 Tracey Ma
Tracey Ma Conrad Kobel2
Conrad Kobel2 Rebecca Ivers
Rebecca Ivers- 1School of Population Health, University of New South Wales, Sydney, NSW, Australia
- 2Australian Health Services Research Institute, University of Wollongong, Wollongong, NSW, Australia
Out-of-home mobility is fundamental to older people's wellbeing and quality of life. Understanding the unmet mobility needs of older people is a necessary starting point for determining how they can be supported to be mobile. This study estimates the extent of unmet mobility needs among older Australians and identifies the characteristics of those most likely to report unmet mobility needs. Analysis was conducted on nationally representative data of 6,685 older Australians drawn from the 2018 Survey of Disability, Aging and Carers conducted by the Australian Bureau of Statistics. Twelve predictor variables from two conceptual frameworks on older people's mobility were included in the multiple logistic regression model. Twelve percent (n = 799) of participants had unmet mobility needs, and associated factors significant in multivariable models included being among the “young-old”, having a lower income, having lower levels of self-rated health, having a long-term condition, being limited in everyday physical activities, experiencing a higher level of distress, being unlicensed, having decreased public transport ability, and residing in major cities. Efforts to support older people's mobility must make equity an explicit consideration, reject a one-size-fits-all approach, and prioritize the accessibility of cities and communities.
1. Introduction
Older people's “ability to move about the city” for the purposes of “social and civic participation and access to community and health services” is paramount to, what the World Health Organization calls, an age-friendly society (1). Indeed, older people's out-of-home mobility is an important contributor to their wellbeing and quality of life (2–4), enabling their access to activities that facilitate health, such as health care services (5), and support their connection to community, such as leisure and social activities (6, 7). Moreover, regardless of the types of out-of-home activities pursued, the act of getting out and about is valued by older people and perceived to be a contributor to their wellbeing (8).
However, while out-of-home mobility is fundamental to the wellbeing of older people, older people's life circumstances pose challenges to their mobility. On average, older people have more leisure time, expanding their opportunities for out-of-home activity participation and out-of-home mobility (9, 10), but less financial resources, which can restrict those opportunities (9). Within this group though, there is much heterogeneity—more so than among young and middle-aged adults—due to individually-specific age-related changes in activity patterns, daily routines, and physiological and psychosocial processes (11, 12). As such, whole-of-population approaches to studying mobility, such as travel behavior modeling aimed at system-level planning, are insufficient for understanding older people's mobility (9). Rather, explicit attention is needed to understand the intricacies of mobility in older age and identify the unique considerations for supporting older people to be mobile.
Existing research on older people's mobility focuses heavily on travel behavior, providing a rich knowledge base for understanding the modes of transportation used (10, 13–15), the factors affecting their use (15–19), and the details of their use (14, 18, 20). Such information is useful for understanding how to support older people's existing modal choices and travel patterns and/or facilitate modal shifts. For example, information on average walking distances of older people may motivate changes to the urban environment to facilitate more active transport use by older people for trips within that distance, with physical activity benefits in mind (13). Likewise, understanding the barriers to public transport use among older people who chose to travel by car can support initiatives to make public transport more attractive to them, especially as they transition away from driving (15). The limitation of such information, however, is that it only captures the segment of the older population who is already mobile and theoretically reaping the wellbeing benefits associated with out-of-home mobility.
Another focus of research on older people's mobility is directed at understanding and identifying transport disadvantage, typically using indicative measures (21, 22) and often in select geographic locations (13, 14, 17, 21, 22). Transport disadvantage research complements travel behavior research by focusing on those not already mobile, at all or to the fullest extent, due to out-of-home mobility difficulties. Transport disadvantage can be indirectly inferred from trip rates (23), household spending on fuel (23), distance or travel time to services (21), levels of car ownership (24), and public transport service levels (25–28). However, while these measures are indicative, they do not directly measure if and the extent to which older people experience out-of-home mobility difficulty. Households that would otherwise be considered “transport disadvantaged” based on the indicators of income and car ownership are not necessarily disadvantaged, as household members may make deliberate decisions about their mobility and location and be well situated to manage their circumstances (24). Indicative measures of “transport disadvantage”, therefore, may not necessarily correspond with actual experiences of out-of-home mobility difficulty.
An alternative approach to examining older people' out-of-home mobility difficulty is to focus on unmet mobility needs. Unmet mobility needs are mobility needs that are unfulfilled due to difficulties accomplishing journeys or activities (29). When self-reported, it captures actual experiences of out-of-home mobility difficulty (30). Studies of older people in England, Norway, Finland, and the United States have examined unmet mobility needs using self-reported measures from nation-wide surveys (9, 30–33). Building on these international studies, this study aims to estimate the extent of unmet mobility needs in the older Australian population and identify the characteristics of older people who are most likely to have unmet mobility needs. Using self-reported measures from a nation-wide survey, this study regards unmet mobility needs to exist when people indicate that they would like to leave home more often than they actually do. This study extends earlier work by using two externally developed conceptual frameworks to guide variable selection and applying them to the largest sample size yet.
2. Materials and methods
Analysis was conducted on data from 6,685 community-dwelling older people (age 65 years or older) from the 2018 Survey of Disability, Aging and Carers (SDAC). The SDAC is a cross-sectional population survey conducted by the Australian Bureau of Statistics (ABS) (34). This survey was conducted from July 2018 to March 2019. The SDAC collects information from people with a disability, older people, and carers of older people and people with disabilities. Households are randomly selected and represent others in that area, in that State, and in Australia. Participation is mandatory for selected households to ensure a representative sample, as per the Census and Statistics Act 1905. Participation involves a face-to-face survey interview with an ABS interviewer. Participants were included in this analysis if they provided complete data. As this study uses secondary data, ethical approval of research was not required.
Analysis involved a multiple logistic regression model in which the outcome variable indicating unmet mobility needs was operationalized as “whether leaves home as often as would like”. Variable values were either “leaves home as often as would like” (i.e., No, there are no unmet mobility needs) or “leaves home, but not as often as would like” (i.e., Yes, there are unmet mobility needs). Twelve predictor variables were included in the model: age, sex, marital status (whether legally or de facto married), main language at home, weekly income, self-rated health, presence of a long-term condition, whether limited in everyday physical activities, level of distress (based on the Kessler Psychological Distress Scale), license status, public transport ability, and residential location.
The inclusion of these variables were supported by two conceptual frameworks: Luiu's framework for assessing unmet travel needs in later life (35) and Webber's framework of the determinants of mobility in older age (36) (see Table 1). Luiu's framework (35) was developed specifically to guide investigations into unmet mobility needs in later life with the suggestion that consideration of all five domains is necessary. These domains were derived from a three-step process: a literature review identifying 14 studies directly addressing factors affecting unmet mobility needs, a methodology assessment of each study, and a content analysis of each study for themes influencing mobility in later life. Webber's framework (36) was developed to overcome discipline-specific and disjointed portrayals of mobility in older age by proposing a comprehensive and interdisciplinary framework that links multiple categories of mobility determinants with multiple life-space locations with multiple means of mobility. It comprises five categories of determinants and has been found to acceptably fit data from a US national sample of older adults (37).
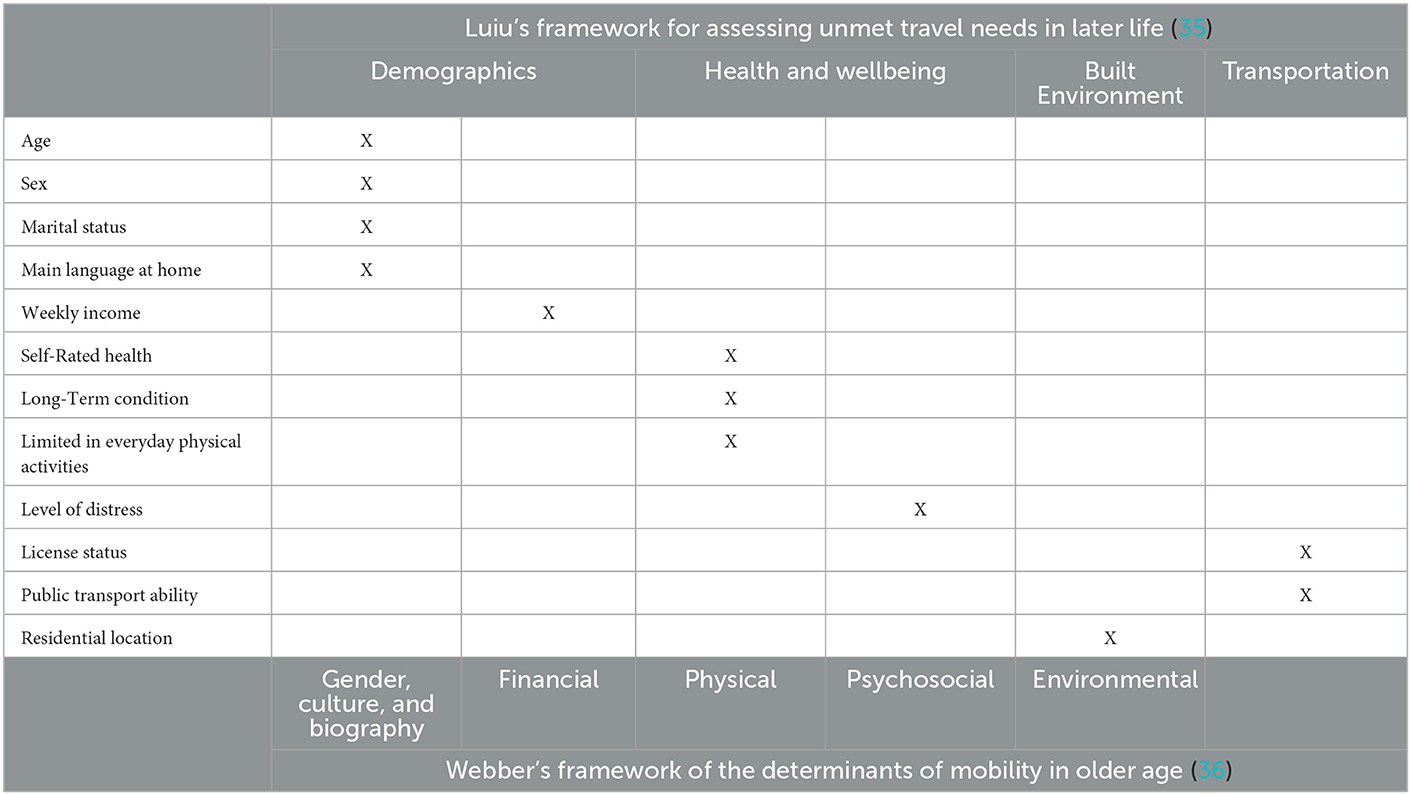
Table 1. Predictor variables.
The glm() function with a logit link function was used to fit the model using the RStudio (v1.1.423) interface for R (v4.0.2). Model results are presented using the tbl_regression() function of the {gtsummary} package (38), in which odds ratios (OR) were calculated by exponentiating model coefficients. The 95% confidence intervals (CI) calculated by the tbl_regression() function are consistent with those generated using the confint() function, which produces CIs based on the log-likelihood function. Results were considered statistically significant if the corresponding CIs do not include the null value. The Nagelkerke pseudo R-squared value was 0.3. The presence of multicollinearity was checked using the Variance Inflation Factor (VIF) with a cut-off of five. Multicollinearity was not present as the highest VIF value was 1.4.
3. Results
The majority of study participants were aged 65–75 (60%), married (64%), spoke English as their main language at home (93%), and had a weekly income of $500 or less (60%). There were slightly more females (52%) than males. Most of them had a long-term condition (87%), experienced low to moderate levels of distress (90%), and were not limited in everyday physical activities (80%). A similar proportion had excellent or very good self-rated health (49%) or good or fair self-rated health (47%). Most participants were licensed (89%) and were able to take all forms of public transport (88%). Participants primarily resided in major cities (62%). Of the 6,685 people included in the study, 96% (n = 6,417) left home in the last 2 weeks. Sample characteristics are presented in Table 2.
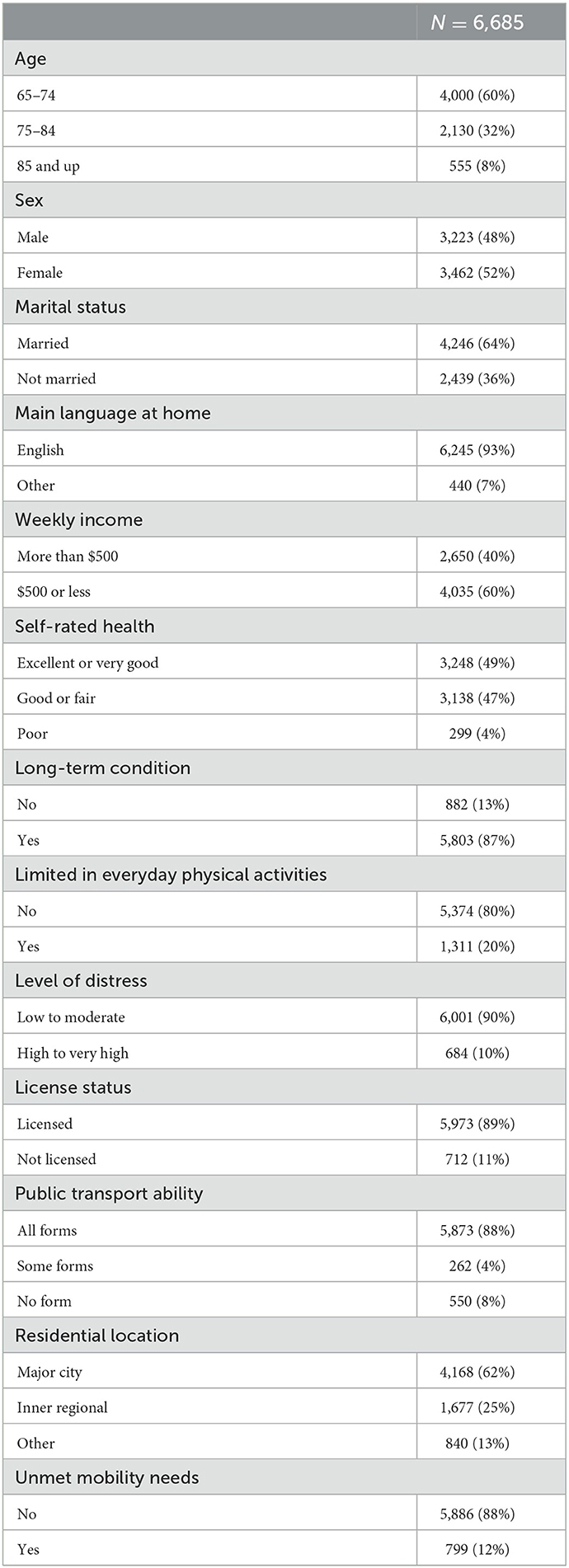
Table 2. Sample characteristics.
Of the 6,685 people included in the study, 799 (12%) reported unmet mobility needs. Among those with unmet mobility needs, more were among the “young–old” (aged 65–74) (56%), female (56%), married (56%), English speaking (91%), and had a weekly income of $500 or less (74%). Additionally, those with good or fair self-rated health (62%), who had a long-term condition (96%), who were limited in everyday physical activities (52%), and who experienced low to moderate levels of distress (65%) were more represented among those with unmet mobility needs. There was also a greater proportion of people with unmet mobility needs who were licensed (74%), were able to take all forms of public transport (65%), and who live in major cities (65%).
Results of the regression analysis are presented in Table 3, with significant values in bold. The model indicates that, when adjusted for other predictors in the model, the following are significantly associated with having unmet mobility needs: being among the “young–old” (aged 65–74), having a lower weekly income, having lower levels of self-rated health, having a long-term condition, being limited in everyday physical activities, experiencing a higher level of distress, being unlicensed, having decreased public transport ability, and residing in major cities. Age, sex, marital status, main language at home, and weekly income are all independently associated with having unmet mobility needs, with the exception of the middle age bracket. However, only age and weekly income remain significant when adjusted. Moreover, when adjusted, their estimated effect diminishes and, for some, reverses direction. Self-rated health, presence of a long-term condition, whether limited in everyday physical activities, and level of distress remain significantly associated with having unmet mobility needs after adjustment, but with a greatly diminished effect. Likewise for license status and public transport ability. For residential location, the “inner regional” value becomes significant after adjustment.
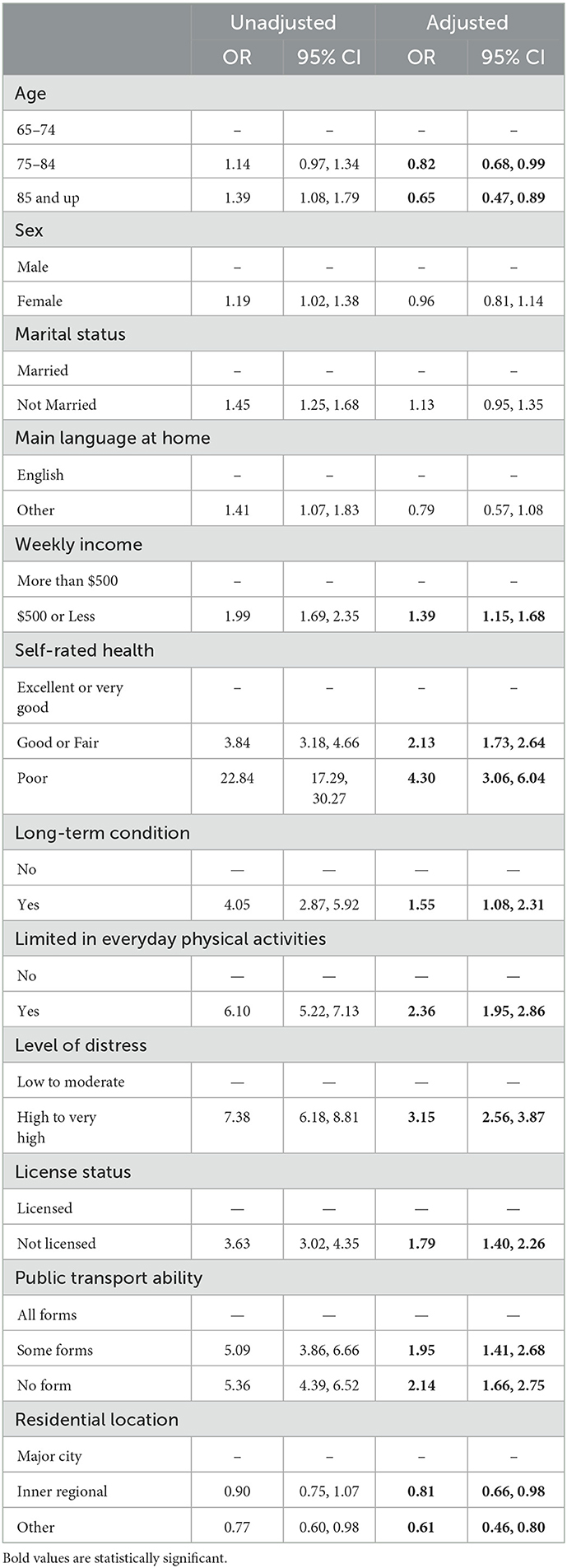
Table 3. Regression analysis of unmet mobility needs.
4. Discussion
Using 2018 data from a population-wide survey of 6,685 older people, this study estimated the extent of unmet mobility needs in the older Australian population and identified the characteristics of those most likely to report unmet mobility needs. This study found that 12% of participants had unmet mobility needs¾ reporting that they would like to leave home more often than they actually do¾, despite the vast majority (96%) of participants already demonstrating some degree of mobility, having left home in the last 2 weeks.
Of the demographic variables, younger age and lower weekly income were found to be independently associated with unmet mobility needs. The presence of an age effect contrasts with similar studies in the United States (30), Norway (31) and England (32), which found no significant age effect after adjustment. The direction of the age effect might be explained by the “young–old” having more out-of-home mobility needs than the older age groups (39), making it harder for them to fulfill those needs and more likely to have unmet mobility needs. Compared to the older age groups, the “young–old” may also be less likely to have supports in place, such as through government funded home care services (40), increasing their likelihood of having unmet mobility needs. Surprisingly, sex is not associated with unmet mobility needs. Although international studies have reported inconsistent results in this regard (30, 31), the expectation that women are more likely to have unmet mobility needs is supported by their tendency to cease driving earlier than men (41), self-regulate their driving more than men (42), and experience more travel difficulties than men (32). However, previous research has also shown that women are more educated, independent, and self-sufficient now than previous generations (43), and, thus, they may find ways to fulfill their mobility needs regardless.
All health and wellbeing variables were independently associated with having unmet mobility needs. This is telling as, together, they capture various dimensions of health and wellbeing (35), both objectively—i.e., presence or absence of a long-term condition and physical limitation—and subjectively—i.e., appraisal of general health and psychological health using well-validated measures (44–47). As health issues can impede all means of mobility (modes of transportation) (48), the association between unmet mobility needs and having lower levels of self-rated health, having a long-term condition, being limited in everyday physical activities, and experiencing a higher level of distress is not surprising. In fact, a systematic review on the unmet mobility needs of older people noted that, despite ambiguity across the literature regarding other predictors, health issues are consistently reported to affect older people's mobility needs (29).
Regarding the built environment and transportation variables, being unlicensed, having decreased public transport ability, and residing in major cities were each independently associated with unmet mobility needs. The link between being unlicensed and having unmet mobility needs is consistent with previous studies that have examined this relationship specifically (9, 31), or the relationship between unmet mobility needs and other indicators of car access/use such as vehicle ownership (32) or driving frequency (30). The link between decreased public transport ability and unmet mobility needs is expected, as, similar to license ownership, public transport ability is indicative of having a particular transport mode at one's disposal, which increases one's ability to fulfill mobility needs. As health affects the ability to take public transport (49), one might expect the effect of public transport ability to disappear after adjusting for the health and wellbeing variables. However, this is not the case, suggesting that this “public transport ability” variable captures something other than health status. One explanation might be found in a study of older people's relationship to public transport, which explored how individuals differed in the extent to which they take ownership over their mobility resources (i.e., elements of their life that enable mobility such as health) and “convert” them into mobility capabilities (i.e., resources that can be deployed to support mobility) (50). It found mobility capabilities, not mobility resources alone, to lead to public transport use. In other words, it is not people's health per se that affects their ability to take public transport, but rather their evaluation of their health. Thus, this “public transport ability” variable may capture that evaluative mechanism (relating health specifically to public transport) while the health and wellbeing variables capture actual health (in general).
The finding that residence in major cities is associated with unmet mobility needs contrasts with findings from Finland (9) and the United States (30), showing an effect in the opposite direction, as well as that from Norway (31) and England (32), showing no location effect after adjustment. Our findings might be explained by the possibility that older people residing outside major cities have adjusted their out-of-home mobility needs to match the availability of amenities in their location. This leads them to have fewer out-of-home mobility needs compared to their urban dwelling counterparts, making it easier for them to fulfill those needs and resulting in them being less likely to have unmet mobility needs. A caveat to our finding, though, is that the residential location variable might be too coarse of a measure, having only three broad values and acting as a proxy for several pieces of information including urban connectivity, public transport availability, and availability of destinations. For example, residents of the City of Sydney, all of whom would be considered to reside in a “major city”, experience much variation in public transport service levels depending on the specific suburb in which they reside (51).
This study demonstrates that realized mobility, the focus of travel behavior research, and unmet mobility needs are two separate phenomena. In other words, a person or population may be “highly” mobile yet still have unmet mobility needs, as evidenced here. The finding that 96% of participants left home in the last two weeks may seem to suggest that out-of-home mobility is not a problem in this group. However, as other findings demonstrate, this is not the case. In some respects, the use of a 2 week time frame for calculating out-of-home mobility conceals the possibility that unmet mobility needs exist, as a high prevalence (96%) is more likely to be calculated within a wide time frame and the higher the prevalence of out-of-home mobility, the less attention is paid to unmet mobility needs. Two weeks could be considered too wide a time frame if one reflects on whether leaving home once in 2 weeks is typical of or sufficient for most people. Thus, this finding should not be overstated. This observation speaks to the limitation of using data from a routine survey, as questions are not fit-for-purpose.
This limitation also extends to the outcome measure, which, as it is operationalized, requires participants to hold two pieces of information in their heads (how often they would like to leave home and how often they actually leave home) and make a comparison between the two. The cognitive effort required to perform such a mental task may reduce the accuracy of the response (52). And this may explain why the prevalence of having unmet mobility needs among participants (12%) is lower than what is expected from the literature (~30%) (29). In contrast, a similar study in Birmingham, UK operationalized unmet mobility needs as “whether there are times when [you] cannot make the trips wanted” (48). It is conceivable that many would answer in the affirmative given the wording of the question. Thus, the operationalization of the outcome measure in this study may result in a conservative estimate of the extent of unmet mobility needs in the older Australian population. Regardless, there is a distinct pattern regarding the characteristics of older Australians most likely to report unmet mobility needs. A strength of this study is the inclusion of a range of measures covering different aspects of older people's mobility, as informed by the literature (35, 36), and the analysis of such measures on a large random sample of older Australians. However, as the survey was cross-sectional in nature, all factors were measured simultaneously, precluding inferences about the temporal link between predictor variables and the outcome of having unmet mobility needs.
Several conclusions arise from the findings. The first conclusion is that equity needs to be an explicit consideration, as older people with fewer personal resources are more likely to have unmet mobility needs. This is evidenced by our findings of higher odds of unmet mobility needs among older people with lower income, diminished health, and fewer transport resources¾ by virtue of being unlicensed or having decreased public transport ability. Notably, diminished health refers not only to physical ability (i.e., whether limited in everyday physical activities), but also to general health and wellbeing (i.e., self-rated health) and psychological health (i.e., level of distress). A second conclusion is that it is health more so than age that is predictive of unmet mobility needs. This is evidenced by the effect size of age being smaller than that of the health and wellbeing variables, supporting previous findings that the health of older people varies widely even among those of the same age group (53). The association between health and unmet mobility needs cannot be understated, as those with poor self-rated health have approximately four times (OR 4.30, 95% CI 3.06–6.04) the odds of having unmet mobility needs compared to those with excellent or very good self-rated health. The implication of this is that efforts to support older people's mobility cannot assume a one-size-fits-all approach and instead needs to be targeted to and inclusive of older people of all levels of health. Further, there is a need to improve the accessibility of cities and communities, such that public transport becomes a feasible option and residential location will no longer be a determining factor in having unmet mobility needs. This also helps to ensure that older people, regardless of their health status, are able to move about the city. This is especially important given Australia and many countries' commitment to aging in place, which prioritizes older people's continued residence in the community rather than in residential aged care.
Although studied internationally, unmet mobility needs have received limited attention in Australia due to a predominant focus on travel behavior and indicative transport disadvantage. By examining unmet mobility needs, this study directly addresses the issue of out-of-home mobility difficulty among older people by estimating its scale and identifying its predictors. Understanding the scale of the issue can inform policy interventions that aim to facilitate a minimum level of fulfilled mobility needs (3, 31). Understanding the predictors can inform policy interventions to be more effective, by considering the dimensions of the issue.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: availability limited to subscribing organizations. Requests to access these datasets should be directed to Australian Bureau of Statistics.
Author contributions
Conceptualization and methodology: TM, CK, and RI. Software, formal analysis, investigation, data curation, writing—original draft preparation, visualization, and project administration: TM. Writing—review and editing and supervision: CK and RI. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by the UNSW Scientia Scholarship Scheme. The funder was not involved in the design and conduct of the research nor in the preparation of the manuscript.
Acknowledgments
The authors would like to acknowledge the following individuals from the Australian Bureau of Statistics for their assistance with accessing and understanding the data: Talei Parker, Lisa Commens, and Penny Boyd.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Global age-friendly cities: a guide (2007). Available from: http://www.who.int/ageing/publications/age_friendly_cities_guide/en/ (accessed on February 14, 2019).
2. Spinney JEL, Scott DM, Newbold KB. Transport mobility benefits and quality of life: A time-use perspective of elderly Canadians. Transport Policy. (2009) 16:1–11. doi: 10.1016/j.tranpol.2009.01.002
3. Nordbakke S, Schwanen T. Well-being and mobility: a theoretical framework and literature review focusing on older people. Mobilities. (2014) 9:104–29. doi: 10.1080/17450101.2013.784542
4. Pantelaki E, Maggi E, Crotti D. Mobility impact and well-being in later life: A multidisciplinary systematic review. Res Transport Econ. (2020) 2020:100975. doi: 10.1016/j.retrec.2020.100975
5. van Gaans D, Dent E. Issues of accessibility to health services by older Australians: a review. Public Health Rev. (2018) 39:20. doi: 10.1186/s40985-018-0097-4
6. Siren A, Hjorthol R, Levin L. Different types of out-of-home activities and well-being amongst urban residing old persons with mobility impediments. J Transp Health. (2015) 2:14–21. doi: 10.1016/j.jth.2014.11.004
7. Fields N, Cronley C, Mattingly SP, Murphy ER, Miller VJ. “You Are Really at Their Mercy”: examining the relationship between transportation disadvantage and social exclusion among older adults through the use of innovative technology. Transp Res Rec. (2019) 2673:12–24. doi: 10.1177/0361198119839969
8. Musselwhite C. Exploring the importance of discretionary mobility in later life. Work Older People. (2017) 21:49–58. doi: 10.1108/WWOP-12-2016-0038
9. Siren A, Hakamies-Blomqvist L. Private car as the grand equaliser? Demographic factors and mobility in Finnish men and women aged 65+. Transp Res Part F: Traff Psychol Behav. (2004) 7:107–18. doi: 10.1016/j.trf.2004.02.003
10. Kim S, Ulfarsson GF. Travel mode choice of the elderly: effects of personal, household, neighborhood, and trip characteristics. Transp Res Rec. (2004) 1894:117–26. doi: 10.3141/1894-13
11. Cagney KA, Cornwell EY. Neighborhoods and health in later life: the intersection of biology and community. In: Annual Review of Gerontology and Geriatrics New York (2010).
12. Kawachi I, Berkman LF. Neighborhoods, Aging, and Functional Limitations. In: Neighborhoods and Health. Oxford, UK: Oxford University Press (2003). Available from: http://www.oxfordscholarship.com/view/10.1093/acprof:oso/9780195138382.001.0001/acprof-9780195138382-chapter-14 (accessed on March 25, 2019).
13. O'Hern S, Oxley J. Understanding travel patterns to support safe active transport for older adults. J Transp Health. (2015) 2:79–85. doi: 10.1016/j.jth.2014.09.016
14. Engels B, Liu GJ. Ageing in Place: The Out-of-Home Travel Patterns of Seniors in Victoria and its Policy Implications. Urban Policy Res. (2013) 31:168–89. doi: 10.1080/08111146.2012.737316
15. Buys L, Snow S, Megen K. van, Miller E. Transportation behaviours of older adults: An investigation into car dependency in urban Australia. Austr J Ageing. (2012) 31:181–6. doi: 10.1111/j.1741-6612.2011.00567.x
16. Shrestha BP, Millonig A, Hounsell NB, Mcdonald M. Review of public transport needs of older people in European context. J Popul Ageing Dordrecht. (2017) 10:343–61. doi: 10.1007/s12062-016-9168-9
17. Truong LT, Somenahalli SVC. Exploring frequency of public transport use among older adults: A study in Adelaide, Australia. Travel Behav Soc. (2015) 2:148–55. doi: 10.1016/j.tbs.2014.12.004
18. Hensher DA. Some insights into the key influences on trip-chaining activity and public transport use of seniors and the elderly. Int J Sustain Transp. (2007) 1:53–68. doi: 10.1080/15568310601097004
19. Lee JS, Zegras PC, Ben-Joseph E. Safely active mobility for urban baby boomers: The role of neighborhood design. Acc Anal Prev. (2013) 61:153–66. doi: 10.1016/j.aap.2013.05.008
20. Habib KMN, Hui V. An activity-based approach of investigating travel behaviour of older people: Application of a time–space constrained scheduling model (CUSTOM) for older people in the National Capital Region (NCR) of Canada. Transportation. (2017) 44:555–73. doi: 10.1007/s11116-015-9667-1
21. Engels B, Liu GJ. Social exclusion, location and transport disadvantage amongst non-driving seniors in a Melbourne municipality, Australia. J Transp Geogr. (2011) 19:984–96. doi: 10.1016/j.jtrangeo.2011.03.007
22. Lange J, Norman P. Quantifying service accessibility/transport disadvantage for older people in non-metropolitan South Australia. Appl Spatial Anal. (2018) 11:1–19. doi: 10.1007/s12061-016-9206-2
23. Li T, Dodson J, Sipe N. Differentiating metropolitan transport disadvantage by mode: Household expenditure on private vehicle fuel and public transport fares in Brisbane, Australia. J Transp Geogr. (2015) 49:16–25. doi: 10.1016/j.jtrangeo.2015.10.001
24. Currie G, Richardson T, Smyth P, Vella-Brodrick D, Hine J, Lucas K, et al. Investigating links between transport disadvantage, social exclusion and well-being in Melbourne—Updated results. Res Transp Econ. (2010) 29:287–95. doi: 10.1016/j.retrec.2010.07.036
25. Pittman N, Day JE. Locating and quantifying public transport provision with respect to social need in Canberra, Australia. Aust Plann. (2015) 52:326–36. doi: 10.1080/07293682.2015.1101007
26. Scheurer J, Curtis C, McLeod S. Spatial accessibility of public transport in Australian cities: Does it relieve or entrench social and economic inequality? JTLU. (2017) 10:911–30. doi: 10.5198/jtlu.2017.1097
27. Currie G. Quantifying spatial gaps in public transport supply based on social needs. J Transp Geogr. (2010) 18:31–41. doi: 10.1016/j.jtrangeo.2008.12.002
28. Currie G. Gap analysis of public transport needs: measuring spatial distribution of public transport needs and identifying gaps in the quality of public transport provision. Transp Res Rec. (2004) 1895:137–46. doi: 10.3141/1895-18
29. Luiu C, Tight M, Burrow M. The unmet travel needs of the older population: a review of the literature. Transp Rev. (2017) 37:488–506. doi: 10.1080/01441647.2016.1252447
30. Kim S. Assessing mobility in an aging society: Personal and built environment factors associated with older people's subjective transportation deficiency in the US. Transp Res Part F: Traff Psychol Behav. (2011) 14:422–9. doi: 10.1016/j.trf.2011.04.011
31. Nordbakke S, Schwanen T. Transport, unmet activity needs and wellbeing in later life: exploring the links. Transportation. (2015) 42:1129–51. doi: 10.1007/s11116-014-9558-x
32. Luiu C, Tight M. Travel difficulties and barriers during later life: Evidence from the National Travel Survey in England. J Transp Geogr. (2021) 91:102973. doi: 10.1016/j.jtrangeo.2021.102973
33. Hjorthol R. Transport resources, mobility and unmet transport needs in old age. Ageing Soc. (2013) 33:1190–211. doi: 10.1017/S0144686X12000517
34. Australian Bureau of Statistics. Survey of Disability, Ageing and Carers. (2018). Available from: https://www.abs.gov.au/statistics/microdata-tablebuilder/available-microdata-tablebuilder/disability-ageing-and-carers-australia (accessed on October 18, 2022).
35. Luiu C, Tight M, Burrow M, A. conceptual framework to assess the unmet travel needs in later life. J Transp Health. (2018) 9:321–31. doi: 10.1016/j.jth.2018.04.002
36. Webber SC, Porter MM, Menec VH. Mobility in Older Adults: A comprehensive framework. Gerontologist. (2010) 50:443–50. doi: 10.1093/geront/gnq013
37. Umstattd Meyer MR, Janke MC, Beaujean AA. Predictors of older adults' personal and community mobility: using a comprehensive theoretical mobility framework. Gerontologist. (2014) 54:398–408. doi: 10.1093/geront/gnt054
38. Sjoberg D, Whiting K, Curry M, Lavery J, Larmarange J. Reproducible summary tables with the gtsummary package. R J. (2021) 13:570–80. doi: 10.32614/RJ-2021-053
39. Alsnih R, Hensher DA. The mobility and accessibility expectations of seniors in an aging population. Transp Res Part A: Policy Pract. (2003) 37:903–16. doi: 10.1016/S0965-8564(03)00073-9
40. Khadka J, Lang C, Ratcliffe J, Corlis M, Wesselingh S, Whitehead C, et al. Trends in the utilisation of aged care services in Australia, 2008–2016. BMC Geriatr. (2019) 19:213. doi: 10.1186/s12877-019-1209-9
41. Choi M, Mezuk B, Lohman MC, Edwards J, Rebok GW. Gender and racial disparities in driving cessation among older adults. J Aging Health. (2012) 24:1364–79. doi: 10.1177/0898264312460574
42. Charlton JL, Oxley J, Fildes B, Oxley P, Newstead S. Self-Regulatory Behaviours of Older Drivers. Annu Proc Assoc Adv Automot Med. (2003) 47:181–94.
43. Coughlin JF. Longevity, lifestyle, and anticipating the new demands of aging on the transportation system. Public Works Manage Policy. (2009) 13:301–11. doi: 10.1177/1087724X09335609
44. Furukawa TA, Kessler RC, Slade T, Andrews G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol Med. (2003) 33:357–62. doi: 10.1017/S0033291702006700
45. Schnittker J, Bacak V. The Increasing Predictive Validity of Self-Rated Health. PLoS ONE. (2014) 9:e84933. doi: 10.1371/journal.pone.0084933
46. Slade T, Grove R, Burgess P. Kessler Psychological Distress Scale: normative data from the 2007 Australian national survey of mental health and wellbeing. Aust N Z J Psychiatry. (2011) 45:308–16. doi: 10.3109/00048674.2010.543653
47. Wuorela M, Lavonius S, Salminen M, Vahlberg T, Viitanen M, Viikari L. Self-rated health and objective health status as predictors of all-cause mortality among older people: a prospective study with a 5-, 10-, and 27-year follow-up. BMC Geriatr. (2020) 20:120. doi: 10.1186/s12877-020-01516-9
48. Luiu C, Tight M, Burrow M. An investigation into the factors influencing travel needs during later life. J Transp Health. (2018) 11:86–99. doi: 10.1016/j.jth.2018.10.005
49. Fatima K, Moridpour S. Measuring public transport accessibility for elderly. MATEC Web Conf. (2019) 259:03006. doi: 10.1051/matecconf/201925903006
50. Ryan J, Wretstrand A, Schmidt SM. Exploring public transport as an element of older persons' mobility: a capability approach perspective. J Transp Geogr. (2015) 48:105–14. doi: 10.1016/j.jtrangeo.2015.08.016
51. Qi Z, Lim S, Hossein Rashidi T. Assessment of transport equity to Central Business District (CBD) in Sydney, Australia. Transport Lett. (2020) 12:246–56. doi: 10.1080/19427867.2019.1584694
52. Brosnan K, Grün B, Dolnicar S. Cognitive load reduction strategies in questionnaire design. Int J Mark Res. (2021) 63:125–33. doi: 10.1177/1470785320986797
Keywords: healthy aging, transport mobility, community mobility, healthy city, age-friendly city
Citation: Ma T, Kobel C and Ivers R (2023) Older people's out-of-home mobility and wellbeing in Australia: Personal, built environment, and transportation factors associated with unmet mobility needs. Front. Public Health 11:1121476. doi: 10.3389/fpubh.2023.1121476
Received: 11 December 2022; Accepted: 19 January 2023;
Published: 20 February 2023.
Edited by:
Na Ta, East China Normal University, ChinaCopyright © 2023 Ma, Kobel and Ivers. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tracey Ma,  dHJhY2V5Lm1hQHVuc3cuZWR1LmF1
dHJhY2V5Lm1hQHVuc3cuZWR1LmF1