 Nils-Torge Telle
Nils-Torge Telle Jörn Moock1
Jörn Moock1 Wulf Rössler
Wulf Rössler Wolfram Kawohl
Wolfram Kawohl- 1Competence Tandem Integrated Services, Innovation Incubator, Leuphana University of Lüneburg, Lüneburg, Germany
- 2Laboratory of Neuroscience (LIM 27), Institute of Psychiatry, University of Sao Paulo, Sao Paulo, Brazil
- 3University of Zurich, Zurich, Switzerland
- 4Department of Psychiatry, Psychotherapy, and Psychosomatics, Center for Social Psychiatry, Psychiatric Hospital, University of Zurich, Zurich, Switzerland
Sickness absence from work due to experienced distress and mental health issues has continuously increased over the past years in Germany. To investigate how this alarming development can be counteracted, we conducted a randomized controlled trial evaluating a job coaching intervention to maintain the working capacity of members of staff and ultimately prevent sickness absence. Our sample included N = 99 employees who reported mental distress due to work-related problems. The intervention group (n = 58) received between 8 and 12 individual job coaching sessions in which they worked with a professional job coach to reduce their mental distress. The control group (n = 41) received a brochure about mental distress. Data were collected before the start of the study, at the end of the job coaching intervention, and at a 3-month follow-up. These data included the number of sickness absence days as the primary outcome and questionnaire measures to assess burnout indicators, life satisfaction, and work-related experiences and behaviors. Compared with the control group, the results indicated no reduction in sickness absence in the intervention group but fewer depressive symptoms, a heightened ability of the participants to distance themselves from work, more experience of work-related success, less depletion of emotional resources, and a greater satisfaction with life when participants had received the job coaching. Thus, although we could not detect a reduction in sickness absence between the groups, job coaching was shown to be a viable intervention technique to benefit employees by contributing to re-establish their mental health. We discuss the implications of the study and outline future research.
Introduction
Work-related mental distress can often develop into more severe forms of mental illness that require therapeutic interventions and cause longer periods of sickness absence. During the last decade, sickness absence in Germany due to experienced mental illness has increased considerably (1) and is generally considered to be a serious problem in Europe (2). Mental illness may also occur as psychological comorbidities of somatic disorders, a fact only rarely noted by most physicians (3). This circumstance may contribute to the increasing number of sickness absence days (1), which ultimately represents a temporary loss of human capital and diminished organizational productivity.
Encouraging results regarding the effectiveness of job coaching have been reported for people with mental disorders receiving individual placement and support (IPS) interventions (4–6) to reintegrate them into the job market. However, it may be more effective to prevent people with mental illness or strain from losing their jobs in the first place. In this regard, supported employment interventions are often used in clinical practice and represent an established tool to help distressed employees maintain their jobs (7). IPS follows eight core principles that are listed in Table 1. Thus, IPS-based job coaching, as a specific supported employment tool, may represent a measure that companies could introduce in order to sustain the ability of their workforce to work viably (8–10).
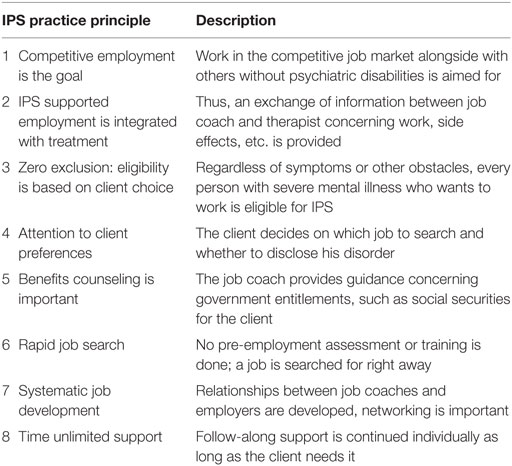
Table 1. The practice principles of IPS Supported Employment according to the Dartmouth IPS Supported Employment Center (http://www.dartmouth.edu/~ips/page48/page79/files/ips-practice-principles-002880029.pdf).
Recent meta-analytic evidence provided by Theeboom et al. (11) generally indicates the effectiveness of job coaching interventions in organizational contexts. The authors of this study report several benefits of such interventions, such as improved well-being, more effective coping and better work attitudes. More specifically, Duijts et al. (12) investigated whether preventive job coaching for employees who were previously identified as being at risk for sickness absence due to psychosocial health complaints [see Ref. (13)] could reduce sickness absence. These researchers found a positive effect of job coaching on objective sickness absence due to psychosocial health complaints in the mid-term (baseline to 8-month follow-up) but only for the intention-to-treat analyses in the long term (8–12 months and the entire year after baseline follow-up). Moreover, the authors report significant effects of job coaching in terms of an improvement in the participants’ self-rated health, less burnout exhaustion as well as fewer depressive reactions for the 1 year after the baseline follow-up period for the per-protocol analyses.
Rationale of the Present Trial and Hypotheses
Although the present study is similar to that of Duijts et al. (12), it differs in three ways. First, the present sample includes employees who subjectively felt mentally distressed and thought that they would benefit from job coaching, as opposed to employees who were specifically identified as being “‘at risk’ for sickness absence due to psychosocial health complaints” [(12), p. 766]. Second, whereas Duijts et al. (12) conducted two three-way consultations during the job coaching intervention by including the related supervisor of the employee in the second and the last coaching sessions, we excluded any third parties and the job coaching was kept confidential between the job coach and the employee. Third, to the best of our knowledge, the present study is the first to examine the effects of job coaching in organizational contexts within a German-speaking population. Based on encouraging IPS research (5, 6) and the results reported by Duijts et al. (12), we aim to investigate (a) whether job coaching can reduce the number of sickness absence days at a 3-month follow-up and (b) whether job coaching improves the mental health of employees who feel distressed.
Materials and Methods
Ethics
The present study has been registered under ISRCTN02422335. It was approved by the ethics committee of Leuphana University of Lüneburg and has been conducted in accordance with the Declaration of Helsinki (14). All participants gave their written informed consent prior to commencing with the study. A study protocol (14) has been published.
The Job Coaching Intervention
We evaluate the concept of an IPS-based job coaching intervention for mentally distressed employees. Traditional IPS has been conceptualized to reintegrate people with mental illness into the open job market with the help of a job coach. In our study, an IPS-based job coaching intervention was tested for its ability to sustain the employees’ capacity to work and support employees who felt hampered in their capacity to work due to mental distress or mental illness that they experienced. The intervention comprises employee-centered, individual job coaching with the ultimate goal of maintaining the job. The job coaching was specifically tailored toward each employee’s problems and the current individual job situation. Furthermore, it enabled the employees to help themselves. The coaching entailed working on a personal job-related problem with a specially trained job coach. During the job coaching intervention, the employees and the job coach first jointly defined personal goals, which the job coach evaluated on a regular basis to facilitate goal achievement. Examples for such goals are to establish communication with the person’s superior, to find a therapist, to make a personal plan for breaks during the working hours, and to seek and handle social interaction at the workplace. The intervention included ~8–12 coaching sessions over a timespan of ~3 months. Due to the highly individualized character of IPS, many parameters, such as length of session, are not standardized but are usually no longer than 1 h.
Study Design
The present study was a randomized controlled trial using a one-factorial design with two groups (job coaching intervention vs. control). After having given their written informed consent, the participants were randomly assigned to either the intervention or the control group via a randomized participation slot list in blocks of 10. After a new participant was assigned a participant ID by one of the job coaches, the project coordinator was solely told the ID and assigned it to a free slot on the participation list. Thus, slots were filled anonymously with participant IDs and consecutively as participants were recruited. The intervention group received the IPS-based job coaching. Participants in the control group were given an information brochure about how to best cope with mental distress.
Data were collected from each participant at three different points in time as part of a standardized interview procedure, including different questionnaires (see Table 2): immediately after the employees were assigned to the intervention or the control group (T0), after 3 months (T1; the end of the job coaching for participants of the intervention group) and after 6 months (T2; 3-month follow-up). The interviews were conducted by a person who had not interacted with the employees before and was, thus, naïve about their specific situations.
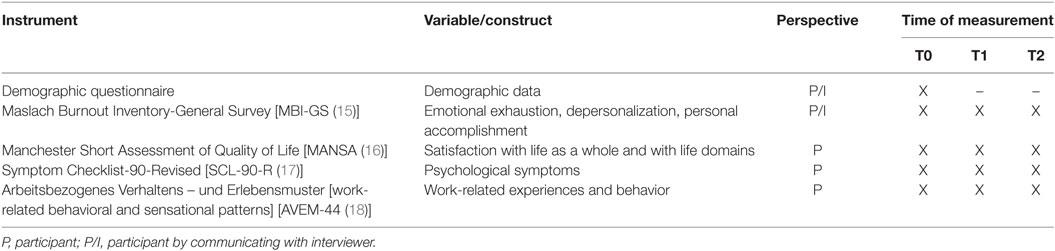
Table 2. Overview of questionnaire-based instruments and when they were administered.
Sample
In order to detect a notable reduction of sickness absence days of 30%, we calculated a required total sample size of N = 108 per group. This calculated sample size is based on a statistical power of 0.8 and an alpha level of α = 0.05, with an assumed effect size of Cohen’s d = 0.3, estimated based on available IPS literature, and a total dropout rate of 20% across all measurement time points.
The sample comprised members of staff from 13 different private corporations and federal and public organizations based in northern Germany. We recruited participants who subjectively felt mentally distressed due to work-related issues or circumstances. Participation was voluntary and concealed from employers and work committees. In order to be eligible for participation, the following criteria had to be fulfilled: employee of a cooperation partner of the present study, self-report of psychological distress, voluntary participation, ability to give informed consent, and age between 18 and 67 (working age). Exclusion criteria were the need for present psychiatric inpatient treatment as well as acute suicidality.
Figure 1 shows the flow of participants in our randomized controlled trial and Table 3 shows the baseline data of the intervention and control group for age, gender, and the different clinical characteristics assessed with the different psychometric questionnaires we administered.
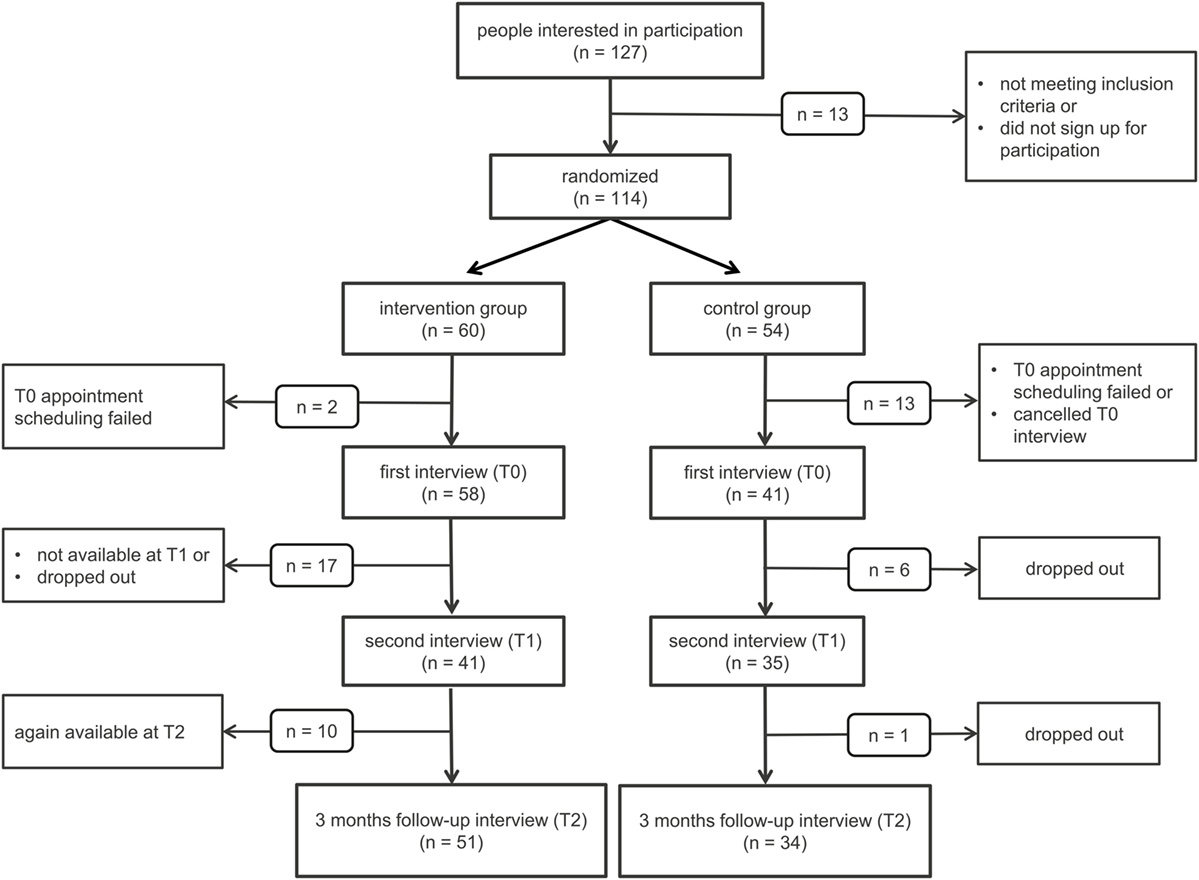
Figure 1. Flow of participants. n, number of participants.
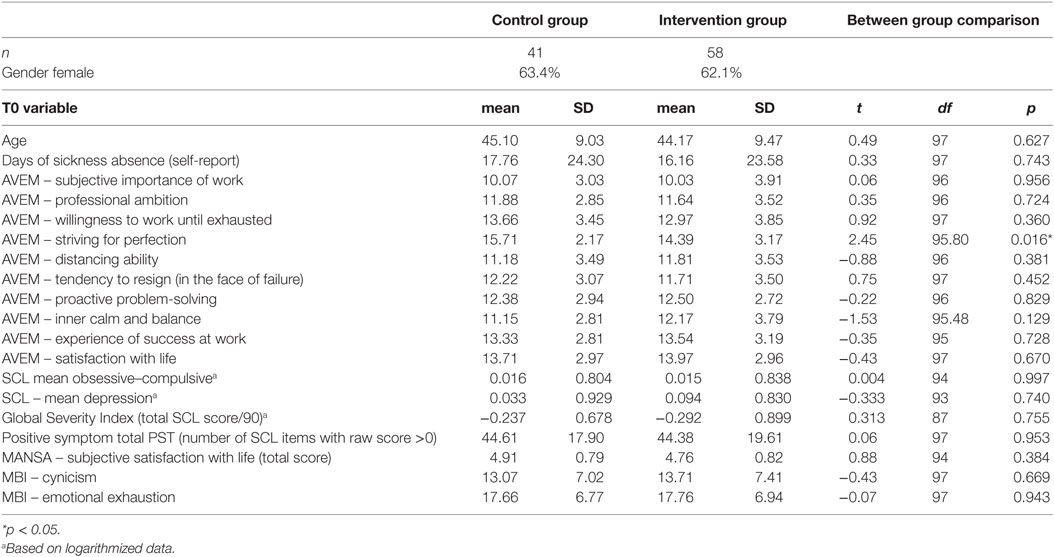
Table 3. Overview and comparison of baseline data between groups.
Data Collection and Dependent Variables
Participants were recruited and data were collected on a rolling basis over a time span of 23 months. The first T0 data of participants was collected in November 2012 and the last participants provided T0 data in April 2014. The first T1 follow-up data were collected in February 2013 and the last T1 follow-up data were collected in July 2014. Regarding T2, the first follow-up data were collected in May 2013 and the last participants provided T2 follow-up data in September 2014. All data collection took place in a one-on-one, face-to-face setting, in a neutral room that was rented specifically for the purpose of the present study. The trial ended as expected after T2 data from the last recruited participant had been collected in September 2014.
The main dependent variable was the self-reported number of days the participants had been absent from work due to illness over the past 6 months (days of sickness absence). This item was included in the demographic questionnaire. Similar to Viering et al. (19), and along with other questionnaires, we also administered the following questionnaire measures to the control and intervention group to assess the participants’ mental health, life satisfaction, and work-related attitudes and behaviors before and after the study: Maslach Burnout Inventory-General Survey (MBI-GS), Manchester Short Assessment of Quality of Life (MANSA), Symptom Checklist-90-Revised (SCL-90-R), and the AVEM-44.
The MBI-GS (15, 20) is a self-report measure to assess the burnout construct with its supposed three dimensions: exhaustion [“fatigue, but without referring to people as the source of those feelings,” (21), p. 224], cynicism [“indifference or a distant attitude toward work” (21), p. 224], and professional efficacy [“social and non-social accomplishments at work” (21), p. 224]. Participants state how often they experience different work-related emotions or have work-related attitudes on a 7-point rating scale ranging from 0 = never to 6 = every day. Past research found satisfactory internal consistencies for the three MBI-GS scales across different occupational groups and nationalities [Cronbach’s alpha for the total sample ranging from 0.75 to 0.86 (22)] and acceptable factorial validity for the three-factor structure (22, 23).
The MANSA (16) is a self-report measure to assess how satisfied people are with their lives. Participants answer 12 of the 16 items on a 7-point satisfaction rating scale ranging from 1 = couldn’t be worse to 7 = couldn’t be better and four items with yes or no. The MANSA has been found to have satisfactory reliability and validity [Cronbach’s alpha = 0.74 (16)].
The SCL-90-R (17) is a self-report measure to assess general psychiatric symptomatology on nine different scales. Participants indicate the severity of symptoms they have experienced over the past 4 weeks on a 5-point rating scale ranging from 0 = not at all to 4 = extremely. The reliability of the SCL-90-R scales can be considered to be between satisfactory and very good [Cronbach’s alpha between 0.74 and 0.97 (24)]. Although the nine dimensions may not represent the best structure of the measure (25, 26), research evidence suggests good concurrent validity (25).
The AVEM-44 is a short version of the self-report AVEM questionnaire that measures the different coping styles that employees use in order to deal with their occupational workload (18). Forty-four statements build 11 scales; the scores are jointly interpreted to represent one of four distinct overall behavioral patterns (health-oriented, protection, risk of excessive demand from oneself, chronic exhaustion, and resignation). For the purposes of the present study, we did not aggregate the data to obtain the patterns but used the sum score of the 11 scales for more detailed analyses. Participants indicate their degree of agreement with different statements on 5-point rating scales ranging from: The statement is… 5 = totally true to 1 = totally not true. Due to high content and structural similarities between the standard and the short form, evidence for their validity apply likewise to both forms (18). Accordingly, the AVEM has been found to have satisfactory convergent, divergent, and criterion validity and Cronbach’s alpha is reported not to be lower than 0.74 for any of the 11 scales (27, 28).
Statistical Analysis
Analyses were carried out using the SPSS statistical software version 22 (SPSS Inc, Chicago, IL, USA) according to the intention-to-treat principle. Baseline characteristics are expressed as mean and SD for continuous variables and percentages for categorical variables, respectively. The effectiveness of the job coaching intervention was evaluated with respect to the self-reported number of sickness absence days, the MBI-GS, the MANSA, the SCL-90-R, and the AVEM-44 measure.
Distributions of data were visually inspected, with several variables violating the assumption of normality. Logarithmic transformation was applied to the variables departing from normality. After the transformation, phobic anxiety, paranoid ideation, somatization, anxiety, psychoticism, hostility, interpersonal sensitivity, experience of social support, professional efficacy, and the positive symptom distress index were still skewed and, thus, excluded from further analysis.
For each of these measures, we conducted regression analyses to investigate whether the changes in scores on the different measures from T0 to T2 were predicted by group affiliation (control or intervention group). In each regression, we controlled for differences in respective T0 values, age, gender, and the professional cluster (private economy, social sector, or public service) of the company/organization. Moreover, we calculated the respective effect sizes Cohen’s d at T2 using the pooled SD in order to account for different group sizes (29). Effect sizes of 0.2, 0.5, and 0.8 were considered as small, medium, and large beneficial effects, respectively (30). Specifically, analyzed sample sizes at T0 were ncontrol = 41 and nintervention = 58; at T1, ncontrol = 35 and nintervention = 41; and at T2, ncontrol = 34 and nintervention = 51. All statistical tests were performed with an alpha level of 0.05. The alpha level was not lowered due to small number of subjects. Additionally, we applied repeated measures ANOVA to investigate any group by time interaction effects for the respective outcome variables.
Results
Randomization Analyses
Comparisons of baseline data showed no significant group differences for gender X2 (1, N = 99) = 0.019, p > 0.05. All comparisons are shown in Table 3. There were no significant differences between the control and intervention group except for one of the AVEM-44 subscales (striving for perfection) for which the control group scored slightly higher.
Reliability Analyses
Table 4 shows the Cronbach’s alpha coefficients for the psychometric instruments at the time points of measurement T0, T1, and T2.
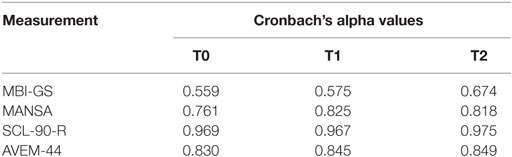
Table 4. Cronbach’s alpha values for the psychometric measurements at the different time points of measurement.
Regression and Repeated Measurements ANOVA Analyses
The self-reported number of sickness absence days – our main outcome variable – was not predicted by group affiliation, p = 0.346, ns. Table 5 details this result and also displays the other regression results for the questionnaire measures, including corresponding effect sizes.
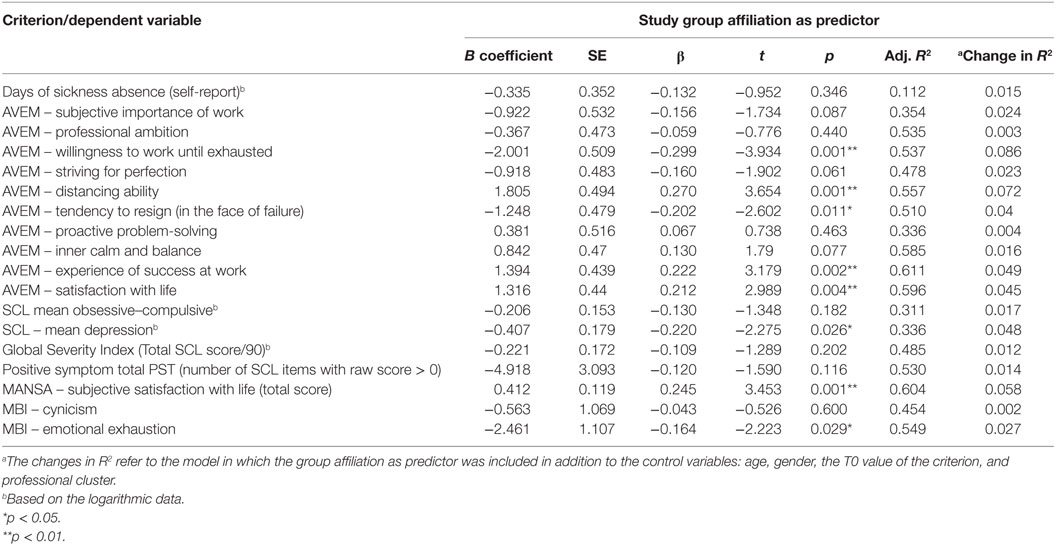
Table 5. Regression results of questionnaire measures.
The regression results shown in Table 5 indicate that some changes in measure and scale values from T0 to T2 were predicted by group affiliation. Participants in the intervention group reported on average fewer depressive symptoms. Moreover, the subscales of the AVEM-44 indicated that job coaching increased the participants’ ability to distance themselves from their work as well as their experience of work-related success. Furthermore, it revealed a reduced tendency to resign in the face of failure and a decreased willingness to work until exhausted. Less depletion of emotional resources was also implied by significantly reduced MBI-GS scores of emotional exhaustion. Life satisfaction significantly increased, which is consistently indicated by the respective AVEM-44 subscale and the MANSA life satisfaction score.
We ran the same regression analyses with the participants’ data obtained at T1. This was done to investigate whether the observed pattern of results at T2 was already present at T1, right after the intervention had ended. All of the scale scores that had failed to be predicted by group affiliation at T2 were also not predicted by group affiliation at T1 (all p > 0.05). Moreover, the scale scores that were significantly influenced by the job coaching intervention at T2 did not prove to be already significant at T1, except for the AVEM-44 subscale of life satisfaction. For this subscale, being in the intervention group predicted a significant increase in life satisfaction scores at T1 with b = 0.96, t(68) = 2.08, p = 0.041.
Effect sizes at T2 indicated that the job coaching had the greatest absolute significant effect on the willingness to work until exhausted (d = 0.82) and on participants’ distancing ability (d = −0.69). The smallest absolute significant effect was observed for emotional exhaustion (d = 0.23).1
In addition to the performed regression analyses, we also checked for any time by group interaction effects using a repeated measures ANOVA. Results mirrored the aforementioned pattern or results of the regression analyses, that is, which effects turned out to be significant and which not, did not change.
Discussion
With the present trial, we evaluated the effectiveness of job coaching as an on-the-job intervention for mentally distressed employees. The application of one-on-one job coaching represents a specific form of supported employment and has been derived from the concept of IPS (4). Contributing to the body of literature on preventive job coaching, we conducted a randomized controlled trial with the self-reported number of sickness absence days as the main outcome criterion. In addition, our study included several questionnaire measures to assess clinical symptoms, burnout indicators, and participants’ satisfaction with different domains of their life, such as their job and their physical and mental health. Both the intervention as well as the control group completed these measures before the study started (T0), after ~3 months (T1), which represented the end of the job coaching sessions for the intervention group, and at a 3-month follow-up (T2).
Regarding self-reported sickness absence days, no significant effect of job coaching was detected when the two groups were compared (at neither T1 nor T2). However, our analyses of the questionnaire measures revealed that compared with the control group the intervention group significantly benefited from the job coaching. Job coaching reduced symptoms of depression as well as emotional exhaustion and improved participants’ distancing ability, their experience of success at work, the tendency to resign, and the satisfaction with their lives. These effects showed for data collected at the 3-month follow-up interview but not directly at the end of the intervention. Immediately after the job coaching had ended, at T1, only the AVEM-44 subscale scores of life satisfaction had already significantly increased.
Generally, our results are consistent with related research that evaluated IPS interventions (4). IPS has been found to be an effective means to reintegrate people with mental disorders into the job market (5). Compared with IPS, the intervention in our trial addressed experienced mental distress at work in an early stage that might have already negatively affected the employees’ work performance. To some extent mirroring our pattern of results, evidence for beneficial effects of job coaching interventions was provided by Duijts et al. (12). These authors also did not find a reduction of “self-reported sickness absence due to psychosocial health complaints” [(12), p. 770] through job coaching, but they reported, however, a reduction of the objective number of sickness absence days in a period from baseline to an 8-month follow-up. Moreover, they also found better self-rated health, less burnout exhaustion and fewer depressive reactions for participants who received job coaching between baseline and 1-year follow-up (12).
Still, there are also more equivocal findings for the effect of coaching interventions on depression, stress levels, or anxiety. While Gyllensten and Palmer (9) reported a significant positive effect on stress and anxiety but not on depression, Grant et al. (8) could not find an effect on anxiety and reported ambiguous relationships for depression and stress. However, meta-analytical findings have recently provided further evidence for the effectiveness of coaching in organizational contexts (11). These findings support the notion that job coaching can improve employees’ well-being, coping abilities, work attitudes, and goal-directed self-regulation. The results of the present research are consistent with this meta-analytical evidence (11) and further corroborate the validity of job coaching as a means to ameliorate employees’ psychological conditions.
Although we did not observe a decline in the self-reported days of sickness absence at a 3-month follow-up between the groups, it could be speculated that this benefit may have a delayed onset. Psychological improvements may need to take effect first to translate into reduced sickness absence. A delayed onset might occur because the psychological effects of job coaching were7 not directly observed at the end of the intervention at T1 but they were present 3 months after the intervention had ended. This fact might indicate that tackling mental distress to create positive behavioral outcomes via job coaching is at least a mid-term process that requires time before the full benefits may become evident. This assumption is, however, somewhat challenged by findings reported by McGonagle et al. (10) who observed coaching benefits immediately at the end of the coaching intervention and also at a 12-week follow-up. Yet, the overall findings reported by McGonagle et al. (10), that is, improved personal well-being but no improved job well-being, are in line with the present results. Still, more research is necessary to further determine the factors that influence and drive the timely dimension in terms of the onset of positive effects of job coaching. Similarly, the generalizability and applicability of job coaching interventions to different work environments and situations should be subject to further research.
Our results still show that job coaching has beneficial outcomes. The effects of improved satisfaction as well as decreased emotional exhaustion and fewer symptoms of depression that we found can contribute to maintaining the work performance of employees. However, it should be noted that job coaching is no therapeutic intervention and is not a substitute for it. When a need for therapy is recognized, the job coach may act as mediator to triangulate between the employee’s supervisor and therapist. This triangulating function adds to the value of job coaching in companies and organizations. It has to be taken into account that disclosure of mental distress or a mental disorder has to be considered deliberately (31). However, a study by Allott et al. (32) revealed that IPS can be done with different disclosure preferences and that disclosure does not predict vocational outcome in persons with recent onset psychosis. If sickness absence can be reduced and jobs can be maintained through job coaching, these effects should also translate into lowered costs and ultimately higher economic returns for the organization. Thus, the introduction of job coaching in organizations would literally pay off.
Limitations
In spite of the promising results found for job coaching as a tool to support mentally distressed employees, some limitations of the present study need to be acknowledged. First, the measurement of the main outcome criterion of sickness absence days needs to be discussed. Participants had to recall their sickness absence days during the past 6 months. Thus, this measure might be inaccurate or prone to recall bias (33, 34). Moreover, it would have been better to ask participants about absence within a shorter timeframe (e.g., 30 or 60 days) as data were collected in 90 days intervals but they had to recall their absence in the past 6 months. Thus, there is an overlap of 3 months between the recalled time periods of sickness absence and the chronological phases of the study. That is, T1 data, collected at the end of the 3 months coaching intervention, include the 3 months prior to the baseline measurement point (T0), since we asked participants to recall their absence in the last 6 months. Similarly, the T2 follow-up data, collected 3 months after the coaching, include the 3 months coaching period. However, T0 data and T2 data, which we investigated with the performed analyses, do not include overlapping time periods since T2 data were collected 6 months after T0. Still, it is important for future studies to address these aspects in the measurement strategy, for example, by only recording data of the intervention period and the follow-up period (e.g., 3 months each) with no overlap, and compare it to baseline data that cover the same period of time prior to the start of the intervention.
Second, the duration of coaching in the present trial may be considered to be rather short compared with, for example, the EQOLISE, the ZInEP or the ZhEPP trials (5, 19, 35). This brevity of coaching may be a reason why we only found partial beneficial effects in our data. Furthermore, we employed only a 3-month follow-up assessment. The follow-up period should be extended since sustainability is an issue in IPS interventions (36). An extended follow-up [see, for example, Ref. (12, 37)] would allow evaluating the sustainability of the intervention and provide a more accurate judgment of its long-term effects.
Third, it needs to be highlighted that the reported internal consistencies of the MBI-GS scale are quite low, with values ranging between 0.559 (T0) and 0.674 (T2). We could not identify any reasons why these coefficients are low, since we administered the standard version of the MBI-GS scale. Although it is widely stated that alpha coefficients should amount to at least 0.70 or greater in order to be regarded as acceptable, Schmitt (38) points out that even if a measure has a lower reliability, this does not necessarily have to be a drawback to its use, if it, for example, covers the construct of interest well. Still, in light of the low internal consistencies of the MBI-GS in the present study, our results for this measure have to be interpreted with caution.
Conclusion
We have shown that job coaching for mentally distressed employees improves several personal domains that contribute to re-establish the employees’ full capacities to work. Although we did not find significantly reduced days of sickness absence when comparing the intervention and control group, job coaching seems to be a viable tool to benefit the psychological conditions of employees. If the re-establishment and maintenance of the employees’ capacity to work translates into reduced sickness absence in the long run, the introduction of a job coaching program may create a win–win situation since reduced sickness absence results in lower costs incurred by the organization. Job coaching can, therefore, be regarded as an effective intervention tool for companies’ health care management systems that benefits both the employees and the organization.
Author Contributions
N-TT, VS, and JM conducted the data processing. N-TT and WK drafted the manuscript. WK and WR conceptualized and conducted the study as principal investigators. WK, SH, and WR supervised the intervention and the data acquisition. All authors read and approved the final version of the manuscript.
Conflict of Interest Statement
The present research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor declared a shared affiliation, though no other collaboration, with the authors WR and WK and states that the process nevertheless met the standards of a fair and objective review.
Acknowledgments
The authors would like to thank Neele T. Garbers, Kathrin Hornung, Katrin Leder, and Nicola Niemeyer who worked as job coaches in the project. The present study has been registered under ISRCTN02422335. http://www.isrctn.com/ISRCTN02422335
Funding
This study is funded by the European Funds for Regional Development and by the Federal State of Lower Saxony within the framework of the Innovation Incubator at the Leuphana University Lüneburg. Grant-No.: CCI NO2007DE161PR001.
Footnote
- ^Please note that the effect sizes were calculated by subtracting the mean values obtained at T2 from the mean values obtained at T0. This means, for example, that the negative effect size of participant’s distancing ability (d = −0.69) indicates an increased distancing ability at T2. Vice versa, the positive effect size of, for example, emotional exhaustion (d = 0.23) indicates that the mean emotional exhaustion was found to be lower at T2 than it had been at T0.
References
1. Meyer M, Mpairaktari P, Glushanok I. Krankheitsbedingte Fehlzeiten in der deutschen Wirtschaft im Jahr 2012. In: Badura B, Ducki A, Schröder H, Klose J, Meyer M, editors. Verdammt zum Erfolg - die süchtige Arbeitsgesellschaft. Berlin: Springer (2013). p. 263–435.
2. Baumann A, Muijen M, Gaebel W. Mental Health and Well-being at the Workplace – Protection and Inclusion in Challenging Times. (2010). Available from: http://www.euro.who.int/__data/assets/pdf_file/0018/124047/e94345.pdf
3. Kawohl W, Lauber C. Arbeit und psychische Gesundheit. In: Rössler W, Kawohl W, editors. Soziale Psychiatrie. Das Handbuch für die psychosoziale Praxis. Stuttgart: Kohlhammer (2013). 122f p.
4. Becker DR, Drake RE. A Working Life for People with Severe Mental Illness. Oxford, New York: Oxford University Press (2003). 214 p.
5. Burns T, Catty J, Becker T, Drake RE, Fioritti A, Knapp M, et al. The effectiveness of supported employment for people with severe mental illness: a randomised controlled trial. Lancet (2007) 370(9593):1146–52. doi:10.1016/S0140-6736(07)61516-5
6. Catty J, Lissouba P, White S, Becker T, Drake RE, Fioritti A, et al. Predictors of employment for people with severe mental illness: results of an international six-centre randomised controlled trial. Br J Psychiatry (2008) 192(3):224–31. doi:10.1192/bjp.bp.107.041475
7. Lauber C, Kawohl W. Supported employment. In: Rössler W, Kawohl W, editors. Soziale Psychiatrie. Das Handbuch für die psychosoziale Praxis. Stuttgart: Kohlhammer (2013). p. 129–37.
8. Grant AM, Curtayne L, Burton G. Executive coaching enhances goal attainment, resilience and workplace well-being: a randomised controlled study. J Posit Psychol (2009) 4(5):396–407. doi:10.1080/17439760902992456
9. Gyllensten K, Palmer S. Can coaching reduce workplace stress? A quasi-experimental study. Int J Evid Based Coach Mentor (2005) 3(2):75–85.
10. McGonagle AK, Beatty JE, Joffe R. Coaching for workers with chronic illness: evaluating an intervention. J Occup Health Psychol (2014) 19(3):385–98. doi:10.1037/a0036601
11. Theeboom T, Beersma B, van Vianen, Annelies EM. Does coaching work? A meta-analysis on the effects of coaching on individual level outcomes in an organizational context. J Posit Psychol (2014) 9(1):1–18. doi:10.1080/17439760.2013.837499
12. Duijts SFA, Kant I, van den Brandt PA, Swaen GMH. Effectiveness of a preventive coaching intervention for employees at risk for sickness absence due to psychosocial health complaints: results of a randomized controlled trial. J Occup Environ Med (2008) 50(7):765–76. doi:10.1097/JOM.0b013e3181651584
13. Duijts SFA, Kant I, Landeweerd JA, Swaen GMH. Prediction of sickness absence: development of a screening instrument. Occup Environ Med (2006) 63(8):564–9. doi:10.1136/oem.2005.024521
14. Kawohl W, Moock J, Heuchert S, Rössler W. Job Maintenance by Supported Employment: An Overview of the “Supported Employment Plus” Trial. Front Public Health eCollection (2015). Available from: http://journal.frontiersin.org/article/10.3389/fpubh.2015.00140/full
15. Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory. Mountain View, CA: Consulting Psychologists Press (1996).
16. Priebe S, Huxley P, Knight S, Evans S. Application and results of the manchester short assessment of quality of life (Mansa). Int J Soc Psychiatry (1999) 45(1):7–12. doi:10.1177/002076409904500102
17. Derogatis LR, Unger R. Symptom checklist-90-revised. In: Weiner IB, Craighead WE, editors. The Corsini Encyclopedia of Psychology. Hoboken, NJ: John Wiley & Sons, Inc (2010). p. 1743–4.
18. Schaarschmidt U, Fischer A. Arbeitsbezogenes Verhaltens- und Erlebensmuster: (AVEM) [Work-Related Behavioral and Sensational Patterns]. Frankfurt am Main: Pearson Assessment & Information GmbH (2008).
19. Viering S, Bärtsch B, Obermann C, Rüsch N, Rössler W, Kawohl W. The effectiveness of individual placement and support for people with mental illness new on social benefits: a study protocol. BMC Psychiatry (2013) 13:195. doi:10.1186/1471-244X-13-195
20. Schaufeli WB, Leiter MP, Maslach C, Jackson SE. The maslach burnout inventory-general survey. In: Maslach C, Jackson SE, Leiter MP, editors. Maslach Burnout Inventory. 3rd ed. Palo Alto, CA: Consulting Psychologists Press (1996). p. 19–26.
21. Taris TW, Schreurs, Paul JG, Schaufeli WB. Construct validity of the Maslach Burnout Inventory-General Survey: a two-sample examination of its factor structure and correlates. Work Stress (1999) 13(3):223–37. doi:10.1080/026783799296039
22. Schutte N, Toppinen S, Kalimo R, Schaufeli WB. The factorial validity of the Maslach Burnout Inventory–General Survey (MBI–GS) across occupational groups and nations. J Occup Organ Psychol (2000) 73:53–66. doi:10.1348/096317900166877
23. Langballe EM, Falkum E, Innstrand ST, Aasland OG. The factorial validity of the maslach burnout inventory-general survey in representative samples of eight different occupational groups. J Career Assess (2006) 14(3):370–84. doi:10.1177/1069072706286497
24. Prinz U, Nutzinger DO, Schulz H, Petermann F, Braukhaus C, Andreas S. Comparative psychometric analyses of the SCL-90-R and its short versions in patients with affective disorders. BMC Psychiatry (2013) 13:104. doi:10.1186/1471-244X-13-104
25. Schmitz N, Hartkamp N, Kiuse J, Franke GH, Reister G, Tress W. The symptom check-list-90-R (SCL-90-R): a German validation study. Qual Life Res (2000) 9:185–93. doi:10.1023/A:1008931926181
26. Urbán R, Kun B, Farkas J, Paksi B, Kökönyei G, Unoka Z, et al. Bifactor structural model of symptom checklists: SCL-90-R and Brief Symptom Inventory (BSI) in a non-clinical community sample. Psychiatry Res (2014) 216(1):146–54. doi:10.1016/j.psychres.2014.01.027
27. Schaarschmidt U, Heitzmann B. Abschlussbericht zum Projekt A11: Rehabilitationsspezifische Diagnostik beruflichens Bewältigungsverhaltens. (2004). Available from: http://forschung.deutsche-rentenversicherung.de/ForschPortalWeb/rehaDoc.pdf?rehaid=BA46AA8D91495DD5C1256E970039715C
28. van Dick R, Wagner U. Der AVEM im Lehrerberuf: Eine Validierungsstudie [The AVEM in teaching occupation: a validity study]. Zeitschrift für Differentielle und Diagnostische Psychologie (2001) 22(4):267–227. doi:10.1024/0170-1789.22.4.267
29. Leonhart R. Effektgrössenberechnung bei Interventionsstudien [effect size computation in intervention studies]. Rehabilitation (2004) 43(4):241–6. doi:10.1055/s-2004-828293
31. Rüsch N, Abbruzzese E, Hagedorn E, Hartenhauer D, Kaufmann I, Curschellas J, et al. Efficacy of coming out proud to reduce stigma’s impact among people with mental illness: pilot randomised controlled trial. Br J Psychiatry (2014) 204:391–7. doi:10.1192/bjp.bp.113.135772
32. Allott KA, Turner LR, Chinnery GL, Killackey EJ, Nuechterlein KH. Managing disclosure following recent-onset psychosis: utilizing the individual placement and support model. Early Interv Psychiatry (2013) 7(3):338–44. doi:10.1111/eip.12030
33. Coughlin SS. Recall bias in epidemiologic studies. J Clin Epidemiol (1990) 43(1):87–91. doi:10.1016/0895-4356(90)90060-3
34. Hassan E. Recall bias can be a threat to retrospective and prospective research designs. Internet J Epidemiol (2005) 3(2). doi:10.5580/2732
35. Nordt C, Brantschen E, Kawohl W, Bärtsch B, Haker H, Rüsch N, et al. “Placement budgets’ for supported employment – improving competitive employment for people with mental illness: study protocol of a multicentre randomized controlled trial. BMC Psychiatry (2012) 12:165. doi:10.1186/1471-244X-12-165
36. Jäger M, Paras S, Nordt C, Warnke I, Bärtsch B, Rössler W, et al. Wie nachhaltig ist supported employment? Eine katamnestische Untersuchung [How sustainable is supported employment? A follow-up investigation]. Neuropsychiatr (2013) 27(4):196–201. doi:10.1007/s40211-013-0085-3
37. Ladegård G. Stress management through workplace coaching: the impact of learning experiences. Int J Evid Based Coach Mentor (2011) 9(1):29–43.
Keywords: job maintenance, sickness absence, individual placement and support, mental health, job coaching
Citation: Telle N-T, Moock J, Heuchert S, Schulte V, Rössler W and Kawohl W (2016) Job Maintenance through Supported Employment PLUS: A Randomized Controlled Trial. Front. Public Health 4:194. doi: 10.3389/fpubh.2016.00194
Received: 12 February 2016; Accepted: 26 August 2016;
Published: 20 September 2016
Edited by:
Meichun Mohler-Kuo, University of Zurich, SwitzerlandReviewed by:
Jürgen Barth, University Hospital Zurich, SwitzerlandAlyssa McGonagle, Wayne State University, USA
Copyright: © 2016 Telle, Moock, Heuchert, Schulte, Rössler and Kawohl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wolfram Kawohl, d29sZnJhbS5rYXdvaGxAYWNjZXNzLnV6aC5jaA==