 Maria João Gregório1,2,3,4†
Maria João Gregório1,2,3,4† Ana M. Rodrigues1,4,5,6†
Ana M. Rodrigues1,4,5,6† Pedro Graça2,3
Pedro Graça2,3 Rute Dinis de Sousa1,4
Rute Dinis de Sousa1,4 Sara S. Dias1,4,7
Sara S. Dias1,4,7 Jaime C. Branco1,4,5,8
Jaime C. Branco1,4,5,8 Helena Canhão1,4,5,9,10*
Helena Canhão1,4,5,9,10*
- 1EpiDoC Unit, Centro de Estudos de Doenças Crónicas (CEDOC) da NOVA Medical School, Universidade Nova de Lisboa (NMS/UNL), Lisboa, Portugal
- 2Faculdade de Ciências da Nutrição e Alimentação da Universidade do Porto, Porto, Portugal
- 3Programa Nacional para a Promoção da Alimentação Saudável, Direção-Geral da Saúde, Lisboa, Portugal
- 4EpiSaúde Scientific Association, Évora, Portugal
- 5Sociedade Portuguesa de Reumatologia, Lisboa, Portugal
- 6Rheumatology Research Unit, Instituto de Medicina Molecular, Lisboa, Portugal
- 7Unidade de Investigação em Saúde (UI), Escola Superior de Saúde do Instituto Politécnico de Leiria, Leiria, Portugal
- 8Serviço de Reumatologia do Hospital Egas Moniz – Centro Hospitalar Lisboa Ocidental (CHLO-E.P.E.), Lisboa, Portugal
- 9Escola Nacional de Saúde Pública da Universidade Nova de Lisboa, Lisboa, Portugal
- 10Serviço Reumatologia, Centro Hospitalar Lisboa Central-HSM, Lisboa, Portugal
Background: Food insecurity is a limited or uncertain access to the adequate food and is a significant public health problem. We aimed to assess determinants of food insecurity and the corresponding health impact in Portugal, a southern European country that faced a severe economic crisis.
Methods: Data were derived from the Epidemiology of Chronic Diseases Cohort Study (EpiDoC), a population-based cohort of 10,661 individuals that were representative of the Portuguese adult population and followed since 2011. A cross-sectional analysis of the third wave of evaluation (EpiDoC 3) was performed between 2015 and 2016. Food insecurity was assessed with the household food insecurity psychometric scale. Socioeconomic, demographic, lifestyle, adherence to Mediterranean diet (MD), self-reported non-communicable disease, health-related quality of life (HRQoL) (EQ-5D-3L), physical function (HAQ score), and health resource consumption information was also collected.
Results: The estimated proportion of food insecurity was 19.3% among a total of 5,653 participants. Food insecure households had low adherence to the MD (OR = 0.44; 95% IC 0.31–0.62). In addition, diabetes (OR = 1.69; 95% IC 1.20–2.40), rheumatic disease (OR = 1.67; 95% IC 1.07–2.60), and depression symptoms (OR = 1.50; 95% IC 1.09–2.06) were independently associated with food insecurity. On average, food insecure households had a lower HRQoL (OR = 0.18; 95% IC 0.11–0.31) and a higher disability (OR = 2.59; 95% IC 2.04–3.29). A significantly higher proportion of food insecure households reported being hospitalized (OR = 1.57; 95% IC 1.18–2.07) and had more public hospital medical appointments (OR = 1.48; 95% IC 1.12–1.94) in the previous 12 months.
Conclusion: We found that food insecurity is highly prevalent in Portugal. Food insecurity was associated with low adherence to the MD, non-communicable chronic diseases, lower quality of life, and higher health resource consumption. Therefore, this study provides valuable insight into the relationship between food security and the diet and health of the population during an economic crisis.
Introduction
Food insecurity is defined as a socioeconomic situation that leads to limited or uncertain access to the nutritious food necessary to maintain a healthy and active life (1). Food insecurity is a significant public health problem and is associated with unhealthy dietary habits and chronic diseases (2–4). Several studies have shown that food insecurity is associated with unhealthy dietary patterns, including reduced intake of fruits, vegetables, and dairy products, and increased intake of energy-dense foods (2, 3). These unhealthy dietary habits are common among food insecure households and may mediate the association between food insecurity and health.
The Mediterranean diet (MD) is a traditional dietary pattern of southern European countries and has been shown to be a healthy diet. This dietary pattern is characterized by a high intake of fruits and vegetables, whole grains, legumes, nuts, and olive oil and a moderate intake of meat. In fact, it is recognized that the MD is associated with lower risk for several chronic diseases, such as cardiovascular events, diabetes, and cancer (5, 6). Some studies have suggested that reduced adherence to the MD in southern European countries during recent years may be related to the European economic crisis (7, 8). This raises questions regarding the impact of the economic crisis on dietary habits, especially those of citizens with food insecurity. Food insecurity may be an important indicator that should be monitored to understand how the socioeconomic situation might be compromising food intake and changing dietary habits.
Food insecurity has been widely studied in the USA and Canada; however, there is a lack of epidemiological data in southern European countries. Addressing food insecurity during an economic crisis is of particular relevance because it is known that periods of economic, political, and social instability tend to notably affect the most vulnerable population strata. In fact, as a result of economic crisis in Portugal, the government adopted austerity policies and large cuts to public expenditure that could lead to inequalities in access to food. Therefore, it is of upmost importance to evaluate food insecurity in a representative sample of the Portuguese population. Moreover, it is important to evaluate the impact of food insecurity on diet and health. The aim of this study was to investigate the prevalence of food insecurity, the association of food insecurity with sociodemographic and economic determinants, and the impact on health status and the consumption of other health resources in a country that faced a recent, severe economic crisis.
Materials and methods
Study Design and Participants
The cross-sectional data presented in this study were collected at the third follow-up evaluation wave of the Epidemiology of Chronic Diseases Cohort Study (EpiDoC 3). The EpiDoC cohort was designed to study health determinants and outcomes, chronic non-communicable diseases, and their impact on health resource consumption. The EpiDoC cohort included adults (greater than 18 years old) who were non-institutionalized and living in private households in the mainland and the islands (Azores and Madeira) of Portugal (9). The EpiDoC sample size calculation was performed in order to capture health-related conditions with a prevalence of at least 0.5%, as described elsewhere (10). The estimated prevalence of household food insecurity was notably higher; thus, our sample size had adequate statistical power for the aim of EpiDoC 3. All of the 10,661 participants of the EpiDoC 1 study who signed the informed consent for follow-up and those who provided their telephone number were enrolled in the subsequent follow-up evaluations of the EpiDoC closed cohort studies (EpiDoC 2 and EpiDoC 3) (11). The flowchart of the EpiDoC cohort is described in Figure 1, and EpiDoC 3 included 5,653 participants.
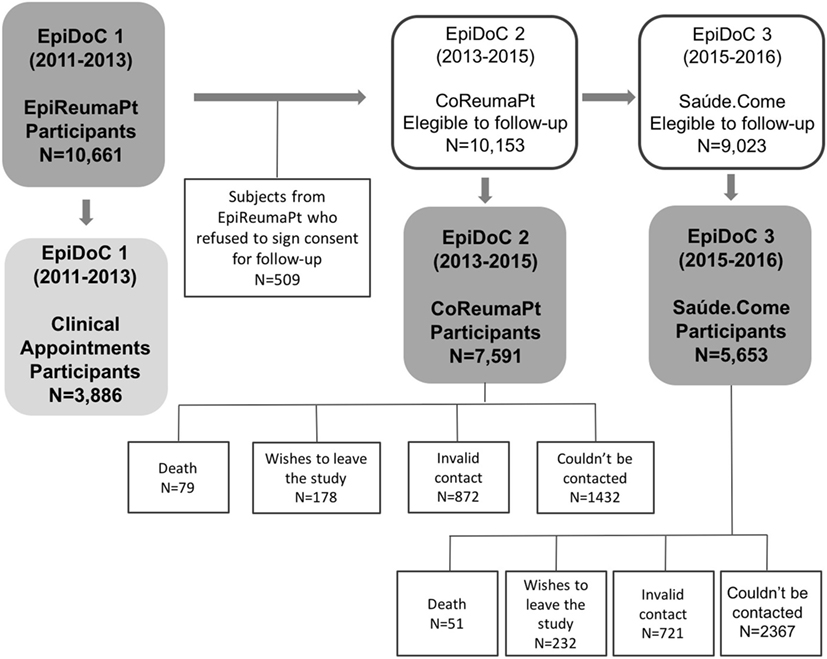
Figure 1. Flowchart of the EpiDoC cohort (consisting of three studies).
Data Collection
In the EpiDoC 3 wave of evaluation, a structured questionnaire was applied through computer-assisted phone call interviews by a trained research assistant team from September 1, 2015 to July 28, 2016. Database access is protected by a unique username and password for each research team member. The questionnaire of EpiDoC 3 was constructed using the core questions of the EpiDoC cohort and adding a food insecurity questionnaire and related items. The questionnaire was tested and improved to ensure respondents’ comprehension of the questions and high response rates.
Measurements
Information on sociodemographics (sex, age, ethnicity, years of education, marital status, and region) were collected in the EpiDoC 1 study. In EpiDoC 3 the structured questionnaire included current household composition, employment status, main source of income, number of children in the household, number of elderly in the household, single-parent family, information regarding the household income perception, and self-reported diseases (high cholesterol level, high blood pressure, diabetes, hyperuricemia, rheumatic disease, allergies, gastrointestinal disease, mental disease, cardiac disease, pulmonary disease, cancer, neurologic disease, and psoriasis).
Health-related quality of life (HRQoL) was assessed using the European Quality of Life questionnaire with five dimensions and three levels (EQ-5D-3L) (12, 13). A higher HRQoL score corresponds to a higher quality of life. Physical function was evaluated based on the Health Assessment Questionnaire (HAQ, 0–3) (14). Higher HAQ scores correspond to reduced functional ability of the individual. We used Portuguese-validated versions of these assessment scales. Data regarding hospitalization in the previous 12 months (Yes/No), number of clinic appointments, doctor visit reduction due to economic difficulties (Yes/No), and stoppage of medication due to economic difficulties (Yes/No) were also recorded. Self-reported height and weight were collected and body mass index (BMI) was calculated and categorized according to the World Health Organization classification (15). Questions concerning lifestyle habits included frequency of alcohol intake (daily, occasionally, never), quantity of alcohol units per week (≤3 alcohol units per week; >3 alcohol units per week but <3 alcohol units per day; >3 alcohol units per day), smoking habits (daily, occasionally, past smoker, never smoked), and frequency and type of physical activity. Physical activity level was classified based on the reported weekly frequency of physical activity: inactive (<1 h/week), moderately active (between 1 and 2.5 h/week), and active (≥2.5 h/week).
To assess adherence to the MD, a PREDIMED (PREvención con DIeta MEDiterránea) questionnaire was applied. This is a 14-item questionnaire with questions based on the number of servings and frequencies of consumption for typical food or food groups of the MD (e.g., olive oil, nuts, fruits, vegetables, pulses, seafood) or questions about the consumption of foods that are not part of the traditional MD (e.g., red or processed meats, sweetened beverages and sweets, commercial bakery, or sugary desserts). A score ≥10 corresponds to a high adherence to the MD, and a score <10 corresponds to a low adherence to the MD (16).
Case Definition and Assessment
Household food insecurity was assessed using a psychometric scale that was adapted and validated for the Portuguese population from the Brazilian Food Insecurity Scale, which was adapted from the US Household Food Security Survey Module (17). This tool was applied by telephone interview to EpiDoC 3 participants. The household food insecurity scale is a tool applied to the individual and collects data regarding food insecurity status of the entire household. This tool measures both quantitative and qualitative components of food insecurity during the last 3 months. A score ranging from 0 to 14 was obtained from the total number of affirmative responses. According to this score, households were classified into four different categories of food insecurity: food security (if total score was 0), low food insecurity (if total score was between 1 and 5 for households with children and between 1 and 3 for households without children), moderate food insecurity (if total score was between 6 and 9 for households with children and between 4 and 5 for households without children), and severe food insecurity (if total score was between 10 and 14 for households with children and between 6 and 8 for households without children) (18, 19).
Statistical Analysis
To verify the representativeness of the sample according to the Portuguese population (mainland and islands), we first compared the participants and non-participants of the EpiDoC 3 study with respect to their sociodemographic, socioeconomic, and health status characteristics. Based on this comparison, we adjusted the weights according to stratification by Nomenclature of Territorial Unit for Statistics (NUTS II) region, gender, and age group. Extrapolation weights were computed and used in the subsequent statistical analyses. These were obtained by calibrating the extrapolation weights originally designed for the EpiDoC 1 study sample (9). Absolute frequencies and weighted proportions were used to summarize categorical variables. Continuous variables were described by weighted mean values and SDs. Prevalence estimates for food insecurity were computed as weighted proportions according to region, age groups, gender, employment status, years of schooling, single-parent family, household with children, household with elderly, household income perception, BMI, and adherence to MD. After a descriptive analysis, participants were categorized as “food secure” (high food security) and “food insecure” (including low, moderate, and severe insecurity groups). Subjects with and without food insecurity were compared. Univariable analyses were first performed considering the study design (crude analysis). Multivariate regression models were used to assess dietary, other lifestyles, anthropometric data (BMI), health-related characteristics, and health-care resource consumption differences between individuals with and without food insecurity. In order to adjust the differences between groups, the following potential confounders were included in the logistic regression analysis: age group, gender, educational level, employment status, and NUTS II (adjusted analysis). Significance level was set at 0.05. All analyses were performed using STATA IC version 12 (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX, USA: StataCorp LP).
Ethical Issues and Personal Protection
Details of the ethical issues of the EpiDoC cohort were previously described (9). The EpiDoC 3 study was performed according to the principles established by the Declaration of Helsinki (20) and revised in 2013 in Fortaleza. The study was reviewed and approved by the National Committee for Data Protection and by the NOVA Medical School Ethics Committee (9).
Results
Food Insecurity Prevalence and Associated Factors in the Portuguese Adult Population
In EpiDoC 3, a total of 5,653 participants were interviewed. The EpiDoC 3 population did not differ from the Portuguese population (Table 1). Between 2015 and 2016, 19.3% of Portuguese households experienced some level of food insecurity during the previous 3 months. Most food insecure households were in the lower level of food insecurity (14.0%), but 3.5 and 1.8% had moderate and severe food insecurity, respectively.
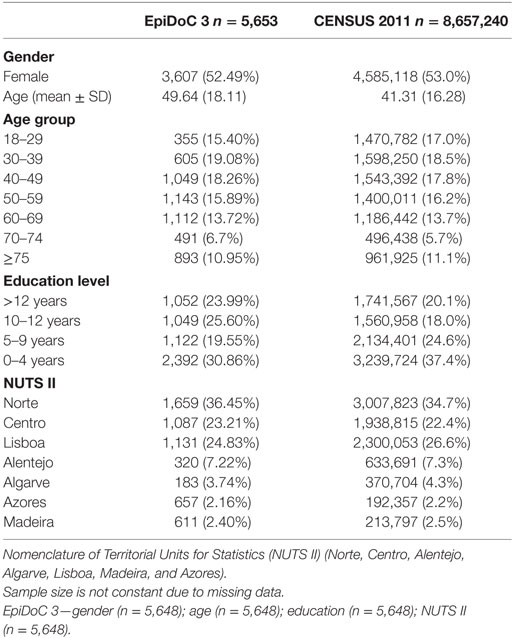
Table 1. Sociodemographic characteristics of the adult Portuguese population: EpiDoC 3 and Census 2011 populations (Portuguese population).
Analysis of the socioeconomic factors associated with food insecurity revealed that women (OR = 1.73; 95% IC 1.37–2.18), the less educated (10–12 vs <12 years: OR = 3.10; 95% IC 1.89–5.07; 5–9 vs <12 years: OR = 4.35; 95% IC 2.75–6.90; 0–4 vs <12 years: OR = 7.11; 95% IC 4.49–11.26), individuals aged between 40 and 49 years (OR = 2.28; 95% IC 1.05–4.97), and individuals aged between 50 and 59 years (OR = 2.42; 95% IC 1.10–5.33) had a higher risk of being food insecure. When compared to individuals in a situation of full-time employment, households of individuals who were part-time employed, domestic workers, or unemployed were more likely to be food insecure (OR = 1.68; 95% IC 1.23–2.30). Households living in the Azores (OR = 1.57; 95% IC 1.12–2.20) and Madeira (OR = 1.94; 95% IC 1.32–2.85) also had higher probabilities of being classified as food insecure (Table 2).
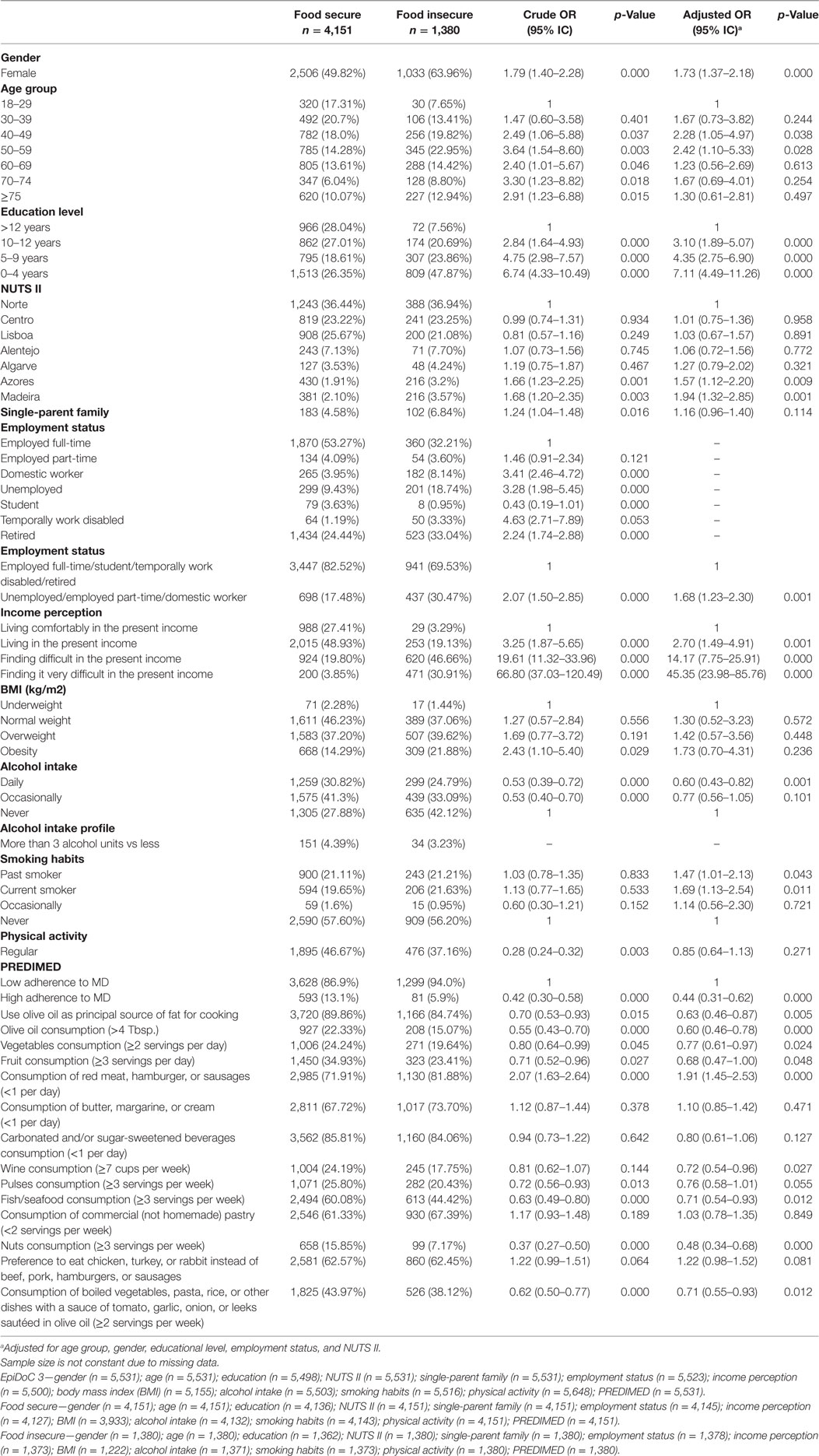
Table 2. Comparison of sociodemographic, socioeconomic, lifestyles characteristics, and Mediterranean diet (MD) characteristics between households with and without food insecurity.
Participants from Food Insecure Households Had Significantly Lower Adherence to the MD
Adherence to the MD was inversely associated with household food insecurity (OR = 0.44; 95% IC 0.31–0.62), even after adjustment for age, gender, educational level, employment status, and NUTS II. Individuals from food insecure households had a lower tendency to use olive oil as principal source of fat for cooking (OR = 0.63; 95% IC 0.46–0.87) and reduced consumption of vegetables ≥2 servings per day (OR = 0.77; 95% IC 0.61–0.97), fruit ≥3 servings per day (OR = 0.68; 95% IC 0.47–1.00), fish or seafood ≥3 servings per week (OR = 0.71; 95% IC 0.54–0.93), and nuts ≥3 servings per week (OR = 0.48; 95% IC 0.34–0.68) (Table 2).
Participants from Food Insecure Households Had a Significantly Lower Quality of Life, Physical Functioning, and Consumed More Health-care Resources
To investigate the association of food insecurity with self-reported non-communicable diseases, weighted proportions were adjusted for age, gender, educational level, employment status, and NUTS II. We found that diabetes (OR = 1.69; 95% IC 1.20–2.40), pulmonary disease (OR = 1.67; 95% IC 1.14–2.45), and rheumatic disease (OR = 1.67; 95% IC 1.07–2.60) were independently associated with household food insecurity. The individuals of food insecure households also had a lower quality of life (EQ-5D-3L score: OR = 0.18; 95% IC 0.11–0.31), a higher physical disability (HAQ score: OR = 2.59; 95% IC 2.04–3.29), and a higher risk of having depression symptoms (OR = 1.50; 95% IC 1.09–2.06). Individuals from food insecure households had been more often hospitalized (OR = 1.57; 95% IC 1.18–2.07), had gone more frequently to medical appointments in hospitals (OR = 1.48; 95% IC 1.12–1.94) since last contact, and presented a higher number of medical appointments in the public sector (OR = 1.07; 95% IC 1.04–1.11). Individuals of food insecure households were more likely to have reported stopping medication (OR = 5.13; 95% IC 3.86–6.82) and reducing doctor visits due to economic constraints (OR = 4.23; 95% IC 3.09–5.78) (Table 3).
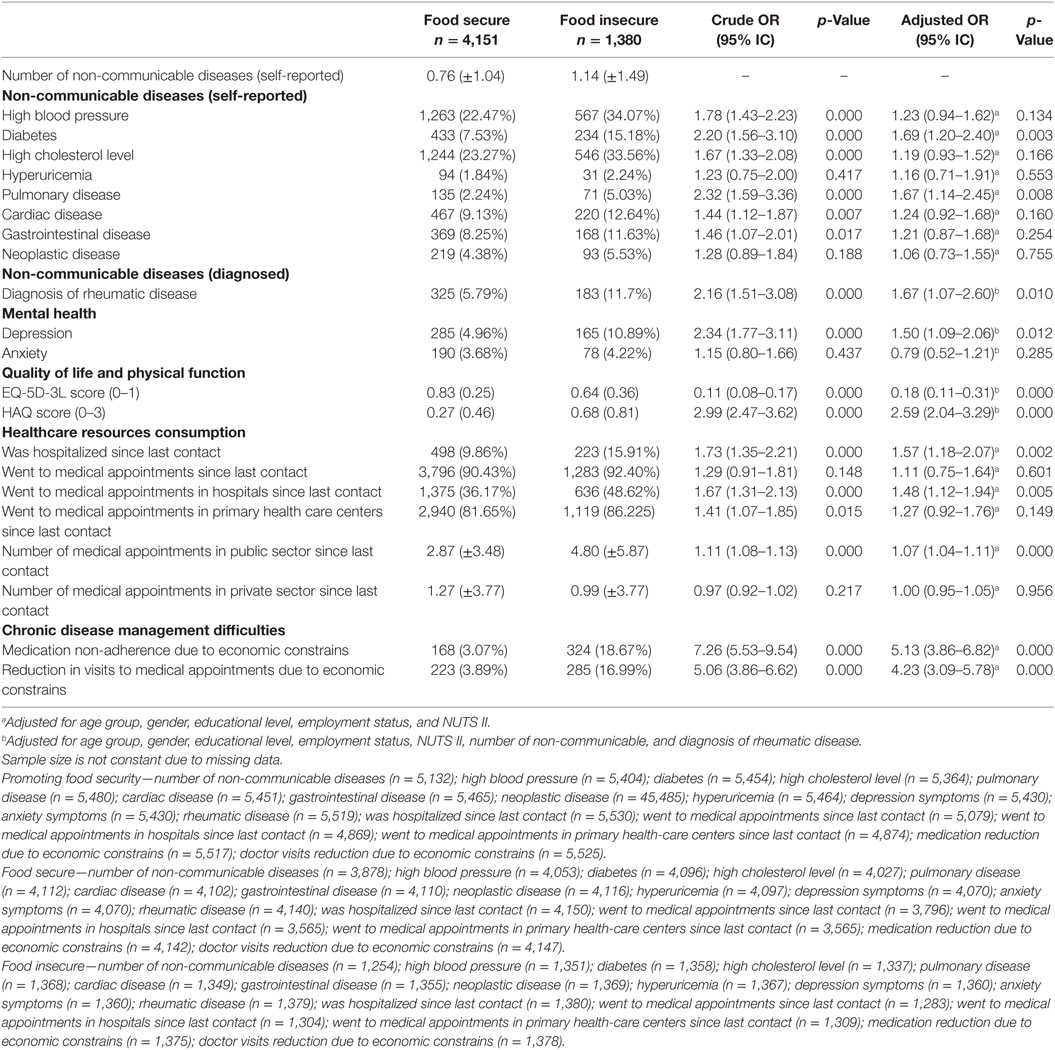
Table 3. Comparison of health status and healthcare resources consumption between households with and without food insecurity.
Discussion
Using a large population-based database from Portugal, a southern European country that faced a severe economic crisis, we found that the major determinants of food insecurity were unemployment or precarious employment conditions, single-parent family, low education level, and insufficient household income perception. These findings are in accordance with previous studies. The national survey on food insecurity in Canada found that lone-parent families, in particular those headed by women, were the most vulnerable to food insecurity (21). Furthermore, lone-parent families, unemployment or precarious employment condition, low education, and low income are sociodemographic and economic determinants of food insecurity reported worldwide (21, 22). In terms of the employment situation, some studies have highlighted the severe impact of a precarious employment situation on health outcomes, even in comparison with an unemployment situation (23).
The estimated prevalence of food insecurity in Portugal between 2015 and 2016 was 19.3%. The Azores and Madeira Islands were the two regions most affected by food insecurity. A previous study conducted in Portugal in 2003, reported a food insecurity prevalence of 8.1% (24). Between 2005 and 2006, data from the last Portuguese National Health Survey estimated a food insecurity prevalence of 16.7% (25). Comparisons between these studies should be made carefully due to the different methodological approaches in terms of sampling method and food insecurity measurement instrument (24, 25). Nevertheless, our study showed a markedly higher prevalence of food insecurity that cannot be explained solely by methodological differences and might suggest an increasing trend in the prevalence of food insecurity during the last 10 years.
Food insecurity was significantly associated with low adherence to the MD. Lower levels of MD adherence were also found among the lower socioeconomic groups in previous studies (26). Food insecurity has been associated with unhealthy dietary patterns, such as a reduced intake of fruit, vegetables, and dairy products and an increased intake of energy-dense foods among food insecure individuals (2, 3). Our data did not show a significant association between food insecurity and overweight individuals or obesity after adjusting for socioeconomic factors; however, there was a trend toward higher rates of overweight individuals and obesity in food insecure households. These results support findings in other countries where social inequalities have been associated with some determinants of obesity (27–29) and other diet-related non-communicable diseases. Unhealthy dietary habits and lower levels of physical activity were previously identified as determinants of obesity and appear to be more common among the lower socioeconomic groups (30, 31).
We have examined the impact of food insecurity on health and health-related issues and found that subjects with food insecurity reported worse HRQoL and more physical disability when compared to subjects without food insecurity. A higher proportion of subjects with food insecurity were found to have diabetes and rheumatic diseases than those with food security. In fact, our results agree with those from other countries that found strong evidence that vulnerable people, who commonly live in food insecure conditions, have a higher risk of poor health (32, 33). Studies have found that socioeconomically vulnerable groups experience higher mortality and morbidity rates for coronary heart disease (34), atherosclerosis, type 2 diabetes mellitus (35), and some cancers (36). Our study also revealed that a high proportion of subjects with food insecurity reported mental illness in the form of self-reported depression symptoms. The consequences of food insecurity in mental health, namely anxiety and depression symptoms, are well-documented in the literature (37). The causal mechanism is not clear and may be bidirectional. Individuals with food insecurity more often reported difficulties in chronic disease management because they experience more frequent non-adherence to medication and reduced medical appointments due to economic constraints. These difficulties in chronic disease management worsen their health status and decrease disease control. In line with our findings, Berkowitz et al. found that food insecurity is strongly associated with medication underuse (38). The present study also showed that food insecurity was associated with a higher proportion of hospitalizations and clinical appointments, stressing that poor disease control in subjects of food insecurity leads to higher health resource consumption. Tarasuk et al. showed that household food insecurity is a predictor of healthcare utilization and cost in Canada (39).
Food insecurity requires improved collaboration between social protection policies and food and nutrition national policies. Social protection policies, particularly in times of economic crises, are important to ensure adequate socioeconomic conditions for the most vulnerable. Of particular concern for these individuals is the access to healthy food. Food and nutrition national policies should address food insecurity questions in their action plans. This could be accomplished by ensuring that food aid programs are providing healthy food baskets for low-income individuals and empowering these vulnerable individuals for healthy eating. Several countries, especially European countries, fail in their food aid programs due to a low capacity to provide nutritionally adequate foods (40). Toward this end, Portugal has recently developed and implemented a new food aid program for low-income households, which considers the nutritional and food recommendations for healthy eating (41).
Our study has some limitations. Due to the cross-sectional nature of the data, it is not possible to establish causal associations between food insecurity and diet and health outcomes. Food insecurity was assessed based on individual self-perception, and the tool used does not allow us to identify how food insecurity differently affects each member of the household. Several strengths should also be pointed out. Data came from a large, nationally representative sample of the adult population who have been followed since 2011. This study design captured different health and health-related measurements that provided relevant information about determinants and consequences of food insecurity.
In conclusion, this study provided strong evidence that food insecurity is a public health problem that is be associated with a lower adherence to a healthy dietary pattern (MD) and to a higher risk for chronic diseases and poor disease control. Food insecurity leads to more health resource consumption and hospitalization. Data from this study provide valuable information to increase awareness of the food insecurity problem in southern European countries facing an economic crisis. It also provides a strong argument to encourage policymakers to increase the resources allocated to reduce social inequalities and poverty. The implementation of inter-sectoral policies addressing food insecurity is an urgently needed strategy to reduce the burden of diet-related non-communicable diseases.
Ethics Statement
Details of ethical issues of EpiDoC cohort were described elsewhere [Rodrigues et al. (9)]. EpiDoC 3 study was performed according to the principles established by the Declaration of Helsinki (World Medical Association, 2013) revised in 2013 in Fortaleza. The study was reviewed and approved by the National Committee for Data Protection and by the NOVA Medical School Ethics Committee [Rodrigues et al. (9)].
Author Contributions
MG and AR contributed equally to this work. HC, AR, and MG designed the study. AR and MG analyzed and interpreted the data and wrote the paper. JB, PG, RS, SD, and HC gave scientific support and revised the manuscript. All authors discussed the results and implications and commented on the manuscript at all stages.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The present project was granted by the Public Health Initiatives Programme (PT06) and financed by the EEA Grants Financial Mechanism 2009–2014.
References
1. Food and Agriculture Organization of the United Nations. The State of Food Insecurity in the World 2001. Rome: Food and Agriculture Organization of the United Nations (2002).
2. Hanson KL, Connor LM. Food insecurity and dietary quality in US adults and children: a systematic review. Am J Clin Nutr (2014) 100(2):684–92. doi:10.3945/ajcn.114.084525
3. Leung CW, Epel ES, Ritchie LD, Crawford PB, Laraia BA. Food insecurity is inversely associated with diet quality of lower-income adults. J Acad Nutr Diet (2014) 114:1943–53. doi:10.1016/j.jand.2014.06.353
4. Vandentorren S, Le Mener E, Oppenchaim N, Arnaud A, Jangal C, Caum C, et al. Characteristics and health of homeless families: the ENFAMS survey in the Paris region, France 2013. Eur J Public Health (2016) 26(1):71–6. doi:10.1093/eurpub/ckv187
5. Martinez-Gonzalez MA, Salas-Salvado J, Estruch R, Corella D, Fito M, Ros E, et al. Benefits of the Mediterranean diet: insights from the PREDIMED study. Prog Cardiovasc Dis (2015) 58(1):50–60. doi:10.1016/j.pcad.2015.04.003
6. Guasch-Ferre M, Salas-Salvado J, Ros E, Estruch R, Corella D, Fito M, et al. The PREDIMED trial, Mediterranean diet and health outcomes: how strong is the evidence? Nutr Metab Cardiovasc Dis (2017) 27(7):624–32. doi:10.1016/j.numecd.2017.05.004
7. Bonaccio M, Di Castelnuovo A, Bonanni A, Costanzo S, De Lucia F, Persichillo M, et al. Decline of the Mediterranean diet at a time of economic crisis. Results from the Moli-sani study. Nutr Metab Cardiovasc Dis (2014) 24(8):853–60. doi:10.1016/j.numecd.2014.02.014
8. Bonaccio M, Bes-Rastrollo M, de Gaetano G, Iacoviello L. Challenges to the Mediterranean diet at a time of economic crisis. Nutr Metab Cardiovasc Dis (2016) 26(12):1057–63. doi:10.1016/j.numecd.2016.07.005
9. Rodrigues AM, Gouveia N, da Costa LP, Eusebio M, Ramiro S, Machado P, et al. EpiReumaPt – the study of rheumatic and musculoskeletal diseases in Portugal: a detailed view of the methodology. Acta Reumatol Port (2015) 40(2):110–24.
10. Ramiro S, Canhao H, Branco JC. EpiReumaPt protocol – Portuguese epidemiologic study of the rheumatic diseases. Acta Reumatol Port (2010) 35(3):384–90.
11. Laires PA, Canhão H, Araújo D, Fonseca JE, Machado P, Mourão AF, et al. CoReumaPt protocol: the Portuguese cohort of rheumatic diseases. Acta Reumatol Port (2012) 37:18–24.
12. Ferreira LN, Ferreira PL, Pereira LN, Oppe M. EQ-5D Portuguese population norms. Qual Life Res (2014) 23(2):425–30. doi:10.1007/s11136-013-0488-4
13. Ferreira LN, Ferreira PL, Pereira LN, Oppe M. The valuation of the EQ-5D in Portugal. Qual Life Res (2014) 23(2):413–23. doi:10.1007/s11136-013-0448-z
14. Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of patient outcome in arthritis. Arthritis Rheum (1980) 23(2):137–45. doi:10.1002/art.1780230202
15. World Health Organization. Physical Status: The Use and Interpretation of Anthropometry Report of a WHO Expert Committee. WHO Technical Report. Geneva: World Health Organization (1995). Series 854.
16. Schroder H, Fito M, Estruch R, Martinez-Gonzalez MA, Corella D, Salas-Salvado J, et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J Nutr (2011) 141(6):1140–5. doi:10.3945/jn.110.135566
17. Gregório MJ, Nogueira PJ, Graça P. The first validation of the household food insecurity scale in a sample of the Portuguese population. In: Gregório MJ, editor. Desigualdades Sociais No Acesso a uma Alimentação Saudável: um Estudo na População Portuguesa. Ph.D., Faculty of Nutrition and Food Sciences of University of Porto (2014).
18. Gregório MJ, Graça P, Nogueira PJ, Gomes S, Santos CA, Boavida J. Proposta metodológica para a avaliação da insegurança alimentar em Portugal. Revista Nutrícias (2012) 21:4–11.
19. Gregório MJ, Graça P, Costa A, Nogueira PJ. Time and regional perspective of food insecurity during the economic crisis in Portugal, 2011–2013. Saúde e Sociedade (2014) 23(4):13–27. doi:10.1590/S0104-12902014000400001
20. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA (2013)310(20):2191–4. doi:10.1001/jama.2013.281053
21. Tarasuk V, Mitchell A, Dachmer N. Household Food Insecurity in Canada 2014. Research to identify policy options to reduce food insecurity. Toronto: PROOF Food Insecurity Policy Research (2016). Available from: http://proof.utoronto.ca/
22. Coleman-Jensen A, Nord M, Andrews M, Carlson S. Household Food Security in the United States in 2011 (No ERR-141). U.S. Department of Agriculture, Economic Research Service (2012).
23. Kim TJ, von dem Knesebeck O. Is an insecure job better for health than having no job at all? A systematic review of studies investigating the health-related risks of both job insecurity and unemployment. BMC Public Health (2015) 15:985. doi:10.1186/s12889-015-2313-1
24. Branco MJ, Nunes B, Cantreiras T. Uma Observação sobre “Insegurança Alimentar”. Lisboa: Instituto Nacional de Saúde Dr Ricardo Jorge (2003).
25. Álvares L, Amaral TF. Food insecurity and associated factors in the Portuguese population. Food Nutr Bull (2014) 35(4):395–402. doi:10.1177/156482651403500401
26. Bonaccio M, Donati M, Iacoviello L, Gaetano GD. Socioeconomic determinants of the adherence to the Mediterranean diet at a time of economic crisis: the experience of the MOLI-SANI study. Agric Agric Sci Procedia (2016) 8:741–7. doi:10.1016/j.aaspro.2016.02.059
27. Sobal J, Stunkard AJ. Socioeconomic status and obesity: a review of the literature. Psychol Bull (1989) 105:260–75. doi:10.1037/0033-2909.105.2.260
28. Dinour LM, Bergen D, Yeh MC. The food insecurity-obesity paradox: a review of the literature and the role food stamps may play. J Am Diet Assoc (2007) 107(11):1952–61. doi:10.1016/j.jada.2007.08.006
29. Robertson A, Lobstein T, Knais C. Obesity and socio-economic groups in Europe: evidence review and implications for action. Brussels: European Commission (2007). Available from: http://ec.europa.eu/health/ph_determinants/life_style/nutrition/documents/ev20081028_rep_en.pdf
30. Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr (2008) 87:1107–17.
31. Drewnowski A. Obesity, diets, and social inequalities. Nutr Rev (2009) 67(1):S36–9. doi:10.1111/j.1753-4887.2009.00157.x
32. Stuff JE, Casey PH, Szeto KL, Gossett JM, Robbins JM, Simpson PM, et al. Household food insecurity is associated with adult health status. J Nutr (2004) 134(9):2330–5. doi:10.1093/jn/134.9.2330
33. Mackenbach JP, Stirbu I, Roskam A-JR, Schaap MM, Menvielle G, Leinsalu M, et al. Socioeconomic inequalities in health in 22 European countries. N Engl J Med (2008) 358:2468–81. doi:10.1056/NEJMsa0707519
34. Rooks RN, Simonsick EM, Miles T, Newman A, Kritchevsky SB, Schulz R, et al. The association of race and socioeconomic status with cardiovascular disease indicators among older adults in the health, aging and body composition study. J Gerontol B Psychol Sci Soc Sci (2002) 57:S247–56. doi:10.1093/geronb/57.4.S247
35. Everson SA, Maty SC, Lynch JW, Kaplan GA. Epidemiologic evidence for the relation between socioeconomic status and depression, obesity, and diabetes. J Psychosom Res (2002) 53:891–816. doi:10.1016/S0022-3999(02)00303-3
36. Ward E, Jemal A, Cokkinides V, Singh GK, Cardinez C, Ghafoor A, et al. Cancer disparities by race/ethnicity and socioeconomic status. Cancer J Clin (2004) 54:78–93. doi:10.3322/canjclin.54.2.78
37. Leung CW, Epel ES, Willett WC, Rimm EB, Laraia BA. Household food insecurity is positively associated with depression among low-income supplemental nutrition assistance program participants and income-eligible nonparticipants. J Nutr (2015) 145(3):622–7. doi:10.3945/jn.114.199414
38. Berkowitz SA, Seligman HK, Choudhry NK. Treat or eat: food insecurity, cost-related medication underuse, and unmet needs. Am J Med (2014) 127(4):303–10. doi:10.1016/j.amjmed.2014.01.002
39. Tarasuk V, Cheng J, Oliveira CD, Dachner N, Gundersen C, Kurdyak P. Association between household food insecurity and annual health care costs. CMAJ (2015) 187(14):E429–36. doi:10.1503/cmaj.150234
40. Neter JE, Dijkstra SC, Dekkers ALM, Ocke MC, Visser M, Brouwer IA. Dutch food bank recipients have poorer dietary intakes than the general and low-socioeconomic status Dutch adult population. Eur J Nutr (2017). doi:10.1007/s00394-017-1540-x
Keywords: economic crisis, food insecurity, Mediterranean diet, non-communicable diseases, health-related quality of life, health resources consumption
Citation: Gregório MJ, Rodrigues AM, Graça P, de Sousa RD, Dias SS, Branco JC and Canhão H (2018) Food Insecurity Is Associated with Low Adherence to the Mediterranean Diet and Adverse Health Conditions in Portuguese Adults. Front. Public Health 6:38. doi: 10.3389/fpubh.2018.00038
Received: 03 November 2017; Accepted: 01 February 2018;
Published: 21 February 2018
Edited by:
Onyebuchi A. Arah, University of California, Los Angeles, United StatesReviewed by:
Mario Ulises Pérez-Zepeda, Instituto Nacional de Geriatría, MexicoTerri Kang Johnson, Dexcom, Inc., United States
Copyright: © 2018 Gregório, Rodrigues, Graça, de Sousa, Dias, Branco and Canhão. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helena Canhão, aGVsZW5hLmNhbmhhb0BubXMudW5sLnB0
†These authors have contributed equally to this work.