 Sherrilene Classen1
Sherrilene Classen1 Sandra M. Winter1Charles Brown2
Sandra M. Winter1Charles Brown2 Jane Morgan-Daniel3
Jane Morgan-Daniel3 Shabnam Medhizadah1*
Shabnam Medhizadah1* Nithin Agarwal2
Nithin Agarwal2- 1Department of Occupational Therapy, University of Florida, Gainesville, FL, United States
- 2University of Florida Transportation Institute, Gainesville, FL, United States
- 3Health Science Center Libraries, University of Florida, Gainesville, FL, United States
Distracted driving, especially driver inattention, is associated with high levels of crash-related fatalities and injury. Teen novice drivers are one of the groups most likely to drive distracted and to suffer its consequences. Teens have a higher risk of engaging in texting or secondary tasks, e.g., eating while driving. Distracted driving interventions to date aim to improve teen and societal safety, but few have achieved effectiveness. A need exists for effective evidence-based distracted driving interventions. We used an integrative review to identify rigorous evidence, and inform the development of a teen distracted driving educational intervention. This five-step review included: identifying the research problem; collecting literature; evaluating literature; synthesizing data; and presenting results. We searched 6 databases, identifying 185 articles. Following three rounds of inclusion screening (title, abstract, and full-text), captured according to a PRISMA flow chart, 17 studies met inclusion. We categorized these studies, conducted in the U.S., as five intervention types that used approaches including presentations, videos or instructional programs, education or training programs, driving simulator training, in-vehicle monitoring or feedback, and integrated programs. Study designs included randomized controlled trials pre-post, quasi-experimental, and experimental designs with prospective longitudinal cohorts. The studies were heterogeneous in design, intervention and outcome. However, three core themes emerged across studies: i.e., hazard awareness, hazard mitigation and attention maintenance are primary critically necessary skills to prevent distracted driving; engaging a parent or adult as a partner in the intervention process from classroom to car contributed to the effectiveness of the intervention; and leveraging technology in training enhanced the effectiveness of the intervention. Study limitations pertained to a focus on short-term effects; sampling distributions that did not account for gender, age, race, and/or ethnicity; types of interventions; and bias. The limitations affect the generalizability of included study findings and, potentially, the review findings, as they may not apply to populations or contexts outside those synopsized. Strengths included our team's expertise in conducting evidence-based reviews, support of a health science librarian, and use of international review guidelines. As an outcome, we are applying findings of the integrated review to develop a computer-based training addressing teen distracted driving.
Introduction
Distracted driving, a specific category of driver inattention, is a public health epidemic associated with high levels of crash-related fatalities and injury (1, 2). Distracted driving has high personal, societal and economic costs. Specifically, in 2010 it was estimated that crashes in which at least one driver was identified as being distracted resulted in the loss of $40 billion in economic costs (e.g., medical costs, legal and court costs, emergency service costs, property damage) and 123 billion in societal harm (3). Risks created by distracted drivers affect the driver, their passengers, and other road users. Basic categories of distractions, next explained, include those associated with visual, cognitive, and/or motor distractions (4). Visual distractions involve taking eyes off the road—such as looking at the radio, or staring at a crash scene. Cognitive distractions occur when the driver is not mentally focused on their driving, such as when creating a voice-to-text message. Motor distractions are tasks such as eating, drinking or grooming, while driving. Distractions may combine the three categories, such as a driver who is placing a call (motor), looking at the phone (visual), and thinking about what to say (cognitive).
In the U.S. in 2015, 10% of fatal crashes were distraction-affected, resulting in 3,477 fatalities (5). A “distraction-affected crash” indicates that one of the drivers involved was identified as distracted at the time of the crash (6). Similarly, 15% of injury crashes in 2015 were distraction affected, resulting in 391,000 injuries (5). However, the scope of the problem is likely underestimated as the assessment and on-scene crash coding to identify distraction are often lacking. Compared to other crash predictors, e.g., the influence of bad weather, determination of distraction factors is more difficult. Despite the difficulty in determining the full extent of the distracted driving problem, we do know that teen drivers represent a significant portion of distraction-impaired drivers (7).
Teens and Distracted Driving
Teens are the group most likely to drive distracted and to suffer its consequences. Amongst drivers of all ages involved in fatal crashes, those ages 15–19 had the highest proportion of drivers judged as distracted at the time of the crash (8). For children, youth, and young adults age 8–24, motor vehicle crashes are the primary cause of death, with teens having the highest proportion of distraction-related fatalities (7).
Today's teens, to a large extent, live connected lives via computers, cell phones, and other electronic devices. Remaining engaged with others in a variety of locations and situations is for many an ingrained habit which has become the societal norm (9, 10). Reports of teen texting vary from 30 to 100 texts a day (9, 11), and over 40% of teens report texting and driving in the last 30 days, according to a Centers for Disease Control and Prevention (CDC) survey (12). In addition to using their phones, teens are more likely to engage in other types of secondary tasks which are distracting and to have longer periods of off-road glances (13). Distracted driving is risky for drivers of all ages, but research shows that these types of behaviors are riskier for novice drivers (14, 15). The proposed reasons for this are tri-fold: First, novice drivers lack skills in hazard anticipation and fail to fully grasp the risks involved in distracted driving (14, 15). For this reason, they may choose to engage in distracted driving in higher-risk driving situations, compared to more experienced drivers (15). Second, teens are not as experienced in hazard mitigation. When driving risks are experienced they do not have the skill set or the level of skill needed to avoid the hazard, or negotiate the hazard, without harm (14). Third, teens have more difficulty with attention maintenance. Teen drivers, often engage in other sensory activities while driving, may be challenged when they are tasked to maintain continuous engagement with a less-stimulating road environment. Thus, they may potentially respond to such a challenge by seeking stimuli that also enable distraction (15). Given the extent of the problem, and the unique factors underlying teen distracted driving as compared to adults, the need for a teen-specific distracted driving intervention is clear.
Intervention Approaches
Documented interventions for distracted driving amongst teens have the potential to improve teen as well as societal safety (1, 14, 16–19). Such intervention approaches include those with positive (e.g., messages encouraging adoption of no phone use in car), negative (e.g., regulation of texting and driving), or adverse reinforcers (e.g., loss of driving privileges for violation of graduated driver licensing rule on passengers) for undesired behaviors and those with a mixture of the aforementioned.
In general, the effectiveness of prior interventions, i.e., translation of the interventions to preventing crashes and saving lives, with teen drivers is low (14). In response, best practices have been put forth specific to teen driver education and training, including the following:
• Using a highly appealing curriculum that is engaging and captures their attention (14);
• Training teens for new knowledge and presenting novel material and learning challenges in a tiered, development-based manner (20);
• Focusing on very specific skills such as “resistance skills” to peer influence or behind-the wheel skills in environments from parking lot to highway (14, 19);
• Providing scenarios to facilitate application of knowledge and rehearsal of driving skills (19, 21); and
• Emphasizing parent education and training in monitoring teen driving (9, 22).
Clearly, distracted driving is a public health issue and a target for intervention (23). Therefore, successful intervention plans to mitigate teen distracted driving are of critical need for teen safety and public health safety.
Rationale and Significance
Efforts to address distracted driving must be developed and implemented in a way that targets the teen drivers' needs in the context of the regulatory environment. Such an environment includes knowledge of statewide resources and/or following procedures related to the state's highway safety, state laws, and state regulations. Currently only a few state-focused teen programs exist. One such program is IMPACT Teen Drivers available in California. The goal of this program is to address teen distracted driving and reckless driving and the content includes resources from informational handouts to videos targeting six stakeholder groups, such as teens and parents. Successes of this program are its nationwide recognition and outreach across states to include Texas and Pennsylvania, and with eight additional community partners. Because no formal program exists in the State of Florida, and in order to meet the needs and requests of the Florida Department of Transportation, and in support of the Strategic Highway Safety Plan for Florida, we synthesized the research published between 2000 and 2017, on teen distracted driving as a foundation for model program development of a computer-based training program.
Aim
The aim of this study was to conduct an integrative review of published research and nationwide model programs on teen distracted driving. An integrative review design provides a synthesis of knowledge on a topic and address the significance of included study results for practice (24). The research question was: According to the distracted driving literature, what are the most efficacious and effective interventions to reduce the number of crashes, injuries, and/or fatalities among teen drivers in the United States?
Methods
A preliminary review by the University of Florida Institutional Review Board indicated an integrative review did not fall under their purview.
Design
We used an integrative review methodology because it is the most appropriate for identifying evidence from teen-distracted driving educational interventions. The five steps that guided this review included: identify the research problem, collect the literature, evaluate the literature, synthesize, and integrate the data and present the results (24, 25). Our approach provided a robust framework for data collection, analysis, and synthesis. We performed this review over two phases where the first included title and abstract screening, and the second included an in-depth full-text extraction and synthesis.
Protocol and Registration
The integrative review framework and the PRISMA-P 2015 checklist guided protocol development. The health sciences librarian's (JMD) preliminary search for related integrative reviews and systematic reviews on October 30, 2017, yielded no relevant registrations in either the JBI Database of Systematic Reviews, or Implementation Reports or in International Prospective Register of Systematic Reviews (PROSPERO). The protocol for this study was not registered, corresponding with PROSPERO's statement that review types other than systematic reviews are not eligible for inclusion (26).
Search Methodology
The health sciences librarian conducted a systematic literature search. The base form of the search strategy was developed through the Population, Interventions, Comparators, Outcomes, and Study Design (PICOS) framework (27). Five inclusion criteria were: participant population included motor vehicle drivers aged 15–19; interventions were related to reducing teen driver inattention and distraction-related motor vehicle crashes, injuries, and/or fatalities; comparators were unspecified; outcomes addressed driving performance in relation to improving driver behavior, attitudes toward risk-taking, and knowledge of forms of distracted driving; and study design was experimental, quasi-experimental, systematic review, or experimental designs with prospective longitudinal cohorts, within the context of efficacious and effective intervention studies. Additional search criteria included publication in the English language, for the time period of January 2000 to November 2017.
Refinement of the search strategy occurred via project team recommendations, MeSH and keyword term testing in PubMed and Web of Science, and peer-review by a second health science librarian. During November 22–23, 2017, the final search was conducted on six bibliographic databases that had been selected as relevant to the topic of interest as displayed in Table 1. These databases included EBSCO Host's CINAHL, PsycINFO, ProQuest's ERIC, PubMed (NCBI), Transport Research International Documentation, and Web of Science. The search strategy was adapted for each database through truncation and phrase-searching (in the title and abstract fields where available), limiters (English language and 2000–2017 publication years), and subject headings (CINAHL Headings, ERIC Descriptors, Thesaurus of Psychological Index Terms, MeSH, Transportation Research Index Terms). Gray literature was identified within these six databases, but was limited to book chapters, conference abstracts, conference proceedings, policy documents, and white papers (28). The completed search strategy is available from the librarian.
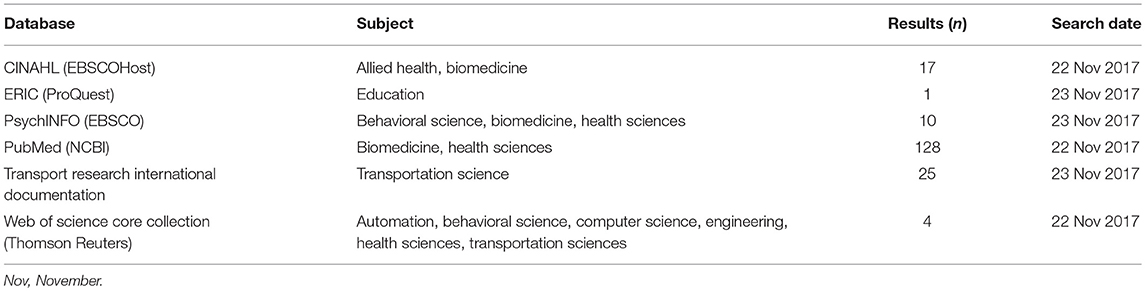
Table 1. Database searched by subject, results and search date.
Search Outcome
A total of 185 studies, retrieved from the database searches, were exported to Mendeley Desktop, and de-duplicated. One-hundred and eighty-five unique studies were identified and progressed to a screening stage where titles and abstracts were retrieved and reviewed. No additional records were identified through other sources.
For agreement between raters after the full-text assessment, (n = 17) a perfect κ of 1.0 was reached for each dyadic group.
Data Abstraction and Synthesis
A title and abstract screening was conducted on these 185 studies. Team members (n = 6) were first randomized into dyad pairs (i.e., three total groups comprising two researchers each). A total of 137 records, that did not match the study's inclusion criteria were excluded. Decisions of team members were analyzed in their dyad pairs for inter-rater reliability. We used Cohen's kappa coefficient (κ) to measure inter-rater agreement, which is considered a more robust measure than simple percent agreement calculation because κ considers the possibility of the agreement occurring beyond chance (29).
Next, a full-text evaluation was performed on the 34 remaining studies. Dyad groupings remained the same, but studies being evaluated were again randomized among the dyad pairs. We excluded 14 studies at full text evaluation stage. Subsequently, we extracted and recorded data from 17 studies using the following subheadings: reference(s), age of population, study type, purpose of study, funding source, location of study, gender characteristics, sample size(s), intervention type(s), study outcomes, study comparisons, intervention duration, effect size(s), effectiveness of interventions, and study limitations. Figure 1 illustrates the process of abstract and full text screening.
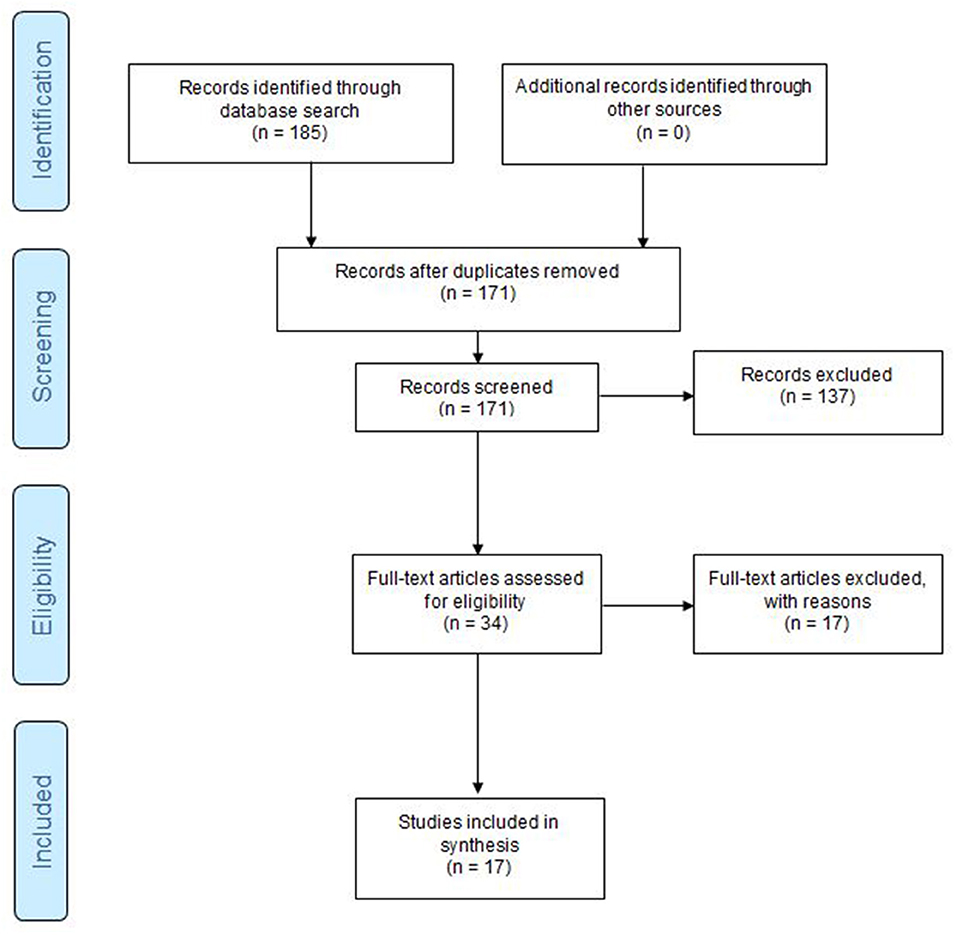
Figure 1. PRISMA P Flow Diagram of abstract screening and full text extraction process. Flow Diagram adopted from Moher et al. (30).
Critical Appraisal
Copper (31) suggests that extraction of specific methodological characteristics of primary studies could be used to evaluate overall quality of the studies. The Joanna Briggs Institute provides a Critical Appraisal Checklist for Randomized Controlled Trials (32). As such, we used a combination of the aforementioned approaches to appraise the studies.
Results
Inter-rater Reliability
The first round of reviews indicated fair agreement with Cohen's kappa (κ) = 0.31–0.34 (0.21–0.40 is considered fair) (29). For this review, the a-priori determined kappa was >0.81. Therefore, re-screening occurred among the groups to arrive at complete agreement with κ = 1.0.
Descriptive Profile of the Primary Studies
The 17 experimental studies that underwent critical review, is displayed in Table 2.
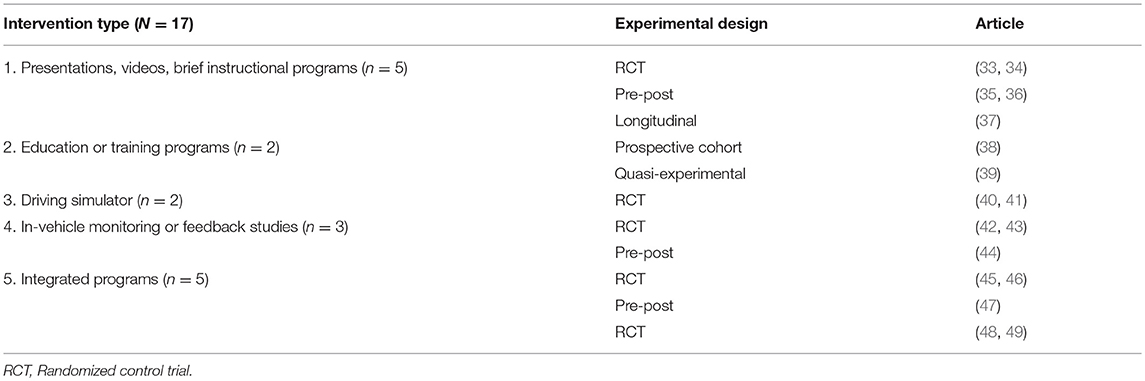
Table 2. Summary of intervention types separated by experimental designs.
These studies all comprised subjects 15- to 19-years old, had experimental designs which included randomized controlled trials (RCT) (n = 10), pre-post designs (n = 4), quasi-experimental trial (n = 1), longitudinal follow up from an experimental design (n = 1) and a prospective cohort following an experimental design (n = 1). While these studies generally examined distracted driving interventions and effectiveness, heterogeneity was observed in the intervention type, as next described.
Interventions
The studies were thematically characterized in relation to the intervention type and delivery methods to help inform our model program in development. Table 2 indicates the five categories of interventions employed by design: presentations, videos, or brief instructional programs (n = 5) (33–37); education or training programs (n = 2) (38, 39); driving simulators (n = 2) (40, 41); in-vehicle monitoring or feedback studies (n = 3), (42–44); and integrated programs (n = 5) (45–49).
Delivery Methods
Since delivery methods were combined in studies, several studies adopted more than one delivery method. However, the majority of interventions utilized educational trainings or presentations (34, 35, 37–39, 45, 48, 49). These methods are easier to present in multiple locations and to larger groups. Alternatively, on-road assessments via self-evaluation or driving performance feedback (33, 42–44, 46, 47) and driving simulation interventions (40, 45–49) provided the ability to learn skills in a real-world setting or simulated environment representative of the real world. Interventions that were PC-based, web-based, or through an e-learning platform had the benefit of remote delivery to teens, parents and other users. Moreover, these modes of delivery accommodated the time, location, and pace of instruction to the participants (33, 46, 47). 36 examined use of instructional videos. Benefits of this mode include that it provides consistent content delivery in a cost-effective way that is not reliant on in-person instruction. Three studies using persuasive messaging leveraged this strategy to shift the attitudes of teens against distracted driving behaviors (33, 35, 39).
At healthcare facilities education teams could work with health care professionals who had a first-hand knowledge of the injury outcomes of distracted driving. Healthcare facilities are uniquely positioned to be able to offer trauma survivor testimony or a mock trauma session (35, 38); and to reinforce experiences with a hospital or trauma center tour (35). Two studies focused on including peers or parents in a peer-generated anti-texting program (39), or a parent-teen driving agreement (34). Messages delivered by peers and parents are recognized as more effective compared to interventions who did not include peers or parents.
Integrated Review Findings
Table 3 displays results from the 17 included studies by design type, authors (year), study details, sample size, effectiveness and funding. The sample sizes ranged from small (N = 12) to large (N = 1,365). Although not always clearly documented in the outcome of the primary studies, the research team categorized the outcomes of each included study in terms of efficacy or effectiveness, with 100% agreement among team members. That is the team assessed if their study outcomes aligned with our outcomes of interest (i.e., teen crashes, injuries, or fatalities as well as driver ability, skill or performance). Of the 17 studies, and based on their findings as published, we categorized studies as effective (or not) or efficacious (or not), or indicate when this detail was not stated. Only 15 of the 17 studies reported funding from state and federal highway traffic safety entities, National Safety Council, associations for law enforcement, teacher associations, or healthcare corporations, among others.
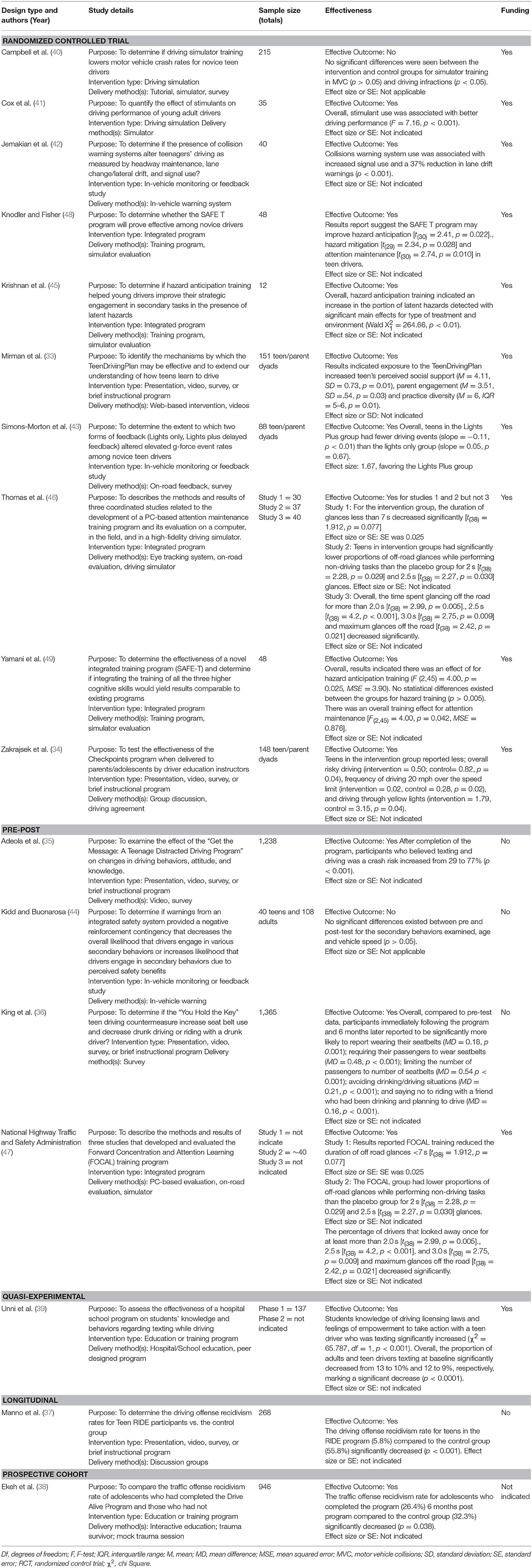
Table 3. Study summaries by design type, author, study details, sample size, effectiveness, funding and outcomes.
Interventions Studied by Type of Experimental Design
Ten of the 17 studies were RCTs, of which all but 1 presented results supporting intervention effectiveness. The most common effective interventions, documented in five studies, focused on one or more of three critical skills underpinning driving: i.e., hazard awareness, hazard mitigation, and attention maintenance (45–49).
Interventions deploying in-vehicle technology, for monitoring or feedback, were less common but two RCTs provided evidence in favor thereof (42, 43). Interventions effective for on-road outcomes of teens' driving behavior targeted a RCT with training content to establish parent/teen driving contract (34), or web-based instructional modules for parents/teens that focused on knowledge for novice drivers and provided teen driving practice guidance (33). A quasi-experimental design was used to study a hospital/school partnership for an educational campaign (39). The campaign targeted teens and adults, who were primarily teachers. This campaign was effective on outcomes of empowering teens to stop others' texting, as well as to curtail personal texting. School observation of drivers' texting behavior at the end of campaign demonstrated an overall decrease of drivers' texting from 13 to 10% with a greater difference for teens vs. adults. Studies that provided support for effectiveness of educational programs among juvenile traffic offenders included a longitudinal study (37) and a prospective cohort study (38). One unique study addressed a sub-population of teens, those with Attention Deficit Hyperactivity Disorder (ADHD), and an intervention of stimulant medication. For teens with ADHD, Cox et al. (41) RCT found that stimulant use, compared to placebo, was associated with improved driving (e.g., more time spent on the road vs. shoulder, smoother braking, less speeding, better speed consistency, appropriate use of brakes, and slower more controlled turns).
Only two interventions were not shown to be effective. The studies with negative results included an RCT study of simulator training with outcomes of motor vehicle crash occurrence or driving infractions in the 6–12 months post-intervention (40), as well as a pre-post study examining the effectiveness of warnings from in-vehicle monitoring measuring engagement in secondary behaviors (i.e., driving distractions) as outcomes (44).
An integration of the results above suggest that a model program to decrease teen distracted driving may contain the following elements: First, hazard awareness, hazard mitigation, and attention maintenance are essential ingredients for curbing distracted driving. Second, in-vehicle technology, for monitoring or feedback, contributes to the success of driving without distraction. Third, a parent/teen driving contract is essential for curtailing distracted driving behaviors. Fourth, partnerships among organizations have beneficial outcomes to mitigate forms of distracted driving, if the partners provide support of a targeted educational campaign addressing such behaviors. Finally, effectiveness for educational programs exist for juvenile traffic offenders (37, 38), or when teens with medical conditions drive with optimal therapeutic dosages of their medications (41).
Discussion
By reviewing and extracting data from 17 studies, we synopsized interventions for distracted driving and recorded outcomes of efficacy or effectiveness. Interventions commonly targeted three elements of driving: hazard awareness, hazard mitigation, and attention maintenance (15). Improvements in these skills were confirmed by interventions targeting one [i.e., hazard anticipation, (45)] or all three of these skills [e.g., Yamani et al. (49)].
The theme of using technology was present in about half of the studies. For example, simulators were used in 7 of the 17 studies as either as a training tool, or as a method of measuring driving performance. Moreover, in-vehicle warnings were also successfully used as interventions to shape teen's driving behaviors such as lane maintenance (42) or smoother acceleration/braking (43).
We identified parent/adult driver involvement as an important attribute to the success of the intervention. Specifically, parent/adult driver involvement lends itself to an educational intervention strategy to improve carry-over of learning, as well as improving the quality and diversity of driving practice (12, 19).
Finally, partnerships among organizations may have beneficial outcomes to mitigate forms of distracted driving, if the partners provide support to a targeted educational campaign addressing such behaviors (39). This finding has specific application for our model educational program in development. That is a computer based training (CBT) program, with collaboration between the Florida Department of Transportation and the University of Florida will target mitigating distracted driving in teens. Potential opportunities also exist to target juvenile offenders, with an expectation of successfully curbing distracted driving after exposure to the CBT.
The last 40 years have seen a downturn in driver education as a component of secondary education in the U.S. and as a priority of NHTSA (20). As new driver education programs and strategies are being developed, research, as is the case in this integrated review, must guide state and national initiatives in the use of the most efficacious and effective strategies. Such strategies may be beneficial in curbing fatalities and injuries from teen distracted-driving crashes.
Limitations
While several of the studies reported effectiveness, only one, the FOCAL program (47) used a longitudinal design and showed long-term outcomes in favor of reduced teen crash risk. Several study authors noted unequal sample distribution in including studies with only males, studies not representing the age range of novice drivers, and studies lacking diversity of race or ethnic background of participants. These types of sampling limitations can compromise internal validity as well as generalizability of results. Generalizability of results may also be a limitation of driving simulator studies or of studies conducted in a particular geographic area. As shown by the breakdown of studies, lack of randomization was a limitation for some studies, and other studies reported low levels of participation and/or attrition that occurred if the study protocol had multiple sessions. The studies were subject to multiple forms of bias. This includes selection bias, i.e., convenience sampling; self-report bias, i.e., asking teens to report their driving behaviors; spectrum bias, i.e., failing to test relevant sub-groups in a study; Hawthorne bias, i.e., behavior may change when observed; learning effects bias, i.e., use of the same simulator scenarios; and order effects, i.e., using the same simulator scenarios without randomization of scenes. We recognize that distracted driving is multi-faceted, however our focus was on observed behaviors representing distraction. Thus, medical conditions, drug use, and/or alcohol use impacting distraction were not examined independently. We included teens between the ages of 15–19 years as a “homogenous group.” Although we acknowledge that heterogeneity and variability exists for driving performance, skill and experience.
Strengths
This review was conducted by an experienced team who followed the PICOS framework and guidance from the Joanna Briggs Institute on conduct of a review (27). The search strategy was implemented by a health science center librarian and studies were selected using clear inclusion and exclusion criteria. A rigorous measure of reliability was used to assess the level of consistency among dyad pairs to include/exclude studies from the abstract and full text reviews. An iterative team approach ensured consensus among team members during all aspects of the integrated review process.
Implications/Future Directions
This review, and the related findings, contributes to developing an evidence-based CBT intervention on teen distracted driving. As such, these findings highlighted the state of empirical knowledge on distracted driving interventions to our stakeholders (i.e., Florida Department of Transportation State Safety Office, advocacy groups for teen driving safety, and teen drivers themselves).
The integrative review identified the vital link between skills training and crash reduction as well as the effectiveness of computer-based interventions. Further, the review suggested an appropriate outline and approach. This includes providing teens with an informational foundation followed by skills training in the areas of hazard awareness, hazard mitigation, and attention maintenance. This occurs within a framework that balances a positive informational approach with an appropriately cautionary approach. Moreover, a CBT will be supported by two organizations, the Florida Department of Transportation and the University of Florida, with a mission driven focus to decrease and prevent teen distracted driving.
Author Contributions
SC developed and designed the review. JM-D carried out the database search for the integrative review. CB, NA, SC, SW, and JM-D assisted with conducting the review and integrating findings. SC wrote the manuscript with support from SW, JM-D, and SM.
Funding
This work was supported by the Department of Transportation, Highway Safety Subgrant (subgrant number DD-18-04-01/G0Q23).
Disclaimer
This report was prepared for the FDOT State Safety Office, Department of Transportation, State of Florida, in cooperation with the National Highway Traffic Safety Administration, U.S. Department of Transportation and/or Federal Highway Administration, U.S. Department of Transportation. The conclusions and opinions expressed in these reports are those of the Subrecipient and do not necessarily represent those of the FDOT State Safety Office, Department of Transportation, State of Florida, and/or the National Highway Traffic Safety Administration, U.S. Department of Transportation and/or Federal Highway Administration, U.S. Department of Transportation, or any other agency of the State or Federal Government.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. National Highway Traffic and Safety Administration. Driver Distraction: A Review of the Current State-of-the-Knowledge. (DOT HS 810 787). Washington, DC: U.S. Department of Transportation (2008).
2. National Highway Traffic Safety Administration. Traffic safety facts 2012: Young drivers. Washington, DC: Department of Transportation (2012).
3. Blincoe LJ, Miller TR, Zaloshnja E, Lawrence BA. The Economic and Societal Impact of Motor Vehicle Crashes 2010. (Revised) (Report No. DOT HS 812 013). Washington, DC: National Highway Traffic Safety Administration (2015).
4. Vegega M, Jones B, Monk C. Understanding the Effects of Distracted Driving and Developing Strategies to Reduce Resulting Deaths and Injuries: A Report to Congress. Washington, DC: National Highway Traffic Safety Administration (2013).
5. National Highway Traffic and Safety Administration. Traffic Safety Facts - Research Note, Distracted Driving 2015. (DOT HS 812 381). Washington, DC National Highway Traffic and Safety Administration (2017).
6. National Traffic Law Center. Investigation and Prosecution of Distracted Driving Cases (DOT HS 812 407). Washington, DC: National Highway Traffic Safety Administration (2017).
7. National Highway Traffic and Safety Administration. Traffic Safety Facts - Research Note, Motor Vehicle Crashes as a Leading Cause of Death in the United States, 2015. (DOT HS 812 499). Washington, DC: National Highway Traffic and Safety Administration (2018).
8. National Highway Traffic and Safety Administration. Trafic Safety Facts: Distracted Driving 2011 (DOT HS 811 737). Washington, DC: National Highway Traffic and Safety Administration (2013).
9. Delgado MK, Wanner KJ, McDonald C. Adolescent cellphone use while driving: an overview of the literature and promising future directions for prevention. Media Commun. (2016) 4:79–89. doi: 10.17645/mac.v4i3.536
10. Foss RD, Goodwin AH. Distracted driver behaviors and distracting conditions among adolescent drivers: findings from a naturalistic driving study. J Adolesc Health. (2014) 54:S50–60. doi: 10.1016/j.jadohealth.2014.01.005
11. Lenhart A. Teens Social Media & Technology Overview 2015: SMARTPHONES Facilitate Shifts in Communication Landscape for Teens. Washington DC (2015). Available online at: www.pewinternet.org/2015/04/09/teens-social-media-technology-2015
12. Olsen EO, Shults RA, Eaton DK. Texting while driving and other risky motor vehicle behaviors among US high school students. Pediatrics. (2013) 131:e1708–15. doi: 10.1542/peds.2012-3462
13. Simons-Morton BG, Guo F, Klauer SG, Ehsani JP, Pradhan AK. Keep your eyes on the road: young driver crash risk increases according to duration of distraction. J Adolesc Health. (2014) 54:S61–7. doi: 10.1016/j.jadohealth.2013.11.021
14. Buckley L, Chapman RL, Sheehan M. Young driver distraction: State of the evidence and directions for behavior change programs. J Adolesc Health. (2014) 54(Suppl. 5):S16–21. doi: 10.1016/j.jadohealth.2013.12.021
15. Carter PM, Bingham CR, Zakrajsek JS, Shope JT, Sayer TB. Social norms and risk perception: predictors of distracted driving behavior among novice adolescent drivers. J Adolesc Health. (2014) 54(Suppl. 5):S32–41. doi: 10.1016/j.jadohealth.2014.01.008
16. Carey RN, Sarma KM. Threat appeals in health communication: messages that elicit fear and enhance perceived efficacy positively impact on young male drivers. BMC Public Health. (2016) 16:1–16. doi: 10.1186/s12889-016-3227-2
17. Layba C, Griffin LW, Jupiter D, Mathers C, Mileski W. Adolescent motor vehicle crash prevention through a trauma center-based intervention program. J Trauma Acute Care Surg. (2017) 83:850–3. doi: 10.1097/TA.0000000000001605
18. Merrikhpour M, Donmez B. Designing feedback to mitigate teen distracted driving: a social norms approach. Acci Anal Prevent. (2017) 104:185–94. doi: 10.1016/j.aap.2017.04.016
19. Winston FK, Mirman JH, Curry AE, Pfeiffer MR, Elliott MR, Durbin DR. Engagement with the TeenDrivingPlan and diversity of teens' supervised practice driving: Lessons for internet-based learner driver interventions. Injur Prevent. (2015) 21:4–9. doi: 10.1136/injuryprev-2014-041212
20. Mayhew DR. Driver education and graduated licensing in North America: past, present, and future. J Safety Res. (2007) 38:229–35. doi: 10.1016/j.jsr.2007.03.001
21. Pollatsek A, Narayanaan V, Pradhan A, Fisher DL. Using eye movements to evaluate a PC-based risk awareness and perception training program on a driving simulator. Hum Factors. (2006) 48:447–64. doi: 10.1518/001872006778606787
22. Dellinger AM, West BA. Health care providers and teen driving safety: topics discussed and educational resources used in practice. Am J Lifestyle Med. (2014) 9:451–6. doi: 10.1177/1559827614554903
23. Lee JD. Dynamics of driver distraction: the process of engaging and disengaging. Ann Adv Automot Med. (2014) 58:24–32.
24. de Souza MT, da Silva MD, de Carvalho R. Integrative review: what is it? How to do it? Einstein. (2010) 8:102–6. doi: 10.1590/s1679-45082010rw1134
25. Hopia H, Latvala E, Liimatainen L. Reviewing the methodology of an integrative review. Scand J Caring Sci. (2016) 30:662–9. doi: 10.1111/scs.12327
26. Universty of York Centre for Reviews and Dissemination. About PROSPERO: Inclusion Criteria. (2008). Available online at: www.crd.york.ac.uk/prospero/#aboutpage
27. University of York Centre for Reviews and Dissemination. Systematic Reviews: CRD's Guidance for Undertaking Reviews in Health Care (York, UK) (2009).
28. Cooper HM, Hedges LV. The Handbook of Research Synthesis. New York, NY: Russell Sage Foundation (1994).
29. Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Measure. (1960) 20:37–46. doi: 10.1177/001316446002000104
30. Moher D, Liberati A, Tetzlaff J, Altman DG, the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of Internal Med. (2009). 151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
31. Cooper HM. Integrating Research: A Guide for Literature Review, 2nd ed. Newbury Park, CA: Sage Publications (1989).
32. Aromataris E, Fernandez R, Godfrey C, Holly C, Kahlil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. Int J Evid Based Healthcare. (2015) 13:132–40. doi: 10.1097/XEB.0000000000000055
33. Mirman JH, Albert WD, Curry AE, Winston FK, Fisher Thiel MC, Durbin DR. TeenDrivingPlan effectiveness: the effect of quantity and diversity of supervised practice on teens' driving performance. J Adolesc Health. (2014) 55:620–6. doi: 10.1016/j.jadohealth.2014.04.010
34. Zakrajsek JS, Shope JT, Greenspan AI, Wang J, Bingham CR, Simons-Morton BG. Effectiveness of a brief parent-directed teen driver safety intervention (checkpoints) delivered by driver education instructors. J Adolesc Health. (2013) 53:27–33. doi: 10.1016/j.jadohealth.2012.12.010
35. Adeola R, Omorogbe A, Johnson A. Get the message: a teen distracted driving program. J Trauma Nursing. (2016) 23:312–20. doi: 10.1097/JTN.0000000000000240
36. King KA, Vidourek RA, Love J, Wegley S, Alles-White M. Teaching adolescents safe driving and passenger behaviors: effectiveness of the you hold the key teen driving countermeasure. J Safety Res. (2008) 39:19–24. doi: 10.1016/j.jsr.2007.10.006
37. Manno M, Maranda L, Rook A, Hirschfeld R, Hirsh M. The reality of teenage driving: the results of a driving educational experience for teens in the juvenile. J Trauma Acute Care Surg. (2012) 73:S267–72. doi: 10.1097/TA.0b013e31826b00f4
38. Ekeh AP, Hamilton SB, D'Souza C, Everrett E, McCarthy MC. Long-term evaluation of a trauma center-based juvenile driving intervention program. J Trauma. (2011) 71:223–6. doi: 10.1097/TA.0b013e31821cc0fd
39. Unni P, Estrada CM, Chung DH, Riley EB, Worsley-Hynd L, Stinson N. A multiyear assessment of a hospital-school program to promote teen motor vehicle safety. J Trauma Acute Care Surg. (2017) 83:289–95. doi: 10.1097/TA.0000000000001521
40. Campbell B, Borrup K, Derbyshire M, Rogers SA, Lapidus G. Efficacy of driving simulator training for novice teen drivers. Connect Med. (2016) 80:291–6.
41. Cox DJ, Merkel L, Moore M, Thorndke F, Muller C, Kovatchev B. Relative benefits of stimulant therapy with OROS methylphenidate versus mixed amphetamine salts extended release in improving the driving performance of adolescent drivers with attention-deficit/hyperactivity disorder. Pediatrics. (2006) 118:704–10. doi: 10.1542/peds.2005-2947
42. Jemakian JS, Bao S, Buonarosa ML, Sayer JR, Farmer CM. Effects of an integrated collision warning system on teenage driver behavior. J Safety Res. (2017) 61:65–75. doi: 10.1016/j.jsr.2017.02.013
43. Simons-Morton BG, Bingham CR, Ouimet MC, Pradhan AK, Chen R, Barretto A, et al. The effect on teenage risky driving of feedback from a safety monitoring system: a randomized controlled trial. J Adolesc Health. (2013) 53:21–6. doi: 10.1016/j.jadohealth.2012.11.008
44. Kidd DG, Buonarosa ML. Distracting behaviors among teenagers and young, middle-aged, and older adult drivers when driving without and with warnings from an integrated vehicle safety system. J Safety Res. (2017) 61:177–85. doi: 10.1016/j.jsr.2017.02.017
45. Krishnan A, Samuel S, Dündar C, Romoser M, Fisher D. Evaluation of a Hazard Anticipation Training Program (STRAP) on secondary task engagement in high risk scenarios. In: Paper Presented at the Transportation Research Board 94th Annual Meeting. Washington, DC (2015).
46. Thomas FD, Pollatsek S, Pradhan A, Divekar G, Blomberg RD, Reagan I, et al. Field and Simulator Evaluations of a PC-Based Attention Maintenance Training program (DTNH22-05-D-35043). Washington, DC: National Highway Traffic and Safety Administration (2011).
47. National Highway Traffic and Safety Administration. NHTSA Computer Training Program Improves Teen Drivers' Attention to the Road (408). Washington, DC: National Highway Traffic and Safety Administration (2011).
48. Knodler MA, Fisher D. Evaluating the Effects of Integrated Training on Minimizing Driver Distraction (UMAR24-22). Cambridge, MA: New England University Transportation Center (2015).
Keywords: distracted driving, adolescent, United State of America, safety management, accidents and fatalities, attention maintenance, hazard mitigation, hazard anticipation
Citation: Classen S, Winter SM, Brown C, Morgan-Daniel J, Medhizadah S and Agarwal N (2019) An Integrative Review on Teen Distracted Driving for Model Program Development. Front. Public Health 7:111. doi: 10.3389/fpubh.2019.00111
Received: 05 September 2018; Accepted: 15 April 2019;
Published: 03 May 2019.
Edited by:
Frederick Robert Carrick, Bedfordshire Centre for Mental Health Research in association with the University of Cambridge (BCMHR-CU), United KingdomReviewed by:
Andrea Bosco, University of Bari Aldo Moro, ItalyCihad Dundar, Ondokuz Mayıs University, Turkey
Copyright © 2019 Classen, Winter, Brown, Morgan-Daniel, Medhizadah and Agarwal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shabnam Medhizadah, cy5tZWRoaXphZGFoQHVmbC5lZHU=