 Kristopher Amaro-Hosey
Kristopher Amaro-Hosey Immaculada Danés
Immaculada Danés Antònia Agustí
Antònia Agustí- 1Clinical Pharmacology Service, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
- 2Department of Pharmacology, Therapeutics and Toxicology, Universitat Autònoma de Barcelona, Barcelona, Spain
- 3Vall d’Hebron Research Institute, Barcelona, Spain
- 4Clinical Pharmacology Service, Vall d’Hebron University Hospital, Barcelona, Spain
Introduction: Adverse drug reactions (ADR) are an important cause of morbidity and mortality in pediatric patients. Due to the disease severity and chemotherapy safety profile, oncologic patients are at higher risk of ADR. However, there is little evidence on pharmacovigilance studies evaluating drug safety in this specific population.
Methods: In order to assess the incidence and characteristics of ADR in pediatric patients with oncohematogical diseases and the methodology used in the studies, a systematic review was carried out using both free search and a combination of MeSH terms. Data extraction and critical appraisal were performed independently using a predefined form.
Results: Fourteen studies were included, of which eight were prospective and half focused in inpatients. Sample size and study duration varied widely. Different methods of ADR identification were detected, used alone or combined. Causality and severity were assessed frequently, whereas preventability was lacking in most studies. ADR incidence varied between 14.4 and 67% in inpatients, and 19.6–68.1% in admissions, mainly in the form of hematological, gastrointestinal and skin toxicity. Between 11 and 16.4% ADR were considered severe, and preventability ranged from 0 to 74.5%.
Conclusion: ADR in oncohematology pediatric patients are frequent. A high variability in study design and results has been found. The use of methodological standards and preventability assessment should be reinforced in order to allow results comparison between studies and centers, and to detected areas of improvement.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=96513, identifier CRD42018096513.
Introduction
Adverse drug reactions (ADR) have been defined by the World Health Organization (WHO) as “a response to a drug which is noxious and unintended, and which occurs at doses normally used in man for the prophylaxis, diagnosis, or therapy of disease, or for modification of physiological function” (WHO, 1972).
ADR are an important cause of morbidity and mortality in patients of all ages, including pediatric population, and are considered a public health problem worldwide (Impicciatore et al., 2001; Clavenna and Bonati, 2009; Thiesen et al., 2013; Durrieu et al., 2014; Ramos et al., 2021). Children are more susceptible to ADR owing to insufficient standardized information, unlicensed and off-label use, unavailability of pediatric formulations, and physiological peculiarities inherent to age (Ramos et al., 2021).
Different systematic reviews and meta-analysis including ADR observational studies have found an incidence of ADR in pediatric inpatients ranging 0.6–16.8%, from 1.8 to 2.09% leading to hospital admission and 1.0–1.46% in outpatient setting (Impicciatore et al., 2001; Clavenna and Bonati, 2009; Smyth et al., 2012). In addition, ADR prevention in outpatients remains a public health and a patient safety challenge (Lombardi et al., 2018). A systematic review including 102 articles assessed preventability in only 19, which ranged from 7 to 98%. This high variability was explained due to a high heterogeneity in study designs, methods and settings (Smyth et al., 2012).
Risk factors for ADR in children are poorly characterized (Bellis et al., 2013; Lombardi et al., 2018). Age on admission, number of drugs, off-label drug use, and oncology diagnosis and treatment have been described as ADR risk factors (Bellis et al., 2013; Thiesen et al., 2013). Moreover, one of these studies stated the risk in oncology patients and found an increased risk for ADR (OR = 1.89 [95% CI 1.36–2.63]) (Thiesen et al., 2013).
Chemotherapy toxicity is a common cause of morbidity and mortality in most pediatric cancer patients, and a frequent cause of mid and long term sequel (Conyers et al., 2018). Even though drugs used in cancer diseases are described as a risk factor of ADR occurrence, and that ADR are frequent in oncology and hematology hospitalization wards, there are very few studies that have quantified or analyzed any of these aspects in pediatric population.
Oncohematological diseases have a high impact on children and their families, and on their quality of life. Improving the knowledge of ADR incidence, characteristics and preventability can be useful to compare results between studies and centers and to detect improvement areas, as a way to offer quality healthcare. Our aim was to perform a systematic review in order to describe the incidence and characteristics of ADR in pediatric oncology and hematology patients, to describe the methodology used in the included studies and, if possible, to identify preventive actions in order to minimize ADR occurrence.
Methods
Study Design
A systematic review of observational studies that evaluated the prevalence, incidence and/or characteristics of ADR in pediatric oncohematology was performed. This study was conducted in accordance with the recommendations of the Joanna Briggs Institute (Munn et al., 2015) for systematic reviews of observational epidemiologic studies that evaluate prevalence and incidence data, and the PRISMA recommendations for systematic reviews (Tricco et al., 2018). This study was registered (CRD42018096513) at PROSPERO systematic review database.
Systematic Literature Search
A systematic literature search was carried out in PubMed from inception to 31st December 2020, both using free search and the combination of different MeSH terms (“Pediatrics,” “Neoplasms,” “Hematology,” “Antineoplastic agents,” “Drug-related side effects and adverse reactions,” “Iatrogenic disease,” “Prevention and control,” “Medical oncology,” and “Primary prevention”). References of the articles assessed for eligibility were also reviewed and included if considered relevant.
Inclusion and Exclusion Criteria
Studies that described the incidence and/or characteristics of ADR in pediatric oncohematology patients or in pediatric population with a differentiated oncohematology subgroup were included in this systematic review. Articles describing infectious outbreaks related to immunosuppression, data from national or international clinical databases of spontaneous pharmacovigilance reporting systems and pharmacovigilance studies including one single drug or specific ADR were excluded. No language or other search filters were applied.
Screening and Data Extraction
All articles were screened independently by two authors (KA-H, ID) to identify relevant studies based on titles and abstracts, and on full texts of potentially relevant papers if study relevance could not be determined from the titles and abstracts. For studies meeting inclusion criteria, data were extracted independently using a standardized data collection form defined and agreed previously. Data extracted included article identification, methodology characteristics (study design, setting, study aim, ADR definition and detection method, and causality, severity and preventability scales used), and relevant results (sample size, study duration, population characteristics, ADR frequency and description, severity and preventability). A third author (AA) participated in the review and in the data extraction in case of disagreement.
Data Analysis and Quality Assessment
\This review focuses on both the incidence of ADR in a high-risk population and on the methodological characteristics of the studies included. Quality assessment was performed independently by two authors (KA-H, ID), using a scale designed and previously published (Laatikainen et al., 2017), available in the Supplementary Material. The scale includes six questions related to study design, study population, ADR definition and identification, causality assessment and result description. Each question can be evaluated as 0 or 1, where 0 indicates the poor quality of the study regarding that item. A third author (AA) participated in the critical appraisal in case of disagreement.
Results
Using the research strategies defined previously, 7,712 studies were retrieved from PubMed database. Forty articles were considered relevant for eligibility and finally, considering inclusion and exclusion criteria, 14 studies were included in the systematic review (Collins et al., 1974; Mitchell et al., 1988; Queuille et al., 2001; Le et al., 2006; Gallagher et al., 2012; Posthumus et al., 2012; Barrett et al., 2013; Call et al., 2014; Langerová et al., 2014; Makiwane et al., 2019; Dittrich et al., 2020; Joseph et al., 2020; Morales-Ríos et al., 2020; Workalemahu et al., 2020). Due to the characteristics of studies found, a meta-analysis was considered not feasible to be carried out. Figure 1 shows the study flow chart.
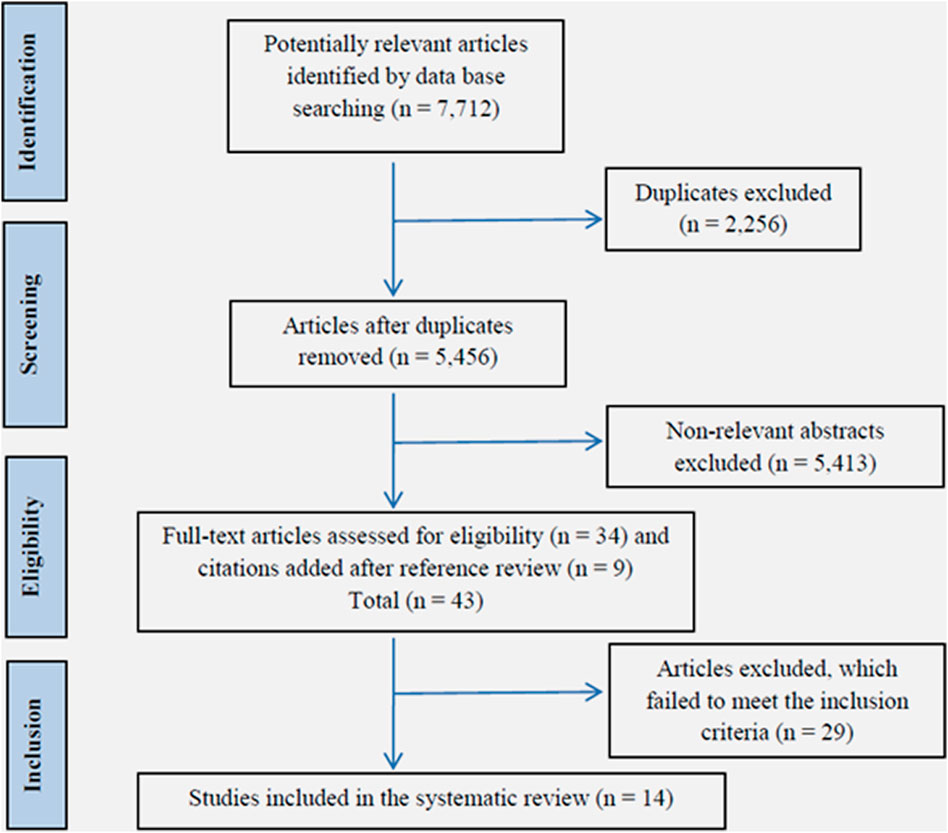
FIGURE 1. Study flow chart.
Study characteristics and main results are summarized in Tables 1–4. Of the 14 studies included, six were carried out in pediatric oncology and hematology patients, and eight were carried out in general pediatrics and included a clear pediatric oncohematology subgroup. Four studies (Collins et al., 1974; Mitchell et al., 1988; Queuille et al., 2001; Le et al., 2006) were published before 2010, and 10 studies (Gallagher et al., 2012; Posthumus et al., 2012; Barrett et al., 2013; Call et al., 2014; Langerová et al., 2014; Makiwane et al., 2019; Dittrich et al., 2020; Joseph et al., 2020; Morales-Ríos et al., 2020; Workalemahu et al., 2020) were published later.
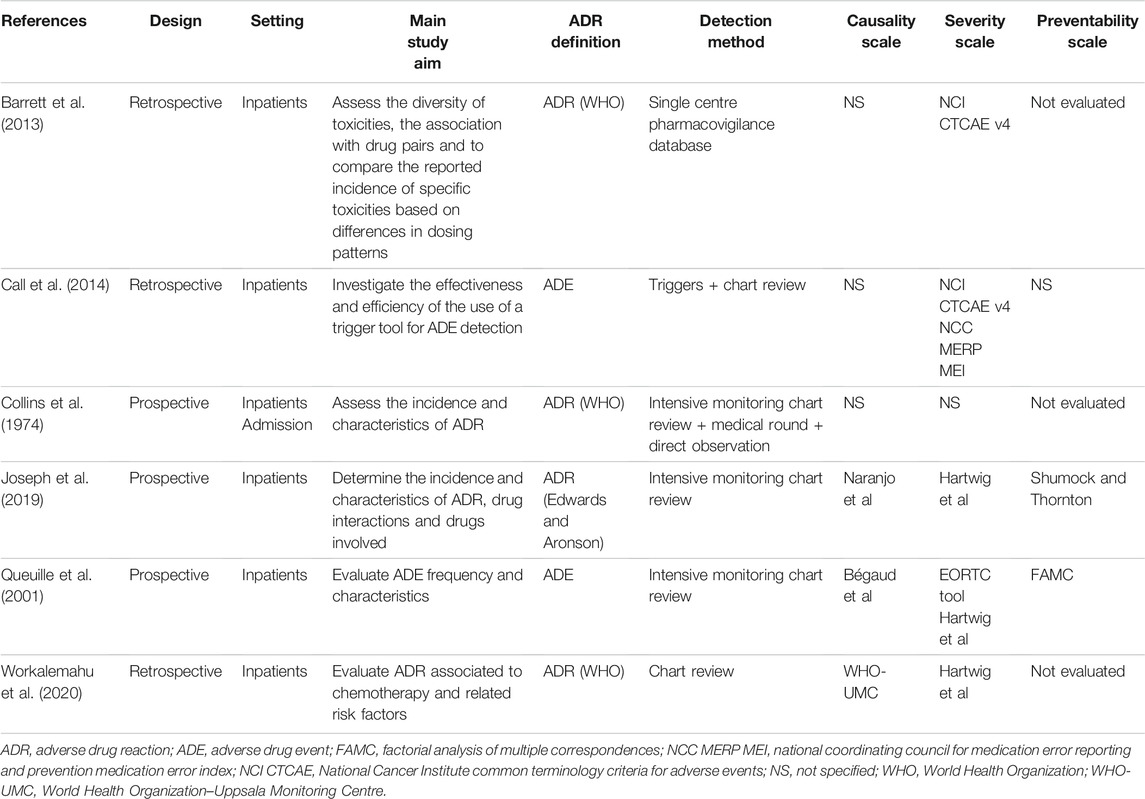
TABLE 1. Methodology characteristics in pediatric oncohematology studies.
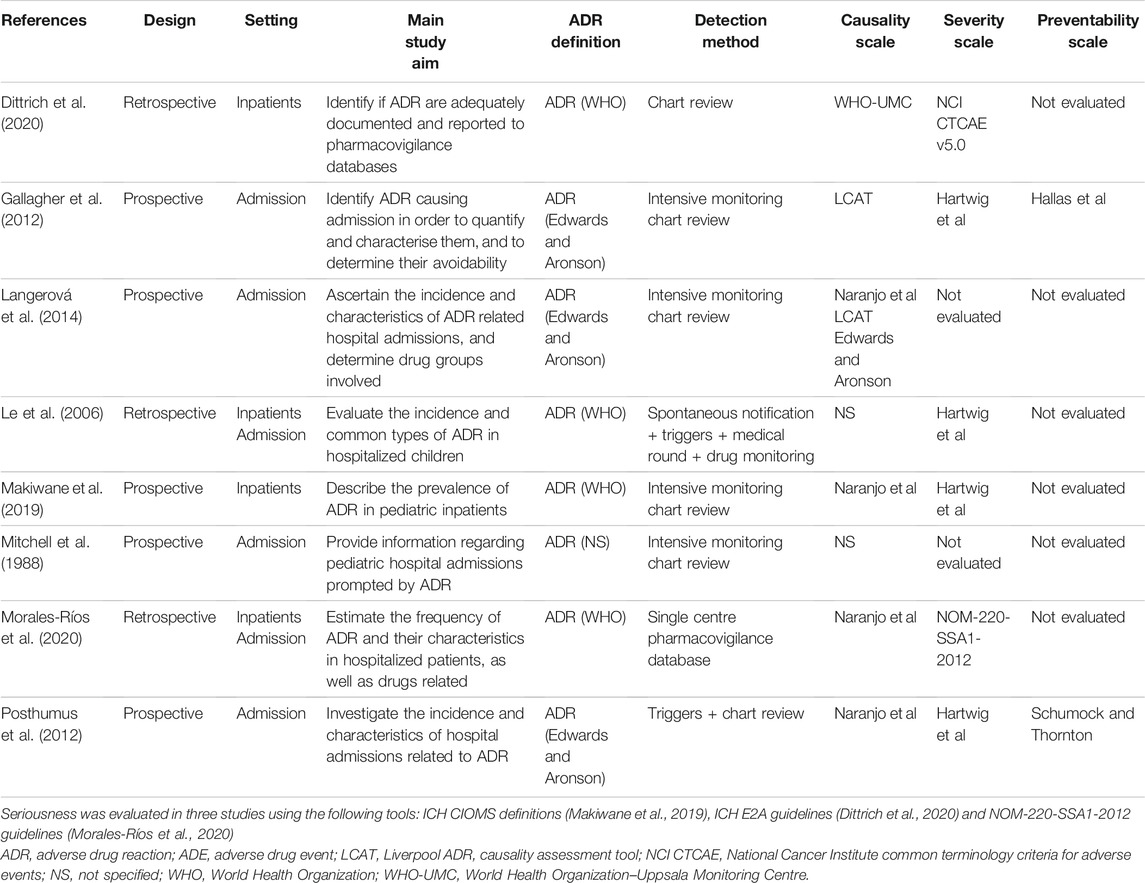
TABLE 2. Methodology characteristics in pediatric studies with oncohematology subpopulation.
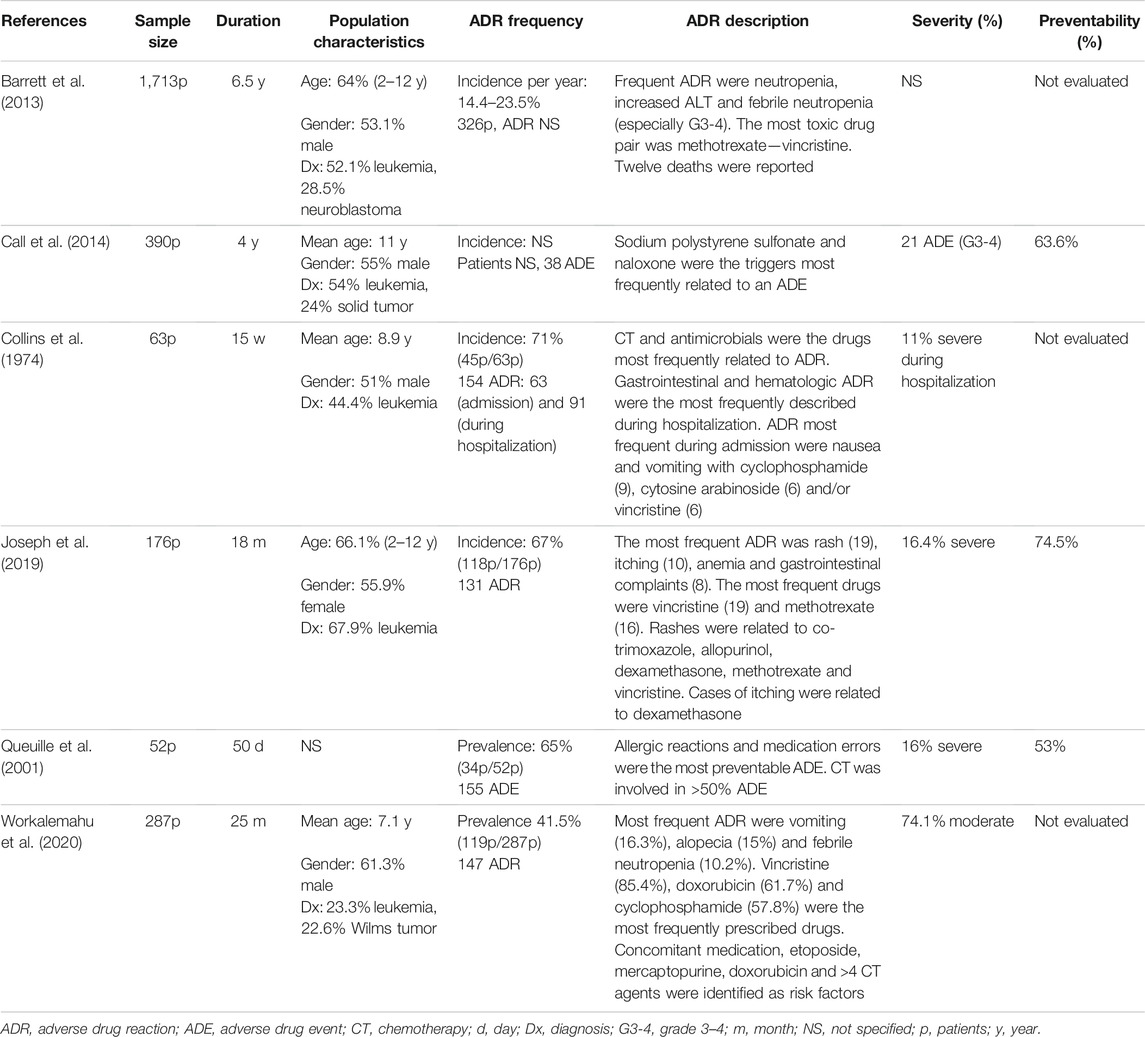
TABLE 3. Clinical results in pediatric oncohematology studies.
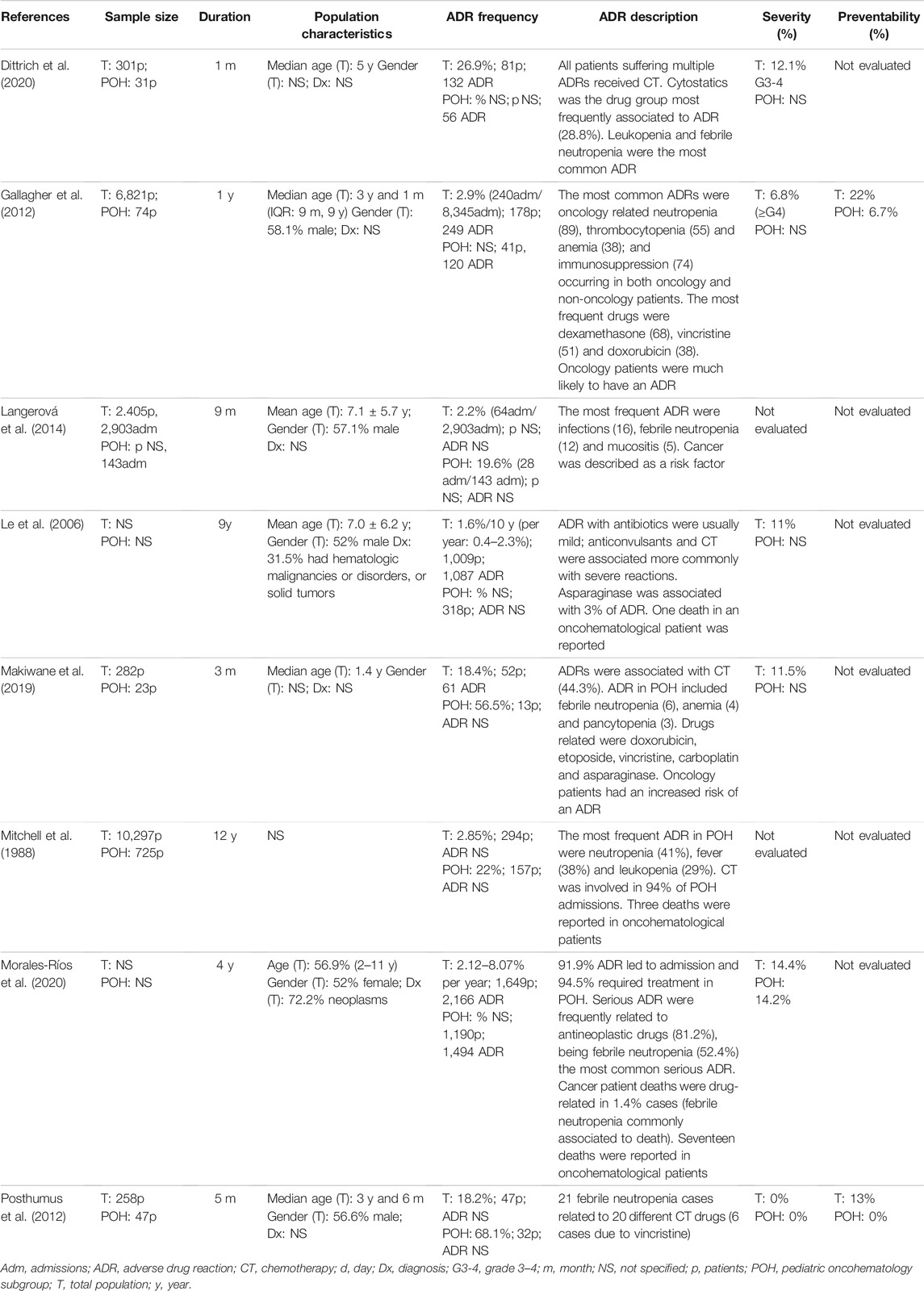
TABLE 4. Clinical results in pediatric studies with oncohematology subpopulation.
Methodological Results
Eight observational studies collected data prospectively, whereas six were performed retrospectively. Seven studies focused on hospitalized patients, four included admissions related to ADR and three analyzed both settings. No studies assessing outpatient setting were found. Twelve studies evaluated ADR, predominantly using WHO or Edward and Aronson definitions, and two studies used adverse drug events (ADE). Causality was estimated in nine studies, using mainly Naranjo and WHO-UMC scales. Severity was assessed in 11 studies, mostly using Hartwig et al. scale and NCI CTCAE criteria. Finally, preventability was only evaluated in five studies out of 14, using Shumock and Thorton in two of them. Ten studies used a single ADR detection method, and four studies used a combination of them: intensive monitoring chart review method was used in seven studies, chart review was used in four studies, and three studies based their results in triggers.
Critical appraisal is summarized in the supplementary material. Most of the studies defined adequately the study population and stated the causality assessment tool used (questions 2 [Q2] and 5 [Q5]). In contrast, results were considered not clearly described in half of the studies (Q6), as the information provided by the original articles on number of patients or ADR was missing. In addition, study design (Q1), ADR definition (Q3), and ADR detection method (Q4) were not clearly mentioned in three studies.
Clinical Results
Sample size varied from 52 to 10,297 patients, as well as study duration, which ranged from 30 days up to 12 years. Age was expressed in means in five studies, as median in four or with percentage of patients in an age range (2–12 years old) in three; age values can be found in Tables 3, 4. Gender varied from 44.1 to 61.3% of males, and was not stated in four studies. Leukemia and solid tumors were the main cancer diagnosis, stated in seven studies. ADR incidence varied depending on study setting: it ranged from 14.4 to 67% in hospitalized patients, 19.6–68.1% in admissions caused by an ADR, and 2.12–71% in studies evaluating both settings. Chemotherapy toxicity described in the studies was related to hematological toxicity (anemia, febrile neutropenia), gastrointestinal toxicity (nausea, vomiting, transaminases increase), and skin (alopecia, rash). Both chemotherapy agents such as methotrexate, doxorubicin or vincristine, and antimicrobials were frequently related to ADR in oncohematology population. Severe ADR frequency described was 11–16.4%, and preventability also varied from 0 to 74.5%. Only four studies reported fatal cases, shown at the results tables.
Four studies included in this systematic review also assessed risk factors for an ADR. In general pediatric studies, Langerová et al. described oncology patients as an independent risk factor (OR = 9.8 [95% CI: 5.8–16.7]), as well as Makiwane et al. (OR = 7.3 [95% CI 3.0–18.9] and Gallagher et al., finding an even higher risk (OR = 29.7 [95% CI 17.4–50.9]). Workalemahu et al. described an increased risk for etoposide (OR = 1.99 [95% CI 0.93–4.27]), mercaptopurine (OR = 3.91 [95% CI 1.1–14.5), doxorubicin (OR = 2.32 [95% CI 1.3–4.2]) and >4 chemotherapy agents (OR = 2.7 [95% CI 1.5–4.7).
Discussion
Even though ADR are an important cause of morbidity and mortality, are frequent in oncology and hematology, and chemotherapy is described as a risk factor, only 14 studies that assessed ADR were found. Incidence rates ranged from 14.4 to 61.3% in hospitalized patients and 19.6–68.1% in ADR leading to admission. A high heterogeneity in methodological aspects reviewed was also described and has likely influenced on the observed results. To our knowledge, this is the first systematic review on pharmacovigilance regarding pediatric oncology and hematology.
As mentioned previously, a high variability regarding methodology was found in almost every aspect of study design: sample size, study duration, study setting, population of interest, ADR detection method, the assessment of severity and preventability, and the different scales used. These findings could be explained by the different aim of each study, the effort to adapt the study to each local environment and available resources, research experience of the team and the moment in which they were designed and carried out, since methodology has evolved over time. These methodological differences have probably influenced on the clinical results found. A systematic review on ADR detection methods in hospitalized children was carried out (Ramos et al., 2021) and found that methods such as intensive monitoring chart review or trigger tools are more effective but time consuming, whereas spontaneous notification showed the lowest rate of detection. They concluded that most of the studies used a combination of methods, which might indicate a growing concern in ADR care in hospitalized children. This improvement in combined methods for ADR detection was previously suggested (Gonzalez-Gonzalez et al., 2013).
To our knowledge, there is no reference quality assessment tool for observational studies with other designs than cohort or case-control studies. A systematic review (Katrak et al., 2004) pointed out the variability in 121 published critical appraisal tools, regarding its intent, components and construction; this finding was later confirmed in another systematic review (Page et al., 2018), which concluded that there are several limitations of existing tools for assessing risk of reporting biases. STROBE statement (von Elm et al., 2007) or Johanna Briggs Institute (Munn et al., 2015) critical appraisal checklists are the most known tools, but their application was complex and troublesome. Therefore, the choice of the checklist used in this systematic review (Laatikainen et al., 2017) was agreed by the research team due to the lack of a standardized tool, its suitability to the type of studies included in the systematic review and to the aim of the critical appraisal analysis, and its easy application. The main area of improvement was the presentation of results, as results were insufficient or missing in half of the studies, and therefore it was considered to be the aspect most susceptible to introduce bias. Moreover, an adequate study design statement, ADR definition and identification clearly mentioned would likely reduce the risk of bias and improve study quality. Ten studies were published after the STROBE statement, which suggests a need to reinforce the use of these tools both during study design and manuscript drafting.
Incidence described in oncohematology pediatric patients was higher, in contrast with studies in pediatrics, which described an overall rate of ADR of 9.53 and 2.09% (hospitalized and admission, respectively) (Impicciatore et al., 2001). This finding is expectable and consistent with chemotherapy safety profile and ADR risk factors, such as cancer diagnosis or number of concomitant drugs. Moreover, it is likely that the use of different scales in causality and severity assessment has influenced on the results observed too.
Hematological, gastrointestinal and skin toxicities are the most frequently described ADR in the articles included, which are in tune with the expected safety profile of conventional chemotherapy. No studies with novel drugs such as monoclonal antibodies or tyrosine kinase inhibitors were found up to 2020. A recently published study (Amaro-Hosey et al., 2021) prospectively assessed drug safety with some specific therapies, including novel drugs and conventional chemotherapy. The most frequent ADR were hematological, infections and gastrointestinal. Incidence using days at risk was calculated regarding novel therapies: 1.1 and 5.3 ADR/100 days at risk for blood disorders and 0.8 and four ADR/100 days at risk for infections, related to pegaspargase and thioguanine respectively; and 0.6 ADR/100 days at risk for infections attributed to rituximab. Only four out of 14 studies included in the systematic review reported fatal cases, and the global incidence of fatal cases could not determined because the total population was not specified in two studies (Le et al., 2006; Morales-Ríos et al., 2020). This finding has been previously described and could either suggest that fatal ADR are very rare in children or are frequently underreported or not suspected (Bouvy et al., 2015).
ADR preventability is a key aspect to analyze, in order to identify areas of improvement to reduce ADR occurrence and improve patients’ life quality. A systematic review (Smyth et al., 2012) identified that preventability was only assessed in 19 out of 102 studies, and ranged from 7 to 98%. This finding is similar to result obtained in the current systematic review, which evidences that it’s an aspect poorly evaluated in pharmacovigilance studies and therefore should be encouraged.
This systematic review tries to add some evidence on an important health problem insufficiently studied that affects a fragile population. Summarized data on characteristics and incidence of ADR in this population is provided, as well as a methodological description in order to find areas of improvement. Defined inclusion and exclusion criteria, the selection of studies in pediatrics with an oncohematology subgroup, the lack of non-standardized critical appraisal tool that fitted the study characteristics and the use of a selected/concrete critical appraisal tool may have introduced bias, but was agreed and considered appropriate to enrich the results and the discussion. Great heterogeneity makes it difficult to compare results, but can also be interpreted as a need to establish methodology standards or to reinforce their use during study design and manuscript drafting, such as STROBE statement. Ultimately, our aim should be to provide a high quality research and healthcare to our patients and to improve their quality of life, regarding drug efficacy and safety.
In conclusion, ADR in oncohematology pediatric patients are more frequent than in general pediatric population, as expected. A high variability in study design and results has been found, which indicates a need to reinforce the use of methodological standards both in study design and manuscript drafting, in order to allow comparability between studies and to identify areas of prevention and improvement. Preventability assessment should be strongly encouraged in order to provide a high quality healthcare and to improve patients’ quality of life.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
KA-H and ID contributed to the conception and design of the study, and contributed to the recording of the data. Substantial contribution to the analysis or interpretation of data for the work was made by KA-H, ID and AA. KA-H wrote the first draft of the manuscript. All authors substantially contributed to the manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.777498/full#supplementary-material
References
Amaro-Hosey, K., Danés, I., Vendrell, L., Alonso, L., Renedo, B., Gros, L., et al. (2021). Adverse Reactions to Drugs of Special Interest in a Pediatric Oncohematology Service. Front. Pharmacol. 12, 670945. doi:10.3389/fphar.2021.670945
Barrett, J. S., Patel, D., Dombrowsky, E., Bajaj, G., and Skolnik, J. M. (2013). Risk Assessment of Drug Interaction Potential and Concomitant Dosing Pattern on Targeted Toxicities in Pediatric Cancer Patients. AAPS J. 15, 775–786. doi:10.1208/s12248-013-9489-z
Bellis, J. R., Kirkham, J. J., Thiesen, S., Conroy, E. J., Bracken, L. E., Mannix, H. L., et al. (2013). Adverse Drug Reactions and Off-Label and Unlicensed Medicines in Children: a Nested Case-Control Study of Inpatients in a Pediatric Hospital. BMC Med. 11, 238. doi:10.1186/1741-7015-11-238
Bouvy, J. C., De Bruin, M. L., and Koopmanschap, M. A. (2015). Epidemiology of Adverse Drug Reactions in Europe: a Review of Recent Observational Studies. Drug Saf. 38, 437–453. doi:10.1007/s40264-015-0281-0
Call, R. J., Burlison, J. D., Robertson, J. J., Scott, J. R., Baker, D. K., Rossi, M. G., et al. (2014). Adverse Drug Event Detection in Pediatric Oncology and Hematology Patients: Using Medication Triggers to Identify Patient Harm in a Specialized Pediatric Patient Population. J. Pediatr. 165, 447–e4. e4. doi:10.1016/j.jpeds.2014.03.033
Clavenna, A., and Bonati, M. (2009). Adverse Drug Reactions in Childhood: a Review of Prospective Studies and Safety Alerts. Arch. Dis. Child. 94, 724–728. doi:10.1136/adc.2008.154377
Collins, G. E., Clay, M. M., and Falletta, J. M. (1974). A Prospective Study of the Epidemiology of Adverse Drug Reactions in Pediatric Hematology and Oncology Patients. Am. J. Hosp. Pharm. 31, 968–975. doi:10.1093/ajhp/31.10.968
Conyers, R., Devaraja, S., and Elliott, D. (2018). Systematic Review of Pharmacogenomics and Adverse Drug Reactions in Paediatric Oncology Patients. Pediatr. Blood Cancer 65. doi:10.1002/pbc.26937
Dittrich, A. T. M., Draaisma, J. M. T., van Puijenbroek, E. P., and Loo, D. M. W. M. T. (2020). Analysis of Reporting Adverse Drug Reactions in Paediatric Patients in a University Hospital in the Netherlands. Paediatr. Drugs 22, 425–432. doi:10.1007/s40272-020-00405-3
Durrieu, G., Batz, A., Rousseau, V., Bondon-Guitton, E., Petiot, D., and Montastruc, J. L. (2014). Use of Administrative Hospital Database to Identify Adverse Drug Reactions in a Pediatric University Hospital. Eur. J. Clin. Pharmacol. 70, 1519–1526. doi:10.1007/s00228-014-1763-1
Gallagher, R. M., Mason, J. R., Bird, K. A., Kirkham, J. J., Peak, M., Williamson, P. R., et al. (2012). Adverse Drug Reactions Causing Admission to a Paediatric Hospital. PLoS One 7, e50127. doi:10.1371/journal.pone.0050127
Gonzalez-Gonzalez, C., Lopez-Gonzalez, E., Herdeiro, M. T., and Figueiras, A. (2013). Strategies to Improve Adverse Drug Reaction Reporting: a Critical and Systematic Review. Drug Saf. 36, 317–328. doi:10.1007/s40264-013-0058-2
Impicciatore, P., Choonara, I., Clarkson, A., Provasi, D., Pandolfini, C., and Bonati, M. (2001). Incidence of Adverse Drug Reactions in Paediatric In/out-Patients: a Systematic Review and Meta-Analysis of Prospective Studies. Br. J. Clin. Pharmacol. 52, 77–83. doi:10.1046/j.0306-5251.2001.01407.x
Joseph, B., Scott, J. X., and Rajanandh, M. G. (2020). Surveillance of Adverse Drug Reactions and Drug-Drug Interactions with Pediatric Oncology Patients in a South Indian Tertiary Care Hospital. J. Oncol. Pharm. Pract. 26, 1103–1109. doi:10.1177/1078155219882081
Katrak, P., Bialocerkowski, A. E., Massy-Westropp, N., Kumar, S., and Grimmer, K. A. (2004). A Systematic Review of the Content of Critical Appraisal Tools. BMC Med. Res. Methodol. 4, 22. doi:10.1186/1471-2288-4-22
Laatikainen, O., Miettunen, J., Sneck, S., Lehtiniemi, H., Tenhunen, O., and Turpeinen, M. (2017). The Prevalence of Medication-Related Adverse Events in Inpatients-A Systematic Review and Meta-Analysis. Eur. J. Clin. Pharmacol. 73, 1539–1549. doi:10.1007/s00228-017-2330-3
Langerová, P., Vrtal, J., and Urbánek, K. (2014). Adverse Drug Reactions Causing Hospital Admissions in Childhood: a Prospective, Observational, Single-centre Study. Basic Clin. Pharmacol. Toxicol. 115, 560–564. doi:10.1111/bcpt.12264
Le, J., Nguyen, T., Law, A. V., and Hodding, J. (2006). Adverse Drug Reactions Among Children over a 10-year Period. Pediatrics 118, 555–562. doi:10.1542/peds.2005-2429
Lombardi, N., Crescioli, G., Bettiol, A., Marconi, E., Vitiello, A., Bonaiuti, R., et al. (2018). Characterization of Serious Adverse Drug Reactions as Cause of Emergency Department Visit in Children: a 5-years Active Pharmacovigilance Study. BMC Pharmacol. Toxicol. 19, 16. doi:10.1186/s40360-018-0207-4
Makiwane, M., Decloedt, E., Chirehwa, M., Rosenkranz, B., and Kruger, M. (2019). Adverse Drug Reactions in Paediatric In-Patients in a South African Tertiary Hospital. J. Trop. Pediatr. 65, 389–396. doi:10.1093/tropej/fmy067
Mitchell, A. A., Lacouture, P. G., Sheehan, J. E., Kauffman, R. E., and Shapiro, S. (1988). Adverse Drug Reactions in Children Leading to Hospital Admission. Pediatrics 82, 24–29. doi:10.1542/peds.82.1.24
Morales-Ríos, O., Cicero-Oneto, C., García-Ruiz, C., Villanueva-García, D., Hernández-Hernández, M., Olivar-López, V., et al. (2020). Descriptive Study of Adverse Drug Reactions in a Tertiary Care Pediatric Hospital in México from 2014 to 2017. PLoS One 15, e0230576. doi:10.1371/journal.pone.0230576
Munn, Z., Moola, S., Lisy, K., Riitano, D., and Tufanaru, C. (2015). Methodological Guidance for Systematic Reviews of Observational Epidemiological Studies Reporting Prevalence and Cumulative Incidence Data. Int. J. Evid. Based Healthc. 13, 147–153. doi:10.1097/XEB.0000000000000054
Page, M. J., McKenzie, J. E., and Higgins, J. P. T. (2018). Tools for Assessing Risk of Reporting Biases in Studies and Syntheses of Studies: a Systematic Review. BMJ Open 8, e019703. doi:10.1136/bmjopen-2017-019703
Posthumus, A. A., Alingh, C. C., Zwaan, C. C., van Grootheest, K. K., Hanff, L. L., Witjes, B. B., et al. (2012). Adverse Drug Reaction-Related Admissions in Paediatrics, a Prospective Single-centre Study. BMJ Open 2, e000934. doi:10.1136/bmjopen-2012-000934
Queuille, E., Bleyzac, N., Auray, J. P., Bertrand, Y., Souillet, G., Philippe, N., et al. (2001). A New Tool for Evaluation of Medication Errors Applied to Pediatric Hematology. Therapie 56, 775–783.
Ramos, S. F., Alvarez, N. R., dos Santos Alcântara, T., Sanchez, J. M., da Costa Lima, E., and de Lyra Júnior., D. P. (2021). Methods for the Detection of Adverse Drug Reactions in Hospitalized Children: a Systematic Review. Expert Opin. Drug Saf. 20, 1225–1236. doi:10.1080/14740338.2021.1924668
Smyth, R. M., Gargon, E., Kirkham, J., Cresswell, L., Golder, S., Smyth, R., et al. (2012). Adverse Drug Reactions in Children-Aa Systematic Review. PLoS One 7, e24061. doi:10.1371/journal.pone.0024061
Thiesen, S., Conroy, E. J., Bellis, J. R., Bracken, L. E., Mannix, H. L., Bird, K. A., et al. (2013). Incidence, Characteristics and Risk Factors of Adverse Drug Reactions in Hospitalized Children - a Prospective Observational Cohort Study of 6,601 Admissions. BMC Med. 11, 237. doi:10.1186/1741-7015-11-237
Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 169, 467–473. doi:10.7326/M18-0850
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., and Vandenbroucke, J. P.STROBE Initiative. (2007). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Epidemiology 18, 800–804. doi:10.7326/0003-4819-147-8-200710160-0001010.1097/EDE.0b013e3181577654
Workalemahu, G., Abdela, O. A., and Yenit, M. K. (2020). Chemotherapy-Related Adverse Drug Reaction and Associated Factors Among Hospitalized Paediatric Cancer Patients at Hospitals in North-West Ethiopia. Drug Healthc. Patient Saf. 12, 195–205. doi:10.2147/DHPS.S254644
Keywords: pharmacovigilance, adverse drug reactions, pediatrics, hematology, oncology, neoplasms, systematic review
Citation: Amaro-Hosey K, Danés I and Agustí A (2022) Adverse Drug Reactions in Pediatric Oncohematology: A Systematic Review. Front. Pharmacol. 12:777498. doi: 10.3389/fphar.2021.777498
Received: 15 September 2021; Accepted: 22 December 2021;
Published: 03 February 2022.
Edited by:
Eloisa Gitto, University of Messina, ItalyReviewed by:
Ashwin Karanam, Pfizer, United StatesEvelyne Jacqz-Aigrain, Institut National de la Santé et de la Recherche Médicale (INSERM), France
Copyright © 2022 Amaro-Hosey, Danés and Agustí. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Immaculada Danés, aWRAaWNmLnVhYi5jYXQ=