 Hanna Edberg
Hanna Edberg Qi Chen
Qi Chen Peter Andiné
Peter Andiné Henrik Larsson
Henrik Larsson Tatja Hirvikoski
Tatja Hirvikoski- 1Paediatric Neuropsychiatry Unit, Department of Women’s and Children’s Health, Centre for Neurodevelopmental Disorders at Karolinska Institutet (KIND), Karolinska Institutet, Stockholm, Sweden
- 2Swedish Prison and Probation Services, Norrköping, Sweden
- 3Northern Stockholm Psychiatric Clinic, Region Stockholm, Stockholm, Sweden
- 4Centre for Psychiatry Research, Region Stockholm, Stockholm, Sweden
- 5Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden
- 6Centre for Ethics, Law and Mental Health (CELAM), Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 7Forensic Psychiatric Clinic, Sahlgrenska University Hospital, Gothenburg, Sweden
- 8Department of Forensic Psychiatry, National Board of Forensic Medicine, Gothenburg, Sweden
- 9School of Medical Sciences, Örebro University, Örebro, Sweden
- 10Habilitation & Health, Region Stockholm, Stockholm, Sweden
Background: Offenders with intellectual disability (ID) constitute a distinct subgroup of offenders with mental disorders. Regarding criminal recidivism, it is unclear whether or not offenders with ID in forensic psychiatric settings differ from offenders without ID. Factors associated with criminal recidivism among offenders with ID have been scarcely investigated.
Aim: To investigate the association between ID and criminal recidivism among offenders sentenced to forensic psychiatric care and to explore the impact of clinical, sociodemographic and offense variables.
Materials and methods: We conducted a retrospective cohort study based on Swedish nationwide registers. A total of 3,365 individuals being sentenced to forensic psychiatric care in Sweden in 1997–2013 were followed from the forensic psychiatric assessment until first reconviction, death, emigration, or 31 December 2013, whichever occurred first. Cox regression models compared rates of recidivism in individuals with and without ID. Impact of clinical, sociodemographic, and offense variables on risk of criminal recidivism was presented as hazard ratios (HRs) with 95% confidence intervals (CIs).
Results: Out of 3,365 offenders sentenced to forensic psychiatric care, 259 (7.7%) were diagnosed with ID. During follow-up (0–17 years, median 6 years), one third (n = 1,099) of the study population relapsed into criminality, giving a recidivism rate of 50.5 per 1,000 person-years. We observed an association between ID and a decreased risk of recidivism (HR 0.8, 95% CI 0.6–1.0, p = 0.063), although this reached statistical significance only for the subgroup of male offenders (HR 0.8, 95% CI 0.6–1.0, p = 0.040) and not females (HR 1.0, 95% CI 0.6–1.8). ID offenders with concurrent ADHD tended to have a higher rate of recidivism (73.9 per 1,000 person-years, HR 1.2, 95% CI 0.6–2.4) than ID offenders without ADHD (42.5 per 1,000 person-years, HR 0.8, 95% CI 0.6–1.1). Amongst ID offenders, concurrent autism spectrum disorder, young age or male sex were not associated with recidivism, while previous criminal convictions were strongly associated with recidivism.
Conclusion: A diagnosis of ID was associated with a lower risk of criminal recidivism among male offenders sentenced to forensic psychiatric care. The association between ADHD and recidivism among ID offenders highlights eligible focus areas in the management of offenders with ID.
Introduction
Intellectual disability (ID) is a neurodevelopmental disorder characterized by early onset, significant impairment of intellectual functioning and adaptive behavior (1, 2), affecting about 1% of the general population (3, 4). Comorbid neurodevelopmental disorders such as ADHD (attention-deficit/hyperactivity disorder) and ASD (autism spectrum disorder) are common among individuals with ID (5, 6). Individuals with ID have been reported as overrepresented in the criminal justice system, but base rates of criminal offending among individuals with ID have been difficult to establish, partially because of inconsistent definitions of ID. Prevalence estimates have ranged from well below to above and beyond that of the general population (7). In Sweden, offenders with severe mental disorders can be sentenced to forensic psychiatric care instead of prison (8). The court can order a forensic psychiatric assessment (FPA) to obtain a multi-professional judgment if an alleged offender suffers from a severe mental disorder. A severe mental disorder is a judicial concept that includes mental, behavioral, or emotional conditions that cause serious functional impairment, such as, under certain circumstances, ID (9). In a forensic psychiatric context, offenders with ID differ from their non-ID counterparts in aspects of clinical and sociodemographic characteristics and criminal behavior; they are younger, less socially established, show a higher frequency of concurrent neurodevelopmental disorders and are more likely to have committed a sexual offense (10–13). Whether offenders with ID also differ from non-ID offenders regarding recidivism rate has not been thoroughly investigated. Similarly, risk factors for re-offending are not well-known in this group.
In their most recent meta-analysis, Bonta et al. noted that intellectual impairment was weakly associated with increased risk of recidivism (14). However, the studies that generated this conclusion were published in the 1980–1990s, a period in which the definition of ID differed from contemporary diagnostic criteria (15, 16). In addition, several of the included studies focused exclusively on arsonists. Furthermore, a study by Gray et al. from 2007, which reported slower recidivism rates among offenders with ID (according to ICD-10, codes F70-79), compared to other offenders with mental disorders (17), was included in the meta-analysis, but later omitted from the analysis as an outlier. Several more recent studies on criminal recidivism rates in populations of offenders with mental disorders do not include ID (18–20). In studies where data on ID or intelligence has been included, study samples have been small (21) or only presented data on selected samples, such as subjects sentenced to community services (22, 23). Hence, it remains uncertain whether or not ID is associated with criminal recidivism among offenders with mental disorders.
Several studies have tried to define risk factors for offending among individuals with ID (24–26), often by describing characteristics of offenders with ID and making comparisons to a non-ID or a non-offender group. A latent class analysis of offenders with mental disorders showed that offenders with ID exhibit particular levels of risk and protective factors for criminal behavior that differentiate them from offenders with other mental disorders, meriting distinction as one of five separate groups. Offenders with ID had the lowest levels of protective factors such as insight, coping, and social skills, as well as treatment compliance (27). Furthermore, comorbid ADHD has been suggested to be associated with increased risk of violent offending among individuals with ID (28). However, when studying risk factors for criminal behavior among individuals with ID, it is important to distinguish between risk factors for offending and risk factors for re-offending. While variables such as externalizing behavioral problems and comorbid mental disorders might be associated with increased risk of offending among individuals with ID (25, 29–31), the same factors might hypothetically prompt an augmented level of support and more extensive rehabilitation measures following a criminal act, which can in turn reduce the risk of re-offending. In Sweden for example, individuals with ID are subject to specific legislation to ensure adequate support (32). In order to receive these services, the individual must be known by the social authorities. A contact with the criminal justice system might be the factor that draws attention to the individual, which initiates support. Measures such as personal assistance, financial support, counseling, adapted housing and daily activities are granted according to the individual need. The greater the need the more extensive the measures of support. Factors associated with first time offending, might therefore induce social support acting as preventive measures on risk of re-offending.
Previous meta-analyses (14, 33) and more recent studies (21, 34) suggest that the strongest predictors of criminal recidivism among offenders with mental disorders are criminogenic variables (i.e., criminal history and deviant lifestyle including substance abuse and antisocial behavior); far exceeding the predictive value of potential clinical variables such as psychiatric comorbidity, prior hospital admissions and psychiatric treatment. A more limited number of studies have focused specifically on factors related to criminal recidivism specifically in ID. A study by Lofthouse et al. bears references to re-offending, by describing how different risk factors can predict future violent behavior (not specifically reconvictions) among offenders with ID. The authors suggest that even though static risk factors (unchangeable factors such as age at first conviction and previous criminal convictions) dominate dynamic factors (e.g., behavioral aspects or clinical symptoms that are amenable to change) in the prediction of the risk of future violent behavior among offenders with ID, dynamic variables serve as proxy risk factors for static risk and are therefore both useful and important in assessment (35). Fitzgerald analyzed the predictive effect of criminal history variables and substance use variables on criminal reconviction among individuals with ID in medium secure hospitals (individuals who had offended, or who had exhibited behavior that might have led to a conviction under different circumstances) and found that criminal history and substance use variables predicted future reconviction in offenders with ID, much the same as among other offenders (36). Marti-Augusti et al. conducted a review on offenders with ID (37), including data on both offending and recidivism. They suggested that in addition to known risk factors, well-described by Bonta et al. (14, 33), clinical variables such as personality disorders were risk factors for reoffending among offenders with ID. However, a number of the referred studies included borderline intellectual functioning, currently not included in the definition of ID (38–40), or were reviews based on studies going back 20–30 years in time (41, 42). Study samples dating back several decades can be problematic since there has been a marked increase of diagnoses of ADHD and ASD during the last 30 years (43, 44), supposedly related to changes in diagnostic practices (45, 46).
To conclude, whether or not ID is associated with criminal recidivism among offenders with mental disorders is unclear. Therefore, the primary aim of the study is to investigate if ID is associated with increased or decreased risk of criminal recidivism among offenders with mental disorders who have been sentenced to forensic psychiatric care. There is a lack of research regarding risk factors for criminal recidivism among offenders with ID. Concurrent neurodevelopmental disorders such as ADHD and ASD among offenders with ID are a potentially tangible intervention target and hence a research area that merits more attention (39, 47). Hence, the secondary aim of the study is to study the effect of clinical, sociodemographic, and offense variables on criminal recidivism among offenders with ID, compared to offenders with other mental disorders.
Materials and methods
Study design
We conducted a population-based cohort study of individuals sentenced to forensic psychiatric care in Sweden using data from the Swedish national registers.
Data
Our data originated from the Central Archive of the National Board of Forensic Medicine, where data from all FPAs in Sweden are registered. Data was pseudonymized and linked to national population-based registers.
Study population
The cohort included 3,365 individuals who were sentenced to forensic psychiatric care after FPA in Sweden between 1 January 1997 and 30 May 2013. During the study period, a total of 8,442 individuals were subject to FPA. All individuals for whom it was possible to identify an index offense were included, which comprised 88% (n = 7,450) of the total population. As described in previous work (13), there were no significant differences in age, sex, psychiatric diagnoses, parental education level, or immigration status between the total source population of 8,442 individuals and the individuals included in the study.
Study setting
Individuals were followed from the date when the result of the FPA was presented to the court until first reconviction date (criminal recidivism), death, emigration from Sweden or 31 December 2013, whatever occurred first. The start of follow-up was chosen since it has been shown that up to 10 percent of individuals sentenced or diverged to forensic psychiatric care commit a new criminal offense whilst under forensic psychiatric care (21, 48–50). The duration of follow-up was up to 17 years (median 6 years).
Exposures
Exposure in the primary analysis was a diagnosis of ID, registered during the FPA. The diagnosis derives from a thorough team-based medical-psychiatric assessment with a psychological assessment of intellectual and adaptive functioning including evaluation using the Swedish version of the Wechsler Adult Intelligence Scale (51). Diagnoses were coded according to the Diagnostic and Statistical Manual of Mental Disorders, 4th version (DSM-IV) (51). DSM-IV codes for ID included 317, 318.0, 318.1, 318.2, 319. Exposure in the secondary analysis was clinical variables (i.e., concurrent psychiatric diagnoses). Sociodemographic variables and offense variables were treated as exposures in the third analysis.
Outcomes
The outcome was defined as first criminal reconviction registered by the court. Main analyses included reconviction of any offense as outcome. Descriptive statistics included sub-categories of crime, including violent non-sexual, sexual and non-sexual non-violent crime.
Covariates
Sociodemographic variables
Sociodemographic data were assessed at the time of the FPA, i.e., right before start of follow-up. Data derived from Swedish population-based registers, including the longitudinal integration database for health insurance and labor market studies covering all Swedish residents ≥ 16 years of age (52), the Multi-Generation Register and the Total Population Register (53). Variables included age (at the time of the FPA if not otherwise specified), sex, immigration status (born in or outside Sweden) and highest parental educational level (<9 years, 9 years, >9 years).
Clinical variables
Clinical variables included psychiatric diagnoses derived from the FPA, coded according to the DSM-IV. Concurrent psychiatric diagnoses included ADHD, ASD, alcohol use disorders, drug use disorders, personality disorders (including antisocial personality disorders, borderline personality disorders, and other personality disorders), schizophrenia, and sexual disorders. Diagnostic codes can be found in Supplementary Table 1.
Offense variables
Offense variables included index crime type (crime resulting in sentence to forensic psychiatric care) and previous crime (yes/no). Criminal offenses were categorized according to the Swedish Penal Code in three categories: violent non-sexual, sexual and non-sexual non-violent. Index crimes were obtained from the Central Archive of the National Board of Forensic Medicine. The Swedish National Council for Crime Prevention (Brå) provided data regarding previous convictions and reconvictions during follow-up. A thorough description of the rationale behind the offense variables can be found in previous work (13).
Statistical analyses
Descriptive characteristics for ID and non-ID offenders at baseline were reported as percentages for categorical variables and medians with interquartile range (IQR) for continuous variables. We constructed cumulative incidence curves for first reconviction for any offense among offenders with and without ID using the Kaplan-Meier method with Log-Rank test. Separate analyses were not performed on sub-categories of crimes because of the limited sample size. The association between ID and rate of recidivism was analyzed using the Cox regression model estimating hazard ratio (HR) with 95% confidence interval (CI). In a sensitivity analysis, the model was stratified by sex.
In order to study the effect of clinical variables (i.e., concurrent psychiatric diagnoses) on the risk of recidivism among ID offenders and non-ID offenders, we calculated the incidence rates of recidivism in different subgroups of psychiatric disorders and used Cox regression analyses to estimate HRs, using individuals without ID and without the clinical variable as the reference group.
In the analysis of association between sociodemographic and offense variables, and recidivism among ID offenders and non-ID offenders, HRs were estimated. Parental educational level was missing in 34.7% of cases. Under the assumption of missing at random, we handled the missing data by applying multiple imputation, with 20 imputed samples (54). We analyzed each imputed dataset and reported the pooled estimates.
All Cox proportional hazard models were adjusted for age, sex, previous convictions, and parental educational level. In the analysis of sociodemographic and offense variables, adjustment was also made for concurrent psychiatric diagnoses. The proportionality of hazard assumption was tested by measuring interactions between covariates and time. Statistical analyses were conducted using the IBM SPSS Statistics 28 software. All statistical tests were two-tailed with p-value < 0.05 considered significant.
Results
Characteristics of the population are presented in Table 1, for ID (n = 259) and non-ID (n = 3,106) offenders. Follow-up time was 0–17.5 years (median 6 years). Out of 3,365 individuals, a total of 1,099 (33%) were convicted of at least one new crime during follow up. Individuals with ID presented slightly lower crude rates of recidivism at end of follow-up than individuals without ID (29 vs. 33%).
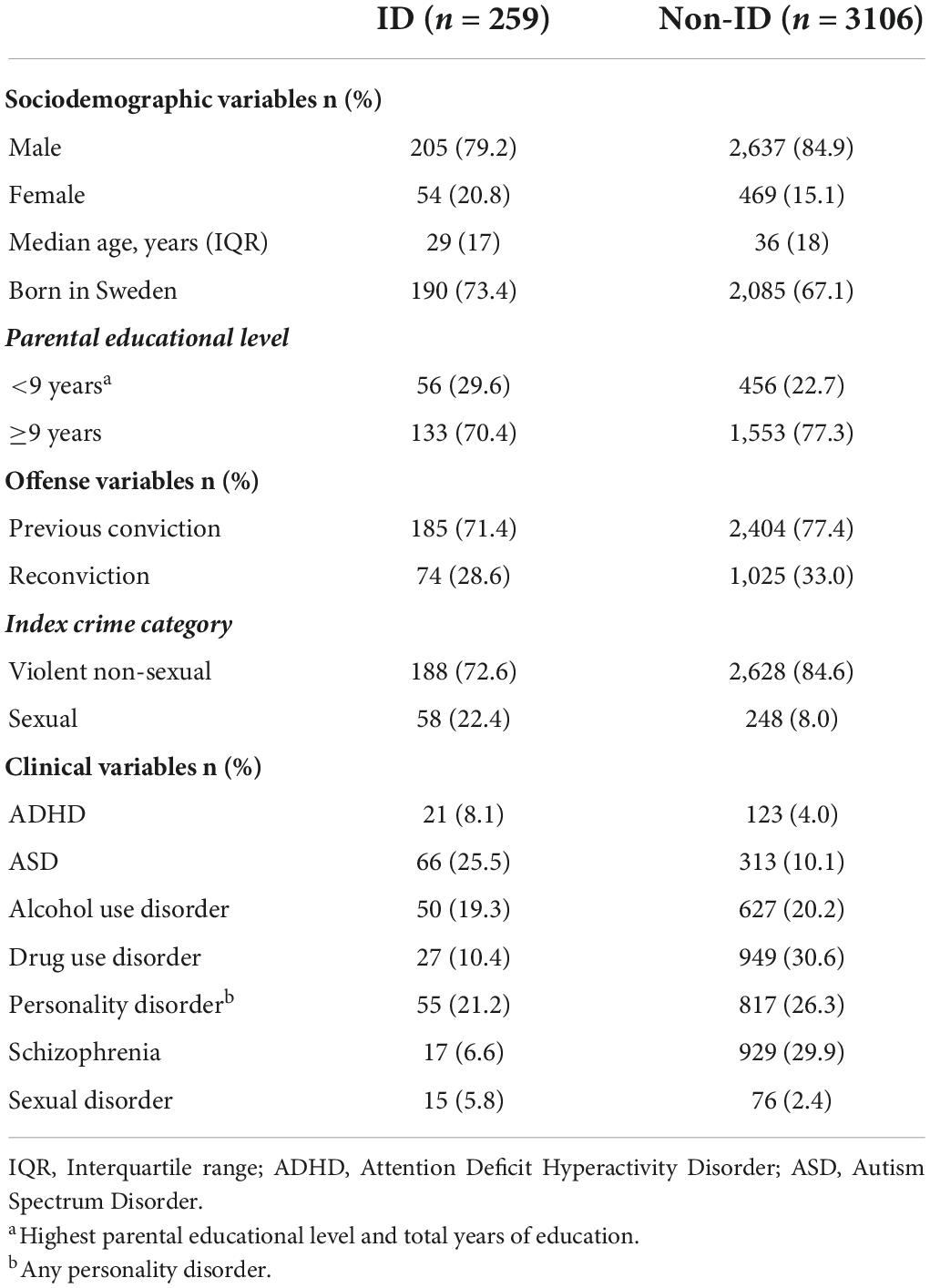
Table 1. Characteristics of offenders with and without ID sentenced to forensic psychiatric care in Sweden in 1997–2013 (n = 3,365).
Association between ID and criminal recidivism
Cumulative incidence curves for first reconvictions during a follow-up are presented in Figure 1. Offenders with ID tend to relapse into crime at a slower pace than offenders without ID after 7 or more years following a sentence to forensic psychiatric care, however, the overall difference did not reach statistical significance (log rank test 1.209, p = 0.272).
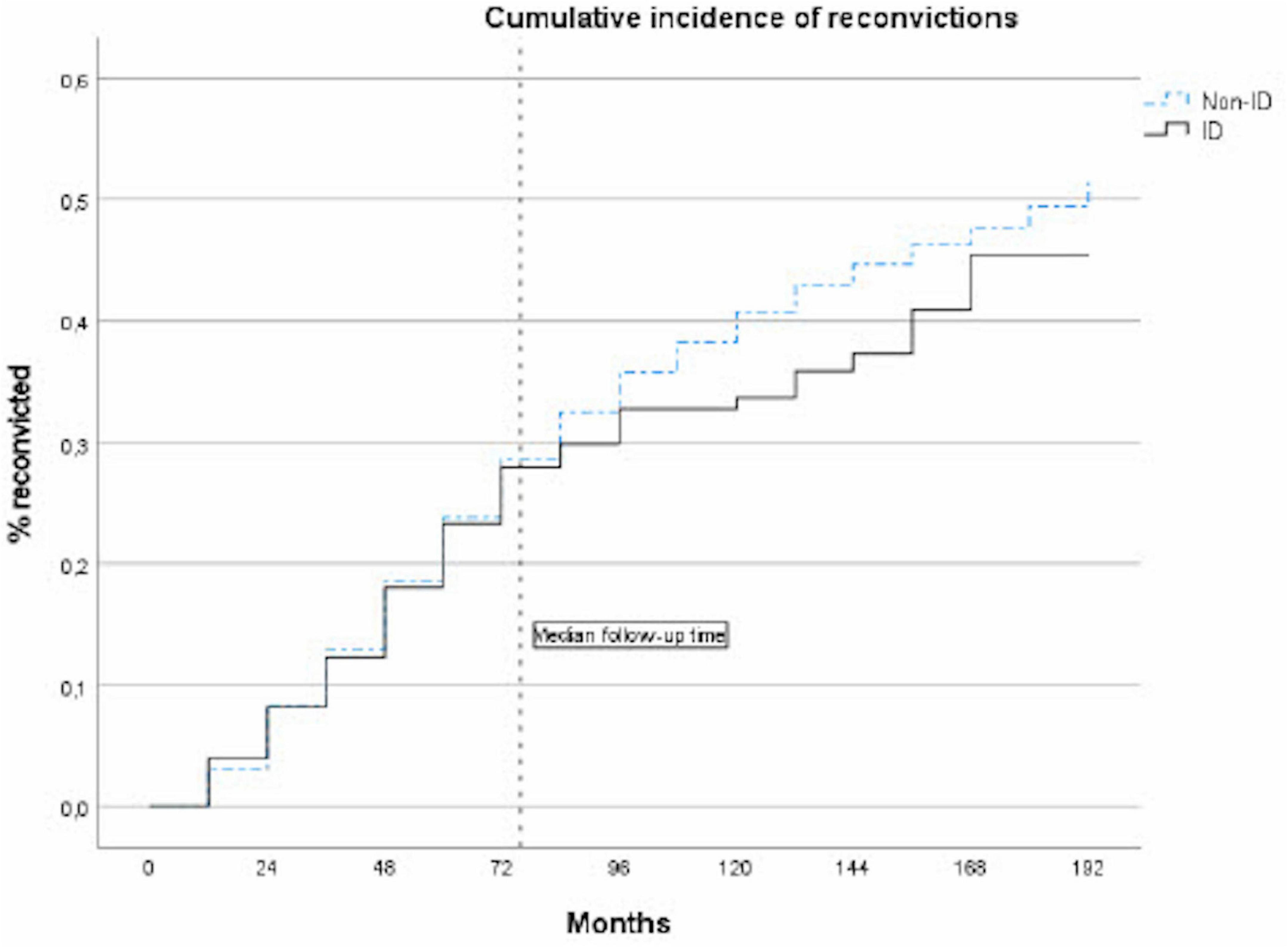
Figure 1. Cumulative incidence of reconvictions, comparing ID and non-ID offenders sentenced to forensic psychiatric care.
In the entire study population, after adjustment for age, sex, previous criminal convictions, and parental educational level, we observed an association between ID and decreased risk of criminal recidivism (HR 0.8, 95% CI 0.6–1.0), although this did not reach statistical significance (p = 0.063) (Table 2). Sex stratified analyses showed that the association was significant among male offenders (HR 0.8, 95% CI 0.6–1.0, p = 0.040), but not among female offenders (HR 1.0, 95% CI 0.6–1.8) (Supplementary Table 2).

Table 2. Estimated hazard ratios for reconvictions, comparing ID and non-ID offenders, adjusted for potential confounders (age, sex, previous convictions, and parental educational level).
Reconviction categories are presented in Table 3. Violent non-sexual reconvictions were more common among ID than among non-ID offenders (35 vs. 24%), non-sexual non-violent reconvictions were more common among non-ID offenders (75 vs. 62%) and sexual reconvictions were uncommon in both groups (2.7% among ID offenders, 1.8% among non-ID offenders).
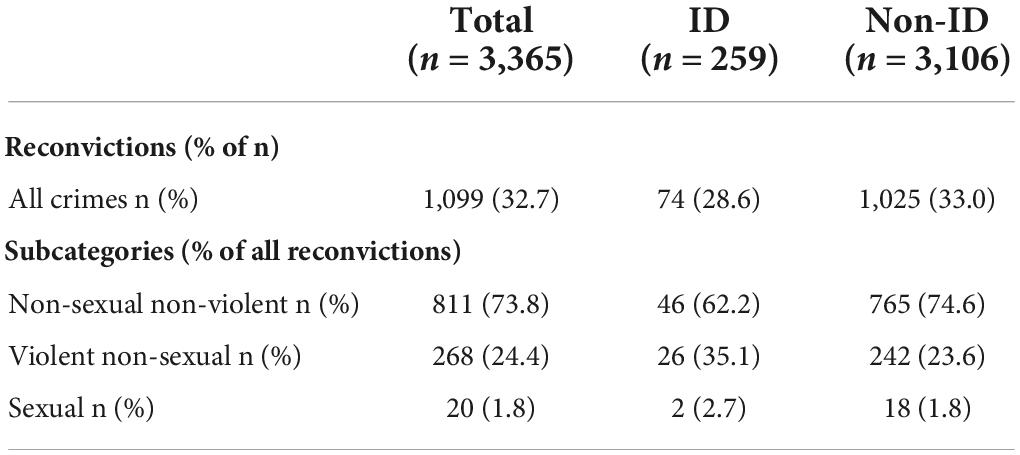
Table 3. Reconvictions at end of follow-up among offenders with and without ID.
Association between clinical variables and criminal recidivism
Results regarding clinical variables are presented in Figures 2, 3 (full data can be found in Supplementary Table 3). Sexual disorders were omitted because of small actual numbers (total cases < 25). Alcohol use disorders showed no association to recidivism and did not differ between ID and non-ID offenders, and was thus omitted from the figure. In both groups, schizophrenia was associated with decreased recidivism risk (ID and schizophrenia: HR 0.2, 95% CI 0.0–1.4; non-ID and schizophrenia: HR 0.7, 95% CI 0.6–0.8). In both groups, increased risk was observed in association with drug use disorders (ID and drug use disorders: HR 1.5, 95% CI 0.9–2.8; non-ID and drug use disorders: HR 1.9, 95% CI 1.6–2.1) and ADHD (ID and ADHD: HR 1.2, 95% CI 0.6–2.4; non-ID and ADHD: HR 1.7, 95% CI 1.3–2.2). In subjects with ID, data could not support an effect of concurrent ASD or personality disorders on recidivism risk (ID and ASD: HR 0.8, 95% CI 0.5–1.3; ID and personality disorders: HR 0.7, 95% CI 0.4–1.2). In subjects without ID, ASD was associated with decreased recidivism risk (non-ID and ASD: HR 0.6, 95% CI 0.5–0.8) and personality disorders with increased recidivism risk (non-ID and personality disorders: HR 1.3, 95% CI 1.2–1.5).
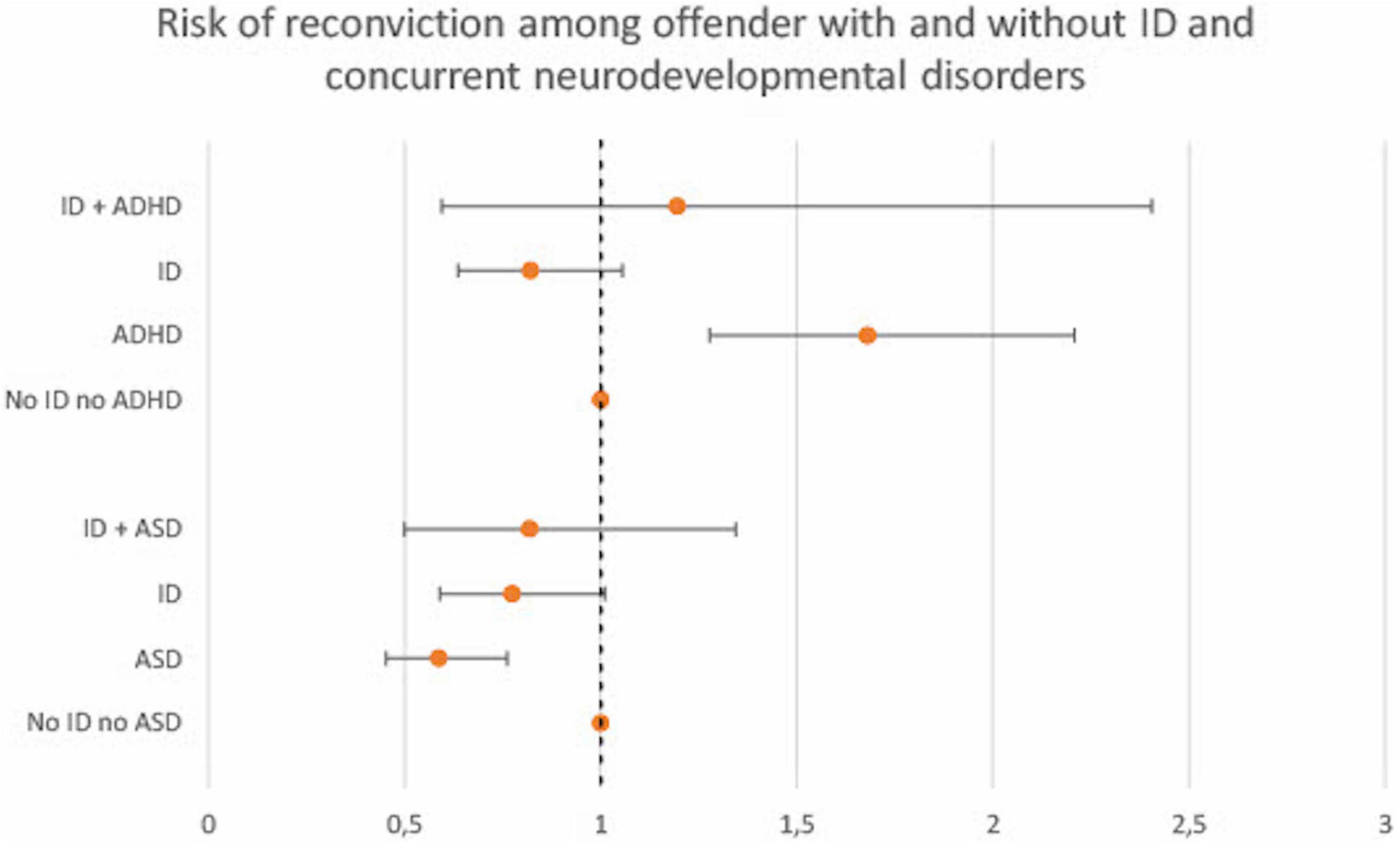
Figure 2. Cox proportional hazard ratios (with 95% CI) for criminal recidivism associated with clinical variables among offenders with and without ID. Reference category for each group are offenders with neither ID nor the clinical variable (ADHD and ASD, respectively). ADHD, Attention Deficit Hyperactivity Disorder; ASD, Autism Spectrum Disorder.
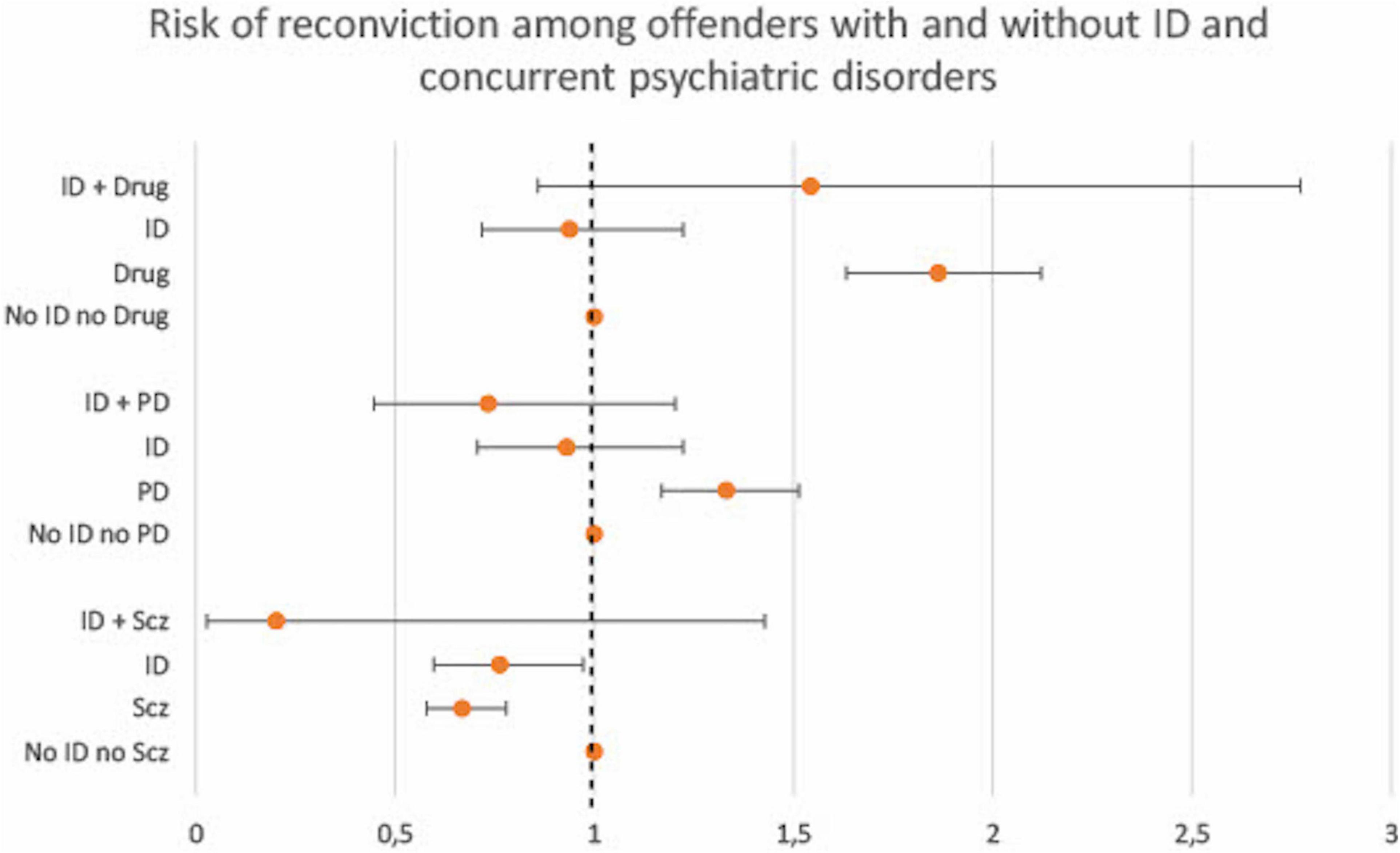
Figure 3. Cox proportional hazard ratios (with 95% CI) for criminal recidivism associated with clinical variables among offenders with and without ID. Reference category for each group are offenders with neither ID nor the clinical variable (drug use disorder, personality disorder or schizophrenia, respectively). Drug, Drug use disorder; PD, Any personality disorder; Scz, Schizophrenia.
Association between sociodemographic and offense variables and criminal recidivism
The final analysis evaluated the association between sociodemographic and offense variables and criminal recidivism, comparing offenders with and without ID. Results are presented in Table 4. Previous criminal convictions showed the strongest association with increased risk of criminal recidivism in both offenders with and without ID (ID and previous convictions: HR 3.0, 95% CI 1.4–6.1; non-ID and previous convictions: HR 1.9, 95% CI 1.5–2.3). Among subjects with ID, being male was not associated with risk of recidivism (ID and male: HR 1.1, 95% CI 0.6–2.0), which was the case among subjects without ID (non-ID and male: HR 1.4, 95% CI 1.1–1.7). Among subject without ID, the youngest age group (age 15–24) was associated with the highest risk of recidivism (non-ID and age 15–24: HR 3.3, 95% CI 2.3–4.8) and the risk decreased gradually with increased age. Among subjects with ID, no obvious association between age and criminal recidivism was seen. The risk did not decrease gradually with age and was equally high among 15–24-year-olds (ID and age 15–24: HR 1.5, 95% CI 0.2–13.0) as among 35–44-year-olds (ID and age 35–44: HR 1.5, 95% CI 0.2–11.9). Being born in Sweden was associated with lower risk of recidivism among subjects with ID (ID and born in Sweden: HR 0.6, 95% CI 0.4–1.0), but did not affect the risk among subjects without ID (non-ID and born in Sweden: HR 1.0, 95% CI 0.6–1.1). Low parental educational level was associated with an increased risk of recidivism among subjects with ID (ID and low parental level: HR 1.6, 95% CI 0.7–3.5) but not among subjects without ID (non-ID and low parental level: HR 1.2, 95% CI 1.0–1.4).
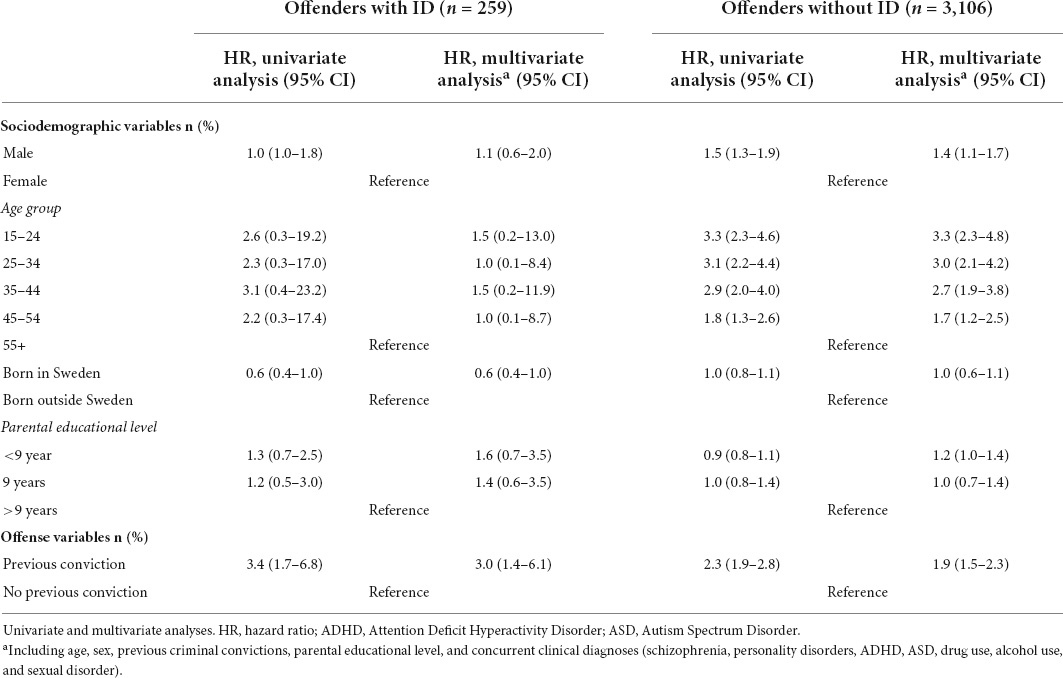
Table 4. Cox proportional hazard ratios for reconvictions associated with sociodemographic and offense variables comparing offenders with and without ID.
Discussion
In this Swedish nationwide register-based cohort study of 3,365 offenders sentenced to forensic psychiatric care, we observed an association between ID and decreased risk of criminal recidivism after adjustment for eligible confounders. This finding is in concordance with the results from Gray et al. who reported that ID individuals reoffended at a significantly lower rate than their non-ID counterparts (17). By contrast, our results can be seen as contradictory to the meta-analysis by Bonta et al. (14), who reported an increased risk of criminal recidivism among offenders with intellectual impairment. Bonta et al. did however employ the concept of “intellectual impairment” in their study, which can include, but is not necessarily synonymous with, a diagnosis of ID. This highlights the importance of distinguishing ID from borderline ID and using clear and transparent definitions in research on ID offenders.
Our results could only verify a risk reduction related to ID among male offenders (constituting over 80% of the current study population). No obvious association between ID and recidivism was observed among females. Future research on a larger sample of female offenders is needed to further investigate the relationship between ID and recidivism.
The impact of psychiatric diagnoses on criminal recidivism risk showed both similarities and discrepancies among offenders with and without ID. ADHD was associated with increased recidivism risk in subjects without ID and a similar tendency was seen in subjects with ID, although not reaching statistical significance. This finding is in line with results from a Swedish cohort study, where the elevated risk of violent offending among ID individuals to a great extent was explained by comorbid ADHD (28). Our data thus suggest that the same is true regarding the risk of reoffending. These findings bear great importance, since ADHD can be successfully treated both in general and offender populations (55, 56) and treatment has been associated with decreased risk of criminal recidivism among offenders (57). Assessment and treatment of concurrent ADHD among ID offenders should be an integrated part of individualized care plans in forensic psychiatric settings.
Concurrent ASD did not affect the recidivism risk in any direction in subjects with ID. Among subjects without ID, however, ASD was associated with decreased risk of criminal recidivism. These are important results since there is limited research on the impact of ASD on offending behaviors among ID offenders (47).
Among offenders with ID, young age and being male were not variables associated with greater risk of reconviction. This finding can be interpreted as a feature distinguishing ID offenders from other offenders with mental disorders (21, 33, 34) and from general adult offenders (58), where being young and male is typically associated with a greater risk of recidivism. However, a recent meta-analysis of 28 studies investigating predictors of criminal recidivism among forensic outpatients did not replicate the findings of Bonta el al. and Gendreau et al. regarding age and sex as risk factors for recidivism (59). Sex was also not associated with recidivism in a study on 315 patients discharged from a medium-secure hospital in the UK (60). In a recent study of 477 offenders with mental disorders by Dean et al. results suggested that while sex was not associated with reconviction rates overall, women reoffended to a higher degree than men during the first 12 months following release (61). Sex differences in criminal recidivism studies in populations of offenders with mental disorders thus present diverging results. Besides offenders with mental disorders being heterogeneous populations making comparisons difficult, another plausible interpretation is that while male sex used to show strong association with criminal recidivism, sex differences in criminal behavior have started to level during the last decades (62): a phenomenon described as a “narrowing gender gap” (63, 64). Our findings add important knowledge to the field, since a number of previous studies on recidivism in ID offenders have not been able to study sex differences due to restricted sample size (36) or sample selection (65). Opposite to our results, young age was suggested as a risk factor for recidivism in a previous study on 67 ID offenders (66). Considering that the vast majority of studies of recidivism in ID offenders suffer from lack of statistical power, each contribution is of importance to increase the knowledge in the field.
More research is needed in order to develop risk assessment instruments with adequate predictive ability. While a number of studies have suggested that well-studied static risk assessment instruments such as the Violence Risk Appraisal Guide (VRAG) (67), HCR-20 (68) and the Psychopathy Checklist (PCL-R) (69, 70) can be used to predict violence and reconvictions among ID offenders (17, 24, 36), these instruments were not developed for use in ID populations, and might therefore lack variables that can be predictive specifically in these individuals. Our study presents data on associations between ID, clinical, sociodemographic and offense variables, and criminal recidivism. These results should not be mistaken as entailing predictive power on individual level (71, 72). However, these group level associations can be of importance in identifying potential risk and protective factors among offenders with ID, in future attempts to develop prediction models of criminal recidivism in this specific population. In addition, while static risk assessments are important in prediction, they are of slightly less use to clinicians in their aim to reduce risk and customize therapeutic interventions. In forensic psychiatric clinical practices, risk assessments serve partially as material for targeting treatment interventions, and thus, clinical and dynamic variables are of greater interest. Our findings are useful in order to tailor treatment programs and adapt adequate preventive measures among ID offenders.
Using data from the FPA, ID diagnoses in the current study were ascertained based on a structured assessment of intellectual level and adaptive behavior and thus in concordance with current diagnostic criteria (73–75). This is a strength since several previous studies on ID offenders suffer from methodological weaknesses including an uncertain definition of ID (47). Using register data, we were able to include 259 ID offenders, which is a considerable amount of individuals in similar research contexts. We were able to study reconvictions during a period of up to 17 years following a sentence to forensic psychiatric care, which addresses the well-known problem in ID offender research, namely, low frequency base-rates of outcome. However, using data from the FPA inevitably entails a selected population of offenders, since only offenders of serious crimes (where incarceration is an applicable sanction) are included. Consequently, our results cannot be generalized to offenders of less severe crimes. In addition, our study population consists of offenders sentenced to forensic psychiatric care in Sweden. However, different countries have different regulations concerning offenders with mental disorders. The Swedish judicial system deviates from many others by not practicing insanity defense legislation. Offenders with severe mental disorders are ascribed legal responsibility and sentences are imposed. Individuals in forensic psychiatric care in Sweden might consequently not be identical to forensic psychiatric populations in other countries, possibly hampering generalizability of results. However, the Swedish system is in accordance with the basic principle of most developed countries, suggesting that an individual who has committed a crime under the influence of a severe mental disorder should not be sentenced prison. We therefore have reason to believe that the Swedish forensic psychiatric population consists of substantially the same patient categories as forensic populations in other countries.
It is important to note that our results present data on recidivism following a sentence to forensic psychiatric care, and not following discharge. An important limitation of the study is that it does not consider time at risk. The main reason is that the eligible registers had inadequate data on discharge dates for individuals in forensic psychiatric care, since the Swedish Patient Register started register specific data for inpatient involuntary psychiatric care in 2010 (representative for the Swedish Patient Register, personal communication, 19 October 2021). This could bias the results in two ways. Firstly, the risk of criminal recidivism is supposedly lower during incarceration. Secondly, there might be a difference in duration of inpatient treatment between offenders with and without ID. Studies comparing the duration of stay in inpatient facilities for ID and non-ID offenders present diverging results (76, 77). However, according to the Swedish National Forensic Psychiatric Register [initiated in 2008 and reaching 96% coverage by 2010 (78)], among individuals sentenced to forensic psychiatric care in Sweden between 2009 and 2021, the median length of stay among individuals with ID equals the average in the entire group including all diagnoses (59 vs. 58 months) (79). It should be noted, that these register data are based on main diagnosis and do not consider comorbidity. An individual with psychosis or affective disorder and concurrent ID might therefore not be registered in the ID group. Offenders with ID have been suggested as presenting with more severe symptoms and lower levels of educational and economic resources, personal strengths and social support than offenders with other mental disorders (77), which could induce a higher level of treatment measures and support, influencing recidivism risk. Unfortunately, our data cannot determine if a longer duration of inpatient care contributed to a lower risk of reconviction among offenders with ID.
A limitation of the study, shared with most other studies on ID offenders, is the sample size. The limited sample of ID offenders hampers certain estimates, such as sub-analyses of clinical categories or female ID offenders. The observation that ID was not associated with increased or decreased recidivism risk among female offenders is of interest, however, data had insufficient statistical power and further studies would be needed to verify this finding.
Individuals with ID are entitled to specific support in Sweden, according to the Act concerning Support and Service for Persons with Certain Functional Impairments (32). This legislation guarantees support for people with extensive functional impairment, such as ID, ensuring that they receive good living conditions and the service and help they need in daily life. Since the majority of individuals who were diagnosed with ID during the FPA were not identified as having ID prior to the assessment (12), it is plausible that the diagnosis could effectuate extra support, both during inpatient care (counseling and daily activities) but especially following discharge (financial support, adapted housing, group home, personal assistance, and contact with habilitation services) which might influence the risk of criminal recidivism. Our finding that the risk of criminal recidivism was lower among male offenders with ID can therefore be regarded as aligned with the legislator’s intention.
The most crucial finding from the current study was that offenders with ID who were sentenced to forensic psychiatric care presented with lower risk of criminal recidivism compared to offenders with other mental disorders. This finding is contrary to data from the meta-analysis by Bonta et al. (14). It highlights the importance of adequate diagnostic terms and definitions, since Bonta et al. employed the term intellectual impairment, which includes, but is not specific to, ID.
Another important finding was that young age and male sex; factors associated with increased risk of offending and re-offending in offender populations, were not associated with increased risk of re-offending among individuals with ID. This is clinically relevant, as many risk assessment instruments include age and sex. The increased risk associated with low age and male sex is so well-established that it will presumably impact the clinical risk assessment, even if actuarial instruments are not used.
Adequate knowledge of recidivism risk and factors associated with increased or decreased risk in clinical subgroups of offenders, such as ID offenders, is of utmost importance to the treating psychiatrist in the forensic psychiatric setting, both in creating treatment plans, in risk assessment and in communication with the court and other representatives from the criminal justice system.
Data availability statement
The datasets presented in this article are not readily available because the present study is based upon data from Swedish National Registers. Swedish Data Protection Laws and the Swedish Ethical Review Authority exert joint protection of register data. Study data is consequently not publicly available. Other researchers may, however, contact Statistics Sweden and the Swedish National Board of Health and Welfare to get access to data from included registers. Requests to access the datasets should be directed to Department of Medical Epidemiology and Biostatistics in Karolinska Institutet, aW50ZXJuc2VydmljZUBtZWIua2kuc2U=.
Ethics statement
The studies involving human participants were reviewed and approved by the Regional Ethical Review Board in Stockholm (2017/2531-31/5). Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
HL collected the data. HE and QC organized the database. HE performed the statistical analyses. HE analyzed the results supervised by TH and QC, and wrote the first draft of the manuscript. TH, HL, PA, and QC proposed manuscript revisions. All authors contributed to the design of the study and conclusion and finally read and approved the submitted version of the manuscript.
Funding
This work was supported by the Stiftelsen Sävstaholm (ST 2020-001 and 2021-005), the Thuring Foundation (2020-00570), and the Swedish Mental Health Fund.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.1011984/full#supplementary-material
References
1. Barron P, Hassiotis A, Banes J. Offenders with intellectual disability: a prospective comparative study. J Intellect Disabil Res. (2004). 48:69–76. doi: 10.1111/j.1365-2788.2004.00581.x
2. Vinkers DJ. Pre-trial reported defendants in the Netherlands with intellectual disability, borderline and normal intellectual functioning. J Appl Res Intellect Disabil. (2013) 26:357–61. doi: 10.1111/jar.12030
3. Harris JC. Intellectual Disability Understanding its Development, Causes, Classification, Evaluation, and Treatment. New York, NY: Oxford University Press (2006). p. 79–98. doi: 10.1093/oso/9780195178852.001.0001
4. Maulik PK, Mascarenhas MN, Mathers CD, Dua T, Saxena S. Prevalence of intellectual disability: a meta-analysis of population-based studies. Res Dev Disabil. (2011) 32:419–36. doi: 10.1016/j.ridd.2010.12.018
5. Buckley N, Glasson EJ, Chen W, Epstein A, Leonard H, Skoss R, et al. Prevalence estimates of mental health problems in children and adolescents with intellectual disability: a systematic review and meta-analysis. Aust N Z J Psychiatry. (2020) 54:970–84. doi: 10.1177/0004867420924101
6. Cooper S-A, Smiley E, Morrison J, Williamson A, Allan L. Mental ill-health in adults with intellectual disabilities: prevalence and associated factors. Br J Psychiatry. (2007) 190:27–35. doi: 10.1192/bjp.bp.106.022483
7. Hayes S. Criminal behavior and intellectual and developmental disabilities: an epidemiological perspective. In: Lindsay WR, Taylor JL editors. The Wiley Handbook on Offenders with Intellectual and Developmental Disabilities: Research, Training, and Practice. Hoboken, NJ: John Wiley and Sons Ltd (2018). p. 21–37. doi: 10.1002/9781118752982.ch2
8. Svennerlind C, Nilsson T, Kerekes N, Andine P, Lagerkvist M, Forsman A, et al. Mentally disordered criminal offenders in the Swedish criminal system. Int J Law Psychiatry. (2010) 33:220–6. doi: 10.1016/j.ijlp.2010.06.003
9. Sveriges Riksdag. Prop. 1990/91:58 Psykiatrisk Tvångsvård m.m. (1990). Available online at: https://www.riksdagen.se/sv/dokument-lagar/dokument/proposition/om-psykiatrisk-tvangsvard-mm_GE0358/html (accessed November 28, 1990).
10. Chaplin E, McCarthy J, Underwood L, Forrester A, Hayward H, Sabet J, et al. Characteristics of prisoners with intellectual disabilities. J Intellect Disabil Res. (2017) 61:1185–95. doi: 10.1111/jir.12441
11. Ray I, Simpson AIF, Jones RM, Shatokhina K, Thakur A, Mulsant BH. Clinical, demographic, and criminal behavior characteristics of patients with intellectual disabilities in a canadian forensic program. Front Psychiatry. (2019) 10:760. doi: 10.3389/fpsyt.2019.00760
12. Edberg H, Chen Q, Andiné P, Larsson H, Hirvikoski T. Clinical characteristics and pharmacological treatment of individuals with and without intellectual disability in pre-trial assessment—a population-based study. Front Psychiatry. (2020) 11:573989. doi: 10.3389/fpsyt.2020.573989
13. Edberg H, Chen Q, Andiné P, Larsson H, Hirvikoski T. Crimes and sentences in individuals with intellectual disability in a forensic psychiatric context: a register-based study. Epidemiol Psychiatr Sci. (2022) 31:e2. doi: 10.1017/S2045796021000718
14. Bonta J, Blais J, Wilson HA. A theoretically informed meta-analysis of the risk for general and violent recidivism for mentally disordered offenders. Aggr Violent Behav. (2014) 19:278–87. doi: 10.1016/j.avb.2014.04.014
16. Gibson R. Differential diagnosis of oligophrenia. AMA Am J Dis Child. (1952) 83:151–3. doi: 10.1001/archpedi.1952.02040060017001
17. Gray NS, Fitzgerald S, Taylor J, MacCulloch MJ, Snowden RJ. Predicting future reconviction in offenders with intellectual disabilities: the predictive efficacy of VRAG, PCL-SV, and the HCR-20. Psychol Assess. (2007) 19:474–9. doi: 10.1037/1040-3590.19.4.474
18. Constantine R, Andel R, Petrila J, Becker M, Robst J, Teague G, et al. Characteristics and experiences of adults with a serious mental illness who were involved in the criminal justice system. Psychiatr Serv. (2010) 61:451–7. doi: 10.1176/ps.2010.61.5.451
19. Hall DL, Miraglia RP, Lee LW, Chard-Wierschem D, Sawyer D. Predictors of general and violent recidivism among SMI prisoners returning to communities in New York State. J Am Acad Psychiatry Law. (2012) 40:221–31.
20. Torgersen LJ. Factors related to Recidivism Among Mentally Disordered Offenders: Differential Impact of Historical and Dynamic Clinical Indicators Across Risk Level [Dissertation]. New York, NY: University at Albany (2013).
21. Pflueger MO, Franke I, Graf M, Hachtel H. Predicting general criminal recidivism in mentally disordered offenders using a random forest approach. BMC Psychiatry. (2015) 15:62. doi: 10.1186/s12888-015-0447-4
22. Canales DD, Campbell MA, Wei R, Totten AE. Prediction of general and violent recidivism among mentally disordered adult offenders: test of the level of service/risk–need–responsivity (LS/RNR) instrument. Crim Justice Behav. (2014) 41:971–91. doi: 10.1177/0093854814523003
23. Grann M, Danesh J, Fazel S. The association between psychiatric diagnosis and violent re-offending in adult offenders in the community. BMC Psychiatry. (2008) 8:92. doi: 10.1186/1471-244X-8-92
24. Fitzgerald S, Gray NS, Alexander RT, Bagshaw R, Chesterman P, Huckle P, et al. Predicting institutional violence in offenders with intellectual disabilities: the predictive efficacy of the VRAG and the HCR-20. J Appl Res Intell Disabil. (2013) 26:384–93. doi: 10.1111/jar.12032
25. Winter N, Holland AJ, Collins S. Factors predisposing to suspected offending by adults with self-reported learning disabilities. Psychol Med. (1997) 27:595–607. doi: 10.1017/S0033291797004777
26. Lindsay WR, Beail N. Risk assessment: actuarial prediction and clinical judgement of offending incidents and behaviour for intellectual disability services. J Appl Res Intell Disabil. (2004) 17:229–34. doi: 10.1111/j.1468-3148.2004.00212.x
27. Janković M, Masthoff E, Spreen M, de Looff P, Bogaerts SA. Latent class analysis of forensic psychiatric patients in relation to risk and protective factors. Front Psychol. (2021) 12:695354. doi: 10.3389/fpsyg.2021.695354
28. Latvala A, Tideman M, Søndenaa E, Larsson H, Butwicka A, Fazel S, et al. Association of intellectual disability with violent and sexual crime and victimization: a population-based cohort study. Psychol Med. (2022) [Online ahead of print]. doi: 10.1017/S0033291722000460
29. Fogden BC, Thomas SD, Daffern M, Ogloff JR. Crime and victimisation in people with intellectual disability: a case linkage study. BMC Psychiatry. (2016) 16:170. doi: 10.1186/s12888-016-0869-7
30. Hodgins S. Mental disorder, intellectual deficiency, and crime: evidence from a birth cohort. Arch Gen Psychiatry. (1992) 49:476–83. doi: 10.1001/archpsyc.1992.01820060056009
31. Raina P, Lunsky Y. A comparison study of adults with intellectual disability and psychiatric disorder with and without forensic involvement. Res Dev Disabil. (2010) 31:218–23. doi: 10.1016/j.ridd.2009.09.008
32. Independent Living Institute. Act Concerning Support And Service For Persons With Certain Functional Impairments (LSS). Stockholm: Independent Living Institute (1993). p. 387.
33. Bonta J, Law M, Hanson K. The prediction of criminal and violent recidivism among mentally disordered offenders: a meta-analysis. Psychol Bull. (1998) 123:123–42. doi: 10.1037/0033-2909.123.2.123
34. Noland E, Strandh M. Historical, clinical and situational risk factors for post-discharge recidivism in forensic psychiatric patients – A Swedish registry study. Int J Law Psychiatry. (2021) 79:101749. doi: 10.1016/j.ijlp.2021.101749
35. Lofthouse RE, Totsika V, Hastings RP, Lindsay WR, Hogue TE, Taylor JL. How do static and dynamic risk factors work together to predict violent behaviour among offenders with an intellectual disability?: static and dynamic risk factors. J Intellect Disabil Res. (2014) 58:125–33. doi: 10.1111/j.1365-2788.2012.01645.x
36. Fitzgerald S, Gray NS, Taylor J, Snowden RJ. Risk factors for recidivism in offenders with intellectual disabilities. Psychol Crime Law. (2011) 17:43–58. doi: 10.1080/10683160903392293
37. Martí-Agustí G, Muñoz García-Largo L, Martin-Fumadó C, Martí-Amengual G, Gómez-Durán EL. Intellectual disability: criminality, assessment and forensic issues. Span J Leg Med. (2019) 45:155–62. doi: 10.1016/j.remle.2019.03.002
38. Cockram J. Careers of offenders with an intellectual disability: the probabilities of rearrest. J Intellect Disabil Res. (2005) 49:525–36. doi: 10.1111/j.1365-2788.2005.00707.x
39. Lindsay WR, Carson D, Holland AJ, Taylor JL, O’Brien G, Wheeler JR. The impact of known criminogenic factors on offenders with intellectual disability: previous findings and new results on ADHD. J Appl Res Intell Disabil. (2013) 26:71–80. doi: 10.1111/jar.12011
40. Lindsay WR, Steptoe L, Wallace L, Haut F, Brewster E. An evaluation and 20-year follow-up of a community forensic intellectual disability service. Crim Behav Ment Health. (2013) 23:138–49. doi: 10.1002/cbm.1859
41. Jones J. Persons with intellectual disabilities in the criminal justice system:review of issues. Int J Offender Ther Comp Criminol. (2007) 51:723–33. doi: 10.1177/0306624X07299343
42. Holland T, Clare ICH, Mukhopadhyay T. Prevalence of ‘criminal offending’ by men and women with intellectual disability and the characteristics of ‘offenders’: implications for research and service development. J Intellect Disabil Res. (2002) 46:6–20. doi: 10.1046/j.1365-2788.2002.00001.x
43. Atladottir HO, Gyllenberg D, Langridge A, Sandin S, Hansen SN, Leonard H, et al. The increasing prevalence of reported diagnoses of childhood psychiatric disorders: a descriptive multinational comparison. Eur Child Adolesc Psychiatry. (2014) 24:173–83. doi: 10.1007/s00787-014-0553-8
44. Elsabbagh M, Divan G, Koh Y-J, Kim YS, Kauchali S, Marcín C, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. (2012) 5:160–79. doi: 10.1002/aur.239
45. Rydell M, Lundström S, Gillberg C, Lichtenstein P, Larsson H. Has the attention deficit hyperactivity disorder phenotype become more common in children between 2004 and 2014? Trends over 10 years from a Swedish general population sample. J Child Psychol Psychiatry. (2018) 59:863–71. doi: 10.1111/jcpp.12882
46. Polanczyk GV, Willcutt EG, Salum GA, Kieling C, Rohde LA. ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. Int J Epidemiol. (2014) 43:434–42. doi: 10.1093/ije/dyt261
47. Taylor JL, Lindsey WR. Offenders with intellectual and developmental disabilities - Future Directions for Research and Practice. In: Lindsay WR, Taylor JL editors. The Wiley Handbook on Offenders with Intellectual and Developmental Disabilities: Research, Training, and Practice. Hoboken, NJ: John Wiley & Sons Ltd (2018). p. 453–71. doi: 10.1002/9781118752982.ch25
48. Baudin C, Nilsson T, Wallinius M, Sturup J, Andiné P. A 24-year follow-up study on recidivism in male mentally disordered sexual offenders with and without psychotic disorders. J Forensic Sci. (2020) 65:1610–8. doi: 10.1111/1556-4029.14327
49. Delfin C, Krona H, Andiné P, Ryding E, Wallinius M, Hofvander B. Prediction of recidivism in a long-term follow-up of forensic psychiatric patients: Incremental effects of neuroimaging data. PLoS One. (2019) 14:e0217127. doi: 10.1371/journal.pone.0217127
50. Nilsson T, Wallinius M, Gustavson C, Anckarsater H, Kerekes N. Violent recidivism: a long-time follow-up study of mentally disordered offenders. PLoS One. (2011) 6:e25768. doi: 10.1371/journal.pone.0025768
51. Wechsler D. Wechsler Adult Intelligence Scale. 4th ed. San Antonio, TX: Pearson (2008). doi: 10.1037/t15169-000
52. Statistics Sweden.Longitudinal Integration Database for Health Insurance and Labor Market Studies (LISA) 1990-2013 [Internet]. (2015). Available online at: https://www.scb.se (accessed June, 2021).
53. Ludvigsson JF, Almqvist C, Bonamy AK, Ljung R, Michaelsson K, Neovius M, et al. Registers of the Swedish total population and their use in medical research. Eur J Epidemiol. (2016) 31:125–36. doi: 10.1007/s10654-016-0117-y
54. Tabachnick BG, Fidell LS. Using Multivariate Statistics. 7th ed. Boston, MA: Pearson Education (2019). p. 58–60.
55. Ginsberg Y, Lindefors N. Methylphenidate treatment of adult male prison inmates with attention-deficit hyperactivity disorder: randomised double-blind placebo-controlled trial with open-label extension. Br J Psychiatry. (2012) 200:68–73. doi: 10.1192/bjp.bp.111.092940
56. Zuddas A, Banaschewski T, Coghill D, Stein MA. ADHD Treatment: Oxford Textbook of Attention Deficit Hyperactivity Disorder. Oxford: Oxford University Press (2018). p. 379–92. doi: 10.1093/med/9780198739258.001.0001
57. Chang Z, Lichtenstein P, Långström N, Larsson H, Fazel S. Association between prescription of major psychotropic medications and violent reoffending after prison release. J Am Med Assoc. (2016) 316:1798–807. doi: 10.1001/jama.2016.15380
58. Gendreau P, Little T, Goggin C. A meta−analysis of the predictors of adult offender recidivism: what works! Criminology. (1996) 34:575–608. doi: 10.1111/j.1745-9125.1996.tb01220.x
59. Eisenberg MJ, van Horn JE, Dekker JM, Assink M, van der Put CE, Heniks J, et al. Static and dynamic predictors of general and violent criminal offense recidivism in the forensic outpatient population: a meta-analysis. Crim Justice Behav. (2019) 46:732–50. doi: 10.1177/0093854819826109
60. Phillips HK, Gray NS, MacCulloch SI, Taylor J, Moore SC, Huckle P, et al. Risk assessment in offenders with mental disorders: relative efficacy of personal demographic, criminal history, and clinical variables. J Interpers Viol. (2005) 20:833–47. doi: 10.1177/0886260504272898
61. Dean K, Singh S, Kemp R, Johnson A, Nielssen O. Characteristics and Re-offending rates amongst individuals found not guilty by reason of mental illness (NGMI): a comparison of men and women in a 25-year Australian Cohort. Int J Forensic Ment Health. (2020) 20:17–30. doi: 10.1080/14999013.2020.1795011
62. Walmsley R. World Female Imprisonment List. (2017). Available online at: https://www.prisonstudies.org/sites/default/files/resources/downloads/world_female_prison_4th_edn_v4_web.pdf [accessed February 4, 2022).
63. Lauritsen JL, Heimer K, Lynch JP. Trends in the gender gap in violent offending: new evidence from the national crime victimization survey. Criminology. (2009) 47:361–99. doi: 10.1111/j.1745-9125.2009.00149.x
64. Schwartz J, Steffensmeier D, Zhong H, Ackerman J. Trends in the gender gap in violence: reevaluating NCVS and other evidence*. Criminology. (2009) 47:401–25. doi: 10.1111/j.1745-9125.2009.00152.x
65. Lindsay WR, Hogue TE, Taylor JL, Steptoe L, Mooney P, O’Brien G, et al. Risk assessment in offenders with intellectual disability: a comparison across three levels of security. Int J Offender Ther Comp Criminol. (2008) 52:90–111. doi: 10.1177/0306624X07308111
66. Alexander RT, Crouch K, Halstead S, Piachaud J. Long-term outcome from a medium secure service for people with intellectual disability. J Intellect Disabil Res. (2006) 50:305–15. doi: 10.1111/j.1365-2788.2006.00806.x
67. Harris GT, Rice ME, Quinsey VL. Violent recidivism of mentally disordered offenders:the development of a statistical prediction instrument. Crim Justice Behav. (1993) 20:315–35. doi: 10.1177/0093854893020004001
68. Webster C, Douglas K, Eaves D, Hart S. HCR-20: Assessing Risk for Violence (Version 2). Burnaby, BC: Simon Fraser University (1997).
69. Hare RD. The Hare Psychopathy Checklist. Toronto, ON: Multi-Health Systems (1991). doi: 10.1037/t01167-000
72. Varga TV, Niss K, Estampador AC, Collin CB, Moseley PL. Association is not prediction: a landscape of confused reporting in diabetes – A systematic review. Diabetes Res Clin Pract. (2020) 170:108497. doi: 10.1016/j.diabres.2020.108497
73. APA. Diagnostic and Statistical Manual of Mental Disorders, Text Revision (DSM-IV-TR). Washington, DC: American Psychiatric Association (2000).
74. APA. Diagnostic and Statistical Manual of Mental Disorders. 5. Arlington, VA: American Psychiatric Association (2013).
75. WHO. The ICD-10 Classification of Mental and behavioural Disorders : Diagnostic Criteria for Research. Geneva: World Health Organization (1993).
76. Lin E, Barbaree H, Selick A, Ham E, Wilton AS, Lunsky Y. Intellectual and developmental disabilities and Ontario’s forensic inpatient system: a population-based cohort study. Psychol Crime Law. (2017) 23:914–26. doi: 10.1080/1068316X.2017.1346100
77. Lunsky Y, Gracey C, Koegl C, Bradley E, Durbin J, Raina P. The clinical profile and service needs of psychiatric inpatients with intellectual disabilities and forensic involvement. Psychol Crime Law. (2011) 17:9–23. doi: 10.1080/10683160903392277
78. Degl’ Innocenti A, Hassing LB, Lindqvist A-S, Andersson H, Eriksson L, Hanson FH, et al. First report from the Swedish National Forensic Psychiatric Register (SNFPR). Int J Law Psychiatry. (2014) 37:231–7. doi: 10.1016/j.ijlp.2013.11.013
79. RättspsyK. New Annual Report Focuses On Somatic Morbidity And Health Promotion Efforts 2021. (2021). Available online at: https://rattspsyk.registercentrum.se/ (accessed July 14, 202)].
Keywords: intellectual disability, criminal recidivism, forensic psychiatry, neurodevelopmental disorder, crime, offender, survival analysis
Citation: Edberg H, Chen Q, Andiné P, Larsson H and Hirvikoski T (2022) Criminal recidivism in offenders with and without intellectual disability sentenced to forensic psychiatric care in Sweden—A 17-year follow-up study. Front. Psychiatry 13:1011984. doi: 10.3389/fpsyt.2022.1011984
Received: 04 August 2022; Accepted: 05 September 2022;
Published: 21 September 2022.
Edited by:
Gábor Gazdag, Jahn Ferenc Dél-Pesti Kórház és Rendelõintézet, HungaryReviewed by:
Ebba Noland, Umeå University, SwedenVicenç Tort Herrando, Parc Sanitari Sant Joan de Déu, Spain
Copyright © 2022 Edberg, Chen, Andiné, Larsson and Hirvikoski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hanna Edberg, aGFubmEuZWRiZXJnQGtpLnNl