 Paula Kiyomi Onaga Yokota1
Paula Kiyomi Onaga Yokota1 Alexandre Rodrigues Marra1*
Alexandre Rodrigues Marra1* Talita Rantin Belucci1Elivane da Silva Victor2Oscar Fernando Pavão dos Santos1Michael B. Edmond3
Talita Rantin Belucci1Elivane da Silva Victor2Oscar Fernando Pavão dos Santos1Michael B. Edmond3
- 1Division of Medical Practice, Hospital Israelita Albert Einstein, São Paulo, Brazil
- 2Instituto Israelita de Ensino e Pesquisa Albert Einstein, Hospital Israelita Albert Einstein, São Paulo, Brazil
- 3Department of Internal Medicine, University of Iowa Carver College of Medicine, Iowa City, IA, USA
Background: Central venous catheters are significant risk factors for bloodstream infection (BSI), which are directly associated with increased morbidity and mortality.
Methods: This study was a retrospective cohort study for the time period of July 2011–June 2014 in patients with central line-associated bloodstream infection (CLABSI) to determine the microbiological profile and antimicrobial adequacy of patients with CLABSI in a tertiary hospital.
Results: One hundred and twenty-one CLABSI cases were identified. Ninety-two percent (n = 111) of patients had monomicrobial BSI. Gram-negative bacteria were the most prevalent (49%, n = 63), with Klebsiella spp. predominating (30%, n = 19). Among the Gram-positive bacteria (n = 43, 33%), coagulase-negative staphylococci was the major pathogen (58%, n = 25), and all isolates were methicillin resistant. Antimicrobial therapy was assessed as adequate in 81% (n = 98) of cases. In-hospital mortality was 36% (n = 43 cases).
Conclusion: Our CLABSI patients had a high mortality, although antimicrobial therapy was appropriate. Gram-negative bacteria were responsible for almost half of the cases and there was a high rate of bacteria resistance to extended-spectrum antibiotics.
Introduction
Central venous catheters (CVCs) are essential for the care of seriously ill patients (1, 2). However, CVCs are significant risk factors for bloodstream infection (BSI), which are directly associated with increased morbidity and mortality, length of hospital stay, and medical and hospital costs (2–4). Each year in the United States, there are an estimated 80,000 new cases of central line-associated bloodstream infection (CLABSI), resulting in over 28,000 deaths among patients in intensive care units, with an attributable cost of more than 2.3 billion dollars (5).
To improve antimicrobial therapy for BSI, it is necessary to understand the microorganism profile as well as the antimicrobial susceptibility of these microorganisms (6–8). In a recent publication from our hospital, which analyzed the impact of the implementation of a sepsis protocol, 60% of our patients developed severe sepsis and septic shock outside of the Emergency Department, which increases the probability of nosocomial infection with antibiotic-resistant microorganisms (9, 10). There are serious concerns about the rapid increase of multidrug resistant bacteria, mainly the Gram-negative microorganisms (10).
Thus, the objectives of this study were to determine the microbiological profile and antimicrobial adequacy of patients with CLABSI in a tertiary hospital.
Materials and Methods
This study was conducted in a 629-bed tertiary care (Hospital Israelita Albert Einstein), private hospital in São Paulo, Brazil, with approximately 194,000 patient-days yearly. This study was approved by the Institutional Review Board (CAAE # 40993115.8.0000.0071) with a waiver of informed consent.
We performed a retrospective cohort study for the time period of July 2011–June 2014, in patients with central line-associated bloodstream infection.
Definitions
Central lines were defined using the definition of the National Healthcare Safety Network (NHSN) (11). The NHSN methodology for CLABSI employs active surveillance with standardized definitions by infection preventionists. The definition of CLABSI was an NHSN defined laboratory-confirmed bloodstream infection that was not secondary to an infection at another body site (11).
The ESKAPE Group
ESKAPE group pathogens were defined as the following: vancomycin resistant Enterococcus faecium, methicillin-resistant Staphylococcus aureus, extended-spectrum beta-lactamase—producing Escherichia coli and Klebsiella species, Klebsiella pneumoniae carbapenemase-hydrolyzing beta-lactamases, multidrug resistant Acinetobacter species, resistant Pseudomonas aeruginosa, and Enterobacter species (12).
Antimicrobial Therapy
As in our previous study (10), antimicrobial therapy was considered appropriate if the bacterial species identified in blood culture was susceptible to at least one of the antibiotics administered within 24 h after the collection of culture. If the isolated microorganism was not susceptible by in vitro testing to the antibiotic(s) used, the therapy was considered inadequate. The microbiology laboratory has an alert system to notify physicians of patients with positive blood culture and their Gram stain results. Also the proper antimicrobial dose, proper interval administration, monitoring of drug levels when appropriate, and avoidance of unwanted drug interactions were evaluated (6) by the pharmaceutical hospital in our medical routine.
Microbiological Methods
All samples were identified by manual or automated methods and confirmed using the Vitek 2 system (bioMerieux Vitek, Inc., Hazelwook, MO, USA). The same organism with identical antimicrobial susceptibility profiles from the same or different anatomic sites in the same patient was considered a single isolate. Antimicrobial susceptibility testing was performed by an automated method or by disk diffusion as described by the Clinical and Laboratory Standards Institute (13).
Statistical Analysis
Continuous variables were described by mean and SD or median and interquartile range (IQR). Categorical variables were described as absolute numbers and percentages. Logistic regression models were used to investigate variables associated with death or adequate antimicrobial therapy. Variables with P < 0.1 in the univariate analysis were included in the multivariate models, which were submitted to stepwise method to select the best subset of predictors to each outcome. Results were presented as odds ratios and 95% confidence intervals. The level of significance was set at 0.05 and analyses were performed with statistical package R (14).
Results
A total of 121 CLABSI cases were identified from July 2011 to June 2014. The mean age of the cases was 67 years (SD = 18), and the median length of hospital stay was 43 days (exact median cannot be calculated as two patients remain hospitalized). Of the cases, 56% (n = 68) were male. ESKAPE group pathogens accounted for 21% (n = 25) of the cases. Polymicrobial CLABSIs accounted for 9% (n = 11) of the cases. Antimicrobial therapy was assessed as adequate in 81% (n = 98) of cases. Cardiac dysfunction occurred in 63% (n = 76) and respiratory dysfunction occurred in 52% (n = 63). In-hospital mortality was 36% (n = 43 cases) (Table 1).
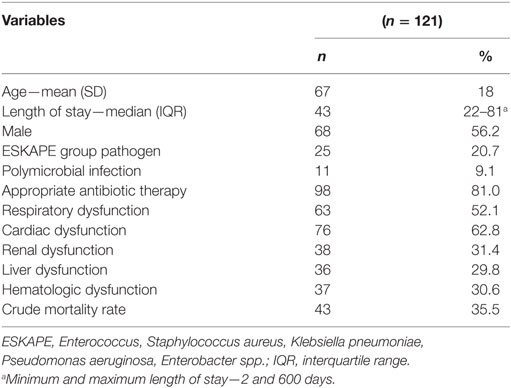
Table 1. Demographic and clinical characteristic of patients with central line-associated bloodstream infection.
In univariate analysis, variables potentially associated with death (P < 0.1) among patients with CLABSI (Table 2) were age, liver dysfunction, cardiac dysfunction, renal dysfunction, hematologic dysfunction, respiratory dysfunction, heart failure, polymicrobial infection, and adequate antimicrobial infection. In the final multivariate model, after stepwise selection, the following variables were statistically significant: age (OR: 1.1, p < 0.01), liver dysfunction (OR: 4.3, p = 0.01); hematologic dysfunction (OR: 6.1, p = 0.01); and renal dysfunction (OR: 10.8, p < 0.01); renal failure (OR: 0.2, p = 0.03); cancer (OR: 4.3, p = 0.04); and polymicrobial infection (OR: 5.9, p = 0.04).
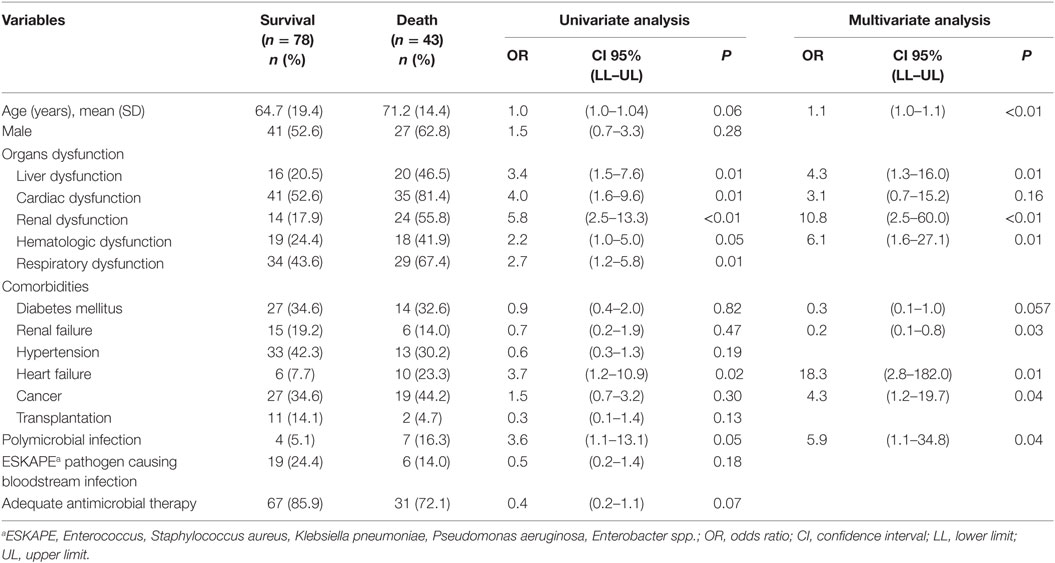
Table 2. Risk factors associated with death in patients with central line-associated bloodstream infection.
Appropriate antimicrobial treatment was administered in 81% of patients (n = 98). All lines in patients with confirmed CLABSI were removed. No variable predicted antimicrobial inadequacy (Table 3). Although there was a trend toward increased mortality with inadequate antimicrobial therapy, it was not statistically significantly different.
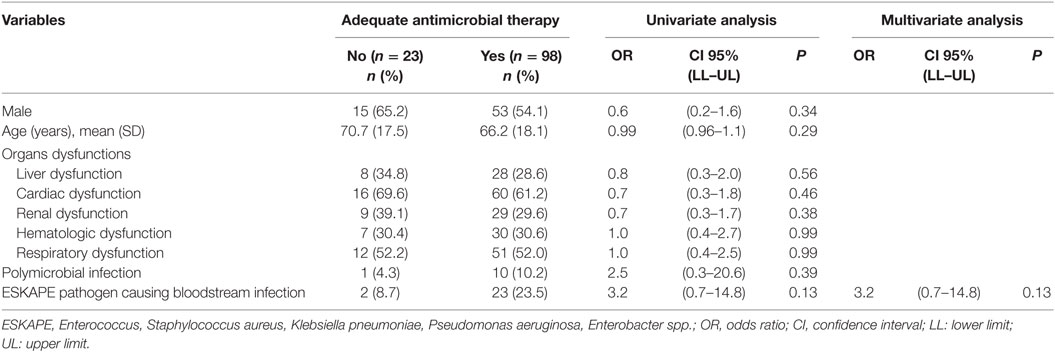
Table 3. Risk factors associated with inadequate antimicrobial therapy in patients with central line-associated bloodstream infection.
Among patients identified with CLABSI, 92% (n = 111) of patients had monomicrobial BSI. Gram-negative bacteria were the most prevalent (49%, n = 63), with Klebsiella spp. predominating (30%, n = 19), followed by P. aeruginosa (17.5%, n = 11), E. coli (15.9%, n = 10), and Enterobacter spp. (12.7%, n = 8). Among the Gram-positive bacteria (n = 43, 33%), coagulase-negative staphylococci was the major pathogen (58%, n = 25), and all isolates were methicillin resistant, followed by S. aureus (23.3%, n = 10) and Enterococcus spp. (14.0%, n = 6). The great majority of S. aureus and Enterococcus spp. were methicillin resistant (90%, n = 9) and vancomycin resistant (83.3%, n = 5), respectively. Among the fungi (18%, n = 23), Candida parapsilosis and Candida albicans were the most prevalent (30%, n = 7, and 22%, n = 5, respectively).
Discussion
Our findings identified the pathogen profile in patients with CLABSI. Regardless of the hospital unit where CLABSI occurred, Gram-negative bacteria, were the most common pathogens, especially Klebsiella spp. (30% of all Gram-negative pathogens), and nearly all of which (95%) were resistant to the third- and fourth-generation cephalosporins. This differs from international studies, including a meta-analysis that assessed 18 studies carried out in different intensive care units, which showed that Gram-positive bacteria are the most prevalent pathogens (15). In the Brazilian Surveillance and Control of Pathogens of Epidemiological Importance Project, the spectrum of pathogens was similar to the present study (16). Fisman et al. demonstrated that geography has a direct influence on the development of BSI caused by Gram-negative bacteria (17).
In our earlier investigation, evaluating patients with severe sepsis and septic shock, the bacterial profile was similar, with a predominance of Gram-negative organisms; however, there was a greater prevalence of E. coli (10). There was a great difference in the proportion of BSI caused by fungi, only 1.5% of cases in the previous study (10), compared to 18% in the current study with 65% in-hospital mortality.
The most common microorganisms responsible for CLABSI change over time. For example, the best practices in ICU care have reduced the proportion of CLABSI due to Gram-positive bacteria (15, 18, 19).
The higher prevalence of Klebsiella spp. was also identified in a previous study (16). Also previous findings described by Correa et al. warned off the increased resistance of K. pneumoniae (20) and reinforced by the European Antimicrobial Resistance Surveillance System in its latest report of hospitals (2011–2012), which was analyzed in 29 European countries (21).
Heart failure was shown to be an independent risk factor for death. In addition, the presence of liver, renal, and hematological dysfunctions significantly increased the risk of death. Moreover, concomitant toxicity of antimicrobial treatment of multidrug resistant microorganisms, particularly with prolonged duration of therapy, adds to the morbidity of the systemic inflammatory response induced by the pathogen (6, 18).
Antimicrobial therapy in a previous study was an independent predictor for lower mortality in patients with severe sepsis and septic shock (10). In our study, inadequacy of therapy showed a trend toward increased mortality. However, the characteristics of these patients show us that appropriate initial antimicrobial treatment of these cases portend a greater chance of error, when polymicrobial infection or ESKAPE pathogens are possible.
The limitations of this study include performance in a single center, which may not allow generalization to other hospitals. Although some information was retrospectively obtained from medical records, the patients were followed prospectively by the hospital epidemiology unit.
In conclusion, our CLABSI patients had a high mortality, although antimicrobial therapy was appropriate. Gram-negative bacteria were responsible for almost half of the cases and there was a high rate of bacteria resistance to extended-spectrum antibiotics.
Ethics Statement
This study was approved by the Institutional Review Board of Albert Einstein Institute of Research (CAAE # 40993115.8.0000.0071) with a waiver of informed consent.
Author Contributions
PY, AM, TB, and EV participated in the data collected and data analysis. PY, AM, OS, and ME participated in the design and coordination. PY, AM, EV, and ME helped to draft the manuscript and to provide critical review of the manuscript. All authors read and approved the final manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We gratefully acknowledge the patients from Hospital Israelita Albert Einstein.
References
1. Blot K, Bergs J, Vogelaers D, Blot S, Vandijck D. Prevention of central line-associated bloodstream infections through quality improvement interventions: a systematic review and meta-analysis. Clin Infect Dis (2014) 59:95–105. doi:10.1093/cid/ciu239
2. Hejjej Z, Nasri M, Sellami W, Gharsallah H, Labben I, Ferjani M. Incidence, risk factors and microbiology of central vascular catheter-related bloodstream infection in an intensive care unit. J Infect Chemother (2014) 20:163–8. doi:10.1016/j.jiac.2013.08.001
3. Marra AR, Cal RGR, Durão MS, Correa L, Guastelli LR, Moura DF Jr, et al. Impact of a program to prevent central line-associated bloodstream infection in the zero tolerance era. Am J Infect Control (2010) 38:434–9. doi:10.1016/j.ajic.2009.11.012
4. Burden AR, Torjman MC, Dy GE, Jaffe JD, Litmann JJ, Nawar F, et al. Prevention of central venous catheter-related bloodstream infection: is it time to add simulation training to the prevention bundle? J Clin Anesth (2012) 24:555–60. doi:10.1016/j.jclinane.2012.04.006
5. Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, et al. An intervention to decrease catheter-related bloodstream infection in the ICU. N Engl J Med (2006) 355(26):2725–32. doi:10.1056/NEJMoa061115
6. Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef M. The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting. Chest (2000) 118:146–55. doi:10.1378/chest.118.1.146
7. Zaragoza R, Artero A, Camarena JJ, Sancho S, González R, Nogueira JM. The influence of inadequate empirical antimicrobial treatment on patients with bloodstream infection in an intensive care unit. Clin Microbiol Infect (2003) 9:412–8. doi:10.1046/j.1469-0691.2003.00656.x
8. Kang CI, Kim SH, Kim HB, Park SW, Choe YJ, Oh MD, et al. Pseudomonas aeruginosa bacteremia: risk factors for mortality and influence of delayed receipt of effective antimicrobial therapy on clinical outcome. Clin Infect Dis (2003) 37:745–51. doi:10.1086/377200
9. Shiramizo SC, Marra AR, Durao MS, Paes AT, Edmond MB, Pavao dos Santos OF. Decreasing mortality in severe sepsis and septic shock patients by implementing a sepsis bundle in a hospital setting. PLoS One (2011) 6:e26790. doi:10.1371/journal.pone.0026790
10. Yokota PKO, Marra AR, Martino MDV, Victor ES, Durao MD, Edmond MB, et al. Impact of appropriate antimicrobial therapy for patients with severe sepsis and septic shock – a quality improvement study. PLoS One (2014) 9(11):e104475. doi:10.1371/journal.pone.0104475
11. Centers for Disease Control and Prevention. Device-Associated Module. Bloodstream Infection Event (Central Line-Associated Bloodstream Infection and Non-Central Line Associated Bloodstream Infection). Atlanta, GA: CDC (2015). Available from: http://www.cdc.gov/nhsn/PDFs/pscManual/4PSC_CLABScurrent.pdf
12. Boucher HW, Talbot GH, Bradley JS, Edwards JE, Gilbert D, Rice LB, et al. Bad bugs, no drugs: no ESKAPE! An update from the Infectious Disease Society of America. Clin Infect Dis (2009) 48:1–12. doi:10.1086/595011
13. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Sixteenth Informational Supplement. CLSI Document M100-S16. Wayne, PA: CLSI (2006).
14. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing. (2015). Available from: http://www.R-project.org/
15. Ziegler MJ, Pellegrini DC, Safdar N. Attributable mortality of central line associated bloodstream infection: systematic review and meta-analysis. Infection (2015) 43:29–36. doi:10.1007/s15010-014-0689-y
16. Marra AR, Camargo Aranha LF, Pignatari ACC, Sukiennik T, Behar PR, Medeiros EA, et al. Nosocomial bloodstream infection in Brazilian hospitals: analysis of 2,563 cases from a prospective Nationwide surveillance study. J Clin Microbiol (2011) 49:1866–71. doi:10.1128/JCM.00376-11
17. Fisman D, Patrozou E, Cameli Y, Perencevich E, Tuite AR, Mermel LA, et al. Geographical variability in the likelihood of bloodstream infections due to Gram-negative bacteria: correlation with proximity to the equator and health care expenditure. PLoS One (2014) 9(12):e114548. doi:10.1371/journal.pone.0114548
18. Anderson DJ, Moehring RW, Sloane R, Schmader KE, Weber DJ, Fowler VG Jr, et al. Bloodstream infections in community hospitals in the 21st century: a multicenter cohort study. PLoS One (2014) 9(3):e91713. doi:10.1371/journal.pone.0091713
19. Climo MW, Yokoe DS, Warren DK, Perl TM, Bolon M, Herwaldt LA, et al. Effect of daily chlorhexidine bathing on hospital-acquired infection. N Engl J Med (2013) 368:533–42. doi:10.1056/NEJMoa1113849
20. Correa L, Martino MD, Siqueira I, Pasternak J, Gales AC, Silva CV, et al. A hospital-based matched case-control study to identify clinical outcome and risk factors associated with carbapenem-resistant Klebsiella pneumoniae infection. BMC Infect Dis (2013) 13:80. doi:10.1186/1471-2334-13-80
21. European Centre for Disease Prevention and Control. ECDC Surveillance Report. Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals 2011-2012. (2015). Available from: http://ecdc.europa.eu/en/publications/Publications/healthcare-associated-infections-antimicrobial-use-PPS.pdf
Keywords: central line-associated infection, inadequate antimicrobial therapy, mortality, blood stream infection, central venous catheters
Citation: Yokota PKO, Marra AR, Belucci TR, Victor ES, Santos OFP and Edmond MB (2016) Outcomes and Predictive Factors Associated with Adequacy of Antimicrobial Therapy in Patients with Central Line-Associated Bloodstream Infection. Front. Public Health 4:284. doi: 10.3389/fpubh.2016.00284
Received: 10 August 2016; Accepted: 14 December 2016;
Published: 23 December 2016
Edited by:
Kurt John Langenbach, American Type Culture Collection, USAReviewed by:
Ronald Paul Rabinowitz, University of Maryland, Baltimore, USAMarquita Vernescia Gittens-St.Hilaire, University of the West Indies, Barbados
Copyright: © 2016 Yokota, Marra, Belucci, Victor, Santos and Edmond. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Rodrigues Marra, YWxleGFuZHJlLm1hcnJhQGVpbnN0ZWluLmJy