 Guillermo F. López Sánchez
Guillermo F. López Sánchez Lee Smith
Lee Smith Louis Jacob
Louis Jacob Jae Il Shin
Jae Il Shin Ai Koyanagi
Ai Koyanagi Shahina Pardhan
Shahina Pardhan- 1Faculty of Health, Education, Medicine and Social Care, School of Medicine, Vision and Eye Research Institute, Anglia Ruskin University, Cambridge, United Kingdom
- 2The Cambridge Centre for Sport and Exercise Sciences, Anglia Ruskin University, Cambridge, United Kingdom
- 3Research and Development Unit, Parc Sanitari Sant Joan de Déu, Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Sant Boi de Llobregat, Barcelona, Spain
- 4Faculty of Medicine, University of Versailles Saint-Quentin-en-Yvelines, Montigny-le-Bretonneux, France
- 5Department of Pediatrics, Yonsei University College of Medicine, Seoul, South Korea
- 6Institució Catalana de Recerca i Estudis Avançats (ICREA), Barcelona, Spain
Objective: This study aimed to explore gender differences in the associations between cataracts and self-reported depression and chronic anxiety in Spanish adults with diabetes.
Methods: Cross-sectional data from the Spanish Health Survey 2017 were analyzed. Inclusion criterion was a positive response to the question “Have you ever been diagnosed with diabetes?” Diabetes, cataracts, depression and chronic anxiety were based on self-reported lifetime diagnosis. Multivariable logistic regression was conducted to assess the association between cataracts and depression or anxiety among respondents with diabetes, stratifying by gender.
Results: Out of a total 23,089 respondents, 2,266 people self-reported suffering from diabetes (50.2% women; average age 69.7 ± 12.7 years; age range 15-98 years). In people with diabetes, the presence of cataracts was associated with significantly higher odds for depression (OR = 1.655; 95% CI = 1.295-2.115). Gender-stratified analyses showed that only women with cataracts were significantly associated with higher odds for depression (OR = 1.762; 95% CI = 1.307-2.374) and chronic anxiety (OR = 1.519; 95% CI = 1.067-2.163).
Conclusion: Cataracts are a significant risk factor for depression and chronic anxiety in Spanish women with diabetes, but not in men. Women with both diabetes and cataracts require assessment for depression and chronic anxiety, and possibly earlier interventions in order to reduce the potential risk of further mental health complications.
Introduction
Globally ~422 million people live with diabetes and prevalence of the condition has been increasing steadily over recent decades (1). In Europe, there are approximately 60 million people with the condition, about 10.3% of men and 9.6% of women aged 25 years and over (2). In Spain, the incidence of diabetes, adjusted for age and gender has been reported to be 11.6 cases/1,000 person-years (95%CI = 11.1-12.1) (3).
Diabetes is associated with multiple health complications. One complication is visual impairment with cataract being a key cause (4). Indeed, people with diabetes are up to five times more likely to develop cataracts compared to those without diabetes (5, 6). Both visual impairment and diabetes separately have been linked to higher levels of depression and anxiety than in the general population. For example, one meta-analysis of seven studies concluded that diabetes is associated with an increased risk of depression (7), and another showed significant positive associations with anxiety disorders (1.20; 95% CI = 1.10-1.31) and elevated anxiety symptoms (1.48; 95%CI = 1.02-1.93), with a pooled OR for all anxiety studies (1.25; 95% CI = 1.10-1.39) (8). Furthermore, another systematic review (9) and a 16-year nationwide population-based longitudinal study (10) suggested that a strong link exists between cataracts and depression. Higher levels of anxiety in people with cataracts have also been suggested (11).
Bener et al. reported that significantly more women with diabetes had depression (63.3 vs. 50.4%) and anxiety (70.1 vs. 61.6%) compared to men (12). With regards to the prevalence of depression in people with cataracts by gender, Liu et al. (13) found that there was a similar prevalence of depression in women (24.2%) and men (23.6%).
Given that diabetes and cataracts are both associated with higher risk for mental health problems, it is possible that people with co-existing diabetes and cataracts would have higher risk of depression and anxiety. In addition, although gender differences have been previously found in prevalence studies for depression and anxiety, it is not known whether gender differences exist in mental health in people who have both diabetes and cataract. Therefore, in accordance with the international recommendations about gender in public health research (14, 15), the aim of the present study was to explore gender differences in the associations between cataracts and self-reported depression and chronic anxiety in Spanish adults with diabetes.
Methods
The Survey
Data from the Spanish National Health Survey 2017 (n = 23,089 adults) were analyzed. This survey was carried out in Spain between October 2016 and October 2017. Details of the survey methods have been published elsewhere (16). A stratified three-stage sampling technique was used to collect the data, considering first census sections, second family dwellings, and third an adult (15 years or more) in each dwelling. The selection of each section within each stratum was carried out with probability proportional to their size. In each section, the dwellings were selected by systematic sampling with equal probability, prior arrangement by dwelling size. This method produces self-weighting samples in each stratum. The random Kish method was used to select the people who had to complete the Adult Questionnaire, assigning equal probability to all the adults of the household. The inclusion criterion to participate in this study was a positive response the question “Have you ever been diagnosed with diabetes?” Therefore, the sample of the present study included the 2,266 people with diabetes of the survey (9.8% of the total survey sample), being representative of the adult population with diabetes residing in Spain. Also, this prevalence of 9.8% is in line with previous studies in Spain, which reported prevalence's from 4.8 to 18.7% (17).
Procedure
The method of data collection used was computer-assisted personal interviewing (CAPI), conducted in the homes of the selected participants. The interviewers, previously trained, completed the questionnaires with the information provided by the participants. The interviews were carried out in the selected dwellings. The personnel in charge of conducting the interviews were assigned a periodic work quota distributed according to the sample design. The interviewer had to make at least 6 visits on three different days to the dwelling, until contacting the home or giving the corresponding incidence. The field work (data collection, inspection, monitoring and first data cleaning) was carried out, under the close supervision of the Spanish Statistical Office, by the company awarded the contract.
All participants signed an informed consent form before responding to the survey questions. This research was conducted in accordance with the Declaration of Helsinki of the World Medical Association and with the regulation of European Union. The file data for public use does not require the approval of an accredited ethics committee for statistical or research purposes.
Depression and Chronic Anxiety
Depression and chronic anxiety were assessed with the following yes–no questions: (1) “Have you ever been diagnosed with depression?”; (2) “Have you ever been diagnosed with chronic anxiety?”. It was considered that the participants that responded yes to the questions had suffered from depression/chronic anxiety. The question for depression has been previously validated (18), and the question for anxiety has been widely used in previous scientific literature (19–23).
Diabetes and Cataracts
Diabetes and cataracts were assessed with the following yes–no questions: (1) “Have you ever been diagnosed with diabetes?”; (2) “Have you ever been diagnosed with cataracts?”. It was considered that the participants that responded yes to the questions had suffered from diabetes/cataracts. Self-reported diabetes is a valid and reliable measure (24–32). Self-report accuracy is also high for cataract (33). Self-report questionnaires are widely used in large population studies where it is difficult to collect clinical data, and the questions used in this study to assess diabetes and cataracts have been already used in various nation-wide studies (20–23, 34).
Covariates
The selection of the control variables was based on bivariate analyses (Table 1) and on past literature (34–37). Sociodemographic variables included gender, age, marital status, living as a couple and education. Education was based on the highest educational level achieved and was categorized as ≤ primary, secondary, and ≥tertiary. Marital status was categorized as married and single/widowed/divorced/separated. Living as a couple was categorized as yes/no. Smoking status was self-reported and categorized as never, current smoker, and past smoker. Alcohol consumption in the last 12 months was self-reported and categorized as yes (any) and no (none). Height and weight were self-reported. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Obesity was defined as BMI ≥ 30 kg/m2, according to World Health Organization (https://www.who.int/health-topics/obesity).
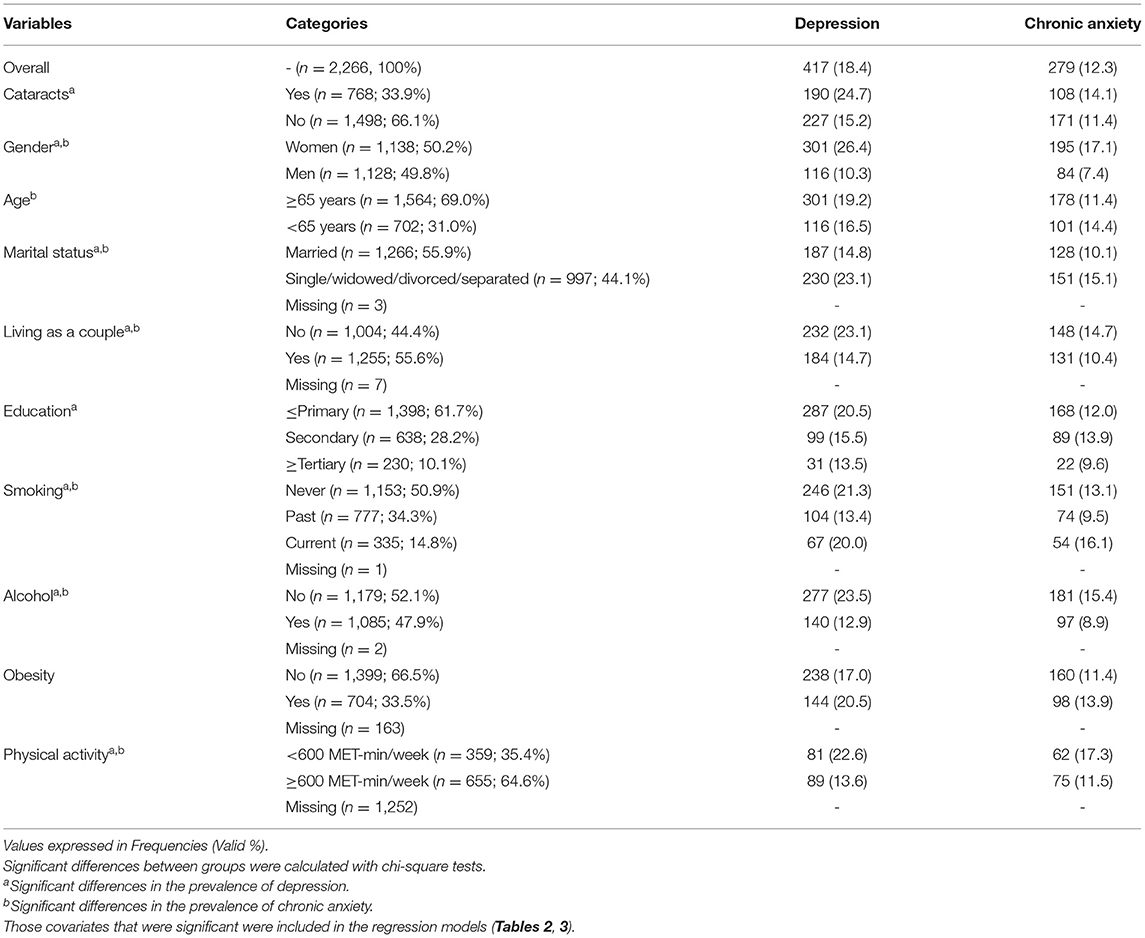
Table 1. Prevalence of depression and chronic anxiety in Spanish adults with diabetes (overall, by cataracts status and by covariates).
The International Physical Activity Questionnaire (IPAQ) short form was used to measure physical activity. The unit of physical activity used was MET-minutes/week, where MET is the Metabolic Equivalent of Task. Total physical activity MET-minutes/week were calculated through the following formula: sum of Walking + Moderate + Vigorous MET-minutes/week scores (38). Participants were divided in two categories according to the guidelines for data processing and analysis of the IPAQ (38) and according to the American Diabetes Association PA guidelines (39): (1) fewer than 600 MET-min/week and (2) at least 600 MET-min/week, equivalent to meeting current PA recommendations. IPAQ was developed for population surveillance of physical activity among adults aged 15–69 years, and its use with older and younger age groups is not recommended (38). Therefore, IPAQ was completed only by people aged 15-69 years and, to avoid losing all the data of people ≥ 70 years, a missing category for physical activity was included in the regression analyses. IPAQ has been validated in adult populations from different countries showing acceptable validity (ρ = 0.30, 95% CI: 0.23-0.36) and reliability (Spearman's ρ = 0.81, 95% CI: 0.79-0.82) (40). Specifically, IPAQ Short Form has been validated among Spanish university students showing adequate validity (41).
Statistical Analysis
The statistical analysis was performed with SPSS 23.0 (IBM, NY, USA). The prevalence of self -reported depression and chronic anxiety in Spanish adults with diabetes was studied, analyzing the differences by cataracts status and by covariates (Table 1). These differences were assessed by Chi-squared tests and those covariates that were significant were included in the regression models (Tables 2, 3).
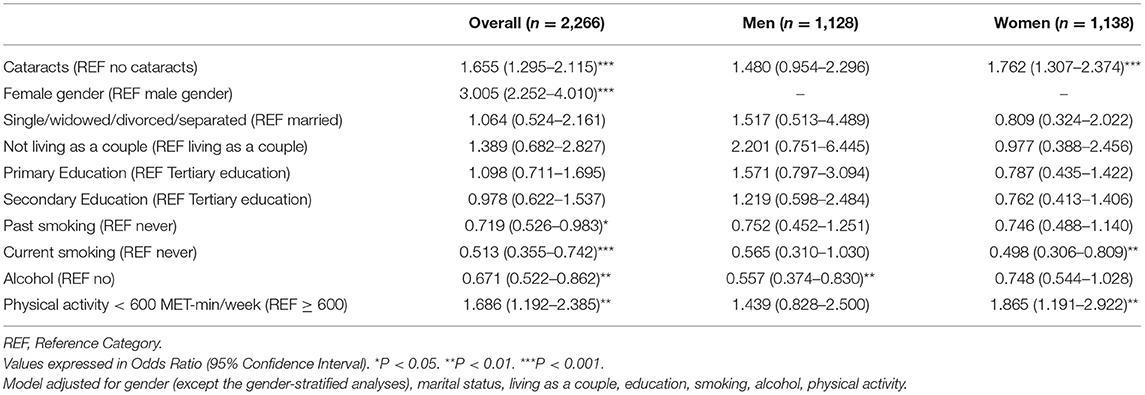
Table 2. Associations between cataracts (exposure) and covariates with depression (outcome) in Spanish adults with diabetes, estimated by multivariable logistic regression (overall and by gender).
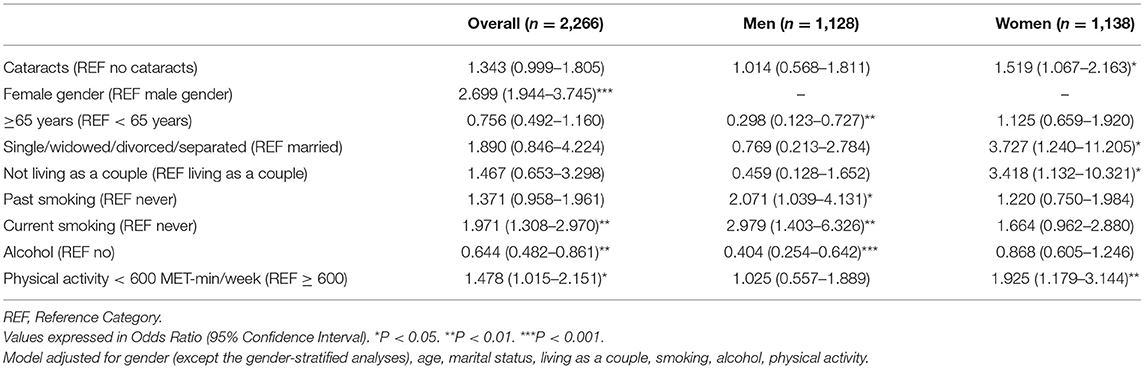
Table 3. Associations between cataracts (exposure) and covariates with chronic anxiety (outcome) in Spanish adults with diabetes, estimated by multivariable logistic regression (overall and by gender).
Multivariable logistic regression examined association between cataracts (exposure) and depression or anxiety (mental health outcome) in men and women. Goodness-of-fit and diagnostic tests were conducted in order to check the suitability of the regression model. The model for depression was adjusted for gender (except the gender-stratified analyses), marital status, living as a couple, education, smoking, alcohol, physical activity. The model for chronic anxiety was adjusted for gender (except the gender-stratified analyses), age, marital status, living as a couple, smoking, alcohol, physical activity. All variables were included in the models as categorical variables. Results from the logistic regression analyses are presented as odds ratios (ORs) with 95% confidence intervals (CIs). There were some missing data for the following variables: marital status (n = 3: 0.13%), living as a couple (n = 7: 0.31%), smoking (n = 1: 0.04%), alcohol (n = 2: 0.09%), obesity (n = 163: 7.19%) and physical activity (n = 1,252: 55.25%). The level of statistical significance was set at p <0.05.
Results
In this self-weighting sample of 2,266 adults with diabetes residing in Spain (50.2% women; average age 69.7 ± 12.7 years, males 67.9 ± 11.9 and females 71.4 ± 13.2; age range 15-98 years, males 15-97 and females 26-98), the overall prevalence of depression was 18.4% and the prevalence of chronic anxiety was 12.3 %. The prevalence of depression among those with cataract was significantly higher than in those without cataract (24.7 vs. 15.2%). Bivariate analysis showed that the groups with the following characteristics had the highest levels of depression: women, ≥65 years, people not married, people not living as a couple, ≤ primary education, people who never smoked, non-alcohol drinkers, obesity, <600 MET-min/week of physical activity. For chronic anxiety groups the following characteristics had the highest levels of chronic anxiety: women, <65 years, not married or not living as a couple, secondary education, current smokers, non-alcohol drinkers, obesity, <600 MET-min/week of physical activity (Table 1).
Multivariable logistic regression showed that, overall, the presence of cataract was associated with significantly higher odds for depression (OR = 1.655; 95% CI = 1.295-2.115). In the gender-stratified analyses, cataracts were significantly associated, only in women, with higher odds for depression (OR = 1.762; 95% CI = 1.307-2.374) and for chronic anxiety (OR = 1.519; 95% CI = 1.067-2.163) (Tables 2, 3).
The suitability of the regression models was assessed. The final model for predicting depression was a significant improvement in fit over the null model [χ2(14) = 160.016, p < 0.001], Pearson's chi-square test indicated that the model fitted the data well [χ2(353) = 350.802, p = 0.523] and the deviance chi-square indicated a good fit [χ2(353) = 378.894, p = 0.164]. The model for predicting chronic anxiety showed a significant improvement in fit over the null model [χ2(13) = 99.045, p < 0.001], Pearson's chi-square test indicated that the model fitted the data well [χ2(235) = 235.049, p = 0.487] and the deviance chi-square indicated good fit [χ2(235) = 251.149, p = 0.224].
Discussion
In this large representative sample of Spanish adults with diabetes, we find, for the first time, that women suffering from diabetes and cataracts show significantly higher odds for depression and for chronic anxiety compared to those women who had diabetes but no cataracts.
While the present findings support previous studies showing higher levels of depression and chronic anxiety in people with diabetes (7, 42), it adds to literature by demonstrating that women who have both diabetes and cataract are at much greater risk of mental health complications compared to women with diabetes but no cataract. Also, women who have both diabetes and cataract are at greater risk of mental health complications compared to men with the same conditions, as the association between cataract and mental health was not significant in men with diabetes. The increased risk of depression and chronic anxiety in women with diabetes who have cataracts is of concern as this dual impairment is likely to continue to increase owing to an aging population which leads to both increased prevalence of diabetes and cataracts (43, 44).
There are several plausible mechanisms that may explain the higher risk of depression in people with diabetes who also have cataracts. First, having more than one condition will amplify depression, as multiple conditions require more adjustments for activities of daily living and managing diabetes in the presence of blurred vision (caused by cataracts). Second, managing diabetes and cataracts may need additional medical interventions, and literature suggests that medical intervention is linked to discomfort and uncertainty (45) and is a stressor for depression. Third, if depression is managed through anti-depression medication, this may actually worsen the status-quo as these have been shown to be a risk factor for cataracts (46). Fourth, people with diabetes who also have cataracts experience reduced vision-related changes in quality of life, which might contribute to the development of depression (47).
Possible reasons for cataracts to be significantly associated with higher odds for depression and anxiety in women with diabetes but not in men could be explained by some biological and genetic differences between men and women. Recent evidence suggests that biological factors such variations in ovarian hormone levels and particularly decreases in estrogen may contribute to the increased prevalence of depression and anxiety in women (48). Women with cataracts are more affected than men with regards to the cataract-related medical interventions that may be required (45) and about the vision-related changes in the Quality of Life caused by cataract (47). Previous research suggests that women also have a lower tolerance for stress than men (49). Future studies should explore these reasons in detail.
The large representative sample of the Spanish population and the novel associations investigated are clear strengths of this study. Findings, however, must be interpreted in light of the study limitations. First, the study is cross-sectional in nature thus it is not known whether those with diabetes and anxiety or depression develop cataracts or those with diabetes and cataracts develop anxiety or depression. It is likely bidirectional. A longitudinal study would further explore the identified associations. Second, participants were asked “have you ever been diagnosed with cataracts,” “have you ever been diagnosed with anxiety (or depression),” and “have you ever been diagnosed with diabetes.” It is therefore possible that those participants who reported affirmatively to all questions did not have all conditions at the same time. Also, it is possible that people who responded affirmatively to having cataracts might have had their cataract removed. If that was the case, then we should in fact see higher odds ratios in people who have not had the operation, and it is possible that what we have shown may be underestimate. Also, all questions were self-reported, introducing self-reporting and recall bias into the findings. Finally, there was information about the chronic conditions studied in the present study (diabetes, cataract, depression and chronic anxiety) that were not included in the survey, such as duration of the disease, treatment and type or severity, being recommendable that future studies consider also these aspects.
Conclusions
In conclusion, cataracts are a significant risk factor for depression and chronic anxiety in Spanish women with diabetes, but not in men. It would be important for healthcare practitioners to take this into account, and manage both cataract and diabetes with appropriate and timely interventions to reduce the risk of further mental health complications, especially in women.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Diabetes (2020). Available online at: https://www.who.int/health-topics/diabetes (accessed October 26, 2021).
2. World Health Organization. Diabetes. Data and Statistics (2020). Available online at: https://www.euro.who.int/en/health-topics/noncommunicable-diseases/diabetes/data-and-statistics (accessed October 26, 2021).
3. Rojo-Martínez G, Valdés S, Soriguer F, Vendrell J, Urrutia I, Pérez V, et al. Incidence of diabetes mellitus in Spain as results of the nation-wide cohort di@ bet. es study. Sci Rep. (2020) 10:1-9. doi: 10.1038/s41598-020-59643-7
4. Kiziltoprak H, Tekin K, Inanc M, Goker YS. Cataract in diabetes mellitus. World J Diabetes. (2019) 10:140. doi: 10.4239/wjd.v10.i3.140
5. Klein BE, Klein R, Wang Q, Moss SE. Older-onset diabetes and lens opacities. The Beaver Dam Eye study. Ophthalmic Epidemiol. (1995) 2:49-55. doi: 10.3109/09286589509071451
6. Saxena S, Mitchell P, Rochtchina E. Five-year incidence of cataract in older persons with diabetes and pre-diabetes. Ophthalmic Epidemiol. (2004) 11:271-7. doi: 10.1080/09286580490510733
7. Mezuk B, Eaton WW, Albrecht S, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care. (2008) 31:2383-90. doi: 10.2337/dc08-0985
8. Smith KJ, Béland M, Clyde M, Gariépy G, Pagé V, Badawi G, et al. Association of diabetes with anxiety: a systematic review and meta-analysis. J Psychosom Res. (2013) 74:89-99. doi: 10.1016/j.jpsychores.2012.11.013
9. McCusker S, Koola MM. Association of ophthalmologic disorders and depression in the elderly: a review of the literature. Prim Care Companion CNS Disord. (2015) 17:e1–e3. doi: 10.4088/PCC.14r01731
10. Chen P, Liu PP, Lin S, Wang J, Huang H, Loh C. Cataract and the increased risk of depression in general population: a 16-year nationwide population-based longitudinal study. Sci Rep. (2020) 10:1-8. doi: 10.1038/s41598-020-70285-7
11. Fazzi L, Dobrianskyj FM, Reggi JRA, Otani VHO, Otani TZS, Uchida RR. The influence of anxiety on quality of life among patients with an indication for cataract surgery. São Paulo Med J. (2015) 133:160-1. doi: 10.1590/1516-3180.2014.9510109
12. Bener A, OAA Al-Hamaq A, E Dafeeah E. High prevalence of depression, anxiety and stress symptoms among diabetes mellitus patients. Open Psychiatry J. (2011) 5:5–12. doi: 10.2174/1874354401105010005
13. Liu Z, Chen C, Gao C, Zhou D. Prevalence and correlates of depressive symptoms among Chinese patients with cataracts treated in tertiary general hospitals. PeerJ. (2020) 8:e9397. doi: 10.7717/peerj.9397
14. Phillips SP. Including gender in public health research. Public Health Rep. (2011) 126:16-21. doi: 10.1177/00333549111260S304
15. World Health Organization. Gender and Health (2020). Available online at: https://www.who.int/health-topics/gender (accessed October 26, 2021).
16. Ministerio de Sanidad, Consumo y Bienestar Social & Instituto Nacional de, Estadística,. Spanish National Health Survey 2017: Methodology (2017). Available online at: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_Metodologia.pdf (accessed October 26, 2021).
17. Ruiz-Ramos M, Escolar-Pujolar A, Mayoral-Sánchez E, Corral-San Laureano F, Fernández-Fernández I. Diabetes mellitus in Spain: death rates, prevalence, impact, costs and inequalities. Gaceta sanitaria. (2006) 20:15-24. doi: 10.1157/13086022
18. Sanchez-Villegas A, Schlatter J, Ortuno F, Lahortiga F, Pla J, Benito S, et al. Validity of a self-reported diagnosis of depression among participants in a cohort study using the Structured Clinical Interview for DSM-IV. (SCID-I). BMC Psychiatry. (2008) 8:1-8. doi: 10.1186/1471-244X-8-43
19. Jacob L, López-Sánchez GF, Carvalho AF, Shin JI, Oh H, Yang L, et al. Associations between mental and oral health in Spain: a cross-sectional study of more than 23,000 people aged 15 years and over. J Affect Disord. (2020) 274:67-72. doi: 10.1016/j.jad.2020.05.085
20. Jacob L, López-Sánchez GF, Yang L, Haro JM, Shin JI, Veronese N, et al. Associations between cataract and multimorbidity: a cross-sectional study of 23,089 adults from Spain. Eye. (2020) 2020:1-8. doi: 10.1038/s41433-020-0962-5
21. Jacob L, Sánchez GFL, Oh H, Shin JI, Grabovac I, Soysal P, et al. Multimorbidity is associated with higher levels of urinary incontinence: a cross-sectional study of 23,089 individuals aged≥ 15 years residing in Spain. Br J Gen Pract. (2020) 71:e71-7. doi: 10.3399/bjgp20X713921
22. López-Bueno R, Bláfoss R, Calatayud J, López Sánchez GF, Smith L, Andersen LL, et al. Association Between Physical Activity and Odds of Chronic Conditions Among Workers in Spain. Prev Chronic Dis. (2020) 17:200105. doi: 10.5888/pcd17.200105
23. López-Sánchez GF, López-Bueno R, Gil-Salmerón A, Zauder R, Skalska M, Jastrzebska J, et al. Comparison of physical activity levels in Spanish adults with chronic conditions before and during COVID-19 quarantine. Eur J Public Health. (2020) 31:161-66. doi: 10.1093/eurpub/ckaa159
24. Schneider AL, Pankow JS, Heiss G, Selvin E. Validity and reliability of self-reported diabetes in the atherosclerosis risk in communities study. Am J Epidemiol. (2012) 176:738-43. doi: 10.1093/aje/kws156
25. Yuan X, Liu T, Wu L, Zou Z, Li C. Validity of self-reported diabetes among middle-aged and older Chinese adults: the China Health and Retirement Longitudinal Study. BMJ Open. (2015) 5:e006633. doi: 10.1136/bmjopen-2014-006633
26. Jackson JM, DeFor TA, Crain AL, Kerby T, Strayer L, Lewis CE, et al. Self-reported diabetes is a valid outcome in pragmatic clinical trials and observational studies. J Clin Epidemiol. (2013) 66:349-50. doi: 10.1016/j.jclinepi.2012.01.013
27. Espelt A, Goday A, Franch J, Borrell C. Validity of self-reported diabetes in health interview surveys for measuring social inequalities in the prevalence of diabetes. J Epidemiol Community Health. (2012) 66:e15. doi: 10.1136/jech.2010.112698
28. Fontanelli MdM, Teixeira JA, Sales CH, Castro MAd, Cesar CLG, et al. Alves Maria Cecilia Goi Porto Validation of self-reported diabetes in a representative sample of São Paulo city. Revista de Saúde Pública. (2017) 51:20. doi: 10.1590/s1518-8787.2017051006378
29. Jackson JM, DeFor TA, Crain AL, Kerby TJ, Strayer LS, Lewis CE, et al. Validity of diabetes self-reports in the Women's Health Initiative. Menopause. (2014) 21:861. doi: 10.1097/GME.0000000000000189
30. Goto A, Morita A, Goto M, Sasaki S, Miyachi M, Aiba N, et al. Validity of diabetes self-reports in the Saku diabetes study. J Epidemiol. (2013) 2013:JE20120221. doi: 10.2188/jea.JE20120221
31. Papier K, Jordan S, Bain C, D'este C, Thawornchaisit P, Seubsman SA, et al. Validity of self-reported diabetes in a cohort of Thai adults. Glob J Health Sci. (2016) 9:1–14. doi: 10.5539/gjhs.v9n7p1
32. Huerta JM, Tormo MJ, Egea-Caparrós JM, Ortolá-Devesa JB, Navarro C. Accuracy of self-reported diabetes, hypertension, and hyperlipidemia in the adult Spanish population. DINO study findings. Revista Española de Cardiología. (2009) 62:143-52. doi: 10.1016/S1885-5857(09)71532-4
33. Bergmann MM, Byers T, Freedman DS, Mokdad A. Validity of self-reported diagnoses leading to hospitalization: a comparison of self-reports with hospital records in a prospective study of American adults. Am J Epidemiol. (1998) 147:969-77. doi: 10.1093/oxfordjournals.aje.a009387
34. López-Sánchez GF, Sánchez-Castillo S, López-Bueno R, Pardhan S, Zauder R, Skalska M, et al. Comparison of physical activity levels in Spanish people with diabetes with and without cataracts. Eur J Public Health. (2020) 30:1201-5. doi: 10.1093/eurpub/ckaa104
35. Bonnet F, Irving K, Terra J, Nony P, Berthezène F, Moulin P. Anxiety and depression are associated with unhealthy lifestyle in patients at risk of cardiovascular disease. Atherosclerosis. (2005) 178:339-44. doi: 10.1016/j.atherosclerosis.2004.08.035
36. González-Carcelén CM, López JN, Sánchez GFL. Levels of physical activity in people with diabetes residing in Spain. Atena J Public Health. (2020) 2:2.
37. Ojofeitimi EO, Adelekan DA, Adeoye A, Ogungbe TG, Imoru AO, Oduah EC. Dietary and lifestyle patterns in the aetiology of cataracts in Nigerian patients. Nutr Health. (1999) 13:61-8. doi: 10.1177/026010609901300202
38. IPAQ group,. Guidelines for Data Processing Analysis of the International Physical Activity Questionnaire (IPAQ) (2005). Available online at: https://sites.google.com/site/theipaq/scoring-protocol (accessed October 26, 2021).
39. Colberg SR, Sigal RJ, Yardley JE, Riddell MC, Dunstan DW, Dempsey PC, et al. Physical activity/exercise and diabetes: a position statement of the American Diabetes Association. Diabetes Care. (2016) 39:2065-79. doi: 10.2337/dc16-1728
40. Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exer. (2003) 35:1381-95. doi: 10.1249/01.MSS.0000078924.61453.FB
41. Rodriguez-Munoz S, Corella C, Abarca-Sos A, Zaragoza J. Validation of three short physical activity questionnaires with accelerometers among university students in Spain. J Sports Med Phys Fitness. (2017) 57:1660. doi: 10.23736/S0022-4707.17.06665-8
42. Engum A. The role of depression and anxiety in onset of diabetes in a large population-based study. J Psychosom Res. (2007) 62:31-8. doi: 10.1016/j.jpsychores.2006.07.009
43. Prokofyeva E, Wegener A, Zrenner E. Cataract prevalence and prevention in Europe: a literature review. Acta Ophthalmol. (2013) 91:395-405. doi: 10.1111/j.1755-3768.2012.02444.x
44. United Nations,. Ageing (2020). Available online at: https://www.un.org/en/sections/issues-depth/ageing/ (accessed October 26, 2021).
45. Price B. Managing patients' anxiety about planned medical interventions. Nurs Standard 2014. (2017) 31:53. doi: 10.7748/ns.2017.e10544
46. Andrade C. Antidepressants, mood stabilizers, antipsychotics, and the risk of cataract. J Clin Psychiatry. (2019) 80:19f12744. doi: 10.4088/JCP.19f12744
47. McGrath D. Depression Cataract. EuroTimes (2017). Available online at: https://www.eurotimes.org/depression-cataract/ (accessed October 26, 2021).
48. Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci. (2015) 40:219. doi: 10.1503/jpn.150205
Keywords: cataracts, chronic anxiety, depression, diabetes, gender
Citation: López Sánchez GF, Smith L, Jacob L, Shin JI, Koyanagi A and Pardhan S (2021) Gender Differences in the Association Between Cataract and Mental Health in Adults With Diabetes: A Cross-Sectional Analysis From the Spanish National Health Survey 2017. Front. Public Health 9:769155. doi: 10.3389/fpubh.2021.769155
Received: 01 September 2021; Accepted: 16 November 2021;
Published: 07 December 2021.
Edited by:
Reza Mohammadpourhodki, Mashhad University of Medical Sciences, IranReviewed by:
Morteza Shamsizadeh, Hamadan University of Medical Sciences, IranRehab Ismail, County Durham and Darlington NHS Foundation Trust, United Kingdom
Ariesanti Tri Handayani, Udayana University, Indonesia
Copyright © 2021 López Sánchez, Smith, Jacob, Shin, Koyanagi and Pardhan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guillermo F. López Sánchez, Z3VpbGxlcm1vLmxvcGV6LXNhbmNoZXpAYXJ1LmFjLnVr; Lee Smith, bGVlLnNtaXRoQGFydS5hYy51aw==; Shahina Pardhan, c2hhaGluYS5wYXJkaGFuQGFydS5hYy51aw==