 Špela Bogataj
Špela Bogataj Katja Kurnik Mesarič1
Katja Kurnik Mesarič1 Tanja Petrušič
Tanja Petrušič Jernej Pajek
Jernej Pajek- 1Department of Nephrology, University Medical Centre Ljubljanag, Ljubljana, Slovenia
- 2Faculty of Sport, University of Ljubljana, Ljubljana, Slovenia
- 3Faculty of Education, University of Ljubljana, Ljubljana, Slovenia
Introduction: Patients with chronic kidney disease treated with hemodialysis (HD) have lower cognitive abilities compared to the age-matched healthy population. Recently, physical exercise and cognitive training have been presented as possible interventions to improve cognitive abilities both in the general population and in patients with chronic diseases. To date, there is no general overview of the current knowledge on how these interventions affect cognitive abilities in HD patients and what tests are used to measure these effects.
Methods: Three electronic databases were searched for randomized controlled studies of physical exercise or cognitive training interventions that examined effects on cognitive abilities/performance in HD patients.
Results: Six articles were included. All included studies used physical exercise as an intervention, with one study also including tablet-based cognitive training. Four studies included an intradialytic approach and two included a home-based intervention. Intervention lasted. A significant intervention effect was observed in three studies compared with the control condition.
Conclusion: The present review suggests that physical exercise might improve or at least not worsen cognitive performance in HD patients, whereas the effect of cognitive training has not yet been adequately studied. There is a need for more sensitive and specific cognitive tests to adequately measure the effects of interventions in the HD population.
Introduction
It is well-documented that cognitive deficits cause progression toward dementia (1, 2). This phenomenon is even more pronounced in clinical populations (3). An example of a vulnerable population with an increased incidence of cognitive impairment is patients with kidney disease treated with hemodialysis (HD). The cognitive decline in HD patients is not only the result of underlying and concomitant diseases but can also be attributed to their changed lifestyle after starting HD. These patients have to travel to a dialysis center every other day, where they spend 4–5 h in a sedentary position during a HD procedure. Many reports a post-dialysis burnout and fatigue lasting for up to 24 h post-dialysis (4). As a result, these patients are less physically active and activate their mental functions to a lesser extent. Moreover, in HD patients, diabetes, a common chronic kidney disease (CKD) comorbidity, was significantly associated with larger cognitive impairment (5). HD treatment itself also contributes to a higher risk of developing dementia by causing ischemic stunning of the brain (6). In addition, dementia risk factors such as obesity, depression, and social isolation are common in the HD population.
It was found that only 13% of HD patients have a normal cognitive function (7). Moreover, clinicians usually fail to recognize declining cognitive performance in these patients; therefore, cognitive impairment is critically underestimated and not appropriately treated (8). It has been reported that <5% of all patients with kidney disease with cognitive impairment have been evaluated or received a medical diagnosis (9). Measurement of cognitive function is not currently part of the physical examination and medical history of CKD patients.
Lately, non-pharmacological interventions have been introduced as possible approaches to mitigate cognitive decline and dementia (3). Studies that examined the effect of exercise interventions on cognitive performance showed conflicting results. A systematic review of exercise intervention studies on cognition in older adults did not provide sufficient evidence that exercise affects cognitive performance (10). Another systematic review concluded that physical activity could delay the progression of cognitive decline in the elderly (11). In a recent study, the authors reported the results of a 6-month aerobic exercise intervention in older adults (>60 years) on cognitive function. Compared to control subjects, participants in the training group showed broad improvement in cognitive abilities, including processing speed, episodic memory, executive functions, and updating (12).
In addition to physical activity, cognitive training programs to improve general and specific cognitive domains are being increasingly used in research on cognitive decline. A meta-analysis of 17 controlled interventional trials of computer-assisted cognitive training in subjects with mild cognitive impairment showed a moderate effect on general cognition (13). In community-dwelling older adults, the ACTIVE trial demonstrated long-term retention of a benefit of 10–14 weeks' cognitive training with significant improvement in cognitive abilities and maintenance of functional status after a 10-year period (14).
Despite the fact that there is a plethora of research on physical and cognitive interventions, most of the focus has been on the general population. There is little research addressing the clinical population. In addition, there is no systematic review of the effect of physical exercise and cognitive training that focuses on patients with CKD undergoing HD. Therefore, the aim of this systematic review was to examine the effects of non-pharmacological interventions in the form of cognitive and physical exercise training on different domains of cognitive performance.
Materials and methods
The review methods and reporting were performed according to the preferred reporting items in systematic review and meta-analyses (PRISMA) guidelines (15).
Eligibility criteria
The PICOS search tool (participant, intervention, comparison, outcome, and study design) was used to determine keywords (Table 1).
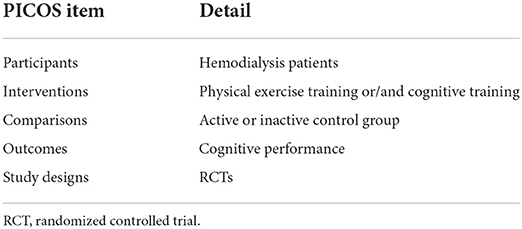
Table 1. “PICOS” items (participants, intervention, comparisons, outcomes, study designs) used to select keywords.
Studies were included in the systematic review if they met the following criteria: (a) randomized controlled trials, (b) published in academic journals, (c) written in English, (d) with participants on hemodialysis and (e) studies that included physical exercise or cognitive training interventions with (f) outcome of cognitive performance. Studies were excluded if study population were CKD patients without kidney replacement therapy or patients on peritoneal dialysis, animal studies, and individual case studies.
Search strategy
To identify potentially relevant studies, we performed a comprehensive literature search in electronic databases including PsycInfo, PubMed and MEDLINE (Ovid) from the database's inception to the final update in August 2022. Medical subject heading (mesh) terms were used, if available, for a qualitative search of potential studies. Search strategies utilized a combination of key words to represent definitions of hemodialysis, cognitive functioning, physical activity interventions and cognitive training. Terms were combined using the “AND” and “OR” Boolean operator (for the full list of search phrases and terms, see Table 2). To increase the likeliness of including all relevant trials, a backward and forward search were performed by screening the citations and references list of the included studies. A flow diagram of the search is presented in Figure 1.

Table 2. Search strategy.
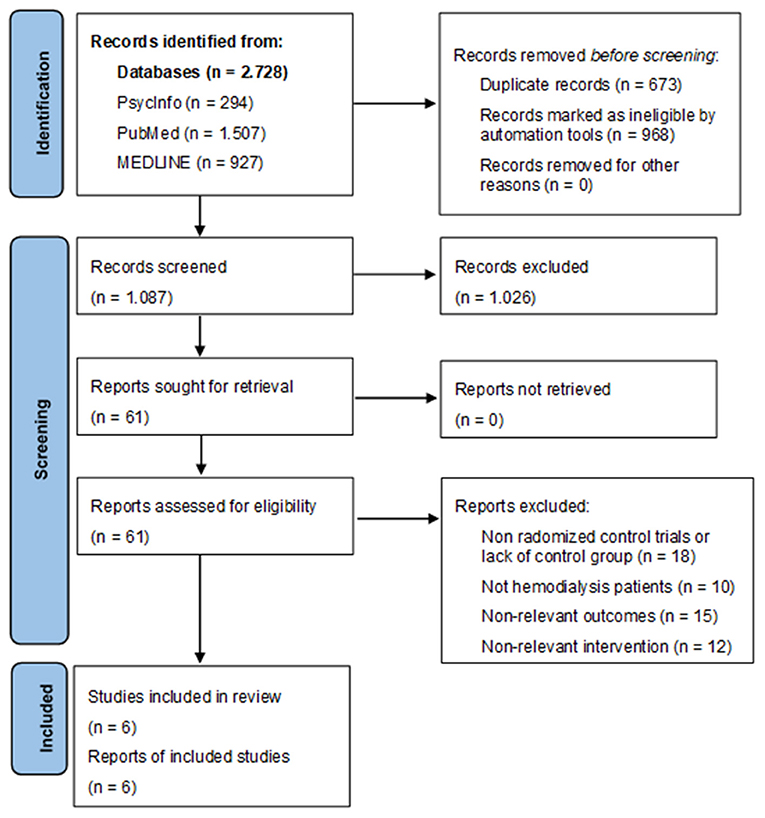
Figure 1. PRISMA flow diagram.
Study selection and data collection procedure
Articles from the above databases were checked for duplicates using EndNote X9. Subsequently, all articles were screened using the Rayyan app (16). In the app, two reviewers (ŠB and KKM) independently reviewed the titles and abstracts of each article in a blinded manner. The decision to include an article was made at the research team meeting. Articles that met the inclusion criteria underwent quality assessment.
Risk of bias assessment
The quality of the included studies was evaluated using the revised Cochrane Collaboration's risk of bias tool (17). The following biases were evaluated: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, bias in selection of the reported result and overall bias. Risk of bias was assessed as low, some concerns or high for each domain and for overall bias.
Results
Study selection
The flow of studies through the review process is reported in Figure 1. Automation tools used in databases were language (English), type of publication (Academic journals) and if possible study type (randomized controlled trial). Duplicate records were removed once the search strategy outputs were combined. Titles and abstracts were screened to identify studies that administered physical activity interventions or cognitive training/interventions to promote cognitive functioning. Full-texts of these articles were read to see whether full inclusion criteria were met. All studies that met inclusion criteria were again screened to determined eligibility for the systematic literature review.
Quality assessment
The bias risks are presented using a risk of bias summary in Figure 2. In the aspects of measurement of outcome, two of the studies were assessed as high risk (18, 19), in the aspects of randomization process three of six included studies were assessed with some concerns (18–20). Three of all included studies were assessed as low risk on all domains and overall (21–23).
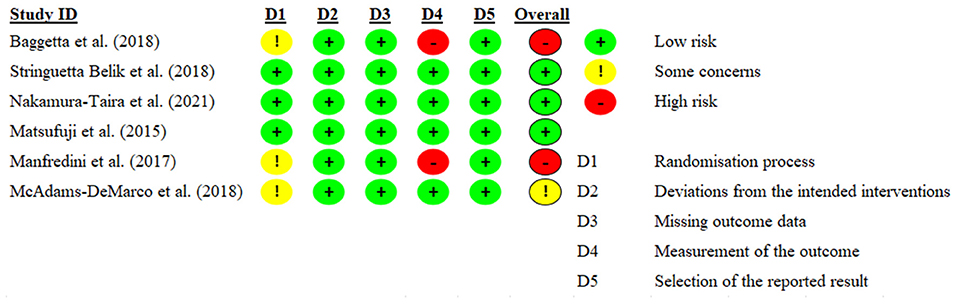
Figure 2. Risk of bias summary.
Study characteristics
The six included studies were published between 2015 and 2021. They included a total of 466 HD patients. Two hundred fourteen patients received a physical exercise intervention and seven patients received a cognitive training intervention. The control group, which received standard treatment or stretching exercises, consisted of 245 HD patients. The average age of participants in the included studies ranged from 48 to 75 years. The youngest patients were in the exercise group of the study by McAdams-DeMarco et al. (20), and the oldest were in the control group of the study by Baggetta et al. (18). Two studies did not report the frequency of exercise. The remaining physical activity studies reported that exercise was performed three times per week. The duration of the intervention ranged from 12 to 24 weeks. The characteristics of the included studies are shown in Table 3.
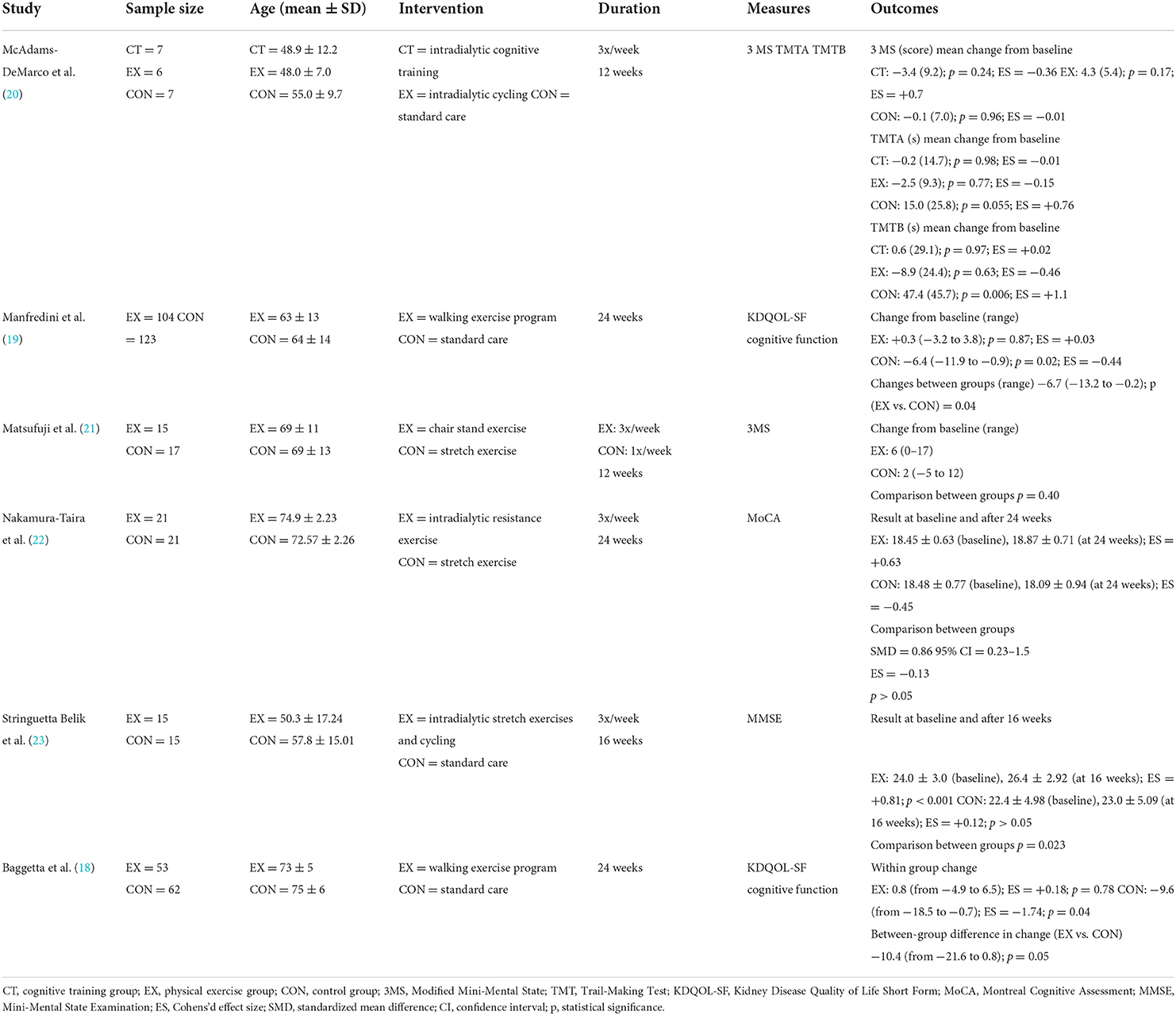
Table 3. Characteristics of included studies.
Two included studies examined the effect of a 6-month home-based walking program on self-reported cognitive function as measured by KDQOL-SF (18, 19). In one study, there was a significant increase in cognitive function (19) and in the other study the control group experienced a decline while an experimental group preserved self-reported cognitive function in older dialysis patients (>65 years) (18). An intradialytic exercise program in the form of stretching exercises and cycling significantly improved cognitive performance as measured by the MMSE in the experimental group compared to the standard care control group (23). Contraindicatory, intradialytic resistance exercise (22) and chair stand exercise program (21) showed no significant effect on cognitive ability as measured by MoCA and 3MS. Only one included pilot study examined the effects of cognitive training (20) with 20 HD patients randomly assigned to a cognitive training group (brain games on tablet computers, n = 7), an intradialytic cycling group (n = 6), or to standard treatment group (n = 7). The intervention lasted 3 months and showed a decline in executive functions and psychomotor speed in the control group, whereas the decline was not observed in either the cycling or cognitive training groups.
Regarding the duration of the intervention, in two studies (20, 21), the 12-week intervention did not result in significant improvement in selected cognitive domains. In the remaining studies, the intervention was delivered for 16 weeks or longer and showed either significant improvement (19, 23) or maintenance of cognitive performance compared to the control group (18, 22).
Cognitive performance/ability was assessed using various validated cognitive tests/questionnaires: Modified Mini-Mental State (3MS), Trail-Making Test A and B (TMTA and TMTB), Kidney Disease Quality of Life Short Form (KDQOL-SF), Montreal Cognitive Assessment (MoCA), and Mini-Mental State Examination (MMSE). Brief description of used tests and questionnaires is offered in Table 4.
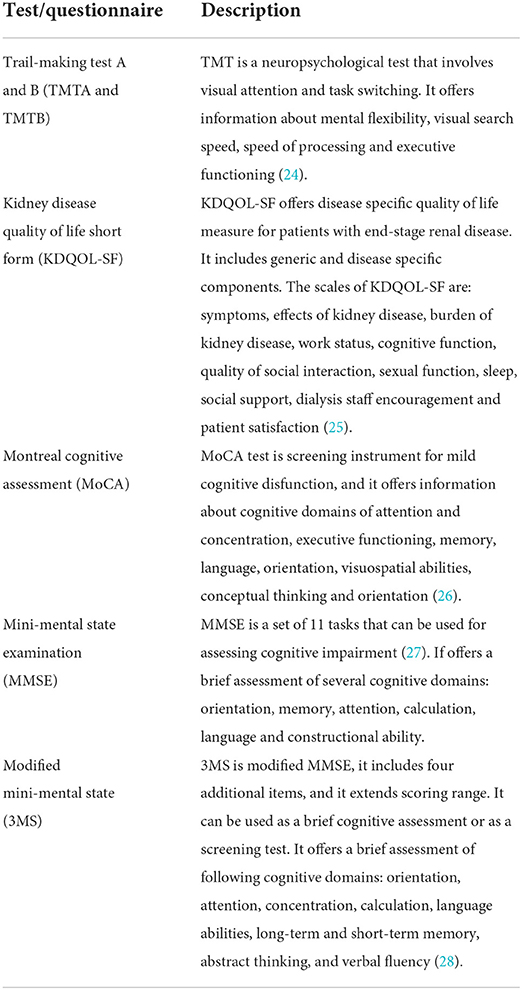
Table 4. Description of cognitive tests/questionnaires.
The MoCA test is a cognitive screening test that has good sensitivity (76.7%) and specificity (78.6%) for assessing cognitive performance in HD patients (29). Another screening test, the MMSE, showed a sensitivity of 55.2% and specificity of 75% (29). The 3MS is a modified version of the MMSE, which showed a sensitivity of 88% and a specificity of 90% as a screening test for dementia in a study of elderly residents (30). In a study by Dobbs and Shergill (31) examining the predictive power of the TMT for driving performance, the TMTA had a sensitivity of 77% and a specificity of 62%, while the TMTB had a sensitivity of 50% and a specificity of 88%. The cognitive domain of the KDQOL-SF had poor sensitivity (range, 28–36%) and modest specificity (range, 77–81%) for identifying poorer memory and executive function in the HD population (32).
Discussion
In the present review, we highlighted the effects of non-pharmacological interventions (physical exercise or cognitive training) on cognitive performance in HD patients. In addition, we presented and described the cognitive tests used in the included studies. The results of a limited number of studies show that physical exercise may significantly improve cognitive performance or at least mitigate cognitive decline in HD patients. Furthermore, there is insufficient evidence to conclude that cognitive training can attenuate cognitive decline in this population.
Lower cognitive functioning is often seen in HD patients (33–35). It has been documented that impaired cognitive abilities limit the ability to adhere to dialysis activities, make informed decisions, follow food and fluid restrictions, and are a risk factor for mortality in HD patients (36–39). Therefore, the recognition of poor cognitive function is crucial for the implementation of prevention and coping strategies to delay patients' cognitive decline. Furthermore, it is well-known that HD patients have poorer physical function compared to healthy individuals (40) and are mostly physically inactive (41), leading to a decreased quality of life (42). A growing number of randomized controlled trials of exercise training in the HD population show improvement in physical performance (43–46), dialysis symptoms (47), bone mineral density (48, 49), dialysis adequacy (50, 51), and quality of life (52). The highest adherence to physical exercise programs was observed in interventions performed during dialysis (53–55) and these interventions generally appear safe. Notwithstanding the positive effects of physical exercise mentioned above, randomized controlled trials investigating the effects on cognitive performance in HD patients are lacking. However, the limited number of studies included in this review suggests that patients may also benefit in this area.
There are several reasons for the positive association between physical activity and improved cognitive performance. Physical activity has been found to prevent cerebral atrophy or even increase hippocampal volume (56). Furthermore, a recent review found that up to 82% of total brain gray matter volume can be altered by physical activity (57). People in good physical condition can tolerate a higher neuropathological load without suffering cognitive impairment (58). The association between a low cognitive score and high risk or incidence of injury indicates a direct relationship between higher cognitive control and executive function (59, 60). Physical exercise may also have a positive effect on patients' cognitive performance by reducing inflammation and thus improving brain plasticity (61, 62). The results of the present review support the findings of the aforementioned studies in HD patients and contribute to the understanding of the relationship between physical exercise and cognitive performance in this population.
Cognitive training is another non-pharmacological intervention that has received attention in the scientific community. In healthy older adults, cognitive training prevented cognitive decline in executive functions, including working memory, abstracting ability, attentional control, inhibitory control, and verbal reasoning (63–65). Studies investigating cognitive training approaches to combat cognitive decline in HD patients are lacking.
This systematic review has its pitfalls, mainly related to the limitations of the included studies. Limitations include the small number of eligible studies, the small sample size of most included studies leading to low statistical power and possibly associated with potential imbalances in the study groups. The appropriateness of cognitive tests used to measure intervention effects is questionable. The instruments used in the included studies (3MS, MoCA, MMSE, KDQOL-SF) are predominantly screening tests to detect mild cognitive impairment, which are vulnerable to learning effects and may lack sensitivity and specificity (32, 66, 67). Therefore, the aforementioned tests are not the best option to detect the effects of the training interventions presented. Future studies should consider using more sensitive and specific tests instead of using tests that only measure global cognitive performance and are subject to the learning effect. It is proposed to develop a neurocognitive battery to systematically assess various cognitive abilities. Suggested cognitive tests with low learning effect, high sensitivity, validity, and reliability could be the Symbol Digit Modalities Test (SDMT), the Computerized Test of Attentional Performance (TAP), and the Trail Making Test (TMTA and TMTB) (24, 68, 69).
This is the first systematic review to demonstrate the effect of non-pharmacological interventions in the form of physical exercise and cognitive training in HD patients. It also provides insight into the instruments used to measure cognitive performance. These results from a small number of studies suggest that physical exercise training may have a positive effect on cognitive performance in HD patients. The effects of cognitive training or a combination of both approaches should be further investigated (70). Intra-dialysis period provides a unique opportunity to study these effects. Patients could use the time spent during the HD session to replace passive activities with activities that benefit their cognitive status. Research in nephrology has only begun to examine the short-term effects of exercise and cognitive training on cognition. Further studies are needed to replicate these findings and to investigate different strategies to maintain or improve cognitive function not only in HD patients but also in pre-dialysis CKD patients and in transplant recipients. In addition, long-term outcomes such as prevention of dementia should also be investigated. Furthermore, more sensitive and reliable instruments are needed to evaluate the effects of interventions on cognitive performance in this population.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Author contributions
ŠB designed the search strategy. JP, KM, TP, and MP revised the design. Title and abstract screening was performed by ŠB and KM. Full text screening was performed by ŠB and JP. MP and TP performed data analysis. Quality assessment was performed by KM and ŠB. ŠB drafted the manuscript, which was revised by JP, KM, TP, and MP. All authors approved the final version of the manuscript.
Funding
The research is funded from ARRS postdoctoral research project Z3-3213 and ARRS research and infrastructure program P3-0323.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Messier C, Gagnon M. Cognitive decline associated with dementia and type 2 diabetes: the interplay of risk factors. Diabetologia. (2009) 52:2471–4. doi: 10.1007/s00125-009-1533-2
2. Pal A, Pegwal N, Kaur S, Mehta N, Behari M, Sharma R. Deficit in specific cognitive domains associated with dementia in Parkinson's disease. J Clin Neurosci. (2018) 57:116–20. doi: 10.1016/j.jocn.2018.08.016
3. Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet. (2020) 396:413–46. doi: 10.1016/S0140-6736(20)30367-6
4. Horigan AE. Fatigue in hemodialysis patients: a review of current knowledge. J Pain Symptom Manage. (2012) 44:715–24. doi: 10.1016/J.JPAINSYMMAN.2011.10.015
5. Cui L, Chen W, Yu X, Ju C. The relationship between cognitive function and having diabetes in patients treated with hemodialysis. Int J Nurs Sci. (2020) 7:60–5. doi: 10.1016/j.ijnss.2019.12.003
6. McIntyre CW. Haemodialysis-induced myocardial stunning in chronic kidney disease - a new aspect of cardiovascular disease. Blood Purif. (2010) 29:105–10. doi: 10.1159/000245634
7. Murray AM. Cognitive impairment in the aging dialysis and chronic kidney disease populations: an occult burden. Adv Chronic Kidney Dis. (2008) 15:123–32. doi: 10.1053/j.ackd.2008.01.010
8. Sehgal AR, Grey SF, DeOreo PB, Whitehouse PJ. Prevalence, recognition, and implications of mental impairment among hemodialysis patients. Am J Kidney Dis. (1997) 30:41–9. doi: 10.1016/S0272-6386(97)90563-1
9. Kurella M, Mapes D, Port FK, Chertow GM. Correlates and outcomes of dementia among dialysis patients: the dialysis outcomes and practice patterns study. Nephrol Dialysis Transpl. (2006) 21:2543–8. doi: 10.1093/ndt/gfl275
10. Snowden M, Steinman L, Mochan K, Grodstein F, Prohaska TR, Thurman DJ, et al. Effect of exercise on cognitive performance in community-dwelling older adults: Review of intervention trials and recommendations for public health practice and research. J Am Geriatr Soc. (2011) 59:704–16. doi: 10.1111/j.1532-5415.2011.03323.x
11. Carvalho A, Rea IM, Parimon T, Cusack BJ. Physical activity and cognitive function in individuals over 60 years of age: a systematic review. Clin Interv Aging. (2014) 9:661–82. doi: 10.2147/CIA.S55520
12. Jonasson LS, Nyberg L, Kramer AF, Lundquist A, Riklund K, Boraxbekk CJ. Aerobic exercise intervention, cognitive performance, and brain structure: results from the physical influences on brain in aging (PHIBRA) study. Front Aging Neurosci. (2017) 8:336. doi: 10.3389/fnagi.2016.00336
13. Hill NTM, Mowszowski L, Naismith SL, Chadwick VL, Valenzuela M, Lampit A. Computerized cognitive training in older adults with mild cognitive impairment or dementia: a systematic review and meta-analysis. Am J Psychiatry. (2017) 174:329–40. doi: 10.1176/appi.ajp.2016.16030360
14. Rebok GW, Ball K, Guey LT, Jones RN, Kim HY, King JW, et al. Ten-year effects of the advanced cognitive training for independent and vital elderly cognitive training trial on cognition and everyday functioning in older adults. J Am Geriatr Soc. (2014) 62:16–24. doi: 10.1111/jgs.12607
15. Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
16. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:1–10. doi: 10.1186/S13643-016-0384-4/FIGURES/6
17. Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Assessing risk of bias in a randomized trial. Cochrane Handbook Syst Rev Interv. (2019) 205–28. doi: 10.1002/9781119536604.CH8
18. Baggetta R, D'Arrigo G, Torino C, Elhafeez SA, Manfredini F, Mallamaci F, et al. Effect of a home based, low intensity, physical exercise program in older adults dialysis patients: A secondary analysis of the EXCITE trial. BMC Geriatr. (2018) 18:248. doi: 10.1186/s12877-018-0938-5
19. Manfredini F, Mallamaci F, D'Arrigo G, Baggetta R, Bolignano D, Torino C, et al. Exercise in patients on dialysis: A multicenter, randomized clinical trial. J Am Soc Nephrol. (2017) 28:1259–68. doi: 10.1681/ASN.2016030378
20. McAdams-DeMarco MA, Konel J, Warsame F, Ying H, Fernández MG, Carlson MC, et al. Intradialytic cognitive and exercise training may preserve cognitive function. Kidney Int Rep. (2018) 3:81–8. doi: 10.1016/j.ekir.2017.08.006
21. Matsufuji S, Shoji T, Yano Y, Tsujimoto Y, Kishimoto H, Tabata T, et al. Effect of chair stand exercise on activity of daily living: a randomized controlled trial in hemodialysis patients. J Renal Nutr. (2015) 25:17–24. doi: 10.1053/J.JRN.2014.06.010
22. Nakamura-Taira N, Horikawa N, Oka F, Igarashi Y, Kobayashi S, Kato S, et al. Quasi-cluster randomized trial of a six-month low-intensity group-based resistance exercise for hemodialysis patients on depression and cognitive function: a 12-month follow-up. Behav Med. (2021) 2021:741–60. doi: 10.1080/21642850.2021.1966302
23. Stringuetta Belik F, Oliveirae Silva VR, Braga GP, Bazan R, Perez Vogt B, Costa Teixeira Caramori J, et al. Influence of intradialytic aerobic training in cerebral blood flow and cognitive function in patients with chronic kidney disease: a pilot randomized controlled trial. Nephron. (2018) 140:9–17. doi: 10.1159/000490005
24. Arnett JA, Labovitz SS. Effect of physical layout in performance of the trail making test. Psychol Assess. (1995) 7:220–1. doi: 10.1037/1040-3590.7.2.220
25. Hays R, Kallich J, Mapes D, Coons S, Amin N. Kidney Disease Quality of Life Short Form (KDQOL-SF), version 1.3: A Manual for Use Scoring. (1997). Available online at: https://www.researchgate.net/profile/Ronald-Hays/publication/274568265_Kidney_Disease_Quality_of_Life_Short_Form_KDQOL-SF_Version_13_A_manual_for_use_and_scoring/links/5cf56b524585153c3db18a19/Kidney-Disease-Quality-of-Life-Short-Form-KDQOL-SF-Version-13-A-manual-for-use-and-scoring.pdf (accessed August 25, 2022).
26. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
27. Pangman VC, Sloan J, Guse L. An examination of psychometric properties of the mini-mental state examination and the standardized mini-mental state examination: implications for clinical practice. Appl Nurs Res. (2000) 13:209–13. doi: 10.1053/APNR.2000.9231
28. Teng E, Chui CH. The modified mini-mental state examination (3MS). J Consult Clin Psychol. (1987) 48:314–8.
29. Tiffin-Richards FE, Costa AS, Holschbach B, Frank RD, Vassiliadou A, Krüger T, et al. The montreal cognitive assessment (MoCA) - a sensitive screening instrument for detecting cognitive impairment in chronic hemodialysis patients. PLoS ONE. (2014) 9:e106700. doi: 10.1371/JOURNAL.PONE.0106700
30. Bland RC, Newman SC. Mild dementia or cognitive impairment: the modified mini-mental state examination (3MS) as a screen for dementia. Can J Psychiatry. (2001) 46:506–10. doi: 10.1177/070674370104600604
31. Dobbs BM, Shergill SS. How effective is the trail making test (Parts A and B) in identifying cognitively impaired drivers? Age Ageing. (2013) 42:577–81. doi: 10.1093/AGEING/AFT073
32. Sorensen EP, Sarnak MJ, Tighiouart H, Scott T, Giang LM, Kirkpatrick B, et al. The kidney disease quality of life cognitive function subscale and cognitive performance in maintenance hemodialysis patients. Am J Kidney Dis. (2012) 60:417–26. doi: 10.1053/j.ajkd.2011.12.029
33. Elias MF, Elias PK, Seliger SL, Narsipur SS, Dore GA, Robbins MA. Chronic kidney disease, creatinine and cognitive functioning. Nephrol Dial Transpl. (2009) 24:2446–52. doi: 10.1093/ndt/gfp107
34. Drew DA, Weiner DE, Sarnak MJ. Cognitive impairment in CKD: pathophysiology, management, and prevention. Am J Kidney Dis. (2019) 74:782–90. doi: 10.1053/j.ajkd.2019.05.017
35. Ng CZ, Tang SC, Chan M, Tran BX, Ho CS, Tam WW, et al. A systematic review and meta-analysis of randomized controlled trials of cognitive behavioral therapy for hemodialysis patients with depression. J Psychosom Res. (2019) 126:109834. doi: 10.1016/j.jpsychores.2019.109834
36. Drew DA, Weiner DE, Tighiouart H, Scott T, Lou K, Kantor A, et al. Cognitive function and all-cause mortality in maintenance hemodialysis patients. Am J Kidney Dis. (2015) 65:303–11. doi: 10.1053/j.ajkd.2014.07.009
37. Alosaimi FD, Asiri M, Alsuwayt S, Alotaibi T, bin Mugren M, Almufarrih A, et al. Psychosocial predictors of nonadherence to medical management among patients on maintenance dialysis </div>. Int J Nephrol Renovasc Dis. (2016) 9:263–72. doi: 10.2147/IJNRD.S121548
38. Angermann S, Schier J, Baumann M, Steubl D, Hauser C, Lorenz G, et al. Cognitive impairment is associated with mortality in hemodialysis patients. J Alzheimer's Dis. (2018) 66:1529–37. doi: 10.3233/JAD-180767
39. Findlay MD, Dawson J, Dickie DA, Forbes KP, McGlynn D, Quinn T, et al. Investigating the relationship between cerebral blood flow and cognitive function in hemodialysis patients. J Am Soc Nephrol. (2019) 30:147–58. doi: 10.1681/ASN.2018050462
40. Bučar Pajek M, Pajek J. Characterization of deficits across the spectrum of motor abilities in dialysis patients and the impact of sarcopenic overweight and obesity. Clin Nutr. (2018) 37:870–7. doi: 10.1016/j.clnu.2017.03.008
41. Johansen KL, Chertow GM, Nga V, Mulligan K, Carey S, Schoenfeld PY, et al. Physical activity levels in patients on hemodialysis and healthy sedentary controls. Kidney Int. (2000) 57:2564–70. doi: 10.1046/j.1523-1755.2000.00116.x
42. Sietsema KE, Amato A, Adler SG, Brass EP. Exercise capacity as a predictor of survival among ambulatory patients with end-stage renal disease. Kidney Int. (2004) 65:719–24. doi: 10.1111/j.1523-1755.2004.00411.x
43. Segura-Ortí E, Kouidi E, Lisón JF. Effect of resistance exercise during hemodialysis on physical function and quality of life: randomized controlled trial. Clin Nephrol. (2009) 71:527–37. doi: 10.5414/cnp71527
44. Groussard C, Rouchon-Isnard M, Coutard C, Romain F, Malardé L, Lemoine-Morel S, et al. Beneficial effects of an intradialytic cycling training program in patients with end-stage kidney disease. Appl Physiol Nutr Metabolism. (2015) 40:550–6. doi: 10.1139/apnm-2014-0357
45. Frih B, Jaafar H, Mkacher W, Ben Salah Z, Hammami M, Frih A. The effect of interdialytic combined resistance and aerobic exercise training on health related outcomes in chronic hemodialysis patients: the tunisian randomized controlled study. Front Physiol. (2017) 8:288. doi: 10.3389/fphys.2017.00288
46. Bogataj Š, Pajek J, Buturović Ponikvar J, HadŽić V, Pajek M. Kinesiologist-guided functional exercise in addition to intradialytic cycling program in end-stage kidney disease patients: a randomised controlled trial. Sci Rep. (2020) 10:2564–70. doi: 10.1038/s41598-020-62709-1
47. Giannaki CD, Hadjigeorgiou GM, Karatzaferi C, Maridaki MD, Koutedakis Y, Founta P, et al. A single-blind randomized controlled trial to evaluate the effect of 6 months of progressive aerobic exercise training in patients with uraemic restless legs syndrome. Nephrol Dial Transpl. (2013) 28:2834–40. doi: 10.1093/ndt/gft288
48. Liao M-T, Liu W-C, Lin F-H, Huang C-F, Chen S-Y, Liu C-C, et al. Intradialytic aerobic cycling exercise alleviates inflammation and improves endothelial progenitor cell count and bone density in hemodialysis patients. Medicine. (2016) 95:e4134. doi: 10.1097/MD.0000000000004134
49. Marinho SM, Moraes C, Barbosa JE, dos SM, Carraro Eduardo JC, et al. Exercise training alters the bone mineral density of hemodialysis patients. J Strength Cond Res. (2016) 30:2918–23. doi: 10.1519/JSC.0000000000001374
50. Parsons TL, Toffelmire EB, King-VanVlack CE. The effect of an exercise program during hemodialysis on dialysis efficacy, blood pressure and quality of life in end-stage renal disease (ESRD) patients. Clin Nephrol. (2004) 61:261–74. doi: 10.5414/cnp61261
51. Bogataj Š, Pajek J, Buturović Ponikvar J, Pajek M. Functional training added to intradialytic cycling lowers low-density lipoprotein cholesterol and improves dialysis adequacy: a randomized controlled trial. BMC Nephrol. (2020) 21:352. doi: 10.1186/s12882-020-02021-2
52. Barcellos FC, Santos IS, Umpierre D, Bohlke M, Hallal PC. Effects of exercise in the whole spectrum of chronic kidney disease: a systematic review. Clin Kidney J. (2015) 8:753–65. doi: 10.1093/ckj/sfv099
53. Johansen KL. Exercise in the end-stage renal disease population. J Am Soc Nephrol. (2007) 18:1845–54. doi: 10.1681/ASN.2007010009
54. Sheng K, Zhang P, Chen L, Cheng J, Wu C, Chen J. Intradialytic exercise in hemodialysis patients: a systematic review and meta-analysis. Am J Nephrol. (2014) 40:478–90. doi: 10.1159/000368722
55. Bogataj Š, Pajek M, Buturović Ponikvar J, Pajek J. Outcome expectations for exercise and decisional balance questionnaires predict adherence and efficacy of exercise programs in dialysis patients. Int J Environ Res Public Health. (2020) 17:261–74. doi: 10.3390/ijerph17093175
56. Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci USA. (2011) 108:3017–22. doi: 10.1073/pnas.1015950108
57. Batouli SAH, Saba V. At least eighty percent of brain grey matter is modifiable by physical activity: a review study. Behav Brain Res. (2017) 332:204–17. doi: 10.1016/j.bbr.2017.06.002
58. Wallace LMK, Theou O, Godin J, Andrew MK, Bennett DA, Rockwood K. Investigation of frailty as a moderator of the relationship between neuropathology and dementia in Alzheimer's disease: a cross-sectional analysis of data from the rush memory and aging project. Lancet Neurol. (2019) 18:177–84. doi: 10.1016/S1474-4422(18)30371-5
59. Wilkerson GB. Neurocognitive reaction time predicts lower extremity sprains and strains. Int J Athletic Ther Train. (2012) 17:4–9. doi: 10.1123/ijatt.17.6.4
60. Herman DC, Barth JC. Neuromuscular performance varies with baseline neurocognition: implications for anterior cruciate ligament injury risk and prevention. Orthop J Sports Med. (2015) 3:2325967115S0009. doi: 10.1177/2325967115S00095
61. Loprinzi PD, Herod SM, Cardinal BJ, Noakes TD. Physical activity and the brain: a review of this dynamic, bi-directional relationship. Brain Res. (2013) 1539:95–104. doi: 10.1016/J.BRAINRES.2013.10.004
62. Nascimento CMC, Pereira JR, Pires De Andrade L, Garuffi M, Ayan C, Kerr DS, et al. Physical exercise improves peripheral BDNF levels and cognitive functions in mild cognitive impairment elderly with different bdnf Val66Met genotypes. J Alzheimers Dis. (2015) 43:81–91. doi: 10.3233/JAD-140576
63. Mahncke HW, Connor BB, Appelman J, Ahsanuddin ON, Hardy JL, Wood RA, et al. Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. Proc Natl Acad Sci USA. (2006) 103:12523–8. doi: 10.1073/pnas.0605194103
64. Levine B, Stuss DT, Winocur G, Binns MA, Fahy L, Mandic M, et al. Cognitive rehabilitation in the elderly: effects on strategic behavior in relation to goal management. J Int Neuropsychol Soc. (2007) 13:143–52. doi: 10.1017/S1355617707070178
65. Anand R, Chapman SB, Rackley A, Keebler M, Zientz J, Hart J. Gist reasoning training in cognitively normal seniors. Int J Geriatr Psychiatry. (2011) 26:961–8. doi: 10.1002/GPS.2633
66. Dong Y, Sharma VK, Chan BPL, Venketasubramanian N, Teoh HL, Seet RCS, et al. The montreal cognitive assessment (MoCA) is superior to the mini-mental state examination (MMSE) for the detection of vascular cognitive impairment after acute stroke. J Neurol Sci. (2010) 299:15–8. doi: 10.1016/j.jns.2010.08.051
67. Lee SH, Cho Aj, Min Y-K, Lee Y-K, Jung S. Comparison of the montreal cognitive assessment and the mini-mental state examination as screening tests in hemodialysis patients without symptoms. Ren Fail. (2018) 40:323–30. doi: 10.1080/0886022X.2018.1455589
68. Benedict RHB, Deluca J, Phillips G, LaRocca N, Hudson LD, Rudick R. Validity of the symbol digit modalities test as a cognition performance outcome measure for multiple sclerosis. Multiple Sclerosis. (2017) 23:721–33. doi: 10.1177/1352458517690821
69. Zimmermann P, Fimm B. Test of Attentional Performance 2.3.1. Vera Fimm, Psychologische Testsysteme. (2017). Available online at: https://www.psytest.de/index.php?page=TAP-2-2&hl=en_US (accessed February 1, 2021).
Keywords: cognitive performance, hemodialysis, physical exercise, cognitive training, cognitive tests, intervention
Citation: Bogataj Š, Mesarič KK, Pajek M, Petrušič T and Pajek J (2022) Physical exercise and cognitive training interventions to improve cognition in hemodialysis patients: A systematic review. Front. Public Health 10:1032076. doi: 10.3389/fpubh.2022.1032076
Received: 30 August 2022; Accepted: 27 September 2022;
Published: 14 October 2022.
Edited by:
Stevo Popovic, University of Montenegro, MontenegroReviewed by:
Predrag R. Bozic, Serbian Institute of Sport and Sports Medicine (SISSM), SerbiaDragan Cvejić, University of Novi Sad, Serbia
Aleksandra Aleksić Veljković, University of Nis, Serbia
Copyright © 2022 Bogataj, Mesarič, Pajek, Petrušič and Pajek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Špela Bogataj, c3BlbGEuYm9nYXRhakBrY2xqLnNp