 Debbie L. Humphries
Debbie L. Humphries Michelle Sodipo
Michelle Sodipo Skyler D. Jackson
Skyler D. Jackson- 1Yale School of Public Health, New Haven, CT, United States
- 2Harvard T.H. Chan School of Public Health, Cambridge, MA, United States
Few guidelines exist for the development of socially responsible health policy, and frameworks that balance considerations of data, strategy, and equity are limited. The Intersectionality-Based Policy Analysis (IBPA) framework utilizes a structured questioning process to consider problems and policies, while applying guiding principles of equity, social justice, power, intersectionality, and diversity of knowledge and input. We apply the IBPA framework’s guiding principles and questions to the pre-vaccine U.S. COVID-19 policy response. Results suggest the IBPA approach is a promising tool for integrating equity considerations in the development of policy solutions to urgent US public health challenges, including the COVID-19 pandemic. We found the IBPA framework particularly useful in differentiating between problems or policies and representations of problems or policies, and in considering the impacts of representations on different groups. The explicit inclusion of short-, medium- and long-term solutions is a reminder of the importance of holding a long-term vision of the equitable public health system we want while working towards immediate change.
Introduction
The field of public health, with its responsibility to protect and care for the public’s health, is routinely involved in policies affecting economics and health. The history of public policies in the U.S. includes stunning successes such as public health efforts to ban smoking in public places, and the widespread availability of potable water and safe sanitation (1, 2). However, public health’s track record also includes policy initiatives with mixed impacts on health and wellness, and policies with negative impacts on public health.
Given the regular conflicts between economic and health interests in the field of public health, particularly in countries such as the U.S. with highly privatized healthcare systems, regular reflective analysis of impacts of public health policies is essential (3). With strong economic pressures on public health policy, frameworks for policy review are needed that can help to highlight potential challenges while explicitly incorporating values of equity, intersectionality, multiple time frames and diverse perspectives. While the field of public health has its own understanding of ethics and social responsibility (4, 5) there is a need for a policy analysis approach that incorporates values and additional perspectives throughout the process to strengthen what public health systems deliver.
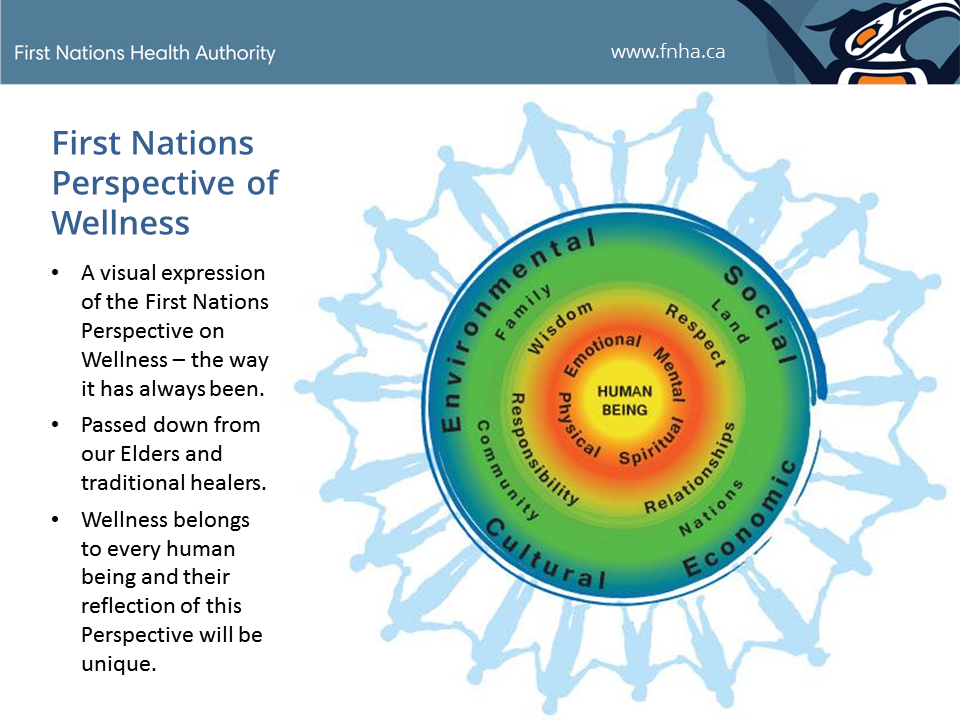
The World Health Organization (WHO) has defined health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”, (6) and this definition is widely used internationally. A more recent model proposed by the First Nations Health Authority (FNHA) in Canada, uses a wellness framing, with human beings nested in circles representing (1) the individual, (2) the components of wellness (e.g., spiritual, mental), (3) values that support wellness (e.g., respect, wisdom), (4) the people and places around us that are important for our wellness (e.g., family, land), (5) the social, cultural, economic and environmental determinants of health and well-being, and (6) the people who stand together representing our communities (Figure 1) (7). The FNHA wellness model makes explicit contextual elements essential for health and wellness that are not visible in the WHO definition. The values that support wellness, and the importance of the people and places around us, highlight the multidirectional relationships essential for holistic wellness.
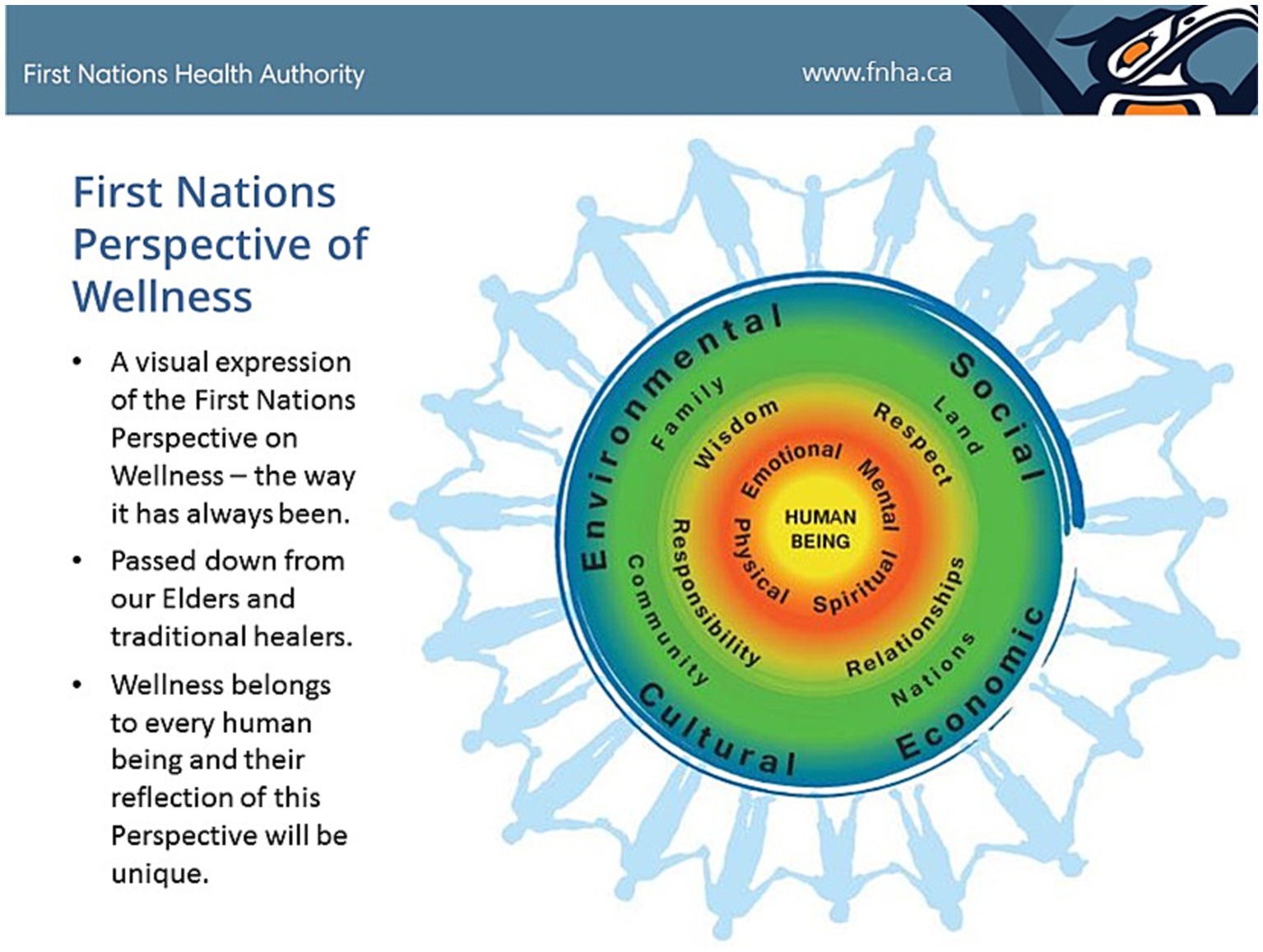
Figure 1. The First Nations Perspective on Health and Wellness aims to visually depict and describe the First Nations Health Authority Vision: Healthy, Self-Determining and Vibrant BC First Nations Children, Families and Communities. https://creativelyunited.org/wp-content/uploads/2019/06/FNPOW.png (7) (Used with permission of the First Nations Health Authority).
{kind=link}
While we might hope for wellness as envisioned in the FNHA approach, an analysis of actual policies provides a lens into what political leaders can deliver. Although public health policies have played a key role in increasing life expectancy and quality of life in the U.S. over the last century, (8, 9) few frameworks have been developed to guide the development of public health responses that are both strategic and data-informed, and also socially humane and equitable. There is a growing awareness of the importance of integrating values such as equity into public health planning, (10) growing out of the documented disparities in health outcomes by race, ethnicity, gender, sexual orientation, and economics (11).
In seeking to understand how varied experiences affect perspectives and experience, the term “Intersectionality” has come into usage to describe the ways systems of power—such as race, gender, sexual orientation, class, and other individual characteristics—intersect to co-construct and constrain individuals’ life possibilities. Intersectional approaches highlight the compounded risks and synergistic disparities experienced by individuals impacted by multiple forces of oppression. In outlining the various ways intersectionality can inform public health crises, scholars have noted that intersectionality has disproportionately been engaged as a theoretical framework and analytical tool. Rarely has the framework been utilized in a manner that embodies intersectionality praxis, “the practical application of intersectionality to facilitate equitable health policy and practice for intersectionally marginalized groups, (…) and arguably most essential wave to address the public health crises of our time” (12). Indeed, even as intersectionality has risen in popularity within recent decades, few studies go beyond disaggregating results by subgroups to truly examine the ways systems of power interlock to mutually construct public health outcomes. Even fewer healthcare frameworks exist that embody and advance intersectionality praxis (13).
Although frameworks have emerged to guide health practice, (14) investigations that operationalize intersectionality to analyze and guide current public health policy are scant. One such example includes the work of Hunting (15), who used an Intersectionality-based Policy Analysis (IBPA) to assess Canada’s health policy concerning fetal alcohol spectrum disorders. Due to its attention to intersectionality, this study uncovered the ways that the gender and colonial processes interlocked to shape policy and harm Aboriginal women. Fagrell Trygg et al. (16) combined a post-structural policy analysis approach with the framework of intersectionality to analyze a government bill proposing a national strategy on substance misuse and problematic gambling. Adopting an intersectional lens produced wariness regarding the adoption of unidimensional population groups (e.g., women), due to an awareness of different health risks and needs within such groups based on other axes of privilege and oppression (e.g., non-immigrant upper-class women vs. immigrant working class women). These works demonstrate the power of intersectionality-based approaches, especially in their ability to describe how interlocking systems of power create different health outcomes for different groups and also to illuminate the underlying mechanisms (e.g., social processes, structural factors, and policy-decisions) that drive and maintain inequities during times of crisis.
The intersectionality-based policy analysis framework
The Intersectionality-based Policy Analysis (IBPA) framework, developed by Hankivsky and colleagues, utilizes a structured questioning process to consider problems and policy approaches while applying eight guiding principles (17). We offer here an application of the IBPA framework to the early COVID-19 pandemic in the context of racial strife and reconciliation in the U.S., as an example of how the framework can be used to illuminate short, medium and long term solutions to complex problems by addressing both immediate and systemic levers for change. We selected this framework based upon the ways it invites participatory reflection and questioning, with open-ended questions and responses. We were also attracted to the explicit focus on integrating principles of equity, social justice and power throughout the analysis process; such values and areas of emphasis are lacking from most frameworks for policy review. In addition, the IBPA is focused on identifying feasible short, medium and long term solutions, which emphasizes the practical and applied potential impacts of this framework. Finally, as discussed below, COVID-19 related disparities have emerged across various dimensions of inequality (e.g., race/ethnicity, socioeconomic status, gender, sexual orientation, and disability status), including their intersections. Thus, we felt that the IBPA framework might help excavate intersectional problems and solutions that would remain obscured with a framework not explicitly calling out intersectionality.
Unpacking the IBPA framework
The IBPA framework combines eight guiding principles with twelve guiding questions (Figure 2). The eight guiding principles (e.g., power, reflexivity, and intersecting categories) identify values to apply when addressing the questions. The separate series of questions are divided into two categories, descriptive and transformative. Descriptive questions center around ways the policy problem has been described. From there the process shifts to the transformative questions, delving deeper into reframing and explicitly integrating the guiding principles with questions of differential experiences and impacts to reshape understanding and approaches to identify potential solutions. Solutions are then assessed for how they address the roots of disparities and social determinants of health.
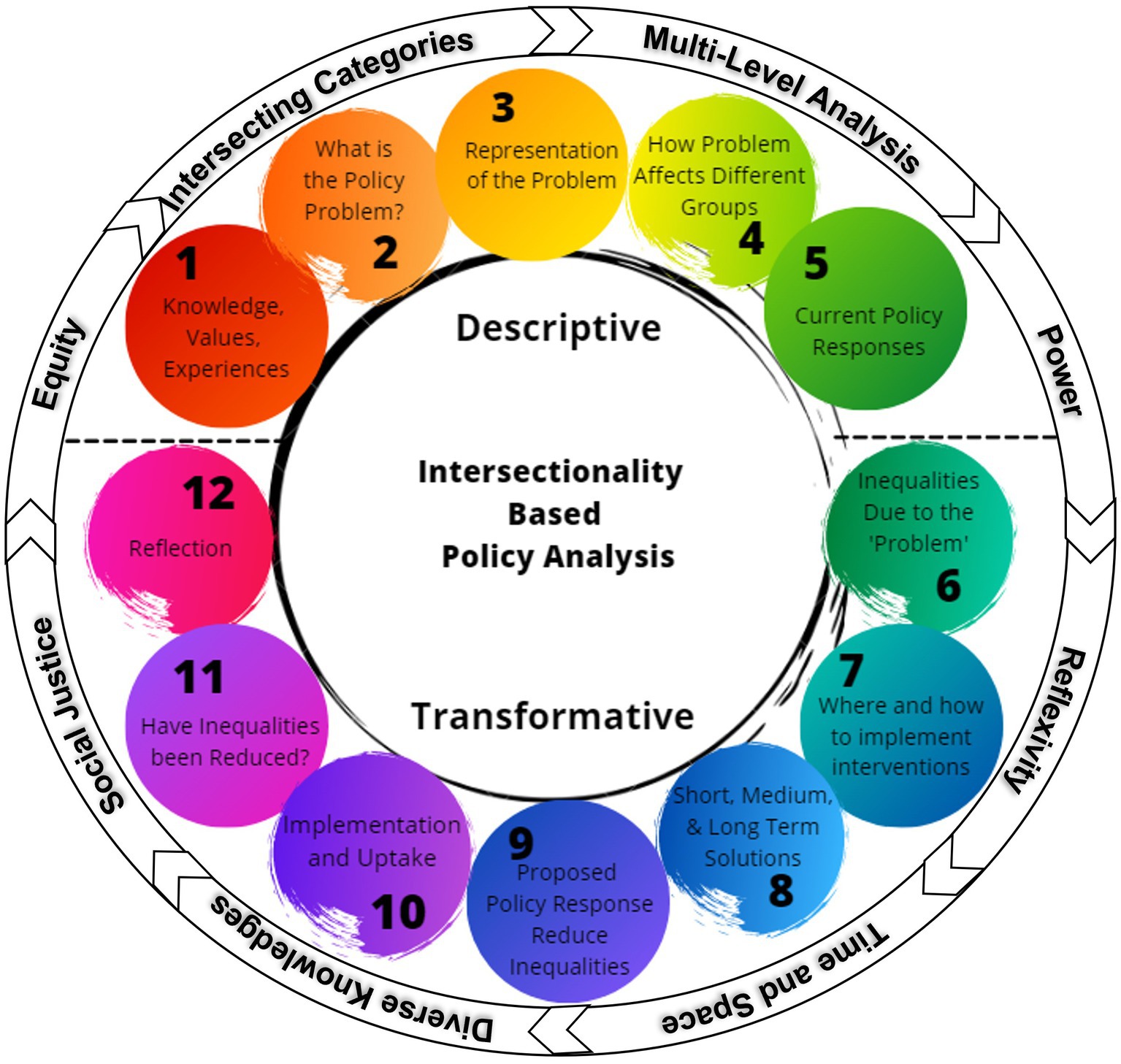
Figure 2. The components of the Intersectionality-based Policy Analysis Framework, including the five descriptive questions, seven transformative questions, and the eight guiding principles that encircle all of the questions (submitting for creative commons licensing).
To ensure all questions are framed in a way that is congruent with the eight guiding principles, teams utilizing the IBPA framework are encouraged to consider each principle when responding to the twelve guiding questions (Table 1). The two sets of questions, together with the application of the guiding principles, create a novel lens for assessing policy solutions to increase policy impact (17). The structured analytical approach provides an important tool for assessing the impacts of public health policy.
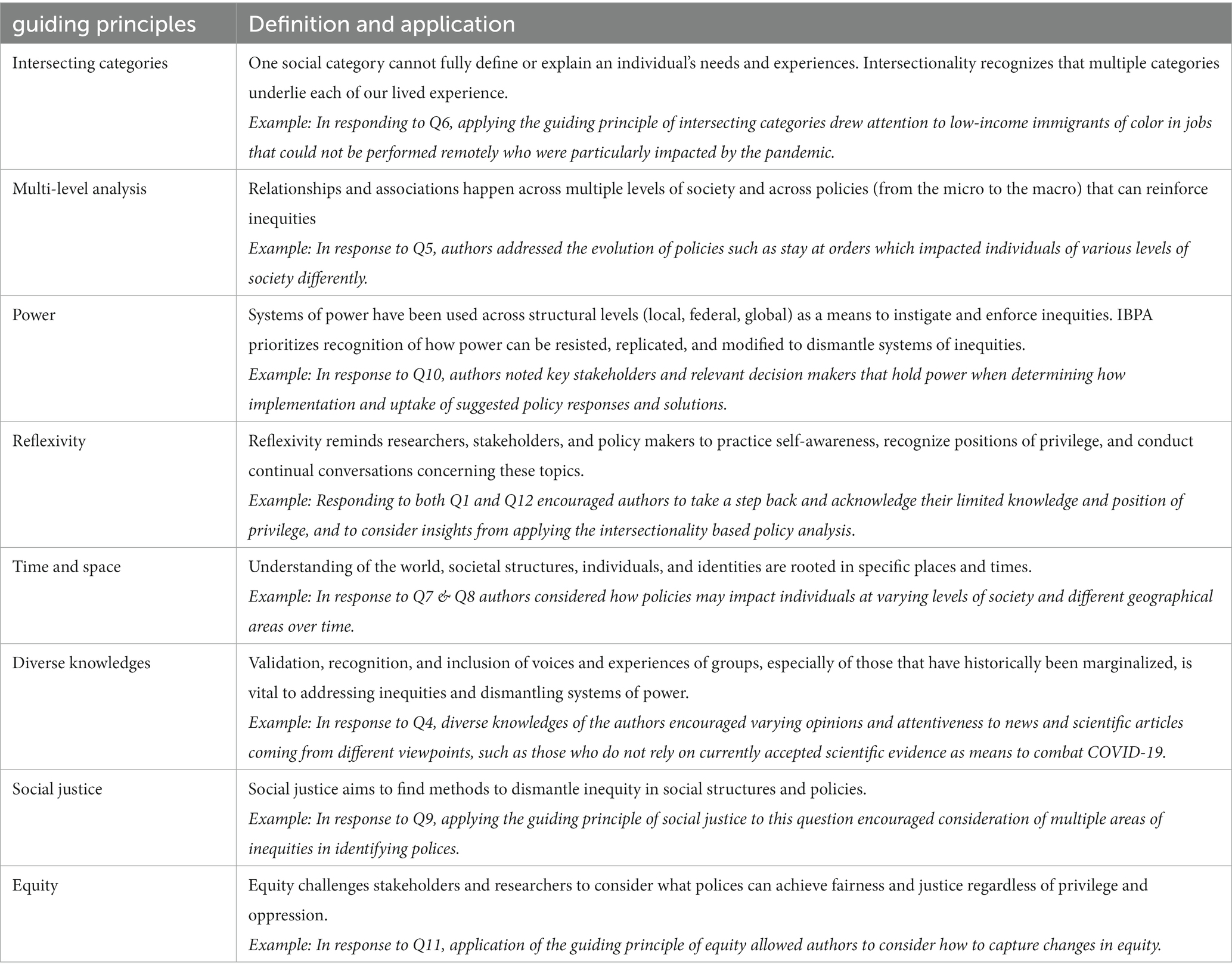
Table 1. Guiding Principles for IBPA [adapted from Hankivsky (18)].
The emergence of a new global pandemic
In late December 2019 reports of a rapidly spreading new coronavirus came out of Wuhan, China. By March 2020 much of the world had restricted travel and human movement to contain the spread of COVID-19. Efforts to curtail the spread had limited success: By December 2020, infections were present in every country, over 83.6 million individuals had tested positive, and more than 1.8 million deaths were attributed to the pandemic globally (7). The U.S. rate of COVID-19 infections was among the worst in the world, with a rate of confirmed infections (>100,000/1 M) in May 2021 that was 11th highest in the world (8). This failure of the U.S. public health system highlights the importance of careful analysis of the U.S. response to the pandemic.
Health disparities in COVID-19
The emergence of COVID-19 had differential effects on the US public based on multiple power-laden demographic factors such as race/ethnicity, gender, socio economic status, sexual orientation, and other dimension of power (13, 19–22). As these systems of power have the ability to compound and interact, public health scholars have called for the greater application of intersectionality to advance equitable policy, surveillance, and intervention related the COVID-19 pandemic (23–25). Further, research has begun to illuminate ways multiple forms of oppression compounded and interlocked to drive unique COVID-related health needs, barriers, and outcomes among multiply-marginalized populations (26–29).
The COVID-19 pandemic was not unrelated to the racial crisis within the U.S. (30). Indeed, early on within the pandemic, it became clear that each of the key health outcomes (e.g., infections, hospitalizations, and deaths) mirrored larger trends within U.S. health disparities, with people of color carrying a disproportionate burden. Second, on May 25, 2020, amidst the ongoing COVID pandemic, a White police officer, Derek Chauvin, knelt for 9 min and 29 s on the neck of George Floyd, a Black man, while he struggled to breathe. George Floyd was killed, and the cellphone recording of his death galvanized communities and individuals around the U.S. Rallies took place in hundreds of communities, as millions marched to say that Black lives in the U.S. have been disregarded for centuries. The death of George Floyd, and the movement growing out of it, highlighted the disparate experiences of White and Black individuals within American institutions, including the health care system.
This article utilizes the shared experience of the COVID-19 pandemic from March to November 20201 to assess the utility of the IBPA for public health policy analysis. While the focus of the article is the IBPA framework and process, the article applies the IBPA framework and an intersectional lens to the COVID-19 pandemic to determine whether this approach might provide additional insights into the dramatic policy failures that led to >400,000 Americans dying in the first year of the pandemic.
Methods
Application of the IBPA framework
The framework was used as a logical structure for evaluating the March–November 2020 COVID-19 responses of the U.S. local, regional, state and national governments charged with public health services and protections. Responses to the pandemic were identified from real time news reports as well as World Health Organization and Centers for Disease Control updates. We drafted and revised responses to each of the twelve questions and sought feedback from colleagues, expanding responses as needed to apply the IBPA framework and capture possible responses around the COVID-19 pandemic. We therefore added an additional question 5a (how are policy responses represented in media and public statements), as our discussions brought to light the importance of explicitly noting the role of the media in politicizing policy responses. With repeated feedback and critical reflection, responses to each question within the framework were developed, clarified, and refined.
Results of the analysis
The COVID-19 pandemic provides a useful example of what happens when there are widely divergent representations of a policy problem. By differentiating between a policy problem (e.g., high rates of COVID transmission within the US) and subjective representations of a problem (e.g., COVID is a hoax) the IBPA provides useful insights into how framing influences and shapes policy responses. By adopting an intersectional lens more nuanced policy considerations and options emerged. Here we consider the process and experience of responding to the questions and particularly the guiding principles brought to bear on the process.
While we provide examples of how specific components of the IBPA can be applied (Tables 1, 2), in the results we focus on the process of completing the IBPA.
Table 2. Application of the Intersectionality-based Policy Analysis framework to the COVID-19 pandemic.
Guiding principles
The team drew on each of the eight guiding principles in completing the IBPA. Table 1 gives illustrative examples of how the guiding principles informed the process. For example, in considering the principle of reflexivity the authors named their own positions of privilege and identified limits to their own knowledge in responding to the questions.
Descriptive questions
After reflecting on the knowledge, values and experiences the authors bring to this area (Q1), we developed a concise statement of the problem “Slowing/controlling transmission of a highly contagious infectious disease transmitted through respiratory, aerosol and contact routes by asymptomatic and symptomatic carriers” (Q2). This definition highlighted the policy challenge, slowing transmission, based on what was known early on about the virus (See Table 2A).
In considering Q3 (“How have representations of the problem come about?”), we were struck by four different elements of how the problem is presented: who is at risk? how serious is the risk? what policy options are possible or appropriate? and what data is available and trusted to draw conclusions about the problem? These areas arose as we applied the principles of equity, power and social justice to the question concerning different representations of the problem. In each of these areas the response highlights the absence of a definitive U.S. statement, and dramatic variation in representations of risk. Based on representations of who is at risk, different stakeholders, together with different states, counties, and cities, proposed varied policy responses (Q4). Underlying the different representations are different political perspectives and reliance on different data about the emerging and ongoing pandemic.
After looking at differential impacts of the representations of the problem, questions four and five encourage a close look at the spectrum of impacts, and the ways the representations of the problem (e.g., risk to travelers from China, risk to older adults, just a mild flu) impacted behaviors and practices in the general public and in the health system (e.g., who could get tested, what personal protective practices were recommended, and what civil policies were enforced on masking). An additional consideration included how media and statements by public officials represented the varied policy responses.
Transformative questions
The transformative questions are designed to incorporate longer-term social and structural determinants into the analysis, encouraging consideration of how longer-term factors may be affecting the situation and how policy options could simultaneously address root causes of disparities (see Table 2B).
By drawing out disparities with respect to the policy problem, Q6 (“What inequalities actually exist in relation to the ‘problem’?”) encourages a breadth of reflections. We considered inequalities across the life cycle of an infection, through the stages of exposure, susceptibility, access to care, response to treatment and further transmission, and disparities in background health conditions that have been observed to increase risk of serious disease. At every stage there were multiple, intersecting psychosocial, behavioral and biological factors affecting compliance with recommended protective behaviors. These include mistrust of health care professionals, history of discrimination leading to lower economic resources, poor nutritional status and greater immunological susceptibility, and cultural differences in households such that individuals living in multigenerational households were at increased risk of transmission when compared with individuals living alone. Utilizing the wide-angle intersectional lens helped to highlight the importance of different household and family structures for transmission and risk, and the need to develop flexible policy responses that address the spectrum of needs.
Q7 [“Where and how can (immediate) interventions be made to improve the problem?”] identifies immediate interventions while considering the guiding principles. We found the guiding principles of multi-level analysis, social justice and intersecting categories to be particularly relevant, as these principles ensure that efforts taken to achieve a larger policy goal do not simultaneously exacerbate existing disparities. Some of the interventions suggested (see Table 2B) were under local or private control, impacting businesses, schools, institutions or municipalities, while other interventions such as testing and contact tracing might involve coordination across multiple governmental levels.
Q8 (“What are feasible short-, medium- and long-term solutions”) builds on Q7, encouraging thoughtful consideration of short-, medium- and long-term solutions. The distinction between immediate interventions in Q7 and short-, medium- and long-term solutions in Q8 emphasizes integrating long term systems change solutions that can incorporate respect for diverse knowledges, reflexivity, time and space. These values are reflected in our response to Q8, where we suggest that consideration of the objectives of the public health system in the U.S. are needed to identify and implement long term solutions to problems such as COVID-19. Suggestions for long term solutions are quite broad, including changes needed in educational systems, how evidence is generated in medicine and public health, and improving infection control requirements within care facilities.
Q9 (“How will proposed policy responses reduce inequities?”) asks for the evidence that the proposed solutions in response to Q8 will reduce inequities. We have identified existing evidence suggesting connections between the proposed solutions and redressing inequities, while also encouraging ongoing assessment. This includes the assessment of our previously identified solutions. We chose to include some innovative approaches that may not yet have generated evidence of their ability to address inequities, given the importance of innovative approaches to address inequities.
Q10 (“How will implementation and uptake be assumed?”) focuses on implementation and uptake, highlighting that without thoughtful implementation plans solutions are rarely effective. Our response notes the importance of individualized road maps for different solutions that will need buy-in from leadership and policy makers across sectors and levels.
Q11 (“How will you know if inequalities have been reduced?”) builds on Q9, seeking identification of clear markers of existing inequities and ways to monitor changes. Reductions in disparities along the COVID-19 continuum (e.g., transmissions, hospitalizations, and deaths) would highlight the effectiveness of the policy proposals.
Q12 (“How has the process of engaging in an IBPA transformed: your thinking about relation and structures of power and inequity; the ways in which you and others engage in the work of policy development, implementation and evaluation; broader conceptualizations, relations and effects of power asymmetry in the everyday world?”) is a capstone question demanding detailed and systemic analysis. Participants are invited into a broader reflection of how the process has transformed ideas and thinking. For example, our experience provided reinforcement of the tight connections between structural disparities in the economic, education and health care systems with the disparities in health outcomes.
Discussion
Since the onset of the COVID-19 pandemic numerous articles have been written about the differential intersectional impacts of the pandemic (21, 22, 26, 27). Authors have highlighted differences in outcomes by intersectional dimensions such as sexual orientation, (22, 27), race/ethnicity (21, 22, 26, 27), and gender (21). However, few have used a full intersectional approach as recommended by Maestripieri, bringing the lenses of age, race/ethnicity, gender, sexual orientation, and socioeconomic status/class to analysis of impacts of the COVID-19 pandemic (24). In addition, research is focused on what Bowleg calls the third wave of intersectionality, analysis of intersectional issues, with few articles moving beyond analysis of impacts to Bowleg’s fourth wave, of intersectional praxis (12). While some studies include suggestions for intersectional praxis, with intersectionality informed recovery strategies (21) and COVID-19 vaccine distribution plans, (28) this article provides a unique example of a praxis-focused analysis that can be brought to bear across the full spectrum of intersectional concerns and can be applied to many program and policy issues.
Our analysis used the IBPA approach to unpack the early U.S. response to the COVID-19 pandemic to assess what insights this approach might give into the dramatic policy failures that led to more than one million Americans dying over the three years of the pandemic (41). Our iterative engagement with the framework’s structured questions and guiding principles raised considerations and stimulated ideas that otherwise may have remained obscured. This illustrative test of the framework’s utility in developing humane, data-driven solutions to contemporary public health problems can serve as a guide for other researchers and policy makers who are interested in using this framework to improve health outcomes.
The detailed questions and guiding principles of the IBPA framework invite identification of upstream drivers of disparities and a long-term perspective, with identification of feasible short-, medium- and long-term solutions (Q8). The wide-angle lens invites consideration of the broader nested influences such as in the FNHA wellness model (Figure 1). That broader perspective, in combination with the guiding principles of equity, social justice and diverse knowledges, highlighted structural (e.g., socioeconomic class differences in employer-provided health insurance, sick leave and other workplace policies), social (e.g., medical mistrust among communities of color), and environmental (e.g., habitat destruction) determinants and modifiers of policy and health impacts.
The strengths of the IBPA include the direct questions in combination with the guiding principles, as well as flexibility in the identification of questions most relevant in particular policy analyses. For example, the differentiation between the myriad representations of the problem and the actual problem enabled thoughtful considerations of the importance of media representations in addressing solutions. The framework requires consideration of evidence and data (e.g., asking for the existing evidence that the proposed solutions will work) without sacrificing attention to equity and fairness (e.g., asking how groups are differentially affected). This multidimensional focus is more likely to generate recommendations that harmonize science, strategy, and social justice to inform health policy. This process also lends itself to inclusion of a diverse group of participants, and inclusion of diverse stakeholders is important to capture a rich combination of policy responses.
We see the IBPA framework as a highly relevant tool for intersectional praxis (42). Identifying drivers of policy problems and modifiers of policy impacts. The IBPA framework and process is a useful tool for reimagining public health in light of the COVID-19 pandemic as researchers have called for (43). This framework can be implemented across a range of policy levels, from an organizational analysis to a governmental analysis. The IBPA framework was particularly useful in differentiating between actual problems or policies and how the problem or policy is being represented, along with generating implications of various representations for different groups. The explicit inclusion of short, medium and long-term solutions is an important reminder of the need for a long-term vision of the public health system while working on shorter term change.
We noted some limitations to the IBPA framework and process, including the emphasis on evidence—a term that is increasingly contested, due to implicit notions of what does (and does not) suffice as evidence within the scientific domain (44). Also, while we agree considering existing evidence is important, we also note that evidence derives from past research—thus, an emphasis on evidence can hamper innovation and novel ideas. Second, we note the flexible nature of this framework and the need for commitment and expertise in applying the values, which may lead to results that vary in rigor and content across researchers. While we appreciate the flexibility of the guiding principles, we also found it challenging to prioritize them to address particular questions. Understanding the different guiding principles, such as reflexivity, diverse knowledges and time and space, takes skill and specialized knowledge.
Conclusion or synthesis
We are at a pivotal point in U.S. history, when contradictory opinions about the responsibilities and rights of government are being expressed and policy discourse is often focused on short term solutions. The public health system, and public health professionals, have long stood for the importance of fair and equitable supports for health for all (11, 38). The IBPA framework is a tool that can be used to design and build a more robust, socially-responsive public health system that better addresses the complex upstream determinants of health disparities in the U.S. and elsewhere (25). The IBPA framework encourages bold thinking and a commitment to build the resilient and socially just public health system our communities need.
Author contributions
DH and MS identified the analytical approach and framework for this work. MS developed the tables and figures. DH drafted the initial manuscript. DH, MS, and SJ contributed to the ideas, revised the tables, figures and manuscript and contributed significantly to the writing. All authors contributed to the article and approved the submitted version.
Funding
SJ acknowledges support from the National Institute of Mental Health (1K01MH122316).
Acknowledgments
The authors thank Patti Gale, Hinckley Jones-Sanpei, and Jason Schwartz for their insightful comments on early versions of the IBPA results and the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^We chose to restrict analysis to before vaccines were available in December 2020.
References
1. Cutler, D, and Miller, G. The role of public health improvements in health advances: the twentieth-century United States. Demography. (2005) 42:1–22. doi: 10.1353/dem.2005.0002
2. Shetty, KD, DeLeire, T, White, C, and Bhattacharya, J. Changes in U.S. hospitalization and mortality rates following smoking bans. J Policy Anal Manage. (2010) 30:6–28. doi: 10.1002/pam.20548
3. Jayatilleke, N, and Mackie, A. Reflection as part of continuous professional development for public health professionals: a literature review. J Public Health (Oxf). (2013) 35:308–12. doi: 10.1093/pubmed/fds083
4. Saracci, R. Counterpoint: Epidemiology's dual social commitment-science and health. Am J Epidemiol. (2021) 190:980–3. doi: 10.1093/aje/kwaa272
5. Savitz, DA. Point: reconciling Epidemiology's aspirations and capabilities. Am J Epidemiol. (2021) 190:977–9. doi: 10.1093/aje/kwaa271
6. World Health Organization. Constitution of the World Health Organization. New York City, NY: World Health Organization (1946).
7. First Nations Health Authority. First nations perspective on health and wellness. (2020) Available at: https://fnha.ca/wellness/wellness-and-the-first-nations-health-authority/first-nations-perspective-on-wellness. (Accessed December 10, 2020)
9. Frieden, TR. Shattuck lecture: the future of public health. N Engl J Med. (2015) 373:1748–54. doi: 10.1056/NEJMsa1511248
10. Richardson, LD. Integrating health equity into practice and policy. J Public Health Manag Pract. (2016) 22:S107–9. doi: 10.1097/PHH.0000000000000372
11. Uzdavines, ML. The great American health care system and the dire need for change: stark law reform as a path to a vital future of value-based care. Texas. (2019) 7:573. doi: 10.37419/LR.V7.I3.3
12. Bowleg, L. Evolving intersectionality within public health: from analysis to action. Am J Public Health. (2021) 111:88–90. doi: 10.2105/AJPH.2020.306031
13. Kopel, J, Perisetti, A, Roghani, A, Aziz, M, Gajendran, M, and Goyal, H. Racial and gender-based differences in COVID-19. Front Public Health. (2020) 8:418. doi: 10.3389/fpubh.2020.00418
14. Hudson, KD, Matsuzaka, S, and Mehrotra, G. Intersectional antiracist advocacy practice in health care organizations. Health Promot Pract. (2023) 24:426–31. doi: 10.1177/15248399221131833
15. Hunting, G. A call for a policy paradigm shift: an intersectionality-based analysis of FASD policy In:. An intersectionality-based policy analysis framework, vol. 1, Institute for Intersectionality Research and Policy. (2012). 93–113.
16. Fagrell Trygg, N, Gustafsson, PE, Hurtig, AK, and Månsdotter, A. Reducing or reproducing inequalities in health? An intersectional policy analysis of how health inequalities are represented in a Swedish bill on alcohol, drugs, tobacco and gambling. BMC Public Health. (2022) 22:1302. doi: 10.1186/s12889-022-13538-6
17. Hankivsky, O, Grace, D, Hunting, G, Giesbrecht, M, Fridkin, A, Rudrum, S, et al. An intersectionality-based policy analysis framework: critical reflections on a methodology for advancing equity. Int J Equity Health. (2014) 13:119. doi: 10.1186/s12939-014-0119-x
18. Hankivsky, O. An intersectionality-based policy analysis framework In:. Institute for Intersectionality Research and Policy. Vancouver, BC: Simon Fraser University (2012)
19. Kantamneni, N. The impact of the COVID-19 pandemic on marginalized populations in the United States: a research agenda. J Vocat Behav. (2020) 119:103439. doi: 10.1016/j.jvb.2020.103439
20. Alcendor, DJ. Racial disparities-associated COVID-19 mortality among minority populations in the US. J Clin Med. (2020) 9:2442. doi: 10.3390/jcm9082442
21. Etowa, J, and Hyman, I. Unpacking the health and social consequences of COVID-19 through a race, migration and gender lens. Can J Public Health. (2021) 112:8–11. doi: 10.17269/s41997-020-00456-6
22. Heslin, KC, and Hall, JE. Sexual orientation disparities in risk factors for adverse COVID-19-related outcomes, by race/ethnicity – behavioral risk factor surveillance system, United States, 2017-2019. MMWR Morb Mortal Wkly Rep. (2021) 70:149–54. doi: 10.15585/mmwr.mm7005a1
23. Bowleg, L. We're not all in this together: on COVID-19, intersectionality, and structural inequality. Am J Public Health. (2020) 110:917. doi: 10.2105/AJPH.2020.305766
24. Maestripieri, L. The Covid-19 pandemics: why intersectionality matters. Front Sociol. (2021) 6:642662. doi: 10.3389/fsoc.2021.642662
25. Poteat, T. Navigating the storm: how to apply intersectionality to public health in times of crisis. Am J Public Health. (2021) 111:91–2. doi: 10.2105/AJPH.2020.305944
26. Nazareno, J, Yoshioka, E, Adia, AC, Restar, A, Operario, D, and Choy, CC. From imperialism to inpatient care: Work differences of Filipino and White registered nurses in the United States and implications for COVID-19 through an intersectional lens. Gend Work Organ. (2021) 28:1426–46. doi: 10.1111/gwao.12657
27. Ruprecht, MM, Wang, X, Johnson, AK, Xu, J, Felt, D, Ihenacho, S, et al. Evidence of social and structural COVID-19 disparities by sexual orientation, gender identity, and race/ethnicity in an urban environment. J Urban Health. (2021) 98:27–40. doi: 10.1007/s11524-020-00497-9
28. Sekalala, S, Perehudoff, K, Parker, M, Forman, L, Rawson, B, and Smith, M. An intersectional human rights approach to prioritising access to COVID-19 vaccines. BMJ Glob Health. (2021) 6:e004462. doi: 10.1136/bmjgh-2020-004462
29. Yee, S, Breslin, ML, Goode, TD, Havercamp, SM, Horner-Johnson, W, Iezzoni, LI, et al. Compounded disparities: Health equity at the intersection of disability, race, and ethnicity. Washington, DC: The National Academies of Sciences, Engineering and Medicine (2018).
30. Elnaiem, AD. Intersectionality in the time of COVID-19: dispatches from a contact tracer. Am J Public Health. (2021) 111:93–4. doi: 10.2105/AJPH.2020.306027
31. Gibney, A, Harutyunyan, O, and Hillinger, S. Totally under control. United States: Neon (2020). 123 p minutes.
32. Huang, P, and Simmons-Duffin, S. White house strips CDC of data collection role for COVID-19 hospitalizations, in National Public Radio NPR (2020).
33. Ludvigson, SC, Ma, S, and Ng, S. COVID-19 and the macroeconomic effects of costly disasters National Bureau of Economic Research (2020).
34. Moore, JT, Pilkington, W, and Kumar, D. Diseases with health disparities as drivers of COVID-19 outcome. J Cell Mol Med. (2020) 24:11038–45. doi: 10.1111/jcmm.15599
35. Paltiel, AD, Zheng, A, and Sax, PE. Clinical and economic effects of widespread rapid testing to decrease SARS-CoV-2 transmission. Ann Intern Med. (2021) 174:803–10. doi: 10.7326/M21-0510
36. Williams, MA, and Koff, WC. How the U.S. should invest in public health before reopening the economy, in fortune. New York City, NY: Meredith Corporation (2020).
37. Gorges, RJ, and Konetzka, RT. Staffing levels and COVID-19 cases and outbreaks in U.S. nursing homes. J Am Geriatr Soc. (2020) 68:2462–6. doi: 10.1111/jgs.16787
38. Awosogba, T, Betancourt, JR, Conyers, FG, Estapé, ES, Francois, F, Gard, SJ, et al. Prioritizing health disparities in medical education to improve care. Ann N Y Acad Sci. (2013) 1287:17–30. doi: 10.1111/nyas.12117
39. Evans, MK, Rosenbaum, L, Malina, D, Morrissey, S, and Rubin, EJ. Diagnosing and treating systemic racism. N Engl J Med. (2020) 383:274–6. doi: 10.1056/NEJMe2021693
40. Feagin, J, and Bennefield, Z. Systemic racism and U.S. health care. Soc Sci Med. (2014) 103:7–14. doi: 10.1016/j.socscimed.2013.09.006
41. Centers for Disease Control and Prevention. COVID Data Tracker. (2023); Available at: https://covid.cdc.gov/covid-data-tracker/#datatracker-home. (Accessed June 28, 2023)
42. Cho, S, Crenshaw, KW, and McCall, L. Toward a field of intersectionality studies: theory, applications, and praxis. Signs J Women Cult Soc. (2013) 38:785–810. doi: 10.1086/669608
43. Brownson, RC, Burke, TA, Colditz, GA, and Samet, JM. Reimagining public health in the aftermath of a pandemic. Am J Public Health. (2020) 110:1605–10. doi: 10.2105/AJPH.2020.305861
Keywords: intersectionality, public health policy analysis, COVID-19, intersectional frameworks, intersectionality praxis, Intersectionality-based Policy Analysis (IBPA)
Citation: Humphries DL, Sodipo M and Jackson SD (2023) The intersectionality-based policy analysis framework: demonstrating utility through application to the pre-vaccine U.S. COVID-19 policy response. Front. Public Health. 11:1040851. doi: 10.3389/fpubh.2023.1040851
Edited by:
Tafadzwa Dzinamarira, University of Rwanda, RwandaReviewed by:
Hyeyoung Nelson, University of Colorado, United StatesLucia Ratiu, Babeș-Bolyai University, Romania
Copyright © 2023 Humphries, Sodipo and Jackson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Debbie L. Humphries, ZGViYmllLmh1bXBocmllc0B5YWxlLmVkdQ==