 Nicolás Muñoz-Urtubia1,2
Nicolás Muñoz-Urtubia1,2 Alejandro Vega-Muñoz3,4*
Alejandro Vega-Muñoz3,4* Guido Salazar-Sepúlveda5,6
Guido Salazar-Sepúlveda5,6 Miguel Ángel García-Gordillo7
Miguel Ángel García-Gordillo7 José Carmelo-Adsuar8
José Carmelo-Adsuar8
- 1Facultad de Filosofía y Humanidades, Universidad Austral de Chile, Valdivia, Chile
- 2Escuela Internacional de Graduados, Universidad de Extremadura, Cáceres, Spain
- 3Centro de Investigación en Educación de Calidad Para la Equidad, Universidad Central de Chile, Santiago, Chile
- 4Facultad de Ciencias Empresariales, Universidad Arturo Prat, Iquique, Chile
- 5Facultad de Ingeniería, Universidad Católica de la Santísima Concepción, Concepción, Chile
- 6Facultad de Ingeniería y Negocios, Universidad de las Américas, Concepción, Chile
- 7Facultad de Ciencias Jurídicas y Empresariales, Universidad de La Frontera, Temuco, Chile
- 8Facultad de Ciencias del Deporte, Universidad de Extremadura, Cáceres, Spain
Introduction: This systematic review aimed to examine the impact of physical activity-based interventions on body mass index (BMI) reduction in children aged 6–12 years.
Methods: A comprehensive search was conducted in the PubMed database following PRISMA guidelines and using the PICOS framework. A total of 13,927 records were retrieved, of which seven studies met the inclusion criteria. Methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT).
Results: Included studies comprised both preventive and treatment-oriented interventions that aimed to reduce BMI through physical activity. Interventions that integrated family and school components, and were grounded in behavioral theories such as Self-Determination Theory and Social Cognitive Theory, showed greater effectiveness in reducing BMI and improving body composition.
Discussion: Multilevel strategies that enhance autonomy, competence, and social support within biopsychosocial frameworks appeared to improve motivation and adherence. Although BMI z-score reductions were modest, they reached clinically meaningful thresholds. These findings support the implementation of context-sensitive, comprehensive strategies involving families, schools, and communities to promote healthy behaviors and sustainable outcomes in pediatric populations.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, PROSPERO CRD42024547428.
1 Introduction
Pediatric obesity is a multifactorial disease influenced by biological, psychological, social and environmental factors (1, 2). Factors such as genetic predisposition, poor diet, sedentary lifestyle, low physical activity, mental health problems, socioeconomic context and family dynamics influence both its development and persistence (3, 4). Understanding pediatric obesity requires a biopsychosocial perspective that considers the complexity of interactions among all its causes (5, 6). Physical activity-based interventions, although the focus of this review, show greater efficacy when framed within comprehensive lifestyle and environmental changes (7).
In this context, obesity is currently regarded as a global health problem due to its relentless growth and high prevalence. Consequently, the rates of childhood overweight and obesity have increased significantly worldwide (8). The World Health Organization (WHO) classifies it as a global pandemic (9, 10), making it an urgent public health issue (10, 11). This situation can trigger various pathologies associated with sedentary lifestyles, with lifelong repercussions (12, 13).
Most health issues associated with a sedentary lifestyle are linked to obesity (14). A particularly noteworthy factor contributing to the rising prevalence of overweight and obesity in children and adolescents is the low rate of physical activity observed in this age group. This is largely due to the extended periods spent sitting during school classes (15, 16) and in front of digital screens (17–19). It is estimated that approximately 80% of children and adolescents worldwide do not meet the minimum recommendations for moderate to vigorous physical activity (MVPA) as set out by the WHO (10, 17, 20).
Overweight and obesity, which are associated with high levels of adiposity, have serious health consequences. These include cardiovascular problems, respiratory problems, and metabolic diseases (21, 22). In addition, they can also negatively affect psychosocial and cognitive health (23, 24). Overweight or obese children are more likely to become adults with the same health problems (10). As children grow older, their physical activity levels tend to decrease, which generates a vicious circle between low physical activity and increased adiposity (17, 25, 26).
The benefits of physical activity in childhood and adolescence are well documented. These benefits include improved body composition (27, 28), increased muscle strength and power (29, 30), increased bone mineral density (30, 31), and development of basic motor skills (32, 33). In addition, physical activity reduces the risk of musculoskeletal injuries (33, 34), improves cardiovascular health (35), and increases insulin sensitivity (27, 36).
Likewise, there are academic and social benefits associated with higher levels of cardiorespiratory fitness and cognitive development in children and adolescents (37, 38). It is therefore of paramount importance to maintain and promote physical activity in this population, as physical fitness is an important indicator of overall health (39–42).
Finally, because the higher body mass index in children and adolescents is associated with higher levels of physical inactivity (19, 24, 43), the aim of this review is to analyse the impact of different types of interventions on reducing BMI in the pediatric population and to identify strategies to improve body composition in children. This will allow the design of better prevention and health promotion approaches in this age group.
Given the above, childhood obesity is a public health challenge that requires effective interventions, with physical activity being a key strategy. From a biopsychosocial perspective, which integrates biological, psychological and social factors, it becomes fundamental to consider not only body mass index (BMI), but also body composition as indicators of change. Furthermore, the effectiveness of these interventions depends on contextual and motivational elements such as family and school participation, the duration and intensity of the programs, and the use of technologies. In this framework, it is relevant to identify which characteristics of physical interventions are associated with better outcomes in the childhood population. Which characteristics of physical activity-based interventions, framed within a biopsychosocial approach, are associated with greater reductions in BMI and improvements in body composition in the childhood population?
2 Methods
The systematic review was registered in the PROSPERO database (CRD42024547428). Available at https://www.crd.york.ac.uk/prospero/. PRISMA guidelines were used for this review (44) and PICOS strategies were used to establish eligibility criteria for the articles (45). The review was performed in PubMed, a free specialized database in biomedicine and health, ensuring that the selected articles were directly related to the topic of interest. In addition, the metadata of the PubMed database allows the incorporation of specific search filters such as: Article type, Species, and Age, in this case Randomized Controlled Trial, Human and Child: 6–12 years.
The use of PubMed in biomedical and health systematic reviews is essential due to its high subject specificity, open access and comprehensive coverage of peer-reviewed literature in medical sciences. Studies such as those by Falagas et al. (46) and AlRyalat et al. (47) highlight that PubMed offers more accurate and relevant searches compared to broader databases such as Scopus or Web of Science, mainly thanks to its indexing system with MeSH terms that optimizes the retrieval of specific information, as well as to the specific metadata that is incorporated into the reported studies, such as: clinical typology, species (human and animal), and age range. In addition, recent research such as Kokol (48) evidence important discrepancies in coverage and funding information between Scopus and WoS, underscoring the need to complement these databases with PubMed to obtain a more complete and reliable view. Therefore, incorporating PubMed guarantees methodological rigor and thematic exhaustiveness, essential elements for the quality of systematic reviews in the field of health.
2.1 Search strategies and data sources
The search was performed in the PubMed electronic database using the search vector with the terms: [body mass index (MeSH Terms)] AND [activity, physical (MeSH Terms)]. The search was limited to articles published since 2020 and was conducted on May 16, 2024. Only articles written in English, which accounts for over 95% of indexed publications, and that were randomized clinical trials (RCTs) were included and gray literature was not considered.
2.2 Eligibility criteria
The selection of articles was based on the PICOS criteria, as shown in Table 1. Only randomized, controlled studies involving pediatric population were included, focusing on the reduction and measurement of participants' BMI. Studies were included regardless of whether the intervention included family, school, or both components. Although the inclusion of these contexts was not a requirement for selection, their presence or absence was subsequently documented and analyzed as a potential factor influencing intervention outcomes. Eligible studies focused on the promotion of healthy lifestyles in children through structured physical activity interventions. Studies involving pharmacological, surgical, or exclusively nutritional approaches were excluded. Studies could target either the prevention or treatment of overweight and obesity, as long as the primary outcome was a change in BMI and the intervention included a physical activity component. This review focused on children aged 6–12 years, as this developmental period is characterized by greater stability in behavioral patterns and body composition compared to early childhood or adolescence, making it an ideal window for implementing and evaluating structured physical activity interventions (49, 50).
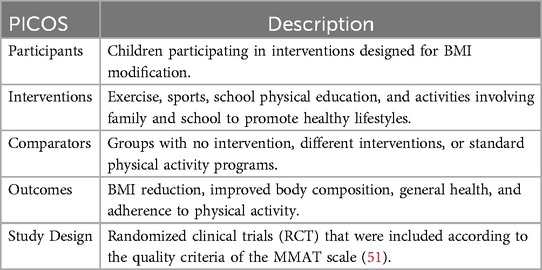
Table 1. Eligibility criteria using PICOS (participants, interventions, comparators, outcomes, and study design).
2.3 Study selection, data extraction and quality assessment
The selection process was carried out in two stages. In the first stage, two independent reviewers evaluated the titles and abstracts of the studies obtained through the search strategy to determine their relevance. Studies that did not meet the inclusion criteria were excluded. Then, in the second stage, the pre-selected studies were subjected to a full text review by the same reviewers to confirm their eligibility. Discrepancies between reviewers were resolved by the intervention of a third reviewer.
Subsequently, details of the interventions and the control group were extracted. This data extraction was performed independently by two reviewers to ensure accuracy. The results obtained were compared and any discrepancies were resolved by discussion or consultation with a third reviewer.
The MMAT (Mixed Methods Appraisal Tool) scale for RCT was applied during the selection and evaluation of studies by three independent reviewers to guarantee quality and methodological rigor, the third being consulted in the event of any discrepancy. The MMAT scale is a checklist based on the synthesis of qualitative and quantitative evidence that includes criteria for the evaluation of mixed studies. The study category is defined, and 7 items are applied according to a score from 0 to 1, obtaining a final percentage measure. Studies are considered to be of high quality >75%, medium quality between 50% and 74% and low quality <49% (51). Of the studies included in this review, only one was of medium quality according to the MMAT scale.
3 Results
The initial PubMed search vector extracted a total of 13,927 records. By applying inclusion filters, such as publication date since 2020, human species, age 6–12 years, gender, study type, and risk control, records are lost at each screening stage. In total, 11,720 records are lost by date, 6 by human species, 1,618 by age, 172 by gender (male, female), 382 by study type, and 22 by risk control. At the end of this process, only articles that meet all inclusion criteria are selected, resulting in a final number of 7 articles for the systematic review (see Figure 1).
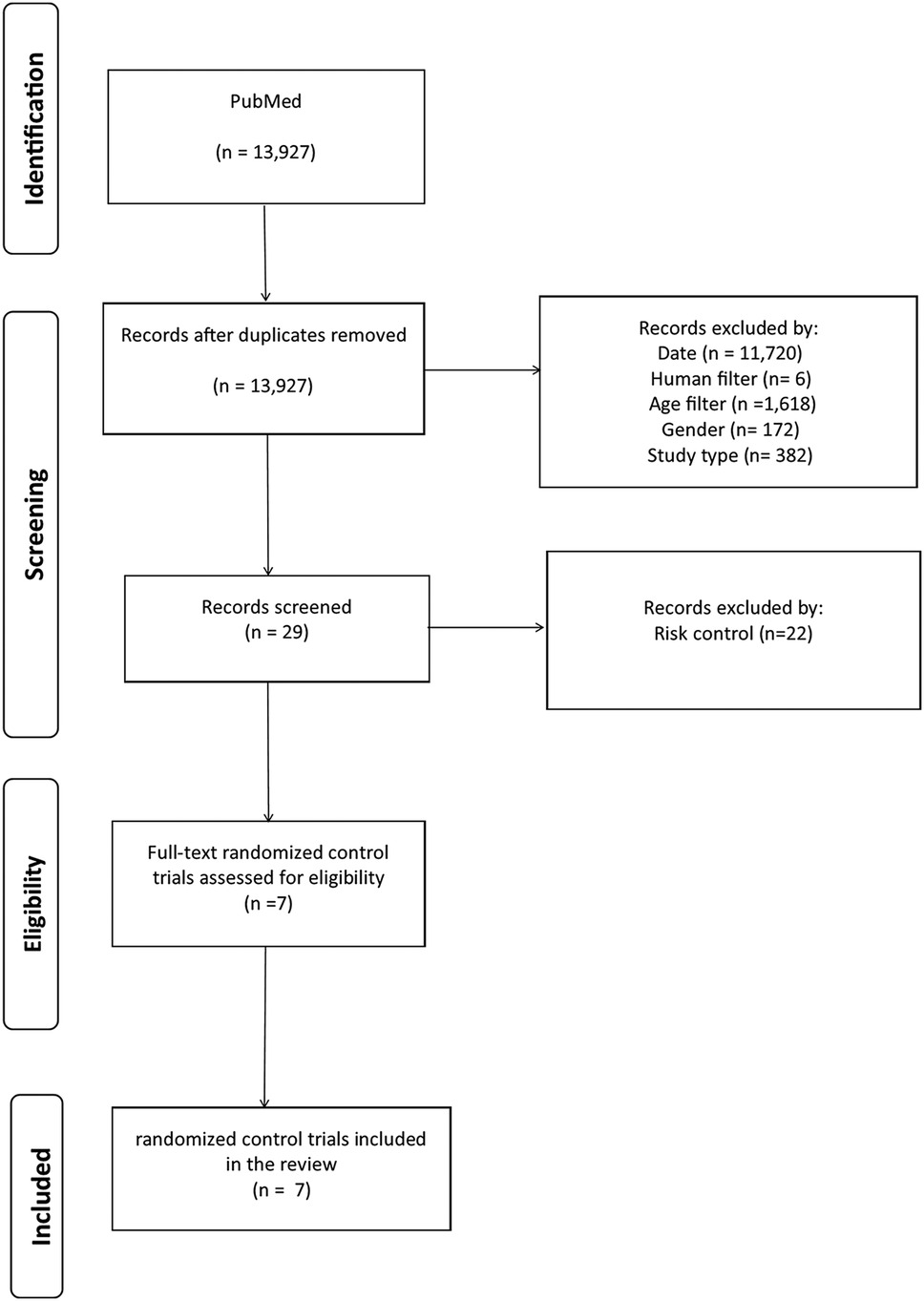
Figure 1. Preferred reporting elements analysis flow for systematic reviews and meta-analyses (PRISMA).
Using the PRISMA guidelines, 7 articles were selected (44). Table 2 shows the details, which are authors, journal, year of publication, citation, indexing, sample and study design. In addition, Table 3 details the eligibility criteria of the articles using the MMAT scale.
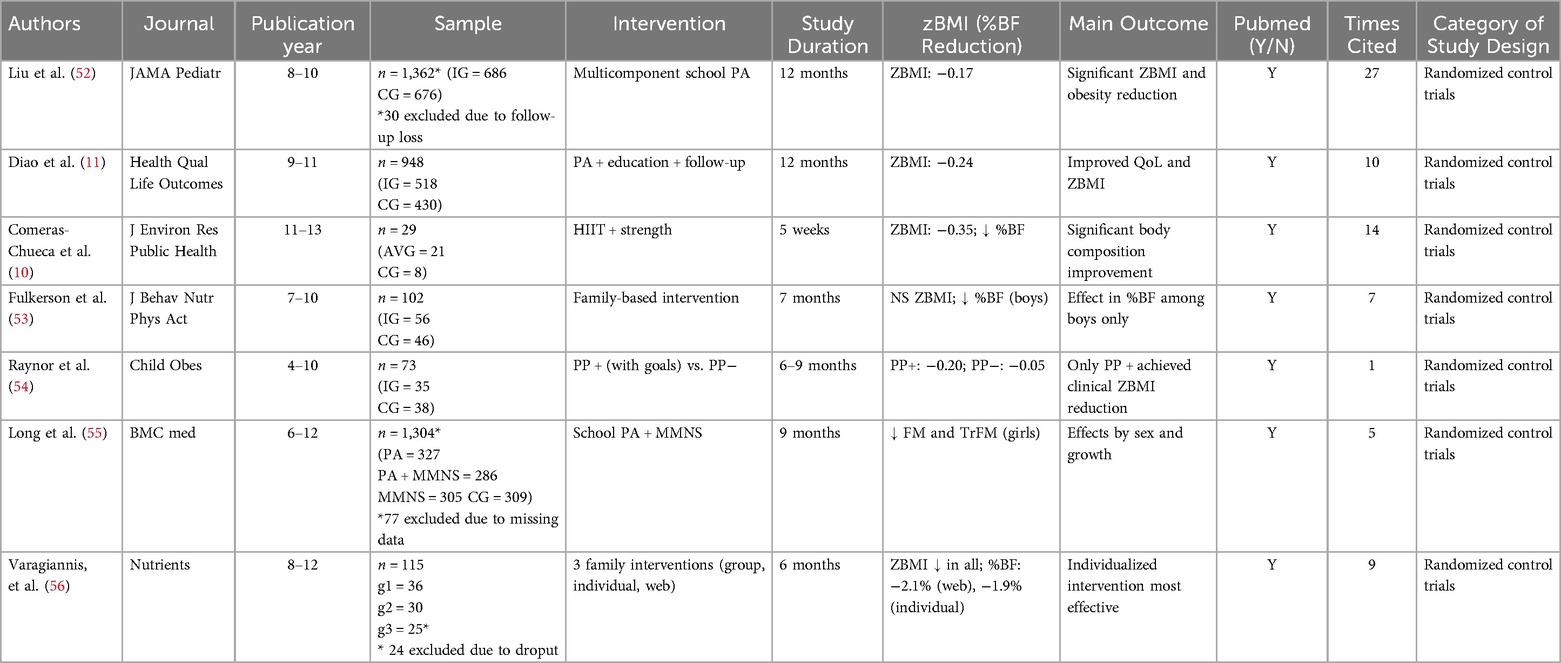
Table 2. Characteristics of selected studies.
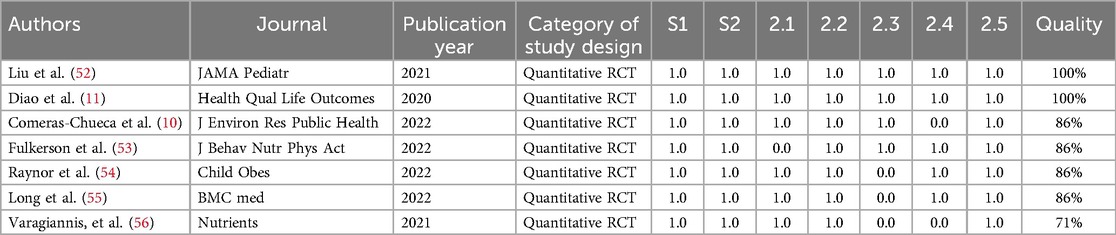
Table 3. Eligibility criteria using the mixed methods assessment tool (MMAT).
The heterogeneity of the results reported in Table 2 prevents progressing towards a meta-analytic analysis. Thus, the studies included in this review were classified according to their main themes into 4 categories as shown in Table 4.
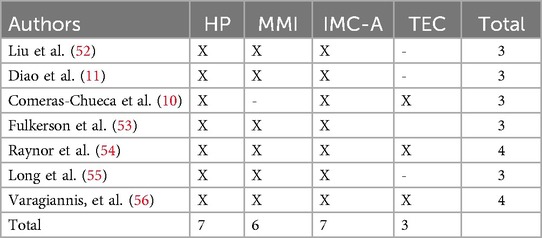
Table 4. Classification according to main themes in 4 categories.
From the articles analyzed, 4 total categories concerning effective interventions related to the decrease of BMI in pediatric population emerged, which are: Health promotion and healthy behavior modification (HP), Integral and multidimensional interventions (MMI), Use of BMI as an indicator of adiposity in pediatric population (BMI-A), Incorporation of technologies in intervention and follow-up (TEC). The results are detailed below.
3.1 Health promotion and healthy behavior modification
Five of the categorized articles focused on interventions involving the family and/or caregivers, the school, or both (11, 52–55). Health promotion and healthy behavior modification focus mainly on educational strategies and programs that promote and shape healthy lifestyle habits in the pediatric population. These include education on balanced diet, promotion of regular physical activity, reduction of screen time and setting nutritional goals for caregivers and families as well as for children and adolescents participating in the programs. Early adoption of lifestyle changes is crucial, since when they are adopted at an early age, they tend to be more stable throughout the different stages of growth.
3.2 Integral and multidimensional interventions
Integral and multimodal interventions include the coordinated participation of different stakeholders, such as family, caregivers, teachers, and the school community at large. These interventions are more effective in improving adherence to BMI reduction interventions in the pediatric population compared to those that do not involve multiple stakeholders. Comprehensive, multidimensional interventions create a holistic supportive environment that facilitates the adoption and maintenance of healthy behaviors through a consistent and cohesive support network. This approach recognizes the importance of a structured and supportive environment that includes not only the immediate family, but also other important stakeholders in the child's life, such as teachers and health professionals, thus ensuring more effective and sustained implementation of lifestyle changes.
3.3 Use of BMI as an indicator of adiposity in the pediatric population
In all the articles reviewed, BMI was used as the gold standard to measure the general adiposity of the subjects. Although one study supplemented BMI data with bioimpedance (56), BMI is confirmed as a reliable tool to assess the risk of being overweight and obesity in childhood. It stands out as a valid option for measuring body fat in the pediatric population, as the poor development of muscle mass at this stage suggests that increases in body mass are mainly due to increased fat mass (57).
3.4 Incorporation of technologies in intervention and follow-up
The use of digital technologies and technological tools facilitates the implementation of interventions as well as monitoring and follow-up during these interventions aimed at reducing BMI in children and adolescents. Within this category were included the use of active video games and accelerometer (10), reports through digital forms (54), use of mobile applications (52) and web pages (56). The inclusion of technology can increase participation, since the tools used allow for more accurate measurement of progress, in addition to generating greater attraction for participants to increase daily physical activity.
4 Discussion
4.1 Framing interventions within a biopsychosocial perspective
The findings of this review underscore that physical activity-based interventions are more effective when framed within a biopsychosocial approach, which incorporates family dynamics, school settings, individual behaviors, and broader social contexts, with families acting not just as contextual modulators, but as active agents whose engagement is central to intervention success.
This integrative perspective is exemplified by Liu et al. (52), whose intervention included both school and family environments through app-based follow-up, emphasizing the influence of parental involvement and environmental support in facilitating behavior change.
This aligns with Engel's biopsychosocial model (5), which posits that complex health outcomes like pediatric obesity result from the interplay between biological, psychological, and social factors. Applying this framework enhances the interpretative power of the current findings.
The review synthesizes evidence supporting the efficacy of physical activity-based interventions in reducing BMI in children aged 6–12 years. While it included both preventive and treatment-focused strategies, the distinction between these two approaches was not a central analytical criterion. For instance, Fulkerson et al. (53) conducted a preventive intervention targeting a general population, whereas Varagiannis et al. (56) focused on treating children with overweight or obesity.
While this review included both preventive and treatment-oriented interventions, few studies clearly specified their primary intent or described baseline characteristics in detail. This lack of differentiation limited the ability to assess outcome variations across subgroups.
Notably, Raynor et al. (54) did report baseline BMI classifications and found that clinically meaningful reductions in BMI z-scores were achieved only in the group involving caregiver goal setting. This suggests that personalized, family-inclusive approaches may be particularly effective in treatment settings.
These distinctions are relevant because children with overweight or obesity at baseline may respond differently than their normal-weight peers, particularly when the intensity and behavioral support of the intervention vary.
4.2 Motivational mechanisms and theoretical foundations
According to Self-Determination Theory (58), intrinsic motivation is strengthened when individuals experience autonomy, competence, and social connectedness. Interventions that support these factors are more likely to foster lasting behavioral change, particularly when tailored to the developmental stage of children and embedded in supportive environments.
This approach is exemplified by Liu et al. (52), whose intervention combined family engagement with school-based activities to enhance environmental and social support.
Supporting this framework, a recent study in Chilean schoolchildren (59) found a significant inverse relationship between BMI and motivation for physical activity. These findings suggest that interventions focusing on motivational components, particularly within educational settings, may yield more effective outcomes. They also underscore the need to go beyond informational strategies and incorporate behavioral reinforcement mechanisms.
Additionally, Bandura's Social Cognitive Theory (60) emphasizes the importance of perceived self-efficacy, observational learning, and social reinforcement in adopting and maintaining health-related behaviors.
Applying this lens, interventions that incorporate role models, parental reinforcement, and peer support may further enhance behavioral adherence, a crucial determinant of long-term outcomes.
While theoretical models such as Self-Determination Theory and Social Cognitive Theory provide a strong foundation for understanding motivation, their application is most effective when combined with active family involvement that reinforces autonomy, competence, and behavioral modeling at home.
4.3 Intervention intensity, duration, and adherence
The included studies exhibited considerable variability in terms of intensity and duration, ranging from short-term interventions to year-long strategies. For example, Comeras-Chueca et al. (10) implemented a 5-week high-intensity program focused on HIIT and strength training, while Liu et al. (52) conducted a 12-month intervention integrating school and family components.
Despite these differences, most studies failed to report the total number of contact hours. None appeared to meet the 26-hour minimum recommended by the U.S. Preventive Services Task Force (USPSTF) for effective pediatric obesity treatment (61). This omission limits the clinical applicability of the findings, as it weakens alignment with established guidelines. The discrepancy between research protocols and clinical standards may also help explain the modest effect sizes observed, reinforcing the need for more intensive, sustained interventions.
Intervention effectiveness was influenced by several key factors, including participant adherence, program continuity, measurement reliability, and the involvement of multiple stakeholders in children's health.
The most successful interventions in reducing BMI and preventing obesity were those that engaged both schools and caregivers. For instance, Jacob et al. (62) emphasized the critical role of family and teacher involvement in improving pediatric BMI. Furthermore, Raynor et al. (54) found that when caregivers were encouraged to set and achieve their own nutritional goals, children's body composition improved even more. These results also align with the recommendations of the WHO Commission on Ending Childhood Obesity, which advocates for school-based and family-centered strategies as core elements of national public health plans aimed at reducing childhood obesity (63).
4.4 Effectiveness and clinical significance of BMI reductions
Across the studies included in this review, reductions in BMI z-scores ranged from −0.17 to −0.35. These values align with prior evidence indicating that even small improvements (≥ −0.1 ZBMI) are associated with clinically meaningful reductions in cardiometabolic risk in children (64).
In addition to BMI changes, some studies reported improvements in body composition. For example, Raynor et al. (54) and Varagiannis et al. (56) documented decreases in total body fat percentage ranging from 1.9% to 2.1%, reinforcing the clinical significance of these interventions, even in short-term formats.
Taken together, the findings suggest that even modest BMI reductions achieved through physical activity-based interventions supported by families and schools are clinically relevant and contribute meaningfully to pediatric obesity prevention within a biopsychosocial framework.
These modest yet clinically meaningful reductions, particularly when supported by families and schools, underscore the value of biopsychosocial strategies in sustainable pediatric obesity prevention.
The role of schools in addressing childhood obesity is especially relevant given current behavioral patterns. Children and adolescents today spend prolonged periods sitting, particularly during school hours, and increasingly engage in screen-based leisure activities (8, 9, 65).
These behavioral trends contribute to low levels of physical activity worldwide. According to global surveillance data, approximately 80% of children and adolescents fail to meet the World Health Organization's recommendation of at least 60 min of moderate-to-vigorous physical activity per day (17, 20). This lack of adherence to basic activity guidelines underscores the need for school-based programs that can interrupt sedentary routines and promote active behaviors throughout the day.
On the other hand, improving BMI outcomes in children requires promoting healthy behaviors beyond physical activity alone. Key strategies include increasing the consumption of fruits and vegetables (66), reducing intake of sugar and ultra-processed foods (67), limiting sedentary and screen time (62, 68), and promoting daily movement (69).
Reviews such as Tremblay et al. (65) support the effectiveness of reducing screen time to under 2 h per day in combination with increasing daily physical activity. However, as highlighted by Spiga et al. (70), dietary interventions alone are generally insufficient to achieve long-term BMI improvements. This reinforces the need for integrated strategies that combine nutritional education with physical activity promotion.
Different approaches have proven useful in increasing MVPA in children, including traditional methods such as aerobic and strength training (71, 72), high-intensity interval training (HIIT) (73, 74), and even active video games. Although not a substitute for structured exercise, these games can complement programs by increasing daily energy expenditure, as suggested by Comeras-Chueca et al. (10). Jurado-Castro et al. (75) further emphasize that increasing daily MVPA should be a central strategy for reducing general adiposity in the pediatric population.
4.5 Limitations of BMI and the need for complementary measures
In addition, despite its limitations, BMI remains a widely used and practical tool for assessing adiposity and obesity risk in pediatric populations. Its consistent use across studies enables comparisons between different groups and settings (70, 76).
Notably, BMI has also demonstrated utility in children with specific conditions such as Down syndrome and autism spectrum disorder. Although these populations may not show significant BMI reductions following interventions, studies indicate that BMI can still serve as a valid indicator for monitoring body composition changes and health risks (77, 78).
These findings support the continued use of BMI as a baseline measure in pediatric health research and practice. However, they also highlight the importance of complementing BMI with other indicators, such as fat percentage, lean mass, or bioimpedance análisis, to better capture the nuanced physiological effects of interventions.
4.6 Multilevel approaches and the role of stakeholders
Our findings confirm that multimodal interventions, those involving families, caregivers, schools, and health professionals, are the most effective for reducing BMI in children. These approaches benefit from the interaction of multiple stakeholders who influence children's daily behaviors and environments.
The integration of technological tools into such interventions has also shown promise. Wearables, mobile applications, and digital platforms can enhance adherence, enable individualized feedback, and improve monitoring capacity. When combined with in-person support and structured routines, these tools may help sustain healthy behaviors over time.
BMI continues to be a viable and widely used indicator for assessing adiposity in pediatric populations; however, its interpretation should prioritize changes in adipose tissue rather than BMI values alone (79). To enhance accuracy, it is recommended to complement BMI with additional assessments such as bioimpedance analysis (13). Furthermore, effective interventions should integrate educational strategies that promote healthy behavior adoption, involving not only schools, parents, and students, but also health professionals. Given that overweight and obesity constitute pressing public health concerns (11), incorporating healthcare system actors is essential for achieving broader and more sustained outcomes (53).
Childhood obesity remains a global public health concern, with significant physical, psychological, and social consequences. School-based interventions have shown particular effectiveness in addressing this issue, especially when multiple strategies are combined.
4.7 Evidence from diverse sociocultural contexts
In China, Liu et al. (52) implemented a multifaceted intervention that included educational activities, modifications to the school environment, and family involvement. This approach led to substantial improvements in anthropometric indicators and health-related behaviors. Similarly, Diao et al. (11) reported that multi-component interventions not only reduced body weight but also enhanced health-related quality of life among children and adolescents.
Evidence from other settings supports these findings. In the United States, the NU-HOME study conducted in rural communities by Fulkerson et al. (53) demonstrated that a family-centered intervention aimed at improving the home food environment and promoting physical activity produced positive outcomes in weight management. Likewise, Raynor et al. (54) showed that implementing the Prevention Plus program in underserved primary care settings was both feasible and well received, emphasizing the importance of tailoring interventions to sociocultural and economic contexts.
In the Global South, Long et al. (55) evaluated the KaziAfya program in South Africa and found that comprehensive school-based strategies, including regular physical activity and health education, effectively improved children's body composition. This approach underscores the school as a key setting for instilling healthy behaviors from an early age, particularly when families, educators, and health professionals are actively involved.
School-based interventions appear most effective when they combine educational content, structural changes, and active community participation. To ensure sustainability and long-term impact, such interventions must also account for cultural, geographic, and socioeconomic diversity.
Taken together, the findings of this review highlight that physical activity-based interventions, particularly those integrating family and school components, and supported by motivational and behavioral strategies, are most effective in promoting BMI reduction in children. To ensure long-term sustainability, such interventions must be embedded within biopsychosocial frameworks that account for cultural, geographic, and socioeconomic diversity. Integrative models that adapt to specific community needs enhance engagement, relevance, and effectiveness, making them key to scalable and equitable public health strategies.
4.8 Implications for future research and public health
A key limitation of this review is the exclusive use of PubMed as the search database, which may have restricted the scope of included studies, as relevant research indexed in other databases such as Scopus or Web of Science might have been omitted. Although the selection process was rigorous, only seven studies were ultimately included from over 13,000 records, which may limit the generalizability of the findings. Future systematic reviews should incorporate additional databases to enhance comprehensiveness and minimize potential selection bias.
In addition, future research should expand beyond BMI as a sole indicator and incorporate additional measures, such as fat percentage, muscle mass, or waist circumference, to more accurately reflect changes in body composition. Longitudinal studies are also needed to assess the sustained impact of interventions over time. Moreover, incorporating digital tools could enhance adherence and support the adoption of healthy behaviors, particularly in children and adolescents, where early prevention and health promotion have long-term benefits.
5 Conclusion
This systematic review confirms that physical activity-based interventions can reduce BMI and improve body composition in children aged 6–12 years, particularly when both families and schools are actively involved. Multilevel strategies that engage caregivers strengthen adherence and motivation through consistent social and environmental support.
While BMI remains a practical tool in pediatric health, its limitations, especially during growth and puberty, highlight the need for complementary indicators such as fat percentage, lean mass, and waist circumference to more accurately reflect physiological changes.
Interventions grounded in Self-Determination Theory and Social Cognitive Theory appear more effective in promoting autonomy, competence, and social connectedness. However, sustained outcomes are most likely when these frameworks are embedded within a broader biopsychosocial perspective that includes families, schools, and community environments.
Although the observed reductions in BMI z-scores were modest, they fall within clinically meaningful thresholds and may contribute to improved cardiometabolic health. Still, the short duration and limited intensity of most interventions indicate the need for more robust, long-term strategies aligned with clinical guidelines.
In conclusion, public health strategies should prioritize comprehensive, context-sensitive physical activity programs that engage families, schools, and communities, not only to reduce excess weight, but also to promote physical literacy, healthy behaviors, and psychosocial well-being.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
NM-U: Writing – original draft, Writing – review & editing, Conceptualization, Formal analysis, Methodology. AV-M: Conceptualization, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing, Funding acquisition. GS-S: Conceptualization, Validation, Writing – original draft, Writing – review & editing, Formal analysis, Funding acquisition. MG-G: Funding acquisition, Validation, Writing – review & editing. JC-A: Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The Article Processing Charge (APC) was partially funded by Universidad Católica de la Santísima Concepción (Code: APC2025). Additionally, the publication fee (APC) was partially financed through the Publication Incentive Fund, 2024, by the Universidad Arturo Prat (Code: APC2025), Universidad de la Frontera (Code: APC2025), Universidad Central de Chile (Code: APC2025) and Universidad de Las Americas (Code: APC2025) and Funding from the Engineering 2030 Project (ING222010004) and support from the UCSC Research Department, Academic Activities Fund 2024.
Acknowledgments
The authors used ChatGPT (OpenAI, GPT-4, https://chat.openai.com) to assist in formulating and clarifying author-developed ideas during the writing process. All content was reviewed and approved by the authors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1449436/full#supplementary-material
References
1. Lobstein T, Jackson-Leach R. Planning for the worst: estimates of obesity and comorbidities in school-age children in 2025. Pediatr Obes. (2016) 11(5):321–5. doi: 10.1111/ijpo.12185
2. Biro FM, Wien M. Childhood obesity and adult morbidities. Am J Clin Nutr. (2010) 91(5):1499S–505. doi: 10.3945/ajcn.2010.28701B
3. Sahoo K, Sahoo B, Choudhury AK, Sofi NY, Kumar R, Bhadoria AS. Childhood obesity: causes and consequences. J Family Med Prim Care. (2015) 4(2):187–92. doi: 10.4103/2249-4863.154628
4. Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes. (2011) 35(7):891–8. doi: 10.1038/ijo.2010.222
5. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. (1977) 196(4286):129–36. doi: 10.1126/science.847460
6. Rankin J, Matthews L, Cobley S, Han A, Sanders R, Wiltshire HD, et al. Psychological consequences of childhood obesity: psychiatric comorbidity and prevention. Adolesc Health Med Ther. (2016) 7:125–46. doi: 10.2147/AHMT.S101631
7. Waters E, de Silva-Sanigorski A, Hall BJ, Brown T, Campbell KJ, Gao Y, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev. (2011) (12):CD001871. doi: 10.1002/14651858.CD001871.pub3
8. López J, Brazo J, Yuste J, Cavichiolli F. Weight status is related to health-related physical fitness and physical activity but not to sedentary behaviour in children. Int J Environ Res Public Health. (2020) 17(12):4518. doi: 10.3390/ijerph17124518
9. Berry E. The obesity pandemic—whose responsibility? No blame, no shame, not more of the same. Front Nutr. (2020) 7:2. doi: 10.3389/fnut.2020.00002
10. Comeras-Chueca C, Villalba-Heredia L, Perez-Lasierra JL, Marín-Puyalto J, Lozano-Berges G, Matute-Llorente Á, et al. Active video games improve muscular fitness and motor skills in children with overweight or obesity. Int J Environ Res Public Health. (2022) 19(5):2642. doi: 10.3390/ijerph19052642
11. Diao H, Wang H, Yang L, Li T. The impacts of multiple obesity-related interventions on quality of life in children and adolescents: a randomized controlled trial. Health Qual Life Outcomes. (2020) 18(1):213. doi: 10.1186/s12955-020-01459-0
12. Malo-Serrano M, Castillo NM, Pajita DD. La obesidad en El Mundo. An la Fac Med. (2017) 78(2):173–8. doi: 10.15381/anales.v78i2.13213
13. Guddal M, Stensland S, Småstuen M, Johnsen M, Heuch I, Zwartz J, et al. Obesity in young adulthood: the role of physical activity level, musculoskeletal pain, and psychological distress in adolescence (the HUNT-study). Int J Environ Res Public Health. (2020) 17(12):4603. doi: 10.3390/ijerph17124603
14. Mendoza-Muñoz M, Vega-Muñoz A, Carlos-Vivas J, Denche-Zamorano Á, Adsuar JC, Raimundo A, et al. The bibliometric analysis of studies on physical literacy for a healthy life. Int J Environ Res Public Health. (2022) 19(22):15211. doi: 10.3390/ijerph192215211
15. Mazoli E, Harriet K, Salmon J, Pesce C, May T, Wei-Peng T, et al. Feasibility of breaking up sitting time in mainstream and special schools with a cognitively challenging motor task. J Sport Heal Sci. (2019) 8:137–48. doi: 10.1016/j.jshs.2019.01.002
16. Parrish AM, Trost SG, Howard SJ, Batterham M, Cliff D, Salmon J, et al. Evaluation of an intervention to reduce adolescent sitting time during the school day: the ‘Stand up for health’ randomised controlled trial. J Sci Med Sport. (2018) 21(12):1244–9. doi: 10.1016/j.jsams.2018.05.020
17. Comeras C, Villalba L, Pérez M, Lozano G, Marín J, Vicente G, et al. Assessment of active video games’ energy expenditure in children with overweight and obesity and differences by gender. Int J Environ Res Public Health. (2020) 17(18):6714. doi: 10.3390/ijerph17186714
18. Salmon J, Arundell L, Hume C, Brown H, Hesketh K, Dunstan DW, et al. A cluster-randomized controlled trial to reduce sedentary behavior and promote physical activity and health of 8-9 year olds: the transform-US! study. BMC Med. (2011) 11:759. doi: 10.1186/1471-2458-11-759
19. Alhusaini AA, Buragadda S, Melam G. Associations among body mass index, sedentary behavior, physical activity, and academic performance in schoolchildren. J Sports Med Phys Fitness. (2020) 60(12):1551–7. doi: 10.23736/S0022-4707.20.10482-1
20. Sutherland R, Campbell E, Lubans D, Morgan P, Okely A, Nathan N, et al. Physical education in secondary schools located in low-income communities: physical activity levels, lesson context and teacher interaction. J Sci Med Sport. (2016) 19(2):135–41. doi: 10.1016/j.jsams.2014.12.003
21. Solomon-Moore E, Salway R, Emm-Collison L, Thompson JL, Sebire SJ, Lawlor DA, et al. Associations of body mass index, physical activity and sedentary time with blood pressure in primary school children from south-west England: a prospective study. Tauler P, editor. PLoS One. (2020) 15(4):e0232333. doi: 10.1371/journal.pone.0232333
22. Cliff DP, Jones RA, Burrows TL, Morgan PJ, Collins CE, Baur LA, et al. Volumes and bouts of sedentary behavior and physical activity: associations with cardiometabolic health in obese children. Obesity. (2014) 22(5):E112–8. doi: 10.1002/oby.20698
23. Romero-Pérez EM, González-Bernal JJ, Soto-Cámara R, González-Santos J, Tánori-Tapia JM, Rodríguez-Fernández P, et al. Influence of a physical exercise program in the anxiety and depression in children with obesity. Int J Environ Res Public Health. (2020) 17(13):4655. doi: 10.3390/ijerph17134655
24. Raine LB, Kao S-C, Drollette ES, Pontifex MB, Pindus D, Hunt J, et al. The role of BMI on cognition following acute physical activity in preadolescent children. Trends Neurosci Educ. (2020) 21:100143. doi: 10.1016/j.tine.2020.100143
25. Kolunsarka I, Gråsten A, Huhtiniemi M, Jaakkaola T. Development of children’s actual and perceived motor competence, cardiorespiratory fitness, physical activity, and BMI. Med Sci Sport Exerc. (2021) 53(12):2653–60. doi: 10.1249/MSS.0000000000002749
26. Lubans L, Morgan P, McCormack A. Adolescents and school sport: the relationship between beliefs, social support and physical self-perception. Phys Educ Sport Pedagog. (2011) 16(3):237–50. doi: 10.1080/17408989.2010.532784
27. Guillem C, Loaiza A, Rial T, Faigenbaum A, Chulvi I. The effects of resistance training on blood pressure in preadolescents and adolescents: a systematic review and meta-analysis. Int J Environ Res Public Health. (2020) 17(21):7900. doi: 10.3390/ijerph17217900
28. Leppänen MH, Henriksson P, Delisle Nyström C, Henriksson H, Ortega FB, Pomeroy J, et al. Longitudinal physical activity, body composition, and physical fitness in preschoolers. Med Sci Sport Exerc. (2017) 49(10):2078–85. doi: 10.1249/MSS.0000000000001313
29. Fang H, Quan M, Zhou T, Sun S, Zhang J, Zhang H, et al. Relationship between physical activity and physical fitness in preschool children: a cross-sectional study. Wen X, editor. Biomed Res Int. (2017) 2017:9314026. doi: 10.1155/2017/9314026
30. Myers A, Beam N, Fakhoury J. Resistance training for children and adolescents. Transl Pediatr. (2017) 6(3):137–43. doi: 10.21037/tp.2017.04.01
31. Gabel L, Mcdonald HM, Nettlefold L, Mckay HA. Physical activity, sedentary time, and bone strength from childhood to early adulthood: a mixed longitudinal HR-pQCT study. J Bone Miner Res. (2017) 32(7):1525–36. doi: 10.1002/jbmr.3115
32. Barnett L, Morgan P, Van Beurden E, Ball K, Lubans D. A reverse pathway? Actual and perceived skill proficiency and physical activity. Med Sci Sport Exerc. (2011) 43(5):898–904. doi: 10.1249/MSS.0b013e3181fdfadd
33. Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput J-P, Janssen I, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. (2016) 41(6 Suppl 3):S197–239. doi: 10.1139/apnm-2015-0663
34. Zwolski C, Quatman C, Paterno M. Resistance training in youth: laying the foundation for injury prevention and physical literacy. Sports Health. (2017) 9(5):436–43. doi: 10.1177/1941738117704153
35. Zhou Z, Li S, Yin J, Fu Q, Ren H, Jin T, et al. Impact on physical fitness of the Chinese champs: a clustered randomized controlled trial. Int J Environ Res Public Health. (2019) 16(22):4412. doi: 10.3390/ijerph16224412
36. Peña G, Heredia J, Lloret C, Martín M, Da Silva M. Iniciación al entrenamiento de fuerza en edades tempranas: revisión. Rev Andaluza Med del Deport. (2016) 9(1):41–9. doi: 10.1016/j.ramd.2015.01.022
37. Kirk S, Kirk E. Sixty minutes of physical activity per day included within preschool academic lessons improves early literacy. J Sch Health. (2016) 86(3):155–63. doi: 10.1111/josh.12363
38. Vetter M, O’Connor H, O’Dwyer N, Orr R. Learning “math on the move”: effectiveness of a combined numeracy and physical activity program for primary school children. J Phys Act Heal. (2018) 15(7):492–8. doi: 10.1123/jpah.2017-0234
39. Caamaño-Navarrete F, Latorre-Román PÁ, Párraga-Montilla JA, Álvarez C, Delgado-Floody P. Association between creativity and memory with cardiorespiratory fitness and lifestyle among Chilean schoolchildren. Nutrients. (2021) 13(6):1799. doi: 10.3390/nu13061799
40. Campbell JP, Turner JE. Debunking the myth of exercise-induced immune suppression: redefining the impact of exercise on immunological health across the lifespan. Front Immunol. (2018) 9:648. doi: 10.3389/fimmu.2018.00648
41. Sawan SA, Nunes EA, Lim C, McKendry J, Phillips SM. The health benefits of resistance exercise: beyond hypertrophy and big weights. Exerc Sport Mov. (2023) 1(1). doi: 10.1249/ESM.0000000000000001
42. Zhao M, Veeranki SP, Magnussen CG, Xi B. Recommended physical activity and all cause and cause specific mortality in US adults: prospective cohort study. BMJ. (2020) 370:m2031. doi: 10.1136/bmj.m2031
43. Gadais T, Caron T, Ayoub M-B, Karelis A, Nadeau L. The role of the teacher in the implementation of a school-based intervention on the physical activity practice of children. Int J Environ Res Public Health. (2020) 17(19):7344. doi: 10.3390/ijerph17197344
44. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
45. Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S. PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res. (2014) 14(1):579. doi: 10.1186/s12913-014-0579-0
46. Falagas ME, Pitsouni EI, Malietzis GA, Pappas G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: strengths and weaknesses. FASEB J. (2008) 22(2):338–42. doi: 10.1096/fj.07-9492LSF
47. AlRyalat SAS, Malkawi LW, Momani SM. Comparing bibliometric analysis using PubMed, Scopus, and Web of Science databases. J Vis Exp. (2019) (152):e58494. doi: 10.3791/58494
48. Kokol P. Discrepancies among Scopus and Web of Science, coverage of funding information in medical journal articles: a follow-up study. J Med Libr Assoc. (2023) 111(3):703–8. doi: 10.5195/jmla.2023.1513
49. Farooq MA, Parkinson KN, Adamson AJ, Pearce MS, Reilly JK, Hughes AR, et al. Timing of the decline in physical activity in childhood and adolescence: Gateshead millennium cohort study. Br J Sports Med. (2018) 52(15):1002–6. doi: 10.1136/bjsports-2016-096933
50. Jago R, Salway R, Emm-Collison L, Sebire SJ, Thompson JL, Lawlor DA. Association of BMI category with change in children’s physical activity between ages 6 and 11 years: a longitudinal study. Int J Obes. (2020) 44(1):104–13. doi: 10.1038/s41366-019-0459-0
51. Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ Inform. (2018) 34(4):285–91. doi: 10.3233/EFI-180221
52. Liu Z, Gao P, Gao A-Y, Lin Y, Feng X-X, Zhang F, et al. Effectiveness of a multifaceted intervention for prevention of obesity in primary school children in China. JAMA Pediatr. (2022) 176(1):e214375. doi: 10.1001/jamapediatrics.2021.4375
53. Fulkerson JA, Horning M, Barr-Anderson DJ, Sidebottom A, Linde JA, Lindberg R, et al. Weight outcomes of NU-HOME: a randomized controlled trial to prevent obesity among rural children. Int J Behav Nutr Phys Act. (2022) 19(1):29. doi: 10.1186/s12966-022-01260-w
54. Raynor HA, Propst S, Robson S, Berlin KS, Barroso CS, Khatri P. Implementing prevention plus with underserved families in an integrated primary care setting. Child Obes. (2022) 18(4):254–65. doi: 10.1089/chi.2021.0071
55. Long KZ, Beckmann J, Lang C, Seelig H, Nqweniso S, Probst-Hensch N, et al. Impact of a school-based health intervention program on body composition among South African primary schoolchildren: results from the KaziAfya cluster-randomized controlled trial. BMC Med. (2022) 20(1):27. doi: 10.1186/s12916-021-02223-x
56. Varagiannis P, Magriplis E, Risvas G, Vamvouka K, Nisianaki A, Papageorgiou A, et al. Effects of three different family-based interventions in overweight and obese children: the “4 your family” randomized controlled trial. Nutrients. (2021) 13(2):341. doi: 10.3390/nu13020341
57. Faigenbaum AD, Kraemer WJ, Blimkie CJR, Jeffreys I, Micheli LJ, Nitka M, et al. Youth resistance training: updated position statement paper from the national strength and conditioning association. J Strength Cond Res. (2009) 23(5 Suppl):S60–79. doi: 10.1519/JSC.0b013e31819df407
58. Ryan R, Deci E. Self-determination theory. In: Maggino F, editor. Encyclopedia of Quality of Life and Well-Being Research. Cham: Springer (2022). Available online at: https://link.springer.com/referenceworkentry/10.1007/978-3-319-69909-7_2630-2
59. Muñoz-Urtubia N, Vega-Muñoz A, Salazar-Sepúlveda G, Contreras-Barraza N, Mendoza-Muñoz M, Ureta-Paredes W, et al. Relationship between body composition and physical literacy in Chilean children (10 to 16 years): an assessment using CAPL-2. J Clin Med. (2024) 13(23):7027. doi: 10.3390/jcm13237027
60. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. (2001) 52:1–26. doi: 10.1146/annurev.psych.52.1.1
61. U.S. Preventive Services Task Force. Screening for obesity in children and adolescents: US preventive services task force recommendation statement. J Am Med Assoc. (2017) 317(23):2417–26. doi: 10.1001/jama.2017.6803
62. Jacob CM, Hardy-Johnson PL, Inskip HM, Morris T, Parsons CM, Barrett M, et al. A systematic review and meta-analysis of school-based interventions with health education to reduce body mass index in adolescents aged 10 to 19 years. Int J Behav Nutr Phys Act. (2021) 18(1):1. doi: 10.1186/s12966-020-01065-9
63. World Health Organization. Report of the Commission on Ending Childhood Obesity. Geneva: WHO (2016) Available online at: https://www.who.int/publications/i/item/9789241510066 (Accessed April 10, 2025).
64. Ford AL, Hunt LP, Cooper A, Shield JP. What reduction in BMI SDS is required in obese adolescents to improve body composition and cardiometabolic health? Arch Dis Child. (2010) 95(4):256–61. doi: 10.1136/adc.2009.165340
65. Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. (2011) 8(1):98. doi: 10.1186/1479-5868-8-98
66. Delgado Floody PA, Caamaño Navarrete F, Jerez Mayorga D, Cofré-Lizama A, Guzmán Guzmán I. The association between children’s food habits, anthropometric parameters and health-related quality of life in Chilean school-age children. Nutr Hosp. (2019) 36(5):1061–6. doi: 10.20960/nh.02643
67. Muñoz-Urtubia N, Vega-Muñoz A, Estrada-Muñoz C, Salazar-Sepúlveda G, Contreras-Barraza N, Castillo D. Healthy behavior and sports drinks: a systematic review. Nutrients. (2023) 15(13):2915. doi: 10.3390/nu15132915
68. Kaul A, Bansal N, Sharma P, Aneja S, Mahato MP. Association of screen time usage and physical activity with overweight and obesity among school-going children in Uttar Pradesh. Cureus. (2023) 15(10):e47690. doi: 10.7759/cureus.47690
69. Wyszyńska J, Ring-Dimitriou S, Thivel D, Weghuber D, Hadjipanayis A, Grossman Z, et al. Physical activity in the prevention of childhood obesity: the position of the European childhood obesity group and the European academy of pediatrics. Front Pediatr. (2020) 8:535705. doi: 10.3389/fped.2020.535705
70. Spiga F, Davies AL, Tomlinson E, Moore TH, Dawson S, Breheny K, et al. Interventions to prevent obesity in children aged 5 to 11 years old. Cochrane Database Syst Rev. (2024) 5(5):CD015328. doi: 10.1002/14651858.CD015328.pub2
71. Ahmadi A, Moheb-Mohammadi F, Navabi ZS, Dehghani M, Heydari H, Sajjadi F, et al. The effects of aerobic training, resistance training, combined training, and healthy eating recommendations on lipid profile and body mass index in overweight and obese children and adolescents: a randomized clinical trial. ARYA Atheroscler. (2020) 16(5):226–34. doi: 10.22122/arya.v16i5.1990
72. Wu J, Yang Y, Yu H, Li L, Chen Y, Sun Y. Comparative effectiveness of school-based exercise interventions on physical fitness in children and adolescents: a systematic review and network meta-analysis. Front Public Heal. (2023) 11:1194779. doi: 10.3389/fpubh.2023.1194779
73. Meng C, Yucheng T, Shu L, Yu Z. Effects of school-based high-intensity interval training on body composition, cardiorespiratory fitness and cardiometabolic markers in adolescent boys with obesity: a randomized controlled trial. BMC Pediatr. (2022) 22(1):112. doi: 10.1186/s12887-021-03079-z
74. Solera-Martínez M, Herraiz-Adillo Á, Manzanares-Domínguez I, De La Cruz LL, Martínez-Vizcaíno V, Pozuelo-Carrascosa DP. High-intensity interval training and cardiometabolic risk factors in children: a meta-analysis. Pediatrics. (2021) 148(4):e2021050810. doi: 10.1542/peds.2021-050810
75. Jurado-Castro JM, Gil-Campos M, Gonzalez-Gonzalez H, Llorente-Cantarero FJ. Evaluation of physical activity and lifestyle interventions focused on school children with obesity using accelerometry: a systematic review and meta-analysis. Int J Environ Res Public Health. (2020) 17(17):6031. doi: 10.3390/ijerph17176031
76. Spiga F, Tomlinson E, Davies AL, Moore TH, Dawson S, Breheny K, et al. Interventions to prevent obesity in children aged 12 to 18 years old. Cochrane Database Syst Rev. (2024) 5(5):CD015330. doi: 10.1002/14651858.CD015330.pub2
77. Martínez-Espinosa RM, Molina Vila MD, Reig García-Galbis M. Evidences from clinical trials in down syndrome: diet, exercise and body composition. Int J Environ Res Public Health. (2020) 17(12):4294. doi: 10.3390/ijerph17124294
78. Arkesteyn A, Van Damme T, Thoen A, Cornelissen V, Healy S, Vancampfort D. Physical activity correlates in children and adolescents with autism spectrum disorder: a systematic review. Disabil Rehabil. (2022) 44(22):6539–50. doi: 10.1080/09638288.2021.1970251
Keywords: body mass index, obesity, prevalence, early intervention, physical activity
Citation: Muñoz-Urtubia N, Vega-Muñoz A, Salazar-Sepúlveda G, García-Gordillo MÁ and Carmelo-Adsuar J (2025) Physical activity based interventions for reducing body mass index in children aged 6–12 years: a systematic review. Front. Pediatr. 13:1449436. doi: 10.3389/fped.2025.1449436
Received: 20 June 2024; Accepted: 4 July 2025;
Published: 18 July 2025.
Edited by:
Andrea Cassidy-Bushrow, Henry Ford Health System, United StatesReviewed by:
Magdalena Żegleń, University School of Physical Education in Krakow, PolandFatma Sargin, Konya Education and Research Hospital, Türkiye
Copyright: © 2025 Muñoz-Urtubia, Vega-Muñoz, Salazar-Sepúlveda, García-Gordillo and Carmelo-Adsuar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alejandro Vega-Muñoz, YWxlamFuZG8udmVnYUB1Y2VudHJhbC5jbA==