 JunSeo Lim
JunSeo Lim- The Research Institute of Nursing Science, College of Nursing, Seoul National University, Seoul, Republic of Korea
Objective: Social robot interventions are being implemented to reduce cognitive decline, depression, and loneliness among older adults. However, the types, functions, and programs of effective social robots have not yet been confirmed. This study investigated whether a social robot intervention is effective in improving cognitive function, depression, loneliness, and quality of life in older adults living alone.
Methods: This study used a non-equivalent control group pre-test–post-test design. It was conducted twice a week, with each session lasting 50 mi; twelve sessions were conducted over 6 weeks. This study was conducted at three senior welfare centers in Korea. In each group, 10 or fewer participants used the PIO social robot. The total participants included 64 people in the experimental (n = 31) and control groups (n = 33), and consisted of older people over 65 years of age living alone.
Results: There was a statistically significant difference in the pre-post values for cognitive function (z = 5.21, p < 0.001), depression (z = −2.99, p = 0.003), and loneliness (t = −4.27, p < 0.001) in the experimental and control groups. However, there was no statistically significant difference for quality of life (z = 1.84, p = 0.066).
Conclusions: It was confirmed that a cognitive intervention program using the social robot PIO can improve cognitive function and reduce depression and loneliness in older adults living alone.
1. Introduction
The global population aged over 65 years is expected to increase from 9.3% in 2020 to approximately 16% in 2050 (1). The population of those aged 65 years and above in Korea was 15.7% in 2020; this population of older adults belongs to an aging society, among which the proportion of those living alone is 19.6% (2). Older adults who live alone experience deterioration in their health owing to aging, economic poverty, dependence due to reduced income, loneliness due to social and psychological conflicts, severance of human relationships, and helplessness due to loss of social roles (3). In addition, older people living alone are more vulnerable compared to those living together concerning physical health, mental health, and quality of life (QoL) due to a lack of social cohesion through family relationships (4), social isolation, and reduced social support (5).
The decline in cognitive function due to aging reduces an individual's ability to adapt and causes emotional problems such as depression and anxiety, making it difficult to form interpersonal relationships that lead to poor QoL (6). Depression affects QoL in the older adults (7, 8), and living alone is a contributing factor to depression (5). Loneliness not only causes suffering in older adults by itself, but also indicates mental disorders such as depression, dementia, suicide, and physical diseases such as hypertension, heart disease, and diabetes (9, 10). Various non-pharmacological interventions are being tried in various ways to prevent cognitive decline and increase cognitive function in the older people. A cognition-based intervention is a comprehensive and complex approach aimed at improving cognitive function, cognitive stimulation, cognitive training, and cognitive rehabilitation (11). Computer-assisted cognitive rehabilitation (CACR) research has been increasing recently. In CACR, the group that received cognitive training using only a computer program saw a significant effect on cognitive function and memory but no effect on emotions or emotional variables (12). Various intervention studies using social robots are being attempted worldwide to alleviate the burden of care for older people amid changes in the family structure. The PARO robot is an emotional support robot that responds to touch, light, sound, and temperature through bodily sensors (13). A meta-analysis of the PARO robot showed that the effects were inconsistent on variables, such as cognitive function, problematic behavior, depression, and loneliness (14, 15). As a result of a cognitive intervention using Sil-Bot, the social robot, thinning of the anterior cingulate cortex was reduced, and age-related structural brain changes could be alleviated (16). Social robot programs for older people are mostly applied by substituting animal-assisted therapy (AAT) programs (17) with them or by placing social robots in centers and through facilitating interaction with them. As per past research, traditional cognitive training, such as stimulating the senses, was performed (18–20), and the study variables were mainly emotional. However, it was difficult to find studies that applied a CACR program to social robots to improve participants' cognitive functions and confirm emotional variables through interactions between social robots and participants.
Therefore, this study aimed to improve the cognitive function of older adults living alone by using the social robot PIO, to which the CACR program was applied. In addition, this study aimed to confirm the effect of reducing depression and loneliness and improving QoL through the interaction of the social robot PIO.
2. Methods
2.1. Study design
This was a non-equivalent control group pre-test–post-test design.
2.2. Participants
Participants were recruited from November 22, 2021 to January 5, 2022, at three senior welfare centers in Seoul, Korea. Forty-one people in the experimental group and 39 in the control group expressed their intentions to participate. Among them, five from the experimental group and three from the control group were excluded because they did not meet the selection criteria; 36 individuals each from the experimental and control groups finally participated in the study. During the study, three of 36 experimental group subjects dropped out due to health problems, two in the program refused to participate, and three out of 36 in the control group did not participate in the investigation due to COVID-19 infections. All participants adhered to the program schedule and attended all the sessions. There were no dropouts during the course of the intervention. The recruitment criteria for participants were as follows: (1) 65 years of age or older, (2) older adults living alone, (3) able to communicate in Korean, and (4) no history of severe mental illness, such as schizophrenia or delusional disorder. Exclusion criteria were: (1) older adults who were in the new cognitive intervention program at the time of the study, (2) history of psychiatric drug use within the last 4 weeks, and (3) having difficulty using their hands. Participants who wished to take part in the program were assigned to the experimental group first, and the control group was selected using convenience sampling by matching participants with those in the experimental group in terms of age, gender, education, and basic livelihood security recipient status. The final data were collected from 64 participants, who were divided into the experimental (n = 31) and control groups (n = 33). The sample size was calculated using G*power (3.1.9.6), with a significance level of 0.05, a large effect size (0.80), and a power of 0.85. According to the preliminary analysis, at least 30 people were required for each group, and an additional 20% were recruited considering the dropout rate.
2.3. Intervention
The intervention in this study was conducted from January 10 to March 2, 2022. During the study period, participants continued to participate in usual care (music, art programs, etc.) that they had previously enrolled in at the senior welfare center, and did not stop or participate in other programs. The experimental group participated in this study's program, and the control group did not. This program was conducted twice a week, 50 min per session, for 6 weeks. Each group of 10 or fewer participants underwent PIO. For smooth progress, two research assistants were used. The program, which consisted of 12 sessions, was structured by a storytelling of the process behind the parrot-shaped robot PIO hatching from an egg and growing into an adult robot. Each session started with the themes of “meeting with the social robot PIO” and “recalling the previous program.” In addition, gymnastics was performed with the social robot PIO to relieve tension and improve intimacy with the robot. Before the 6th session, “Teaching movements and gymnastics,” gymnastics was performed while watching a video, and after the 6th session, gymnastics was performed while watching the movements of the social robot PIO. The program lasted about 30 min according to the contents of each session. The ending involved “Expressing your impression about the program” and “Saying goodbye to social robot PIO” (Table 1). Participants were configured to naturally stimulate cognition and emotion in the process of PIO programs (Figure 1).
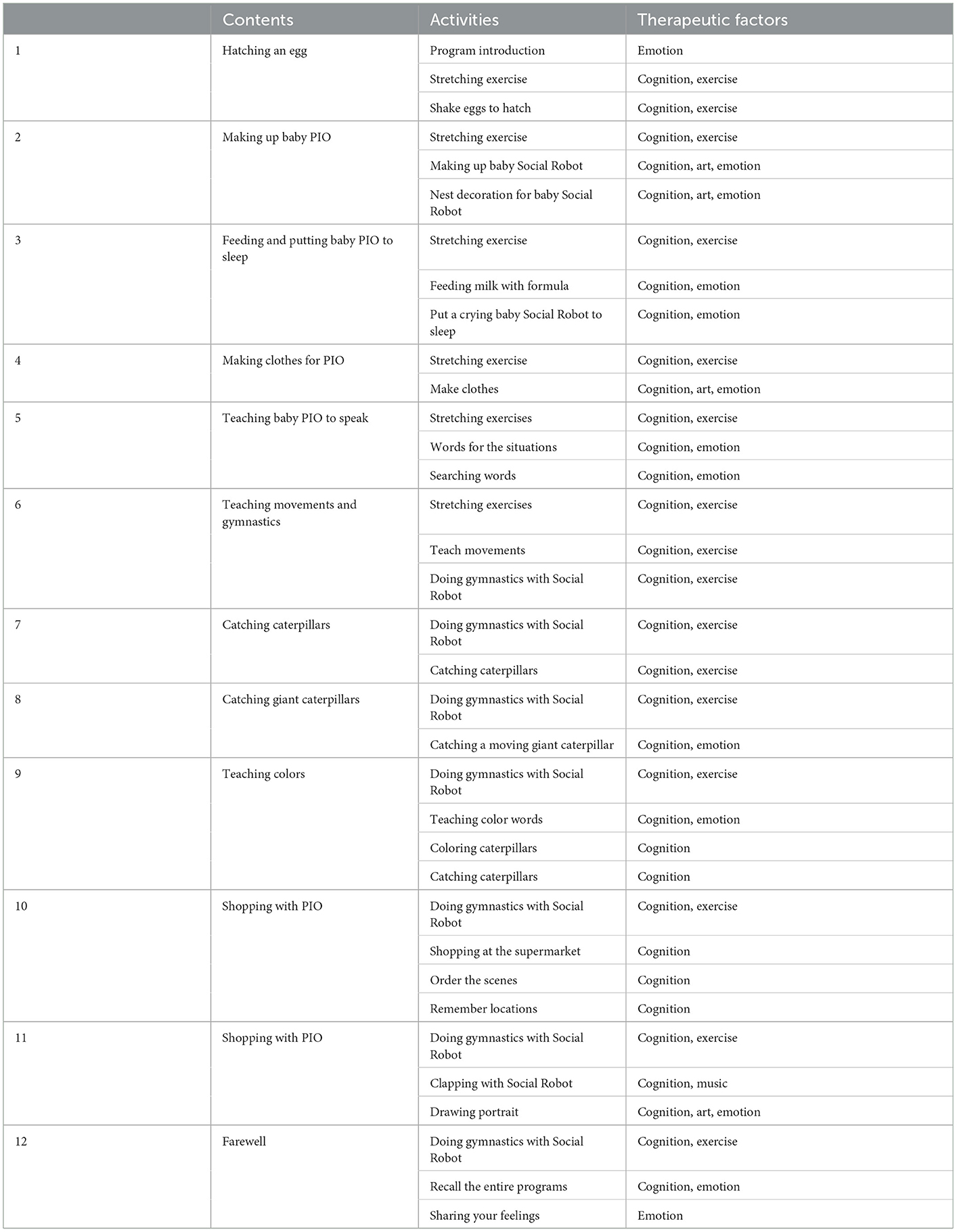
Table 1. Contents of PIO program.
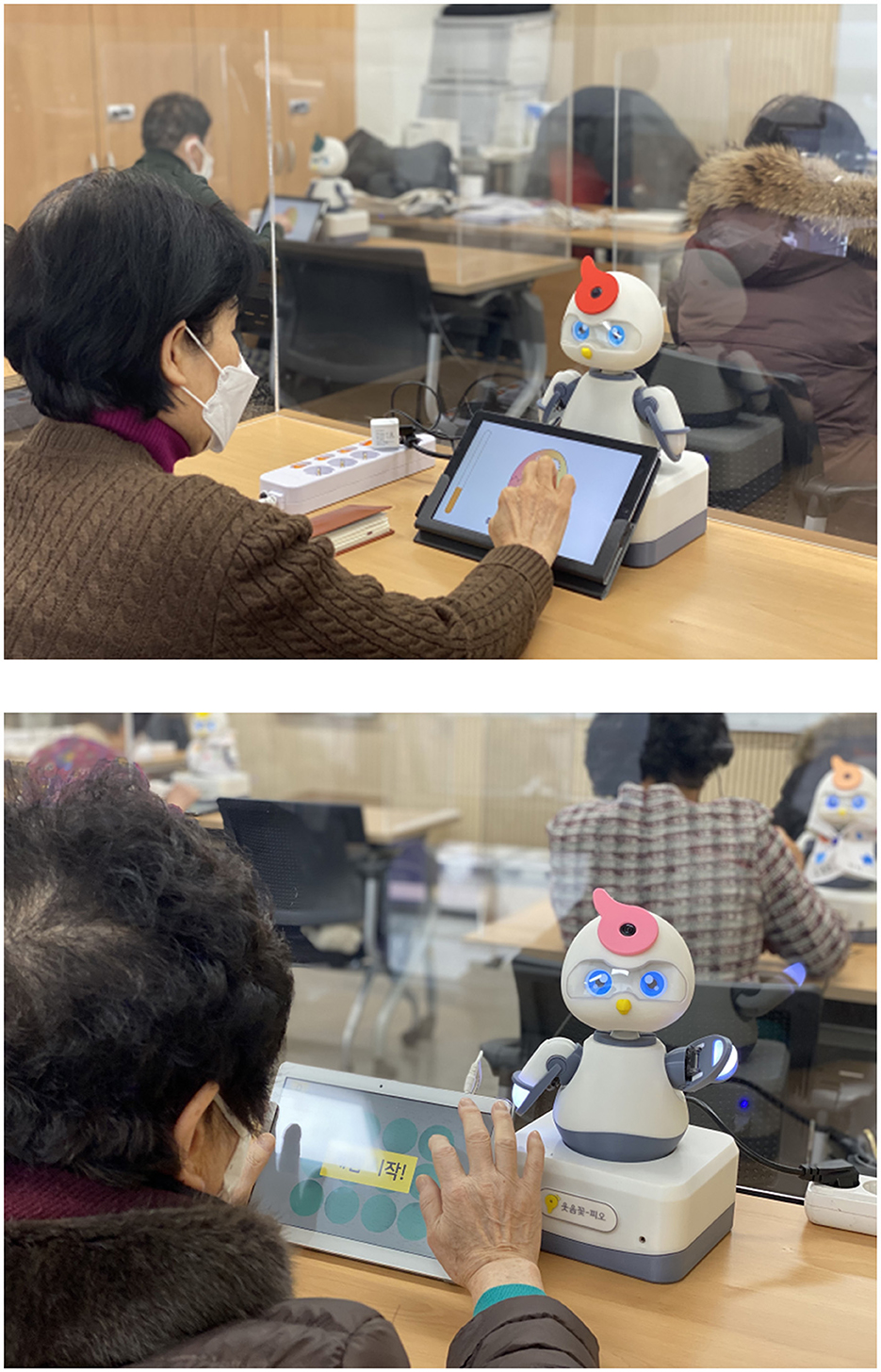
Figure 1. Participants conducting PIO program.
2.4. Social robot PIO
The social robot PIO is a parrot-shaped robot developed by Why Dots for cognitive-emotional programs with older people and older adults with dementia. The social robot PIO expresses various emotions through the eyes of an LCD display, and it is possible to implement structured conversations and various movements according to the program composition when performing a program with subjects. The size of the social robot was 200 ×170 ×325 mm, and its weight was approximately 2 kg (Figure 2).
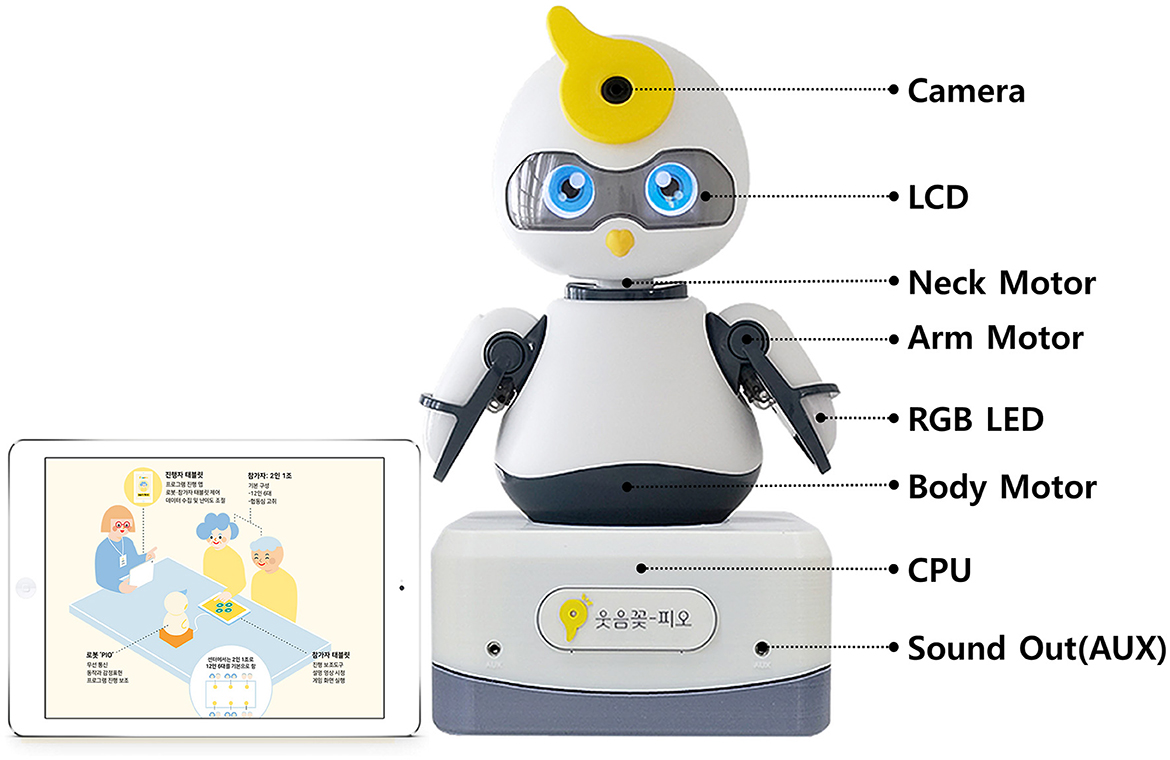
Figure 2. Social robot PIO (Version 2.0).
2.5. Instruments
2.5.1. K-MMSE~2:SV
The Korean-Mini Mental State Examination, 2nd Edition (K-MMSE~ 2): SV (Standard Version) by Kang et al. (21), which translated the 2010 revised Mini-Mental State Examination (MMSE) developed by Folstein et al. (22) into Korean, was used. The K-MMSE~2:SV comprises seven subscales in the following order: registration, orientation to time, orientation to place, recall, attention and calculation, language, and drawing. At the time of instrument development, Cronbach's α was 0.69 (21). In this study, Cronbach's α was 0.73.
2.5.2. Depression
The Geriatric Depression Scale Short Form: Korean Version (GDSSF-K), a tool developed by Sheikh and Yesavage (23), which was translated and modified by Kee (24), was used to measure depression. The GDSSF-K consists of 15 items and “yes” or “no” answers to each question. The higher the score, the greater the depression. At the time of development, the Cronbach's α was 0.88. In this study, the Cronbach's α was 0.79.
2.5.3. Loneliness
The Revised UCLA Loneliness Scale (RULS), developed by Russel et al. (25), was used to measure loneliness; the scale was translated into Korean by Kim (26). It consists of 20 items on a four-point Likert scale, and the higher the score, the greater the degree of loneliness. At the time of tool development, Cronbach's α was 0.93. In this study, Cronbach's α was 0.87.
2.5.4. QoL
QoL was measured using the EQ-5D-3L (Euro Quality of life-5Dimension-3Level) tool developed by the EuroQol group. The EQ-5D-3L consists of five domains: mobility, self-care, usual activities, pain/discomfort, anxiety/depression. In this study, the QoL tariff by Lee et al. (27) was used for calculation. In the sub-domain, the raw score was reverse-coded, with a higher score indicating a higher QoL. At the time of instrument development, Cronbach's α was 0.64 (28). In this study, the Cronbach's α was 0.61.
2.6. Statistical analysis
The data collected were analyzed using STATA 17. Descriptive statistics were used to demonstrate the demographic characteristics. The homogeneity between groups was analyzed using the t-test, χ2 test, and Fisher's exact test. Tests of major variables to confirm the effectiveness of the program were analyzed with an independent t-test for normal distribution and Mann-Whitney U test for alternative distribution. The level of significance was set at P < 0.05.
3. Results
3.1. General characteristics
Demographic characteristics and health information of the participants are summarized in Table 2. In the experimental group, there were 29 (93.5%) females and 2 (6.5%) males; the control group comprised 28 (84.8%) females and 5 (15.2%) males. Concerning age, 11 (35.5%) were 70–74 years old in the experimental group; 11 (33.3%) were 75–79 years old in the control group. Regarding level of education, the majority of elementary school graduates were 9 (29.0%) in the experimental group and 17 (51.5%) in the control group. Regarding marital status, bereavement was common in 18 (58.1%) and 24 (72.7 %) patients in the experimental and control groups, respectively. Regarding the presence or absence of children, there were 29 (93.5%) in the experimental group and 28 (84.8%) in the control group. Regarding the presence or absence of companion animals, 28 (90.3%) participants in the experimental group and 31 (93.9%) in the control group did not have companion animals. Regarding religion, Buddhism was the most common, with 14 (45.2%) participants in the experimental group, and Christianity was the most common, with 12 (36.4%) in the control group. Regarding religion, Buddhism was the most common, with 14 (45.2%) participants in the experimental group, and Christianity was the most common, with 12 (36.4%) in the control group. There were 10 (32.3%) and 18 (54.6%) patients in the experimental and control groups, respectively. Twenty-five (80.6%) patients in the experimental group and 26 (78.8%) in the control group had no physical disabilities. Twenty-four (77.4%) patients in the experimental group and 23 (69.7%) in the control group did not have a basic livelihood.
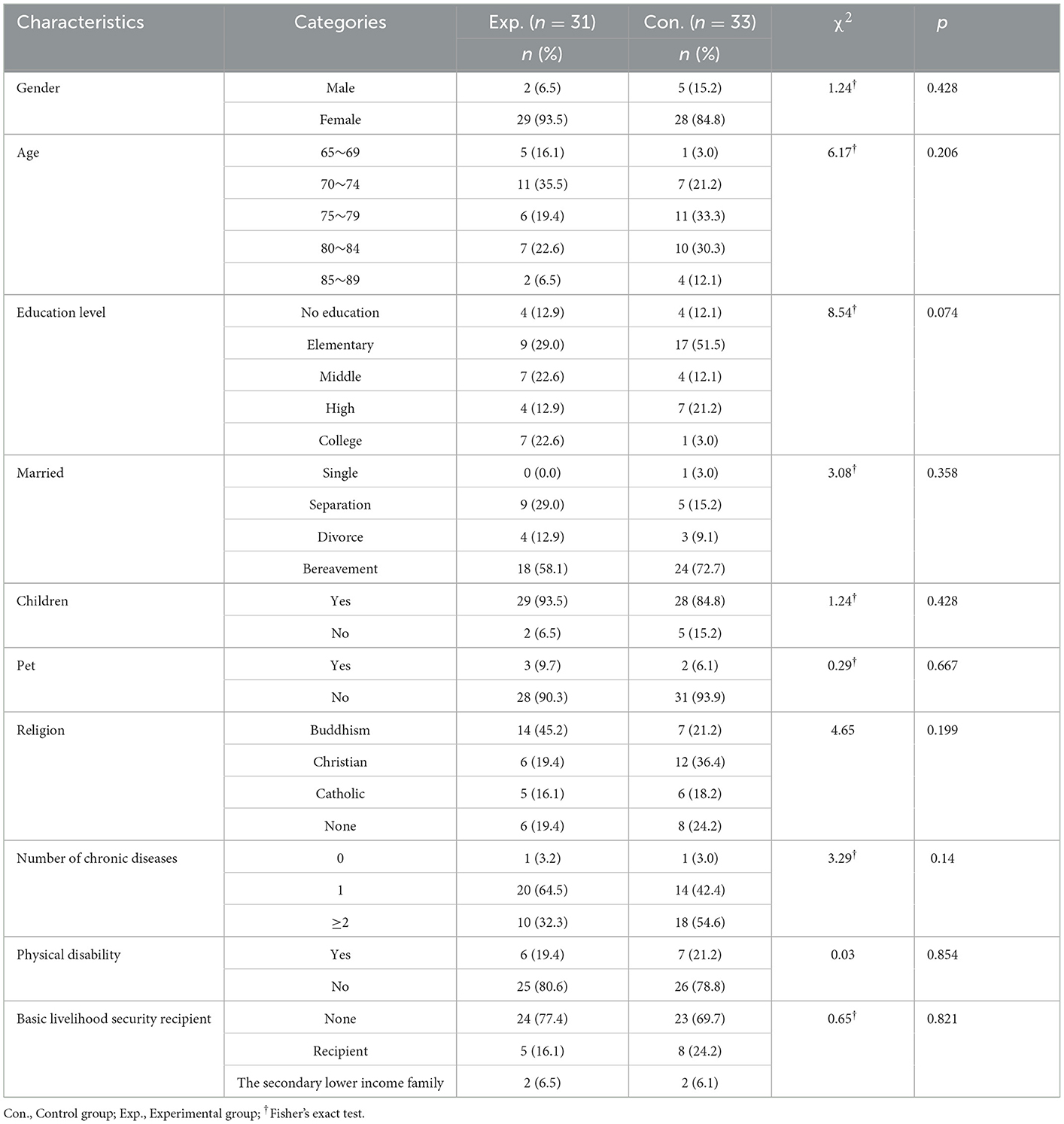
Table 2. Homogeneity test of general characteristics (N = 64).
3.2. Effects of PIO interventions on cognition function
For the cognition function variable, the difference between the pre-post scores of the experimental and control groups were statistically significant (z = 5.21, p = 0.001). The experimental group increased by 3.00 ± 2.73, and the median (IQR) increased to 2 (3), the control group decreased by −0.61 ± 1.78, and the median value (IQR) decreased to −1 (3). On the subscale, location orientation (z = 3.41, p < 0.001), attention and counting (z = 3.71, p < 0.001), and language (z = 2.62, p = 0.009) increased significantly, but registration (z = −0.53, p = 0.595), temporal orientation (z = 1.70, p = 0.089), memory recall (z = 1.66, p = 0.097), and drawing (z = 0.92, p = 0.357) did not show statistically significant differences (Table 3).
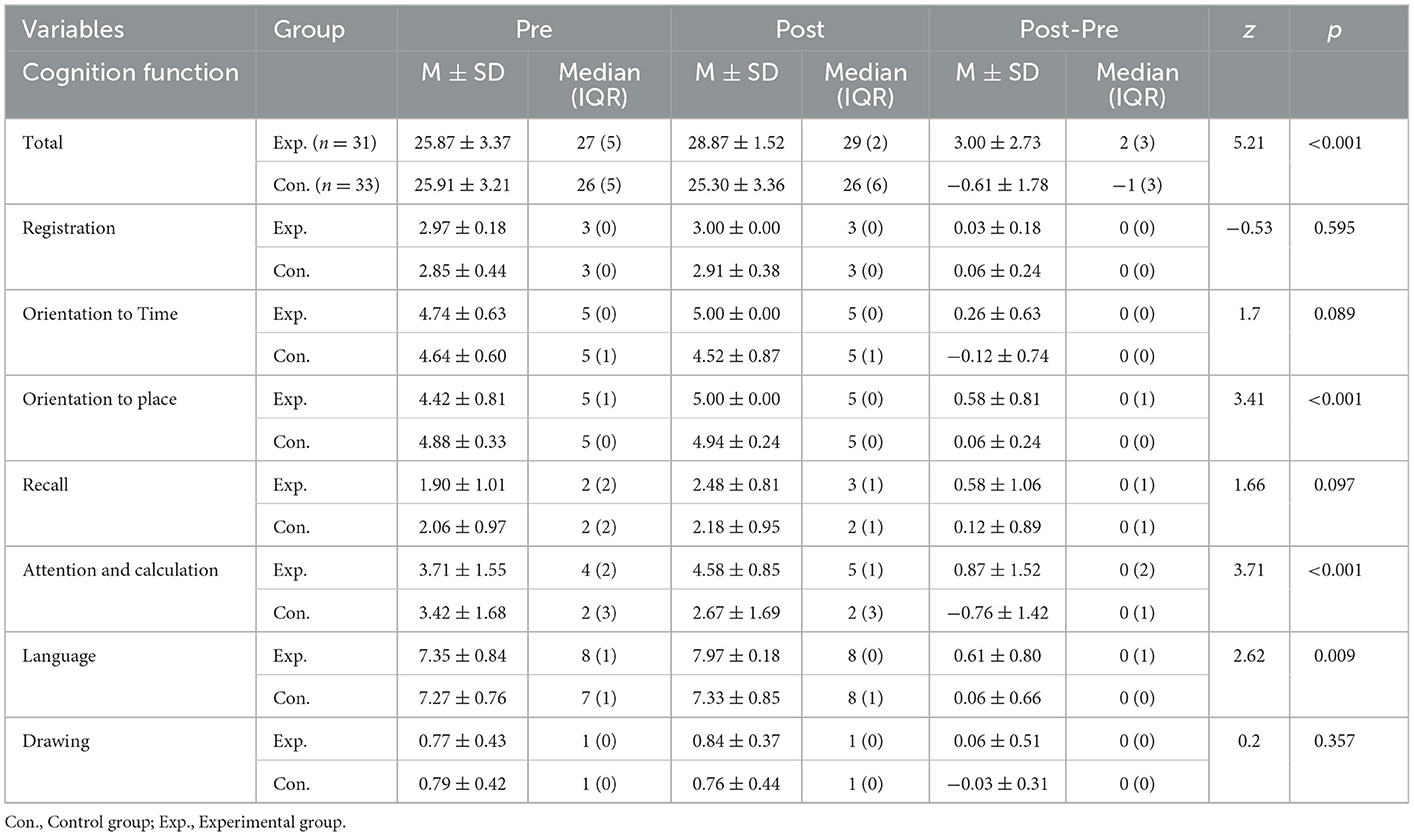
Table 3. Comparison of cognition function (N = 64).
3.3. Effects of PIO interventions on depression, loneliness, and QoL
For the depressive variable, the difference between the pre-post scores of the experimental and control groups were statistically significant (z = −2.99, p = 0.003). The experimental group decreased by −2.42 ± 3.36, and the median (IQR) decreased to −2 (3), the control group increased by 0.03 ± 2.82, and the median (IQR) was 0 (3). For the loneliness variable, the difference between the pre-post scores of the experimental and control groups was statistically significant (t = −4.27, p < 0.001). The experimental group decreased by −11.26 ± 9.34, and the median (IQR) decreased to −12 (14), the control group decreased by −0.55 ± 10.64, and the median (IQR) was 1 (16). Regarding QoL variables, the difference between the pre-post scores of the experimental and control groups was not statistically significant (z = 1.84, p = 0.066). The experimental group increased by 0.07 ± 0.12, and the median (IQR) increased to 0.09 (0.14); the control group increased by 0.03 ± 0.10, and the median (IQR) was 0 (0.96). On the subscale, mobility (z = 3.21, p < 0.001) increased significantly, but self-care (z = 1.03, p = 0.302), usual activities (z = 1.02, p = 0.310), and anxiety/depression (z = 1.85, p = 0.064) did not show any statistically significant difference. Pain/discomfort (z = −0.63, p = 0.530) decreased, but the difference was not statistically significant (see Table 4).
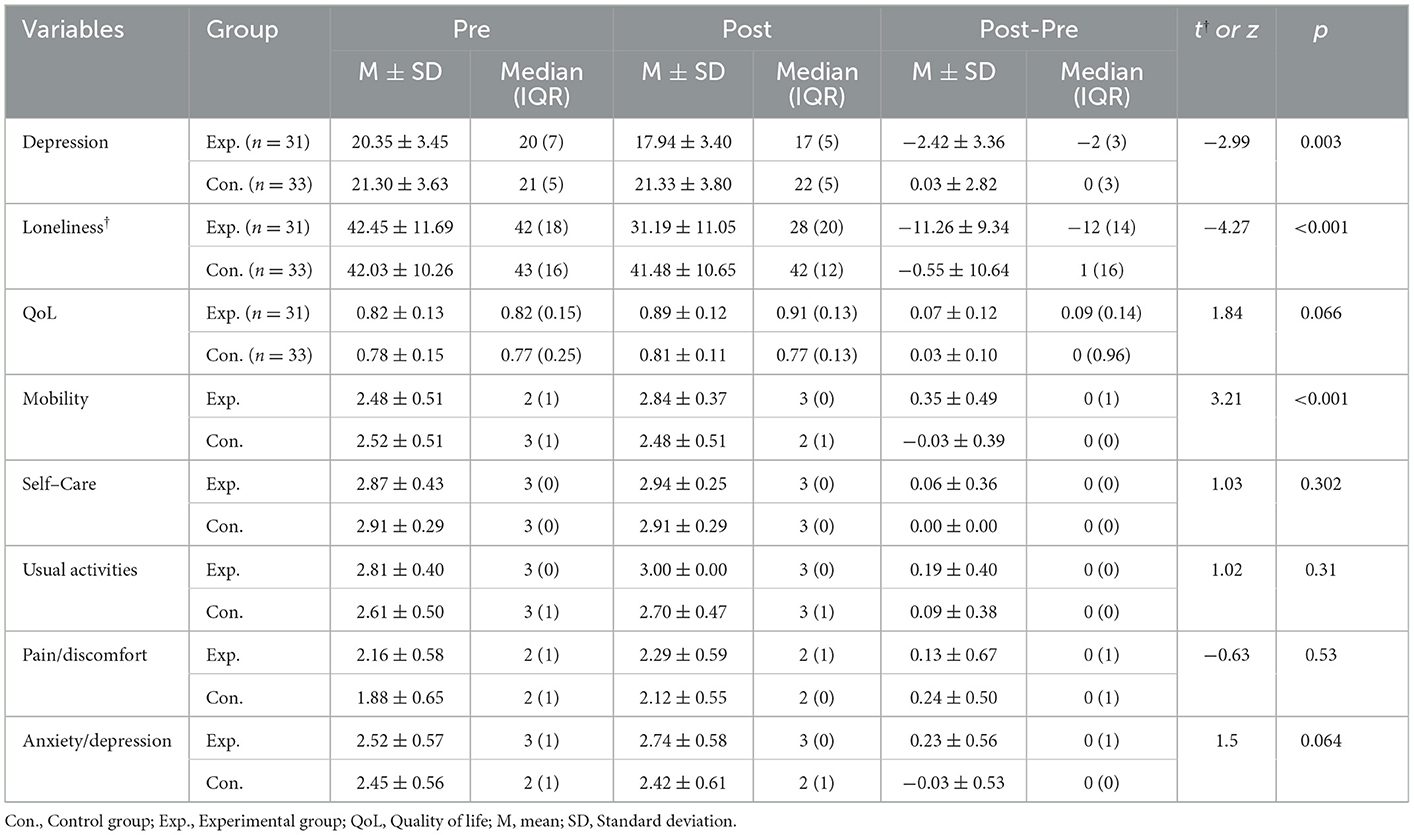
Table 4. Comparison of depression, loneliness and QoL (N = 64).
4. Discussion
The results showed that the cognitive function scores improved, depression and loneliness scores decreased, and the difference between groups in the pre-post change was statistically significant. In contrast, the QoL score improved, but the between-group difference was not statistically significant.
In this study, the cognitive function score of the experimental group increased compared to that before the intervention, while that of the control group decreased. Regarding the MMSE tool, a decrease of 1–3 points can be judged as a clinically meaningful result (29). Therefore, it can be concluded that the program using the PIO robot improved the cognitive function of older adults living alone. There have been few studies on cognitive intervention programs using social robots for older people, and most of them have shown an improvement in cognitive function scores, but without any statistically significant difference (16, 30–33). In particular, the Sil-Bot robot was not able to derive statistically significant results from cognitive function variables even though it was composed of a program including the elements of CACR; however, this program was distinct as it derived statistically significant results. In a study that evaluated cognitive function using the harp-seal PARO robot for older people with dementia, the cognitive function score decreased after the intervention (18, 20, 34). This seems to be because the robot intervention consisting of an AAT program is hard to operate among older adults who have not been diagnosed with dementia; it is difficult to proceed because the program is monotonous, and its effectiveness is difficult to verify in older people with dementia. Multitasking ability demands, such as allocating and shifting attention, may induce additional brain activity in older adults (16). This program required a lot of multitasking between the PIO and participants, and the session was configured to increase emotional interaction with the PIO. A study showed that a multi-domain cognitive training program is more suitable for increasing brain neuroplasticity than monotherapy such as occupational therapy, exercise therapy, or art therapy (35); moreover, repetition was shown to enhance cognitive function in older adults, which is consistent with previous studies showing that it is effective to apply a program that integrates emotional and physical stimulation as well as cognitive stimulation (36).
The experimental group participating in the program had a more significant decrease in depression scores than the control group. This is also consistent with the results of a previous study that simultaneously confirmed the subject's cognitive function and depression, using the Sil-Bot robot (31). However, Oh et al. (37) configured a complex program with play content including recreational functions preferred by older people as a Silver-Care-Robot so that the robot and participants could interact, but both cognitive function and depressive variables decreased after the intervention. Petersen et al. (18) and Liang et al. (34), who performed interventions with the PARO robot for older adults with dementia, reported a statistically significant decrease in depression, but Robinson et al. (38) and Júranson et al. (39) found that depression scores in the experimental group increased after the intervention. As such, depending on the type of social robot and characteristics of the intervention method, the effect on the depressive variable is inconsistent. Social robots are useful for their attachment to humans, simple communication, and responsiveness to learning and training, such as the relationship between humans and dogs (40). Based on the storytelling method for participants to grow their PIO, this program was designed to increase attachment through interactions between participants and the PIO. By giving the PIO a name, making clothes, and so on, it was possible to nurture the PIO and encourage the participants to perform the program well, and by performing various actions, emotional communion with the participant was increased. Therefore, it is judged that this program increased the attachment between participants and the PIO and lowered depression. This study was conducted during the COVID-19 pandemic, and conversations between participants were prohibited during the program to ensure their safety. Therefore, the study results can be seen as the interaction effect between the participant and the PIO, rather than the interaction effect between the participants during the program.
In this study, the experimental group had a more statistically significant decrease in loneliness than the control. It was judged as effective to have an emotional bond through attachment in the process of hatching and growing from an egg, just like raising a real pet to promote an emotional bond between the participant and PIO. In a previous study that used the dog-shaped social robot AIBO, Kanamori et al. (41) reported that loneliness in older people decreased, but this was not statistically significant; Banks et al. (42) reported that loneliness decreased statistically significantly. It was reported that loneliness decreased in the intervention using the PARO robot, but the difference was not statistically significant (38). Loneliness variables were inconsistent in the social robot interventions.
Loneliness is a subjective emotion that appears by recognizing a lack of close social contact or emotional bonding (43); depression and loneliness closely interact with each other (44). This study was conducted during the COVID-19 pandemic by minimizing interaction and social contact between participants to confirm the significant effect of depressive variables. Therefore, to reduce depression or loneliness, it is necessary to construct a program for social contact and emotional bonds between subjects through social robots, or to develop a program for creating emotional bonds between social robots and participants. Older people who regularly participate in exercise programs for physical activity have improved self-esteem and reduced loneliness (40, 45). This program consisted of “Gymnastics with PIO” and participants continued stretching before and during each session. Participants observed that they paid more attention to the movement of the PIO than to the movie clip on the tablet PC.
The quality of the QoL score improved in the experimental group, but the difference was not statistically significant. Similarly, Júranson et al. (46) reported that the PARO robot improved the QoL score for older people with moderate dementia, but it was not statistically significant; however, the score was statistically significant for those with severe dementia. Valentï Soler et al. (20) reported that QoL was significantly improved by using the PARO robot. The QoL measurement tool used in this study was EQ-5D-3L. According to a study on the validity and reliability of the EQ-5D tool targeting Koreans, Koreans do not actively express their social and cultural health problems, showing a relatively high ceiling effect (47). Therefore, the participants answered their health-related questions positively in the pre-measurement; however, in the post-measurement, they may have answered their health status more exaggeratedly, so it was judged that the QoL score decreased after the intervention. Therefore, after assessing the items in the instrument and the composition of this program, it is recommended that subsequent researchers use the EQ-VAS (Euro Quality of life-Visual Analog Scale) rather than the EQ-5D-3L.
5. Limitations
This study was conducted during the COVID-19 pandemic. Although it was implemented as a group program, social interactions between participants were controlled for their safety. Therefore, it was possible to control for confounding variables through interactions between participants. Randomized controlled trials could not be conducted because of restrictions on gatherings due to COVID-19 and the anxiety of older adults living alone or within group programs. In addition, pre-and follow-up measurements are required to confirm whether the effect of the program continues; however, follow-up measurements were not performed.
6. Conclusions
The PIO robot program was confirmed to be effective in cognitive function, depression, and loneliness for the older adults living alone. If this program is applied to older adults living alone in the community, cognitive decline and progression to dementia may be prevented. This reduce the nation's social burden. When nurses directly implement the PIO program intervention, they can provide customized nursing care by identifying the actual function of the patient, which can be utilized effectively in nursing practice.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University. The approval number is IRB No. 2108/002-012. The patients/participants provided their written informed consent to participate in this study.
Author contributions
The author confirms being the sole contributor of this work and has approved it for publication.
Funding
This study was supported by a Health Fellowship Foundation of 2021. However, the researchers retained full independence in this study.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Economic UNDO and Division SAP. World population ageing 2020 highlights: Living arrangements of older persons, UN. (2020).
3. Li IC, Kuo H-T, Lin K-C, Wu Y-C. The Effects of Depressive Symptoms on Quality of Life Among Institutionalized Older Adults in Taiwan. Perspect Psychiatr Care. (2014) 50:58–64. doi: 10.1111/ppc.12029
4. Kim J-G. The impact of family type on health behavior of elderly people. J Welf Aged. (2011) 51:35–56. doi: 10.21194/kjgsw.51.201103.35
5. Russell D, Taylor J. Living alone and depressive symptoms: the influence of gender, physical disability, and social support among hispanic and non-hispanic older adults. J Gerontol B Psychol Sci Soc Sci 64B. (2009) 95–104. doi: 10.1093/geronb/gbn002
6. Zelinski EM, Gilewski MJ. A 10-item Rasch modeled memory self-efficacy scale. Aging Ment Health. (2004) 8:293–306. doi: 10.1080/13607860410001709665
7. Kondo N, Kazama M, Suzuki K, Yamagata Z. Impact of mental health on daily living activities of Japanese elderly. Prev Med. (2007) 46:457–62. doi: 10.1016/j.ypmed.2007.12.007
8. Murata C, Kondo K, Hirai H, Ichida Y, Ojima T. Association between depression and socio-economic status among community-dwelling elderly in Japan: The Aichi Gerontological Evaluation Study (AGES). Health Place. (2008) 14:406–14. doi: 10.1016/j.healthplace.2007.08.007
9. Heinrich LM, Gullone E. The clinical significance of loneliness: A literature review. Clin Psychol Rev. (2006) 26:695–718. doi: 10.1016/j.cpr.2006.04.002
10. Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N, et al. (2017). An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health, 152, 157–71. doi: 10.1016/j.puhe.2017.07.035
11. Clare L, Woods B. Cognitive rehabilitation and cognitive training for early-stage Alzheimer's disease and vascular dementia. Cochr Datab System Rev. (2003) 2003:CD003260. doi: 10.1002/14651858.CD003260
12. García-Casal JA, Loizeau A, Csipke E, Franco-Martín M, Perea-Bartolomé MV, Orrell M. Computer-based cognitive interventions for people living with dementia: a systematic literature review and meta-analysis. Aging Mental Health. (2017) 21:454–467. doi: 10.1080/13607863.2015.1132677
13. Wada K, Ikeda Y, Inoue K, Uehara R. Development and preliminary evaluation of a caregiver's manual for robot therapy using the therapeutic seal robot Paro. In: 19th International Symposium in Robot and Human Interactive Communication, IEEE (2010). p. 533–538. doi: 10.1109/ROMAN.2010.5598615
14. Leng M, Liu P, Zhang P, Hu M, Zhou H, Li G, et al. Pet robot intervention for people with dementia: A systematic review and meta-analysis of randomized controlled trials. Psychiatry Res. (2019) 271:516–25. doi: 10.1016/j.psychres.2018.12.032
15. Pu L, Moyle W, Jones C, Todorovic M. The effectiveness of social robots for older adults: a systematic review and meta-analysis of randomized controlled studies. Gerontologist. (2019) 59:e37–51. doi: 10.1093/geront/gny046
16. Kim GH, Jeon S, Im K, Kwon H, Lee BH, Kim GY, et al. Structural brain changes after traditional and robot-assisted multi-domain cognitive training in community-dwelling healthy elderly. PLoS One. (2015) 10:e0123251. doi: 10.1371/journal.pone.0123251
17. Koh IS, Kang HS. Effects of intervention using PARO on the cognition, emotion, problem behavior, and social interaction of elderly people with dementia. J Korean Acad Commun Health Nurs. (2018) 29:300–9. doi: 10.12799/jkachn.2018.29.3.300
18. Petersen S, Houston S, Qin H, Tague C, Studley J. The utilization of robotic pets in dementia care. J Alzheimer's Disease. (2017) 55:569–74. doi: 10.3233/JAD-160703
19. Pu L, Moyle W, Jones C, Todorovic M. The effect of using PARO for people living with dementia and chronic pain: A pilot randomized controlled trial. J Am Med Dir Assoc. (2020) 21:1079–85. doi: 10.1016/j.jamda.2020.01.014
20. Valentï Soler M, Agþera-Ortiz L, Olazarãn Rodrïguez J, Mendoza Rebolledo C, Përez Muóoz A, Rodrïguez Përez I, et al. Social robots in advanced dementia. Front Aging Neurosci. (2015) 7:133. doi: 10.3389/fnagi.2015.00133
21. Kang Y, Jahng S, Kim SY. Korean-Mini Mental State Examination, (K-MMSE-2) user's guide: Inpsyt. Seoul: Hakjisa Publisher. (2020).
22. Folstein MF, Robins LN, Helzer JE. Mini Mental State Examination, 2nd Edn. Lutz: Psychological Assessment Resources, Inc. (2010).
23. Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. (1986) 5:165–73. doi: 10.1300/J018v05n01_09
24. Kee B-S. A preliminary study for the standardization of geriatric depression scale short form-Korea version. J Korean Neuropsychiatr Assoc. (1996) 35:298–307.
25. Russell D, Peplau LA, Cutrona CE. The revised UCLA Loneliness Scale: concurrent and discriminant validity evidence. J Pers Soc Psychol. (1980) 39:472. doi: 10.1037/0022-3514.39.3.472
26. Kim OS. Korean version of the revised UCLA loneliness scale: Reliability and validity test. J Nurses Acad Soc. (1997) 27:871–9. doi: 10.4040/jnas.1997.27.4.871
27. Lee Y-K, Nam H-S, Chuang L-H, Kim K-Y, Yang H-K, Kwon I-S, et al. South Korean time trade-off values for EQ-5D health states: modeling with observed values for 101 health states. Value Health. (2009) 12:1187–93. doi: 10.1111/j.1524-4733.2009.00579.x
28. Euroqol-Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy. (1990) 16:199–208. doi: 10.1016/0168-8510(90)90421-9
29. Andrews JS, Desai U, Kirson NY, Zichlin ML, Ball DE, Matthews BR. Disease severity and minimal clinically important differences in clinical outcome assessments for Alzheimer's disease clinical trials. Alzheimer's Dement. (2019) 5:354–63. doi: 10.1016/j.trci.2019.06.005
30. Otake-Matsuura M, Tokunaga S, Watanabe K, Abe MS, Sekiguchi T, Sugimoto H, et al. Cognitive Intervention Through Photo-Integrated Conversation Moderated by Robots (PICMOR) Program: A Randomized Controlled Trial. Front Robot AI. (2021) 8:54. doi: 10.3389/frobt.2021.633076
31. Park E-A, Jung A-R, Lee K-A. The Humanoid Robot Sil-Bot in a Cognitive Training Program for Community-Dwelling Elderly People with Mild Cognitive Impairment during the COVID-19 Pandemic: A Randomized Controlled Trial. Int J Environ Res Public Health. (2021) 18:8198. doi: 10.3390/ijerph18158198
32. Sawami K, Kimura M, Kitamura T, Kawaguchi M, Furusumi M, Suishu C, et al. Cognitive ability and psychological effectiveness of brain training dance robot therapy for elderly people. OA J Neuropsychiatry. (2019). doi: 10.33118/oaj.neuro.2019.01.004
33. Tanaka M, Ishii A, Yamano E, Ogikubo H, Okazaki M, Kamimura K, et al. Effect of a human-type communication robot on cognitive function in elderly women living alone. Med Sci Monit Int Med J Exp Clin Res. (2012) 18:CR550. doi: 10.12659/MSM.883350
34. Liang A, Piroth I, Robinson H, Macdonald B, Fisher M, Nater UM, et al. A pilot randomized trial of a companion robot for people with dementia living in the community. J Am Med Dir Assoc. (2017) 18:871–8. doi: 10.1016/j.jamda.2017.05.019
35. Kim C, Park M, Kim S. Analysis of trends in non-pharmacological studies for elders with dementia in Korea. J Korean Gerontol Nurs. (2012) 14:129–41.
36. Shin H, Chung S. Program development and evaluation of integrative play therapy for older people with suspected early dementia. J Play Ther. (2015) 19:95–109.
37. Oh J-H, Yi Y-J, Shin C-J, Park C, Kang S, Kim J, et al. Effects of silver-care-robot program on cognitive function, depression, and activities of daily living for institutionalized elderly people. J Korean Acad Nurs. (2015) 45:388–96. doi: 10.4040/jkan.2015.45.3.388
38. Robinson H, Macdonald B, Kerse N, Broadbent E. The psychosocial effects of a companion robot: a randomized controlled trial. J Am Med Dir Assoc. (2013) 14:661–7. doi: 10.1016/j.jamda.2013.02.007
39. Júranson N, Pedersen I, Rokstad AMM, Ihlebaek C. Effects on symptoms of agitation and depression in persons with dementia participating in robot-assisted activity: a cluster-randomized controlled trial. J Am Med Dir Assoc. (2015) 16:867–73. doi: 10.1016/j.jamda.2015.05.002
40. Miklõsi Á, KORONDI P, Matellãn V, Gãcsi M. Ethorobotics: A new approach to human-robot relationship. Front Psychol. (2017) 958. doi: 10.3389/fpsyg.2017.00958
41. Kanamori M, Suzuki M, Oshiro H, Tanaka M, Inoguchi T, Takasugi H, et al. Pilot study on improvement of quality of life among elderly using a pet-type robot. In: Proceedings 2003 IEEE International Symposium on Computational Intelligence in Robotics and Automation. Computational Intelligence in Robotics and Automation for the New Millennium (Cat. No. 03EX694), IEEE (2003). p. 107–112.
42. Banks MR, Willoughby LM, Banks WA. Animal-assisted therapy and loneliness in nursing homes: use of robotic versus living dogs. J Am Med Dir Assoc. (2008) 9:173–7. doi: 10.1016/j.jamda.2007.11.007
43. Victor C, Scambler S, Bond J, Bowling A. Being alone in later life: loneliness, social isolation and living alone. Rev Clin Gerontol. (2000) 10:407–17. doi: 10.1017/S0959259800104101
44. Singh A, Misra N. Loneliness, depression and sociability in old age. Ind Psychiatry J. (2009) 18:51. doi: 10.4103/0972-6748.57861
45. Mackenzie MJ, Chung HD, Zuniga KE, Woods JA, McAuley E. Multilevel modeling of exercise effects on loneliness in older adults. In: Annals of Behavioral Medicine, New York, NY: Springer (2014). p. S178–S178.
46. Júranson N, Pedersen I, Rokstad AMM, Ihlebaek C. Change in quality of life in older people with dementia participating in Paro-activity: A cluster-randomized controlled trial. J Adv Nurs. (2016) 72:3020–33. doi: 10.1111/jan.13076
Keywords: social robot, cognitive function, depression, loneliness, quality of life, older adults
Citation: Lim J (2023) Effects of a cognitive-based intervention program using social robot PIO on cognitive function, depression, loneliness, and quality of life of older adults living alone. Front. Public Health 11:1097485. doi: 10.3389/fpubh.2023.1097485
Received: 14 November 2022; Accepted: 23 January 2023;
Published: 06 February 2023.
Edited by:
Waqas Sami, Azra Naheed Medical College, PakistanReviewed by:
Xiaoyan Chen, Zigong City Mental Health Center, ChinaYuya Watanabe, Meiji Yasuda Life Foundation of Health and Welfare, Japan
Copyright © 2023 Lim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: JunSeo Lim,  anVuc2VvQHNudS5hYy5rcg==
anVuc2VvQHNudS5hYy5rcg==