 Šime Smolić
Šime Smolić Nikola Blaževski
Nikola Blaževski Margareta Fabijančić
Margareta Fabijančić- Department of Macroeconomics and Economic Development, Faculty of Economics and Business, University of Zagreb, Zagreb, Croatia
The COVID-19 pandemic exacerbated issues regarding access to healthcare for older people, by far the most vulnerable population group. In particular, older adults avoided seeking medical treatment for fear of infection or had their medical treatments postponed or denied by health facilities or health professionals. In response, remote medical services were recognized as an essential adjustment mechanism to maintain the continuity of healthcare provision. Using the SHARE Corona Survey data, we estimate logistic and multilevel regression models for the remote care of 44,152 persons aged 50 and over in 27 European countries and Israel. Our findings suggest that those aged 80+ were the least likely to use remote healthcare. However, women, better educated individuals, older adults who lived in urban areas, those with no financial strain, and active Internet users used remote medical consultations more often. Those who reported poor or fair health status, two or more chronic diseases, or hospitalization in the last 12 months were significantly more likely to use remote healthcare. Furthermore, remote medical consultations were more frequent for those who had their healthcare postponed or went without it due to fear of coronavirus infection. Finally, older adults used remote care more frequently in countries with less healthcare coverage and lower health expenditures. Health systems should prioritize vulnerable groups in maintaining continuity in access to healthcare, despite the availability of remote care. Policymakers should improve telemedicine regulation and offer incentives for providers of remote healthcare services by adapting reimbursement policies. Remote medical care could play an important role in maintaining healthcare access for older adults and increasing health systems' preparedness in future health emergencies.
Introduction
The unexpected effects of the coronavirus disease (COVID-19) pandemic have led to significant adaptations of health systems in providing healthcare services. One of the adjustment mechanisms includes the more frequent use of telemedicine to maintain continuity in healthcare provision that has been interrupted by epidemic control measures known as stay-at-home orders, lockdowns or social distancing for both COVID-19 patients and those with non-COVID-19 related conditions. The simplest definition of telemedicine is the remote delivery of efficient healthcare services using different innovative information and communication technologies (ICTs) (1). Since the benefits of telemedicine have been recognized in previous public health emergencies, for example, for the Severe acute respiratory syndrome (SARS) or Middle East respiratory syndrome (MERS) (2), this experience has been used, adjusted for the COVID-19 pandemic.
Telemedicine can improve access to healthcare for patients living in remote areas, for example, in rural communities of developing countries who experience limited access to healthcare more often (3). Moreover, it can deploy large numbers of providers rapidly, facilitating the triage and supply clinical services when health facilities cannot meet demands (4). Additionally, it can reduce the risk of complications in individuals with chronic conditions (5) or improve medication adherence for people with chronic diseases (6). Furthermore, remote consultations can help control virus transmission and minimize risk exposure for vulnerable populations (7–9) or improve access to healthcare for patients who fear contagion in health facilities (10, 11).
Altogether, telemedicine has been an efficient, convenient, and affordable healthcare delivery method. It has been used decades before the onset of the COVID-19 pandemic on a relatively small scale, mainly due to professional, technological, or legal barriers (6, 12). However, the COVID-19 pandemic accelerated the implementation and expansion of telehealth and led to a significant change in its perception and role within health systems. The great potential of telemedicine is identified through the more efficient provision of healthcare services for older patients since they put a great deal of pressure on public health spending (13). Besides that, those aged 65 and over were the most vulnerable of the population in the COVID-19 pandemic, both in terms of morbidity and mortality (14–17). Considering that one in five inhabitants of the European Union (EU) in 2020 was 65 years or older (18), the challenges for health systems are unquestionable. Older people with chronic diseases are exposed to a greater risk of adverse long-term consequences of limited access to healthcare (19), and are more likely to experience social isolation and loneliness due to social distancing (20, 21). Consequently, age-friendly remote medical services should, to some extent, mitigate these challenges.
Although we have observed an increase in the reach of telemedicine since the outbreak in European countries, we have little knowledge about older adults who have been using it. This study's primary goal is to better understand the characteristics of older adults that use remote medical care. It explores the relationship between the utilization of remote medical consultations and sociodemographic- and health(care)- related characteristics of older Europeans during the COVID-19 pandemic. To analyze remote healthcare among older adults in the pandemic, we use data collected in the first (June–August 2020) and second (June–August 2021) SHARE Corona Survey (SCS) and supplement them with data from previous SHARE waves. Accordingly, we address the following research questions: (1) Which sociodemographic characteristics are associated with the use of remote medical consultations since the outbreak in Europe and Israel? (e.g., were older adults living in rural areas more likely to use remote medical consultations compared with those living in urban areas?), and (2) Can we relate health system characteristics, for example, organization or financial resources, with older adults' use of remote medical care during the COVID-19 pandemic? The following section presents the international experience of telemedicine and its use among the older population, followed by materials and methods and a section assigned for research results. The final part of the paper provides a discussion and conclusions.
Telemedicine in the International Context and Its Use Among Older Adults
International Experience of Telemedicine in the COVID-19 Pandemic
As face-to-face medical consultations have been discouraged, the use and financing of remote consultations (e.g., virtual or phone call visits) have been encouraged since the outbreak. Following the positive experience in China (22, 23), governments in other countries (e.g., Australia, Canada, the United States, and England) relaxed their regulatory frameworks and made their health systems more flexible in response to the COVID-19 pandemic (24, 25). It has been confirmed that countries that invested in telemedicine before the outbreak were more likely to ensure the necessary care for patients (26). Unfortunately, many developing countries where the coverage of telemedicine health services is negligible had not previously invested in telemedicine, and many people are unaware of its practical benefits (12, 27). Bhaskar et al. (28) share perhaps the most detailed study of the state of telemedicine globally before and during the COVID-19 pandemic. They examined telemedicine development and implementation measures in different countries, identified barriers, and proposed actions to integrate telemedicine into public health framework. Many parts of the world (e.g., Africa, the Caribbean, Latin America, and South Asia) either have no national telemedicine frameworks (e.g., in countries like Bangladesh and Mexico); the implementation of telemedicine is hampered due to poorly developed communication technology, conflicts, and war (e.g., in Africa); or its uptake is still relatively slow (e.g., in Argentina) (28). Many European countries recorded a rapid increase in the volume of remote consultations, for example, in primary care (e.g., in Croatia, Malta, Poland, Sweden, and the UK). Remote consultations have increased further in other countries (e.g., Austria, Belgium, Denmark, Estonia, France, Germany, Italy, Luxembourg, and Switzerland) (29). The following examples from several countries illustrate the status of telehealth after the outbreak.
In Germany, Peine et al. (30) investigated the perception of telemedicine. They concluded that medical professionals accept telemedicine, but the many technical and regulatory burdens, especially in university hospitals compared with private health providers, were critical obstacles for additional development. Following the outbreak, France was eager in promoting the use and reimbursement of telemedicine (e.g., for patients with COVID-19 symptoms and those with confirmed COVID-19), while in Italy, telemedicine was not included in the basic package of health services until the end of March 2020 (31). The French healthcare system recognized the telemedicine system before COVID-19—both in terms of regulation and its implementation (28). The limited reach of telemedicine in Italy has been linked to Italian unpreparedness to deal with the COVID-19 health crisis. Here, the telemedicine application was limited mainly due to a lack of implementation and integration of telemedicine services in the national health system from previous years (32). Another example is the UK, where general practitioners were recommended to use video or telephone triage whenever possible to reduce face-to-face contacts (33). Parisien et al. (34) found a positive correlation between COVID-19 disease burden, measured by COVID-19 cases, and the utilization of telehealth services in orthopedic departments across the US. It is essential to mention that even after lifting the lockdown restrictions in April or May 2020, the interest in remote (online) consultations was still sustained (29).
Use of Telemedicine to Meet Healthcare Needs of Older Adults
Many studies have explored the use of telehealth among older adults during the COVID-19 pandemic and most of them reported positive experiences in terms of patient satisfaction (13, 35–37). An analysis of almost four million consultations at the primary care level between February 17 and May 10, 2020 revealed a more than twofold increase in telephone and electronic video consultations for adults 65 and older in the UK (33). This expansion in terms of video and remote consulting in UK general practice after the COVID-19 outbreak is described as “the biggest evolving natural experiment in general practice in our lifetimes” (38). A study by Gareri et al. (39) found that remote monitoring, either by telephone or video, could protect against the negative consequences of limited access to healthcare for geriatric outpatients. Besides this, Custodero et al. (5) also confirmed telemedicine's usefulness in remotely monitoring the health status of older outpatients. Liu et al. (36) concluded that frail older adults and those without a caregiver to attend assessments with them were less likely to use remote medical care. Bhaskar et al. (13) view the telehealth/telemedicine solutions for the elderly (e.g., home monitoring or telemedicine for those with mental health conditions) as a tool that could lower the burden on public health facilities and an interface that could connect medical specialists with nursing care staff, carers, and patients.
Even though the COVID-19 pandemic prompted many older adults to start using telehealthcare, a “digital divide” between younger and older generations is still evident since older adults are less likely to use or be interested in using telehealthcare (40). This finding has been confirmed in studies before the COVID-19 pandemic; for example, Kontos et al. (41) showed that older men and those with lower education and income in the US were less likely to engage in eHealth activities compared to their counterparts. Additionally, several studies in the early stage of the pandemic in China stress that older people were less prone to use telemedicine applications (9, 42). However, the shift to remote mental healthcare for NHS older adults in the UK did not seem dramatic (43), while in France, the share of older adults (aged 70+) in teleconsultations increased enormously during lockdown (29).
Finally, there are still many unanswered questions about the impact of telemedicine on access to healthcare for older people. Based on earlier works, it seems that this impact is somewhat unclear (35) and the use of telehealth among older people should be viewed from different angles: one where we can see the advantages and another where we observe weaknesses, for example, difficulties to treat patients with cognitive impairment, lack of privacy, technical issues, and so on (12, 13).
Materials and Methods
Data and Variables
We gathered publicly available data from the first and the second SHARE Corona Survey (SCS) (n = 44,152) (44, 45). SHARE (The Survey of Health, Ageing and Retirement in Europe) is a cross-national panel survey that collects microdata on health and the socioeconomic status of individuals aged 50+ in 28 European countries and Israel (46–48). The SCS, which was implemented as a quick response within the SHARE study to understand the effects of the COVID-19 pandemic, asked various questions about key life domains affected by the COVID-19 outbreak, including access to healthcare and the use of remote medical consultations. Data in the first SCS were collected via 20–25-min telephone interviews (CATI) from June to August 2020 (49). Additionally, respondents who participated in the first SCS were interviewed again in the second SCS from June to August 2021. Besides the SCS datasets, we use data collected in previous regular SHARE waves (50–57).
Outcome Variable
The outcome binary variable indicates the use of remote medical consultations since the outbreak. It has been constructed from the following question: “Since the outbreak of Corona, how many remote medical consultations over the phone, computer, or any other electronic means, did you have, if any, with or without video?” This question was asked in the second SCS only, and it captures the use of telehealth in almost a one-and-a-half-year period.
Explanatory Variables
We use a set of sociodemographic variables (age, gender, living arrangement, education, financial situation, urbanity, and Internet use) and selected health-related variables (e.g., self-reported health, number of chronic illnesses, healthcare use, and unmet healthcare) (see Table 1). The age of respondents is divided into three categories to account for the occupationally active (ages 50–64), young retirees (ages 65–79), and the oldest individuals (age 80+), and the education of respondents is divided into low, medium or high, based on ISCED 2011 classification. The variable “lives with others vs. lives alone” represents the individuals' living arrangements. Simultaneously, the latest available area of residence could be either rural (rural area or village) or urban and is drawn from the regular SHARE waves and the second SCS. Financial situation is a self-reported household financial situation by financial respondents, while the variable “Internet use” indicates if respondents ever used the Internet, for example, e-mailing or searching for information on health-related issues after the outbreak. From the list of health-related variables, we have included: self-rated health (SRH), ranging from poor to excellent and dichotomized into “fair or poor” and “good and better”; the number of chronic conditions (less than two conditions vs. two or more chronic conditions); a dichotomous variable indicating whether the respondent was treated in hospital in the last 12 months; a dummy variable to tell if a respondent has had scheduled medical treatment postponed by a doctor or medical facility; and another one suggesting medical treatments foregone for fear of coronavirus infection. We also employed country controls using a set of country dummies and accounted for health system characteristics: prevailing type of health system financing and organization (Bismarck vs. Beveridge), Universal Health Coverage (UHC) index of service coverage (score below/above 80), health expenditures per capita (in euros adjusted for purchasing power parity) and the number of doctors per 100 thousand inhabitants. Additionally, we excluded respondents in nursing homes (n = 385) and interviews collected from proxy respondents (n = 1,269). Thus, our final working sample is restricted to 44,152 respondents following the exclusion of randomly missing values for all explanatory variables (the percentages of missing data range from none to a maximum of 2.3% for the variable marking the household economic situation).
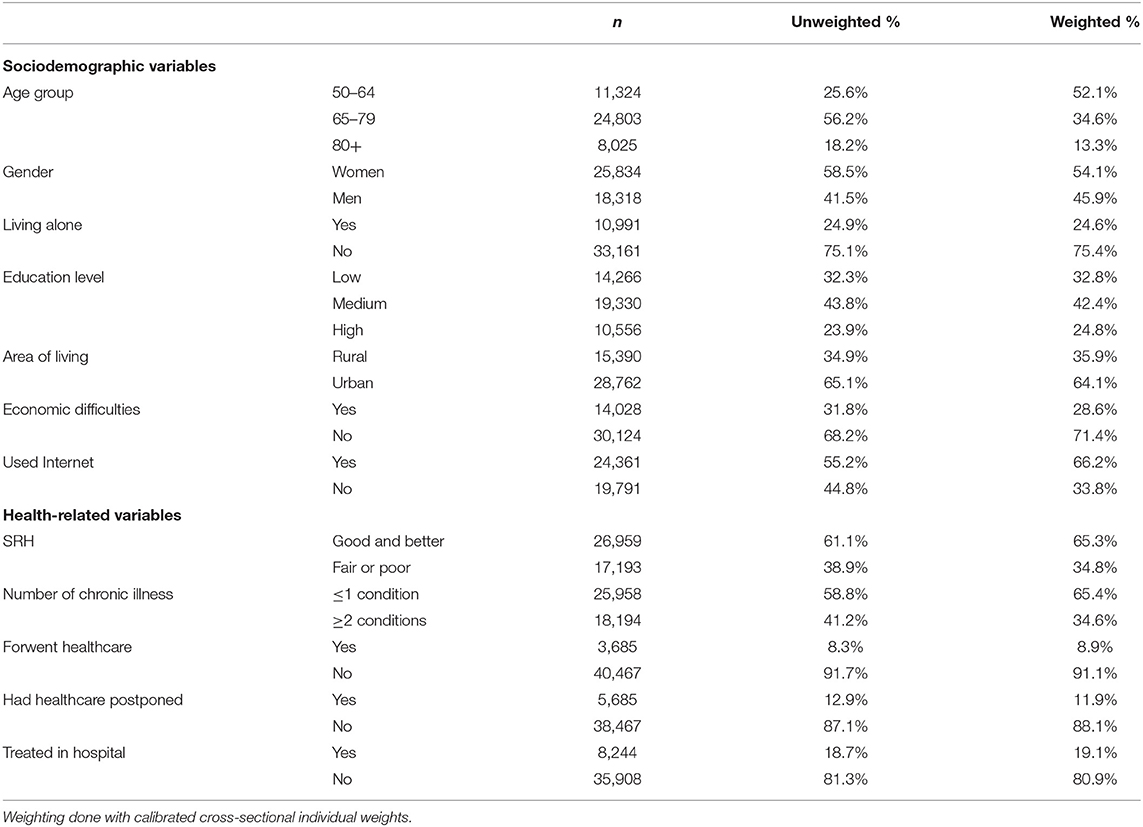
Table 1. Weighted and unweighted description of the sample micro-level explanatory variables (n = 44,152).
Data Analysis
Descriptive analyses were carried out to estimate the use of remote medical consultation among people aged 50 and over from the outbreak of the COVID-19 pandemic until the summer of 2021. All categorical variables were reported as count and (un)weighted percentages, while continuous variables were presented as mean. Next, we constructed a multivariable logistic regression model to assess our outcome variable. Each explanatory variable has been previously tested with our outcome variable before being included in the model (chi-square and t-test; see Tables 1–3). We apply country controls in our pooled logistic regression model to account for different impacts of the COVID-19 pandemic. We then estimate a multilevel logistic regression model and compare it with the pooled logistic regression results (see Table 4). In the next step, we used a multilevel model to explore (country) macro-level factors' effects on the odds of having remote medical consultations during the COVID-19 health crisis. The following section interprets our study results using odds ratios and average marginal effects associated with selected significant micro or macro-level explanatory variables.
Results
Micro-Level Explanatory Variables
In our sample from 27 European countries and Israel, almost one in three [33%, 95% CI (31.2, 34.8)] older adults aged 50 and over have had remote medical consultations over the phone, computer, or any other electronic means, with or without video. Figure 1 shows the percentages of older adults who had remote medical consultations by country. Heterogeneity in remote medicine use between European countries is apparent. In Austria and Germany, around 5% and in Latvia and Lithuania, about 70% of those aged 50 and over reported having remote medical consultations since the outbreak.
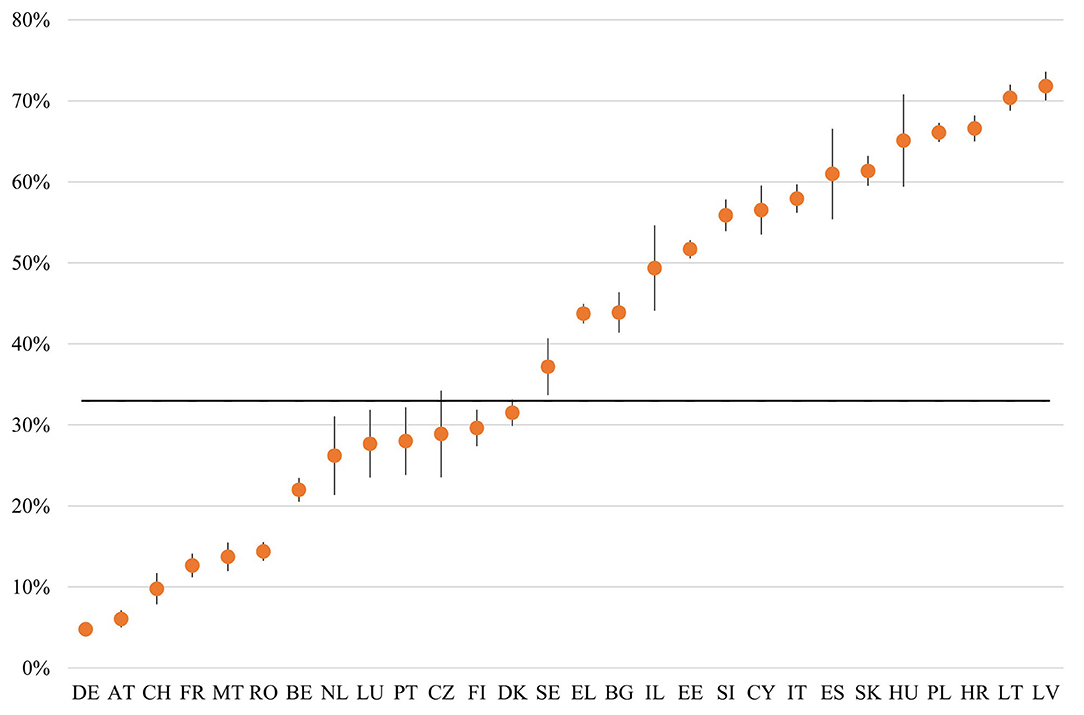
Figure 1. The percentage of respondents aged 50 and over who had remote medical consultations since the outbreak by country (second SCS June–August 2021). Note: Black line represents the sample average–otherwise weighted data with 95% CI.
Table 1 presents descriptive information on the micro-level explanatory variables. Besides the weighted data, we have included unweighted percentages for sample variables1.
Table 2 shows the results of testing (chi-square tests) of each micro-level explanatory variable independently of the outcome variable (univariate analysis). Use of remote medical consultations after the outbreak was higher among those aged 65–79 (34.1 vs. 32.7% 50–64 and 31.2% 80+), among women (34.8 vs. 30.8% men), and those who lived with others (33.4 vs. 31.6% living alone). It was more common among those with low education (42.5 vs. 27.7% high) and with economic difficulties (45.2 vs. 28.1% without difficulties), older adults in urban areas (36.1 vs. 27.5% in rural), and among those who never used the Internet for e-mailing, searching for information, making purchases, or for any other purpose at least once after the outbreak. Additionally, the use of remote medical consultations is more likely among those with fair or poor overall health (40.5 vs. 29% in good health or better), with two or more chronic diseases (39.7 vs. 29.4% with less than one chronic disease), individuals who have forgone medical treatment due to fear of coronavirus infection (35.3 vs. 32.8%) and those who had their scheduled medical treatment postponed by doctor or health facility (47.5 vs. 31%). Finally, we can see that those treated in the hospital in the last 12 months were significantly more likely to have had remote medical consultations after the outbreak.
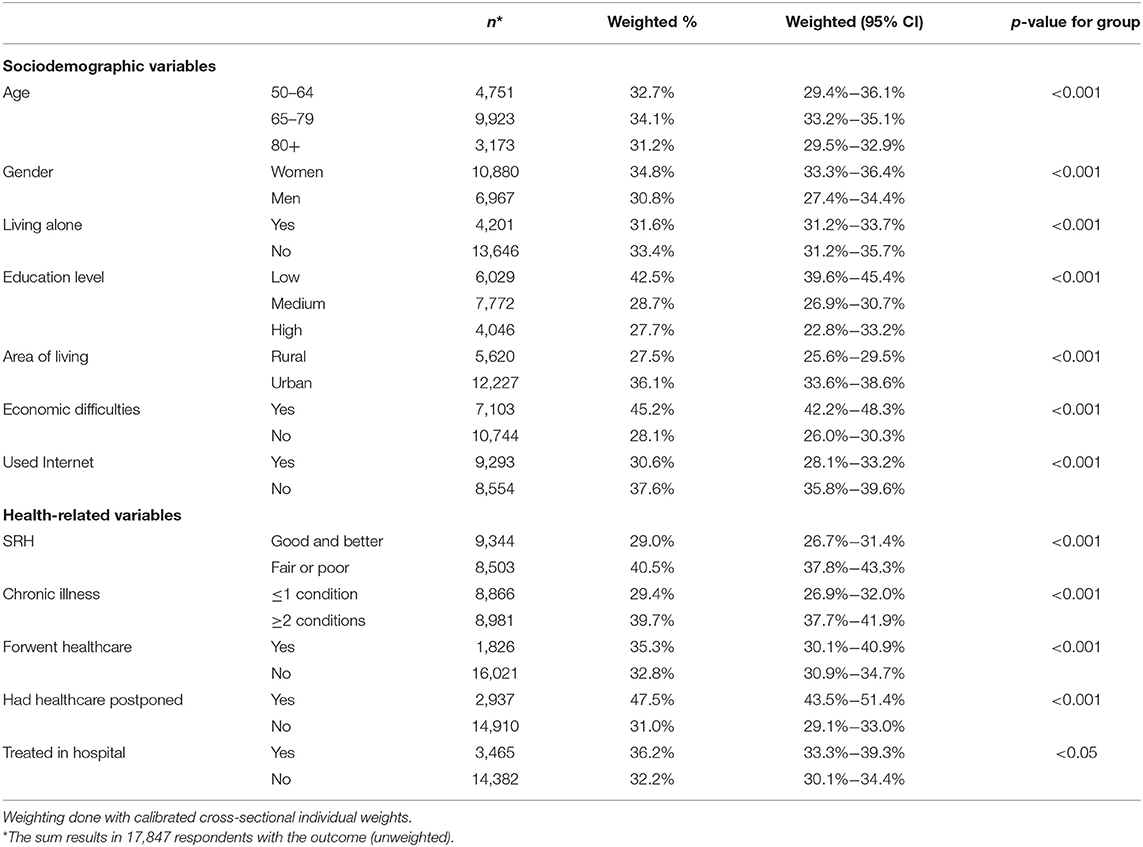
Table 2. Use of remote medical consultations among people aged 50 and over in 27 European countries and Israel based on the second SCS June–August 2021.
Macro-Level Explanatory Variables
Table 3 describes the characteristics of macro-level explanatory variables for the countries in the sample. Estimations (not presented here) show that older adults aged 50 and over from countries where the UHC index was below 80 were more likely to use remote medical consultations after the outbreak (52 vs. 31.8% in countries with UHC ≥80; p < 0.001). Moreover, the use of remote medical consultations among people aged 50 and over was more prevalent in countries where healthcare is financed dominantly through health insurance contributions (48.7 vs. 37.7% in countries with tax financing; p< 0.001). Finally, we have tested the association between per capita health expenditures and health system resources—captured by the number of practicing physicians—and remote medical consultations among older adults. Persons aged 50 and over were less likely to use remote medical consultations in countries where health expenditures per capita were larger. A similar finding appears for the number of practicing physicians.
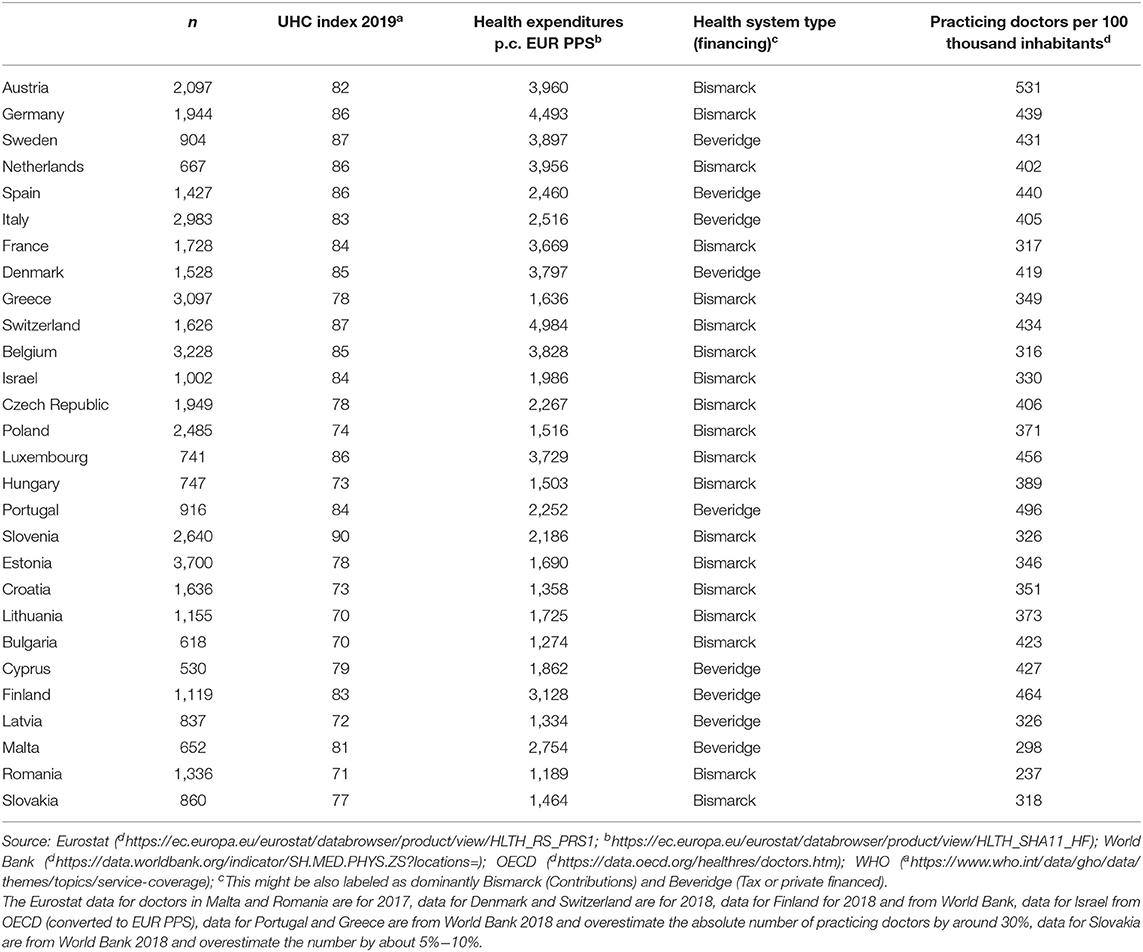
Table 3. Health system characteristics of countries in the sample.
Empirical Approach and Results
Table 4 presents estimated odds ratios from the pooled logistic regression model with country controls and a multilevel logistic regression model. In the multilevel regression model, we nested individuals in countries and allowed intercepts to vary across countries. The results allowed us to stress the determinants of remote medical consultations among older adults during the COVID-19 pandemic. Then we used multilevel modeling to investigate the effects of country-level variables on the odds of having remote medical consultations during the pandemic. Since macro-level variables exhibit a moderate to strong correlation, they have been added to the models successively.
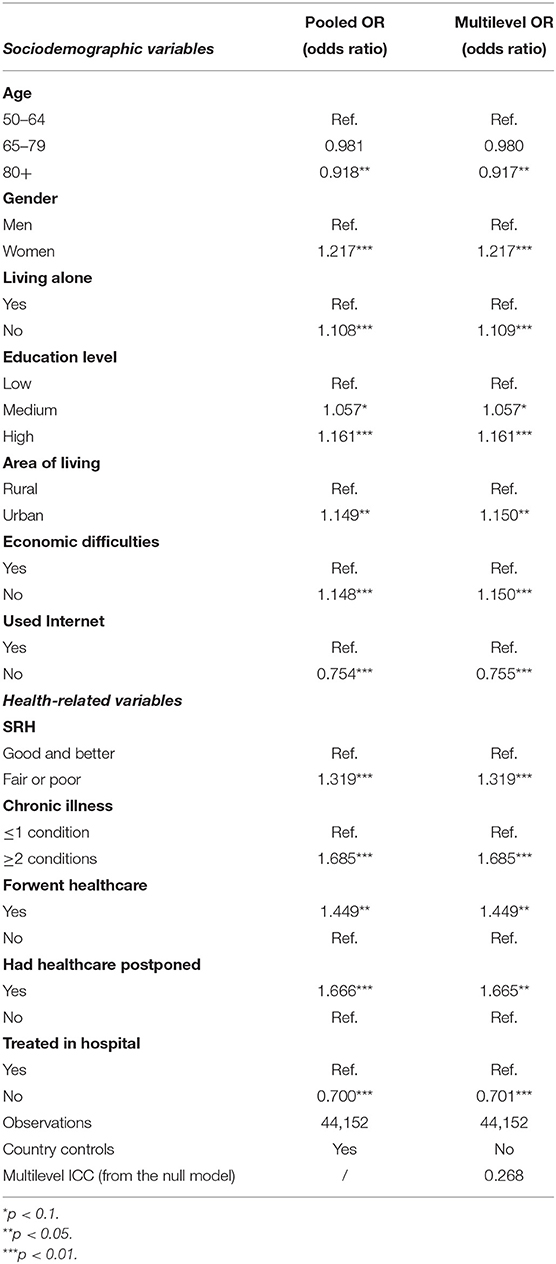
Table 4. Determinants of remote medical consultations among older adults in Europe and Israel after the outbreak of the COVID-19 pandemic.
As expected, the oldest individuals (80+) were the least likely to use remote medical consultations [OR = 0.92, 95% CI (0.85, 0.99)], while on the other hand, women were more likely to use remote care [OR = 1.22, 95% CI (1.16, 1.27)]. The effects of education are noticeable, as more educated older adults aged 50 and over had greater odds of reporting the use of remote care [OR = 1.16, 95% CI (1.09, 1.24)]. Those who lived in urban areas [OR = 1.15, 95% CI (1.09, 1.20)] and who did not experience financial difficulties [OR = 1.15, 95% CI (1.08, 1.21)] were more likely to use remote medical consultations. Being an active user of the Internet increased the odds significantly of using remote medical care among the population aged 50 and over (the odds of remote consultations for this group were around 25% higher). Moreover, health-related variables turned out to be significant predictors of remote care use during the pandemic. Older adults who reported poor or fair SRH [OR = 1.32, 95% CI (1.25, 1.39)] and those with two or more chronic health conditions [OR = 1.69, 95% CI (1.61, 1.77)] were significantly more likely to use remote medical consultations. Further, the odds of reporting remote medical consultation use were 30% lower for older adults who have not been treated in hospital in the last 12 months (before the interview) compared to those who have been hospitalized. Moreover, the odds of using remote healthcare were higher for those who had their scheduled medical treatment(s) postponed (by 67%) or had forgone medical treatment due to fear of coronavirus infection (by 45%). In Figure 2, we show predicted outcome probabilities with 95% confidence intervals for healthcare forgone or postponed, separately for men and women.
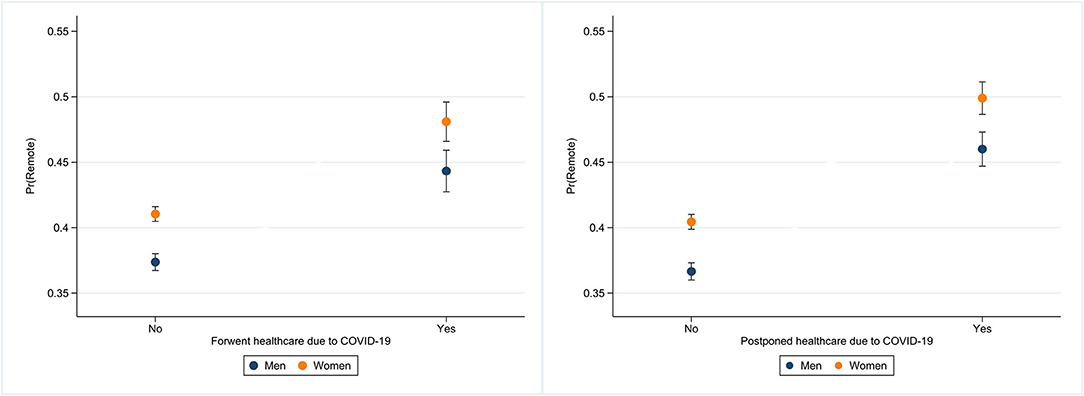
Figure 2. Estimated probabilities of remote medical consultations for men and women and healthcare forgone or postponed.
From Table 5, we can see that respondents from countries with lower UHC index (UHC <80) were 3.4 times more likely to use remote medical consultations compared to respondents in countries with very high UHC index. Further, higher health expenditures per capita were associated with slightly lower odds of using remote care among older adults after the outbreak. We also found greater odds of using remote care for older adults in countries where the tax financing of healthcare prevails and where the average number of practicing physicians is lower, but these results were insignificant. Additionally, in Figure 3 we present predicted outcome probabilities of significant explanatory macro-level variables.
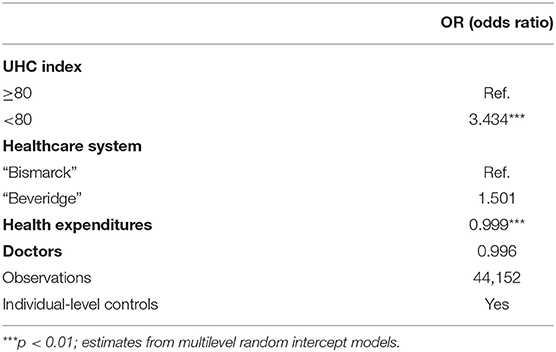
Table 5. Country context effects on the use of remote medical consultations among older adults.
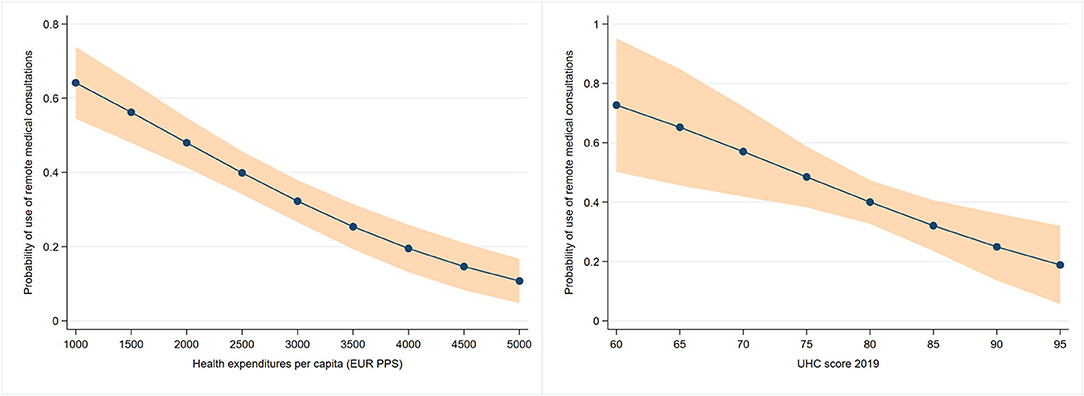
Figure 3. Predictive margins at specified values of macro-level variables.
Discussion
This study analyzed the characteristics of individuals aged 50 and over in 27 European countries and Israel who have used remote medical consultations after the COVID-19 outbreak. Since many aspects of medical care have been disrupted by COVID-19, remote medical consultations, at least partially, helped mitigate the backlog in healthcare provision across Europe. When it comes to population groups that have felt this pandemic's most harmful health consequences, older people, especially those with chronic illnesses, can be placed at the top of the vulnerability scale. Many studies have confirmed that the elderly have been the most vulnerable group during the pandemic [see, e.g., (58) or (59)]. Barriers to accessing adequate healthcare triggered many negative consequences for the current health status of older adults. Additionally, delayed medical care utilization and discontinued care—more pronounced during the COVID-19—are expected to adversely affect older adults' health status in the future (60). Here, telemedicine is a promising tool with great potential in reducing unmet healthcare needs (61) and its uptake in some countries after the outbreak was exceptional (33).
One goal of this study was to identify the characteristics of persons aged 50 and over who had remote medical consultations after the outbreak and the other was to explore whether using remote medical consultations was associated with the features of healthcare systems. We found significant differences in the prevalence of remote medical consultations among European countries and Israel, ranging from about 5% in Germany to over 70% in Latvia. We have shown that persons aged 80+, men, and those with poorer socioeconomic statuses were less likely to use remote medical care during the COVID-19 pandemic. Our findings align with those reported in previous studies, such as Kontos et al.'s (41) for the US adult population. Still, this finding is concerning because older individuals could experience the most adverse effects of any population due to missed healthcare during the pandemic.
Furthermore, urbanity was associated with greater odds of remote care use among older Europeans. This finding might be related to the fact that digital infrastructure is better in urban communities, although telemedicine is more often perceived as a facilitator of unmet healthcare in rural areas (3). Our results indicate that more active users of the Internet, and probably those with higher levels of digital literacy, had greater odds of using remote medical consultations. This is in line with conclusions that limited access to broadband Internet and Internet facilities is the main obstacle in the deployment of telemedicine (13) and is a more significant issue, especially in developing countries (7). From this perspective, the message for policymakers is that deeper penetration of digital infrastructure is essential for this segment of healthcare provision to develop.
Health-related variables showed significance in predicting the use of remote medical consultations during the COVID-19 pandemic. Persons aged 50 and over with poorer subjective and objective health statuses were significantly more likely to use remote medical consultations. On the one hand, this could indicate that the COVID-19 pandemic pushed them to switch to this method of accessing healthcare. Still, on the other hand, it could mean that healthcare providers have supplied more remote medical consultations to them because of limitations in the provision of healthcare caused by the pandemic. The latter could suggest the adaptation of healthcare providers and finding new ways of healthcare delivery in the current health crisis. Our following important finding is about the association of unmet healthcare—scheduled medical treatment(s) postponed and medical treatments forgone due to fear of coronavirus infection—and use of remote medical consultations. Generally, the odds of using remote medical care were significantly larger for older adults with unmet healthcare needs. This finding could lead to the conclusion that remote care buffered some unmet healthcare during the COVID-19 pandemic and contributed to continuity in healthcare provision.
Macro-level explanatory variables have been employed to account for health system features that might affect the use of telehealth in different countries [see, e.g., (29)]. Our estimates show that older adults were less likely to use remote medical consultations in countries with a very high UHC index of service coverage. Additionally, we observed lower odds of using remote care among older adults after the outbreak in countries with bigger health expenditures. One could expect that larger densities of practicing physicians were associated with lower prevalences of remote medical consultation, but this variable was insignificant.
To conclude, many countries face problems concerning telehealth to ensure access to regular healthcare. In general, health systems should support both providers and users of telehealth services. However, our findings suggest that health systems should prioritize certain groups for which the continuity in access to healthcare might be a challenge. In particular, these include the oldest individuals (men), people with multiple chronic diseases, those in poor socioeconomic conditions, those living in rural areas, those living alone, and those with poor or no digital skills. Policy strategies may include ongoing support for telehealth, telemedicine regulation, incentives for providers of telehealth services in terms of reimbursement policies, and education about telemedicine. There is evidence that telemedicine can ease the burdens of healthcare delivery in the COVID-19 crisis and improve its access and efficiency (13), but we should be aware that it has limited reach for certain patients who have inadequate resources and access to telemedicine (62). Nevertheless, its importance has already been recognized in some countries (e.g., Denmark), which have incorporated telemedicine into their digitization strategies (29). In addition, telehealth is also of great importance to the European Commission (63), especially in addressing the difficulties in accessing medical services and improving patient outcomes and health system efficiency (64). As the world's population becomes an aging one and we learn to live with COVID-19, remote medical care is a crucial healthcare method that can be accessed safely by older people and ease burdens on healthcare systems.
Further research should also focus on methods that could improve telemedicine penetration and acceptance among at-risk groups in the general population. Inequitable access to telemedicine should be addressed with the expansion of broadband Internet infrastructure and related communication technology, including education and knowledge sharing among both patients (and their families) and medical staff (62, 65). Telemedicine implementation should be accompanied by the harmonization of existing and the introduction of the new regulations to ensure service quality standards and the protection of patient data and privacy. Policymakers should raise awareness of telemedicine benefits for both patients and the healthcare workforce; as already mentioned, telemedicine can act as a link between medical specialists, local nursing home/caring staff, and patients (13). Telemedicine uptake and implementation also need to be accompanied by adequate financial support (e.g., reimbursement), with special emphasis on making it available to at-risk groups—older adults and especially those in poor health and poor socioeconomic conditions.
Limitations
This study has several limitations. First, many variables are self-reported, and self-reporting bias cannot be disregarded. Second, differences in remote medical consultations usage might result from cross-cultural differences in different countries or other unobserved health system features. Third, the study's design did not permit us to differentiate between various kinds of remote medical consultations after the outbreak and we considered all kinds of remote consultations.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found at: http://www.share-project.org/data-documentation/share-data-releases.html. All data used in our study are available free of charge to all scientific users world-wide after individual registration (http://www.share-project.org/data-access/user-registration.html). SHARE data are DOI registered datasets. Each wave and each release is assigned a persistent DOI. In our article we use SHARE data from Waves 1, 2, 3, 4, 5, 6, 7, 8 and 9 (DOIs: 10.6103/SHARE.w1.800, 10.6103/SHARE.w2.800, 10.6103/SHARE.w3.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8ca.800, 10.6103/SHARE.w8.800, and 10.6103/SHARE.w9ca.800).
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the University of Mannheim and Ethics Council of the Max Planck Society. For more details see: http://www.share-project.org/fileadmin/pdf_documentation/SHARE_ethics_approvals.pdf. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
ŠS contributed to the conceptualization, methods, implications, and wrote the first draft of the manuscript. NB organized the database. ŠS, NB, and MF contributed equally in performing the statistical analyses. NB and MF wrote sections of the manuscript. All authors contributed to manuscript revision and read and approved the submitted version.
Funding
This work was supported by the EU Horizon 2020 SHARE-COVID19 project [grant number 101015924]. The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, and SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, and DASISH: GA N°283646), Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, and SSHOC: GA N°823782) and by DG Employment, Social Affairs & Inclusion through VS 2015/0193, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the US National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see www.share-project.org).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
This publication is based on the SHARE Wave 8 1st SHARE Corona Survey data (10.6103/SHARE.w8ca.800) and the SHARE Wave 9 2nd SHARE Corona Survey data (10.6103/SHARE.w9ca.800). In addition, this paper uses data from SHARE Waves 1, 2, 4, 5, 6, 7 and 8 (DOIs: 10.6103/SHARE.w1.800, 10.6103/SHARE.w2.800, 10.6103/SHARE.w3.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, and 10.6103/SHARE.w8.800), see Börsch-Supan et al. (47) for methodological details.
Footnotes
1. ^More details about the weighting procedure in SHARE study is available at http://www.share-project.org/faqs/7-weights.html.
References
1. World Health Organization (WHO). Telemedicine: Opportunities and Developments in Member States. Report on the Second Global Survey on eHealth. Geneva: World Health Organization (2010).
2. Lee I, Kovarik C, Tejasvi T, Pizarro M, Lipoff JB. Telehealth: helping your patients and practice survive and thrive during the COVID-19 crisis with rapid quality implementation. J Am Acad Dermatol. (2020) 82:1213–4. doi: 10.1016/j.jaad.2020.03.052
3. Wootton R, Geissbuhler A, Jethwani K, Kovarik C, Person DA, Vladzymyrskyy A, et al. Long-running telemedicine networks delivering humanitarian services: experience, performance and scientific output. Bull World Health Organ. (2012) 90:341-347D. doi: 10.2471/BLT.11.099143
4. Smith AC, Thomas E, Snoswell CL, Haydon H, Mehrotra A, Clemensen J, et al. Telehealth for global emergencies: implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. (2020) 26:309–13. doi: 10.1177/1357633X20916567
5. Custodero C, Senesi B, Pinna A, Floris A, Vigo M, Fama M, et al. Validation and implementation of telephone-administered version of the Multidimensional Prognostic Index (TELE-MPI) for remote monitoring of community-dwelling older adults. Aging Clin Exp Res. (2021) 33:3363–9. doi: 10.1007/s40520-021-01871-6
6. Hassan TA, Sáenz JE, Ducinskiene D, Cook JP, Imperato JS, Zou KH. New strategies to improve patient adherence to medications for noncommunicable diseases during and after the COVID-19 era identified via a literature review. J Multidiscip Healthc. (2021) 14:2453. doi: 10.2147/JMDH.S313626
7. Bokolo AJ. Use of telemedicine and virtual care for remote treatment in response to COVID-19 pandemic. J Med Syst. (2020) 44:132. doi: 10.1007/s10916-020-01596-5
8. Li HL, Chan YC, Huang JX, Cheng SW. Pilot study using telemedicine video consultation for vascular patients' care during the COVID-19 period. Ann Vasc Surg. (2020) 68:76–82. doi: 10.1016/j.avsg.2020.06.023
9. Li P, Liu X, Mason E, Hu G, Zhou Y, Li W, et al. How telemedicine integrated into China's anti-COVID-19 strategies: case from a national referral center. BMJ Health Care Inform. (2020) 27:e100164. doi: 10.1136/bmjhci-2020-100164
10. Macinko J, Woolley NO, Seixas BV, Andrade FB, Lima-Costa MF. Health care seeking due to COVID-19 related symptoms and health care cancellations among older Brazilian adults: the ELSI-COVID-19 initiative. Cad Saúde Pública. (2020) 36 (Suppl. 3):e00181920 doi: 10.1590/0102-311x00181920
11. Omboni S, McManus RJ, Bosworth HB, Chappell LC, Green BB, Kario K, et al. Evidence and recommendations on the use of telemedicine for the management of arterial hypertension: an international expert position paper. Hypertension. (2020) 76:1368–83. doi: 10.1161/HYPERTENSIONAHA.120.15873
12. Doraiswamy S, Jithesh A, Mamtani R, Abraham A, Cheema S. Telehealth use in geriatrics care during the COVID-19 pandemic—a scoping review and evidence synthesis. Int J Environ Res Public Health. (2021) 18:1755. doi: 10.3390/ijerph18041755
13. Bhaskar S, Bradley S, Chattu VK, Adisesh A, Nurtazina A, Kyrykbayeva S, et al. Telemedicine as the new outpatient clinic gone digital: position paper from the pandemic health system resilience program (REPROGRAM) International Consortium (Part 2). Frontiers in Public Health. (2020) 8:410. doi: 10.3389/fpubh.2020.00410
14. Bonanad C, García-Blas S, Tarazona-Santabalbina F, Sanchis J, Bertomeu-González V, Fácila L, et al. The effect of age on mortality in patients with COVID-19: a meta-analysis with 611,583 subjects. J Am Med Dir Assoc. (2020) 21:915–8. doi: 10.1016/j.jamda.2020.05.045
15. Kang SJ, Jung SI. Age-related morbidity and mortality among patients with COVID-19. Infect Chemother. (2020) 52:154–64. doi: 10.3947/ic.2020.52.2.154
16. Owen RK, Conroy SP, Taub N, Jones W, Bryden D, Pareek M, et al. Comparing associations between frailty and mortality in hospitalized older adults with or without COVID-19 infection: a retrospective observational study using electronic health records. Age Ageing. (2021) 50:307–16. doi: 10.1093/ageing/afaa167
17. Sanyaolu A, Okorie C, Marinkovic A, Patidar R, Younis K, Desai P, et al. Comorbidity and its impact on patients with COVID-19. SN Compr Clin Med. (2020) 2:1069–76. doi: 10.1007/s42399-020-00363-4
18. Eurostat. Population structure indicators at national level: Share of population in a certain age group compared to the total population (2022). Available online at: https://ec.europa.eu/eurostat/databrowser/product/view/DEMO_PJANIND (accessed January 6, 2022).
19. Smolić Š, Čipin I, Međimurec P. Access to healthcare for people aged 50+ in Europe during the COVID-19 outbreak. Eur J Ageing. (2021). doi: 10.1007/s10433-021-00631-9
20. Atzendorf J, Gruber S. Depression and loneliness of older adults in Europe and Israel after the first wave of covid-19. Eur J Ageing. (2021). doi: 10.1007/s10433-021-00640-8
21. Douglas M, Katikireddi SV, Taulbut M, McKee M, McCartney G. Mitigating the wider health effects of covid-19 pandemic response. BMJ. (2020) 369:m1557. doi: 10.1136/bmj.m1557
22. Hong Z, Li N, Li D, Li J, Li B, Xiong W, et al. Telemedicine during the COVID-19 pandemic: experiences from Western China. J Med Internet Res. (2020) 22:e19577. doi: 10.2196/19577
23. Song X, Liu X, Wang C. The role of telemedicine during the COVID-19 epidemic in China—experience from Shandong province. Crit Care. (2020) 24:178. doi: 10.1186/s13054-020-02884-9
24. Bidmead E, Marshall A. Covid-19 and the ‘new normal': are remote video consultations here to stay? Br Med Bull. (2020) 135:16–22. doi: 10.1093/bmb/ldaa025
25. Webster P. Virtual health care in the era of COVID-19. Lancet. (2020) 395:1180–1. doi: 10.1016/S0140-6736(20)30818-7
26. Hollander JE, Carr BG. Virtually perfect? Telemedicine for COVID-19. N Engl J Med. (2020) 382:1679–81. doi: 10.1056/NEJMp2003539
27. Kadir MA. Role of telemedicine in healthcare during COVID-19 pandemic in developing countries. Telehealth Med Today. (2020) 5. doi: 10.30953/tmt.v5.187
28. Bhaskar S, Bradley S, Chattu VK, Adisesh A, Nurtazina A, Kyrykbayeva S, et al. Telemedicine as the new outpatient clinic gone digital: position paper from the pandemic health system resilience program (REPROGRAM) International Consortium (Part 1). Front Public Health. (2020) 8:644. doi: 10.3389/fpubh.2020.556720
29. European Observatory on Health Systems and Policies, Richardson E, Aissat D, Williams GA, Fahy N. Keeping what works: remote consultations during the COVID-19 pandemic. Eurohealth. (2020) 26:73−6. World Health Organization. Regional Office for Europe. Available online at: http://www.apps.who.int/iris/handle/10665/336301 (accessed March 12, 2022).
30. Peine A, Paffenholz P, Martin L, Dohmen S, Marx G, Loosen SH. Telemedicine in Germany during the COVID-19 pandemic: multi-professional national survey. J Med Internet Res. (2020) 22:19745. doi: 10.2196/19745
31. Ohannessian R, Duong TA, Odone A. Global telemedicine implementation and integration within health systems to fight the COVID-19 pandemic: a call to action. JMIR Public Health Surveill. (2020) 6:e18810. doi: 10.2196/18810
32. Omboni S. Telemedicine during the COVID-19 in Italy: a missed opportunity? Telemed E-Health. (2020) 26:973–5. doi: 10.1089/tmj.2020.0106
33. Joy M, McGagh D, Jones N, Liyanage H, Sherlock J, Parimalanathan V, et al. Reorganization of primary care for older adults during COVID-19: a cross-sectional database study in the UK. Br J Gen Pract. (2020) 70:e540–7. doi: 10.3399/bjgp20X710933
34. Parisien RL, Shin M, Constant M, Saltzman BM, Li X, Levine WN, et al. Telehealth utilization in response to the novel coronavirus (COVID-19) pandemic in orthopaedic surgery. J Am Acad Orthop Surg. (2020) 28:e487–92. doi: 10.5435/JAAOS-D-20-00339
35. Kunonga TP, Spiers GF, Beyer FR, Hanratty B, Boulton E, Hall A, et al. Effects of Digital technologies on older people's access to health and social care: umbrella review. J Med Internet Res. (2021) 23:e25887. doi: 10.2196/25887
36. Liu L, Goodarzi Z, Jones A, Posno R, Straus SE, Watt JA. Factors associated with virtual care access in older adults: a cross-sectional study. Age Ageing. (2021) 50:1412–15. doi: 10.1093/ageing/afab021
37. Murphy M, Scott LJ, Salisbury C, Turner A, Scott A, Denholm R, et al. Implementation of remote consulting in UK primary care following the COVID-19 pandemic: a mixed-methods longitudinal study. Br J Gen Pract. (2021) 71:e166–77. doi: 10.3399/BJGP.2020.0948
38. Khan N, Jones D, Grice A, Alderson S, Bradley S, Carder P, et al. A brave new world: the new normal for general practice after the COVID-19 pandemic. BJGP Open. (2020) 4:bjgpopen20X101103. doi: 10.3399/bjgpopen20X101103
39. Gareri P, Fumagalli S, Malara A, Mossello E, Trevisan C, Volpato S, et al. Management of older outpatients during the COVID-19 pandemic: the GeroCovid ambulatory study. Gerontology. (2021) 28:1–6. doi: 10.1159/000516969
40. Horrell LN, Hayes S, Herbert LB, MacTurk K, Lawhon L, Valle CG, et al. Telemedicine use and health-related concerns of patients with chronic conditions during COVID-19: survey of members of online health communities. J Med Internet Res. (2021) 23:e23795. doi: 10.2196/23795
41. Kontos E, Blake KD, Chou WY, Prestin A. Predictors of eHealth usage: insights on the digital divide from the Health Information National Trends survey 2012. J Med Internet Res. (2014) 16:e3117. doi: 10.2196/jmir.3117
42. Li P, Luo Y, Yu X, Wen J, Mason E, Li W, et al. Patients' perceptions of barriers and facilitators to the adoption of E-hospitals: cross-sectional study in Western China. J Med Internet Res. (2020) 22:e17221. doi: 10.2196/17221
43. Patel SY, Mehrotra A, Huskamp HA, Uscher-Pines L, Ganguli I, Barnett ML. Trends in outpatient care delivery and telemedicine during the COVID-19 pandemic in the US. JAMA Intern Med. (2021) 181:388. doi: 10.1001/jamainternmed.2020.5928
44. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 8 COVID-19 Survey. Release version: 8.0.0 SHARE-ERIC Data set. Munich. (2022). doi: 10.6103/SHARE.w8ca.800
45. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 9 COVID-19 Survey. Release version: 8.0.0 SHARE-ERIC Data set. Munich. (2022). doi: 10.6103/SHARE.w9ca.800
46. Bergmann M, Scherpenzeel A, Börsch-Supan A. SHARE Wave 7 Methodology: Panel Innovations and Life Histories. Munich: Munich Center for the Economics of Aging (MEA). (2019).
47. Börsch-Supan A, Brandt M, Hunkler C, Kneip T, Korbmacher J, Malter F, et al. Data resource profile: the survey of health, ageing and retirement in Europe (SHARE). Int J Epidemiol. (2013) 42:992–1001. doi: 10.1093/ije/dyt088
48. Malter F, Börsch-Supan A. SHARE Wave 6: Panel innovations and collecting Dried Blood Spots. Munich: Munich Center for the Economics of Aging (MEA). (2017).
49. Scherpenzeel A, Axt K, Bergmann M, Douhou S, Oepen A, Sand G, et al. Collecting survey data among the 50+ population during the COVID-19 outbreak: the Survey of Health, Ageing and Retirement in Europe (SHARE). Surv Res Methods. (2020) 14:217–21. doi: 10.18148/srm/2020.v14i2.7738
50. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 1. Release version: 8.0.0 SHARE-ERIC Data set. (2022). doi: 10.6103/SHARE.w1.800
51. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 2. Release version: 8.0.0 SHARE-ERIC Data set. (2022). doi: 10.6103/SHARE.w2.800
52. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 3. Release version: 8.0.0 SHARE-ERIC Data set. (2022). doi: 10.6103/SHARE.w3.800
53. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 4. Release version: 8.0.0 SHARE-ERIC Data set. (2022). doi: 10.6103/SHARE.w4.800
54. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 5. Release version: 8.0.0 SHARE-ERIC Data set. (2022). doi: 10.6103/SHARE.w5.800
55. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 6. Release version: 8.0.0 SHARE-ERIC Data set. (2022). doi: 10.6103/SHARE.w6.800
56. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 7. Release version: 8.0.0 SHARE-ERIC Data set. (2022). doi: 10.6103/SHARE.w7.800
57. Börsch-Supan A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 8. Release version: 8.0.0 SHARE-ERIC Data set. (2022). doi: 10.6103/SHARE.w8.800
58. Arnault L, Jusot F, Renaud T. Economic vulnerability and unmet healthcare needs among the population aged 50+ years during the COVID-19 pandemic in Europe. Eur J Ageing. (2021) 5:1–15. doi: 10.1007/s10433-021-00645-3
59. Daoust JF. Elderly people and responses to COVID-19 in 27 Countries. PLoS ONE. (2020) 15:e0235590. doi: 10.1371/journal.pone.0235590
60. Jang S, Kim CO. Care Inequality among older adults during the COVID-19 pandemic. Ann Geriatr Med Res. (2020) 24:229–31. doi: 10.4235/agmr.20.0096
61. Holaday LW, Oladele CR, Miller SM, Dueñas MI, Roy B, Ross JS. Loneliness, sadness, and feelings of social disconnection in older adults during the COVID−19 pandemic. J Am Geriatr Soc. (2021) 70:329–40. doi: 10.1111/jgs.17599
62. Ortega G, Rodriguez JA, Maurer LR, Witt EE, Perez N, Reich A, et al. Telemedicine, COVID-19, and disparities: policy implications. Health Policy Technol. (2020) 9:368–71. doi: 10.1016/j.hlpt.2020.08.001
63. Kolitsi Z, Kalra D, Wilson P, Martins H, Stroetmann V, Schulz C, et al. DigitalHealthEurope recommendations on the European Health Data Space. (2021). Available online at: https://digitalhealtheurope.eu/wp-content/uploads/DHE_recommendations_on_EHDS_July_2021.pdf (accessed March 19, 2022).
64. European Commission. Green Paper on Ageing: Fostering Solidarity Responsibility between Generations. (2021). Available online at: https://ec.europa.eu/info/sites/default/files/1_en_act_part1_v8_0.pdf (accessed March 19, 2022).
Keywords: SHARE Corona Survey, older adults, remote medical consultations, COVID-19, health expenditures, unmet healthcare
Citation: Smolić Š, Blaževski N and Fabijančić M (2022) Remote Healthcare During the COVID-19 Pandemic: Findings for Older Adults in 27 European Countries and Israel. Front. Public Health 10:921379. doi: 10.3389/fpubh.2022.921379
Received: 15 April 2022; Accepted: 15 June 2022;
Published: 15 July 2022.
Edited by:
Anthony Bokolo Jr., Institute for Energy Technology, NorwayReviewed by:
Getaneh Baye Mulu, Debre Berhan University, EthiopiaDan Morgenstern-Kaplan, Anahuac University of North Mexico, Mexico
Alma Nurtazina, Semey State Medical University, Kazakhstan
Copyright © 2022 Smolić, Blaževski and Fabijančić. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Šime Smolić, c3Ntb2xpY0BlZnpnLmhy