 Anna Blair
Anna Blair Ellie MacGregor
Ellie MacGregor Nikki Lee
Nikki Lee- 1Healthy Children Project, East Sandwich, MA, United States
- 2Academy of Lactation Policy and Practice, Forestdale, MA, United States
- 3Private Practice Lactation Consultant, Elkins Park, PA, United States
Childhood obesity is a global public health issue. As the prevalence of childhood obesity continues to rise, identification of potential interventions by public health policy makers, and health care providers is imperative. Breastfeeding, the most optimal method of infant feeding, has been demonstrated to protect against childhood obesity. Lactation support providers (LSPs) play a key role in providing education, care, and support to families considering a feeding choice. Access to professional lactation care increases breastfeeding initiation, exclusivity, and duration rates, regardless of the credential that the LSP holds. The aims of the current study were to examine the relationship between childhood obesity and breastfeeding rates in Pennsylvania (PA) counties; to examine the relationship between geographic access to professional LSPs in PA counties and breastfeeding rates; and to examine the relationship between geographic access to professional LSPs and childhood obesity in PA counties. Data were collected on 617 professional LSPs in 67 PA counties. There are 608 Certified Lactation Counselors (CLCs) and 144 International Board Certified Lactation Consultants (IBCLCs) in PA. County-level breastfeeding rates, childhood obesity rates, and the number of CLCs and IBCLCs were tested for significance at the p < 0.01 level using a two-tailed significance test and bivariate Pearson's correlation. The results show a significant, inverse relationship between breastfeeding rates and childhood obesity prevalence at the county level, p < 0.01. There is also a significant, inverse relationship between the number of CLCs and the number of all professional LSPs and childhood obesity rates at the county level, p < 0.01. Thus, the availability of breastfeeding support is significantly related to breastfeeding rates and inversely related to childhood obesity rates across Pennsylvania.
Introduction
Obesity is a global public health crisis and is strongly correlated with chronic health conditions such as diabetes, cardiovascular disease, and high blood pressure. Among children and adolescents aged 2–19 years, obesity rates are on the rise (1). According to the World Health Organization (WHO), 41 million infants and young children were overweight or obese in 2016 (2). There has been a ten-fold increase in the number of obese children and adolescents over the last four decades (3). The Centers for Disease Control and Prevention (CDC) National Center for Health Statistics (NCHS) found the obesity prevalence was 13.9% among 2- to 5-year-olds, 18.4% among 6- to 11-year-olds, and 20.6% among 12- to 19-year olds. Hispanic youth (25.8%) and non-Hispanic African American youth (22.0%) had a higher prevalence of obesity than among non-Hispanic white (14.1%) youth and non-Hispanic Asian (11.0%) youth (4).
Interventions to reduce childhood obesity are multi-faceted and must include several components. Among these interventions, breastfeeding—a behavioral variable—has been shown to decrease the risk of childhood obesity and is inversely associated with weight gain velocity and BMI among infants (5–7). While any breastfeeding is protective against childhood obesity, the WHO recommends exclusive breastfeeding for 6 months, as it conveys the strongest protective effect (8). In a recent meta-analysis, recent review, researchers concluded that exclusively breastfed infants have a 31% lower chance of later developing overweight and obesity (9). In addition, formula-fed infants consume more milk and gain weight more rapidly than breastfed infants (10). The National Academy of Medicine recommends breastfeeding as part of a broader strategy to preventing childhood obesity and recognizes that the U.S. is falling short in its efforts to support breastfeeding (11). Breastfeeding is part of the CDC's plan for state implementation of obesity prevention strategies which include nutrition, breastfeeding, physical activity, and decreased screen time (12). The promotion, protection and support of breastfeeding for the first 6 months is a critically important public health priority.
Despite the evidence that breastfeeding is the optimal feeding method for infants, breastfeeding rates remain low across the U.S. According to the CDC's 2018 Breastfeeding Report Card, among infants born in 2015 in the United States, 4 out of 5 (83.2%) started to breastfeed, but just over half (57.6%) were breastfeeding at 6 months, and only about one-third (35.9%) continued breastfeeding to 12 months (13). When parents receive support from a professional LSP who provides education and counseling during the breastfeeding process, breastfeeding initiation and duration rates increase (14). Interventions provided by LSPs within their respective Scopes of Practice, such as implementing the best practice of placing mother and baby skin-to-skin for the first hour immediately following birth, educating a family about early infant feeding cues, and delivering face-to-face anticipatory guidance to families have all been shown to increase breastfeeding duration and exclusivity (15, 16).
The United States Breastfeeding Committee (USBC), the American College of Obstetricians and Gynecologists (ACOG), and the CDC recognize Certified Lactation Counselors (CLCs) and International Board Certified Lactation Consultants (IBCLCs) as professional breastfeeding supporters (17–19). However, there are currently only 4.57 CLCs and 3.79 IBCLCs per 1,000 live births in the U.S. (20).
Informed by this evidence, the aims of the current study were: to examine the relationship between childhood obesity and breastfeeding rates in PA counties; to examine the relationship between geographic access to professional LSPs in PA counties and breastfeeding rates; and to examine the relationship between geographic access to professional LSPs and childhood obesity in PA counties.
Materials and Methods
Design
This is a cross-sectional, observational study using retrospective data.
Setting
PA is estimated to have a population of 12.81 million according to projections from the 2010 U.S. Census Bureau data. This makes PA the sixth most populous state in the country. 8.9 million residents live in urban areas of the state and 2.7 million residents live in the rural areas of the state. As of July 1, 2018, 81.8% of the population in PA identified as White, 12% identified as Black or African American, and 7.6% identified as Hispanic or Latino (21).
According to the PA Department of Health, 16.8% of children in grades K-6 during the 2017–2018 school year were considered obese (22). Among children born in 2015, 83.8% breastfed at least once, 59.2% were breastfeeding at 6 months and 39% were breastfeeding at 12 months (23).
According to the most recent publicly available data, there are 608 CLCs and 144 IBCLCs in PA. With 137,682 live births in 2017, this indicates that there are 4.42 CLCs per 1,000 births and 1.05 IBCLCs per 1,000 births in the state (24–27).
Measurement
We measured the distribution of CLCs and IBCLCs, county level breastfeeding rates, and county level childhood obesity rates across PA. Data were collected from multiple sources. The obesity rates of children in grades K-6 were published by the Pennsylvania Department of Health in September 2019. The percent of live births to mothers who breastfed in PA was published in February 2018 by the PA Department of Health (28). The total births by county in Pennsylvania were published in 2018 by the PA Department of Health (29).
The number of CLCs in PA was obtained on December 2, 2019 from the Academy of Lactation Policy and Practice (ALPP) (30). CLCs were assumed to have remained in the zip code listed when they obtained their certification. The number of IBCLCs was obtained from the International Lactation Consultant Association (ILCA) and combined with data obtained from the United States Lactation Consultant Association (USLCA) on December 2, 2019 (31). To find the number of IBCLCs on ILCA, a 283-mile search radius was used around Philadelphia, Pittsburg, and Beaver Springs. These names were cross-referenced with one another to ensure that each individual was counted only once. To find the number of IBCLCs on USLCA, a 10-mile search radius was used to search each unique zip code within the state. These names were cross-referenced with one another to ensure that each individual was counted only once. Next, the IBCLCs populated from both directories were cross-referenced to ensure that each individual was counted only once. Each individual was then counted as a LSP in their respective county. The density percentage of CLCs and IBCLCs was calculated by county to demonstrate the prevalence of professional LSPs per live births. This density percentage was calculated by taking the number of LSPs per county and dividing the total live births per county. Data on the definitions of rural, urban, and suburban counties in Pennsylvania were obtained from The Center for Rural Pennsylvania (32). Counties were designated as urban or rural in Table 1.
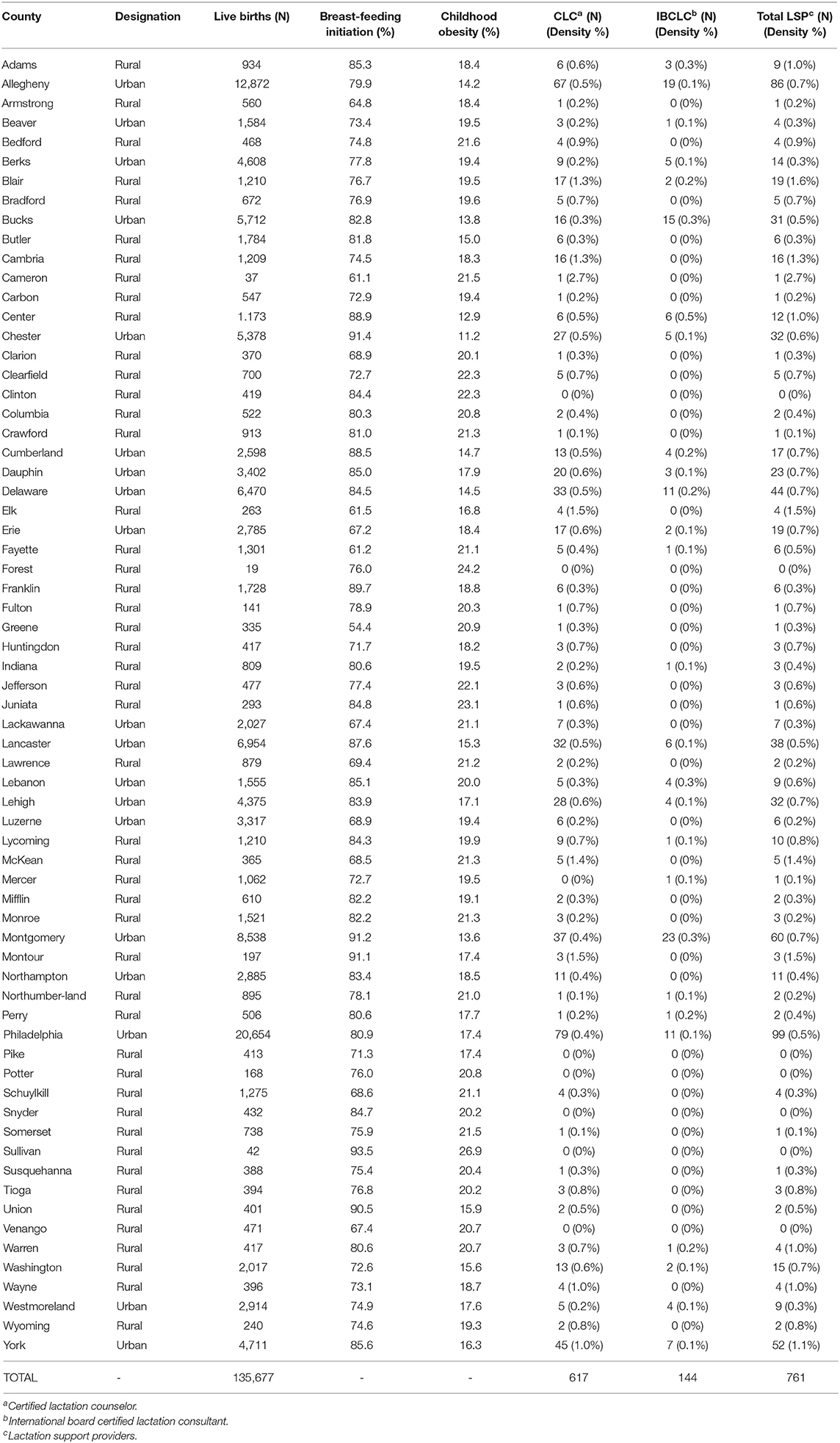
Table 1. Professional lactation support providers in PA counties.
Data Analysis
To understand the relationship between childhood obesity and breastfeeding in PA counties, we ran a two-tailed significance test at the 0.01 level and a bivariate Pearson's correlation. We graphed the linear relationship on a scatter plot. To understand the relationship between geographic access to CLCs and childhood obesity by PA county, we ran a two-tailed significance test at the 0.01 level and a bivariate Pearson's correlation. We graphed the linear relationship on a scatter plot. Further, we examined the relationship between geographic access to CLCs and breastfeeding rates by PA county by running ANOVA tests to test for significant differences in the number of CLCs by PA county and the percentage of births to mothers who breastfed at the 0.05 level. This analysis was repeated to examine the relationship between all professional LSPs and breastfeeding rates by PA county. Results were mapped to demonstrate geographic access, or lack thereof, to LSPs across the state. To understand the relationship between professional lactation support and childhood obesity by PA county, we ran a two-tailed significance test at the 0.01 level and a bivariate Pearson's correlation. We graphed the linear relationship on a scatter plot. All data analysis was conducted using IBM SPSS Statistics version 26.0 (33).
Results
Among children in grades K-6, there is a significant, inverse correlation between childhood obesity and breastfeeding rates by county in PA, r(66) = −0.395, p < 0.01 (Figure 1). During the 2017–2018 school year, 160,220 (16.8%) of children fell within, or above, the 95th percentile of weight (defined as obese). Rates of obesity were highest in the northwest area of the state.
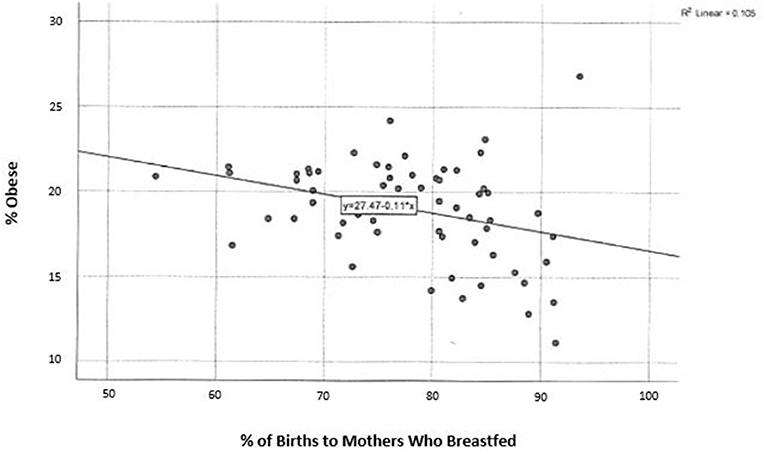
Figure 1. Percent of live births to mothers who breastfed and childhood obesity in Pennsylvania.
LSPs are unequally distributed throughout the state, with more LSPs populated in urban areas. The least amount of CLCs are located in the northwest area, excluding Erie county (Figure 2). There is a significant, inverse correlation between obesity rates and geographic access to CLCs in the state, r(66) = −0.526, p < 0.01 (Figure 4). According to the PA Department of Health, the southeastern counties of PA have the highest breastfeeding rates in the state (Table 1). In these counties, childhood obesity rates are the lowest among all geographic districts (15.2%).
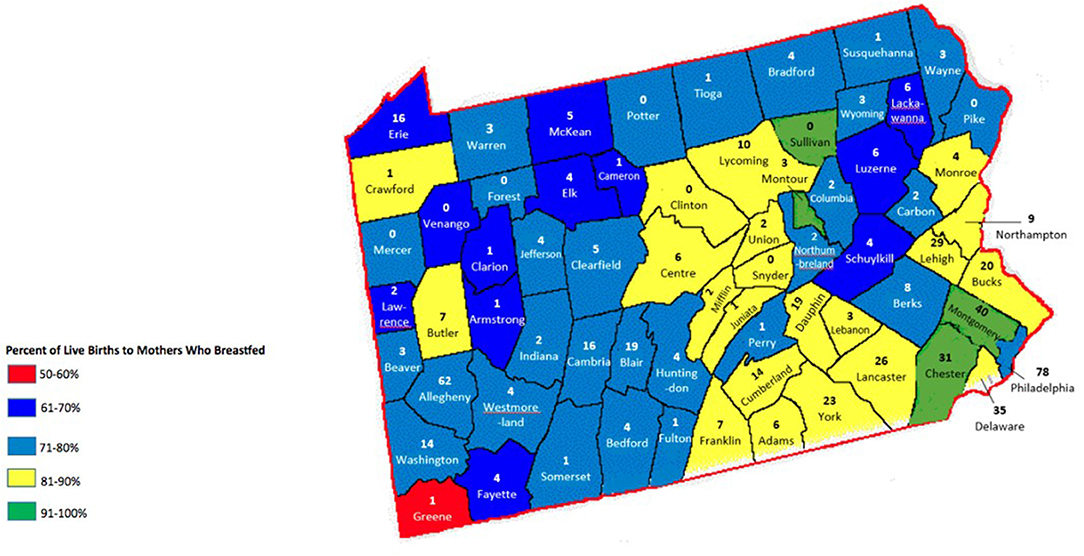
Figure 2. Certified lactation counselors in Pennsylvania counties.
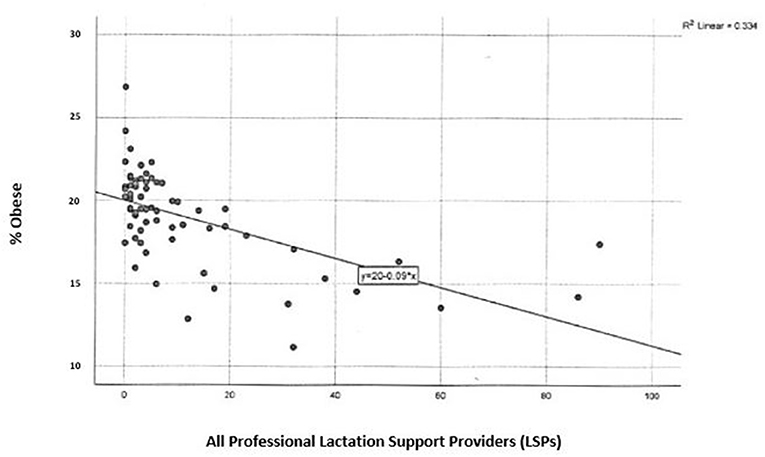
Figure 3. Professional lactation support providers and childhood obesity in Pennsylvania.
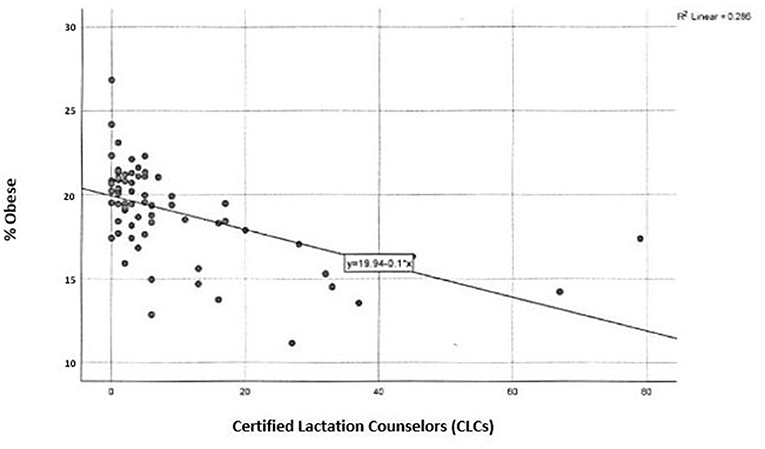
Figure 4. Certified lactation counselors and childhood obesity in Pennsylvania.
In counties where there are more CLCs and therefore families have greater geographic access to a CLC by proximity, breastfeeding rates are higher, r(66) = 0.277, p < 0.05 (Figure 2). In counties where there are more professional LSPs, breastfeeding rates are the highest, r(66) = 0.307, p < 0.05 (Figure 5).
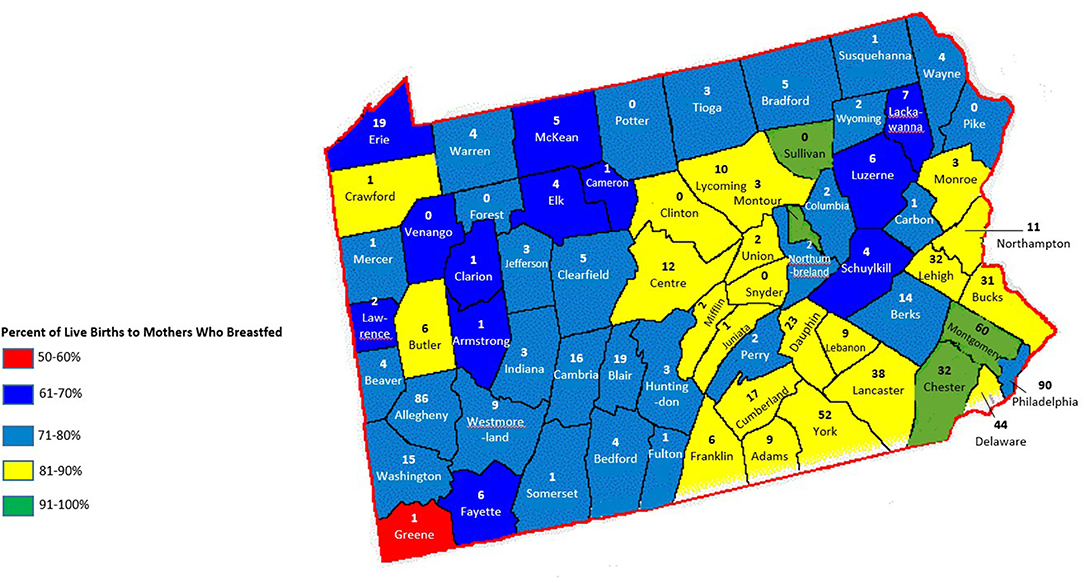
Figure 5. All lactation support professionals in Pennsylvania counties.
There are 761 professional LSPs in PA, of which 617 are CLCs and 144 are IBCLCs (Table 1). The highest concentrations of all LSPs in PA are in the southeast district of the state and there are more CLCs spread throughout all counties in PA as compared to IBCLCs (Figure 5). There is a significant, inverse relationship between childhood obesity rates and geographic access to all professional LSPs in the state, r(66) = −0.567, p < 0.01 (Figure 3).
Discussion
The data we have examined show an association between low rates of childhood obesity in counties with more LSPs in PA. LSPs, such as CLCs and IBCLCs, who support families to achieve their personal breastfeeding goals, play a pivotal role in increasing breastfeeding initiation and continuation rates.
Childhood obesity is a complex public health issue. No single factor has led to the drastic increases in childhood obesity in the U.S. Rather, research suggests that complementary changes have simultaneously decreased a child's daily energy expenditure while increasing caloric intake (34). One's diet and level of physical activity—the two risk factors most strongly correlated to obesity—have changed significantly over the past two decades. While lifestyle is a primary factor contributing to obesity among adults, infant feeding choice is a primary factor contributing to childhood obesity in early life (35). The relationship between childhood obesity and breastfeeding rates observed in this study supports the existing evidence that breastfeeding and breastfeeding support by professional LSPs can be assumed to be a protective factor against childhood obesity across PA.
Breastfeeding as an infant feeding choice should be viewed as a public health strategy to address the rising rates of childhood obesity in PA. Equitable geographic access to professional lactation support, as examined in this study, is only one component contributing to the ability to seek care when breastfeeding. Paying for LSP care may also affect a family's decision to seek help and support (36). In rural PA counties, the average household income for families is generally lower than that of families in urban counties across the state (37). Financial accessibility may be a primary consideration when accessing lactation support in rural communities.
Passed in 2010, the Affordable Care Act (ACA) requires insurers to provide coverage of breastfeeding supplies and support services (38). As some post-implementation analyses have shown, breastfeeding initiation rates did increase post-ACA implementation (39). Unfortunately, many private and public insurance companies are not paying for lactation care and services and have not reimbursed their policyholders for these costs if incurred. With limited geographic access to a professional LSP and the financial strain of receiving support, families in rural counties in PA may be discouraged from seeking help and, as a result, may not continue to breastfeed their children. As demonstrated in the current study, rural counties in PA, specifically those in the northwest district, have the highest rates of childhood obesity across the state and the lowest density of professional LSPs.
Structural barriers, such as a lack of Baby-Friendly designated hospitals, may also have an effect on breastfeeding initiation and continuation rates (40, 41). The Baby-Friendly Hospital Initiative was launched to establish environments and educational services that enhance breastfeeding experiences for new parents. The overarching goal of the initiative is to improve breastfeeding outcomes, including increased initiation, duration, and exclusivity rates. There are 14 (5.6%) Baby-Friendly designated hospitals in Pennsylvania out of the total 90 hospitals/birthing centers. Comparatively, 16.7% of U.S. hospitals/birthing centers are designated Baby-Friendly (42). In addition, 20 hospitals have received Keystone 10 designation, of which 14 are also Baby-Friendly designated. The Keystone 10 Initiative is a quality improvement initiative aimed at supporting breastfeeding families in PA through improvements to birthing facilities (43). Eighty-four out of the 90 hospitals/birthing facilities have started the process for improving maternity care services that support breastfeeding by enrolling in the Keystone 10 program. To date, less than half have completed 6 of the 10 steps to fulfill the requirements for Keystone designation. Of the 14 designated hospitals in PA, only one is located in a rural county (44). One remedy to address this disparity might be policies directed at increasing the number of Baby-Friendly hospitals through incentivizing the designation process for hospitals in rural counties (45).
Limitations
Several limitations to this study exist. First, the current study only examines geographic access to CLCs and IBCLCs and breastfeeding rates in PA. There is no data included to analyze access to La Leche League Leaders, WIC peer counselors, breastfeeding educators, doulas, lactation educators, or any other LSP in the community. The influence of breastfeeding support of any kind on breastfeeding rates should not be understated.
The IBCLC data were collected using publicly available data from the ILCA and USLCA online search databases, which are membership organizations. If an IBCLC is not listed as a provider in their county on the ILCA or the USLCA websites, they were not included in the total number of IBCLCs per county. A preferred data source using per county counts from the International Board Certified Lactation Consultant Examiners (IBLCE) was not made available for this research.
The current study utilizes retrospective data to assess the relationship between childhood obesity prevalence, breastfeeding rates, and geographic access to professional lactation support. Due to the nature of the available data, potential confounding variables were not controlled for. The strength of the current study and its results validate the need for a future, prospective study on this subject where potential confounding variables can be controlled.
Finally, many LSPs may hold their LSP credential, but may not be actively working in that role. These individuals were counted as a LSP in PA, but may be working in a different role, with limited interaction between themselves and breastfeeding families.
The facilitation of breastfeeding and assisting families in reaching their breastfeeding goals often requires support beyond the immediate postnatal period. Lactation support, counseling, and education provided by a CLC or an IBCLC is just one of many factors contributing to a successful breastfeeding experience.
Conclusions
We examined the relationship between breastfeeding rates, childhood obesity, and breastfeeding support from a CLC and from all professional LSPs in PA counties. Clearly, available breastfeeding support is significantly related to an increase in breastfeeding rates and a decrease in childhood obesity rates across PA. This analysis can be replicated in other states to increase equitable access to lactation support and counties in PA can use this blueprint as a strategy to increase breastfeeding rates and decrease rates of childhood obesity.
Data Availability Statement
All datasets generated for this study are included in the article/supplementary material.
Ethics Statement
Ethical approval for this study was not required in accordance with local legislation and national guidelines. No human studies are presented in this manuscript. This retrospective study involved the counts of individuals in the public arena using only publicly available or accessible records without contact with the individual/s. The current research is based on a review of published/publicly reported literature.
Author Contributions
AB and EM: conceptualization. AB, EM, and NL: data curation, methodology, and writing—review and editing. EM: formal analysis and software and writing—original draft.
Conflict of Interest
The authors declare the following areas of interest: the authors hold the professional LSP credentials, CLC, and IBCLC. One author was employed by the Academy of Lactation Policy and Practice (issuer of the credential CLC), one author was employed by the Healthy Children Project, Inc. (an organization that provides training for both the CLC and IBCLC examination preparation), and one author holds the credential ANLC and is a lactation consultant in private practice in PA.
Acknowledgments
Numerical data were organized by research assistant, Maret Gable.
References
1. Centers for Disease Control and Prevention. Overweight and Obesity. (2019). Retrieved from: https://www.cdc.gov/obesity/data/childhood.html (accessed January 4, 2020).
2. World Health Organization. Commission on Ending Childhood Obesity. (2019). Retrieved from: https://www.who.int/end-childhood-obesity/en/ (accessed January 4, 2020).
3. World Health Organization. Commission on Ending Childhood Obesity. (2019). Retrieved from: https://www.who.int/end-childhood-obesity/en/ (accessed January 4, 2020).
4. Hales CM, Carroll MD, Fryar CD, Ogden CL Centers for Disease Control and Prevention - National Center for Health Statistics. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. (2017). Retrieved from: https://www.cdc.gov/nchs/data/databriefs/db288.pdf (accessed January 4, 2020).
5. Wang L, Collins C, Ratliff M, Zie B, Wang Y. Breastfeeding reduces childhood obesity risks. Child Obes. (2017) 13:197–204. doi: 10.1089/chi.2016.0210
6. Azad MB, Vehling L, Chan D, Klopp A, Nickel NC, McGavock JM, et al. Infant feeding and weight gain: separating breast milk from breastfeeding and formula from food. Pediatrics. (2018) 142:e20181092. doi: 10.1542/peds.2018-1092
7. Kalies H, Heinrich J, Borte M, Schaaf B, von Berg A, von Kries R, et al. The effect of breastfeeding on weight gain in infants: results of a birth cohort study. Eur J Med Res. (2005) 10:36–42.
8. World Health Organization. Exclusive Breastfeeding to Reduce the Risk of Childhood Overweight and Obesity. (2014). Retrieved from: https://www.who.int/elena/titles/bbc/breastfeeding_childhood_obesity/en/ (accessed January 31, 2020).
9. Horta BL, de Mola CL, Victora CG. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure, and type-2 diabetes: a systematic review and meta-analysis. Acta Paediatr. (2015) 104:30–7. doi: 10.1111/apa.13133
10. Pandelova ME, Lopez WL, Kasham S, Leclercq C, Piccinelli R, Schramm KW. Assessment of energy intake of infants exclusively fed with infant formulae available on the European market. Int J Food Sci Nutr. (2009) 60:212–9. doi: 10.1080/09637480903183495
11. Institute of Medicine of the National Academies. Early Childhood Obesity Prevention Policies. (2011). Retrieved from: https://www.nap.edu/resource/13124/Young%20Child%20Obesity%202011%20Report%20Brief.pdf (accessed on January 8, 2020).
12. Centers for Disease Control & Prevention, Division of Nutrition Physical Activity and Obesity National Center for Chronic Disease Prevention and Health Promotion. State Obesity Prevention Efforts Targeting the Early Care and Education Setting. (2018) Retrieved from: https://www.cdc.gov/obesity/strategies/early-care-education/pdf/ECE_2018_QuickStartActionGuide_April2018_508.pdf (accessed on January 29, 2020).
13. Centers for Disease Control & Prevention, Division of Nutrition Physical Activity and Obesity National Center for Chronic Disease Prevention and Health Promotion. Breastfeeding Report Card, United States. (2018). Retrieved from: https://www.cdc.gov/breastfeeding/pdf/2018breastfeedingreportcard.pdf (accessed on January 8, 2020).
14. Patel S, Patel S. The effectiveness of lactation consultants and lactation counselors on breastfeeding outcomes. J Hum Lact. (2016) 32:530–41. doi: 10.1177/0890334415618668
15. Widström AM, Brimdyr K, Svensson K, Cadwell K, Nissen E. Skin-to-skin contact the first hour after birth, underlying implications and clinical practice. Acta Paediatrica. (2019) 108:1192–204. doi: 10.1111/apa.14754
16. Moore ER, Bergman N, Anderson GC, Medley N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. (2016) 11:CD003519. doi: 10.1002/14651858.CD003519.pub4
17. Centers for Disease Control & Prevention, Division of Nutrition Physical Activity and Obesity National Center for Chronic Disease Prevention and Health Promotion. Breastfeeding Report Card: Progressing Toward National Breastfeeding Goals. (2016). Retrieved from: https://www.cdc.gov/breastfeeding/pdf/2016breastfeedingreportcard.pdf (accessed January 4, 2020).
18. United States Breastfeeding Committee. Lactation Support Provider Training Directory. (2019). Retrieved from: http://www.usbreastfeeding.org/page/trainingdirectory (accessed January 15, 2020).
19. American College of Obstetricians and Gynecologists. Find Breastfeeding Professionals. (2019) Retrieved from: https://www.acog.org/About-ACOG/ACOG-Departments/Breastfeeding/Find-Breastfeeding-Professionals (accessed January 15, 2020).
20. Centers for Disease Control & Prevention, Division of Nutrition Physical Activity and Obesity National Center for Chronic Disease Prevention and Health Promotion. Breastfeeding Report Card, United States. (2018). Retrieved from: https://www.cdc.gov/breastfeeding/pdf/2018breastfeedingreportcard.pdf (accessed on January 8, 2020).
21. United States Census Bureau. QuickFacts: Pennsylvania. (2018). Retrieved from: https://www.census.gov/quickfacts/fact/table/PA/PST045218# (accessed January 3, 2020).
22. Pennsylvania Department of Health. School Health Statistics: Growth Screens/BMI-For-Age Percentiles. (2019). Retrieved from: https://www.health.pa.gov/topics/Documents/School%20Health/2017-18%20BMI%20by%20Co.pdf (accessed January 4, 2020).
23. Pennsylvania Department of Health. School Health Statistics: Growth Screens/BMI-For-Age Percentiles. (2019). Retrieved from: https://www.health.pa.gov/topics/Documents/School%20Health/2017-18%20BMI%20by%20Co.pdf (accessed January 4, 2020).
24. National Vital Statistics System – National Center for Health Statistics. Births: Provisional Data for 2017. (2018). Retrieved from: https://www.cdc.gov/nchs/data/vsrr/report004.pdf (accessed January 4, 2020).
25. Academy of Lactation Policy and Practice. Statistical Report: Number of Current CLCs in the U.S. & Territories. Retrieved from: www.alpp.org/pdf/Statistical-Report-CLCs.pdf (accessed December 2, 2019).
26. International Lactation Consultant Association. Find A Lactation Consultant Directory. (2019). Retrieved from: www.ilca.org/why-ibclc/falc (accessed December 2, 2019).
27. United States Lactation Consultant Association. Find An IBCLC Directory. Retrieved from: www.uslca.org/resources/find-an-ibclc (accessed December 2, 2019).
28. Pennsylvania Department of Health. Percent of Live Births to Mothers who Breastfed by County, Pennsylvania Resident Occurrences, 2016. (2018). Retrieved from: https://www.health.pa.gov/topics/Documents/Programs/Infant%20and%20Children%20Health/5-18_Breastfeeding%20By%20County%202016%20-%20Map_BFH.pdf (accessed December 2, 2019).
29. Pennsylvania Department of Health. Resident Live Births by Age of Mother, Counties, and Pennsylvania, 2018. (2018). Retrieved from: https://www.health.pa.gov/topics/HealthStatistics/VitalStatistics/BirthStatistics/Documents/Birth_Age_Cnty_2018.pdf (accessed March 18, 2020).
30. Pennsylvania Department of Health. Percent of Live Births to Mothers who Breastfed by County, Pennsylvania Resident Occurrences, 2016. (2018). Retrieved from: https://www.health.pa.gov/topics/Documents/Programs/Infant%20and%20Children%20Health/5-18_Breastfeeding%20By%20County%202016%20-%20Map_BFH.pdf (accessed December 2, 2019).
31. Academy of Lactation Policy and Practice. Statistical Report: Number of Current CLCs in the U.S. & Territories. Retrieved from: www.alpp.org/pdf/Statistical-Report-CLCs.pdf (accessed December 2, 2019).
32. The Center for Rural Pennsylvania. Rural Urban Definitions. (2014). Retrieved from: https://www.rural.palegislature.us/demographics_rural_urban.html (accessed December 30, 2019).
34. Anderson PM, Butcher KF. Childhood obesity: trends and potential causes. Fut Child. (2006) 16:19–45. doi: 10.1353/foc.2006.0001
35. Woo Baidal JA, Locks LM, Cheng ER, Blake-Lamb TL, Perkins ME, Taveras EM. Risk factors for childhood obesity in the first 1,000 days: a systematic review. Am J Prev Med. (2016) 50:761e79. doi: 10.1016/j.amepre.2015.11.012
36. Levesque JF, Harris MF, Russell G. Patient-centered access to health care: conceptualizing access at the interface of health systems and populations. Int J Equity Health. (2013) 12:18. doi: 10.1186/1475-9276-12-18
37. U.S. Census Bureau. 2013-2017 American Community Survey 5-Year Estimates. Retrieved from: www.factfinder.census.gov (accessed December 30, 2019).
38. Hawkins SS, Dow-Fleisner S, Noble A. Breastfeeding and the affordable care act. Pediatr Clin North Am. (2015) 62:1071–91. doi: 10.1016/j.pcl.2015.05.002
39. Hawkins SS, Noble A, Baum CF. Effect of the affordable care act on disparities in breastfeeding: the case of maine. Am J Public Health. (2017) 107:1119–21. doi: 10.2105/AJPH.2017.303763
40. Munn AC, Newman SD, Mueller M, Phillips SM, Taylor SN. The impact in the United States of the baby-friendly hospital initiative on early infant health and breastfeeding outcomes. Breastfeed Med. (2016) 11:222–30. doi: 10.1089/bfm.2015.0135
41. Phillip BL, Merewood A, Miller LW, Chawla N, Murphy-Smith MM, Gomes JS, et al. Baby-Friendly hospital initiative improves breastfeeding initiation rates in a US hospital setting. Pediatrics. (2001) 108:677–81. doi: 10.1542/peds.108.3.677
42. Baby Friendly USA. Celebrating 500 Baby-Friendly Designated Facilities in the United States. (2018). Retrieved from: https://www.babyfriendlyusa.org/news/baby-friendly-usa-celebrates-major-milestone-of-500-baby-friendly-designated-facilities-in-the-united-states/ (accessed December 18, 2019).
43. Pennsylvania Department of Health. Keystone 10 Initiative. (2020). Retrieved from: https://www.health.pa.gov/topics/programs/Breastfeeding/Pages/Keystone-10-Initiative.aspx (accessed February 5, 2020).
44. Pennsylvania Department of Health. Keystone 10 Initiative. (2020). Retrieved from: https://www.health.pa.gov/topics/programs/Breastfeeding/Pages/Keystone-10-Initiative.aspx (accessed February 5, 2020).
45. Baby Friendly USA. Baby-Friendly Facilities A-Z and By State. (2020). Retrieved from: www.babyfriendlyusa.org/for-parents/baby-friendly-facilities-by-state/ (accessed on December 18, 2019).
Keywords: breastfeeding, childhood obesity, lactation support provider, certified lactation counselor, international board certified lactation consultant
Citation: Blair A, MacGregor E and Lee N (2020) Childhood Obesity and Breastfeeding Rates in Pennsylvania Counties—Spatial Analysis of the Lactation Support Landscape. Front. Public Health 8:123. doi: 10.3389/fpubh.2020.00123
Received: 05 February 2020; Accepted: 26 March 2020;
Published: 21 April 2020.
Edited by:
Dora Il'yasova, Georgia State University, United StatesReviewed by:
Chris Fradkin, Pontifical Catholic University of Rio de Janeiro, BrazilKatalin Papp, University of Debrecen, Hungary
Copyright © 2020 Blair, MacGregor and Lee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ellie MacGregor, ZWxsaWVAYWxwcC5vcmc=