 Sören Kliem1*
Sören Kliem1* Malte Sandner2,3
Malte Sandner2,3 Tilman Brand4Sebastian Fischer1
Tilman Brand4Sebastian Fischer1 Anna Lohmann1
Anna Lohmann1 Marie Lisanne Schepan4,5
Marie Lisanne Schepan4,5 Gabriella Conti6
Gabriella Conti6 Dirk Baier7,8*
Dirk Baier7,8*
- 1Department of Social Welfare, Ernst-Abbe-Hochschule Jena, Jena, Germany
- 2Department of Business Administration, Georg Simon Ohm University of Applied Sciences Nuremberg, Nuremberg, Germany
- 3Department of Education, Training, and Employment Over the Life Course, Institut für Arbeitsmarkt- und Berufsforschung, Nürnberg, Germany
- 4Department of Prevention and Evaluation, Leibniz Institute for Prevention Research and Epidemiology (LG), Bremen, Germany
- 5Department of Health Sciences, University of Bremen, Bremen, Germany
- 6Department of Economics, University College London, London, United Kingdom
- 7Institute of Delinquency and Crime Prevention, Zurich University of Applied Sciences, Zürich, Switzerland
- 8Faculty of Law, University of Zurich, Zürich, Switzerland
Background: The Nurse-Family Partnership (NFP) is an evidence-based home visiting program shown to improve maternal and child outcomes. Pro Kind is the first German adaptation of NFP, implemented between 2006 and 2012. While earlier evaluations demonstrated short- and medium-term benefits, no European trial has yet assessed long-term effects into adolescence.
Objectives: This study protocol outlines the third phase of the Pro Kind randomized controlled trial (RCT), designed to evaluate the program’s effectiveness 14–16 years post-intervention. Primary aims are to assess adolescent and maternal outcomes related to mental health, parenting, risk behaviors, and life satisfaction, as well as potential long-term economic effects.
Methods: The original RCT enrolled 755 pregnant women with psychosocial risk factors, randomly assigned to an intervention (n = 394) or control group (n = 361). The intervention comprised structured home visits from midwives or tandem teams (midwife + social worker) from pregnancy until the child’s second birthday. The 15-year follow-up combines self-report data (via online interviews and questionnaires) and administrative records on employment, social benefits, and criminal justice involvement. Discussion: This study represents the first long-term follow-up of an NFP adaptation in Europe. While U.S. trials of NFP provide evidence of the program’s effectiveness, these results cannot be generalized to European welfare contexts. This underscores the need for long-term evaluations of NFP adaptations in Europe to generate evidence that can inform policy and ensure evidence-based decision making.
Introduction
Sustained Nurse Home Visiting programs (SNHVs) are considered one of the most thoroughly evaluated preventive approaches in Western industrialized nations to support socioeconomically disadvantaged families and to reduce health and developmental inequalities among children (1). These programs involve long-term (up to three years) repeated and regular home visits by trained family visitors (usually registered nurses, midwives, or social workers). Home visits typically begin during pregnancy and are continued postnatally. The Nurse-Family Partnership program (NFP) (2), developed in the 1970s by David Olds, is regarded as a prototypical example of SNHVs. The theoretical framework of the program is based on self-efficacy theory (3), human ecology (4), and attachment theory (5). NFP aims to improve prenatal health, strengthen parenting skills, and promote maternal life-course development in terms of education and employment. It comprises up to 64 home visits from pregnancy (preferably < 29 weeks of gestation) until the child's second birthday, conducted by specially trained and certified registered nurses. Since its development in the 1970s, NFP has been evaluated in the United States in several large-scale randomized controlled trials (RCTs).
The first RCT was conducted in the late 1970s in Elmira, a small town in the rural Chemung County in the Southern Tier region of New York State, with an initial sample of N = 400 mothers (Elmira Trial, 1978–1980) (6). For the subsequent comparative analysis, the NFP intervention group (IG: n = 116, nurse home visits from pregnancy until age 2) was compared with a composite control group (CG: n = 184, developmental screenings and, in some cases, transportation for prenatal appointments). The study primarily targeted young, first-time mothers with low educational attainment and low income. The home visits focused particularly on improving prenatal health (e.g., reducing smoking and substance use, promoting healthy nutrition), strengthening parenting skills (especially responsive caregiving and safe home environments), and fostering maternal self-efficacy and future planning, (e.g., continuing education, entering employment, preventing unplanned subsequent pregnancies). On average, approximately nine prenatal home visits (range: 0–16) and about 23 postnatal home visits (range: 0–59) were conducted during the first two years after birth, with a frequency of weekly visits during the first four weeks postpartum, followed by biweekly visits until the 21st month, and thereafter monthly visits [see (7)]. For the Elmira Trial, follow-up studies are now available up to 17 years after completion of the intervention [19-year follow-up (19yrs-fu)] (7).
The second RCT was conducted in Memphis, Tennessee, in an urban setting with a high poverty rate (Memphis Trial, 1990–1991) (8). The target group consisted predominantly of African American, unmarried, first-time mothers with low educational attainment and limited employment opportunities. A total of N = 1.139 mothers were enrolled in the study. For subsequent comparative analyses, the NFP condition (n = 228) was compared with a control condition (n = 515) similar to that used in the Elmira Trial. The program structure followed the model tested in Elmira but incorporated a stronger focus on health promotion in contexts of urban poverty. On average, approximately seven prenatal home visits (range: 0–18) and about 26 postnatal home visits (range: 0–71) were conducted during the first two years after birth (8). In addition to improving prenatal health, particular emphasis was placed on preventing substance abuse and enhancing socioeconomic prospects through education and employment planning [see (8)]. Follow-up assessments extend to child age 18 years (9). Furthermore, data on maternal and child mortality are available for a 20-year follow-up (10).
In the third trial in Denver, Colorado (Denver Trial, 1994–1995) (11), NFP was examined in a multi-ethnic urban setting. The multi-ethnic sample (46% Mexican American, 35% white non-Hispanic, 15% African American, 4% other) comprised first-time mothers with multiple psychosocial risk factors (including low income, single-parent status, and low educational attainment). The intervention structure followed the standard NFP protocol, with home visits delivered either by registered nurses (n = 235) or by paraprofessionals (n = 245). Both groups were compared with a control condition comprising n = 255 mothers. On average, registered nurses conducted approximately seven (range: 0–17) prenatal home visits and about 21 (range: 0–71) postnatal home visits from birth until the child's second birthday. Paraprofessionals conducted about six (range: 0–21) prenatal and approximately 17 (range: 0–78) postnatal visits (12). For the Denver Trial, follow-up studies are available up to the 9 years after the initial trial [9-year follow-up (9yrs-fu)] (13). Overall, the three RCTs demonstrate diverse and, in some cases, long-term intervention effects across different developmental domains. At the prenatal level, findings include a reduction in nicotine consumption during pregnancy [Elmira (14), Denver (11)], increased birth weight for boys [Memphis (15)], lower incidence of hypertensive pregnancy disorders [Elmira + Memphis, pooled (16)], fewer preterm births among very young mothers [14–16 years, Elmira (17)], and improved breastfeeding behavior [Elmira + Memphis (16)]. With regard to child health and developmental domains, improvements were observed in maternal parenting behavior during childhood and adolescence [Elmira: 1–2yrs-fu (14), Memphis: 6yrs-fu (15)], reduced rates of domestic violence, child abuse, and neglect [Elmira: 4–15yrs-fu (18), Memphis: 2–3yrs-fu (15, 19), Denver: 4yrs-fu, (20)], as well as lower rates of injury-related hospital visits [Elmira: 2yrs-fu (21), Memphis: 6yrs-fu, (20)]. In medium terms, improvements were also observed in attention-related abilities [Denver: 2–6yrs-fu, (13)], cognitive abilities [Elmira: 3–4yrs-fu (14); Memphis: girls: 6yrs-fu, boys: 6–12yrs-fu (15, 22); Denver: 4yrs-fu, (20)] and language skills [Denver: 2–6yrs-fu (13, 20)] in children, as well as lower prevalence rates of emotional problems and behavioral difficulties [Memphis: 6yrs-fu (15, 22), Denver: 6–9yrs-fu (13)]. Long-term follow-ups into late adolescence provide evidence of sustained effects such as lower crime rates and convictions [Elmira: 11–19yrs-fu (7), Memphis: girls: 18yrs-fu, (9)], improved academic performance [Memphis: 12–18yrs-fu (9, 23)], lower rates of adolescent substance use [Elmira: 12–15yrs-fu (16, 24), Memphis: 12yrs-fu (23)], and fewer teenage pregnancies among girls [Elmira: 19yrs-fu (7)]. Analyses from the Memphis Trial also indicate a long-term effect (20yrs-fu) of lower child mortality among NFP children compared to the control group (10). Mothers likewise benefited from the intervention in the form of fewer closely spaced pregnancies (within 24 months) and fewer abortions within 48 months postpartum (All Trials 16). Overall, NFP mothers reported lower rates of subsequent births [Elmira: 15yrs-fu (18), Memphis: 9yrs-fu (25), Denver: 4yrs-fu (20)]. In addition, NFP mothers showed higher labor force participation and reduced dependence on welfare benefits [Elmira: 4–15yrs-fu (18, 26), Memphis: 12yrs-fu (27)] as well as improvements in mental health [Memphis: 2–6yrs-fu (15)]. Furthermore, there were fewer maternal arrests [Elmira: 4–15yrs-fu (18)], fewer impairments due to alcohol and drug use [Elmira: 4–15yrs-fu (18)], and a reduced maternal mortality rate [Memphis: 20yrs-fu (10)].
In addition to the three original U.S. NFP studies (Elmira, Memphis, Denver), a recent cluster-randomized controlled trial (CRCT) was conducted to examine the scalability and implementation of NFP within the U.S. Medicaid system in South Carolina [2016–2020, N = 5.670 Medicaid-eligible mothers (28)]. The target group comprised first-time mothers eligible for Medicaid who often face multiple stressors such as poverty, limited access to health services, and unstable living conditions. The program structure followed the NFP standard (home visits by nurses from pregnancy until the child's second birthday; prenatal: 9 visits median, 18 mean) but was more strongly integrated into public service structures and supplemented with components to improve birth outcomes (e.g., prevention of preterm birth) and to reduce hospitalizations. The focus was on preventive health, parenting competence, and life planning, with particular attention to feasibility in large-scale state welfare-programs. The results to date (follow-up assessments are planned up to child age nine years) showed no significant effects on the primary birth outcomes [e.g., preterm birth, low birth weight, small for gestational age, perinatal mortality (28), birth intervals (1yr-fu) (29); or child mortality, severe injuries, and indicators of child abuse and neglect (2yrs-fu) (30)].
In addition, two further U.S. RCTs have been conducted on the SNHV program Minding the Baby (MtB), with partially long follow-up assessments [phase 1: 3–5yrs-fu, 2002–2005, N = 105 mothers at risk of adversity (31, 32); phase 2: 8yrs-fu, 2008–2011, N = 124 mothers at risk of adversity (33, 34)]. MtB was developed at Yale University in the early 2000s and targets first-time mothers and mothers aged 14–25 years (32, 35). Home visits usually begin during pregnancy and continue until the child's second birthday. Unlike NFP, home visits are conducted in a tandem model by advanced practice nurses and clinical social workers. The program focuses on strengthening the attachment relationship, promoting parental sensitivity and reflective functioning, and supporting the child's healthy emotional and cognitive development. The U.S. MtB studies have shown that children were more likely to have secure attachment and less likely to have disorganized attachment (31, 33) and, in infancy, exhibited fewer interaction problems (among adolescent mothers, 32). Additionally, MtB families were more likely to be fully vaccinated, young mothers were less likely to have a subsequent child after their first birth, and there were fewer child protection reports (31). In later follow-ups (3–5yrs-fu), lower levels of externalizing behavior problems (32), lower obesity rates (35), fewer general behavior problems were found. In [8yrs-fu] more frequent supportive parenting practices were found (34).
In addition to these U.S. trials, various international and high-quality evaluations (i.e., RCTs) of SNHVs have been conducted in countries with universal healthcare systems. These include international adaptations of NFP from the Netherlands [VoorZorg, 2yrs-fu, 2007–2009, N = 460 young [<25 years], first-time mothers with low socioeconomic status [SES] plus at least one additional risk factor (36, 37)], England [Building Blocks [BB], 7yrs-fu, 2010–2013, N = 1.645 teenage [<20 years] mothers with low SES (38, 39)], Germany [ProKind, 7yrs-fu, 2006–2010, N = 755 first-time mothers with low SES plus at least one risk factor (40–42)], and Canada (British Columbia Healthy Connections Project [BCHCP], 2yrs-fu, 2013–2016, N = 739 first-time mothers with low SES (43)], as well as adaptations of MtB from the UK [2yrs-fu, N = 148 young [<25 years] mothers (44)], and Denmark [2yrs-fu, 2018–2022, N = 256 young [<25 years] mothers (45)]. Furthermore, two additional RCTs are available for the Australian right@home (AUS) program [6yrs-fu, 2013–2014, N = 722 mothers with at least two risk factors (46, 47)] and its precursor, the Maternal Early Childhood Sustained Home-visiting (MECSH) program [2yrs-fu, 2005–2008, N = 208 mothers with at least one risk factor (48)]. Similar to NFP, home visits in these programs are delivered by registered nurses and extend from pregnancy until the child's second birthday but include additional modules to promote language and literacy development [see (49, 50)].
While SNHV studies conducted in universal healthcare contexts have reported some positive effects regarding birth and pregnancy outcomes [smoking: VoorZorg (51)] as well as positive medium-term outcomes (0–4yrs) for mothers [e.g., parental responsiveness: ProKind (52), MECSH (53), right@home AUS (49); parental self-efficacy: MECSH (53), ProKind (54), right@home AUS (49); breastfeeding: BB (55), VoorZorg (51), MECSH (56); postpartum health: MECSH (56), right@home AUS (49); home learning environment: ProKind (57), right@home AUS (46), VoorZorg (37)], and children [e.g., cognitive and psychomotor development: BB (55), ProKind (57); language: BB (55), right@home AUS (49); behavioral difficulties and emotional problems: MtB UK (58), VoorZorg (37)].
To date only three of these studies have provided extensive long-term (>6 yrs) evaluations. First, the BB study in England (39) linked educational, health and social administrative data up to age seven and reported modest benefits in reading (key stage 1), but no consistent effects across other educational (writing, mathematics, scientific understanding), health (e.g., use of emergency departments due to injuries or ingestion) or child protection outcomes (e.g., reports to social services and official designations as “Child in Need”). Second, the 6yrs-fu of the Australian right@home program (59) reported improvements in children's socio emotional adjustment, social competence and executive functioning, alongside higher maternal wellbeing and warmer parenting, although no significant effects were found for children's general health, school achievement, emotional abuse or maternal distress, general health or self-efficacy. Compared to these studies, the German ProKind trial provides a comparable but slightly longer observation window. At the 7yrs-fu, the program was associated with significant reductions in internalizing and externalizing child behavior, higher maternal wellbeing, and decreases in abusive and neglectful parenting [see (41, 42)].
Building on this evidence, the present paper introduces the protocol for the long-term follow-up of ProKind (approx. 15yrs-fu). This study will be the first to examine whether the intervention effects of an SNHV program in a European welfare state persist into adolescence, thereby extending the existing international evidence beyond early and middle childhood and into a developmental stage marked by heightened social, emotional, and behavioral challenges (60).
The German adaption of NFP – the ProKind study
In Germany, the concept of early intervention (“Frühe Hilfen”) was introduced in the 1970s as part of healthcare and child welfare programs [Nationales Zentrum Frühe Hilfen (NZFH)]. Despite the development of numerous initiatives, there was a lack of comprehensive evaluation research (61). To address this gap, the Federal Ministry for Family Affairs, Senior Citizens, Women and Youth (BMFSFJ) launched the “Early Support and Social Early Warning Systems” program in 2006. These efforts led to increased attention and conceptual differentiation of early support measures in Germany, particularly regarding prevention and child protection. One such initiative is the ProKind study, a multicenter RCT adapting the NFP program for Germany (40). The intervention within the ProKind study was conducted between 2006 and 2012 in the German federal states of Bremen (a city-state in northern Germany known for its urban environment and relatively high levels of social disparities), Lower Saxony (a largely rural state with pockets of urbanization and a diverse socio-economic landscape), and Saxony (an eastern state characterized by its post-reunification socio-economic challenges and unique demographic structure).
Sample at baseline and randomizations procedure
At the time of baseline data collection (2008–2009), women in the 12th to a maximum of the 28th gestational week were recruited based on the following inclusion criteria: (a) an ongoing pregnancy (<28 weeks), (b) at least one financial risk factor [e.g., receipt of unemployment benefits (ALG II), debt], (c) at least one additional social or personal stress factor (e.g., being underage, lack of a school diploma, personal experiences of abuse or neglect) and (d) at least basic knowledge of the German language to enable communication with the German-speaking family companions (≙ A1–A2 language level). Participants were recruited through various intermediaries, including gynecologists, midwives, youth welfare offices, psychosocial counseling centers, and employment agencies. In total, N = 1.157 interested pregnant women registered to participate in the project. Of these, n = 263 did not meet the inclusion criteria, and n = 139 declined participation after receiving detailed information about the project. The final sample of N = 755 women was randomly assigned to an intervention group (IG, n = 394) or a control group (CG, n = 361) using Efron's Biased Coin Design (62), stratified by municipality (urban vs. rural), age (≤18 vs. >18 years), and maternal nationality (German vs. non-German). The women were, on average, 21 years old at the start of the project; approximately 88% were unmarried (about 28% were single parents), and about 12% had a migration background. Only about 18% reported that the current pregnancy was unwanted. The CG did not receive any study-related interventions but had access to the regular services of the German healthcare system (treatment as usual, TAU). This includes the statutory right to midwifery care during pregnancy, childbirth, and the postpartum period, as enshrined in the German Midwifery Act (HebG) and the Midwifery Training and Examination Regulation (HebAPrV).
Adaptation
Although the adaptation of the NFP program closely adhered to its original guidelines and curriculum, several key differences were implemented in the German version. A significant change was made regarding the professional background of the family companions. While the U.S. NFP program employs family nurses (specially trained pediatric nurses), the ProKind study utilized state-certified and NFP-trained midwives as family companions. This change was based on the strong integration of midwives in Germany's primary healthcare system. In Germany, midwifery is a highly respected profession providing care and support to individuals during pregnancy, childbirth, and the postpartum period. The legal foundations are regulated through the Midwifery Act (HebG) and the Midwifery Training and Examination Regulation (HebAPrV), which define the requirements for professional practice, including a state-recognized three-year training program with theoretical and practical components, a state examination, regular continuing education, and comprehensive documentation duties. Additionally, midwives must document all treatments and maintain these records for at least ten years. Furthermore, German law guarantees every woman statutory midwifery care during pregnancy, delivery, and the first twelve weeks postpartum. This statutory assistance, however, focuses exclusively on health-related aspects, is limited in duration, and does not follow a structured curriculum. All family companions in the ProKind study were required to have extensive experience working with families experiencing adversities and to demonstrate a respectful and sensitive approach to the mothers. Consistent with the NFP model, only female family companions were employed to foster trust and rapport with the participants.
Additionally, the ProKind study evaluated two different delivery models for home visits. In the first model, visits were conducted exclusively by midwives, referred to here as the Continuous Model (CM), which closely aligns with the original NFP program. In the second model, referred to as the Tandem Model (TM), the intervention was carried out by a team consisting of a midwife and a state-certified social worker (equivalent to a bachelor's degree in social work). In this model, the midwife conducted visits during pregnancy, while the social worker took over approximately two months after the birth. The conceptual rationale for the TM was twofold: (a) In Germany, prenatal and perinatal care provided by midwives is generally covered by statutory health insurance, while early childhood social support for disadvantaged families is funded through social legislation. The TM sought to align with these financing structures, and (b) the TM aimed to leverage the distinct competencies of midwives and social workers. Midwives contributed medical expertise in areas such as childbirth, infant nutrition, and early child development, while social workers provided case management skills and experience in addressing child abuse and neglect within institutional frameworks.
However, current empirical evidence indicates that the quality of the relationship between practitioner and family is a key driver of effectiveness in preventive home-visiting programs (63, 64). A central strength of the original NFP model lies in the therapeutic relationship between the nurse and the first-time mother, which is deliberately fostered through continuity, trust, and long-term engagement (9, 65). Since the TM involves a handover from midwife to social worker shortly after birth, it may potentially entail the risk of interrupting this continuity of care at a particularly sensitive developmental stage. Such a transition could make it more difficult for families to establish and maintain a stable working alliance, which is regarded as a central mechanism of program effectiveness. Continuous support by a single professional, as implemented in the CM, may therefore be more conducive to sustaining trust and engagement. Taken together, these considerations suggest that the TM could potentially entail certain structural disadvantages compared to a faithful adaptation of the original NFP design that emphasizes relational continuity as a core element of its effectiveness.
Intervention
After enrollment in the project, participants were usually visited at home every two weeks, either exclusively by specially trained family midwives (CM) or sequentially by a tandem team of family midwives and social workers (TM). Exceptions included a weekly visit schedule in the first month of the intervention and during the 8th–12th weeks of the child's life, as well as a monthly visit schedule in the last three months of the intervention before the child's second birthday. Each home visit followed a structured procedure. In accordance with the NFP program six focus areas (domains) are addressed while working with the participants in the intervention setting. These domains are generally regarded as the most important risk and protective factors for the prevention of negative pregnancy outcomes, child abuse or neglect, developmental delay and limited economic independence. The topics of each visit were divided into six domains:
1. Maternal Health: This area was the focus during pregnancy and covered topics such as managing physical changes, birth preparation, healthy nutrition, physical activity, sleep, oral hygiene, and the consumption of nicotine, alcohol, and substances.
2. A Healthy Environment: This involved an assessment of the home environment, the implementation of safety measures to prevent accidents, securing household items, and addressing issues such as mold and secondhand smoke.
3. Personal Future Plans: The focus was on future planning (including returning to education or work, and further family planning), as well as organizing daily life and identifying personal strengths and weaknesses.
4. Maternal/Parental Role: This area took up most of the time during home visits from the birth of the child until the child's second birthday. It covered topics such as infant care, nutrition, development, parenting, and promoting positive parent-child interactions.
5. Social Networks: This addressed social support from partners, parents, and friends, the maintenance of family and friendship relationships, conflict resolution, and non-violent communication.
6. Use of Social and Health Services: Information was provided about services important for addressing immediate needs and building support networks, including prenatal check-ups, child health examinations, mother-child groups, and official appointments.
A total of K = 62 home visitors delivered the intervention, consisting of k = 37 midwives, k = 24 social workers, and one pediatric nurse. The average age of the home visitors was 40 years (SD = 7.8) at the start of the intervention. All home visitors were female and held German nationality. Each home visitor underwent approximately 16 days of in-service training, following the NFP curriculum. The NFP guidelines were translated into German, supplemented with culturally and contextually appropriate materials, and delivered by the German supervisory team. Training sessions covered program theories and their practical applications, including guidelines and specific intervention modules. While there were some profession-specific training modules (e.g., client-centered communication for midwives, feeding practices in early childhood for social workers), the curriculum was generally consistent across both staffing models. Moreover, home visitors received about one hour of clinical supervision weekly. All supervisors (N = 6, each with a degree in social work or psychology and additional coaching qualifications) completed a five-day training on the core principles of the program at the NFP National Office in the United States. Overall, the families received an average of 32.7 visits (SD = 18.6), with a range of 0–94 visits, which is slightly comparable with U.S. NFP trials ranging from approx. 28 visits (Denver) to approx. 33 visits (Memphis) [see (66)]. Furthermore Sandner (66) demonstrates that the typical distribution of visit content across pregnancy, infancy, and toddlerhood in ProKind closely matched NFP averages and recommendations, particularly in core areas such as maternal health, maternal and parental role, and life course development. Across all families, approx. 13.000 home visits were conducted within the Pro Kind project. The average length of a home visit was 82 min (SD = 12.4). Families in the CM received on average 32.4 visits (SD = 18.1), while those in the TM received 33.0 visits (SD = 19.4), with no statistically significant difference between the two groups. The average duration of the visits was 82.6 min (SD = 12.4) in the CM and 79.6 min (SD = 14.3) in the TM.
Program participation
As in the original NFP program, participation in Pro Kind was voluntary. Consequently, not all mothers in the experimental group remained in the program until their child's second birthday, and therefore, not all program content could be delivered as intended. A total of n = 166 out of the n = 394 randomized mothers in the experimental group (42.2%) dropped out of the intervention prematurely. The reasons for termination can be divided into endogenous and exogenous causes: Endogenous termination causes are those deliberately or indirectly caused by the mother, such as an explicit request to terminate the program or loss of contact. Exogenous termination causes are those resulting from external circumstances, such as the child being taken into custody by the youth welfare office, the sudden death of the child, or the mother relocating to an area where further home visits could not be provided. During the first intervention phase (before the birth of the child), n = 52 mothers terminated the program prematurely, of which n = 38 (73.1%) were endogenous terminations. During the second intervention phase (after birth up to the child's first birthday), an additional n = 87 mothers dropped out, with n = 48 (55.2%) being endogenous terminations. During the last intervention phase (from the child's first to second birthday), only n = 27 more mothers did not complete the program as intended, with n = 17 (63.0%) due to endogenous termination causes. Comparing program participation between the two staffing models revealed that program participation at the end of the implementation was higher in the TM compared to the CM [TM: 47% vs. CM: 38%, p = .06 (67)]. Overall, the rate of 42.2% is comparable to the results in the latest US trial of the NFP reporting 44% program discontinuation [see (11)].
Results of completed follow-up phases
ProKind has been evaluated in two follow-up phases: The first project phase (Phase 1) spanned from the 36th gestational week (GW) to the age of 36 months of the reference children (54) and was funded by the German Federal Ministry for Family Affairs, Senior Citizens, Woman and Youth [BMFSJ, funding code: IIA6-25080820V6], the Günter-Reimann-Dubbers Foundation [no funding code available], the Dürr Foundation [no funding code available], and the TUI Foundation [no funding code available]. The second project phase (7yrs-fu, phase 2) was conducted at the time of school entry (ages 6–10) of the reference children (40, 41) and was funded by the German Federal Ministry of Education and Research (BMBF funding code: 01EL1408; now: BMFTR).
The number of completed interviews at each follow-up assessment is summarized in Figure 1 by study arm (IG vs. CG) and intervention model (CM vs. TM). In the IG (n = 394), n = 276 interviews (70.0%) were completed at 36 weeks of gestation, n = 265 (67.3%) at child age six months, n = 227 (57.6%) at 12 months, and n = 178 (45.2%) at 24 months. In the CG (n = 361), n = 247 interviews (68.4%) were completed at 36 weeks of gestation, n = 240 (66.5%) at six months, n = 205 (56.8%) at 12 months, and n = 168 (46.5%) at 24 months. At the 7yrs-fu, n = 274 interviews (70.0%) were completed in the IG and n = 258 (71.5%) in the CG.
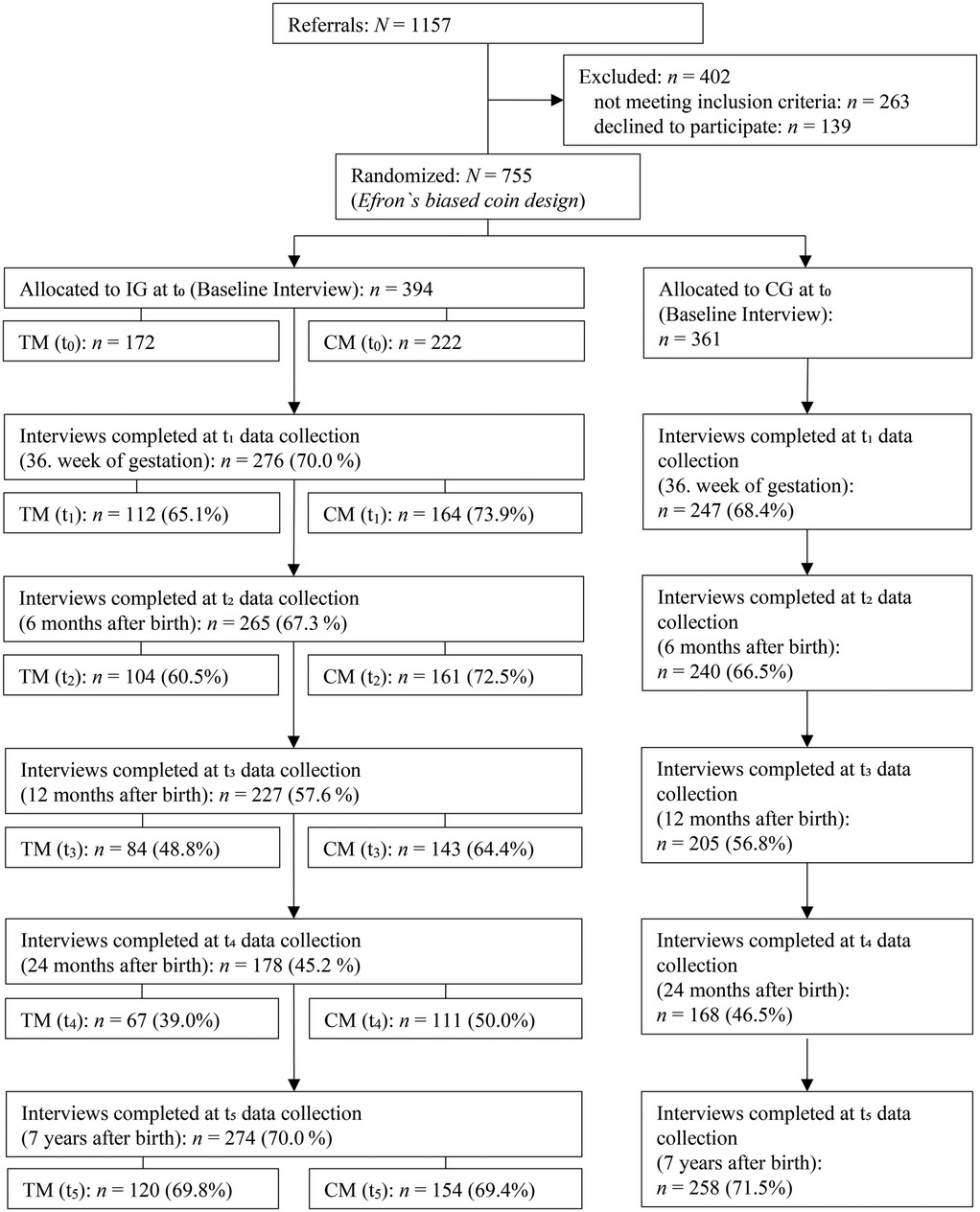
Figure 1. Flowchart of response rates broken down by IG and CG, with subdivision of IG into CM and TM (t0–t5). IG, intervention group; CG, control group; TM, tandem model; CM, continuous model.
In the CM, n = 161 interviews (72.5%) were completed at six months, n = 143 (64.4%) at 12 months, n = 111 (50.0%) at 24 months, and n = 154 (69.4%) at the 7yrs-fu. In the TM, n = 104 interviews (60.5%) were completed at six months, 84 (48.8%) at 12 months, n = 67 (39.0%) at 24 months, and n = 120 (69.8%) at the 7yrs-fu. These figures refer solely to completed interviews and do not reflect program participation.
Sandner and Jungmann (57), based on the BSID-II, found lower rates of cognitive developmental delay among girls in the intervention group compared to the control group, even after adjustment for relevant risk factors. This advantage was evident in the first year of life and persisted in attenuated form into the second year, whereas no differences were observed for boys. A dimensional analysis of the BSID-II further indicated consistently small, though not consistently significant, effects for girls. Sierau et al. (54), and Sandner et al. (68) identified small but statistically significant differences in favor of the intervention group with respect to parental self-efficacy, perceived social support, and reduced stress. No effects were observed for parenting behavior, attachment, empathy, locus of control, life satisfaction, children's socio-emotional development, or health-related behaviors. Conti et al. (52), using micro-analytical observations, demonstrated context-dependent improvements in mother–child interactions for mothers and daughters. By contrast, no positive effects, and in some cases even negative effects, were found for boys and their mothers.
Administrative data analyses likewise indicated selective advantages. Sandner et al. (68) reported lower prescription rates of certain medications and higher utilization of dental preventive care during pregnancy, while no consistent differences emerged with regard to children's medical service use. Herrmann et al. (69), in a subsample, found more favorable maternal dental health values in the intervention group. Finally, Sandner (66) documented higher fertility rates and more favorable pregnancy outcomes among mothers in the intervention group.
Kliem and Sandner (41), in the context of the 7yrs-fu of the German Pro Kind program and based on the preregistered primary outcome domains [see (40)], demonstrated that the intervention produced significant improvements across several key outcome areas. Children in the IG showed lower rates of internalizing, externalizing, and overall behavioral problems compared to the CG, with effects being particularly pronounced among boys. Mothers in the IG also reported higher life satisfaction and reduced psychological distress. In terms of parenting practices, there was a significant reduction in abusive behavior (with boys additionally experiencing fewer instances of neglect) as well as less dysfunctional parenting behavior.
In a differentiated analysis, the effectiveness of the two implementation models of the ProKind program was examined independently. Schepan et al. (42) demonstrated that the CM proved superior in several outcome domains. It showed greater improvements in maternal mental health, maternal life satisfaction, and reductions in both dysfunctional and abusive parenting practices. In addition, the CM displayed tendencies toward advantages in reducing externalizing behavioral problems in children. By contrast, the TM was only effective in reducing children's internalizing behavioral problems. No effects were found for children's academic performance or life satisfaction. Additional analyses by Conti, Kliem & Sandner (70) indicated that only the CM was associated with a significant reduction in the 12-month prevalence of affective disorders (ICD F30–F39) among mothers and hyperkinetic disorders (ICD F90–F98) among children. Moreover, the CM was linked to lower rates of severe accidents requiring hospitalization as well as a tendency toward fewer foster care placements (71).
The third phase of the ProKind research
This study protocol focuses on the third ProKind program phase funded by the BMBF (funding code: 01EL2013). Up to date no SNHV study conducted within a universal healthcare system has examined the long-term follow-ups of the U.S. NFP-studies (with observation periods of to 20 years). The primary goal of this research project is therefor to evaluate the long-term effectiveness of the ProKind program for adolescents aged approx. 14–17 years and their mothers (15yrs-fu; third project phase). This time point appears particularly important, as adolescence represents a critical transitional phase in which cognitive, academic, and socio-emotional competencies are consolidated that are highly relevant for the subsequent life course. During this developmental period, profound biological maturation processes (e.g., hormonal and neurobiological changes during puberty) overlap with significant cognitive and psychosocial developments, such as changes in emotion and self-regulation, self-concept, and the structure and meaning of peer relationships (60, 72). Adolescence is also considered a particularly sensitive period for the first onset of mental disorders from a developmental psychopathology perspective (73). In addition, this life stage is characterized by a marked increase in risky behaviors (e.g., substance use, sexual risk-taking) and engagement in illegal activities (74–76). These patterns are closely linked to the biological and psychosocial developmental processes of adolescence, such as heightened sensitivity to reward stimuli and increased sensation seeking, combined with still immature cognitive control capacities, as the development of the prefrontal cortex lags behind that of subcortical reward systems (77, 78). These changes interact with pre-existing risk factors from childhood, including adverse attachment experiences [e.g., (79)] and cumulative burdens of early adverse childhood experiences [ACEs; (80, 81)]. Numerous longitudinal studies have shown that ACEs (such as abuse, neglect, parental mental illness, substance-related problems, or domestic violence) are associated in a dose–response manner with an increased long-term risk of mental disorders, chronic somatic diseases, reduced social participation, and elevated mortality (82, 83). Longitudinal studies such as the Dunedin birth cohort also demonstrate that early self-control and self-regulation are linked in a dose–response relationship with later academic achievement, physical and mental health, and reduced criminality in adulthood (84). From a developmental psychology perspective, it can therefore be assumed that the early strengthening of key protective factors in early childhood (such as secure attachment, emotional and cognitive self-regulation skills, parental competence, the absence of experiences of violence, and family stability) not only reduces the likelihood of socio-emotional disorders during adolescence but also lowers the risk of problematic behaviors such as substance use, school dropout, or delinquent behavior. Long-term follow-ups of the U.S. NFP over periods of 15–20 years support this assumption, demonstrating sustained positive effects on educational attainment, psychosocial adjustment, and reduced delinquency rates (9, 85). With regard to the ProKind study, the results of the 7yrs-fu (lower rates of internalizing and externalizing behavioral problems, higher maternal life satisfaction and reduced psychological distress, reductions in abusive and neglectful parenting practices) (41, 42, 70) can, in context of existing longitudinal evidence, be interpreted as indicative of potential long-term effects. Longitudinal studies have shown that early externalizing disorders are associated with later delinquency, substance abuse, and school dropout (86–88), whereas emotional neglect and maltreatment markedly increase the risk of depression, anxiety disorders, and relationship difficulties in adolescence and adulthood (89, 90).
The follow-up study can be divided into six domains: (a) interviewer training, (b) collection of contact information, (c) data collection, (d) acquisition of administrative data, and (e) data analysis. The participating institutions are involved in these domains as follows: Ernst-Abbe-Hochschule – University of Applied Sciences (EAH): (a), (b), (c), (e); Institute for Employment Research in Nuremberg (IAB) of the Federal Employment Agency: (d), (e); Leibniz Institute for Prevention Research and Epidemiology (BIPS): (e). In accordance with SPIRIT guidelines (91) an overview of the ProKind follow-up schedule can be found in Figure 2. Starting in March 2020, the Covid pandemic and related containment measures caused significant disruptions to the project's feasibility and led to a substantial delay in the planned timeline. First, during the acute phase of the pandemic, data collection could not be carried out as originally planned in participants' homes, as had been done in previous phases of the project (40). This was due to the unmanageable effort required to submit hygiene protocols to local health authorities and the unacceptable health risks for all parties involved, even with a hygiene protocol in place. Second, there was a risk of treatment effect contamination, as the acute pandemic situation and the varying Covid-19 containment measures were expected to impact the variables under investigation, including life satisfaction, experience of violence, and psychological abnormalities in children (92).
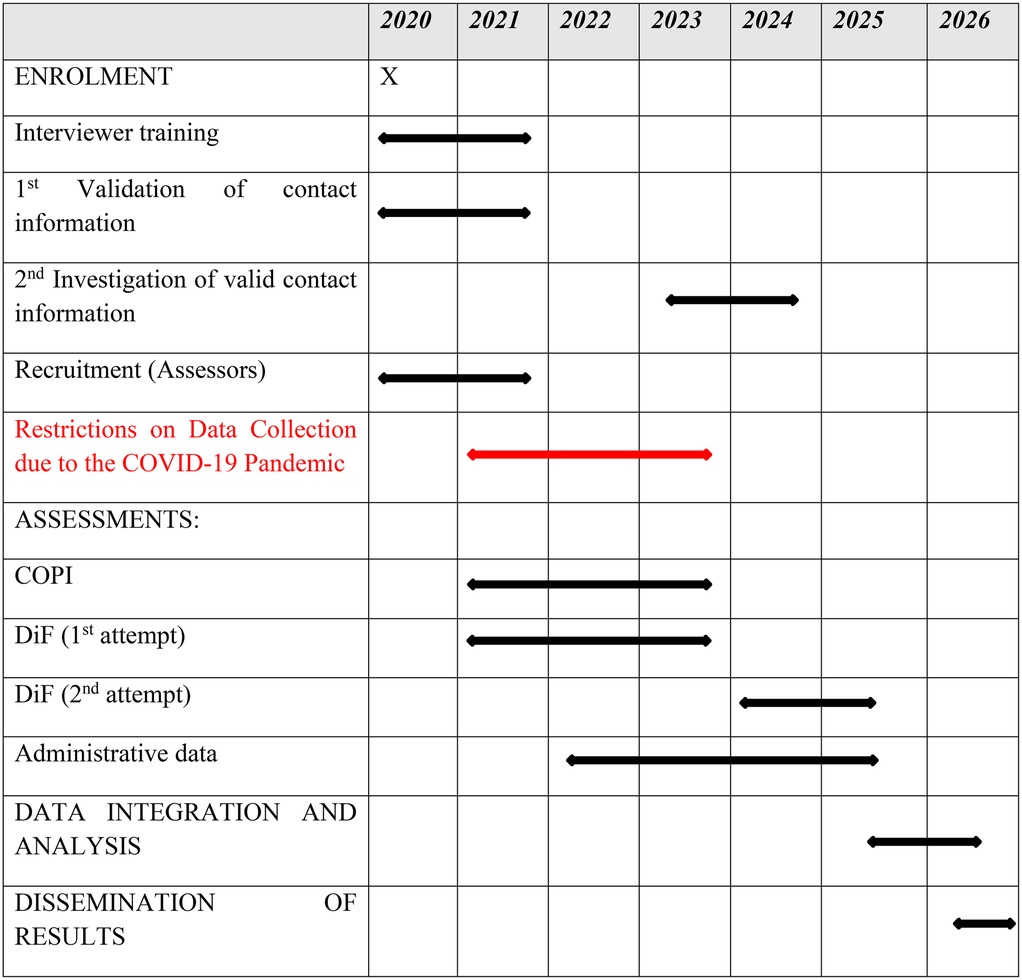
Figure 2. SPIRIT template of the schedule of enrolment, interventions, and assessments.
The exclusion of such contamination effects was deemed essential for the meaningful calculation of treatment effects and for the successful completion of the overall project. For these reasons, it was decided, in consultation with the project sponsors, to pause the start of data collection until the risk of treatment effect distortion could be considered minimal. In addition to this necessary adjustment to external circumstances, changes were also made to the mode of assessment. To avoid being permanently dependent on the unpredictable course of the pandemic, the project consortium decided to forgo home visits and instead implement digital data collection. Accordingly, online personal interviews (COPI) were conducted by trained test administrators who were blinded to the treatment condition, and digital questionnaires (DiF) were used for data collection. This required converting all test materials into an online-administrable format, which involved additional labor-intensive steps, such as establishing a technical and digital infrastructure, creating sample videos for the target group to illustrate the new survey format, and conducting pre-tests. This adaptation necessitated a reduction in the originally planned scope of administration, resulting in the inability to administer some originally intended outcome domains. As a result, the research project experienced a significant delay and underwent several changes to the original pre-registration plan (DRKS). The study documentation is available in the German Clinical Trials Register (DRKS; ID: DRKS00025962, registration date: 08 November 2021; Last update in DRKS: 09 July 2024). The DRKS has been recognized as a WHO Primary Registry since October 2008. The protocol is reported according to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT; Supplementary Table S1).
Procedure and re-engagement strategy
As part of the adjusted procedure, all project staff underwent extensive training at the beginning. The training content included not only the manual-compliant administration of the psychological testing procedures used but also handling challenging interview situations (e.g., with aggressive or traumatized participants). Comprehensive quality assurance measures are being implemented, including checks on the quality of the COPI after the first and second interviews, as well as, starting from the second interview, in a rhythm of ten interviews (10% supervision rate). Detailed feedback is provided to the interviewers during these reviews.
Participants were identified through a data linkage with the German municipal registration offices (Einwohnermeldeamt, EMA), which yielded updated address information for n = 703 families. This linkage provided the most recent address information, thereby enabling reliable contact with participants for the purposes of the follow-up study. A project assistant first initiates personal contact by sending a letter inviting participants to update their telephone number. Upon receiving this information, the assistant contacted the participant by phone to schedule appointments for the COPI interviews (mother and children) and to provide the corresponding link for the DiF questionnaire. Participation in the COPI and the DiF is voluntary. Participants face no disadvantages if they choose not to participate. Withdrawal from the study is possible at any time, either verbally or written. If a participant withdraws consent, all identifying data are deleted and the remaining data are processed anonymously. To date, this has occurred in n = 17 cases, corresponding to approximately 2.3% of the total sample (N = 755). All participants will be informed in an appropriate and simple language about the study results. Each participant (mothers and children) receives €50 as compensation for their time invested in the COPI and DiF. The Ethics Committee of University Hospital of Jena (Registration No.: 2021-2372-Bef) approved the study design and procedure. Additionally, administrative data from various sources is utilized.
Consistent with the second phase of the ProKind study, information is collected regarding prior employment, periods of unemployment, welfare receipt, participation in qualification programs during unemployment, and employment details from the Technical Data Center (FDZ) of the IAB in Nuremberg, which is part of the German Federal Employment Agency. Participants had the option to provide self-reported data but withhold permission for researchers to access administrative data. Furthermore, the data linkage with the EMA allows access to official records on mortality of both children and mothers as well as on further births of the participating mothers and their children. Regular inquiries are made to the Federal Central Criminal Register (Bundeszentralregister, BZR). This register records criminal convictions by German courts, certain decisions by administrative authorities, notes on incapacity to be held criminally responsible, and special judicial determinations, as well as subsequent decisions and facts related to these entries. When the relevant conditions are met, foreign convictions of German nationals or individuals born or residing in Germany are also entered into the register. An anonymized report for scientific research purposes is unrestrictedly possible.
Power analyses indicated that with a one-sided test at α = .05 and statistical power of 1–β = .80, the trial is adequately powered to detect small effects. Calculations were based on the original allocation proportions of the study (n = 394 in the IG and n = 361 in the CG). Three scenarios were considered. Scenario 1 assumes administrative data with an expected re-engagement of 93% (n ≈ 700) which allows the detection of effects of at least ES = 0.19. Scenario 2 assumes a response rate of about 70% (n ≈ 530) as observed in the 7yrs-fu (41) which allows the detection of effects of at least ES = 0.22. Scenario 3 assumes a more conservative retention rate of 60% (n ≈ 450) which allows the detection of effects of at least ES = 0.23. According to Cohen (93), these values correspond to small effect sizes.
Research aims and objectives
The overarching aim of the ProKind long-term follow-up study is to examine whether the medium-term program effects observed in earlier phases can be sustained or re-emerge during adolescence. The trial is designed to evaluate whether early home-visiting support contributes to improved trajectories of mental health, parenting, and overall family well-being into late adolescence. In line with the theoretical model of NFP and international evidence from RCTs of intensive home-visiting programs, three primary outcomes were defined.
First, child mental health will be assessed through standardized instruments [Child Behavior Checklist, CBCL 6/18 (94); Revised Youth Self-Report 11-18, YSR/11-18R (95)], as the prevention of emotional and behavioral disorders represents the central long-term goal of the program (10, 13, 22). Furthermore, through the repeated use of the CBCL/YSR, developmental trajectories can be consistently captured and distortions caused by switching instruments can be avoided. The procedure also provides both maternal and child reports, which allows perspectives from different informants to be incorporated in a consistent manner across developmental stages.
Second, maternal mental health will be assessed through the short form of the Depression-Anxiety-Stress Scale (DASS-21) (96) as maternal psychological well-being is a crucial determinant of parenting behavior, child outcomes, and the effectiveness of family-focused prevention programs.
Third, child maltreatment will be examined using the Conflict Tactics Scales – Parent Child (CTS-PC) (97) and the Multidimensional Neglectful Behavior Scale (MNBS) (98), given that prevention of abuse and neglect is a key target of early intervention programs and strongly associated with later adverse developmental trajectories. Third, these three main outcomes are not only theoretically central but also directly comparable with other RCTs of nurse home-visiting programs, which consistently demonstrated sustained effects in these domains [e.g., (9, 27)].
Table 1 summarizes the outcome hypotheses along with their respective operationalizations, associated informants, and survey methods. The selection of instruments and scales was guided by criteria of high psychometric quality, validity, and appropriateness. All instruments employed are particularly suited to measuring family health, living conditions, and child development. Following a multi-informant approach, various tools were used to incorporate the perspectives of both the child and the mother. A key consideration is whether the underlying research questions are (a) based on a direct outcome hypothesis of the “Pro Kind” program (primary outcome), (b) based on an outcome hypothesis but considered less likely (secondary outcome), or (c) pertain to a construct measured for further research purposes but not regarded as a primary target criterion of the intervention. Due to the volume of data collected, only the primary and secondary outcome domains are presented.
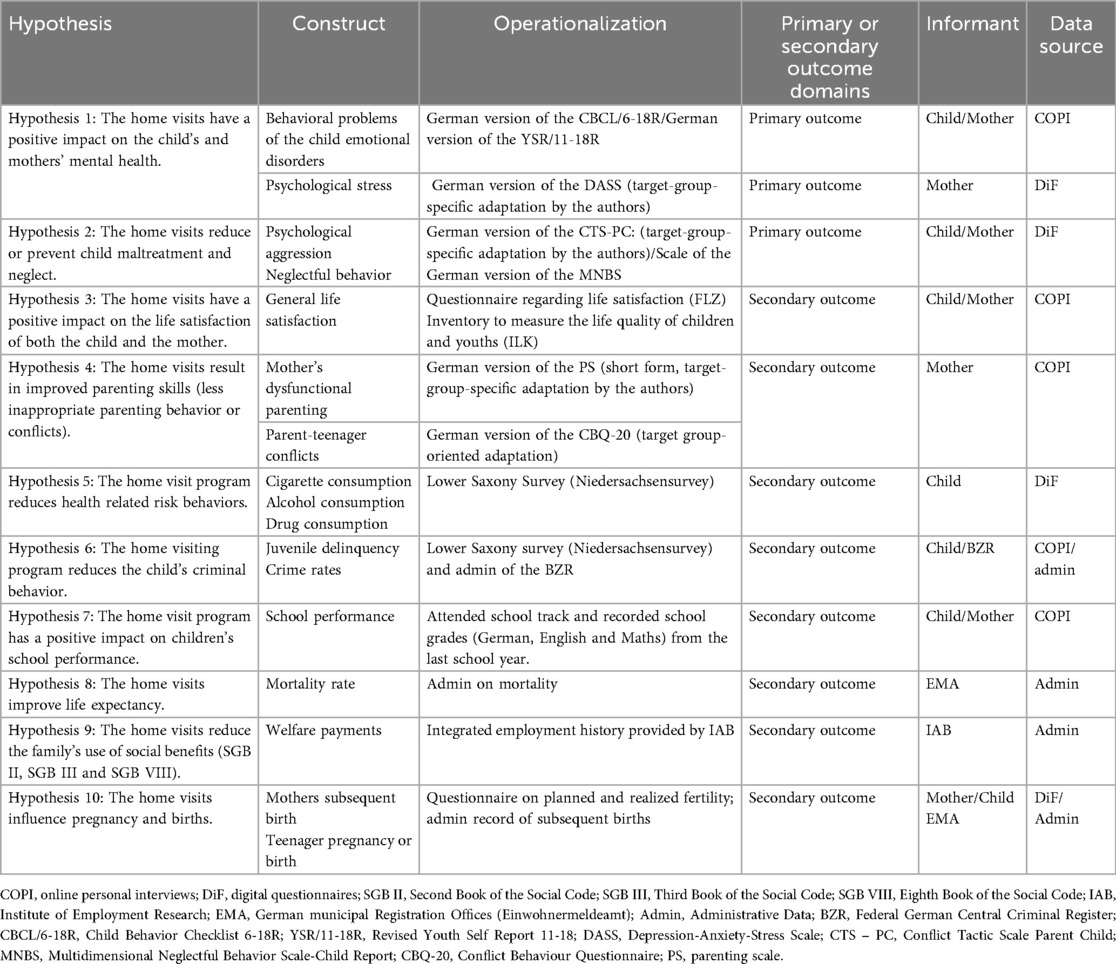
Table 1. Approach to evaluate the long-term effectiveness of the ProKind project.
Measuring instruments
Primary outcomes
Mental health of children
The CBCL 6/18 assesses behavioral problems, emotional problems, somatic complaints, and social competencies of school-aged children and adolescents from the parents' perspective (94, 95). The eight problem scales can be aggregated into internalizing and externalizing disorder scales and a total score. The German manual reports adequate internal consistencies for the total problem score and the internalizing and externalizing scales, with Cronbach's α > .80.
The YSR/11-18R, derived from the CBCL/6-18, captures competencies and problems of adolescents aged 11–18 years, similar to the CBCL/6-18, but uses a self-report measure (94). The translated version from Döpfner and colleagues was used (95). The internal consistency of the total problem score is very high (Cronbach's α ≥ .93), while the internalizing and externalizing behavior scales demonstrate good reliability (Cronbach's α > .80).
Maternal distress
The short form of the DASS-21, adapted via forward-backward translation, is used to assess negative emotional states based on their frequency over the past four weeks (1 = “never” to 4 = “very often”) (96). The DASS-21 includes three dimensions: depression (e.g., dysphoria and hopelessness), anxiety (e.g., autonomic arousal and situational fear), and stress (e.g., chronic, nonspecific arousal and irritability).
Child maltreatment and neglect
The CTS-PC, adapted via forward-backward translation, is the parent-child version of the CTS and measures psychological and physical maltreatment, neglect, and non-violent discipline of children by parents (99). In the present studies, 31 items were used in the mothers' interviews and 16 items in the children's interviews. The CTS-PC captures the subscales Non-Violent Discipline, Psychological Aggression, Physical Assault, and Neglect.
The MNBS, whose German version was developed as part of the LIFE study at the University of Leipzig, is an instrument for assessing various forms of parental behavior related to child neglect (98). Different versions of the MNBS exist, all of which measure the extent to which the following needs of the child have been neglected: physical needs (e.g., food and clothing), emotional needs (e.g., affection and support), supervisory needs (e.g., addressing misbehavior and knowing the child's whereabouts), and cognitive needs (e.g., reading or helping with homework). The MNBS is available as a self-report measure for parents of children aged 0–15 years (Form P/PS). In the present study, eight items were presented to both mothers and children.
Secondary outcomes
Dysfunctional parenting behavior
The short form of the Parenting Scale (PS) is a measure designed to assess dysfunctional parental disciplinary practices (100, 101). Based on a child behavior scenario, parents are asked to rate their own behavior between a functional and a dysfunctional approach. Two subscales—overreactivity (mothers: α = 0.77) and laxness (mothers: α = 0.73)—as well as a total score (mothers: α = 0.79) can be calculated.
Children's life satisfaction
The Inventory for Assessing the Quality of Life in Children and Adolescents (ILK) is a tool for measuring the quality of life in children and adolescents (102). The quality of life is divided into different domains, which are separately assessed in the ILK: school, family, peer relationships, and interests and leisure activities. Additionally, two health-related domains—physical health and mental health—are included. Beyond the individual domains, an overall assessment of quality of life is also provided. The internal consistencies of the quality-of-life score, based on child and adolescent self-reports, range between Cronbach's α = .55 and .63.
Mothers' life satisfaction
The Short Form of the Questionnaire for Life Satisfaction (FLZ) is designed to measure relevant aspects of life satisfaction in mothers across various life domains, such as health, financial situation, leisure time, relationship with their own children, or housing (103). In addition to assessing domain-specific life satisfaction, the FLZ allows for the estimation of general life satisfaction, calculated as the sum of seven out of the ten scales. The internal consistency for the total score is satisfactory (Cronbach's α = .74 for mothers). The FLZ has been normed on a representative German sample, with additional norms available for various age and occupational groups.
Child's consumption of alcohol, cigarettes, and Cannabis
The frequency of alcohol, cigarette, and cannabis consumption is assessed using questions from the Lower Saxony Survey 2019 (104).
Parent-teenager conflicts
The Conflict Behavior Questionnaire (CBQ-20; adapted via forward-backward translation) is a 20-item self-report instrument designed to assess perceived conflict and communication behavior between parents and children from the mothers' perspective (CBQ-E version). The items refer to the past two weeks and are answered with “true” (agreement) or “false” (disagreement). The results of the CBQ-20 correlate at .96 with the longer version of the CBQ, which contains 73 items (105) and has demonstrated high internal consistency (106).
Academic performance of children
Data referring to current school type, grade repetition, educational aspirations, current grades in German, English, and Mathematics is collected.
Child's criminal behavior
Criminal and violent behavior are assessed using questions from the Lower Saxony Survey 2019 (104). Criminal behavior is measured with 9 items. Example items include: “Have you ever deliberately stolen something from a shop, department store, or store?” Violent behavior is assessed with 6 items. Example items include: “Have you ever demanded money or possessions (e.g., a jacket, watch, shoes) from someone and seriously threatened violence if they did not hand them over or pay?” In addition, data from the BZR for the ProKind children's/adolescents' cohort will be gathered. These data include information on criminal convictions and relevant judicial decisions.
Mortality rate
Data from the EMA will be obtained to assess mortality rates.
Social benefit receipt
The IAB provides comprehensive data on integrated employment biographies as well as data from the SGB II performance statistics, accessed via the IAB's sampling frame (LST-S).
Subsequent pregnancy and desire for children
In line with previous surveys in the ProKind project and as a continuation, mothers are asked about their current family life and future family planning. This includes questions regarding contraception methods or an (already realized) additional desire for children. Administrative data further allow the tracking of how many subsequent children the mothers have had. In addition, adolescents from the ProKind cohort are asked about experiences with pregnancies and births. Administrative data further allows the identification of whether adolescents of the child cohort have already become parents.
Data analysis
The primary and secondary analyses will be conducted on an intention-to-treat basis. We will standardize and recode all continuous outcomes such that positive values correspond to beneficial effects. The reported effect sizes (ESs) will be interpreted as group differences in standard deviations (SDs) of the CG. Confidence intervals (CIs) for the ESs will be obtained using bootstrap methods with 5,000 replications. One-sided tests (p < .05) will be conducted under the assumption that the intervention is not harmful.
Following the analytic strategy used in the 7yrs-fu of ProKind (41), as well as in recent evaluations of the trial (42, 71), to address missing observations from families who did not participate in the follow-up and to account for the imbalance in a few baseline risk factors (e.g., maternal aggression and mental health problems) between IG and CG, treatment effects will be estimated using augmented inverse probability weighting (AIPW) in combination with the “least absolute shrinkage and selection operator” (lasso) to select relevant control and weighting variables (107).
The AIPW technique assigns weights to observed cases based on the inverse of their probability of loss to follow-up estimated by logit functions, thereby mitigating potential selection bias caused by attrition. In a second step a linear weighted function with additional control variables is estimated. The variables used in the logit functions for the weighting and the control variables for the linear weighted function are selected by lasso, a machine learning algorithm. By weighting participants according to their inverse probability of remaining in the study, the analytic sample is reweighted to more closely resemble the original randomized population, thereby improving both internal validity and generalizability of the findings. Due to findings of the last program phase, all primary and secondary outcomes will be analyzed regarding any differential effects, while controlling for children's gender (41) and delivery model (42).
Discussion
The aim of the study is to conduct a follow-up survey regarding the effectiveness of the German adaptation of the NFP program, approximately 15 years after the intervention ended. As part of a biopsychosocial evaluation, the long-term effectiveness of the ProKind program is being assessed at the individual level for mothers and their children. This includes examining domains previously assessed in earlier phases, such as parenting competence, life satisfaction, and instances of child abuse and neglect. Furthermore, the study explores health-related risk behaviors (e.g., smoking, alcohol, and drug use), mortality rates (administrative data), fertility rates (administrative data) and legally significant behaviors (e.g., youth delinquency by self-report, administrative Data), which are particularly impactful during adolescence - a crucial stage of development. Moreover, the study will examine the long-term fiscal impacts of the home visiting program on the welfare state. In collaboration with the IAB, data linkage with social security records is conducted to analyze information on employment histories and social benefit claims of the participants. This outcome analysis is of particular interest, as data linkage ensures a very high follow-up rate of approximately 90%.
The long-term evaluation of the ProKind sample is of critical importance for two main reasons. First, no study to date has assessed the long-term effectiveness of NFP program in the European context. Second, some of the most relevant findings related to NFP have emerged five to 20 years after the intervention concluded (24, 108). With this in mind, this randomized controlled trial (RCT) was specifically designed to enable a long-term follow-up, achieved through robust retention efforts and the inclusion of measures that predict long-term outcomes, such as the cognitive development and behavior of the child. Consequently, any successes or limitations of NFP identified in trials conducted when children are two years old may not fully reflect the program's impact, as these findings could be reevaluated or even contradicted during subsequent stages of the children's development.
Limitations
Besides its strengths, the present study also has several limitations that should be considered when interpreting the findings. First, due to the COVID-19 pandemic and the associated infection control measures, significant adjustments had to be made to the study procedures, resulting in considerable delays to the project timeline. Given the profound significance of this study for the German social and healthcare system, this cautious approach to addressing the pandemic's impact remains essential. Contamination of the research findings by pandemic-related effects would have severely limited the interpretability of the results, rendering them unreliable and unsuitable for providing actionable recommendations for the German social and healthcare landscape. Although the research plan originally envisaged the use of standardized performance measures, these could not be implemented due to pandemic-related restrictions. Instead, the assessment of educational outcomes in the present phase relies on self-reported school grades. This method raises concerns regarding the accuracy of retrospective reports by mothers or children, which may create a risk of recall bias. Moreover, educational research consistently shows that grades are only imperfect indicators of actual academic competence, particularly when compared to standardized achievement tests. In later follow-up phases beyond the scope of the present protocol, standardized tests in reading comprehension and basic mathematics could be implemented to provide a more valid and reliable assessment of children's educational outcomes.
Second, most data will be collected via self-report, which may be affected by biases such as social desirability or recall inaccuracies. This applies in particular to psychological, social, and family-related measures. At the same time, for several important domains, administrative data is available (e.g., mortality, fertility, criminal records from the Federal Central Register, social insurance data), which provide more objective indicators and help counterbalance these potential weaknesses. Future research should aim to further expand the integration of register-based information, for example by linking educational data such as school grades or certificates, as well as child welfare data from youth welfare offices (e.g., out-of-home placements or protective measures), in order to strengthen the validity and breadth of the findings. However, such linkages remain difficult to implement in the European context due to strict data protection regulations, which substantially limit systematic access to and use of such data.
Third, the high loss to follow-up during the initial project phase, with rates of about 55% by the 24-month assessment (54), which is substantially above the commonly recommended 20% threshold for RCTs. Such high attrition rates limit the generalizability of the findings, as selective participation may bias estimates toward more resilient or resourceful families and reduce confidence in the representativeness of the intervention effects. This also complicates the interpretation of long-term outcomes, since early selective loss may systematically affect which families remain available for later follow-up assessments. In contrast, retention improved considerably in the 7yrs-fu, with response rates of about 70% in both groups (41). Importantly, in this later phase advanced statistical methods were applied, including inverse probability weighting (IPW). In this procedure, the probability of remaining in the study was modeled using baseline characteristics such as maternal age, socioeconomic status, partnership status, and mental health indicators. Participants who shared characteristics with those lost to follow-up received higher weights in the analysis, thereby reducing selection bias. IPW thus not only improves internal validity but also tackles the problem of generalizability, as it makes the analytic sample more closely resemble the original randomized population. This marks a significant methodological improvement compared to Phase I and will strengthen the robustness and validity of future findings. Nevertheless, even with such procedures, some degree of residual bias cannot be entirely ruled out in long-term evaluations.
Fourth, the widespread availability of German midwifery care in the CG represents an important contextual factor. Using health insurance data, Sandner et al. (68) demonstrated that around 70% of mothers in the CG made use of at least one statutory midwifery visit. It is therefore conceivable that this high baseline level of standard care may have attenuated the likelihood of detecting additional program effects in domains such as maternal physical health or breastfeeding outcomes.
Fifth, the study sample is not fully representative of the migrant population in Germany. The inclusion criteria required sufficient German language proficiency, which effectively excluded families with limited or no German skills. As a result, the proportion of participants with a migration background was only about half of that observed in the general population. This selective exclusion reduces the generalizability of the findings. Future adaptations of early home visiting programs should make efforts to integrate additional resources, such as interpreters, or ensure the engagement of multilingual midwives and/or social workers, in order to include families with limited host-country language skills and thereby better represent this especially vulnerable group.
Lastly, the original trial design concerns the inclusion criteria for pregnant participants, which were based on a binary classification (e.g., “female gender”). From a contemporary perspective, this approach may appear restrictive and insufficiently inclusive, as it does not reflect the diversity of gender identities and experiences of pregnancy. While such a classification reflected the dominant research practices and clinical terminology of the time, current standards emphasize the importance of inclusive and precise language in both study design and reporting (109, 110). Acknowledging this limitation is important to document potential sources of bias in participant selection and to demonstrate awareness of evolving conceptualizations of gender in health research. Future adaptations of the program and related evaluations should therefore consider gender-sensitive inclusion criteria and language that better capture the diversity of people who may benefit from such interventions.
Implications
While studies from the United States provide robust evidence supporting the effectiveness of the NFP, these findings cannot be directly applied to European countries due to contextual differences. This is particularly evident in Germany, where comparable early childhood support programs receive substantial public funding. For example, the Federal Government invested up to €177 million in the Netzwerk Frühe Hilfen (National Center for Early Support) between 2012 and 2015. However, no long-term RCT has been carried out to assess the effectiveness of home-visiting programs within the framework of early childhood support in Germany. This gap highlights the pressing need for a rigorous evaluation to ensure evidence-based decision-making in this critical area.
It is important to note that the original ProKind trial experienced relatively high attrition during the early intervention phase, which could challenge the generalizability of the results. Nevertheless, retention improved markedly by the 7yrs-fu, with approximately 70% of participants re-engaged (41). These figures compare favorably with US NFP-trials [e.g., Elmira: 15yrs-fu (83%), 19yrs-fu (78%) and Memphis: 12yrs-fu (83%) (7, 27)]. In our design we proactively address attrition through structured re-engagement strategies that include repeated data linkage. This approach enables sustained contact with participants over extended periods and ensures the feasibility of future follow-up assessments. In addition, the use of administrative data sources such as mortality records, fertility information, social insurance data, and criminal justice registries provides an important complement to self-report measures. These data reduce the risk of bias due to selective nonresponse and thereby enhance the validity of the long-term findings.
Ethics statement
The University Hospital of Jena (Registration No.: 2021-2372-Bef) authorized the study's design and procedure. Consent was obtained from all participants. Mothers furthermore provided parental consent prior to assessment of the children. Given the observational nature of this follow-up study and the use of administrative data, an independent Data Monitoring Committee (DMC) was not deemed necessary.
Author contributions
SK: Conceptualization, Project administration, Writing – original draft, Writing – review & editing. MS: Project administration, Writing – review & editing. TB: Project administration, Writing – review & editing. SF: Writing – review & editing. AL: Writing – review & editing. MS: Writing – review & editing. GC: Writing – review & editing. DB: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was fully funded by the German Federal Ministry of Education and Research (BMBF funding codes: 01EL2013A/D, 01EL2013B, 01EL2013C) The funder was not and will not be involved in the design of the study, the collection, analysis and interpretation of data or the writing of the protocol. Open access funding by Zurich University of Applied Sciences (ZHAW).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. The authors utilized ChatGPT to enhance linguistic clarity and readability of the manuscript, as they are non-native English speakers. Following this linguistic assistance, the authors thoroughly reviewed, revised, and approved the final text, and assume full responsibility for the content of this publication.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1606749/full#supplementary-material
References
1. Molloy C, Beatson R, Harrop C, Perini N, Goldfeld S. Systematic review: effects of sustained nurse home visiting programs for disadvantaged mothers and children. J Adv Nurs. (2021) 77(1):147–61. doi: 10.1111/jan.14576
2. Olds DL. The nurse-family partnership: an evidence-based preventive intervention. Infant Ment Health J. (2006) 27(1):5–25. doi: 10.1002/imhj.20077
3. Bandura A. Social learning theory of aggression. J Commun. (1978) 28(3):12–29. doi: 10.1111/j.1460-2466.1978.tb01621.x
4. Bronfenbrenner U. Contexts of child rearing: problems and prospects. Am Psychol. (1979) 34(10):844–50. doi: 10.1037/0003-066X.34.10.844
6. Olds DL, Henderson CR Jr, Tatelbaum R, Chamberlin R. Improving the life-course development of socially disadvantaged mothers: a randomized trial of nurse home visitation. Am J Public Health. (1988) 78(11):1436–45. doi: 10.2105/ajph.78.11.1436
7. Eckenrode J, Campa M, Luckey DW, Henderson CR, Cole R, Kitzman H, et al. Long-term effects of prenatal and infancy nurse home visitation. Arch Pediatr Adolesc Med. (2010) 164(1):9–15. doi: 10.1001/archpediatrics.2009.240
8. Kitzman H, Olds DL, Henderson CR, Hanks C, Cole R, Tatelbaum R, et al. Effect of prenatal and infancy home visitation by nurses on pregnancy outcomes, childhood injuries, and repeated childbearing: a randomized controlled trial. JAMA. (1997) 278(8):644–52. doi: 10.1001/jama.1997.03550080054039
9. Kitzman H, Olds DL, Knudtson MD, Cole R, Anson E, Smith JA, et al. Prenatal and infancy nurse home visiting and 18-year outcomes of a randomized trial. Pediatrics. (2019) 144(6):e20183876. doi: 10.1542/peds.2018-3876
10. Olds DL, Kitzman H, Cole R, Robinson J, Sidora K, Luckey DW, et al. Nurse home visiting and mortality. JAMA Pediatr. (2014) 168(9):800–6. doi: 10.1001/jamapediatrics.2014.472
11. Olds DL, Robinson J, Pettitt L, Luckey DW, Holmberg J, Ng RK, et al. Home visiting by paraprofessionals vs. nurses. Pediatrics. (2002) 110(3):486–96. doi: 10.1542/peds.110.3.486
12. Korfmacher J, O’Brien R, Hiatt S, Olds D. Differences in program implementation between nurses and paraprofessionals providing home visits during pregnancy and infancy: a randomized trial. Am J Public Health. (1999) 89(12):1847–51. doi: 10.2105/ajph.89.12.1847
13. Olds DL, Holmberg JR, Donelan-McCall N, Luckey DW, Knudtson MD, Robinson J. Effects of home visits by paraprofessionals and by nurses on children: follow-up of a randomized trial at ages 6 and 9 years. JAMA Pediatr. (2014) 168(2):114–21. doi: 10.1001/jamapediatrics.2013.3817
14. Olds DL, Henderson CR Jr, Tatelbaum R, Chamberlin R. Improving the delivery of prenatal care and outcomes of pregnancy: a randomized trial of nurse home visitation. Pediatrics. (1986) 77(1):16–28. doi: 10.1542/peds.77.1.16
15. Heckman JJ, Holland ML, Makino KK, Pinto R, Rosales-Rueda M. An Analysis of the Memphis Nurse-Family Partnership Program. Cambridge, MA: National Bureau of Economic Research (2017). (NBER Working Paper No. 23610).
16. Miller TR. Projected outcomes of nurse-family partnership home visitation during 1996–2013, USA. Prev Sci. (2015) 16(6):765–77. doi: 10.1007/s11121-015-0572-9
17. Olds DL. Preventing child maltreatment and crime with prenatal and infancy support of parents: the nurse-family partnership. J Scand Stud Criminol Crime Prev. (2008) 9(S1):2–24. doi: 10.1080/14043850802450096
18. Olds DL, Eckenrode J, Henderson CR Jr, Kitzman H, Powers J, Cole R, et al. Long-term effects of home visitation on maternal life course and child abuse and neglect: fifteen-year follow-up of a randomized trial. JAMA. (1997) 278(8):637–43. doi: 10.1001/jama.1997.03550080047038
19. Kitzman H, Olds DL, Sidora K, Henderson CR Jr, Hanks C, Cole R, et al. Enduring effects of nurse home visitation on maternal life course: a 3-year follow-up of a randomized trial. JAMA. (2000) 283(15):1983–9. doi: 10.1001/jama.283.15.1983
20. Olds DL, Robinson J, Pettitt L, Luckey DW, Holmberg J, Ng RK, et al. Effects of home visits by paraprofessionals and by nurses: age 4 follow-up results of a randomized trial. Pediatrics. (2004) 114(6):1560–8. doi: 10.1542/peds.2004-0961
21. Olds DL, Henderson CR Jr, Kitzman H. Does prenatal and infancy nurse home visitation have enduring effects on qualities of parental caregiving and child health at 25 to 50 months of life? Pediatrics. (1994) 93(1):89–98. doi: 10.1542/peds.93.1.89
22. Olds DL, Kitzman H, Cole R, Robinson J, Sidora K, Luckey DW, et al. Effects of nurse home-visiting on maternal life course and child development: age 6 follow-up results of a randomized trial. Pediatrics. (2004) 114(6):1550–9. doi: 10.1542/peds.2004-0962
23. Kitzman HJ, Olds DL, Cole RE, Hanks CA, Anson EA, Arcoleo KJ, et al. Enduring effects of nurse home visiting. Arch Pediatr Adolesc Med. (2010) 164(5):412–8. doi: 10.1001/archpediatrics.2010.76
24. Olds D, Henderson CR Jr, Cole R, Eckenrode J, Kitzman H, Luckey D, et al. Long-term effects of nurse home visitation on children’s criminal and antisocial behavior: 15-year follow-up of a randomized controlled trial. JAMA. (1998) 280(14):1238–44. doi: 10.1001/jama.280.14.1238
25. Olds DL, Kitzman H, Hanks C, Cole R, Anson E, Sidora-Arcoleo K, et al. Effects of nurse home visiting on maternal and child functioning: age-9 follow-up of a randomized trial. Pediatrics. (2007) 120(4):e832–45. doi: 10.1542/peds.2006-2111
26. Glazner JE, Bondy J, Luckey DW, Olds DL. Effect of the Nurse Family Partnership on Government Expenditures for Vulnerable First-time mothers and Their Children in Elmira, New York, Memphis, Tennessee, and Denver, Colorado (#90XP0017): Final Report to the Administration for Children and Families. Washington, DC: US Department of Health and Human Services (2004).
27. Olds DL, Kitzman HJ, Cole RE, Hanks CA, Arcoleo KJ, Anson EA, et al. Enduring effects of prenatal and infancy home visiting by nurses on maternal life course and government spending: follow-up of a randomized trial among children at age 12 years. Arch Pediatr Adolesc Med. (2010) 164(5):419–24. doi: 10.1001/archpediatrics.2010.49
28. McConnell MA, Rokicki S, Ayers S, Allouch F, Perreault N, Gourevitch RA, et al. Effect of an intensive nurse home visiting program on adverse birth outcomes in a medicaid-eligible population: a randomized clinical trial. JAMA. (2022) 328(1):27–37. doi: 10.1001/jama.2022.9703
29. Rokicki S, Oviedo D, Perreault N, Zera C, McGregor AJ, Bates MA, et al. Home visits and the use of routine and emergency postpartum care among low-income people: a secondary analysis of a randomized clinical trial. JAMA Netw Open. (2024) 7(12):e2451605. doi: 10.1001/jamanetworkopen.2024.51605
30. Swanson K, Ayers S, Oviedo D, Zhou RA, Bates MA, Baicker K, et al. Intensive nurse home visiting and early childhood outcomes: a randomized clinical trial. JAMA Pediatr. (2025) 179(8):857–66. doi: 10.1001/jamapediatrics.2025.1600
31. Sadler LS, Slade A, Close N, Webb DL, Simpson T, Fennie K, et al. Minding the baby: enhancing reflectiveness to improve early health and relationship outcomes in an interdisciplinary home visiting program. Infant Ment Health J. (2013) 34(5):391–405. doi: 10.1002/imhj.21406
32. Ordway MR, Sadler LS, Dixon J, Close N, Mayes L, Slade A. Lasting effects of an interdisciplinary home visiting program on child behavior: preliminary follow-up results of a randomized trial. J Pediatr Nurs. (2014) 29(1):3–13. doi: 10.1016/j.pedn.2013.04.006
33. Slade A, Holland ML, Ordway MR, Carlson EA, Jeon S, Close N, et al. Minding the baby®: enhancing parental reflective functioning and infant attachment in an attachment-based, interdisciplinary home visiting program. Dev Psychopathol. (2020) 32(1):123–37. doi: 10.1017/S0954579418001463
34. Londono Tobon A, Condon E, Sadler LS, Holland ML, Mayes LC, Slade A. School age effects of minding the baby—an attachment-based home-visiting intervention—on parenting and child behaviors. Dev Psychopathol. (2022) 34(1):55–67. doi: 10.1017/S0954579420000905
35. Ordway MR, Sadler LS, Holland ML, Slade A, Close N, Mayes LC. A home visiting parenting program and child obesity: a randomized trial. Pediatrics. (2018) 141(2):e20171076. doi: 10.1542/peds.2017-1076. Erratum in: Pediatrics. (2018) 141(6):e20180770. doi: 10.1542/peds.2018-077029339565
36. Mejdoubi J, van den Heijkant S, Struijf E, van Leerdam F, HiraSing R, Crijnen A. Addressing risk factors for child abuse among high risk pregnant women: design of a randomised controlled trial of the nurse family partnership in Dutch preventive health care. BMC Public Health. (2011) 11:823. doi: 10.1186/1471-2458-11-823
37. Mejdoubi J, van den Heijkant SC, van Leerdam FJ, Heymans MW, Crijnen A, Hirasing RA, et al. The effect of VoorZorg, the Dutch nurse-family partnership, on child maltreatment and development: a randomized controlled trial. PLoS One. (2015) 10(4):e0120182. doi: 10.1371/journal.pone.0120182
38. Owen-Jones E, Bekkers MJ, Butler CC, Cannings-John R, Channon S, Hood K, et al. The effectiveness and cost-effectiveness of the family nurse partnership home visiting programme for first time teenage mothers in England: a protocol for the building blocks randomised controlled trial. BMC Pediatr. (2013) 13:114. doi: 10.1186/1471-2431-13-114
39. Robling M, Lugg-Widger F, Cannings-John R, Sanders J, Angel L, Channon S, et al. The Family Nurse Partnership to Reduce Maltreatment and Improve Child Health and Development in Young Children: The BB:2–6 Routine Data-linkage follow-up to Earlier RCT. Southampton, UK: NIHR Journals Library (2021). doi: 10.3310/phr09020
40. Kliem S, Sandner M, Lohmann A, Sierau S, Dähne V, Klein AM, et al. Follow-up study regarding the medium-term effectiveness of the home-visiting program “pro kind” at age 7 years: study protocol for a randomized controlled trial. Trials. (2018) 19:323. doi: 10.1186/s13063-018-2707-3
41. Kliem S, Sandner M. Home visiting in Germany: 7-year outcomes. Pediatrics. (2021) 148(2):e2020049610. doi: 10.1542/peds.2020-049610
42. Schepan ML, Sandner M, Conti G, Kliem S, Brand T. Maternal and child health following 2 home visiting interventions vs control: five-year follow-up of a randomized clinical trial. JAMA Pediatr. (2025) 179(4):367–74. doi: 10.1001/jamapediatrics.2024.5929
43. Catherine NLA, MacMillan H, Cullen A, Zheng Y, Xie H, Boyle M, et al. Effectiveness of nurse-home visiting in improving child and maternal outcomes prenatally to age two years: a randomised controlled trial (British Columbia healthy connections project). J Child Psychol Psychiatry. (2024) 65(5):644–55. doi: 10.1111/jcpp.13846
44. Longhi E, Murray L, Hunter R, Wellsted D, Taylor-Colls S, MacKenzie K, et al. The NSPCC UK minding the baby® (MTB) home-visiting programme, supporting young mothers (aged 14–25) in the first 2 years of their baby’s life: study protocol for a randomised controlled trial. Trials. (2016) 17(1):486. doi: 10.1186/s13063-016-1618-4
45. Pontoppidan M, Hirani JC, Friis-Hansen M. Minding the baby versus usual care: effects on parental sensitivity and parent-child interaction in a cluster quasi-randomized trial. Attach Hum Dev. (2025) 27(4):567–90. doi: 10.1080/14616734.2025.2534608
46. Goldfeld S, Price A, Bryson H, Bruce T, Mensah F, Orsini F, et al. ‘Right@home’: a randomised controlled trial of sustained nurse home visiting from pregnancy to child age 2 years, versus usual care, to improve parent care, parent responsivity and the home learning environment at 2 years. BMJ Open. (2017) 7(3):e013307. doi: 10.1136/bmjopen-2016-013307
47. Price A, Bryson H, Mensah FK, Kenny B, Wang X, Orsini F, et al. Embedding nurse home visiting in universal healthcare: 6-year follow-up of a randomised trial. Arch Dis Child. (2023) 108(10):824–32. doi: 10.1136/archdischild-2023-325662
48. Kemp L, Harris E, McMahon C, Matthey S, Vimpani G, Anderson T, et al. Early childhood sustained home-visiting (MECSH) trial: design, method and sample description. BMC Public Health. (2008) 8:424. doi: 10.1186/1471-2458-8-424
49. Goldfeld S, Price A, Smith C, Bruce T, Bryson H, Mensah F, et al. Nurse home visiting for families experiencing adversity: a randomized trial. Pediatrics. (2019) 143(1):e20181206. doi: 10.1542/peds.2018-1206
50. Goldfeld S, Bryson H, Mensah F, Gold L, Orsini F, Perlen S, et al. Nurse home visiting and maternal mental health: 3-year follow-up of a randomized trial. Pediatrics. (2021) 147(2):e2020025361. doi: 10.1542/peds.2020-025361
51. Mejdoubi J, van den Heijkant SC, van Leerdam FJ, Crone M, Crijnen A, HiraSing RA. Effects of nurse home visitation on cigarette smoking, pregnancy outcomes and breastfeeding: a randomized controlled trial. Midwifery. (2014) 30(6):688–95. doi: 10.1016/j.midw.2013.08.006
52. Conti G, Poupakis S, Sandner M, Kliem S. The effects of home visiting on mother-child interactions: evidence from a randomized trial using dynamic micro-level data. Child Abuse Negl. (2021) 115:105021. doi: 10.1016/j.chiabu.2021.105021
53. Kemp L, Harris E, McMahon C, Matthey S, Vimpani G, Anderson T, et al. Benefits of psychosocial intervention and continuity of care by child and family health nurses in the pre- and postnatal period: process evaluation. J Adv Nurs. (2013) 69(8):1850–61. doi: 10.1111/jan.12052
54. Sierau S, Brand T, Manzoni P, Jungmann T. Effects of home visitation on families. Prev Sci. (2016) 17(1):40–51. doi: 10.1007/s11121-015-0573-8
55. Robling M, Bekkers M-J, Bell K, Butler CC, Cannings-John R, Channon S, et al. Nurse-led home-visitation for teenage mothers. Lancet. (2016) 387:146–55. doi: 10.1016/S0140-6736(15)00392-X
56. Kemp L, Harris E, McMahon C, Matthey S, Vimpani G, Anderson T, et al. Child and family outcomes of a long-term nurse home visitation programme: a randomised controlled trial. Arch Dis Child. (2011) 96(6):533–40. doi: 10.1136/adc.2010.196279
57. Sandner M, Jungmann T. Gender-specific effects of early childhood intervention: evidence from a randomized controlled trial. Labour Econ. (2017) 45:59–78. doi: 10.1016/j.labeco.2016.11.006
58. Longhi E, Murray L, Wellsted D, Hunter R, MacKenzie K, Taylor-Colls S, et al. Minding the Baby® (MTB) Home-Visiting Programme for Vulnerable Young Mothers: Results of a Randomised Controlled Trial in the UK. London: NSPCC (2019).
59. Price A, Zhang J, Goldfeld S, Carlin J, Mensah F. Evaluating the “right@home” randomized trial of nurse home visiting using linked administrative data at school transition. Int J Popul Data Sci. (2024) 9(2):2400. doi: 10.23889/ijpds.v9i2.2400
60. Steinberg L, Morris AS. Adolescent development. Annu Rev Psychol. (2001) 52:83–110. doi: 10.1146/annurev.psych.52.1.83
61. Taubner S, Munder T, Unger A, Wolter S. Effectiveness of early prevention programs in Germany: a systematic review and a meta-analysis. Prax Kinderpsychol Kinderpsychiatr. (2013) 62(8):598–619. doi: 10.13109/prkk.2013.62.8.598
62. Efron B. Forcing a sequential experiment to be balanced. Biometrika. (1971) 58(3):403–17. doi: 10.1093/biomet/58.3.403
63. Bower KM, Nimer M, West AL, Gross D. Parent involvement in maternal, infant, and early childhood home visiting programs: an integrative review. Prev Sci. (2020) 21(5):728–47. doi: 10.1007/s11121-020-01129-z
64. Braaten SM, Nix RL, Gill S, Hostetler MM, McNeil CB, Francis LA, et al. What makes home visits effective? An examination of therapeutic mechanisms in the recipe 4 success preventive intervention. Early Child Res Q. (2025) 72:112–21. doi: 10.1016/j.ecresq.2025.02.012
65. Olds D, Donelan-McCall N, O’Brien R, MacMillan H, Jack S, Jenkins T, et al. Improving the nurse-family partnership in community practice. Pediatrics. (2013) 132(Suppl 2):S110–7. doi: 10.1542/peds.2013-1021I
66. Sandner M. Effects of early childhood intervention on fertility and maternal employment: evidence from a randomized controlled trial. J Health Econ. (2019) 63:159–81. doi: 10.1016/j.jhealeco.2018.11.003
67. Jungmann T, Brand T, Dähne V, Herrmann P, Günay H, Sandner M, et al. Comprehensive evaluation of the pro kind home visiting program: a summary of results. Ment Health Prev. (2015) 3(3):89–97. doi: 10.1016/j.mhp.2015.06.001
68. Sandner M, Cornelissen T, Jungmann T, Herrmann P. Evaluating the effects of a targeted home visiting program on maternal and child health outcomes. J Health Econ. (2018) 58:269–83. doi: 10.1016/j.jhealeco.2018.02.008
69. Herrmann P, Meyer K, Sandner M, Jungmann T, Rahman A, Geurtsen W, et al. Zahnärztliche Gesundheitsfrühförderung in der Frühen Hilfe – Eine randomisierte Kontrollgruppenstudie. Dtsch Zahnärztl Z. (2014) 69(10):573–83. doi: 10.3238/dzz.2014.0573-0583
70. Conti G, Kliem S, Sandner M. Early home visiting delivery model and maternal and child mental health at primary school age. AEA Pap Proc. (2024) 114:401–6. doi: 10.1257/pandp.20241087
71. Conti G, Sandner M, Brand T, Kliem S. Efficacy of delivery models in early intervention: findings from Germany’s nurse-family partnership on family and child welfare services and pediatric medical incidents in high-risk families. Child Abuse Negl. (2025) 166:107513. doi: 10.1016/j.chiabu.2025.107513
72. Masten AS, Cicchetti D. Developmental cascades. Dev Psychopathol. (2010) 22(3):491–5. doi: 10.1017/S0954579410000222
73. Rapee RM, Oar EL, Johnco CJ, Forbes MK, Fardouly J, Magson NR, et al. Adolescent development and risk for the onset of social-emotional disorders: a review and conceptual model. Behav Res Ther. (2019) 123:103501. doi: 10.1016/j.brat.2019.103501
74. Blonigen DM. Explaining the relationship between age and crime: contributions from the developmental literature on personality. Clin Psychol Rev. (2010) 30(1):89–100. doi: 10.1016/j.cpr.2009.10.001
75. Moffitt TE. Male antisocial behaviour in adolescence and beyond. Nat Hum Behav. (2018) 2:177–86. doi: 10.1038/s41562-018-0309-4
76. Mori C, Temple JR, Browne D, Madigan S. Association of sexting with sexual behaviors and mental health among adolescents: a systematic review and meta-analysis. JAMA Pediatr. (2019) 173(8):770–9. doi: 10.1001/jamapediatrics.2019.1658
77. Casey BJ, Jones RM, Hare TA. The adolescent brain. Ann N Y Acad Sci. (2008) 1124:111–26. doi: 10.1196/annals.1440.010
78. Steinberg L. A dual systems model of adolescent risk-taking. Dev Psychobiol. (2010) 52(3):216–24. doi: 10.1002/dev.20445
79. Waters SF, Thompson RA. Children’s perceptions of emotion regulation strategy effectiveness: links with attachment security. Attach Hum Dev. (2016) 18(4):354–72. doi: 10.1080/14616734.2016.1170051
80. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am J Prev Med. (1998) 14(4):245–58. doi: 10.1016/s0749-3797(98)00017-8
81. Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health. (2017) 2(8):e356–66. doi: 10.1016/S2468-2667(17)30118-4
82. Kalmakis KA, Chandler GE. Health consequences of adverse childhood experiences: a systematic review. J Am Assoc Nurse Pract. (2015) 27(8):457–65. doi: 10.1002/2327-6924.12215
83. Merrick MT, Ford DC, Ports KA, Guinn AS, Chen J, Klevens J, et al. Vital signs: estimated proportion of adult health problems attributable to adverse childhood experiences and implications for prevention—25 states, 2015–2017. MMWR Morb Mortal Wkly Rep. (2019) 68(44):999–1005. doi: 10.15585/mmwr.mm6844e1
84. Moffitt TE, Arseneault L, Belsky D, Dickson N, Hancox RJ, Harrington H, et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proc Natl Acad Sci. (2011) 108(7):2693–8. doi: 10.1073/pnas.1010076108
85. Welsh BC, Sullivan CJ, Olds DL. When early crime prevention goes to scale: a new look at the evidence. Prev Sci. (2010) 11(2):115–25. doi: 10.1007/s11121-009-0159-4
86. Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev. (1993) 100(4):674–701. doi: 10.1037/0033-295X.100.4.674
87. Odgers CL, Moffitt TE, Broadbent JM, Dickson N, Hancox RJ, Harrington H, et al. Female and male antisocial trajectories: from childhood origins to adult outcomes. Dev Psychopathol. (2008) 20(2):673–716. doi: 10.1017/S0954579408000333
88. Fergusson DM, Horwood LJ, Ridder EM. Show me the child at seven: the consequences of conduct problems in childhood for psychosocial functioning in adulthood. J Child Psychol Psychiatry. (2005) 46(8):837–49. doi: 10.1111/j.1469-7610.2004.00387.x
89. Widom CS, Czaja S, Dutton MA. Child abuse and neglect and intimate partner violence victimization and perpetration: a prospective investigation. Child Abuse Negl. (2014) 38(4):650–63. doi: 10.1016/j.chiabu.2013.11.004
90. Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med. (2012) 9(11):e1001349. doi: 10.1371/journal.pmed.1001349
91. Chan AW, Boutron I, Hopewell S, Moher D, Schulz KF, Collins GS, et al. SPIRIT 2025 statement: updated guideline for protocols of randomised trials. JAMA. (2025) 334(5):435–43. doi: 10.1001/jama.2025.4486
92. Entringer TM, Kröger H. Psychische Gesundheit im zweiten Covid-19-Lockdown in Deutschland. SOEPpapers 1136. Berlin: Deutsches Institut für Wirtschaftsforschung (DIW) (2021).
93. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates (1988).
94. Achenbach TM, Rescorla LA. Child Behavior Checklist for ages 6–18 (CBCL/6–18, ASEBA CBCL/6–18) [Database record]. APA PsycTests. (2001) doi: 10.1037/t47452-000
95. Döpfner M, Plück J, Kinnen C. CBCL/6-18R, TRF/6-18R, YSR/11-18R: Deutsche Schulalter-Formen der Child Behavior Checklist. Göttingen: Hogrefe (2014).
96. Lovibond PF, Lovibond SH. Depression anxiety stress scales. Behav Res Ther. (1995) 33:335–43. doi: 10.1016/0005-7967(94)00075-U
97. Straus MA, Hamby SL, Finkelhor D, Moore DW, Runyan D. Parent–child conflict tactics scales. Child Abuse Negl. (1998) 22(4):249–70. doi: 10.1016/S0145-2134(97)00174-9
98. Straus MA, Kinard EM, Williams LM. Multidimensional Neglect Scale (MNS) [Database record]. APA PsycTests. (1995) doi: 10.1037/t02378-000
99. Straus MA, Hamby SL, Finkelhor D, Moore DW, Runyan D. Identification of child maltreatment with the parent-child conflict tactics scales: development and psychometric data for a national sample of American parents. Child Abuse Negl. (1998) 22(4):249–70. doi: 10.1016/s0145-2134(97)00174-9
100. Arnold DS, O’Leary SG, Wolff LS, Acker MM. The parenting scale: a measure of dysfunctional parenting in discipline situations. Psychol Assess. (1993) 5:137–44. doi: 10.1037/1040-3590.5.2.137
101. Kliem S, Walper S, Schindler A. Partnergewalt und kindliche entwicklung. Prax Kinderpsychol Kinderpsychiatr. (2019) 68(1):63–80. doi: 10.13109/prkk.2019.68.1.63
102. Mattejat F, Remschmidt H. ILK – Lebensqualität bei Kindern und Jugendlichen. Göttingen: Hogrefe (1998).
103. Fahrenberg J, Myrtek M, Schumacher J, Brähler E. Fragebogen zur Lebenszufriedenheit (FLZ). Göttingen: Hogrefe (2001).
104. Krieg Y, Rook L, Beckmann L, Kliem S. Jugendliche in Niedersachsen. Ergebnisse des Niedersachsensurveys 2019. Forschungsbericht Nr. 154. Hanover: Kriminologisches Forschungsinstitut Niedersachsen e.V. (KFN) (2020). Available online at: https://kfn.de/wp-content/uploads/Forschungsberichte/FB_154.pdf (Accessed August 27, 2025).
105. Robin AL, Foster SL. Conflict Behavior Questionnaire–Parent Version (CBQ) [Database record]. APA PsycTests (1989). doi: 10.1037/t60684-000
106. Prinz RJ, Foster S, Kent RN, O’Leary KD. Conflict in mother–adolescent dyads. J Appl Behav Anal. (1979) 12(4):691–700. doi: 10.1901/jaba.1979.12-691
107. Chernozhukov V, Chetverikov D, Demirer M, Duflo E, Hansen C, Newey W, et al. Double/debiased machine learning for treatment and structural parameters. Econom J. (2018) 21(1):C1–C68. doi: 10.1111/ectj.12097
108. Olds DL, Kitzman H, Knudtson MD, Anson E, Smith JA, Cole R. Effect of home visiting by nurses on maternal and child mortality: results of a 2-decade follow-up of a randomized clinical trial. JAMA Pediatr. (2014) 168(9):800–6. doi: 10.1001/jamapediatrics.2014.472
109. Thorne N, Yip AK, Bouman WP, Marshall E, Arcelus J. The terminology of identities between, outside and beyond the gender binary: a systematic review. Int J Transgend. (2019) 20(2-3):138–54. doi: 10.1080/15532739.2019.1640654
Keywords: nurse family partnership program, sustained nurse home visiting programs (SNHVs), randomized controlled trial (RCT), follow-up, study protocol
Citation: Kliem S, Sandner M, Brand T, Fischer S, Lohmann A, Schepan ML, Conti G and Baier D (2025) Follow-up study on the long-term effectiveness of the home-visiting program “ProKind”: study protocol for a randomized controlled trial. Front. Pediatr. 13:1606749. doi: 10.3389/fped.2025.1606749
Received: 6 April 2025; Accepted: 11 September 2025;
Published: 8 October 2025.
Edited by:
Renaud Becquet, Bordeaux Population Health Research Centre (Inserm, IRD, Bordeaux University), FranceReviewed by:
Andrea Lanfranchi, Interkantonale Hochschule für Heilpädagogik (HfH), SwitzerlandNicole Catherine, Simon Fraser University, Canada
Copyright: © 2025 Kliem, Sandner, Brand, Fischer, Lohmann, Schepan, Conti and Baier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sören Kliem, c29lcmVuLmtsaWVtQGVhaC1qZW5hLmRl; Dirk Baier, ZGlyay5iYWllckB6aGF3LmNo; ZGlyay5iYWllckBpdXMudXpoLmNo