 Yan Liu1
Yan Liu1 Ying Zhu2
Ying Zhu2 Liyuan Jiang3*Chao Lu3Lijuan Xiao4Jiayu Chen2Ting Wang2Lujun Deng3Haida Zhang3Yingying Shi5Tingting Zheng6Min Feng7Tiantian Ye2Jing Wang8
Liyuan Jiang3*Chao Lu3Lijuan Xiao4Jiayu Chen2Ting Wang2Lujun Deng3Haida Zhang3Yingying Shi5Tingting Zheng6Min Feng7Tiantian Ye2Jing Wang8- 1The Second Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, China
- 2Zhejiang Chinese Medical University, Hangzhou, China
- 3Department of Acupuncture and Rehabilitation, Hangzhou Hospital of Traditional Chinese Medicine, Hangzhou, China
- 4Chun'an County Hospital of Traditional Chinese Medicine, Hangzhou, China
- 5Dingqiao Hospital of Hangzhou Hospital of Traditional Chinese Medicine, Hangzhou, China
- 6Department of Rehabilitation Medicine, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, China
- 7Department of Maternal Health Care, Maternity and Child Health Care Centers of Hechi, Hechi, China
- 8Department of Rehabilitation, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China
Background: Diastasis rectus abdominis (DRA) is one of the common complications during pregnancy and post-partum, which has psychological and physical effects on post-partum women. Acupuncture, a worldwide alternative therapy, has attracted wide attention in preventing and treating diseases related to pregnancy and childbirth. This study aims to evaluate the efficacy of acupuncture combined with physical training in treating post-partum rectus muscle dissociation.
Methods: This is a randomized, controlled trial of DRA in post-partum conducted at Hangzhou Hospital of Traditional Chinese Medicine Affiliated with Zhejiang University of Chinese Medicine. The primary purpose is to evaluate the effectiveness of acupuncture and physical training on DRA in post-partum women. The study will be conducted from March 2022 to March 2023. The acupuncture group received acupuncture and physical training (n = 48), the sham acupuncture group received sham acupuncture and physical training (n = 48), and the physical training group received physical training (n = 48). These experiments perform once/day, five times a week for 2 weeks, followed up for half a year after the end of the course of treatment. Our tests perform a course of treatment, which includes a total of 10 consecutive treatments. Furthermore, the patient will be followed up for half a year after the treatment. Primary and secondary indicators, including inter recti distance (IRD), linea alba (LA) tension, the MOS item short-form health survey (SF-36), short-form McGill pain questionnaire-2 (SF-MPQ-2), body mass index (BMI), waist-to-hip ratio (WHR), leeds dyspepsia questionnaire (LDQ), menstrual distress questionnaire (MDQ), 10 items of edinburgh post-natal depression scale (EPDS-10), the modified body self-image scale (MBIS), international consultation incontinence questionnaire short-form (ICIQ-SF) and hernia-related quality-of-life survey (HerQles), which will be evaluated before and after treatment and half a year after treatment. Adverse events and side effects during each treatment will be collected and recorded.
Discussion: There is evidence that acupuncture and physical training can treat DRA in post-partum. In this study, we evaluate the effectiveness of acupuncture in post-partum with DRA.
Highlights
- Between 35 and 70% of post-partum rectus muscle dissections fail to recover without any treatment or exercise.
- This paper presents a treatment method for post-partum rectus abdominal separation.
- Acupuncture for post-partum rectus separation as a technique of internal rectus stimulation.
Background
Diastasis recti abdominis is a condition in which both rectus abdominal muscles disintegrate to the sides, accompanied by the extension of the linea alba tissue and bulging of the abdominal wall (1). 30–70% of pregnant women develop DRA during pregnancy (2). Between 35 and 70 percent of pregnant women do not recover after giving birth without treatment or exercise (3). In addition, 39% to 45% of women still have DRA at 6 months post-partum, and the incidence of DRA at 1 year post-partum is 23–32% (1). DRA has both psychological and physical effects on post-partum women. Women with DRA primarily receive the application of support band and abdominal band during pregnancy and post-partum (4), electrical stimulation, surgical repair (5), and physical training (6). There is a lack of unified and effective treatment, and there are few studies on the efficacy and safety of DRA physical training (5, 7). As a worldwide alternative therapy, acupuncture has received wide attention in preventing and treating diseases related to pregnancy and childbirth.
Acupuncture combined with physical training can significantly improve tissue excitability, which improves blood circulation and systolic muscle function (8) and adjust the mechanical balance of the post-partum abdominal muscle group. In abdominal physical training, the increase of abdominal pressure makes the pelvic floor vulnerable to adverse effects and causes or exacerbates pelvic floor dysfunction. Acupuncture can well cause the secondary synergism of pelvic floor muscles by activating the transverse abdomens (9, 10).
However, the long-term efficacy is still unclear, and there is a lack of solid objective evidence. To date, no RCT studies the impact of acupuncture on DRA or evaluates the standardized application of DRA by acupuncture. This study comprehensively evaluates the effectiveness and safety of acupuncture in the treatment of post-partum DRA, the effective, and safety of DRA physical training. It provides a reference for clinical treatment of post-partum DRA.
Hypothesis
The hypothesis is that intervention with acupuncture is better than physical training in these outcomes of the inter recti distance (IRD) of DRA. We also expect to prove that acupuncture can be an ideal safe and conservative alternative for patients with DRA who fail in conventional physiotherapy.
Methods
This study protocol was developed under the Recommendations for Interventional Trials 2013 Statement (SPIRIT 2013) (11) (Table 1) and the Consolidated Reporting Trials statement (CONSORT 2010) when applicable (12).
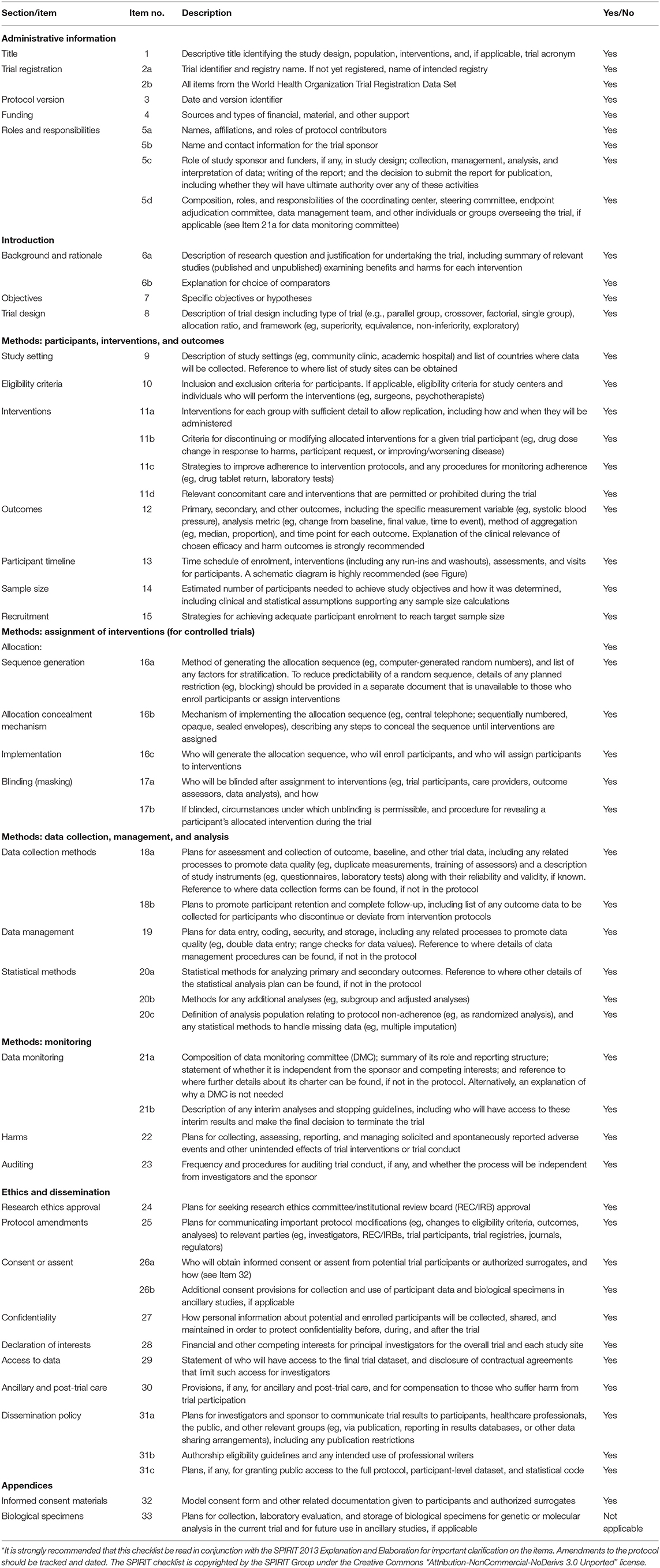
Table 1. SPIRIT 2013 checklist: recommended items to address in a clinical trial protocol and related documents*.
Study Design and Setting
This randomized, controlled clinical trial is carried out at the Hangzhou Hospital of Traditional Chinese Medicine Affiliated to Zhejiang Chinese Medical University, Hangzhou, China (Figure 1).
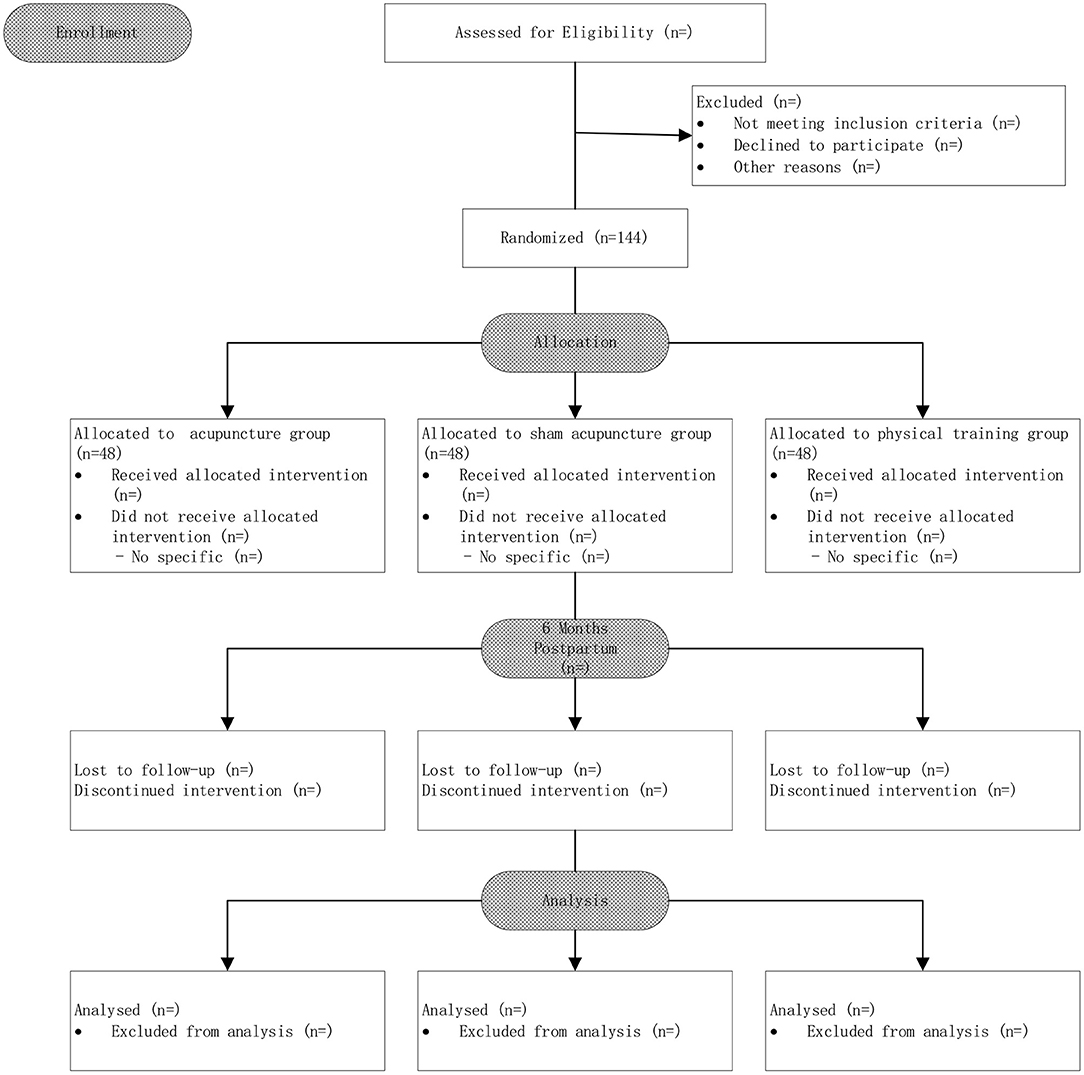
Figure 1. Flow chart of the study design.
Sample Size
According to previous similar reports (13), the average value of IRD in the physical training group was 2.09 after treatment, and the average value of IRD in the acupuncture and physical training group was expected to be 1.43 after treatment in this study. Three groups were set up in this study. The test level was α = 0.05, the test efficiency was 1–β = 0.90, and the two-sided test was conducted. The sample size was estimated by PASS15.0 software (13), effectiveness size is 0.313249. Considering 2-sided P-values to be deemed statistically significant at P < 0 0.05 and a power of 90%, 43 participants would be required per group (nQuery Advisor, version 4.0; Statistical Solutions). Estimating that 10% of patients might be lost to follow-up, we planned to enroll a total of 144 participants, with 48 in each group.
Participants and Recruitment
The study was conducted from March 2022 to March 2023. The acupuncture group received acupuncture and physical training (n = 48), the sham acupuncture group received sham acupuncture and physical training (n = 48), and the physical training group received physical training (n = 48).
Participants were recruited from inclusion criteria:
(1) A female aged 18–45 years with no previous history of pathological rectus abdominal dissection;
(2) Vaginal delivery, 42 days to 1 year post-partum;
(3) DRA diagnostic criteria:
• The patient should keep in the supine position, with knees bending about 90°, the whole body relaxed, and the soles of the feet flat. The examiner shall put the abdomen of one hand finger on the umbilical level of the patient;
• The patient is told to breathe through the abdomen and to lift one's head and shoulders slightly off the bed;
Measuring the width of the finger inserted by the examiner, DRA is diagnosed when IRD ≥ 2 cm (14–16).
(4) No cognitive barriers, able to understand and communicate correctly;
(5) Have not received treatment for DRA in other hospitals or institutions;
(6) Those who sign the informed consent cooperate with the treatment and can adhere to the completion of all treatment as planned.
Patients who meet the above six criteria can be included in this study.
The subjects studied for DRA in post-partum women should follow the following exclusion criteria:
(1) One is suspected or diagnosed with severe spinal lesions (such as spinal fractures, metastases, inflammatory or infectious diseases, cauda equina syndrome/widespread neurological disease) and neurological injury;
(2) One has motor contraindications or severe infectious diseases such as fractures, severe heart disease, hypertension, cancer;
(3) Any plans for surgery soon;
(4) History of cesarean section;
(5) Abdominal operation history;
(6) Any of the above shall be excluded.
Randomization and Binding
A total of 144 eligible patients were recruited and randomly assigned at a 1:1:1 ratio to receive acupuncture treatment or sham acupuncture treatment or be placed on a physical training. Central randomization, using an online or messaging system, was performed by the Brightech Magnsoft Data Services. The randomization sequence was generated in blocks of varying sizes and stratified by centers.
The acupuncture and sham acupuncture groups were blinded, while those in the physical training group were not. All clinical examinations were performed by Haida Zhang and Lujun Deng physiotherapists blinded to data collected through the questionnaire. Due to iodophor disinfection traces in the abdomen after electroacupuncture, the therapists knew the groups, so Yingying Shi performed electroacupuncture treatment after rehabilitation exercise first. All the therapists did not know the purpose of the experiment.
The acupuncture and sham acupuncture groups were blinded, while those in the physical training group were not. All clinical examinations were performed by Haida Zhang and Lujun Deng, two physiotherapists blinded to data collected. Due to iodophor disinfection traces in the abdomen after electroacupuncture, the therapists knew the groups. So Yingying Shi performed electroacupuncture treatment after rehabilitation exercise first. Outcome assessors, data collectors, and statisticians did not know the purpose of the experiment and were blinded to the treatment allocation.
Intervention
1. Acupuncture group: the patient was placed in the supine position, exposing the abdomen, and acupoints RN12 (Zhongwan), RN10 (Xiawan), ST25 (Tianshu), GB26 (Dai Mai), RN6 (Qi Hai), and RN4 (Guanyuan) were selected. The selection of acupoints was based on the previous literature and clinical experience of DRA. The skin at the acupoints was routinely disinfected, and the disposable sterile acupuncture needles were used for vertical acupuncture of 25–40 mm, 30 min once/day, five times a week for 2 weeks (Figure 2A).
2. Sham acupuncture group: non-penetrating sham acupuncture is performed on the same points as the treatment group on the abdomen. Streitberger placebo needles with blunt tips are used. When they are fixed on the skin through plastic rings, patients will feel a pricking sensation, simulating a skin puncture. However, instead of penetrating the skin, the needles retract up into the shaft when pressed against the skin. We will formulate and follow standardize step-by-step instructions and operations to use the same rituals in the acupuncture and sham acupuncture groups as far as possible, 30 min once/day, five times a week for 2 weeks (Figure 2B).
3. Physical training group: (1) Abdominal breathing: supine position, lower limb hip, and knee flexion, foam bricks are clamped between the legs. the abdomen will be humped while inhaling and is forced to the navel while exhaling. Abdominal muscles and pelvic floor muscles are forced to contract at the same time, ten times a group for three groups. (2) Left and right-side leg rotation: buckling, supine, legs down to the right. inhale, abdominal bulge, expiratory when abdomen muscle contraction, to, make double leg down to the left (power is core abdominal muscles, legs, not too much), the therapist skill on the right side of the internal, external oblique muscle in patients with muscle contraction, the muscle belly line direction, the other patients on your knees. Apply some resistance according to the patient's strength of the force. Do it alternately, 10 times on each side. (3) Stretch legs after stomach retraction: Patients prone position, the abdominal pad is a soft pillow, inhale, abdominal bulge, expiratory when abdomen muscle contraction (imagine navel carried from pillow side), in turn, the waist, on the left side of the hips, on the left side of the thigh, to raise the left lower limb, the core in the waist, leg without over pressure, and avoid the contralateral compensatory, therapists place the fourth finger near the lumbar spine feeling the relaxation from torn muscle contraction. Alternating left and right, do 10 reps on each side. (4) Ventral flat training: the patient is in the right described position, elbow flexion support on the bed surface, hip extension, calf flexion and thigh 90 degrees, abdominal uplift when inhaling, abdominal muscles when exhaling, upper body, buttocks and left lower limb straight lift off the bed surface, left upper limb lift, upper arm against the head, ear sticking, maintain relaxation after 10 s. Core in the abdomen, other parts of the body cannot apply excessive force. Alternating left and right, do 10 reps on each side (Figure 3).
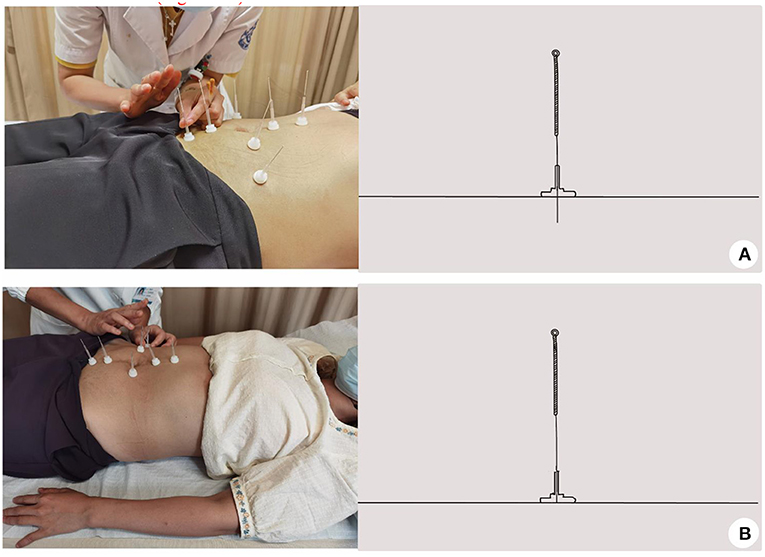
Figure 2. The schematic diagram of acupuncture and sham acupuncture group. (A) Acupuncture group; (B) Sham acupuncture group.
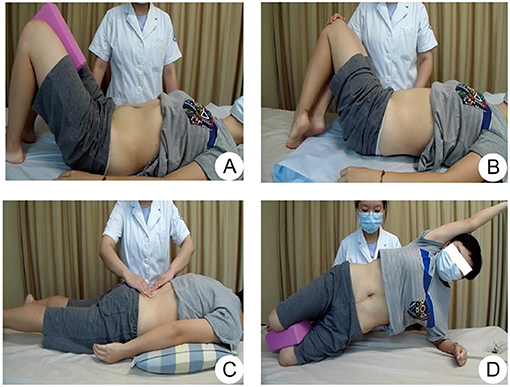
Figure 3. The flow chart of physical training group. (A) Abdominal breathing; (B) Left and right-side leg rotation; (C) Stretch legs after stomach retraction; (D) Ventral flat training.
The trial must end when the following happened: (1) When severe adverse reactions occur on the patient during the trial; (2) When serious complications or deteriorations happen; (3) When the patient is asked to withdraw from the clinical study; (4) When the patient does not cooperate or accept any treatment with the treatment-personnel repeatedly explaining ineffective.
We gather the patients into a WeChat chatting group to answer their questions anytime to prevent the above situations. We try to cooperate and share any knowledge of DRA with our patients to contact them more fluently and smoothly. Furthermore, when the patient gets any other problems, we will have the treatment and record the changes in the patient's condition. During the trial, any other treatment on DRA is not allowed in case of being interfered with. If one happened, the patient must withdraw from the study.
Primary Outcome
We consider the IRD as the primary outcome of DRA treatment (7). The same ultrasonic doctor will measure and evaluate before and after the treatment and after a 6-month follow-up.
Secondary Outcomes
1. LA tension evaluation: IRD, continuous midpoint of umbilical cord and knife-edge, level of the umbilical cord, can be measured by ultrasound. Elastography images can be graded using a modified five-point method (17). The scoring criteria were as follows:1 point indicated that most of the lesions or lesions were green; 2 points are red and green areas with <20%; 3 points means the red area is >20% but <50%; 4 points are areas with or without green that are more than 50% red but <80% or more than 80%. Measurements and assessments were made before and after treatment and after 6 months of follow-up.
2. SF-36: It includes physical function, physical pain, general health status, energy, social function, emotional function, mental health, and indicators of health changes in the past year (18). It can reflect a comprehensive summary of the quality of life of the respondents. The higher the score, the healthier you are. Cronbach's α coefficient was 0.838, and Spearman-Brown coefficient was 0.828, indicating good reliability and validity. Measurement and evaluation will be performed before and after the 6-month follow-up.
3. SF-MPQ-2: This is a systemic pain assessment for patients with low back pain. The following quantitative/semi-quantitative data can be obtained from this scale: (1) PRI: The total score of all selected words. (2) NCW: VAS evaluation in the chart. (3) PPI: 6-degree NRS was used to evaluate the total pain intensity. Cronbach's α coefficient is more significant than 0.8, indicating reasonable confidence and validity. Measurements and assessments were made before treatment and after 6 months of follow-up.
4. BMI: The index is used to assess whether a person is thin or overweight. The ratio of being too small (<18.5 for Asian adults) or too large (≥24 for Asian adults) represents an increased incidence of certain diseases and reflects human health status. Measurements and assessments were made before and after treatment and after six months of follow-up.
5. WHR: It is an essential indicator of central obesity and female attractiveness. Measurements and assessments were made before and after treatment and after 6 months of follow-up.
Other Observation Items
1. LDQ: The questionnaire is a dimensional-symptom-specific scale tool for assessing disease conditions. The Cronbach's α coefficient of the table is 0.908, and the Cronbach's α coefficient of each dimension is 0.448–0.990, indicating good internal consistency and high measurement reliability (19). Measurements and assessments were made before and after treatment and after 6 months of follow-up.
2. MDQ: To assess the status of the menstrual disease. The overall Cronbach's α coefficient was 0.937 (P < 0.001), and the Cronbach's α coefficients of each dimension ranged from 0.652 to 0.862 (20). Measurements and assessments were made before and after treatment and after 6 months of follow-up.
3. EPDS-10: The revised EPDS has a confidence of 0.76, content validity of 0.93, and a recommended critical value of 9.5 points (21). The measurement and evaluation will be taken before and after the treatment and after a 6-month follow-up.
4. MBIS: MBIs have been shown to work via changes in specific aspects of psychopathology, such as cognitive biases, affective dysregulation, and interpersonal effectiveness (22). The measurement and evaluation will be taken before and after the treatment and after a 6-month follow-up.
5. ICIQ-SF: International Association for Urine Control Questionnaire. The Chinese version of Cronbach's α coefficient indicates an internal consistency of 0.72–0.8 (22). After the inspection. Measurements and assessments were made before and after treatment and after 6 months of follow-up.
Adverse Events Reporting and Safety Monitoring
Safety: Adverse events (AE), side effectiveness (SE) such as falls, joint sprains will be recorded during the evaluation.
Compliance: Incomplete information and number of shedding for the two selected cases were recorded during and after the evaluation.
Acupuncture and exercise training were used as intervention items in this study. Before participating in the study, each subject underwent clinical diagnosis and contraindications, and detailed records were made during the treatment process. DURING THE EXPERIMENT, any AE, SE (fall, joint sprain, bleeding, post-stitch, needle blocking, etc.) will be recorded in detail and reported to the project leader. Subjects with adverse events will be treated in the hospital where the project is being implemented, and the project team will bear the treatment and examination costs.
Data Analysis
Based on Preliminary experiment results, we estimated that each of the three clinical researchers involved in the trial would recruit around 28 patients in 3 months. In order to retain most of the patients during follow-up, we gather the patients into a WeChat chatting group to answer their questions anytime. Moreover, actively cooperate with their appointment time. We expect the loss to follow-up to be below 10%.
Baseline characteristics and clinical outcomes are described based on the intention-to-treat population (n = 144). Continuous variables are presented as mean (SD), and categorical variables are described as number and percentage.
The principal analysis for primary and secondary outcomes will be a generalized linear model (GLM) including the intervention arm, the dependent variable's baseline score, and other variables imbalanced at baseline as covariates. The dependent variable will be the post-intervention score. The GLM does not need a normal distribution in the dependent variable. However, the distribution of the variables will be analyzed using de Shapiro- Wilk test to perform an adequate descriptive analysis. The choice of the link function will depend on the distribution of the variable.
Other variables will be added as confounders in the model as secondary sensitivity analyses. We will first fit separate models, including each confounder, one at a time. Those variables whose inclusion in the model changes the estimates' treatment effectiveness by at least 10% will be considered as confounders. As suggested in the CONSORT statement, decisions about confounders will not be based on P-value.
Missing data of withdrawn participants will be accommodated with multiple imputation procedures in Stata 25.0 software (Stata Corporation). All P-values were from 2-sided tests, and results were deemed statistically significant at P < 0.05.
Discussion
There is evidence that physical training can improve DRA (13, 23). To date, however, previous research focuses on how to reduce IRD for DRA treatment (24) but ignores its safety and effectiveness on physiological, psychological, and other systemic regulation. In the process of DRA exercise rehabilitation, individual differences in proprioception of abdominal wall and pelvic floor and cooperative motor control ability should be considered, and patient education and self-perception ability training should be paid attention to. At present, there are no published data on the effectiveness of acupuncture in post-partum with Diastasis Recti Abdominis by A Randomized Controlled Clinical Trial Study.
Increasing adherence to self-care is a challenge in diseases such as DRA. An acupuncture-based intervention to replace single physical training may improve DRA in the future. This study aims to evaluate the effectiveness and safety of acupuncture in post-partum with Diastasis Recti Abdominis to bring the gospel to most DRA patients.
Limitation
First, the extrapolation of the research conclusions of RCT to clinical practice is faced with challenges, e.g. limited sample size. Besides, it is difficult to implement traditional RCT during patient follow-up.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Hangzhou Hospital of TCM. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
YL: data analyses, figure preparation, and manuscript preparation. YZ: questionnaire evaluation and manual data measurement before treatment. LJ: responsible for the design of randomization, project funding, and study initiation. CL: ultrasound evaluation. LX: responsible for the design of randomization. JC, TW, and TY: responsible for data entry. LD and HZ: recovery treatment. YS: acupuncture treatment. TZ, MF, and JW: responsible for guidance and statistics. All authors approved the final version of the manuscript.
Funding
This RCT was funded by Zhejiang Traditional Chinese Medicine Science and Technology Plan Project (Project Number: 2021ZQ065).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We want to thank Dr. Yonggang Huang from the Department of Hernia, and Abdominal Surgery, Hangzhou First People's Hospital, Zhejiang University School of Medicine provided HerQles form of the Chinese version.
Abbreviations
AE, Adverse Event; BMI, Body Mass Index; DRA, Diastasis Recti Abdominis; OR, Odds Ratio; PASS, Power Analysis and Sample Size; IRD, Inter Recti Distance; PRI, Pain Rating Index; NWC, Number of Words Chosen; PPI, Present Pain Intensity; ICC, Intraclass Correlation Coefficients; WHR, Waist-to-Hip Ratio; LDQ, Leeds Dyspepsia Questionnaire; MDQ, Menstrual Distress Questionnaire; MI, Multiple Imputation; PMM, Pattern Mixture Model; SF-36, The MOS Item Short Form Health Survey; LA, Linea Alba; SF-MPQ-2, Short-Form McGill Pain Questionnaire-2; EPDS-10, 10 Items of Edinburgh Post-natal Depression Scale; MBIS, The Modified Body Self-Image Scale; ICIQ-SF, International Consultation Incontinence Questionnaire Short-Form; HerQles, Hernia-Related Quality-of-Life Survey; SE, Side Event; GLM, Generalized linear model.
References
1. Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, Bø K. Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain. Br J Sports Med. (2016) 50:1092–6. doi: 10.1136/bjsports-2016-096065
2. Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. (1988) 68:1082–6. doi: 10.1093/ptj/68.7.1082
3. Fernandes da Mota PG, Pascoal AGBA, Carita AIAD, Bø K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Manual Ther. (2015) 20:200–5. doi: 10.1016/j.math.2014.09.002
4. Gustavsson C, Eriksson-Crommert M. Physiotherapists' and midwives' views of increased inter recti abdominis distance and its management in women after childbirth. BMC Womens Health. (2020) 20:37. doi: 10.1186/s12905-020-00907-9
5. Michalska A, Rokita W, Wolder D, Pogorzelska J, Kaczmarczyk K. Diastasis recti abdominis - a review of treatment methods. Ginekol Pol. (2018) 89:97–101. doi: 10.5603/GP.a2018.0016
6. Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. (2007) 18:321–8. doi: 10.1007/s00192-006-0143-5
7. Thabet AA, Alshehri MA. Efficacy of deep core stability exercise program in postpartum women with diastasis recti abdominis: a randomised controlled trial. J Musculoskelet Neuronal Interact. (2019) 19:62–8.
8. Puentedura EJ, Buckingham SJ, Morton D, Montoya C, Fernandez de Las Penas C. Immediate changes in resting and contracted thickness of transversus abdominis after dry needling of lumbar multifidus in healthy participants: a randomized controlled crossover trial. J Manipul Physiol Ther. (2017) 40:615–23. doi: 10.1016/j.jmpt.2017.06.013
9. Chen F, Zhou J, Wu W, Qian X. Study on the therapeutic effect of floating needle therapy combined with pressing acupoint embedding for female stress urinary incontinence after childbirth: a randomized trial. Ann Palliative Med. (2021) 10:7786–93. doi: 10.21037/apm-21-1382
10. Yao L, Li F, Wang D, Sheng S. Evaluation of acupuncture treatments of postpartum female pelvic floor dysfunction by four-dimensional transperineal pelvic floor ultrasound. Medicine. (2021) 100:e27236. doi: 10.1097/MD.0000000000027236
11. Chan A-W, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, KrleŽa-Jerić K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. (2013) 158:200–7. doi: 10.7326/0003-4819-158-3-201302050-00583
12. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c332. doi: 10.1136/bmj.c332
13. Gluppe S, Ellström Engh M, Kari B. Women with diastasis recti abdominis might have weaker abdominal muscles and more abdominal pain, but no higher prevalence of pelvic floor disorders, low back and pelvic girdle pain than women without diastasis recti abdominis. Physiotherapy (2021) 111:57–65. doi: 10.1016/j.physio.2021.01.008
14. Kaufmann RL, Reiner CS, Dietz UA, Clavien PA, Vonlanthen R, K4ser SA. Normal width of the linea alba, prevalence, and risk factors for diastasis recti abdominis in adults, a cross-sectional study. Hernia (2021) doi: 10.1007/s10029-021-02493-7 [Epub ahead of print].
15. Manetti G, Lolli MG, Belloni E, Nigri G. A new minimally invasive technique for the repair of diastasis recti: a pilot study. Surg Endosc. (2021) 35:4028–34. doi: 10.1007/s00464-021-08393-2
16. Qu E, Wu J, Zhang M, Wu L, Zhang T, Xu J, et al. The ultrasound diagnostic criteria for diastasis recti and its correlation with pelvic floor dysfunction in early postpartum women. Quant Imaging Med Surg. (2021) 11:706–13. doi: 10.21037/qims-20-596
17. Itoh A, Ueno E, Tohno E, Kamma H, Takahashi H, Shiina T, et al. Breast disease: clinical application of US elastography for diagnosis. Radiology. (2006) 239:341–50. doi: 10.1148/radiol.2391041676
18. Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. (1992) 305:160–4. doi: 10.1136/bmj.305.6846.160
19. Kelly JF, Magill M, Slaymaker V, Kahler C. Psychometric validation of the Leeds Dependence Questionnaire (LDQ) in a young adult clinical sample. Addict Behav. (2010) 35:331–6. doi: 10.1016/j.addbeh.2009.11.005
20. Clark CT, Sit DKY, Driscoll K, Eng HF, Confer AL, Luther JF, et al. Does screening with the MDQ and EPDS improve identification of bipolar disorder in an obstetrical sample? Depress Anxiety. (2015) 32:518–26. doi: 10.1002/da.22373
21. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
22. O'Reilly GA, Cook L, Spruijt-Metz D, Black DS. Mindfulness-based interventions for obesity-related eating behaviours: a literature review. Obesity Rev. (2014) 15:453–61. doi: 10.1111/obr.12156
23. Benjamin DR, van de Water AT, Peiris CL. Effects of exercise on diastasis of the rectus abdominis muscle in the antenatal and postnatal periods: a systematic review. Physiotherapy (2014) 100:1–8. doi: 10.1016/j.physio.2013.08.005
Keywords: acupuncture, diastasis recti abdominis, post-partum, intrabdominis stimulation, randomized controlled trial
Citation: Liu Y, Zhu Y, Jiang L, Lu C, Xiao L, Chen J, Wang T, Deng L, Zhang H, Shi Y, Zheng T, Feng M, Ye T and Wang J (2021) Efficacy of Acupuncture in Post-partum With Diastasis Recti Abdominis: A Randomized Controlled Clinical Trial Study Protocol. Front. Public Health 9:722572. doi: 10.3389/fpubh.2021.722572
Received: 10 June 2021; Accepted: 22 November 2021;
Published: 13 December 2021.
Edited by:
Yi-Hung Chen, China Medical University, TaiwanReviewed by:
Chien-Chen Huang, Medical University, TaiwanChung-Hung Wu, Taichung Tzu Chi Hospital, Taiwan
Copyright © 2021 Liu, Zhu, Jiang, Lu, Xiao, Chen, Wang, Deng, Zhang, Shi, Zheng, Feng, Ye and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liyuan Jiang, amlhbmdsaXl1YW41MjBqQDE2My5jb20=