civil Hospital of Guadalajara, Guadalajara, Mexico
- 7Hospital Psiquiatrico Infantil Juan N Navarro, Servicios de Atención Psiquiátrica, Mexico City, Mexico
- 8Centro Médico Nacional 20 de Noviembre (CMN), Mexico City, Mexico
- 9Instituto de Ciencias Aplicada y Tecnología, Universidad Nacional Autónoma de México, Mexico City, Mexico
Introduction: Multisystem inflammatory syndrome in children associated with coronavirus disease 2019 (MIS-C), a novel hyperinflammatory condition secondary to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, is associated with severe outcomes such as coronary artery aneurysm and death.
Methods: This multicenter, retrospective, observational cohort study including eight centers in Mexico, aimed to describe the clinical characteristics and outcomes of patients with MIS-C. Patient data were evaluated using latent class analysis (LCA) to categorize patients into three phenotypes: toxic shock syndrome-like (TSSL)-MIS-C, Kawasaki disease-like (KDL)-MIS-C, and nonspecific MIS-C (NS-MIS-C). Risk factors for adverse outcomes were estimated using multilevel mixed-effects logistic regression.
Results: The study included 239 patients with MIS-C, including 61 (26%), 70 (29%), and 108 (45%) patients in the TSSL-MIS-C, KDL-MIS-C, and NS-MIS-C groups, respectively. Fifty-four percent of the patients were admitted to the intensive care unit, and 42%, 78%, and 41% received intravenous immunoglobulin, systemic glucocorticoids, and anticoagulants, respectively. Coronary artery dilatation and aneurysms were found in 5.7% and 13.2% of the patients in whom coronary artery diameter was measured, respectively. Any cause in-hospital mortality was 5.4%. Hospitalization after ten days of symptoms was associated with coronary artery abnormalities (odds ratio [OR] 1.6, 95% confidence interval [CI] 1.2–2.0). Age ≥10 years (OR: 5.6, 95% CI: 1.4–2.04), severe underlying condition (OR: 9.3, 95% CI: 2.8–31.0), platelet count <150,000 /mm3 (OR: 4.2, 95% CI: 1.2–14.7), international normalized ratio >1.2 (OR: 3.8, 95% CI: 1.05–13.9), and serum ferritin concentration >1,500 mg/dl at admission (OR: 52, 95% CI: 5.9–463) were risk factors for death.
Discussion: Mortality in patients with MIS-C was higher than reported in other series, probably because of a high rate of cases with serious underlying diseases.
1. Introduction
Multisystem Inflammatory Syndrome in Children (MIS-C), temporally associated with coronavirus disease 2019 (COVID-19), also known as pediatric multisystem inflammatory syndrome, is a novel hyperinflammatory condition secondary to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and shares features with Kawasaki disease, toxic shock syndrome, and acute COVID-19. MIS-C was first described in April 2020 in the United Kingdom, followed by case reports in other countries (1, 2).
The clinical case definition of MIS-C varies slightly among different health agencies (2–5). Clinical features include fever, gastrointestinal symptoms, conjunctival injection, rash, and elevated inflammatory markers. Potential complications include shock, multi-organ failure, and myocardial and coronary artery involvement similar to those observed in Kawasaki disease (6–8). Many patients with MIS-C have evidence of SARS-CoV-2 infection within several weeks before disease onset (9–11). The estimated incidence of MIS-C is 3–5 per 10,000 among individuals aged <21 years who are infected with SARS-CoV2. Studies in ethnically diverse countries reported a higher incidence of MIS-C in Hispanic and Afro-descendant individuals, emphasizing the need to characterize the clinical spectrum of MIS-C in specific populations (12).
Several reports have suggested the existence of different MIS-C phenotypes, including the Kawasaki disease-like (KDL)-MIS-C, the toxic shock syndrome-like (TSSL)-MIS-C, as well as the nonspecific MIS-C with predominantly acute respiratory involvement (NS-MIS-C). Differentiating MIS-C from acute COVID-19 and other hyperinflammatory conditions can be challenging for healthcare providers. The treatment approach for MIS-C includes intravenous immunoglobulin (IVIG), systemic glucocorticoids, and anti-inflammatory biological agents; the efficacy of these treatments relies on the timely diagnosis of MIS-C.
Despite its low prevalence, MIS-C is a serious life-threatening condition. Therefore, this study aimed to examine the clinical characteristics and outcomes of KDL-MIS-C, TSSL-MIS-C, and NS-MIS-C among patients with MIS-C in eight tertiary-care pediatric centers in Mexico. We also performed exploratory analyses to identify coronary artery abnormalities and death-related factors.
2. Materials and methods
2.1. Study design
This was a multicenter, retrospective, observational cohort study including patients diagnosed with MIS-C in one of the eight participating pediatric tertiary care centers in Mexico. Four centers were located in Mexico City: Federico Gómez Mexico Children's Hospital, National Institute of Pediatrics, Siglo XXI Medical Center's Pediatrics Hospital, and. Guadalajara Civil Hospital was located in Guadalajara, Jalisco; Villa Hermosa Children's Hospital was located in Villa Hermosa, Tabasco, and one investigator collected data on cases from the state of Tamaulipas.
The study was approved by Federico Gómez Mexico Children's Hospital Institutional Review Board (approval no. HIM-2022-015) and the local ethics review board of the remaining participating centers.
Probable MIS-C cases were identified by the review of medical records of patients admitted to the emergency room, intensive care unit (ICU), or the general hospital ward for COVID-19. Patient files were evaluated to determine if they met the MIS-C case definition of the Centers for Disease Control and Prevention (Chart 1) (2).
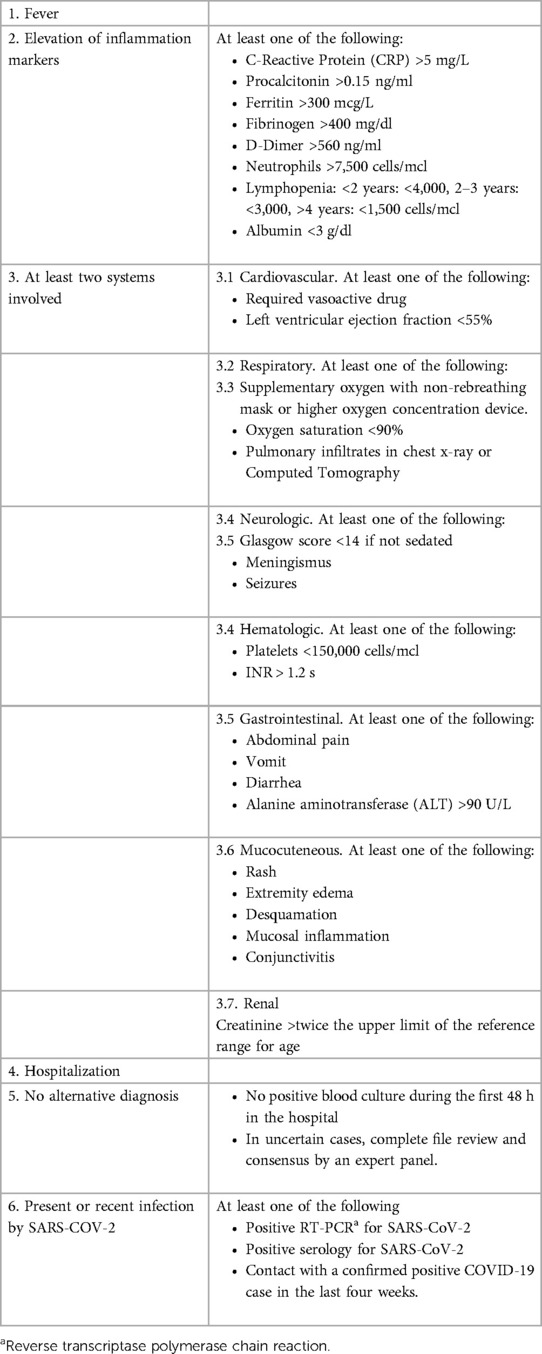
Chart 1. Case definition criteria for MIS-C.
Local investigators at participating centers collected data from the medical records using REDCap (Research Electronic Data Capture) software hosted at Federico Gómez Mexico Children's Hospital. Personal identifiers were kept confidential at participating centers and were not registered in the general database. Data were retrieved from REDCap, inconsistencies and missing data were corrected through direct communication with local investigators, units of measurement were unified, and variables were converted as necessary.
The worst value measured within the first three days of hospitalization was obtained for laboratory parameters with more than one measurement. Life support measures (respiratory support and vasopressor utilization) and the use of IVIG, systemic glucocorticoids, and anticoagulant therapy were documented as primary therapeutic interventions. Outcomes of interest were admission, length of ICU stay and hospitalization, need for invasive mechanical ventilation, vasopressor support, myocardial depression (left ventricular ejection fraction <55%), coronary aneurysm (coronary artery diameter z-score ≥2.5) and coronary artery dilatation (diameter z-score >2 to <2.5) on the echocardiographic evaluation performed during hospitalization, and in-hospital mortality.
In the present study, severe respiratory involvement was defined as the presence of infiltrates on chest x-ray or computed tomography plus the need for either oxygen therapy at 80% or higher concentration or positive pressure ventilation. Additionally, “gastrointestinal symptoms” was defined as the presence of at least one of the following: abdominal pain, diarrhea, and emesis. Severe underlying conditions included cancer and other immunosuppressive states, neuromuscular disability, chronic respiratory diseases except for asthma, congenital cardiac disorders, and chronic kidney failure.
Centers involved had different capacities to perform echocardiograms. When performed, echocardiograms were done either by a trained cardiologist who made an extensive heart evaluation, including the diameter of coronary arteries, or by emergency staff where the main aim was measurement of ventricular function for life support-oriented purposes.
2.2. Statistical analysis
Descriptive analyses were conducted using STATA v.14.0 (StataCorp, Houston, TX, USA). Categorical variables were reported as frequencies, and continuous variables were reported as medians with interquartile ranges.
In the present study, we utilized latent class analysis (LCA) to classify 239 patients into the TSSL-PIMS, KDL-PIMS, and U-PIM groups, congruent with the phenotypes identified in previous studies (13–15). LCA is a probabilistic modeling algorithm that allows clustering cases by associating indicator categorical variables. Three-class LCA was conducted using the R software package “poLCA” with 100 iterations to identify the clusters. The fit of each model was assessed using the Bayesian information criterion score. Indicator variables used in the final LCA model were the 20 features of Kawasaki disease, KDL-MIS-C, NS-MIS-C-TS, and TSSL-MIS-C (Table 1 and Supplementary Chart S1).
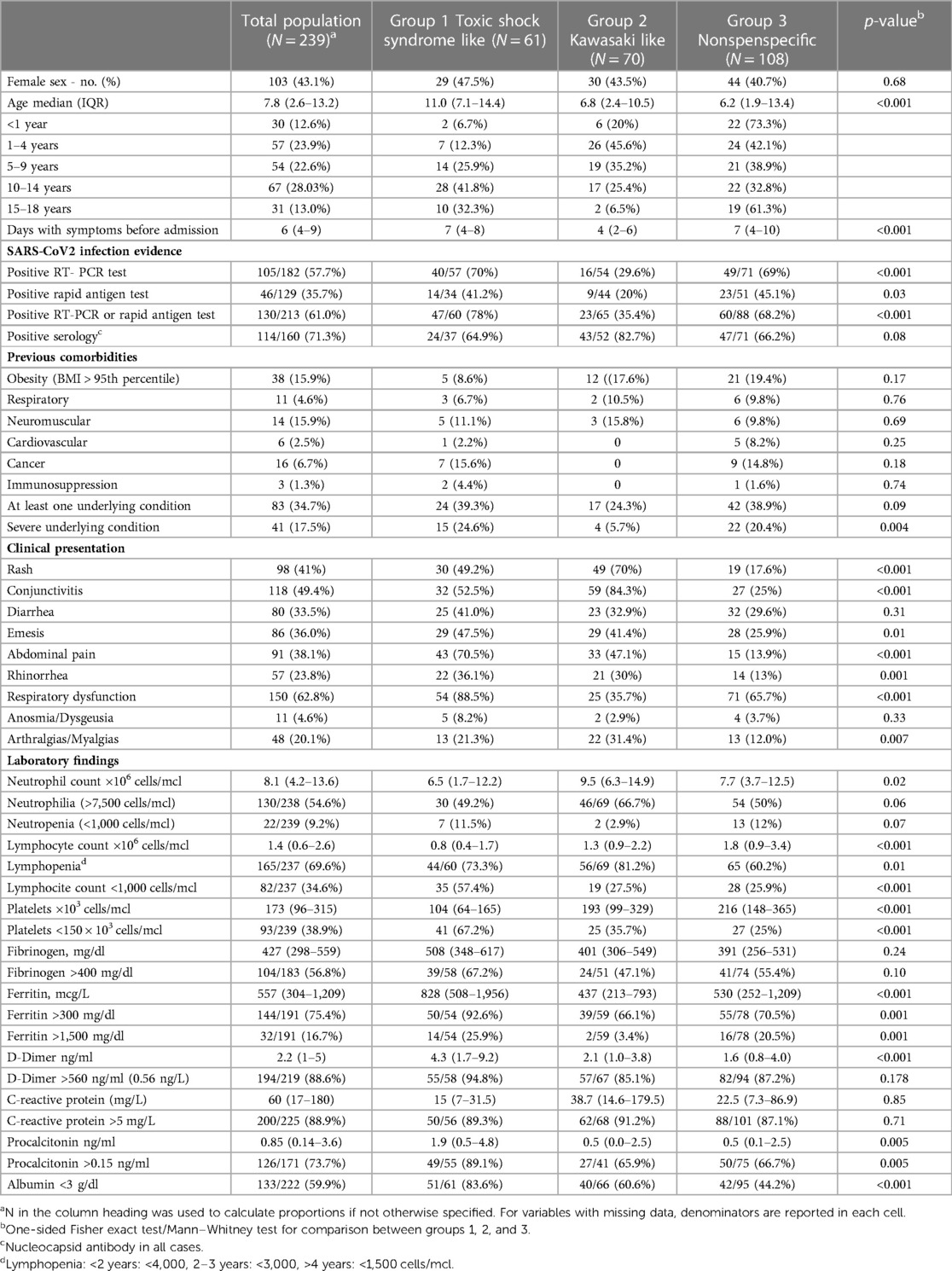
Table 1. Clinical presentation of cases with MIS-C.
Potential heterogeneity among the participating centers was addressed by determining 95% confidence intervals (CIs) of the frequencies of measured outcomes using random-effects meta-analysis. Odds ratios (ORs) with 95% CIs of pooled data were calculated using clustered-robust standard error adjustment. ORs adjusted for the participating centers were calculated using multilevel mixed-effects logistic regression.
3. Results
Of the 264 identified patients, 6, 11, and 8 were excluded due to duplicate records, lack of evidence on multi-organ involvement, and lack of evidence of previous SARS-CoV-2 infection or confirmed epidemiological contact, respectively. Tables 1, 2 summarize the clinical characteristics and outcomes of the remaining 239 patients included in the final analysis.
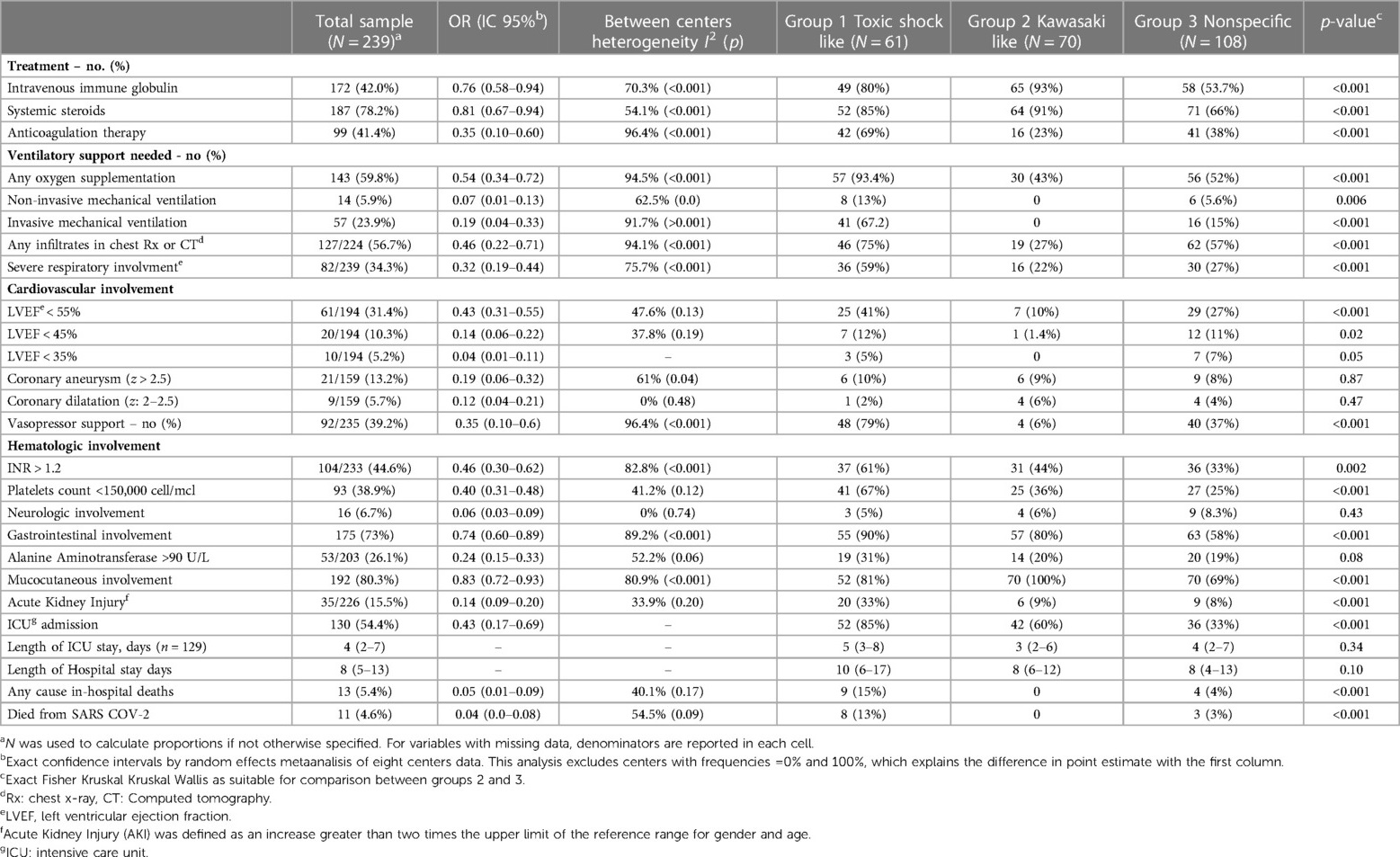
Table 2. Treatment and outcomes of cases with MIS-C.
LCA indicated that 61 (26%), 70 (29%), and 108 (45%) of the patients exhibited the clinical profiles of TSSL-MIS-C, KDL-MIS-C, and NS-MIS-C, respectively (Table 1). The median age was higher in the TSSL-MIS-C group than in the overall cohort (11 [IQR: 7.1–14.4] vs. 7.8 [IQR: 2.6–13.2] years). Duration of clinical symptoms before diagnosis was significantly shorter in the KDL-MIS-C group than in the other two clinical groups (p < 0.001). Additionally, the frequency of virologic positivity for acute SARS-CoV-2 infection was lower (p < 0.001) and the frequency of serologic positivity tended to be higher (p = 0.08) in the KDL-MIS-C group than in the other two clinical groups. Only four (5.7%) children in the KDL-MIS-C group had a severe underlying condition, while it was present in 15 (24.6%) and 22 (20.4%) of the TSSL-MIS-C and NS-MIS-C, respectively. The levels of plasma inflammatory markers were highest in the TSSL-MIS-C group compared with the other two clinical groups.
Table 2 describes treatments and outcomes in the total study population and the three clinical groups. IVIG and systemic glucocorticoids were administered in 172 (42%) and 187 (78.2%) of the patients, respectively; both treatments were more frequently (93% and 91%) administered to patients in the KDL-MIS-C group. Anticoagulant therapy was prescribed in 99 (41.4%) of the whole cohort and administered more frequently (60%) in the TSSL-MIS-C group. Oxygen supplementation and vasopressor support were required in 143 (59%) and 92 (39%) of the whole cohort, respectively.
An echocardiogram was performed in 194 cases, of which 159 reported values of coronary arteries diameters. Left ventricular ejection fraction was below 55% in 61/195 (31%) of the patients, and coronary artery dilatation and aneurysm were observed in 9/159 (5.7%) and 21/159 (13.2%), respectively. The entire cohort's median in-hospital stay was eight days (IQR: 5–13), and about half (54.4%) of the patients were admitted to the ICU. There were 13 in-hospital deaths (5.4%), including eight patients with severe underlying conditions and two from causes unrelated to SARS-COV-2 infection. Most deaths (69%) occurred in the TSSL-MIS-C group, whereas none occurred in the KDL-MIS-C group.
Hematologic, neurologic, gastrointestinal, mucocutaneous, and renal dysfunction were frequently observed, with frequency variability among the clinical groups. Prolonged coagulation time based on international normalized ratio, low platelet count, gastrointestinal symptoms, and acute renal injury were more frequent in the TSSL-MIS-C group (61%, 67%, 90%, and 33% of the patients, respectively) than in the other clinical groups.
Coronary aneurysm or dilatation occurred in 27 (11.3%) patients (2). After adjustment for cluster effect, symptom duration >10 days before hospital admission was the only factor significantly associated with coronary artery abnormalities (OR: 1.6, 95% CI: 1.2–2.0) (Table 3).
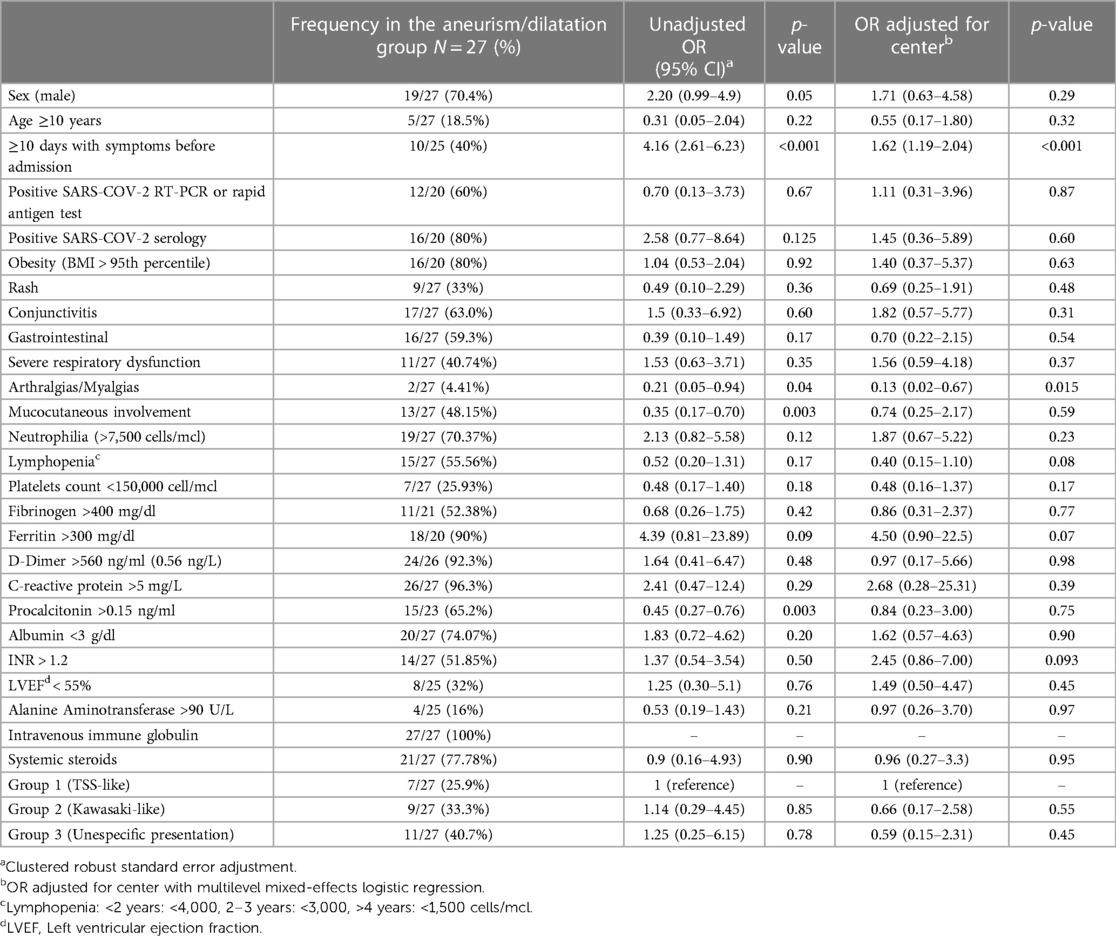
Table 3. Coronary artery aneurism or dilatation associated factors.
There were thirteen deaths; eight of them had a severe underlying condition. Three cases with a fatal outcome were on antineoplastic chemotherapy, one case with medulloblastoma was on palliative care, and a kidney transplant recipient had a diagnosis of sepsis with a possible respiratory infection. Besides, one of the cancer patients with a germ cell tumor developed a deep vein thrombosis. A case with chronic granulomatous diseases, a patient with Down syndrome, and a case with a severe neuromuscular disability had diagnoses of pneumonia on admission. Of the five previously healthy cases, one presented as a nephrotic syndrome and myocarditis, and another received the diagnosis of hepatorenal syndrome on admission. The three remaining cases presented with severe respiratory distress syndrome, heart failure, and coagulopathy.
Risk factors for death were age ≥10 years (OR: 5.6, 95% CI: 1.4–2.04), presence of at least one underlying condition (OR: 5.3, 95% CI: 1.5–18.4), severe underlying condition such as cancer (OR: 9.3, 95% CI: 2.8–31.0), platelet count <150,000 /mm3 (OR: 4.2, 95% CI: 1.2–14.7), international normalized ratio >1.2 at admission (OR: 3.8, 95% CI: 1.05–13.9), and serum ferritin concentration >1,500 mg/dl (OR: 52, 95% CI: 5.9–463) (Table 4).
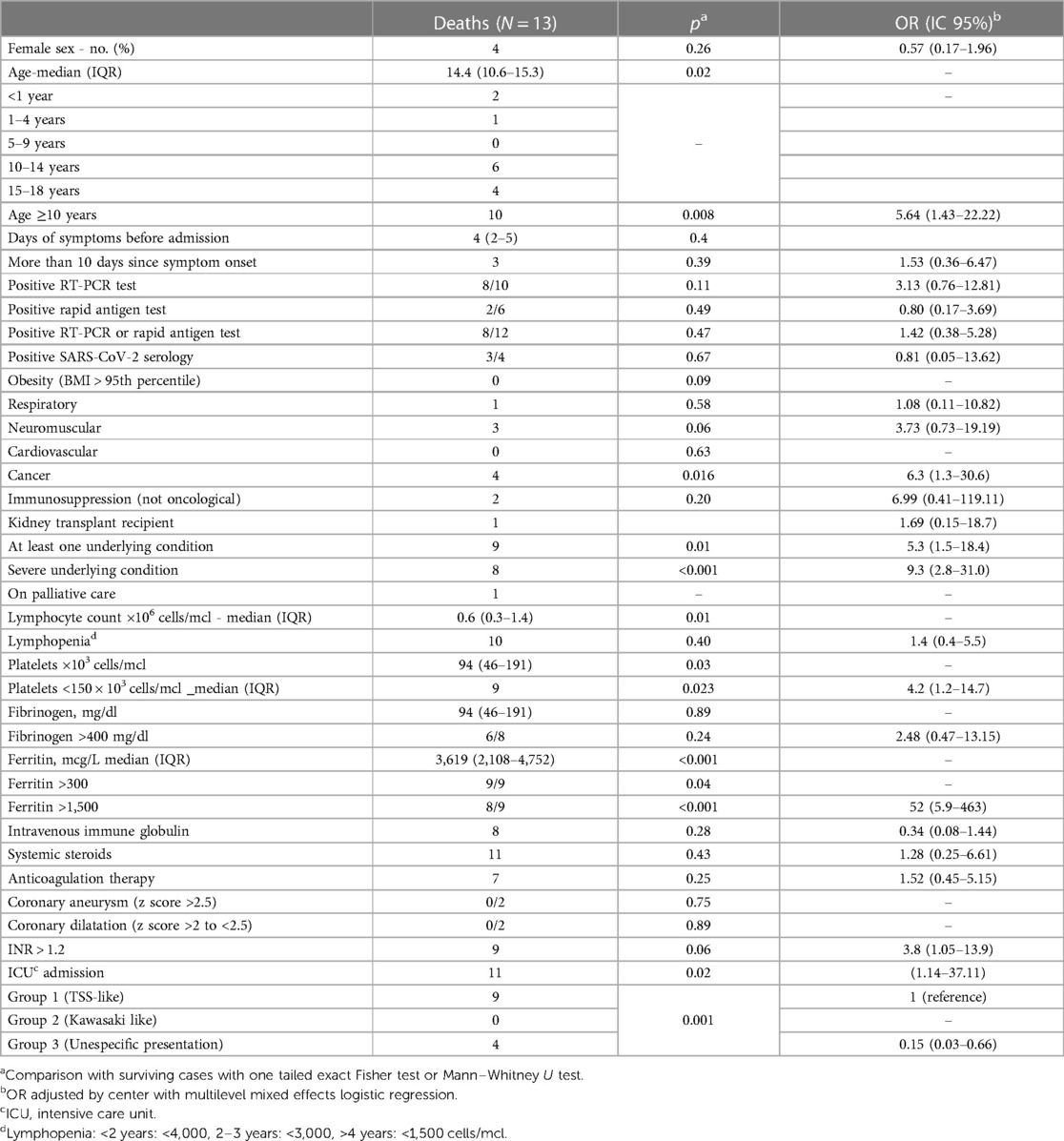
Table 4. Characteristics of deaths and associated conditions.
The patient population was not homogeneous among the eight participating centers. Heterogeneity was high for almost all calculated treatment and outcome frequencies, and I2, a measure of heterogeneity, was 50% for most of the factors. Accordingly, association measures were adjusted for the center effect. A significant cluster effect of the reporting center was demonstrated for every evaluated factor in Tables 3, 4. Disaggregated data collected from the five centers with more included cases are presented in Supplementary Tables S1, S2.
4. Discussion
MIS-C, a recently characterized clinical presentation secondary to SARS-CoV-2 infection, is closely associated with Kawasaki disease and toxic shock syndrome. In the present study, we aimed to summarize the clinical characteristics and outcomes of patients with MIS-C treated in eight pediatric tertiary care centers across Mexico. Our analyses reveal that our study shares several similarities with those reported previously while exhibiting some differences, thus highlighting the high heterogeneity in disease presentation and outcomes among the participating centers.
It is relevant and essential to examine the clinical characteristics, disease management, and outcomes of MIS-C due to the potentially severe consequences such as death (16–18), damage to coronary arteries, and the toll on healthcare resources necessary for its management. The present cohort's mortality rate was 4.6%, which exhibited high heterogeneity across the centers, ranging from 0% to 13.5%. Similarly, the rate of coronary artery abnormalities, which was 18.9% in the overall cohort, ranged from 0% to 56.3% across the participating centers. Published systematic reviews estimate mortality and a rate of coronary artery abnormalities ranging from 0% to 4% and from 11.6% to 21.7%, respectively, in patients with MIS-C, according to the systematic reviews (14, 19–22). In the present study, coronary artery abnormalities were observed in all three clinical groups, with no significant difference in frequency.
Among the factors that might explain the high heterogeneity in outcomes between the centers included in our study and the previously published case series are (i) a wide spectrum of clinical presentation in the presence of relatively nonspecific diagnostic criteria that are currently used for MIS-C, (ii) variations in ethnicity and prevalence of comorbid conditions, and (iii) variations in access, diagnostic paths, and therapeutic interventions across different healthcare systems.
Attempts have been made to classify cases according to their predominant clinical characteristics to address the lack of specific diagnostic criteria and, thus, phenotype heterogeneity. In the present study, we utilized LCA to classify 239 patients into the TSSL-MIS-C, KDL-MIS-C, and U-PIM groups, congruent with the phenotypes identified in previous studies (13–15) In the present study, patient age differed among the clinical groups; additionally, the frequency of virologic positivity was lower, and the frequency of serologic positivity was higher in the KDL-MIS-C group than in the other two clinical groups, suggesting different underlying pathologic mechanisms at play. Multiple pathologic mechanisms have been shown to be altered in MIS-C, including the possible involvement of superantigens and autoantibodies (23). The levels of plasma inflammatory markers were highest in the TSSL-MIS-C group. Additionally, the rate of life support measures and mortality rate were highest in this group. The vagueness of the current clinical criteria for MIS-C might be partially responsible for the wide variation in the rate of these three clinical phenotypes reported by each center, suggesting a lack of clarity among physicians for the threshold of clinical manifestations that eventually leads to the diagnosis of MIS-C (Supplementary Table S1).
Demographic and preexisting medical conditions of patients in different published series and clinical groups widely vary, likely accounting for some of the heterogeneity observed in outcomes.
In the present study, 34.7% of the cohort had underlying conditions, which was higher than that reported by Radia et al. and Antúnez et al. (24). In the present cohort, severe underlying conditions were present in 17.5% of the patients varying from 3.6% to 23.1% across the participating centers. In addition, the frequency of patients with cancer/immunosuppressive disorders or neuromuscular conditions was four to tenfold. In contrast, the observed frequency of obesity (15.9%) was not as high as that reported by other studies (25). Notably, 9 of the 13 deaths in the present cohort had a severe underlying condition, and the mortality was highest in the center with the highest rate of patients with severe underlying conditions and the highest proportion of patients with TSSL-MIS-C. These findings suggest that the high rate of severe underlying conditions might explain the relatively high mortality observed in the present cohort.
Although the centers included in the present study are tertiary care reference hospitals, they belong to different healthcare systems with different protocols for service delivery and different resources for the management of patients during the COVID-19 pandemic; the difference in frequencies of IVIG utilization (from 45% to 94%) might be a reflection of this aspect. In addition, there is evidence of an association between delayed access to health services and worst outcomes, which might explain differences in risk for bad outcomes across different geographic locations (11). Of note, the only factor that was significantly associated with the development of coronary artery abnormalities after adjustment for center effect was a delay of ≥10 days in hospital admission after the onset of symptoms, a factor likely influenced by socioeconomic and geographic factors.
Factors associated with mortality were age ≥10 years, severe underlying condition, thrombocytopenia, hyperferritinemia, and toxic shock syndrome phenotype. A study in a larger cohort might reveal an association with other factors, such as IVIG use and coagulopathy. Abrams et al. reported that older age, non-Hispanic black ethnicity, disease onset before June 1, 2020, and high levels of serum D-dimer, troponin, atrial natriuretic peptide, C-reactive protein (CRP), ferritin, and interleukin-6 were associated with ICU admission in patients with MIS-C. The authors also reported abdominal pain and shortness of breath as clinical findings at hospitalization admission predicting subsequent ICU admission (26).
According to most systematic reviews, myocarditis is the most frequent complication observed in patients with MIS-C; however, it was not examined in the present study due to the lack of a standardized definition among the participating centers. However, left ventricular ejection fraction, which was below 55% in 31% of the cohort, might be considered a proxy for this outcome. In addition, we did not evaluate socioeconomic status, ethnicity, and the levels of D-dimer, troponin-B, natriuretic peptide, or interleukin-6, which were assessed in previous studies.
Our study has several limitations. One of them is related to the heterogeneity of participating centers, the variable reliability of data captured in the different centers, and the high frequency of missing data for some variables. Also, cardiologic outcomes are limited to a single in-hospital measurement with a lack of follow-up. Besides, data collection was started months before the publication of updated case definition criteria for multisystem inflammatory syndrome in children associated with SARS-CoV-2 infection (5). With the updated criteria, 32 cases would not have been included in the final analysis. Of these, 19 observations would not have met the criteria regarding the involvement of two or more systems after the elimination of the respiratory, renal, and neurological criteria, and the modification of the hematological system criteria. Thirteen cases that did have two or more systems involved according to the new criteria had a CRP < 3.0 mg/dl and thus would not have been included; however, these 13 cases did have elevation of at least another inflammation marker according to definitions given in Chart 1.
In conclusion, death was an infrequent outcome in patients with MIS-C, occurring mainly in older patients with severe underlying conditions, whereas coronary aneurysms were primarily associated with delayed treatment. Extrapolation of the frequency of observed outcomes to the general population might not be valid due to the high frequency of comorbid conditions and the heterogeneity of participating centers. The causal association of risk factors with adverse outcomes should be further analyzed in longitudinal studies with sufficient statistical power to adjust for multiple confounding factors found in the present cohort.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by Hospital Infantil de México Federico Gómez Ethics and Investigation Review Board del Hospital Infantil de México Federico Gómez. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
MFCP, NGG, and HMG contributed to the conception and design of the study. HMG coordinated interinstitutional collaboration. NGG and RVS organized the database. MFCP and NGG performed the statistical analysis. MAYN, NGG, and MFCP wrote the first draft of the manuscript. All authors contributed to data gathering and manuscript revision and read and approved the submitted version.
Funding
The authors declare that this study received funding from Hospital Infantil de Mexico Federico Gómez. The funder was not involved in the study design, collection, analysis, or interpretation of data.
Acknowledgments
We acknowledge the authorities of participating centers for the facilities to perform this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1167871/full#supplementary-material.
References
1. Licciardi F, Pruccoli G, Denina M, Parodi E, Taglietto M. SARS-CoV-2 – induced kawasaki-like hyperin flammatory syndrome : a novel COVID phenotype in children. Pediatrics. (2021) 146(2):1–5. doi: 10.1542/peds.2020-1711
2. Centers for Disease Control and Prevention. HAN Archive - 00432 | Health Alert Network (HAN). Available at: https://emergency.cdc.gov/han/2020/han00432.asp (Cited December 13, 2021).
3. Royal College of Paediatrics and Child Health. Guidance paediatric multisystem inflammatory syndrome temporallly associated with Cov-19. Royal College of Paediatrics and Child Health. (2020). p. 1–6. Available at: https://www.rcpch.ac.uk/resources/paediatric-multisystem-inflammatory-syndrome-temporally-associated-covid-19-pims-guidance
4. Jiang L, Tang K, Levin M, Irfan O, Morris SK, Wilson K, et al. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect Dis. (2020) 20(11):e276–88. doi: 10.1016/S1473-3099(20)30651-4
5. Walensky RP, Bunnell R, Layden J, Kent CK, Gottardy AJ, Leahy MA, et al. Morbidity and mortality weekly report council of state and territorial epidemiologists/CDC surveillance case definition for multisystem inflammatory syndrome in children associated with SARS-CoV-2 infection-United States centers for disease control and prevention MMWR editorial and production staff (Serials) MMWR editorial board CONTENTS. Vol. 71, Recommendations and Reports (2022).
6. Feldstein LR, Tenforde MW, Friedman KG, Newhams M, Rose EB, Dapul H, et al. Characteristics and outcomes of US children and adolescents with Multisystem Inflammatory Syndrome in Children (MIS-C) compared with severe acute COVID-19. JAMA. (2021) 325(11):1074–87. doi: 10.1001/jama.2021.2091
7. Son MBF, Murray N, Friedman K, Young CC, Newhams MM, Feldstein LR, et al. Multisystem inflammatory syndrome in children — initial therapy and outcomes. N Engl J Med. (2021) 385(1):23–34. doi: 10.1056/NEJMoa2102605
8. Davies P, Evans C, Kanthimathinathan HK, Lillie J, Brierley J, Waters G, et al. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Health. (2020) 4(9):669–77. doi: 10.1016/S2352-4642(20)30215-7
9. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. (2020) 395(10237):1607–8. doi: 10.1016/S0140-6736(20)31094-1
10. Dufort EM, Koumans EH, Chow EJ, Rosenthal EM, Muse A, Rowlands J, et al. Multisystem inflammatory syndrome in children in New York state. N Engl J Med. (2020) 383(4):347–58. doi: 10.1056/NEJMoa2021756
11. Belay ED, Abrams J, Oster ME, Giovanni J, Pierce T, Meng L, et al. Trends in geographic and temporal distribution of US children with multisystem inflammatory syndrome during the COVID-19 pandemic. JAMA Pediatr. (2021) 175(8):837–45. doi: 10.1001/jamapediatrics.2021.0630
12. Payne AB, Gilani Z, Godfred-Cato S, Belay ED, Feldstein LR, Patel MM, et al. Incidence of multisystem inflammatory syndrome in children among US persons infected with SARS-CoV-2. JAMA Netw Open. (2021) 4(6):e2116420. doi: 10.1001/jamanetworkopen.2021.16420
13. Flood J, Shingleton J, Bennett E, Walker B, Amin-Chowdhury Z, Oligbu G, et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 (PIMS-TS): prospective, national surveillance, United Kingdom and Ireland, 2020. Lancet Reg Health Eur. (2021) 3:1–11. doi: 10.1016/j.lanepe.2021.100075
14. Godfred-Cato S, Abrams JY, Balachandran N, Jaggi P, Jones K, Rostad CA, et al. Distinguishing multisystem inflammatory syndrome in children from COVID-19, kawasaki disease and toxic shock syndrome. Pediatr Infect Dis J. (2022) 41(4):315–23. doi: 10.1097/INF.0000000000003449
15. Geva A, Patel MM, Newhams MM, Young CC, Son MBF, Kong M, et al. Data-driven clustering identifies features distinguishing multisystem inflammatory syndrome from acute COVID-19 in children and adolescents. EClinicalMedicine. (2021) 40:9–10. doi: 10.1016/j.eclinm.2021.101112
16. Laverty M, Salvadori M, Squires SG, Ahmed M, Eisenbeis L, Lee S, et al. Multisystem inflammatory syndrome in children in Canada. Can Commun Dis Rep. (2021) 47(11):461–5. doi: 10.14745/ccdr.v47i11a03
17. Baradaran A, Malek A, Moazzen N, Shaye ZA. COVID-19 associated multisystem inflammatory syndrome: a systematic review and meta-analysis. Iran J Allergy Asthma Immunol. (2020) 19:570–88. doi: 10.18502/ijaai.v19i6.4927
18. Ruvinsky S, Voto C, Roel M, Fustiñana A, Veliz N, Brizuela M, et al. Multisystem inflammatory syndrome temporally related to COVID-19 in children from Latin America and the Caribbean region: a systematic review with a meta-analysis of data from regional surveillance systems. Front Pediatr. (2022) 10:871765. doi: 10.3389/fped.2022.881765
19. Hoste L, Van PR, Haerynck F. Multisystem inflammatory syndrome in children related to COVID-19: a systematic review. Eur J Pediatr. (2021) 180(7):2019–34. doi: 10.1007/s00431-021-03993-5
20. Radia T, Williams N, Agrawal P, Harman K, Weale J, Cook J, et al. Multi-system inflammatory syndrome in children & adolescents (MIS-C): a systematic review of clinical features and presentation. Paediatr Respir Rev. (2021) 38:51–7. doi: 10.1016/j.prrv.2020.08.001
21. Yasuhara J, Watanabe K, Takagi H, Sumitomo N, Kuno T. COVID-19 and multisystem inflammatory syndrome in children: a systematic review and meta-analysis. Pediatr Pulmonol. (2021) 56(5):837–48. doi: 10.1002/ppul.25245
22. Santos MO, Gonçalves LC, Silva PAN, Moreira ALE, Ito CRM, Peixoto FAO, et al. Multisystem inflammatory syndrome (MIS-C): a systematic review and meta-analysis of clinical characteristics, treatment, and outcomes. J Pediatr. (2022) 98:338–49. doi: 10.1016/j.jped.2021.08.006
23. Porritt RA, Binek A, Paschold L, Rivas MN, McArdle A, Yonker LM, et al. The autoimmune signature of hyperinflammatory multisystem inflammatory syndrome in children. J Clin Invest. (2021) 131(20):e151520. doi: 10.1172/JCI151520
24. Antúnez-Montes OY, Escamilla MI, Figueroa-Uribe AF, Arteaga-Menchaca E, Lavariega-Saráchaga M, Salcedo-Lozada P, et al. COVID-19 and multisystem inflammatory syndrome in Latin American children: a multinational study. Pediatr Infect Dis J. (2021) 40(1):e1–e6. doi: 10.1097/INF.0000000000002949
25. Miller A, Zambrano L, Yousaf AR, Abrams JY, Meng L, Wu MJ. Multisystem infalmmatory syndrome in children-United States, February 2020–July 2021. Clin Infect Dis. (2022) 75(1):e1165–75. doi: 10.1093/cid/ciab1007
26. Abrams JY, Oster ME, Godfred-Cato SE, Bryant B, Datta SD, Campbell AP, et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: a retrospective surveillance study. Lancet Child Adolesc Health. (2021) 5(5):323–31. doi: 10.1016/S2352-4642(21)00050-X
Keywords: multisystem inflammatory syndrome, coronary aneurism, coronavirus disease (COVID)-19, Mexico, multicenter study, pediatric, severe acute respiratory syndrome coronavirus (SARS-CoV)
Citation: Yamazaki-Nakashimada MA, Márquez-González H, Miranda-Novales G, Neme Díaz GA, Prado Duran SA, Luévanos Velázquez A, Castilla-Peon MF, González-García N, Sánchez Duran MA, Márquez Aguirre MP, Villasis-Keever MA, Aragón Nogales R, Núñez-Enríquez JC, Martinez Bustamante ME, Aguilar Argüello C, Ramírez de los Santos J, Pérez Barrera A, Palacios Cantú LA, Membrila Mondragón J, Vizcarra Alvarado P, Jiménez Juárez RN, Olivar López V, Velasco-Segura R and López Chávez A (2023) Characteristics and outcomes of multisystem inflammatory syndrome in children: A multicenter, retrospective, observational cohort study in Mexico. Front. Pediatr. 11:1167871. doi: 10.3389/fped.2023.1167871
Received: 17 February 2023; Accepted: 27 March 2023;
Published: 18 May 2023.
Edited by:
Elizabeth Secord, Wayne State University, United StatesReviewed by:
Eric John McGrath, Wayne State University, United StatesMatthew Adams, Wayne State University, United States
Shira Jolene Gertz, Cooperman Barnabas Medical Center, United States
© 2023 Yamazaki-Nakashimada, Márquez-González, Miranda-Novales, Neme Díaz, Prado Duran, Luévanos Velázquez, Castilla-Peon, González-García, Sánchez Duran, Márquez Aguirre, Villasis-Keever, Aragón Nogales, Núñez-Enríquez, Martinez Bustamante, Aguilar Argüello, Ramírez de los Santos, Pérez Barrera, Palacios Cantú, Membrila Mondragón, Vizcarra Alvarado, Jiménez Juárez, Olivar López, Velasco-Segura and López Chávez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria F. Castilla-Peon ZmVybmFuZGFjYXN0aWxsYXBlb25AZ21haWwuY29t Nadia González-García bmFnb256YWxlekBoaW1mZy5lZHUubXg=
Specialty Section: This article was submitted to Pediatric Immunology, a section of the journal Frontiers in Pediatrics