 Susana Ochoa1,2,3,4*
Susana Ochoa1,2,3,4* Victoria Espinosa1,3,4
Victoria Espinosa1,3,4 Raquel López-Carrilero1,3,4Irene Martinez1Alejandro De Haro Barrera1Irene Birulés1,5Ana Barajas6
Raquel López-Carrilero1,3,4Irene Martinez1Alejandro De Haro Barrera1Irene Birulés1,5Ana Barajas6 Trinidad Pélaez1,2
Trinidad Pélaez1,2 Luciana Díaz-Cutraro1,3,4,7Marta Coromina1
Luciana Díaz-Cutraro1,3,4,7Marta Coromina1 Alexandre González-Rodríguez8
Alexandre González-Rodríguez8 Marina Verdaguer-Rodríguez1,3,4,9
Marina Verdaguer-Rodríguez1,3,4,9 Alfonso Gutiérrez-Zotes2,10Carolina Palma-Sevillano7,11Cristian Montes12Judith Gallego13Beatriz Paya14
Alfonso Gutiérrez-Zotes2,10Carolina Palma-Sevillano7,11Cristian Montes12Judith Gallego13Beatriz Paya14 Francesc Casanovas2,15María Roldán15Emma Noval14Paloma Varela Casals11Miriam Salas-Sender13Ana Aznar16Rosa Ayesa-Arriola2,14Esther Pousa2,17
Francesc Casanovas2,15María Roldán15Emma Noval14Paloma Varela Casals11Miriam Salas-Sender13Ana Aznar16Rosa Ayesa-Arriola2,14Esther Pousa2,17 Manuel Canal-Rivero12
Manuel Canal-Rivero12 Nathalia Garrido-Torres12Clara Montserrat15Laura Muñoz-Lorenzo18Josep María Crosas19
Nathalia Garrido-Torres12Clara Montserrat15Laura Muñoz-Lorenzo18Josep María Crosas19  on behalf of Spanish Metacognition Group
on behalf of Spanish Metacognition Group- 1Parc Sanitari Sant Joan de Déu, Sant Boi de Llobregat, Spain
- 2Centro de Investigación Biomédica en Red de Salud Mental, Instituto de Salud Carlos III, Madrid, Spain
- 3Fundació Sant Joan de Déu, Esplugues de Llobregat, Barcelona, Spain
- 4Etiopatogènia i tractament dels trastorns mentals greus (MERITT), Institut de Recerca Sant Joan de Déu, Esplugues de Llobregat, Barcelona, Spain
- 5Facultat de Psicologia Departament de Cognició, Desenvolupament i Psicologia de l'Educació, Universistat de Barcelona, Barcelona, Spain
- 6Departament de Psicologia, Facultat de Psicologia Clínica I de la Salut. Serra Húnter Programme, Universitat Autònoma de Barcelona, Barcelona, Spain
- 7Department of Psychology, FPCEE Blanquerna, Universitat Ramon Llull, Barcelona, Spain
- 8Department of Mental Health, CIBERSAM, Mutua Terrassa University Hospital, Fundació Docència i Recerca Mutua Terrassa, University of Barcelona, Terrassa, Spain
- 9Department of Clinical and Health Psychology, Universitat Autònoma de Barcelona, Cerdanyola del Vallès, Barcelona, Spain
- 10Hospital Universitari Institut Pere Mata, Institut d’Investigació Sanitària Pere Virgili-CERCA, Universitat Rovira i Virgili, Reus, Spain
- 11Hospital de Mataró, Consorci Sanitari del Maresme, Barcelona, Spain
- 12Virgen del Rocío University Hospital, Network Centre for Biomedical Research in Mental Health (CIBERSAM), Institute of Biomedicine of Seville (IBiS), First-episode Psychosis Research Network of Andalusia (Red PEPSur), University of Seville, Seville, Spain
- 13Fundació Vidal i Barraquer, Barcelona, Spain
- 14Department of Psychiatry, Marqués de Valdecilla University Hospital, IDIVAL. School of Medicine, University of Cantabria, Santander, Spain
- 15Hospital del Mar Medical Research Institute (IMIM) of Barcelona, Autonomous University of Barcelona, Barcelona, Spain
- 16Centre d’Higiene Mental Les Corts, Barcelona, Spain
- 17Department of Psychiatry, Hospital de la Santa Creu i Sant Pau, Institut d’Investigació Biomèdica-Sant Pau (IIB-Sant Pau), Barcelona, Spain
- 18Departamento de Psiquiatría, IIS-Fundación Jiménez Díaz, Madrid, Spain
- 19Department of Mental Health, Hospital Universitari Parc Taulí, Institut d’Investigació i Innovació Parc Taulí I3PT, Universitat Autònoma de Barcelona, Sabadell, Catalonia, Spain
Background: More than half of women with psychosis take care of their children despite the difficulties caused by the disease. Additionally, these kids have a higher risk of developing a mental health disorder. However, no interventions have been developed to meet these needs. Metacognitive Training (MCT) is a psychological intervention that has demonstrated its efficacy in improving cognitive insight, symptom management and social cognition in people with first-episode psychosis (FEP). Additionally, MCT has shown better results in women than men with FEP. This study aims to adapt and evaluate the efficacy of MCT-F in mothers and adolescent children in an online group context with the main purpose of improving family relationships, cognitive awareness and symptoms in women with psychosis and increase their children’s knowledge of the disease and their functioning. As secondary objectives, it also aims to evaluate improvements in metacognition, social cognition, symptoms, protective factors and self-perception of stigma.
Materials and methods: A quasi-experimental design with participants acting as their own control will be carried out. Forty-eight mothers with psychosis and their adolescent children (between 12 and 20 years old) recruited from a total of 11 adult mental health care centers will receive MCT-F. Participants will be evaluated 11 weeks before the intervention (T1), at baseline (T2), and post-intervention (T3) with a cognitive insight scale, as a primary outcome. Measures of metacognitive and social cognition, symptoms, cognitive functioning, family and social functioning, protective factors (self-esteem, resilience, and coping strategies) and self-perceived stigma will be addressed as secondary outcomes. Assessment will also address trauma and attachment in mothers and, lastly, the feasibility and acceptability of MCT-F in both participant groups.
Discussion: This will be the first investigation of the efficacy, acceptability, and viability of the implementation of MCT-F. The results of this study may have clinical implications, contributing to improving mothers’ with psychosis and adolescents’ functioning and better understanding of the disease, in addition to the possible protective and preventive effect in adolescents, who are known to be at higher risk of developing severe mental disorders.
Clinical trial registration:https://clinicaltrials.gov/, identifier [NCT05358457].
1 Introduction
1.1 Women and motherhood in schizophrenia and other psychosis
Schizophrenia is a chronic disease with a heterogeneous course. Several factors have been described as influencing the course of the illness, among them, gender has been found to be a determinant factor (Ochoa et al., 2006). Previous research suggests that women with psychosis have fewer admissions to acute psychiatric units and higher frequencies of diagnoses of schizoaffective or delusional disorders than males (Iniesta et al., 2012) as well as a better premorbid adjustment, course of the illness, social functioning, and treatment response than males (Ochoa et al., 2012; Riecher-Rössler et al., 2018; Seeman, 2020). In this line, more than 60% of women with psychosis are married (Usall, 2001), and between 50 and 60% are mothers (McGrath et al., 1999; Howard et al., 2001), which is a similar percentage to that found in women without a mental disorder diagnosis (Haukka et al., 2003).
Although motherhood has been explored in other diagnoses, little has been studied in mothers with schizophrenia and most of them are centered in pregnancy and post-partum, leading to the development of specialized mother-baby units (Wan et al., 2008; Gentile and Fusco, 2019). In previous research, it was found that mothers with schizophrenia express significantly more need in taking care of their children than men (Ochoa et al., 2001). Indeed, a specific instrument was developed for the assessment of their specific needs (CAN-M) (Howard et al., 2007). The difficulties of mothers with schizophrenia could be related to several aspects such as illness severity, problems in reasoning biases, attributional errors and social cognitive impairments, presence of social stressors, self-stigma associated with the illness, and a lack of protective factors to deal with them (Wan et al., 2008). In fact, custody loss is a main fear for many of these mothers (Dolman et al., 2013) and is experienced more often than in parents without mental health problems (Kaplan et al., 2019).
1.2 Adolescent children of mothers with schizophrenia
Adolescence is one of the most difficult and crucial periods in life, when the importance of relating to others and self-reflection is highly present (Weil et al., 2013; Arnett, 2023). Moreover, during adolescence, social cognition-emotional recognition, theory of mind, attributional style, and social perception become instrumental in social relationships and in the development of the social brain (Kilford et al., 2016; Steenhuis et al., 2020). On the other hand, adolescents whose mothers are diagnosed with psychosis have specific challenges. For instance, when a mother has developed psychosis, it can lead to difficulty expressing feelings to their children and the disorder can be treated as a family secret (Cooklin, 2013). However, it is well demonstrated that all children and adolescents need support to understand the disorder in order to avoid developing wrong beliefs and attributions to their mother’s potentially irrational behavior (Riebschleger et al., 2009). With this purpose, Blake et al. (2015) developed a guide for mothers with psychosis and their families with recommendations on how to talk about the illness and avoid experiencing negative states such as anxiety, anger, denial, sadness, and guilt.
Nevertheless, some women with psychosis have difficulty expressing feelings with their children that could derive from those unpredictable life situations and the family setting could become chaotic and confusing (Cudjoe et al., 2023). Aldridge and Becker (2003) found adolescents of mothers with psychosis often assume adult responsibilities. Moreover, they could identify with their mother and became hyper alert to their own behavior due to fears of developing the same symptoms (Cooklin, 2013). Thus, symptoms observed in these children can range from emotional and behavioral problems to cognitive impairments and social difficulties (Radley et al., 2022b), which become more evident in adolescence. Consequently, several studies have emphasized the importance of psychoeducation and coping skills to avoid isolation and promote resilience (Pitman and Matthey, 2004; Riebschleger et al., 2009).
1.3 Psychological interventions for mothers with psychosis and their adolescent children
Around 70% of children living with parents with mental health problems will experience mental health difficulties (Cooklin, 2010). Particularly, the estimated risk of developing schizophrenia is of approximately 10% in individuals who have a parent with psychosis, increasing to 50% if both parents are affected (Hannon et al., 2016). Moreover, Goldstein et al. (2013) reported that the heritability of psychosis is linked to the X chromosome, finding a higher prevalence of maternal history of the mental disorder. In the same line, Barajas et al. (2019) also found higher prevalence of delusions in FEP patients whose mothers have psychosis. This association may be due to genetic aspects, but also to environmental factors such as problems in family dynamics (Cudjoe et al., 2023).
Even though there are several programs addressed to high-risk adolescents, aimed to avoid the transition to psychosis (Schmidt et al., 2015), these are indicated when the adolescent has already presented subclinical symptoms or a decline in functioning. Given the evidence demonstrating the issues that adolescent children of mothers with psychosis face, they should receive interventions before the symptoms or decline in functioning are evident.
Conversely, limited research exists on developing and evaluating interventions specifically tailored to mothers with psychosis and their adolescent children (Wan et al., 2008). Recently, a systematic review (Tapias et al., 2021) aimed to explore psychological interventions addressed to children and adolescents whose parents have a mental disorder suggested that little research has been conducted in this topic. Although some studies included samples of people with psychosis, none of them addressed psychosis interventions and some studies’ samples included less than 5% of people with psychotic disorders. Of those studies, few studies specifically targeted mothers (Rosenblum et al., 2017) or the adolescent period (Pitman and Matthey, 2004; Fraser and Pakenham, 2008). Furthermore, although some interventions include parents and offspring together, only one intervention, kidstime project by Wolpert et al. (2015), included parents with psychosis in their sample. Although only 5 families were included in the study, the results show an improvement in their knowledge of the illness and better relationships in the family. However, interventions focusing solely on psychoeducation about parental mental illness or parenting skills have been shown to be insufficient in improving cognitive biases and social cognition (Wolpert et al., 2015; Marston et al., 2016),
Thus, the evidence of interventions is scarce, and we should highlight two clear deficiencies: (1) the lack of studies focused on mothers with psychosis and (2) the interventions available for mental disorders address increasing knowledge of the illness but none aim to improve errors in cognitive biases, social cognition or self-reflectiveness.
1.4 Metacognitive training for psychosis
Metacognitive training for psychosis (MCT) (Moritz and Woodward, 2007) is a low-threshold approach based on a cognitive behavioral intervention combined with psychoeducation. The intervention is based on a normalizing approach in which those cognitive biases more frequent in people with psychosis are commented on in an illustrative and entertaining way. MCT is freely available in 37 languages1 and other versions of the program have been developed for other disorders (depression, borderline personality and obsessive-compulsive disorders, among others). Studies suggests MCT might be more effective in enhancing cognitive insight compared to cognitive remediation (Balzan et al., 2019) treatment and usual (TAU) (Lam et al., 2015) or psychoeducational interventions (Ochoa et al., 2017; Ahuir et al., 2018). A 3-year follow-up randomized controlled trial involving a 3-year follow-up randomized controlled trial, found that MCT was more effective in improving quality of life and self-esteem compared to an active control group that received cognitive remediation (Moritz et al., 2014). A recent meta-analyze has shown that MCT is effective in reducing positive and negative symptoms and enhance cognitive biases, self-esteem, and functioning (Penney et al., 2022). Additionally, MCT has good acceptability and tolerability (Moritz et al., 2011). The Spanish Metacognition Group has also demonstrated the effectiveness of MCT in people with FEP, finding improvements in cognitive insight, symptoms, social cognition, and irrational beliefs (Ochoa et al., 2017; Birulés et al., 2020; Salas-Sender et al., 2020). Interestingly, it was found that women with psychosis benefited more from the MCT intervention than their male counterparts regarding general symptoms, cognitive insight and social cognition, suggesting that MCT is a gender sensitive intervention (Salas-Sender et al., 2020). Jointly addressing the metacognition of two family members could increase the effectiveness of the intervention, as it allows for the collaborative identification of cognitive biases as well as alternative interpretations and the shared use of intervention tools.
As a result of the COVID-19 pandemic, research has demonstrated the viability of the use of telemedicine to treat people with psychosis (Santesteban-Echarri et al., 2020). Likewise, psychological treatments such as MCT delivered online, may be an attractive intervention to young people as they are familiar with new technologies, and to women clients due to their caregiving responsibilities (Chiauzzi et al., 2020). It is also promising due to potentially becoming a non-stigmatizing way of receiving psychological treatment and its increased cost-effectiveness (Andersson and Titov, 2014; Osma et al., 2022).
To summarize, a personalized intervention addressed to cover the needs of mothers with psychosis in the care of their adolescent children is necessary. These adolescents have a higher risk of developing a mental health disorder, not just due to genetic reasons but also as a result of their family situation. In addition, adolescence is a crucial stage in the development of metacognitive strategies and the sense of self. In this context, MCT-F has the potential for mothers to work together with their adolescent children on metacognitive strategies, while potentially achieving better functioning and greater understanding to one another, thus enhancing the family relationships.
1.5 Study aims
The objective of this study is to evaluate the efficacy of Family Metacognitive Training (MCT-F) in mothers with psychosis and adolescent children in an online group setting to improve family relationships, cognitive insight, symptoms of women with psychosis, and increase their children’s knowledge of the disease. As secondary objectives, we aim to evaluate improvements in metacognition and social cognition, symptoms, protective factors and self-perception of stigma. Finally, we aim to evaluate the feasibility and acceptability of MCT-F in both mothers with psychosis and their adolescent children.
We expect that MCT-F will be effective to improve cognitive insight in mother with psychosis as first hypothesis. As a secondary hypothesis we expect that MCT-F will improvement familiar functioning, metacognition and social cognition variables, as attributional style and Theory of mind, protective factors such as self-esteem, resilience and coping strategies and will decrease self-stigma in mothers. Regarding adolescent children’s participants, we hypothesize that MCT-F will increase children’s knowledge of their mothers’ disease and help them to better understand their mother’s thoughts and their understanding of metacognition and, consequently, to decrease anxiety and depressive symptoms. Furthermore, we expect an improvement in familiar functioning, metacognition and social cognition variables, as well as in protective factors such as: self-esteem, resilience, and coping strategies. More precisely, we expect that all outcomes’ measures will significantly improve from pre- to post-assessment and significant differences when compare with control evaluation. We will control the analysis by cognition functioning, previous trauma and attachment of the mother, presence of the illness before motherhood and attachment of the adolescent with their mother. Finally, we expected that MCT-F Twill be feasible and acceptable to both mothers and their adolescent children.
2 Materials and methods
2.1 Study design and procedure
The study follows a quasi-experimental design with participants acting as their own control. It was approved by the ethic committees of each participating center and by the Research and Ethics Committee of Parc Sanitari Sant Joan de Déu (PSSJD) (coordinating center) and it conforms to the declaration of Helsinki. All participants meeting the inclusion criteria will receive MCT-F. We will conduct three assessments separated by 11 weeks: an initial no-intervention period of eleven weeks (T1), baseline (T2); and post-intervention (T3).
A complete flowchart of the study can be found in Figure 1. All potentially eligible study participants are recruited from March 2024 to May 2024 by their referring mental health professional from the following 11 participating centers of outpatient mental health services: Hospital de la Santa Creu y Sant Pau (Barcelona), Fundación Jiménez Diaz (Madrid), Corporació Sanitària i Universitària Parc Taulí (Sabadell, Barcelona), Centre d’Higiene Mental de Les Corts (Barcelona), Institut Pere Mata (Reus, Tarragona), Hospital Marqués de Valdecillas (Santander), Parc Salut Mar (Barcelona), Hospital de Mataró (Mataró, Barcelona), Fundació Vidal i Barraquer (Barcelona), Hospital Virgen del Rocío (Sevilla), Mutua de Terrassa (Terrasa, Barcelona), and the coordinating center Parc Sanitari Sant Joan de Déu (Sant Boi, Barcelona). All selected mothers are informed of the study objectives and methodology by their referring mental health professional and sign the required informed consent form. In the case of adolescent participants under the age of 18, in addition to their own consent, the consent of their parents, guardians, or legal representatives is obtained. Then, a psychologist from the research team contacts participating mother by telephone to confirm if she and her adolescent child/children accomplish inclusion criteria. After confirmation of their eligibility, they are enrolled in the study. Specific schedules for the administration of the instruments and the data collection procedure are described below.
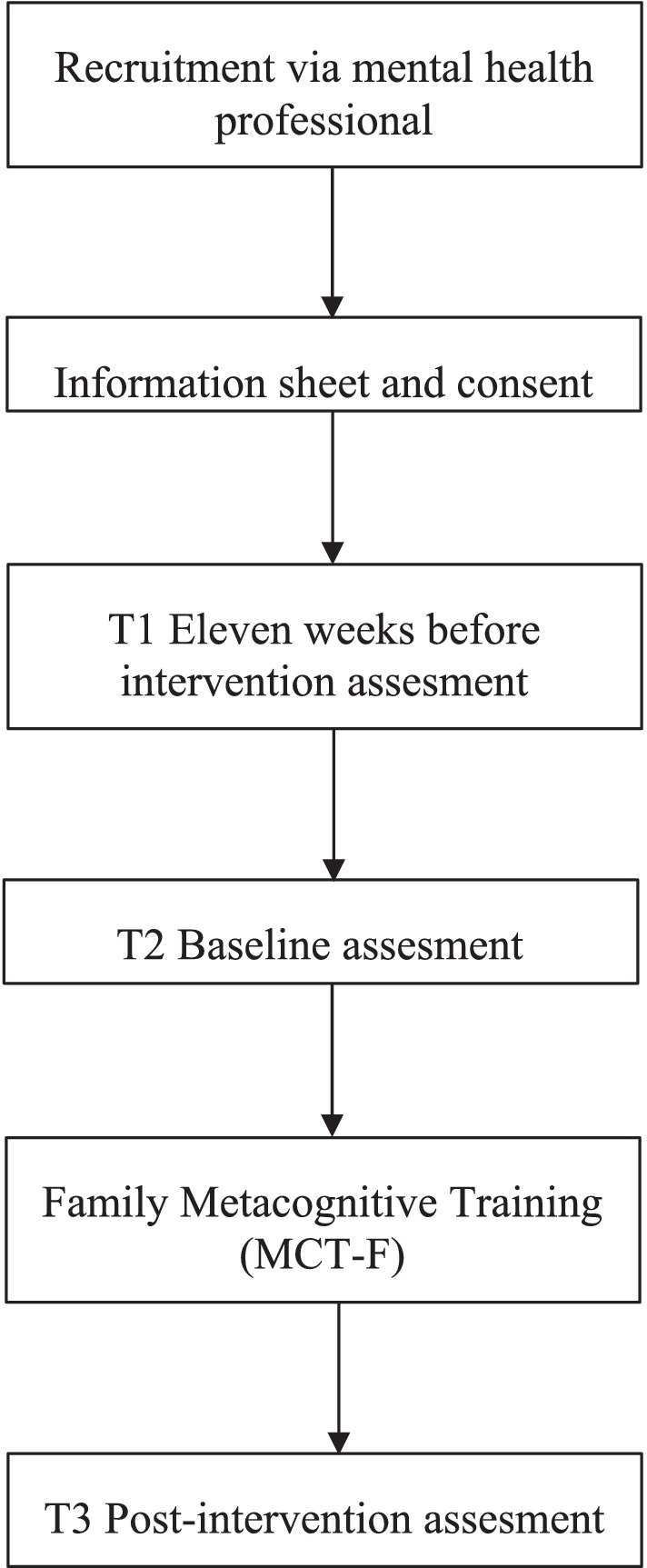
Figure 1. Flowchart of the study.
2.2 Participants
The clinical trial’s sample is comprised of mothers with psychosis with their adolescent children (12–20 years old). Mothers are receiving treatment in one of the outpatient mental health services of the participating groups cited in the previous section.
Inclusion criteria for mother enrolment are as follows: (1) to have a diagnosis of schizophrenia, unspecified psychotic disorder, delusional disorder, schizoaffective disorder, brief psychotic disorder, or schizophreniform disorder (according to DSM-5 criteria); (2) to be a mother to one or more adolescents between 12 and 20 years old; (3) psychopathological stability considering no presence of hospitalization in the previous 3 months.
Exclusion criteria include: (1) to have traumatic brain injury, dementia, or intellectual disability (premorbid IQ ≤ 70); (2) to present PANSS scores ≥5 in hostility, lack of cooperation or suspiciousness, to guarantee a good relationship in the group; (3) to have a substance dependence disorder.
If participant mothers should have more than one adolescent child, all are invited to participate in the study.
Inclusion criteria for adolescents’ enrolment are as follows: (1) to be aged between 12 and 20 years old, (2) to live with their mothers, (3) to be interested in participating in the training with their mothers. The age range of the adolescents in this study was shortened to ensure that they understood and could develop the content of the MCT and also to create age-matched intervention groups of adolescent children.
The exclusion criteria of adolescents include: (1) having a traumatism brain damage or (2) intellectual disability (premorbid IQ ≤ 70).
2.3 Measures
Several domains are assessed with mothers and adolescents.
2.3.1 Mothers’ assessment
2.3.1.1 Mothers’ assessment includes the following instruments
All participants complete a sociodemographic questionnaire (age, educational level, marital status, employment status, diagnosis, pharmacological treatment and other data of interest). The duration of untreated psychosis (DUP) is provided by each patient’s referent psychiatrist and relatives. Diagnosis and treatment are collected from their clinical history. Mothers will be asked about the presence of diagnoses in their adolescent children, and it will be taking into account in the analyses as possible confounder variable.
2.3.1.2 Metacognition and social cognition
- The Beck Cognitive Insight Scale (BCIS) (Beck, 2004; Gutiérrez-Zotes et al., 2012) is a self-administered scale composed of 15 items that assesses cognitive insight, yielding a self-reflectiveness subscale and a self-certainty subscale, as well as a Composite Index score. The coefficient of the self-reflectiveness and self-certainty scores was, respectively, 0.59 and 0.62 for the Spanish validation.
- The Cognitive Bias Questionnaire (CBQ) (Peters et al., 2010; Corral et al., 2021) is used for the assessment of the most frequent cognitive biases in psychotic disorders. This questionnaire has a self-administered format, with 30 descriptions of everyday situations, 15 focused on Anomalous Perceptions (AP) and 15 on Threatening Situations (TS). The subject must choose from three options the one that best describes how he or she would think about the situation. Cronbach’s alpha was 0.87 for the total scale (30 items), 0.76 for the AP scale (15 items), and 0.78 (15 items) for the TE scale for the Spanish version.
- Jumping to Conclusions (JTC) reasoning bias (Garety et al., 1991; Dudley et al., 1997). A Spanish version of the Bead Task translated by the research team is used to assess this common cognitive bias in psychosis. Three trials with different conditions are implemented: a probabilistic trial with an 85/15 ratio, a second probabilistic trial with a 60/40 ratio, and salient tasks. JTC bias is considered present if the decision is taken before the third ball.
- The Ambiguous Intentions Hostility Questionnaire (AIHQ) (Combs et al., 2007) is used to evaluate hostile social-cognitive biases in paranoia. It comprises 15 vignettes of negative interpersonal situations and the participants are asked to answer questions about how they would react in each situation. The AIHQ has demonstrated good levels of internal consistency (alpha = 0.84–0.86). The AIHQ has been recently validated for use in the Spanish context and is currently in the process of publishing.
- The Hinting Task (Corcoran et al., 1995; Gil et al., 2012) measures theory of mind. Participants are given three situation in which a character hints to another and they must guess what the character really means in each situation. This task has demonstrated its efficacy as a reliable instrument for discriminating between patients with schizophrenia and controls and has showed a Cronbach’s alpha of 0.69 in the Spanish validation.
- The Faces Test (Baron-Cohen et al., 1997; Huerta-Ramos et al., 2021) measures facial emotion recognition. A total of 20 pictures of a woman displaying an emotion are shown to the participants. Subjects must choose between two options of which emotion better describes each face shown. Psychometric properties of the Spanish version show a Cronbach’s alpha of 0.75.
- The Situational Feature Recognition Test 2 (SFRT-2) (Corrigan et al., 1996; Gómez-Gastiasoro et al., 2018) assesses social perception in patients with schizophrenia. This assessment tool consists of nine situations (five familiar and four unfamiliar) with 14 options for related or non-related actions and goals (six correct responses and eight distractor items for each feature). The Spanish adaptation of SFRT-2 has demonstrated Cronbach’s alphas ranging from 0.83 to 0.90.
2.3.1.3 Clinical symptoms
-The Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987; Peralta Martín and Cuesta Zorita, 1994) is a structured interview widely used in clinical practice that allows clinical and general symptoms. The PANSS is composed of three subscales: positive (7 items), negative (7 items), and general (16 items), where higher scores indicate higher levels of severity of the symptoms. The PANSS is the most used scale for the assessment of psychotic symptoms. The Cronbach’s alphas for the subscales ranges between 0.72 and 0.80 in the Spanish version.
-The Calgary Depression Scale for Schizophrenia (CDSS) (Addington et al., 1990; Sarró, 2004) is a nine-item structured interview scale that assesses affective symptoms in psychosis. Psychometric properties of the Spanish version show a Cronbach’s alpha of 0.83.
-The Scale of Unawareness of Mental Disorder (SUMD) (Amador et al., 1993; Ruiz et al., 2008) is used to assess awareness of their illness in people with schizophrenia, according to the assessing professional. The scale consists of three general items that evaluates awareness of mental disorder, awareness of the effects of medication and awareness of the social consequences of the disorder; and of 17 items related to specific symptoms, which make up two subscales: awareness and attribution. Good to excellent interrater reliability between evaluators has been reported for the Spanish version, with interclass correlations between 0.82 and 0.91.
2.3.1.4 Social and familiar functioning
- The Family Environmental Scale (FES) (Moos et al., 1974; Fernández-Ballesteros and Sierra, 1989). This questionnaire assesses interpersonal relationships between family members. For this study we use the dimension of family interpersonal relations, composed of 30 items with a true or false response format that measures three dimensions: cohesion (e.g., “In my family, there is a strong feeling of union”), expressiveness (e.g., “At home, we talk openly about whatever we want to discuss”) and conflict (e.g., “Our family members are in conflict with each other”). The Cronbach’s alphas for each dimension are 0.85, 0.80, and 0.86, respectively.-The Satisfaction With Life Scale (SWLS) (Diener et al., 1985; Pons et al., 2000; Muñoz de Arenillas et al., 2010) is a 5-item instrument that assesses the respondent’s degree of satisfaction with their life. The Cronbach’s alpha obtained in the Spanish version is of 0.83.
- The Global Assessment of Functioning (GAF) (Endicott, 1976). This scale measures patients’ general functioning. Clinical and social functioning measures will be included. The validated Spanish version of the DSM-IV was used (American Psychiatric Association, 1996).
2.3.1.5 Protective factors
- The Rosenberg Self-Esteem Scale (RSES) (Martín-Albo et al., 2007) explores through 10 items personal self-esteem understood as feelings of personal worth and self-respect. Cronbach’s alpha for the Spanish version was 0.85.
- The Connor-Davidson Resilience Scale (CD-RISC 10) (Connor and Davidson, 2003; Notario-Pacheco et al., 2011). The 10-item scales assess resilience through three dimensions: self-efficacy-tenacity, personal control and social competence. Cronbach’s alfa for the Spanish version was 0.81.
- The Coping Strategies Inventory (CSI-SF) (Tobin et al., 1989; Cano-García et al., 2007; Tous-Pallarés et al., 2022) is a 16-item questionnaire aimed at measuring the frequency of use of primary coping strategies and the perception of coping self-efficacy. The Spanish version of the CSI-SF has demonstrated good internal consistency, as indicated by a Cronbach’s alpha of 0.86.
- The Self Stigma Questionnaire (SSQ) (Ochoa et al., 2015) assesses self-stigma through 14 items and it has been validated in people with psychosis. The results for the Spanish version indicated good psychometric properties, with Cronbach’s alpha ranging between 0.75 and 0.90.
2.3.1.6 Cognitive functioning
- The Vocabulary subscale from Wechsler Adults Intelligence Scale (WAIS) (Wechsler, 2008) is used to explore premorbid intelligence quotient (IQ) in FEP (González-Blanch et al., 2011). It is a task based on an individual’s general knowledge of linguistic information (phonology and semantics), which has been generally associated with crystallized intelligence.
- The Trail Making Test (TMTA-B) (Reitan, 1958; Sánchez-Cubillo et al., 2009) is a test integrating two parts: part A measures the speed of processing and part B measures mental flexibility. In each test the participant is asked to draw a line between 24 consecutive circles that are randomly arranged on a page. The TMT-A uses all numbers, whereas the TMT-B alternates numbers and letters, requiring the patient to switch between numbers and letters in consecutive order. The score represents the amount of time required to complete the task. The average for the TMT-B is 75 s, with deficiencies noted >273 s for the Spanish version.
- The Screen for Cognitive Impairment in Psychiatry (SCIP) (Purdon, 2005; Pino et al., 2008) assesses cognitive difficulties in patients with severe psychiatric disorders. Spanish version showed an average time for administration of 16.02 (SD = 5.01) and an internal consistency Cronbach’s alpha value of 0.73.
2.3.1.7 Attachment and trauma
-The Psychosis Attachment Measure (PAM) (Berry et al., 2006; Sheinbaum et al., 2013) is a 16-item self-report scale designed to measure adult attachment in people with psychosis. For the Spanish version of the PAM, Cronbach’s alpha coefficients of 0.81 and 0.78 were found for the anxiety and avoidance subscales, respectively.
-The Maltreatment and Abuse Chronology of Exposure Scale (MACE) (Teicher and Parigger, 2015) consists of 52 items that measures severity of exposure to ten types of maltreatment and provides an overall severity score and multiplicity score. Prior to this study, the MACE was adapted and translated into Spanish has been utilized in previous studies (Montoro et al., 2023).
2.3.2 Adolescents’ assessment
Adolescent children assessment includes the following instruments:
All adolescents complete a sociodemographic questionnaire.
2.3.2.1 Metacognitive and social cognition
Adolescents are assessed with the same battery of instruments as their mothers.
2.3.2.2 Clinical symptoms
-The Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997; Fonseca-Pedrero et al., 2011). The 25-item scale provides scores for 5 subscales including emotional symptoms, conduct problems, symptoms of hyperactivity/ inattention, peer problems, and prosocial behavior. In the Spanish version, Cronbach’s alpha ranged from 0.58 (behavioral problems) to 0.71 (emotional symptoms).
2.3.2.3 Social and familiar functioning
Adolescents are assessed with the with the FES as their mothers because it has been validated for the age population.
Satisfaction with Life Scale for Children and Adolecents (SWLS-N) (Diener et al., 1985; Sandín et al., 2015) is an age-downward version of the measure of life satisfaction developed by Diener. It is a 5-item, self-report instrument in which respondents are asked to indicate the degree to which t are satisfied each statement is true of their satisfaction with their life. The Spanish version of SWLS scale has demonstrated an alpha de Cronbach of 0.89 (García-Escalera et al., 2017).
The Children’s Global Assessment Scale (CGAS) (Shaffer, 1983) is an adaptation of the Global Assessment Scale (GAS) that assesses the level of functioning for a child or adolescent during a specified time period. It consists of a single score that ranges from 1 (most impaired) to 100 (healthiest). The CGAS has obtained good levels of reliability, with diagnostic agreement values between judges (kappa coefficient) higher than 0.90 (Santamarina-Perez et al., 2020).
2.3.2.4 Protective factors
Adolescents are assessed with the same battery of instruments as their mothers. These instruments have been validated for the age population, except for the Self-Stigma Questionnaire (SSQ), which is not administered.
2.3.2.5 Attachment
- The short version of Cartes, Modèles Indivuels de Relation (CaMir-R) (Balluerka et al., 2011) is a questionnaire aimed at measuring attachment cognitions. It is based on the subjects’ evaluations of past and present attachment experiences and family functioning. The Spanish version of the CaMir-R has demonstrated good internal consistency, as indicated by a Cronbach’s alpha of 0.81.
2.3.2.6 Cognitive functioning
- The Vocabulary subscale from Wechsler Adults Intelligence Scale (WAIS) (Wechsler, 2008) is used to explore the premorbid intelligence quotient (IQ) in adolescents aged 16 years or older. For those participants younger than 16, the Vocabulary subscale of the Wechsler Intelligence Scale for Children (Wechsler, 2014) is used.
- The Matrix Reasoning Task of the Wechsler Intelligence Scale for Children (Wechsler, 2008, 2014) measures visual processing and abstract, spatial perception.
- The Trail Making Test (TMTA-B) (Reitan, 1958; Sánchez-Cubillo et al., 2009) is applied using scales from the age range of the study.
2.3.2.7 Feasibility and acceptability
All mothers and adolescent’s participants are also asked about the perceived value and usefulness of the intervention and the delivery format through a brief self-reported questionnaire divided into two parts. The first part consists of 8 generic items on an 11-point Likert scale from 0 (“not at all”) to 10 (“completely”). The second part consists of 8 short open-ended questions. Finally, we will evaluate the impact of the program’s aim to increase adolescent children’s knowledge of their mothers’ disease with the following items: “To what extent do you feel you understand your mom’s disease before participating in the training?” and “To what extent do you feel you understand your mom’s disease after participating in the training?” with Likert-type response options (from 0 “Not at all” to 5 “Completely”).
In addition, after each session participants are asked to answer two questions to measure the perceived usefulness and enjoyment of each module: “How much did you enjoy it?” and “How useful did you find it?”
2.4 Data collection
Assessments are conducted at the three afore mentioned time points. Evaluators have been trained in psychological evaluation. The neuropsychological assessment will be carried out in the presence of the participants. The rest of the assessment will be conducted on another day and online to increase the feasibility and prevent fatigue due to the large number of assessment instruments. The assessment of the mother and the adolescent will be conducted separately but the same evaluator. Instruments used in each evaluation and the corresponding informant (mother or adolescent) is reported in Table 1. Types and dosages of the mothers’ medication as well as attendance to psychological and/or pharmacological treatment for the adolescent children will be recorded at the three time points of assessment.
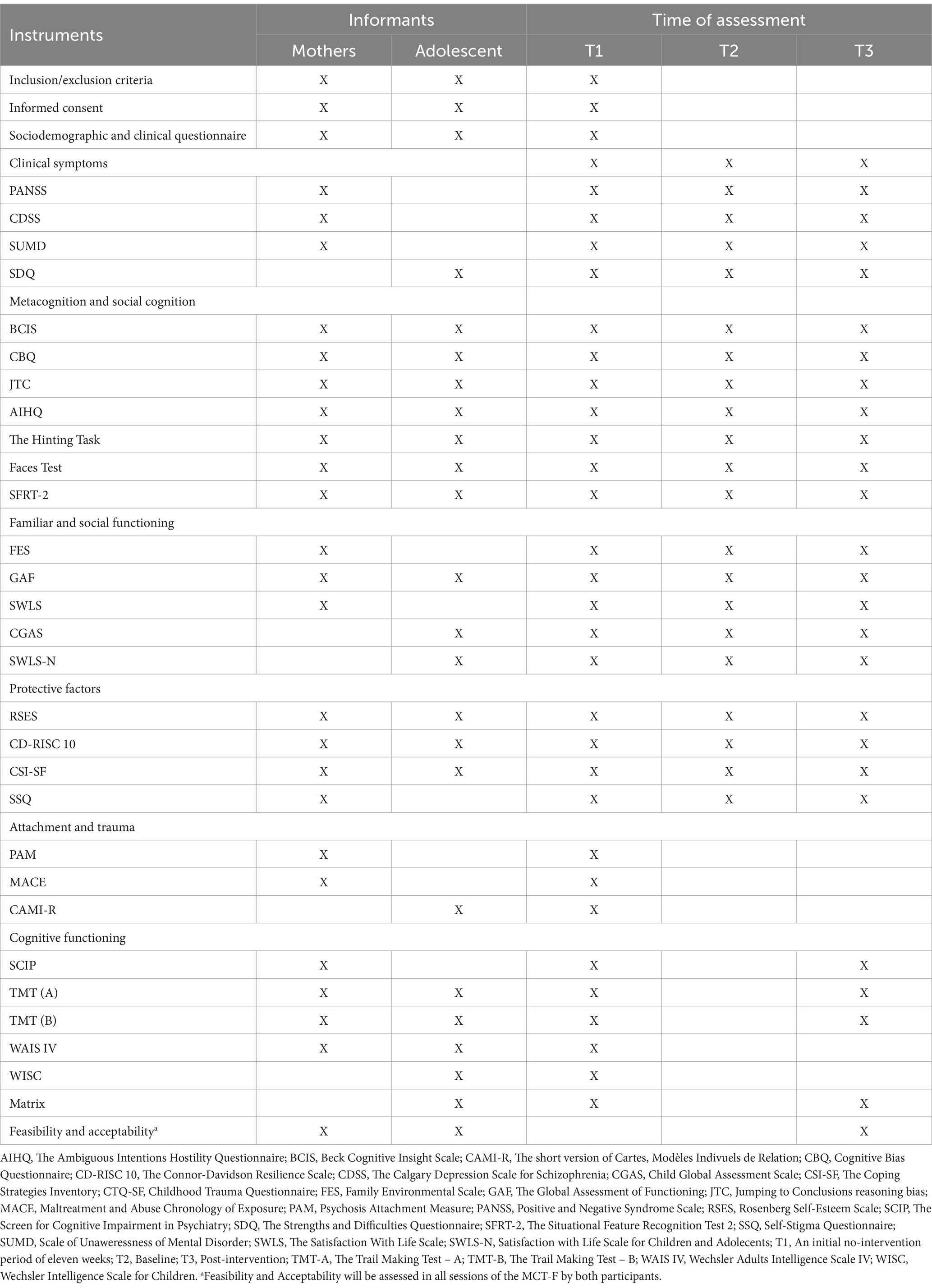
Table 1. Measures used in the study with mothers and their adolescent children.
2.5 Interventions
The intervention consists of an adaptation of classical MCT to a family setting (MCT-F), that is, for mothers with psychosis and their adolescent children in a group setting with other peers. Metacognitive training for psychosis is a psychological intervention that combines psychoeducation with a cognitive behavioral intervention in a metacognitive approach (Moritz and Woodward, 2007). It consists of a normalizing approach to work on cognitive biases which present in the general population but that are more prevalent in people with psychosis, as they are involved in the appearance and maintenance of delusions (Freeman, 2007; Moritz and Woodward, 2007).
Before the quasi-experimental study, a first stage consisted of adapting MCT to this population using the first six steps of the ADAPT-ITT method through a participatory approach, which included the first-person perspective and involved qualitative and quantitative methods. While the core components of the original MCT intervention were retained, patients, relatives, adolescents, and experts participated to ensure that MCT-F was appropriate and acceptable (Espinosa et al., 2024).
The final version of MCT-F consists of 11 online weekly group sessions lasting 60 min. The groups will be composed of 3–4 mothers with psychosis, their adolescent children and two therapists. This group size is large enough to allow for some participants’ absence from sessions without leaving those attending feeling exposed. It is also manageable for two facilitators. Furthermore, participants will be allocated to their groups based on the teenagers’ ages (aged 12–16 and 16–20) to adapt examples and vocabulary and so they feel more comfortable sharing experiences. Mothers and adolescents will be able to attend sessions from the same room or from separate places, to facilitate attendance and the intimacy of both participating groups. Therapists will also be local community references to the participating mothers to enhance adherence and assure the inclusion of the study’s information in their clinical records. Although there is no minimum number of group sessions that participants must attend, the attendance of each participant will be recorded.
The material available to use during MCT-F is made up of power-point presentations. Each module contains therapeutic material including psychoeducational information, exercises, case examples and demonstrations. The first session is added as a psychoeducation session to explain the psychotic illness, metacognition, and training objectives. Seven of the therapeutic modules address cognitive bias and errors that are frequently seen in problem-solving in psychosis. The other two modules work with depression, self-esteem, and self-stigma. Lastly, we added an additional session, after third session, with mothers and adolescent children attending separately to facilitate speaking openly about feelings or concerns without their relatives.
All mother participants will also receive their treatment as usual (TAU). In order to account for differences in TAU over the different centers the mothers participate in, we will collect the specific treatment characteristics of the TAU offered in each institution.
2.6 Sample size calculation
Taking as a reference previous data on effectiveness of MCT in women samples (Salas-Sender et al., 2020), the sample size necessary for the study to have adequate power has been estimated. With an alpha of 0.05, a power of 0.90, a difference between pre-treatment and post-treatment in cognitive insight (self-certainty) of 2 points in the intervention vs. −0.48 in the control, and with a SD of 4.14 in the reference group, as well as considering possible losses of 25%, the final sample calculation is estimated to be of 48 mothers (with their respective children) in total.
2.7 Data analysis
The main analysis variable will involve the difference between scores in the control assessment and intervention assessment for the cognitive insight assessed in the mothers with psychosis. Secondary outcomes will be the changes in other assessments of metacognition and social cognition variables, familiar and social functioning, cognitive distortions, cognitive functioning, protective factors, and self-stigma.
The changes in the cognitive insight scales’ scores will be analyzed using repeated measures regression methods. Changes in the scores of symptoms, metacognition and social cognition, social functioning, understanding of the disease, self-esteem, resilience and coping strategies in adolescent children will be analyzed using repeated measures regression methods, with the final score of the scale as the dependent variable. Two additional analyses will be carried out to examine the robustness of the results. First, the intention-to-treat analysis will be performed after replacing missing values for the dropout cases using the method “last observation carried forward” (LOCF). Next, the analyses will be performed only with data from participants who complete the treatment and who have been evaluated at both time points. Finally, the satisfaction of patients undergoing group treatment will also be analyzed.
All the analyses will be controlled by medication changes, cognitive functioning, attachment, trauma, start of the illness before motherhood and type of TAU (in mothers), and the presence of mental disorders or attendance to psychological and/or pharmacological treatment (in adolescents).
3 Discussion
To our knowledge, this is the first study aiming to adapt and assess the effectiveness of Family Metacognitive Training (MCT-F) in a sample of mothers with psychosis and their adolescent children. We will also evaluate the feasibility and acceptability of the adapted intervention. It is novel in this context, in that not only does it address patient symptoms and cognitive awareness, but also the family relationship. It also aims to improve the children’s understanding of the disease and their functioning. As secondary objectives, MCT-F is seeking to increase metacognition and social cognition, improve symptoms, protective factors, and self-perception of stigma in both family members.
Considering the efficacy of MCT in women with first-episode psychosis (Ochoa et al., 2017), we similarly expect mothers with psychosis who receive MCT-F will improve in cognitive insight, as well as symptoms and other metacognitive and social cognition measures. In addition, women with FEP have shown better responses to psychological interventions, not only in terms of improvements but in compliance and motivation, so we expect the results in these mothers to be even better (Villeneuve et al., 2010). Additionally, we hypothesize that mothers that receive MCT-F will increase their familial and social functioning, and protective factors such as self-esteem, resilience and coping strategies, and will see reductions in self-stigma. MCT (Moritz and Woodward, 2007) focuses on different cognitive biases, social cognition variables (ToM, emotional perception, and attribution bias), depressed mood and low self-esteem in paranoid ideation. All these aspects can help mothers by offering them alternative ways of interpreting situations and experiences, while reducing social cognition difficulties by improving their ability to understand their children’s mental states.
Although no previous research has been done in the lines of the present study, other interventions involving children of parents with other mental disorders found that psychoeducation improves depressive symptoms, familiar functioning, understanding of the parent’s disorder, resilience and coping strategies (Tapias et al., 2021). We hypothesize that this intervention could be equally helpful to the adolescents, to better understand their mother’s thoughts and their understanding of metacognition and, consequently, to decrease anxiety and depressive symptoms. Furthermore, we expect an increase in familiar and social functioning, as well as in protective factors such as self-esteem, resilience and coping strategies. While there is a gap in study of metacognition and social cognition in the adolescent population (Tapias et al., 2021), we have found evidence for different social cognitive and metacognitive affectations as a function of having a mother or a father with a history of mental illness (Mendoza-García et al., 2022). Thus, we consider high-risk adolescents may benefit from the group MCT-F and improve in these areas.
Some features of the present study can be considered assets. First of all, it contributes to the still scarce literature on the efficacy of psychological intervention for mothers with psychosis and their adolescent children. A second strength of our study is the participatory nature of the adaptation process which involved patients, relatives, adolescents, mental health professionals and researchers. Using a variety of methods (e.g., consensus group discussions, interviews, desk reviews), we triangulated data to inform evidence-based adaptations. Thirdly, contrary to most similar studies aiming to evaluate the efficacy of these interventions (Radley et al., 2022c), this study will assess feasibility and acceptability not only in mothers, but also in the adolescent children. Furthermore, from our point of view, evaluating the impact of familiar interventions on metacognition and social cognition, in addition to traditional clinical variables, cognition functioning, protective factors and self-stigma perception is also especially important to consolidate this approach as an effective therapy. Finally, MCT-F has the advantages of an online-based treatment, including better cost-effectiveness and addressing current barriers to access mental health services in a non-stigmatizing way. Further, it adds the benefit of encouraging the recruitment of patients residing in remote areas without specialized care resources.
Once MCT-F’s clinical utility is confirmed, these findings will have important clinical implications. First, the availability of psychological therapy would help these families to deal with these cognitive distortions that are more present in the disease and that have therefore the exacerbation of symptoms and problems in social and family relationships (Radley et al., 2022a). Thus, an intervention such as MCT-F targeting symptoms, social cognition, and metacognition difficulties could improve mothers’ awareness of their children’s mental states and difficulty in providing adequate care to them and, consequently, prevent loss of custody. On the other hand, working on the presence of these cognitive distortions in a normalized way in those high-risk adolescents can be useful as a preventive approach to avoid the appearance of these distortions and consequently the symptoms associated with schizophrenia (Riches et al., 2019; Seeman, 2021).
Study limitations must also be acknowledged. The main limitations of the present study are the lack of a comparison group and the small sample size. A quasi-experimental design was chosen given that impairments in recruiting and retaining people with psychosis and their families are well-established in previous research, potentially biasing clinical research samples (Polillo et al., 2021). Additionally, the comprehensive assessment included, encompassing numerous scales and questionnaires, may impact the quality of participant responses and affect the results. To address this, the assessment will be conducted in different sessions, featuring varied questions and assessments to sustain participant engagement. Another limitation of the study is the potential difficulty isolating the impact of MCT-F on outcome measures. We expect that participants acting as their own control and the statistical analyses mentioned above can increase the robustness of the study results and address these limitations. In addition, the online design nature of this trial may encourage adherence, as it allows a better adjustment to adolescents’ school schedules and the use of new technologies is well accepted by them. To confirm this, we will collect the participants’ rate of attendance to control for this variable. However, the use of online modality could also reinforce family secrecy or feelings of isolation. Also, the absence of inclusion of other family members (e.g., the other caregiver) may hinder changes in the environment. In this sense, this pilot study would be the first step toward obtaining preliminary data.
If the results of this study show that MCT-F is effective, the next steps will include larger sample sizes, follow-up periods, comparison of face-to-face and online modalities, exploration of active or passive control conditions to be able to clearly attribute effects to MCT-F, and potentially adding more peer groups sessions (where mothers and adolescent children attend separately) or other family member (such as co-parent). Finally, as there appears to be a growing tendency for men with psychosis to become fathers, we also consider that fathers with psychosis could especially benefit from MCT-F which can be explored in future trials.
4 Conclusion
To summarize, a personalized intervention addressed to meet the needs of women in care of their adolescent children is necessary. Currently no therapy along these lines has been designed or evaluated worldwide. Should Family Metacognitive Training prove effective for mothers with psychosis and their adolescent children, it could contribute to expanding the psychotherapeutic approaches available for these families. MCT-F could both help to understand one another and to deal with daily problems for both family members, while also improving symptoms in mothers and decrease their children’s higher risk of developing mental disorders.
Ethics statement
This study has been evaluated and approved by each of the Ethics Committees of the participating centers. This clinical trial has been registered (clinicaltrials.gov) (identifier: NCT05358457). All participants are being provided with an information sheet explaining the objectives and procedure of the study as well as the confidentiality of the data collected. All participants will be asked in writing for their consent in accordance with the Declaration of Helsinki and Law 14/2007 on Biomedical Research.
Author contributions
SO: Writing – original draft, Writing – review & editing, Funding acquisition, Investigation, Project administration, Supervision. VE: Writing – original draft, Writing – review & editing, Methodology. RL-C: Writing – review & editing, Conceptualization, Methodology. IM: Writing – original draft. AHB: Writing – original draft. IB: Writing – review & editing. AB: Writing – review & editing. TP: Writing – review & editing. LD-C: Writing – review & editing. MC: Writing – review & editing. AG-R: Writing – review & editing. MV-R: Writing – review & editing. AG-Z: Writing – review & editing. CP-S: Writing – review & editing. CrM: Writing – review & editing. JG: Writing – review & editing. BP: Writing – review & editing. FC: Writing – review & editing. MR: Writing – review & editing. EN: Writing – review & editing. PV: Writing – review & editing. MS-S: Writing – review & editing. AA: Writing – review & editing. RA-A: Writing – review & editing. EP: Writing – review & editing. MC-R: Writing – review & editing. NG-T: Writing – review & editing. ClM: Writing – review & editing. LM-L: Writing – review & editing. JC: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Spanish Ministry of Health Carlos III (PI21/00012) and the Fondo Europeo de Desarrollo Regional (FEDER).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
Addington, D., Addington, J., and Schissel, B. (1990). A depression rating scale for schizophrenics. Schizophr. Res. 3, 247–251. doi: 10.1016/0920-9964(90)90005-R
Ahuir, M., Cabezas, Á., Miñano, M. J., Algora, M. J., Estrada, F., Solé, M., et al. (2018). Improvement in cognitive biases after group psychoeducation and metacognitive training in recent-onset psychosis: a randomized crossover clinical trial. Psychiatry Res. 270, 720–723. doi: 10.1016/J.PSYCHRES.2018.10.066
Aldridge, J., and Becker, S. (2003). The effects of mental illness on parents and relationships with their children. Bristol: The Policy Press. Available at: https://bristoluniversitypressdigital.com/display/book/9781847425676/ch002.xml
Amador, X. F., Strauss, D. H., Yale, S. A., Flaum, M. M., Endicott, J., and Gorman, J. M. (1993). Assessment of insight in psychosis. Am. J. Psychiatry 1, 873–879. doi: 10.1176/ajp.150.6.873
American Psychiatric Association (1996). Manual Diagnóstico y Estadístico de los Trastornos Mentales DSM-IV. Barcelona, Spain: Masson.
Andersson, G., and Titov, N. (2014). Advantages and limitations of internet-based interventions for common mental disorders. World Psychiatry 13, 4–11. doi: 10.1002/WPS.20083
Arnett, J. J. (2023). Emerging adulthood: the winding road from the late teens through the twenties. Available at: https://books.google.com/books/about/Emerging_Adulthood.html?hl=es&id=tFTfEAAAQBAJ
Balluerka, N., Lacasa, F., Gorostiaga, A., Muela, A., and Pierrehumbert, B. (2011). Versión reducida del cuestionario CaMir (CaMir-R) para la evaluación del apego. Psicothema 23, 486–494.
Balzan, R. P., Mattiske, J. K., Delfabbro, P., Liu, D., and Galletly, C. (2019). Individualized metacognitive training (MCT+) reduces delusional symptoms in psychosis: a randomized clinical trial. Schizophr. Bull. 45, 27–36. doi: 10.1093/SCHBUL/SBY152
Barajas, A., Pelaez, T., González, O., Usall, J., Iniesta, R., Arteaga, M., et al. (2019). Predictive capacity of prodromal symptoms in first-episode psychosis of recent onset. Early Interv. Psychiatry 13, 414–424. doi: 10.1111/EIP.12498
Baron-Cohen, S., Wheelwright, S., and Jolliffe, T. (1997). Is there a “language of the eyes”? Evidence from normal adults, and adults with autism or Asperger syndrome. Vis. Cogn. 4, 311–331. doi: 10.1080/713756761
Beck, A. (2004). A new instrument for measuring insight: the Beck cognitive insight scale. Schizophr. Res. 68, 319–329. doi: 10.1016/S0920-9964(03)00189-0
Berry, K., Wearden, A., Barrowclough, C., and Liversidge, T. (2006). Attachment styles, interpersonal relationships and psychotic phenomena in a non-clinical student sample. Personal. Individ. Differ. 41, 707–718. doi: 10.1016/j.paid.2006.03.009
Birulés, I., López-Carrilero, R., Cuadras, D., Pousa, E., Barrigón, M. L., Barajas, A., et al. (2020). Cognitive insight in first-episode psychosis: changes during metacognitive training. J. Person. Med. 10, 1–13. doi: 10.3390/JPM10040253
Blake, P., Collins, A., and Seeman, M. V. (2015). Women and psychosis: an information guide Centre for Addiction and Mental Health. Available at: https://www.camh.ca/-/media/health-info-files/guides-and-publications/women-and-psychosis-en.pdf
Cano-García, F., Rodríguez-Franco, L., and Garcia-Martínez, J. (2007). Adaptación Española del Inventario de Estrategias de Afrontamiento. Actas Espa. Psiquiatr. 35, 29–39.
Chiauzzi, E., Clayton, A., and Huh-Yoo, J. (2020). Videoconferencing-based Telemental health: important questions for the COVID-19 era from clinical and patient-centered perspectives. JMIR Ment Health 2020 7:E24021. doi: 10.2196/24021
Combs, D. R., Penn, D. L., Wicher, M., and Waldheter, E. (2007). The ambiguous intentions hostility questionnaire (AIHQ): a new measure for evaluating hostile social-cognitive biases in paranoia. Cogn. Neuropsychiatry 12, 128–143. doi: 10.1080/13546800600787854
Connor, K. M., and Davidson, J. R. T. (2003). Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 18, 76–82. doi: 10.1002/da.10113
Cooklin, A. (2010). “Living upside down”: being a young carer of a parent with mental illness. Adv. Psychiatr. Treat. 16, 141–146. doi: 10.1192/APT.BP.108.006247
Cooklin, A. (2013). Promoting children’s resilience to parental mental illness: engaging the child’s thinking. Adv. Psychiatr. Treat. 19, 229–240. doi: 10.1192/APT.BP.111.009050
Corcoran, R., Mercer, G., and Frith, C. D. (1995). Schizophrenia, symptomatology and social inference: investigating “theory of mind” in people with schizophrenia. Schizophr. Res. 17, 5–13. doi: 10.1016/0920-9964(95)00024-G
Corral, L., Labad, J., Ochoa, S., Cabezas, A., Muntané, G., Valero, J., et al. (2021). Cognitive biases questionnaire for psychosis (CBQp): Spanish validation and relationship with cognitive insight in psychotic patients. Front. Psych. 11:596625. doi: 10.3389/fpsyt.2020.596625
Corrigan, P. W., Silverman, R., Stephenson, J., Nugent-Hirschbeck, J., and Buican, B. J. (1996). Situational familiarity and feature recognition in schizophrenia. Schizophr. Bull. 22, 153–161. doi: 10.1093/schbul/22.1.153
Cudjoe, E., Tam, C. H. L., Effah, D., Amegashie, E. F., and Tweneboah, A. O. (2023). Living with parental mental illness is like a roller coaster: reflections on children’s lifeworld in the family setting. J. Clin. Nurs. 32, 3516–3527. doi: 10.1111/jocn.16417
Diener, E., Emmons, R. A., Larsen, R. J., and Griffin, S. (1985). The satisfaction with life scale. J. Pers. Assess. 49, 71–75. doi: 10.1207/s15327752jpa4901_13
Dolman, C., Jones, I., and Howard, L. M. (2013). Pre-conception to parenting: a systematic review and meta-synthesis of the qualitative literature on motherhood for women with severe mental illness. Arch. Womens Ment. Health 16, 173–196. doi: 10.1007/s00737-013-0336-0
Dudley, R. E. J., John, C. H., Young, A. W., and Over, D. E. (1997). Normal and abnormal reasoning in people with delusions. Br. J. Clin. Psychol. 36, 243–258. doi: 10.1111/j.2044-8260.1997.tb01410.x
Endicott, J. (1976). The global assessment scale. Arch. Gen. Psychiatry 33:766. doi: 10.1001/archpsyc.1976.01770060086012
Espinosa, V., Arin-González, P., Jiménez-Lafuente, A., Pardo, N., López-Carrilero, R., Birulés, I., et al. (2024). Family metacognitive training (MCT-F): adapting MCT to mothers with psychosis and their adolescent children. Behav. Sci. 14:97. doi: 10.3390/bs14020097
Fernández-Ballesteros, R., and Sierra, B. (1989). Escalas de Clima Social FES, WES, CIES y CES. Madrid: TEA.
Fonseca-Pedrero, E., Paino, M., Lemos-Giráldez, S., and Muñiz, J. (2011). Prevalencia de la sintomatología emocional y comportamental en adolescentes españoles a través del strengths and difficulties questionnaire (SDQ) = prevalence of emotional and behavioral symptoms in spanish adolescents using the strengths and difficulties questionnaire (SDQ) (SDQ). Rev. Psicopatol. Psicol. Clín. 16:17. doi: 10.5944/rppc.vol.16.num.1.2011.10348
Fraser, E., and Pakenham, K. I. (2008). Evaluation of a resilience-based intervention for children of parents with mental illness. Aust. N. Z. J. Psychiatry 42, 1041–1050. doi: 10.1080/00048670802512065
Freeman, D. (2007). Suspicious minds: the psychology of persecutory delusions. Clin. Psychol. Rev. 27, 425–457. doi: 10.1016/J.CPR.2006.10.004
García-Escalera, J., Valiente, R. M., Chorot, P., Ehrenreich-May, J., Kennedy, S. M., and Sandín, B. (2017). The Spanish version of the unified protocol for Transdiagnostic treatment of emotional disorders in adolescents (UP-A) adapted as a school-based anxiety and depression prevention program: study protocol for a cluster randomized controlled trial. JMIR Res. Protoc. 6:e149. doi: 10.2196/resprot.7934
Garety, P. A., Hemsley, D. R., and Wessely, S. (1991). Reasoning in deluded schizophrenic and paranoid patients. J. Nerv. Ment. Dis. 179, 194–201. doi: 10.1097/00005053-199104000-00003
Gentile, S., and Fusco, M. L. (2019). Schizophrenia and motherhood. Psychiatry Clin. Neurosci. 73, 376–385. doi: 10.1111/PCN.12856/FULL
Gil, D., Fernández-Modamio, M., Bengochea, R., and Arrieta, M. (2012). Adaptación al español de la prueba de teoría de la mente Hinting Task. Rev. Psiquiatr. Salud Ment. 5, 79–88. doi: 10.1016/j.rpsm.2011.11.004
Goldstein, J. M., Cherkerzian, S., Tsuang, M. T., and Petryshen, T. L. (2013). Sex differences in the genetic risk for schizophrenia: history of the evidence for sex-specific and sex-dependent effects. Am. J. Med. Genet. B Neuropsychiatr. Genet. 162, 698–710. doi: 10.1002/AJMG.B.32159
Gómez-Gastiasoro, A., Peña, J., Zubiaurre-Elorza, L., Ibarretxe-Bilbao, N., and Ojeda, N. (2018). Spanish adaptation and validation of the situational feature recognition test 2 (SFRT-2) in patients with schizophrenia and healthy controls. Psychiatry Res. 270, 225–231. doi: 10.1016/j.psychres.2018.09.051
González-Blanch, C., Pérez-Iglesias, R., Rodríguez-Sánchez, J. M., Pardo-García, G., Martínez-García, O., Vázquez-Barquero, J. L., et al. (2011). A digit symbol coding task as a screening instrument for cognitive impairment in first-episode psychosis. Arch. Clin. Neuropsychol. 26, 48–58. doi: 10.1093/arclin/acq086
Goodman, R. (1997). The strengths and difficulties questionnaire: a research note. J. Child Psychol. Psychiatry Allied Discip. 38, 581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x
Gutiérrez-Zotes, J. A., Valero, J., Cortés, M. J., Labad, A., Ochoa, S., Ahuir, M., et al. (2012). Adaptación española de la Escala de Insight Cognitivo de Beck (EICB) en esquizofrénicos. Actas Esp. Psiquiatr. 40, 2–9.
Hannon, E., Dempster, E., Viana, J., Burrage, J., Smith, A. R., Macdonald, R., et al. (2016). An integrated genetic-epigenetic analysis of schizophrenia: evidence for co-localization of genetic associations and differential DNA methylation. Genome Biol. 17:176. doi: 10.1186/s13059-016-1041-x
Haukka, J., Suvisaari, J., and Lönnqvist, J. (2003). Fertility of patients with schizophrenia, their siblings, and the general population: a cohort study from 1950 to 1959 in Finland. Am. J. Psychiatry 160, 460–463. doi: 10.1176/APPI.AJP.160.3.460
Howard, L., Hunt, K., Slade, M., O’Keane, V., Senevirante, T., Leese, M., et al. (2007). Assessing the needs of pregnant women and mothers with severe mental illness: the psychometric properties of the Camberwell assessment of need - mothers (CAN-M). Int. J. Methods Psychiatr. Res. 16, 177–185. doi: 10.1002/mpr.227
Howard, L. M., Kumar, R., and Thornicroft, G. (2001). Psychosocial characteristics and needs of mothers with psychotic disorders. Br. J. Psychiatry 178, 427–432. doi: 10.1192/bjp.178.5.427
Huerta-Ramos, E., Ferrer-Quintero, M., Gómez-Benito, J., González-Higueras, F., Cuadras, D., Del Rey-Mejías, A. L., et al. (2021). Translation and validation of Baron Cohen’s face test in a general population from Spain. Actas Espan. Psiquiatr. 49, 106–113.
Iniesta, R., Ochoa, S., and Usall, J. (2012). Gender differences in service use in a sample of people with schizophrenia and other psychoses. Schizophr. Res. Treat. 2012, 1–6. doi: 10.1155/2012/365452
Kaplan, K., Brusilovskiy, E., O’Shea, A. M., and Salzer, M. S. (2019). Child protective service disparities and serious mental illnesses: results from a national survey. Psychiatr. Serv. 70, 202–208. doi: 10.1176/APPI.PS.201800277
Kay, S. R., Fiszbein, A., and Opler, L. A. (1987). The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 13, 261–276. doi: 10.1093/schbul/13.2.261
Kilford, E. J., Garrett, E., and Blakemore, S. J. (2016). The development of social cognition in adolescence: an integrated perspective. Neurosci. Biobehav. Rev. 70, 106–120. doi: 10.1016/j.neubiorev.2016.08.016
Lam, K. C. K., Ho, C. P. S., Wa, J. C., Chan, S. M. Y., Yam, K. K. N., Yeung, O. S. F., et al. (2015). Metacognitive training (MCT) for schizophrenia improves cognitive insight: a randomized controlled trial in a Chinese sample with schizophrenia spectrum disorders. Behav. Res. Ther. 64, 38–42. doi: 10.1016/j.brat.2014.11.008
Marston, N., Stavnes, K., Van Loon, L. M. A., Drost, L. M., Maybery, D., Mosek, A., et al. (2016). A content analysis of intervention key elements and assessments (IKEA): What’s in the black box in the interventions directed to families where a parent has a mental illness? Child Youth Serv. 37, 112–128. doi: 10.1080/0145935X.2016.1104041
Martín-Albo, J., Núñez, J. L., Navarro, J. G., and Grijalvo, F. (2007). The Rosenberg self-esteem scale: translation and validation in university students. Span. J. Psychol. 10, 458–467. doi: 10.1017/S1138741600006727
McGrath, J. J., Hearle, J., Jenner, L., Plant, K., Drummond, A., and Barkla, J. M. (1999). The fertility and fecundity of patients with psychoses. Acta Psychiatr. Scand. 99, 441–446. doi: 10.1111/J.1600-0447.1999.TB00990.X
Mendoza-García, S., García-Mieres, H., Lopez-Carrilero, R., Sevilla-Llewellyn-Jones, J., Birulés, I., Barajas, A., et al. (2022). Influence of maternal and paternal history of mental health in clinical, social cognition and metacognitive variables in people with first-episode psychosis. J. Pers. Med. 12:1732. doi: 10.3390/jpm12101732
Montoro, I., Moreno, L., Mulet, P., Miró, C., Leunda, A., Llaurador-Coll, M., et al. (2023). Maximal sensitivity to child maltreatment at the ages of 6 and 11 years is associated with the risk of bipolar disorder. J. Interpers. Violence 38, 3030–3054. doi: 10.1177/08862605221106128
Moos, R. H., Insel, P. M., and Humphrey, B. (1974). Preliminary manual for family environment scale work environment scale group environment scale. Palo Alto, CA: Consulting Psychologists Press.
Moritz, S., Andreou, C., Schneider, B. C., Wittekind, C. E., Menon, M., Balzan, R. P., et al. (2014). Sowing the seeds of doubt: a narrative review on metacognitive training in schizophrenia. Clin. Psychol. Rev. 34, 358–366. doi: 10.1016/J.CPR.2014.04.004
Moritz, S., Veckenstedt, R., Randjbar, S., Vitzthum, F., and Woodward, T. S. (2011). Antipsychotic treatment beyond antipsychotics: metacognitive intervention for schizophrenia patients improves delusional symptoms. Psychol. Med. 41, 1823–1832. doi: 10.1017/S0033291710002618
Moritz, S., and Woodward, T. S. (2007). Metacognitive training for schizophrenia patients (MCT): a pilot study on feasibility, treatment adherence, and subjective efficacy. Germ. J. Psychiatry. 20, 619–625. doi: 10.1097/YCO.0b013e3282f0b8ed
Muñoz de Arenillas, R., Fernández Borrero, M., Pérez-Moreno, P. J., and Fernández Bellido, M. (2010). Evidencias de validez de la adaptación al español de la Escala de Satisfacción con la Vida (SWLS) en una muestra de estudiabtes universitarios. Metodol. Encues. 12, 45–62.
Notario-Pacheco, B., Solera-Martínez, M., Serrano-Parra, M. D., Bartolomé-Gutiérrez, R., García-Campayo, J., and Martínez-Vizcaíno, V. (2011). Reliability and validity of the Spanish version of the 10-item Connor-Davidson resilience scale (10-item CD-RISC) in young adults. Health Qual. Life Outcomes 9:63. doi: 10.1186/1477-7525-9-63
Ochoa, S., López-Carrilero, R., Barrigón, M. L., Pousa, E., Barajas, A., Lorente-Rovira, E., et al. (2017). Randomized control trial to assess the efficacy of metacognitive training compared with a psycho-educational group in people with a recent-onset psychosis. Psychol. Med. 47, 1573–1584. doi: 10.1017/S0033291716003421
Ochoa, S., Martínez-Zambrano, F., Garcia-Franco, M., Vilamala, S., Ribas, M., Arenas, O., et al. (2015). Development and validation of the self-stigma questionnaire (SSQ) for people with schizophrenia and its relation to social functioning. Compr. Psychiatry 62, 93–99. doi: 10.1016/j.comppsych.2015.06.011
Ochoa, S., Usall, J., Cobo, J., Labad, X., and Kulkarni, J. (2012). Gender differences in schizophrenia and first-episode psychosis: a comprehensive literature review. Schizophr. Res. Treat. 2012, 1–9. doi: 10.1155/2012/916198
Ochoa, S., Usall, J., Haro, J. M., Araya, S., Autonell, J., Busquets, E., et al. (2001). Comparative study of the needs of patients with schizophrenia by gender. Actas Espan. Psiquiatr. 29, 165–171.
Ochoa, S., Usall, J., Villalta-Gil, V., Vilaplana, M., Márquez, M., Valdelomar, M., et al. (2006). Influence of age at onset on social functioning in outpatients with schizophrenia. Eur. J. Psychiatry 20, 157–163. doi: 10.4321/S0213-61632006000300003
Osma, J., Peris-Baquero, O., Suso-Ribera, C., Farchione, T. J., and Barlow, D. H. (2022). Effectiveness of the unified protocol for transdiagnostic treatment of emotional disorders in group format in Spain: results from a randomized controlled trial with 6-months follow-up. Psychother. Res. 32, 329–342. doi: 10.1080/10503307.2021.1939190
Penney, D., Sauvé, G., Mendelson, D., Thibaudeau, É., Moritz, S., and Lepage, M. (2022). Immediate and sustained outcomes and moderators associated with metacognitive training for psychosis: a systematic review and Meta-analysis. JAMA Psychiatry 79, 417–429. doi: 10.1001/JAMAPSYCHIATRY.2022.0277
Peralta Martín, V., and Cuesta Zorita, M. J. (1994). Validation of positive and negative symptom scale (PANSS) in a sample of Spanish schizophrenic patients. Actas Luso-Espanol. Neurol. Psiquiatr. Cienc. Afines 22, 171–177.
Peters, E., Moritz, S., Wiseman, Z., Greenwood, K., Kuipers, E., Schwannauer, M., et al. (2010). The cognitive biases questionnaire for psychosis (CBQP). Schizophr. Res. 117:413. doi: 10.1016/j.schres.2010.02.759
Pino, O., Guilera, G., Rojo, J. E., Gómez-Benito, J., Bernardo, M., Crespo-Facorro, B., et al. (2008). Spanish version of the screen for cognitive impairment in psychiatry (SCIP-S): psychometric properties of a brief scale for cognitive evaluation in schizophrenia. Schizophr. Res. 99, 139–148. doi: 10.1016/j.schres.2007.09.012
Pitman, E., and Matthey, S. (2004). The SMILES program: a group program for children with mentally ill parents or siblings. Am. J. Orthopsychiatry 74, 383–388. doi: 10.1037/0002-9432.74.3.383
Polillo, A., Voineskos, A. N., Foussias, G., Kidd, S. A., Sav, A., Hawley, S., et al. (2021). Using digital tools to engage patients with psychosis and their families in research: survey recruitment and completion in an early psychosis intervention program. JMIR Ment. Health 8:e24567. doi: 10.2196/24567
Pons, D., Atienza, F. L., Balaguer, I., and García-Merita, M. L. (2000). Satisfaction with life scale: analysis of factorial invariance for adolescents and elderly persons. Percept. Mot. Skills 91, 62–68. doi: 10.2466/pms.2000.91.1.62
Purdon, S. E. (2005). The screen for cognitive impairment in psychiatry (SCIP): instructions and three alternate forms. Edmonton: PNL Inc.
Radley, J., Barlow, J., and Johns, L. C. (2022a). Parenting and psychosis: an experience sampling methodology study investigating the inter-relationship between stress from parenting and positive psychotic symptoms. Br. J. Clin. Psychol. 61, 1236–1258. doi: 10.1111/bjc.12389
Radley, J., Barlow, J., and Johns, L. C. (2022b). Sociodemographic characteristics associated with parenthood amongst patients with a psychotic diagnosis: a cross-sectional study using patient clinical records. Soc. Psychiatry Psychiatr. Epidemiol. 57, 1897–1906. doi: 10.1007/s00127-022-02279-x
Radley, J., Sivarajah, N., Moltrecht, B., Klampe, M. L., Barlow, J., and Johns, L. C. (2022c). A scoping review of interventions designed to support parents with mental illness that would be appropriate for parents with psychosis. Front Psychiatry. 12:787166. doi: 10.3389/fpsyt.2021.787166
Reitan, R. M. (1958). Validity of the trail making test as an Indicator of organic brain damage. Percept. Mot. Skills 8, 271–276. doi: 10.2466/pms.1958.8.3.271
Riches, S., Arseneault, L., Bagher-Niakan, R., Alsultan, M., Crush, E., and Fisher, H. L. (2019). Protective factors for early psychotic phenomena among children of mothers with psychosis. Front. Psych. 10:422447. doi: 10.3389/FPSYT.2018.00750/BIBTEX
Riebschleger, J., Tableman, B., Rudder, D., Onaga, E., and Whalen, P. (2009). Early outcomes of a pilot psychoeducation group intervention for children of a parent with a psychiatric illness. Psychiatr. Rehabil. J. 33, 133–141. doi: 10.2975/33.2.2009.133.141
Riecher-Rössler, A., Butler, S., and Kulkarni, J. (2018). Sex and gender differences in schizophrenic psychoses—a critical review. Arch. Womens Ment. Health 21, 627–648. doi: 10.1007/s00737-018-0847-9
Rosenblum, K. L., Muzik, M., Morelen, D. M., Alfafara, E. A., Miller, N. M., Waddell, R. M., et al. (2017). A community-based randomized controlled trial of mom power parenting intervention for mothers with interpersonal trauma histories and their Young children. Arch. Womens Ment. Health 20, 673–686. doi: 10.1007/S00737-017-0734-9
Ruiz, A., Pousa, E., Duñó, R., Crosas, J., Cuppa, S., and García, C. (2008). Spanish adaptation of the scale to asses unawareness of mental disorder (SUMD). Actas Espan. Psiquiatr. 36, 111–1198.
Salas-Sender, M., López-Carrilero, R., Barajas, A., Lorente-Rovira, E., Pousa, E., Barrigón, M. L., et al. (2020). Gender differences in response to metacognitive training in people with first-episode psychosis. J. Consult. Clin. Psychol. 88, 516–525. doi: 10.1037/ccp0000468
Sánchez-Cubillo, I., Periáñez, J. A., Adrover-Roig, D., Rodríguez-Sánchez, J. M., Ríos-Lago, M., Tirapu, J., et al. (2009). Construct validity of the trail making test: role of task-switching, working memory, inhibition/interference control, and visuomotor abilities. J. Int. Neuropsychol. Soc. 15, 438–450. doi: 10.1017/S1355617709090626
Sandín, B., Chorot, P., and Valiente, R. M. (2015). Escala de Satisfacción con la Vida para Niños y Adolescentes (SWLS-C) Universidad Nacional de Educación a Distancia [Unpublished Questionnaire].
Santamarina-Perez, P., Mendez, I., Singh, M. K., Berk, M., Picado, M., Font, E., et al. (2020). Adapted dialectical behavior therapy for adolescents with a high risk of suicide in a community clinic: a pragmatic randomized controlled trial. Suicide Life Threat. Behav. 50, 652–667. doi: 10.1111/sltb.12612
Santesteban-Echarri, O., Piskulic, D., Nyman, R. K., and Addington, J. (2020). Telehealth interventions for schizophrenia-spectrum disorders and clinical high-risk for psychosis individuals: a scoping review. J. Telemed. Telecare 26, 14–20. doi: 10.1177/1357633X18794100
Sarró, S. (2004). Cross-cultural adaptation and validation of the Spanish version of the Calgary depression scale for schizophrenia. Schizophr. Res. 68, 349–356. doi: 10.1016/S0920-9964(02)00490-5
Schmidt, S. J., Schultze-Lutter, F., Schimmelmann, B. G., Maric, N. P., Salokangas, R. K. R., Riecher-Rössler, A., et al. (2015). EPA guidance on the early intervention in clinical high risk states of psychoses. Eur. Psychiatry 30, 388–404. doi: 10.1016/J.EURPSY.2015.01.013
Seeman, M. V. (2020). “Gender and outcome in schizophrenia” in Schizophrenia treatment outcomes eds. A. Shrivastava, and A. De Sousa (Switzerland: Springer International Publishing), 15–25.
Seeman, M. V. (2021). Sex differences in schizophrenia relevant to clinical care. Expert. Rev. Neurother. 21, 443–453. doi: 10.1080/14737175.2021.1898947
Shaffer, D. (1983). A Children’s global assessment scale (CGAS). Arch. Gen. Psychiatry 40:1228. doi: 10.1001/archpsyc.1983.01790100074010
Sheinbaum, T., Berry, K., and Barrantes-Vidal, N. (2013). Spanish version of the psychosis attachment measure: adaptation process and psychometric properties - Proceso de adaptación al español y propiedades psicométricas de la psychosis attachment measure. Salud Ment. 36:403. doi: 10.17711/SM.0185-3325.2013.050
Steenhuis, L. A., Pijnenborg, G. H. M., van der Stouwe, E. C. D., Hartman, C. A., Aleman, A., Bartels-Velthuis, A. A., et al. (2020). The longitudinal association between preadolescent facial emotion identification and family factors, and psychotic experiences in adolescence (the TRAILS study). Child Psychiatry Hum. Dev. 51, 187–199. doi: 10.1007/S10578-019-00922-4
Tapias, E., Coromina, M., Grases, N., and Ochoa, S. (2021). Psychological Treatments with Children 762 of Parents with Mental Illness: A Systematic Review. Child Youth Care Forum 50, 1107–1130. doi: 10.1007/S10566-021-09608-2
Teicher, M. H., and Parigger, A. (2015). The ‘maltreatment and abuse chronology of exposure’ (MACE) scale for the retrospective assessment of abuse and neglect during development. PLoS One 10:e0117423. doi: 10.1371/journal.pone.0117423
Tobin, D. L., Holroyd, K. A., Reynolds, R. V., and Wigal, J. K. (1989). The hierarchical factor structure of the coping strategies inventory. Cogn. Ther. Res. 13, 343–361. doi: 10.1007/BF01173478
Tous-Pallarés, J., Espinoza-Díaz, I. M., Lucas-Mangas, S., Valdivieso-León, L., and Gómez-Romero, M. D. R. (2022). CSI-SF: Propiedades psicométricas de la versión española del inventario breve de estrategias de afrontamiento. Anal. Psicol. 38, 85–92. doi: 10.6018/analesps.478671
Usall, J. (2001). Gender differences in a sample of schizophrenic outpatients. Compr. Psychiatry 42, 301–305. doi: 10.1053/comp.2001.24582
Villeneuve, K., Potvin, S., Lesage, A., and Nicole, L. (2010). Meta-analysis of rates of drop-out from psychosocial treatment among persons with schizophrenia spectrum disorder. Schizophr. Res. 121, 266–270. doi: 10.1016/j.schres.2010.04.003
Wan, M. W., Moulton, S., and Abel, K. M. (2008). A review of mother-child relational interventions and their usefulness for mothers with schizophrenia. Arch. Womens Ment. Health 11, 171–179. doi: 10.1007/S00737-008-0010-0
Wechsler, D. (2008). Wechsler adult intelligence scale–fourth edition (WAIS–IV). Antonio: Psychological Corporation.
Wechsler, D. (2014). “Manual de aplicación y correción (WISC-V)” in PsychCorp, vol. 33. Madrid: Pearson.
Weil, L. G., Fleming, S. M., Dumontheil, I., Kilford, E. J., Weil, R. S., Rees, G., et al. (2013). The development of metacognitive ability in adolescence. Conscious. Cogn. 22, 264–271. doi: 10.1016/J.CONCOG.2013.01.004
Wolpert, M., Hoffman, J., Martin, A., Fagin, L., and Cooklin, A. (2015). An exploration of the experience of attending the Kidstime programme for children with parents with enduring mental health issues: parents’ and young people’s views. Clin. Child Psychol. Psychiatry 20, 406–418. doi: 10.1177/1359104514520759
Keywords: mothers with psychosis, adolescents’ mental health, metacognitive training, family intervention, protocol, clinical trial
Citation: Ochoa S, Espinosa V, López-Carrilero R, Martinez I, Barrera ADH, Birulés I, Barajas A, Pélaez T, Díaz-Cutraro L, Coromina M, González-Rodríguez A, Verdaguer-Rodríguez M, Gutiérrez-Zotes A, Palma-Sevillano C, Montes C, Gallego J, Paya B, Casanovas F, Roldán M, Noval E, Varela Casals P, Salas-Sender M, Aznar A, Ayesa-Arriola R, Pousa E, Canal-Rivero M, Garrido-Torres N, Montserrat C, Muñoz-Lorenzo L and Crosas JM (2024) Effectiveness of family metacognitive training in mothers with psychosis and their adolescent children: a multicenter study protocol. Front. Psychol. 15:1359693. doi: 10.3389/fpsyg.2024.1359693
Edited by:
Lara Guedes De Pinho, University of Evora, PortugalReviewed by:
Ana Isabel Morais, University of Evora, PortugalMareike Samaan, Evangelische Krankenhaus Königin Elisabeth Herzberge (KEH), Germany
Copyright © 2024 Ochoa, Espinosa, López-Carrilero, Martinez, Barrera, Birulés, Barajas, Pélaez, Díaz-Cutraro, Coromina, González-Rodríguez, Verdaguer-Rodríguez, Gutiérrez-Zotes, Palma-Sevillano, Montes, Gallego, Paya, Casanovas, Roldán, Noval, Varela Casals, Salas-Sender, Aznar, Ayesa-Arriola, Pousa, Canal-Rivero, Garrido-Torres, Montserrat, Muñoz-Lorenzo and Crosas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susana Ochoa, susana.ochoa@sjd.es