 María Dolores Salas-González1*
María Dolores Salas-González1* Laura M. Bermejo2
Laura M. Bermejo2 Liliana G. González-Rodríguez1
Liliana G. González-Rodríguez1 María Del Carmen Lozano-Estevan1
María Del Carmen Lozano-Estevan1 Rosa M. Ortega2
Rosa M. Ortega2 Ana M. López-Sobaler2
Ana M. López-Sobaler2- 1Grupo de Investigación VALORNUT, Departamento de Nutrición y Ciencia de los Alimentos, Facultad de Farmacia, Universidad Complutense de Madrid, Madrid, Spain
- 2Grupo de Investigación VALORNUT, Departamento de Nutrición y Ciencia de los Alimentos, Facultad de Farmacia, Universidad Complutense de Madrid, Instituto de Investigación Sanitaria del Hospital Clínico San Carlos (IdISSC), Madrid, Spain
Introduction: Being more active, being less sedentary, and sleeping enough are associated with adequate body weight and adiposity in children. However, few researchers have analyzed these different lifestyle behaviors and the adherence to 24 h movement guidelines with respect to insulin resistance (IR) at school age. Therefore, we aimed to analyse the association between the adherence to 24 h movement guidelines (physical activity, sedentary time, sleep) and IR in Spanish schoolchildren.
Methods: A cross-sectional study of 839 children (8–13 years, 51.1% girls) were studied. Anthropometric, biochemical, and lifestyle behavioral data were collected. IR was defined as HOMA-IR>3.16. Compliance with the 24 h movement guidelines were defined as ≥60 min/day of moderate and/or vigorous physical activity, <120 min/day of screen time, and 9–11 h/day of sleep time. Associations between adherence to the 24 h movement guidelines and IR were performed by multivariate logistic regression analyses.
Results: The IR in our sample was 5.0%, being higher in girls. Compliance with physical activity or screen time, but not with sleep recommendations, was associated with lower fasting glucose, fasting insulin, and HOMA-IR values. A low adherence to 24 h movement guidelines was associated with a higher risk of IR (odds ratio (95% CI): 2.150 [1.089–4.247]), especially in girls (odds ratio (95% CI): 2.800 [1.180–6.645]).
Conclusion: Higher physical activity levels and lower screen times were associated with a lower risk of IR in schoolchildren, underlining the importance of adhering to as many healthy lifestyle recommendations as possible.
1. Introduction
Insulin resistance (IR) plays an important role in the pathogenesis of comorbid diseases associated with obesity, such as type 2 diabetes mellitus, coronary heart disease, and metabolic syndrome (1). IR has been reported as early as childhood and has been associated in children with alterations in other health parameters, such as dyslipidaemia or elevated blood pressure (2, 3).
There is a growing body of evidence to show the positive associations between different aspects related to the movement [sufficient physical activity (4), limited screen time (5), and appropriate sleep duration (6)] with the children and adolescent health.
Several studies have linked moderate and/or vigorous physical activity (MVPA) with a higher quality of life, better health status, and a lower prevalence of cardiometabolic diseases during school age and adolescence (4, 7–10).
Although an increased sedentary lifestyle has typically been associated with a lack of physical activity, the two can coexist dependently or independently (11). Regardless of physical activity, sedentary behavior has been associated with leading causes of mortality and risk of chronic diseases such as cardiovascular disease and type 2 diabetes mellitus (12, 13). Finally, sedentary behaviors such as TV watching, computer use and general screen time are common behaviors in childhood and adolescence, which are associated with increased body weight and alterations in lipid and glycemic profile (8).
Moreover, associations have been found between sleep deprivation and decreased insulin sensitivity, unhealthy eating habits, sedentary lifestyles, and overweight or obesity (6, 14, 15). Similarly, good sleep habits have also been shown to be a fundamental aspect of human health during all periods of life (16).
MVPA, decreased sedentary activities and adequate sleep duration and quality have been associated in adult reviews and meta-analyses with better weight status, lower RI, lower likelihood of type 2 diabetes mellitus and even lower mortality in several types of cardiovascular disease (17, 18). Furthermore, the relationship between these three aspects of lifestyle and body weight status and adiposity in children and adolescents is well-established (19–21).
Based on the evidence on child health, some organizations such as the World Health Organization have proposed recommendations on physical activity for children and adolescents (at least 60 min of moderate and/or vigorous physical activity) (22). The American Academy of Sleep Medicine has also proposed recommendations on adequate sleep for proper health (9–12 h per day for schoolchildren aged 6–12 years and 8–10 h per day for adolescents aged 13–18 years) (23). Moreover, Tremblay et al. (24) developed 24-h movement guidelines for children and youth, which integrated recommendations of three patterns: physical activity (at least 60 min of MVPA), sedentary time (< 120 min/day of screen time), and sleep duration (9–11 h/day) (24). Adherence to these guidelines has been associated with lower cardiometabolic risk (25) and overall health in children and adolescents (26, 27).
However, the relationship between different lifestyle patterns, separately and especially in combination, and IR at school-age has not been sufficiently studied, and the relationship remains unclear. Therefore, our aim with this study was to evaluate the lifestyle patterns of a group of Spanish schoolchildren and to analyze the association between the adherence to specific 24 h movement guidelines or a combination of them and IR at school age in order to contribute knowledge in this area and to evaluate the association between lifestyle and IR at school age.
2. Methods
2.1. Study sample
The cross-sectional observational study included a convenience sample of schoolchildren aged 8–13 years from five Spanish provinces (A Coruña, Barcelona, Madrid, Sevilla, and Valencia) (Figure 1). In each province, we randomly selected schools from a list of primary schools with at least two classes per grade. We contacted the management teams of 55 schools by telephone, and we arranged an interview to explain the characteristics and objectives of the study. Once we had obtained permission from the management teams (22 schools), we called the families of the children with ages in the target age range to a meeting to explain the aim and details of the study and to resolve any doubts they might have. Subsequently, we asked the parents or legal guardians of the schoolchildren to sign a written consent for their children to participate in the study.
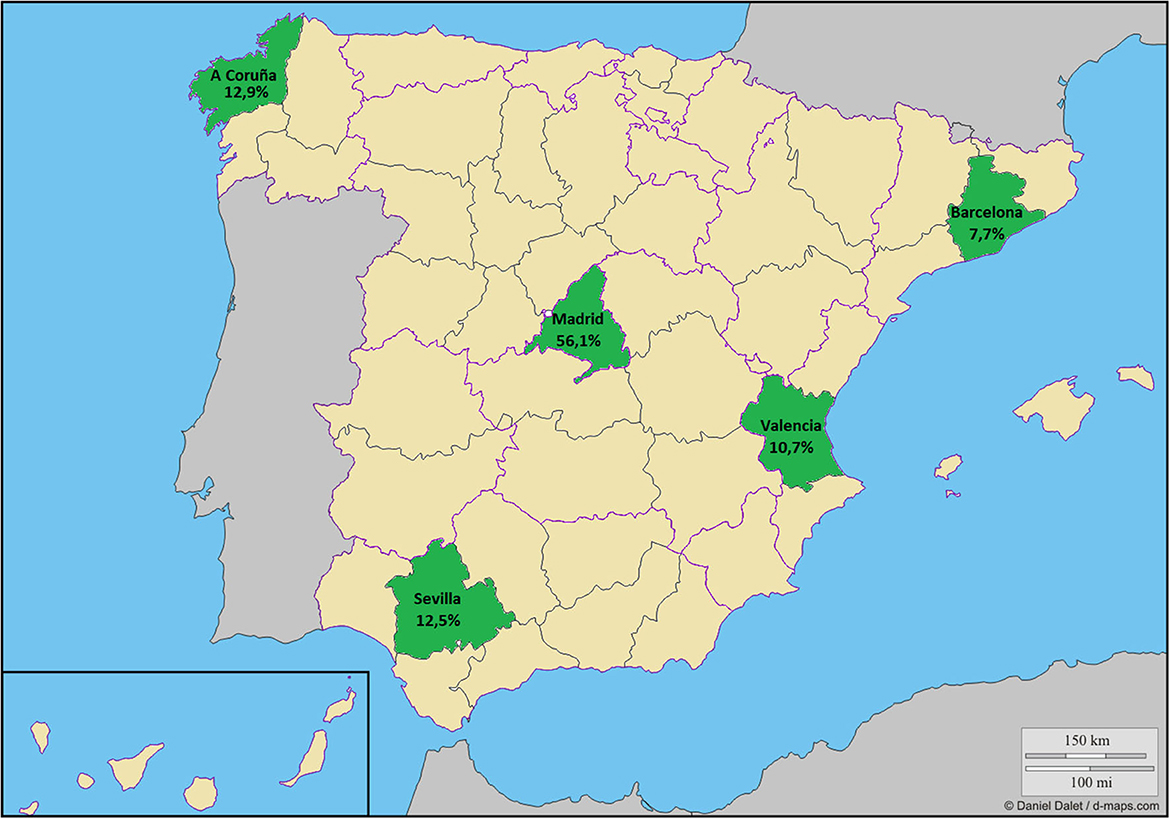
Figure 1. Sample distribution. Modified from “https://d-maps.com/carte.php?num_car=5672&lang=es”.
The inclusion criteria were children aged between 8 and 13 years in the 4th, 5th, or 6th grade of primary school; written informed consent signed by the children's parents and/or guardians; and acceptance of all study conditions.
The exclusion criteria were presenting any disease that could modify the results of the study: metabolic or chronic diseases (diabetes, renal pathologies, etc.); impossibility of attending school on the days agreed for the tests; and receiving pharmacological treatment that could interfere with the results of the study. Measurements were made between February 2005 and June 2009.
Our potential sample included 3,850 schoolchildren. This potential sample size was calculated based on the number of schools that had agreed to participate (22 schools), that each school could have from 1 to 3 different grade levels (4th, 5th, and/or 6th grade), that in some schools there is more than one classroom of the same level, and that the average number of students in each classroom is 25. Of these, 1,035 obtained written consent from their parents or guardians to participate in the study, so the approximate acceptance rate was 27%. Finally, 839 children had a complete daily activities questionnaire and valid biochemical data (Figure 2).
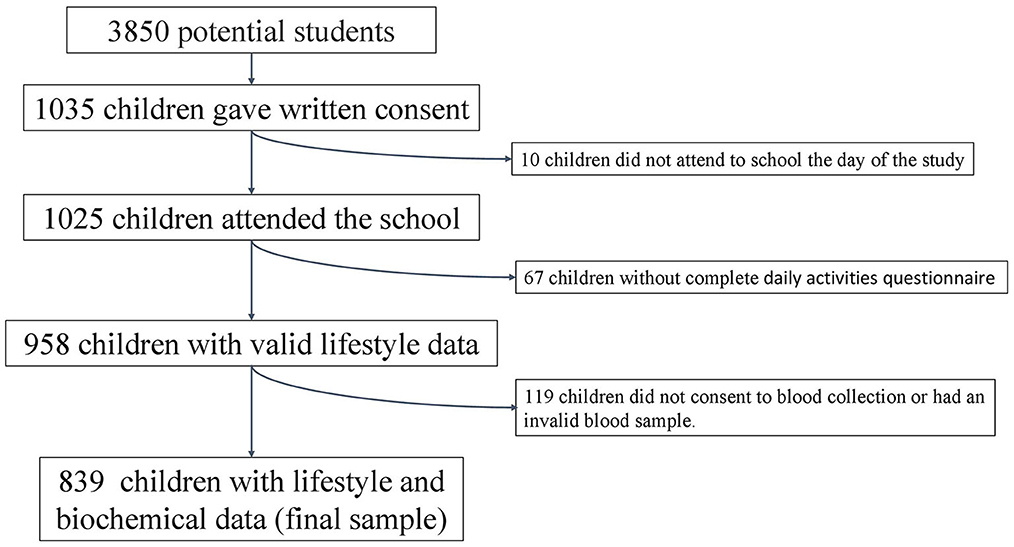
Figure 2. Flow chart of the selection process.
The participating children underwent a socio-demographic, lifestyle, anthropometric and biochemical study at the school by qualified research staff.
We conducted this study in accordance with the guidelines established in the Declaration of Helsinki, and all procedures involving human subjects/patients were approved by the Human Research Review Committee of the Faculty of Pharmacy of the Complutense University of Madrid (PI060318, approved on 17 March 2006).
2.2. Socio-demographic data
We used a self-completed survey by the parents/guardians of the children, including questions related to the demographic characteristics of the schoolchildren (sex, date of birth, and maximum level of education attained by the parents).
2.3. Anthropometric data
Anthropometric measurements (weight and height) were recorded by qualified personnel. The study was conducted in the schools during morning hours and following the standards established by the WHO (28). For the measurements, the subjects were barefoot and wore only underwear.
Weight and height were determined with a digital electronic scale (range: 0.1–150 kg, accuracy: 100 g; SECA ALPHA, GMBH, Igny, France) and a Harpenden digital stadiometer (range: 70–205 cm, accuracy: 1 mm; Pfifter, Carlstadt, NJ, USA). We calculated the body mass index (BMI) of the subjects using the formula weight (kg)/height2 (m2). Subsequently, we calculated the BMI z-score (zBMI) according to WHO growth standards (29).
2.4. Biochemical data
Blood samples were collected by venipuncture between 08:00 and 09:00 after 12 h of fasting. The nursing staff verified the adequacy of the fasting period before collecting the blood. Samples were collected at the school.
We colourimetrically determined plasma glucose levels by the glucose oxidase–peroxidase method (30) (Vitros GLU Slides, Rochester, NY, USA; CV = 2–8%). We measured insulin levels with an immunochemiluminometric assay (31) (Abbott Diagnostics, Madrid, Spain; CV = 4.8%). We used the homeostasis model assessment value (HOMA-IR) to reflect the degree of IR (32, 33): HOMA-IR = [basal glucose (mmol/L) × basal insulin (μU/mL)]/22.5. We considered IR present when the HOMA-IR was >3.16 (34).
2.5. The 24-h movement guidelines
We assessed lifestyle behaviors with an adapted daily activities questionnaire recording the children's usual daily activities, which had to be jointly completed by parents and children (35) and which has been used in previous studies (36–38). The questionnaire asked about the time spent on different activities usually carried out during the day: sleeping; being in class; studying; eating at different meals; playing sedentary games (PC, video game consoles) or watching TV; actively playing in the street and at home; in gymnastics or other sports activities at school; at recess and in extracurricular activities; and traveling between home and school and other activities, and the mode of transport used.
We then grouped the time spent on the different activities into the following categories: sleeping, very light activities (activities that are performed lying down, sitting, or standing, such as painting, playing an instrument, cooking, etc.); light activities (equivalent to walking on a flat surface at 4–5 km/h, such as cleaning the house, golf, table tennis, etc.); and moderate and/or vigorous activities (physical activities that require more energy expenditure such as cycling, skiing, tennis, dancing, basketball, football, rugby, running, etc.).
We classified children according to the 24 h movement guidelines (24) as “non-sedentary” if they restricted screen time to < 2 h/day (24) and as “physically active” if they performed at least 60 min of MVPA per day (24). We considered adequate sleep time if the child slept between 9 and 11 h (24).
The percentage of children complying with one, two, three or none of the recommendations of the 24 h movement guidelines was calculated. Schoolchildren were classified according to their adherence to a healthy lifestyle as follows: “low adherence”, if they complied with one or none of the recommendations of the 24 h movement guidelines, and “high adherence” if they complied with two or three recommendations.
2.6. Statistical analysis
Descriptive data are expressed as means and standard deviations for continuous variables and as percentages for categorical variables. We compared the data according to sex, lifestyle, and presence or absence of IR. We used the Kolmogorov–Smirnov test to determine the normality of the data. For comparison of means, we used the Mann–Whitney U-test if the distribution of variables was not normal and Student's t-test for normal distributions as well as the two-way ANOVA test. We compared categorical variables using the chi2 test and the Z-test of proportions. We calculated Spearman correlation coefficients between the hours spent on the different activities and HOMA-IR. We performed logistic regression analysis to identify risk or protective factors for IR, and we report odds ratios (OR) and 95% confidence intervals (CI). We considered a p-value of < 0.05 statistically significant. We performed all calculations with IBM SPSS Statistics for Windows, version 28.0 (Armonk, NY: IBM Corp, published in 2021).
2.7. Post-hoc power calculation
Post-hoc power analysis was calculated with G*Power (v. 3.1.9.6, Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) using an alpha error of 0.05, a sample size (n1= 367 and n2= 472) and an effect size of 0.35 to detect differences on HOMA-IR values according to adherence to the 24-h movement guidelines.
3. Results
These children were previously studied in another context (37, 38). The potential initial sample size was approximately 3,850 participants, which was calculated considering the number of schools that agreed to participate (n = 22), number of students per classroom (n = 25), and number of classrooms per grade (between two and three). Subsequently, 1,035 schoolchildren (49.2% boys) obtained written consent from their parents or guardians to participate in the study. Ten children were not in school on the day of the anthropometric study. We obtained valid lifestyle data from 958 schoolchildren (49.3% boys) and valid blood samples from 890 subjects (48.4% boys). The final sample was 839 individuals (48.9% boys) with complete biochemical and lifestyle data (Figure 2).
Table 1 shows the sociodemographic, anthropometric, biochemical, and lifestyle data of the total sample and by sex. We found no differences in age or parental education by sex. Boys had a higher zBMI and fasting glucose values than girls, but lower fasting insulin and HOMA-IR values. Of the children, 5% presented IR, the percentage being higher in girls (6.8 vs. 3.2%, p < 0.05). Boys spent more hours in front of the TV and computer, so they had more screen time than girls. Boys performed more MVPA than girls. 50.5% of schoolchildren spend < 2 h in front of the screen and only 31.9% of schoolchildren spend more than 1 h of MVPA per day. Overall, boys adhered less to screen time recommendations (45.9 vs. 55.0% for girls, p < 0.05) and more to physical activity recommendations (41.2 vs. 23.1%, p < 0.05) than girls. In addition, the recommendation on sleep is the one most frequently complied with by both sexes (82.4%), no differences between sex groups were seen.
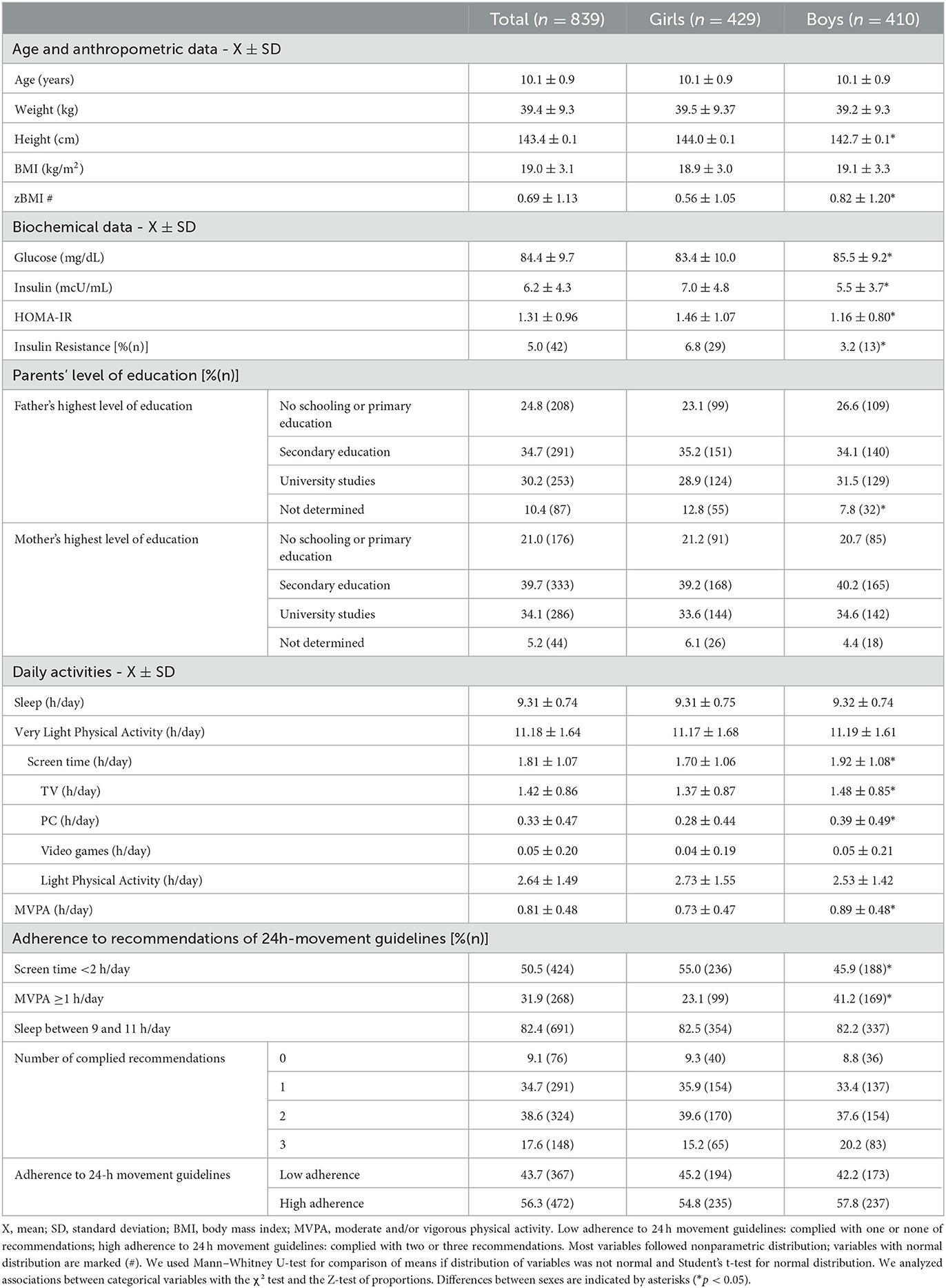
Table 1. Anthropometric, biochemical, sociodemographic, and lifestyle parameters according to sex.
Table 2 shows age, sociodemographic, anthropometric, and lifestyle data according to sex and presence of IR. We found no differences in age or parents' educational level according to IR status. Girls with IR spent more time on computers and screens in general and in very light activities, and they spent less time on light activities and MVPA than girls without IR. Therefore, fewer girls with IR met the 24 h movement guidelines for screen time (34.5 vs. 56.5%, p < 0.05) and physical activity (6.9 vs. 24.3%, p < 0.05) compared with girls without IR, with no difference in sleep time. In boys, we found no differences in their lifestyles based on having IR, except that boys with IR were less compliant with sleep recommendations than boys without IR (61.5 vs. 83.1%, p < 0.05).
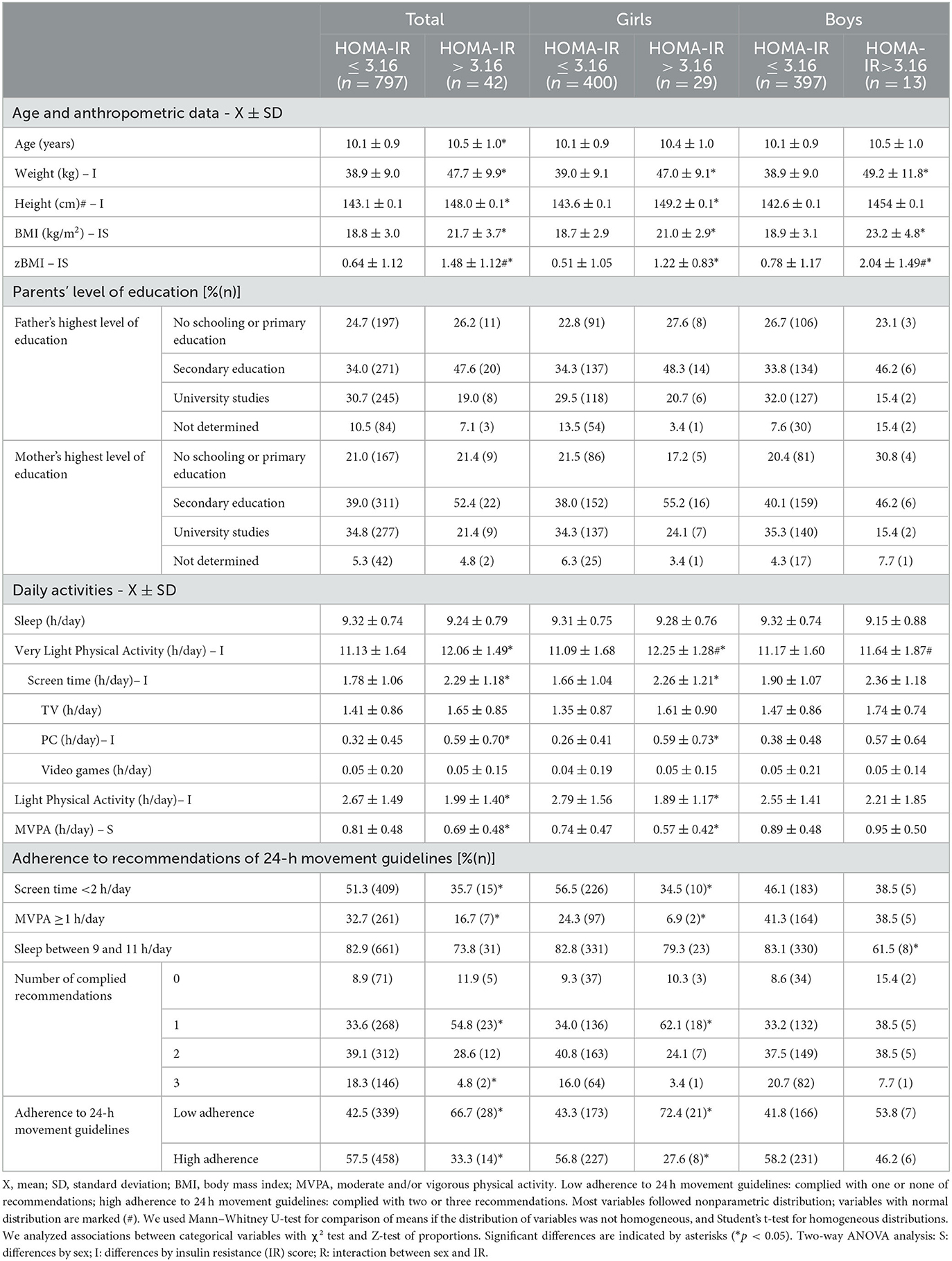
Table 2. Anthropometric, sociodemographic, and lifestyle parameters according to sex and HOMA-IR.
Because only two children with IR complied with all three lifestyle recommendations, we decided to group subjects into low adherence (adherence to one or none of the recommendations) and high adherence (adherence to two or three recommendations) for statistical analysis. A lower percentage of girls with IR had high adherence to the 24 h movement guidelines compared with girls without IR (27.6 vs. 56.8%, p < 0.05). We observed no significant differences based on the presence of IR in the boys.
Table 3 shows the different biochemical parameters and IR according to adherence to the 24 h movement guidelines. Children who did not follow the recommendations for screen time or physical activity and those with lower adherence to the 24 h movement guidelines had higher fasting insulin levels and HOMA-IR values. We found no significant differences according to the sleep recommendations for either sex.
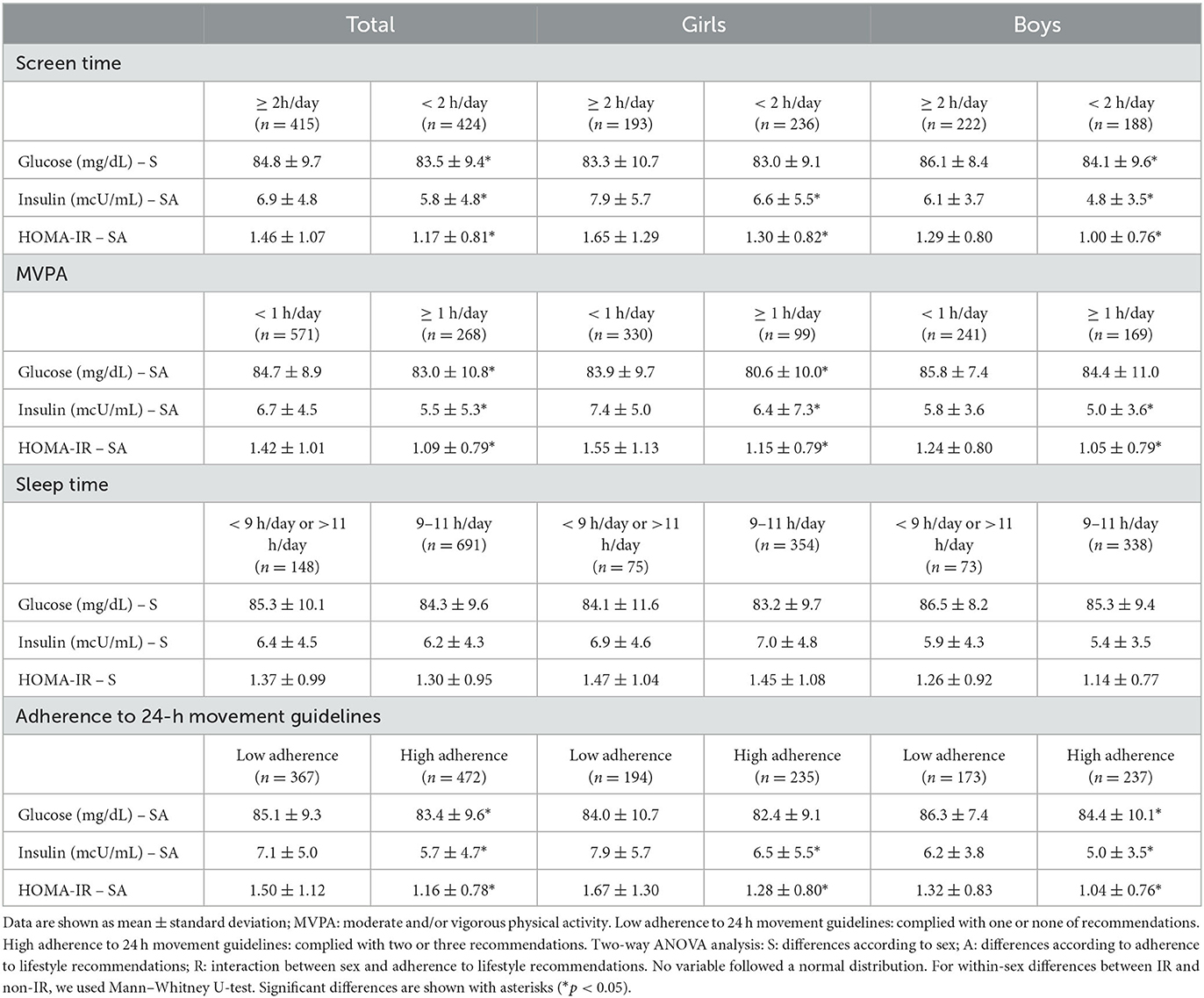
Table 3. Biochemical parameters according to sex and lifestyle parameters.
HOMA-IR directly and significantly correlated with screen time and very light physical activity, and indirectly correlated with light physical activity, MVPA, sleep time, and the number of recommendations met. These associations were maintained when boys and girls were separately analyzed, except for the sleep time (Table 4).
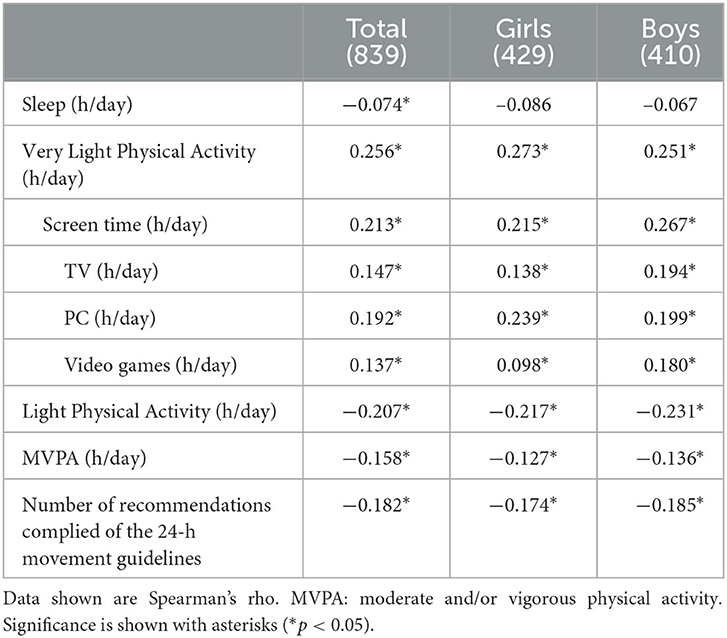
Table 4. Correlations between lifestyle variables and HOMA-IR.
The results of logistic regression analysis showed that low adherence to 24 h movement guidelines was associated with increased risk of IR both in the total sample and in girls. In girls, non-adherence to screen time or physical activity recommendations was associated with an increased risk of IR in the crude model, but the association disappeared when corrected for age and zBMI. There was no association with sleep time. In addition, no significant association was found in boys (Table 5).
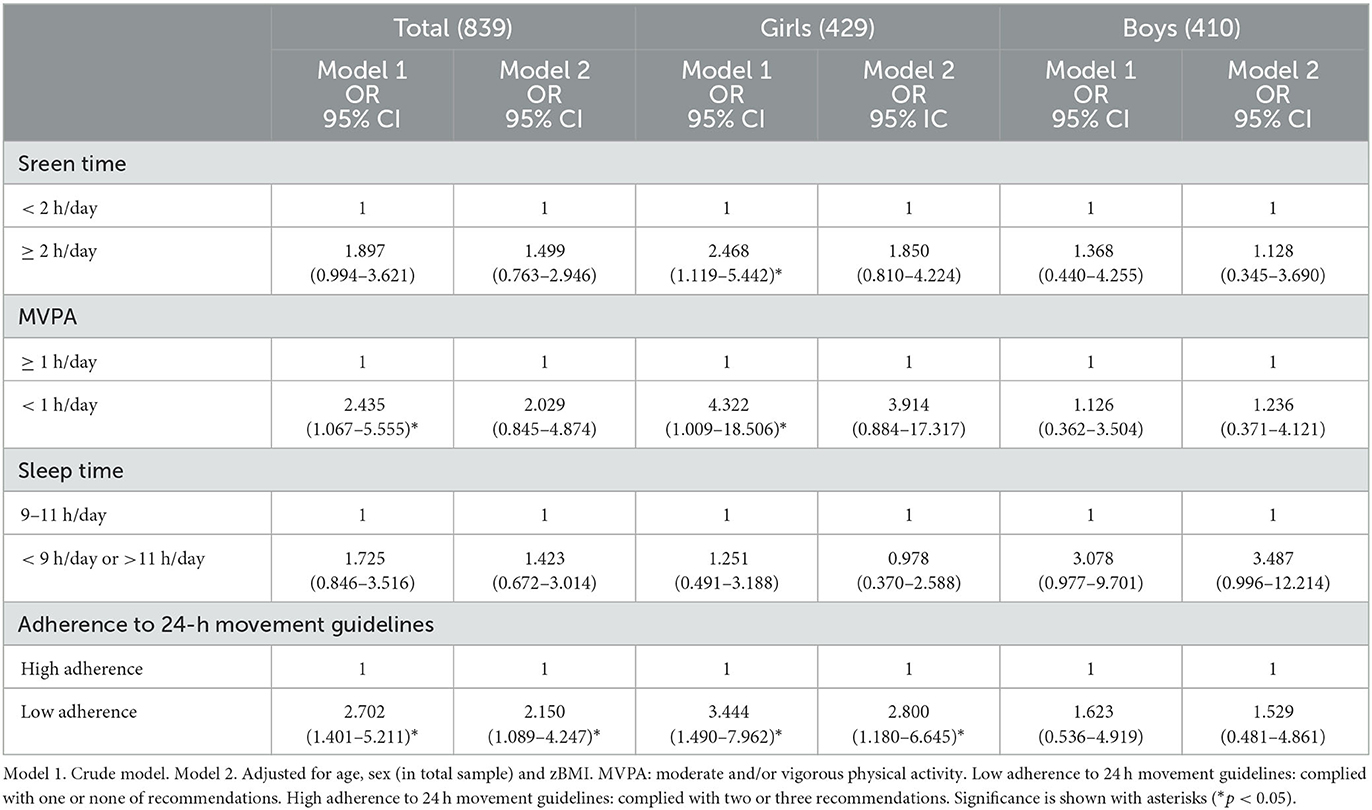
Table 5. Associations between lifestyle parameters and IR by sex. Logistic regression analysis.
4. Discussion
Our findings showed that schoolchildren with IR had a less active lifestyle in general and had higher levels of screen time than those without IR, especially girls. Children who met the recommendations for physical activity or screen time or had higher adherence to 24 h movement guidelines had lower fasting glucose, fasting insulin, and HOMA-IR levels. Finally, increased adherence to lifestyle recommendations was associated with a lower risk of IR.
In our study, 43.7% of schoolchildren had low adherence to 24 h movement guidelines (complying with only one or none of the recommendations), similar to that reported in another Spanish child population (39.2%) (39) and lower than that reported in an international study (62.9%) (40). The low adherence to lifestyle recommendations in our study was mainly due to the low adherence to physical activity recommendations, because it was lower than the adherence to sleep and screen time recommendations.
About half of our schoolchildren adhered to the screen time guidelines, spending < 2 h in front of a screen. This figure is difficult to compare with those in other studies as the percentage of children meeting screen time recommendations widely varies from 8.1 to 98.4% in the 6–12 years age group, as shown by a recent meta-analysis (41). However, approximately half of the sample dedicated more hours to sedentary leisure than is recommended.
The time devoted by our population to MVPA was 49 min, being higher in boys. These data are similar to those published in a study on Spanish children aged 7 to 11 years (44 min) (39) and are lower than those reported in a Finnish child population aged 3–6 years (1 h 25 min) (42). Only 31.9% of the sample spent at least 1 h on MVPA, and this figure was even lower for girls.
In our study and in the bibliography, schoolchildren spend too much time on sedentary leisure (41) and less time than recommended on physical activity (39, 40). This indicates that, in general, schoolchildren are sedentary and inactive, and policies should be strengthened to reverse this situation, which can lead to serious health problems. Moreover, boys and girls have different lifestyles, with boys being more active but more sedentary. Therefore, recommendations and interventions should be tailored to sex to ensure greater adherence.
The recommendation of the 24 h movement guidelines most followed by our schoolchildren was for sleep time, as observed in other studies (36, 42). The children in our study slept an average of 9 h 19 min, lower than that reported in Spanish children in the ALADINO-2019 study (10 h 17 min) (43), but similar to that of a U.S. study of children aged 9–10 years (44) and in a Swedish study of children 10 to 12 years old (9 h) (45). Sleep recommendations were not met by 17.5% of children, a figure higher than that of other European countries (46). This is surprising because, according to the COSI strategy, Spanish children are among those who spend more time sleeping compared with other European countries (47), although this difference may be due to the COSI strategy being applied in children aged 6–9 years, an age somewhat younger than ours, and children sleep less as they age (48).
Regarding the relationship of compliance with the 24 h movement guidelines to IR, sedentary schoolchildren in our study (≥2 h/day of screen time) had higher HOMA-IR values. This result is consistent with those of the European IDEFICS study of children aged 2–17 years (49) and in English (7–13 years) (50) and Spanish schoolchildren (5–14 years) (51). This potential relationship between sedentary lifestyles and IR may have been due to less muscle activity and energy expenditure, causing alterations in homeostasis. Spending more time in sedentary activities may result in a lower rate of glucose processing in skeletal muscle, accompanied by less inhibition of glucose production in the liver (52).
In addition, our schoolchildren who performed more than 60 min of MVPA per day had lower HOMA-IR values. In a study of Indian children, physical activity during early adolescence was found to play a protective role against IR (53). The IDEFICS study assessed cross-sectional associations between physical activity and the clustering of cardiometabolic risk factors (such as IR), and moderate activity time negatively correlated with cardiometabolic risk score (54). Physical activity can influence IR through various potential mechanisms, one of which is the absence of skeletal muscle contractions being associated with reduced blood flow, which decreases circulating glucose transport to muscle (55). MVPA is associated with increased glucose uptake by skeletal muscle, leading to a decrease in blood glucose (56).
Considering sleep as part of a healthy lifestyle to prevent IR is important, as a lack of sleep is associated with elevated stress levels as well as hypothalamic–pituitary–adrenal regulation, which may lead to neuroendocrine disruption, which in turn may cause dysregulation in glucose–insulin metabolism (57). However, the results of studies on the relationship between sleep and IR in children and adolescents are controversial. In our study, sleep duration was not associated with IR, as observed in the IDEFICS study, conducted on children aged 2–15 years (58), and in the HELENA study, conducted on adolescents aged 12.5–17.5 years (59). However, this differs from the results of the ABCD Growth Study, conducted in Brazil on adolescents aged 11–18 years, where this component was the only one related to HOMA-IR (60). A narrative review in a pediatric population concluded that the relationship between sleep and HOMA-IR is not yet clearly established, although “convincing evidence” exists of an association between sleep duration and biomarkers of type 2 diabetes mellitus (including HOMA-IR) (61). The lack of association in our study could be explained by the high percentage of children who adhered to the sleep recommendation, which was the most followed guideline.
Similar to our results, Werneck et al. found that having several inappropriate lifestyle behaviors, or low adherence to recommendations, increases the risk of elevated HOMA-IR, although in this study, in addition to the lifestyle behaviors we analyzed, skipping breakfast was also considered (60).
Therefore, our study agrees with other studies in the relationship between screen time and physical activity with lower IR (49–51, 53, 54). While on the relationship between sleep duration and IR, the results remain controversial, with some studies finding a relationship (60, 61), and others, such as ours and other studies (58, 59), finding no association.
However, to our knowledge, only Werneck et al. (60) and ourselves have jointly assessed these parameters in relation to IR and we have both observed that adherence to various lifestyle factors is more robustly related to IR. Therefore, this is one of the first studies to assess a possible closer relationship by jointly assessing these lifestyle parameters in association with IR.
As other authors have pointed out, our results showed that examining the relationship between a single lifestyle behavior and health is not appropriate. Therefore, different lifestyle recommendations should be combined to further examine the relationship between lifestyle and health outcomes, such as cardiometabolic risk or IR (25–27).
Since this is one of the first studies to jointly assess lifestyle in relation to IR in children. And the results suggest that analyzing lifestyle factors separately may not address the problem of IR, a pooled analysis should be conducted to analyze the risk of IR. In addition, physical activity and sedentary time seem to be more related to IR than sleep in this study sample.
Given that IR is related not only to obesity but also to other comorbidities since childhood and based on the results of our work. It is important to carry out health policies, recommendations and studies that are not limited to including increased physical activity or decreased sedentary lifestyle, but should be comprehensive, including more physical activity, less sedentary leisure (such as screens nowadays) and correct sleep habits, as these activities should be approached as a whole.
One of the main strengths of our study is the large sample size, although the sample is a convenience one and therefore not representative of the Spanish population.
One of the main limitations was that being a large study, we could not perform Tanner's clinical staging and did not obtain information on the pubertal status of the participants, which could have influenced the prevalence of IR. Moreover, as we used a questionnaire to measure lifestyle and no other methods, such as accelerometers, the data may have been overestimated. Another possible limitation was that, as only a small sample followed all the recommendations, they had to be arbitrarily grouped for the analysis. Ethnicity was not collected in the study, and approximately half of the subjects did not answer about their country of origin, although the majority of those who reported were Spanish. Finally, our study had a cross-sectional design that highlighted the existence of associations but cannot demonstrate causal relationships and the sample studied is a convenience one, so the conclusions of our study should be confirmed in future research. Furthermore, although the sample size was not calculated a priori, a post hoc power analysis was performed and showed that our study had a high power (99%) to detect differences in mean HOMA-IR values according to adherence to 24 h movement patterns. Nevertheless, it would have been desirable to determine the sample size a priori and to use a probability sampling method.
Future lines of research are based on carrying out an intervention study in Spanish schoolchildren of the same age to verify the results obtained. In this study we intend to use an accelerometer in addition to the lifestyle questionnaire, in order to validate the questionnaire and to have non-self-reported lifestyle data.
In conclusion, we found that about half of the schoolchildren had low adherence to the 24 h movement guidelines. Sleep time was the most followed recommendation, and physical activity was the least. Girls were less physically active but also spent less time on screens. Our study showed that higher adherence to recommended lifestyle patterns was inversely associated with IR, especially in girls and when several lifestyle factors were combined. Intervention studies are needed that can confirm the possible protective effect of increasing adherence to the 24 h movement guidelines on IR in schoolchildren.
Data availability statement
The datasets analysed for this study are available upon reasonable request from MDS-G (bWFzYWxhMDZAdWNtLmVz).
Ethics statement
The present study protocol was reviewed and approved by the Ethics Committee of the Faculty of Pharmacy of the Complutense University of Madrid, in Spain (PI060318, approved on 17 March 2006). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
AML-S and RMO contributed to conception and design of the study. MDS-G, LMB, MCL-E, and LGG-R collected and processed data. MDS-G performed the statistical analysis and wrote the first draft of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the FISS project PI060318, INCERHPAN-UCM contract 210/2008, and a predoctoral contract financed by the Complutense University of Madrid and Banco Santander (CT63/19-CT64/19).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
IR, Insulin resistance; HOMA-IR, Homeostasis model of insulin resistance; MVPA, Moderate and/or vigorous physical activity; BMI, Body mass index; zBMI, BMI z-score; X, Mean; SD, Standard deviation.
References
1. Sinaiko AR, Steinberger J, Moran A, Prineas RJ, Vessby B, Basu S, et al. Relation of body mass index and insulin resistance to cardiovascular risk factors, inflammatory factors, and oxidative stress during adolescence. Circulation. (2005) 111:1985–91. doi: 10.1161/01.CIR.0000161837.23846.57
2. Chiarelli F, Marcovecchio ML. Insulin resistance and obesity in childhood. Eur J Endocrinol. (2008) 159:S67–74. doi: 10.1530/EJE-08-0245
3. Williams DE, Cadwell BL, Cheng YJ, Cowie CC, Gregg EW, Geiss LS, et al. Prevalence of impaired fasting glucose and its relationship with cardiovascular disease risk factors in US adolescents, 1999-2000. Pediatrics. (2005) 116:1122–6. doi: 10.1542/PEDS.2004-2001
4. Marker AM, Steele RG, Noser AE. Physical activity and health-related quality of life in children and adolescents: a systematic review and meta-analysis. Health Psychol. (2018) 37:893–903. doi: 10.1037/hea0000653
5. Qi J, Yan Y, Yin H. Screen time among school-aged children of aged 6-14: a systematic review. Glob Health Res Policy. (2023) 8:12. doi: 10.1186/s41256-023-00297-z
6. Krietsch KN, Chardon ML, Beebe DW, Janicke DM. Sleep and weight-related factors in youth: a systematic review of recent studies. Sleep Med Rev. (2019) 46:87–96. doi: 10.1016/j.smrv.2019.04.010
7. Chaput JP, Saunders TJ, Carson V. Interactions between sleep, movement and other non-movement behaviours in the pathogenesis of childhood obesity. Obesity Reviews. (2017) 18:7–14. doi: 10.1111/OBR.12508
8. Duncan S, Duncan EK, Fernandes RA, Buonani C, Bastos KDN, Segatto AFM. Modifiable risk factors for overweight and obesity in children and adolescents from São Paulo, Brazil. BMC Public Health. (2011) 11:585. doi: 10.1186/1471-2458-11-585
9. Wafa SW, Shahril MR, Ahmad AB, Zainuddin LR, Ismail KF, Aung MM, et al. Association between physical activity and health-related quality of life in children: a crosssectional study. Health Qual Life Outcomes. (2016) 14:1–6. doi: 10.1186/s12955-016-0474-y
10. Silva DR, Werneck AO, Collings PJ, Fernandes RA, Barbosa DS, Ronque ERV, et al. Physical activity maintenance and metabolic risk in adolescents. J Public Health. (2018) 40:493–500. doi: 10.1093/pubmed/fdx077
11. Biddle SJH, García Bengoechea E, Wiesner G. Sedentary behaviour and adiposity in youth: a systematic review of reviews and analysis of causality. Int. J Behav Nutr Phys Activity. (2017) 14:1–21. doi: 10.1186/s12966-017-0497-8
12. Patterson R, McNamara E, Tainio M, de Sá TH, Smith AD, Sharp SJ, et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur J Epidemiol. (2018) 33:811–29. doi: 10.1007/s10654-018-0380-1
13. Kivimäki M, Singh-Manoux A, Pentti J, Sabia S, Nyberg ST, Alfredsson L, et al. Physical inactivity, cardiometabolic disease, and risk of dementia: an individual-participant meta-analysis. BMJ. (2019) 365:495. doi: 10.1136/bmj.l1495
14. Rosi A, Calestani MV, Parrino L, Milioli G, Palla L, Volta E, et al. Weight status is related with gender and sleep duration but not with dietary habits and physical activity in primary school italian children. Nutrients. (2017) 9:579. doi: 10.3390/nu9060579
15. Felso R, Lohner S, Hollódy K. Erhardt, Molnár D. Relationship between sleep duration and childhood obesity: Systematic review including the potential underlying mechanisms. Nutr Metab Cardiovasc Dis. (2017) 27:751–61. doi: 10.1016/j.numecd.2017.07.008
16. Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, et al. National Sleep Foundation's updated sleep duration recommendations: final report. Sleep Health. (2015) 1:233–43. doi: 10.1016/J.SLEH.2015.10.004
17. Cavallo FR, Golden C, Pearson-Stuttard J, Falconer C, Toumazou C. The association between sedentary behaviour, physical activity and type 2 diabetes markers: A systematic review of mixed analytic approaches. PLoS ONE. (2022) 17:289. doi: 10.1371/JOURNAL.PONE.0268289
18. Elagizi A, Kachur S, Carbone S, Lavie CJ, Blair SN. A review of obesity, physical activity, and cardiovascular disease. Curr Obes Rep. (2020) 9:571–81. doi: 10.1007/S13679-020-00403-Z
19. Rubín L, Gába A, Dygrýn J, Jakubec L, Materová E, Vencálek O. Prevalence and correlates of adherence to the combined movement guidelines among Czech children and adolescents. BMC Public Health. (2020) 20:1–15. doi: 10.1186/S12889-020-09802-2
20. Moitra P, Madan J, Verma P. Independent and combined influences of physical activity, screen time, and sleep quality on adiposity indicators in Indian adolescents. BMC Public Health. (2021) 21:25–45. doi: 10.1186/S12889-021-12183-9
21. Laguna M, Ruiz JR, Lara MT, Aznar S. Recommended levels of physical activity to avoid adiposity in Spanish children. Pediatr Obes. (2013) 8:62–9. doi: 10.1111/J.2047-6310.2012.00086.X
22. Chaput J-P, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, et al. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: summary of the evidence. Int J Behav Nutr Phys Activity. (2020) 17:141. doi: 10.1186/s12966-020-01037-z
23. Paruthi S, Brooks LJ, D'Ambrosio C, Hall WA, Kotagal S, Lloyd RM, et al. Recommended amount of sleep for pediatric populations: a consensus statement of the american academy of sleep medicine. J Clin Sleep Med. (2016) 12:785–6. doi: 10.5664/jcsm.5866
24. Tremblay MS, Carson V, Chaput J-P, Connor Gorber S, Dinh T, Duggan M, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. (2016) 41:S311–27. doi: 10.1139/apnm-2016-0151
25. Leppänen MH, Haapala EA, Väistö J, Ekelund U, Brage S, Kilpeläinen TO, et al. Longitudinal and cross-sectional associations of adherence to 24-hour movement guidelines with cardiometabolic risk. Scand J Med Sci Sports. (2022) 32:255–66. doi: 10.1111/sms.14081
26. Chen ST, Liu Y, Tremblay MS, Hong JT, Tang Y, Cao ZB, et al. Meeting 24-h movement guidelines: Prevalence, correlates, and the relationships with overweight and obesity among Chinese children and adolescents. J Sport Health Sci. (2021) 10:349. doi: 10.1016/J.JSHS.2020.07.002
27. Rollo S, Antsygina O, Tremblay MS. The whole day matters: Understanding 24-hour movement guideline adherence and relationships with health indicators across the lifespan. J Sport Health Sci. (2020) 9:493–510. doi: 10.1016/J.JSHS.2020.07.004
28. World Health Organization. Physical Status: The Use and Interpretation of Anthropometry. Report of the WHO Expert Committee. (1995) 543:82. doi: 10.1253/circj.cj-11-0982
29. WHO. WHO/Europe | Nutrition - Body mass index - BMI. World Health Organization. (2021). Available online at: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed January 17, 2023).
30. Neese JW, Duncan PBD. Development and evaluation of a Hexokinase/Glucose-6-Phosphate Dehydrogenase Procedure for Use as a National Glucose Reference Method. New York, NY: US Public Health Service, Center for Disease Control, Bureau of Laboratories, Clinical Chemistry Division (1976)
31. Del Kenz H, Bergmann P. Evaluation of immunochemiluminometric assays for the measurement of insulin and C-peptide using the ADVIA Centaur®. Clin Lab. (2004) 50:171–174.
32. Albareda M, Rodríguez-Espinosa J, Murugo M, de Leiva A, Corcoy R. Assessment of insulin sensitivity and beta-cell function from measurements in the fasting state and during an oral glucose tolerance test. Diabetologia. (2000) 43:1507–11. doi: 10.1007/s001250051561
33. Tripathy D, Carlsson M, Almgren P, Isomaa B, Taskinen MR, Tuomi T, et al. Insulin secretion and insulin sensitivity in relation to glucose tolerance: lessons from the Botnia Study. Diabetes. (2000) 49:975–80. doi: 10.2337/diabetes.49.6.975
34. Keskin M, Kurtoglu S, Kendirci M, Atabek ME, Yazici C. Homeostasis model assessment is more reliable than the fasting glucose/insulin ratio and quantitative insulin sensitivity check index for assessing insulin resistance among obese children and adolescents. Pediatrics. (2005) 115:e500. doi: 10.1542/peds.2004-1921
35. Ortega RM, Requejo AM, López-Sobaler AM. Activity Questionnaire. In Nutriguía. Manual of Clinical Nutrition in Primary Care; (2015) Editorial Médica Panamericana: Madrid, Spain. Available online at: https://www.ucm.es/idinutricion/file/cuestionario-de-actividad-escolares?ver (accessed January 17, 2023).
36. Peral-Suárez Á, Cuadrado-Soto E, Perea JM, Navia B, López-Sobaler AM, Ortega RM. Physical activity practice and sports preferences in a group of Spanish schoolchildren depending on sex and parental care: a gender perspective. BMC Pediatr. (2020) 20:1–10. doi: 10.1186/S12887-020-02229-Z/TABLES/3
37. Rodríguez-Rodríguez E, Salas-González MD, Ortega RM, López-Sobaler AM. Leukocytes and Neutrophil–Lymphocyte Ratio as Indicators of Insulin Resistance in Overweight/Obese School-Children. Front Nutr. (2022) 0:1318. doi: 10.3389/FNUT.2021.811081
38. Salas-González MD, Aparicio A, Loria-Kohen V, Ortega RM, López-Sobaler AM. Association of healthy eating index-2015 and dietary approaches to stop hypertension patterns with insulin resistance in school children. Nutrients. (2022) 14:4232. doi: 10.3390/NU14204232
39. Peral Suárez Á, Navia Lombán B, Cuadrado-Soto E, Perea Sánchez JM, González Rodríguez LG, Ortega-Anta RM. Weight status, body composition, and diet quality of Spanish school children according to their level of adherence to the 24-hour movement guidelines. Nutr Hosp. (2020) 38:73–84. doi: 10.20960/nh.03127
40. Roman-Viñas B, Chaput JP, Katzmarzyk PT, Fogelholm M. Proportion of children meeting recommendations for 24-hour movement guidelines and associations with adiposity in a 12-country study. Int J Behav Nutr Phys Act. (2016) 13:49. doi: 10.1186/S12966-016-0449-8
41. Tapia-Serrano MA, Sevil-Serrano J, Sánchez-Miguel PA, López-Gil JF, Tremblay MS, García-Hermoso A. Prevalence of meeting 24-hour movement guidelines from pre-school to adolescence: a systematic review and meta-analysis including 387,437 participants and 23 countries. J Sport Health Sci. (2022) 11:427. doi: 10.1016/J.JSHS.2022.01.005
42. Leppänen MH, Ray C, Wennman H, Alexandrou C, Sääksjärvi K, Koivusilta L. Compliance with the 24-h movement guidelines and the relationship with anthropometry in Finnish preschoolers: the DAGIS study. BMC Public Health. (2019). 19:1–8. doi: 10.1186/S12889-019-7967-7
43. Agencia Española de Seguridad Alimentaria y Nutrición (AESAN). Estudio ALADINO. Estudio sobre la Alimentación, Actividad Física, Desarrollo Infantil y Obesidad en España 2019. Madrid (2020).
44. Guerrero MD, Barnes JD, Chaput JP, Tremblay MS. Screen time and problem behaviors in children: exploring the mediating role of sleep duration. Int J Behav Nutr Phys Act. (2019) 16:1–14. doi: 10.1186/S12966-019-0862-X
45. Dahlgren A, Sjöblom L, Eke H, Bonn SE, Trolle Y, Lagerros. Screen time and physical activity in children and adolescents aged 10–15 years. PLoS ONE. (2021) 16:455. doi: 10.1371/JOURNAL.PONE.0254255
46. Whiting S, Buoncristiano M, Gelius P, Abu-Omar K, Pattison M, Hyska J, et al. Physical activity, screen time, and sleep duration of children aged 6-9 years in 25 countries: an analysis within the who European childhood obesity surveillance initiative (COSI) 2015-2017. Obes Facts. (2021) 14:32–44. doi: 10.1159/000511263
47. López-Sobaler AM, Aparicio A, Salas-González MD, Loria Kohen V, Bermejo López LM. Childhood obesity in Spain and associated factors. Nutr Hosp. (2021) 38:27–30. doi: 10.20960/NH.03793
48. Carno MA, Hoffman LA, Carcillo JA, Sanders MH. Developmental stages of sleep from birth to adolescence, common childhood sleep disorders: overview and nursing implications. J Pediatr Nurs. (2003) 18:274–83. doi: 10.1016/S0882-5963(03)00087-3
49. Sina E, Buck C, Veidebaum T, Siani A, Reisch L, Pohlabeln H, et al. Media use trajectories and risk of metabolic syndrome in European children and adolescents: the IDEFICS/IFamily cohort. Int J Behav Nutr Phys Act. (2021) 18:134. doi: 10.1186/S12966-021-01186-9
50. Nightingale CM, Rudnicka AR, Donin AS, Sattar N, Cook DG, Whincup PH, et al. Screen time is associated with adiposity and insulin resistance in children. Arch Dis Child. (2017) 102:612. doi: 10.1136/ARCHDISCHILD-2016-312016
51. Leis R, Jurado-Castro JM, Llorente-Cantarero FJ, Anguita-Ruiz A, Iris-Rupérez A, Bedoya-Carpente JJ, et al. Cluster analysis of physical activity patterns, and relationship with sedentary behavior and healthy lifestyles in prepubertal children: genobox cohort. Nutrients. (2020) 12:1288. doi: 10.3390/NU12051288
52. Macías N, Espinosa-Montero J, Monterrubio-Flores E, Hernández-Barrera L, Medina-Garcia C, Gallegos-Carrillo K, et al. Screen-based sedentary behaviors and their association with metabolic syndrome components among adults in Mexico. Prev Chronic Dis. (2021) 18:1–12. doi: 10.5888/PCD18.210041
53. Kehoe SH, Krishnaveni G, Veena S, Kiran KN, Karat SC, Dhubey A. Active children are less adipose and insulin resistant in early adolescence; evidence from the Mysore Parthenon Cohort. BMC Pediatr. (2019) 19:1855. doi: 10.1186/S12887-019-1855-2
54. Jiménez-Pavón D, Konstabel K, Bergman P, Ahrens W, Pohlabeln H, Hadjigeorgiou C, et al. Physical activity and clustered cardiovascular disease risk factors in young children: a cross-sectional study (the IDEFICS study). BMC Med. (2013) 11:172. doi: 10.1186/1741-7015-11-172
55. Tremblay MS, Colley RC, Saunders TJ, Healy GN, Owen N. Physiological and health implications of a sedentary lifestyle. Appl Physiol Nutr Metab. (2010) 35:725–40. doi: 10.1139/H10-079
56. Holloszy JO. Exercise-induced increase in muscle insulin sensitivity. J Appl Physiol. (2005) 99:338–43. doi: 10.1152/JAPPLPHYSIOL.00123.2005
57. Hirotsu C, Tufik S, Andersen ML. Interactions between sleep, stress, and metabolism: from physiological to pathological conditions. Sleep Sci. (2015) 8:143–52. doi: 10.1016/J.SLSCI.2015.09.002
58. Thumann BF, Michels N, Felso R, Hunsberger M, Kaprio J, Moreno LA, et al. Associations between sleep duration and insulin resistance in European children and adolescents considering the mediating role of abdominal obesity. PLoS ONE. (2020) 15:5049. doi: 10.1371/JOURNAL.PONE.0235049
59. Rey-López JP, de Carvalho HB, de Moraes ACF, Ruiz JR, Sjöström M, Marcos A, et al. Sleep time and cardiovascular risk factors in adolescents: the HELENA (healthy lifestyle in europe by nutrition in adolescence) study. Sleep Med. (2014) 15:104–10. doi: 10.1016/J.SLEEP.2013.07.021
60. Werneck AO, Agostinete RR, Cayres SU, Urban JB, Wigna A, de Moraes Chagas LG. Association between Cluster of Lifestyle Behaviors and HOMA-IR among Adolescents: ABCD Growth Study. Medicina. (2018) 54:96. doi: 10.3390/MEDICINA54060096
Keywords: insulin resistance, children, schoolchildren, lifestyle behaviors, 24-h movement guidelines
Citation: Salas-González MD, Bermejo LM, González-Rodríguez LG, Lozano-Estevan MDC, Ortega RM and López-Sobaler AM (2023) Adherence to 24-h movement guidelines in Spanish schoolchildren and its association with insulin resistance: a cross-sectional study. Front. Public Health 11:1146580. doi: 10.3389/fpubh.2023.1146580
Received: 17 January 2023; Accepted: 19 June 2023;
Published: 10 July 2023.
Edited by:
Hassane Zouhal, University of Rennes 2 – Upper Brittany, FranceReviewed by:
Jian Ding, University of Malaya, MalaysiaJagmeet Madan, SNDT Women's University, India
Copyright © 2023 Salas-González, Bermejo, González-Rodríguez, Lozano-Estevan, Ortega and López-Sobaler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Dolores Salas-González, bWFzYWxhMDZAdWNtLmVz