 Amare Terfe
Amare Terfe Temima Jemal
Temima Jemal Tolossa Waqkene
Tolossa Waqkene- 1Department of Environmental Health Science, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
- 2Department of Environmental Health Science and Technology, Institute of Health, Jimma University, Jimma, Ethiopia
- 3Department of Public Health, Dawo District Health Office, Woliso, Ethiopia
The prevalence of work-related musculoskeletal disorders particularly low back pain is significantly high among common informal or small-scale enterprises within developing countries like weaving. However, there is little information on risk factors for low back pain in the informal sector such as the weaving sector in the areas of Addis Ababa as well as in Ethiopia. Therefore this study was aimed to assess the magnitude of low back pain and its associated factors among traditional cloth weavers in the Gulele sub-city, Addis Ababa, Ethiopia. A cross-sectional study with internal comparison was conducted from June 1, 2022, and August 30, 2022. A total of 660 traditional cloth weavers were included in the study by using a systematic random sampling method to select participants in each of cooperatives as well as individual households in 5 woredas in Gulele sub-city. The data was analyzed and managed using SPSS version 20. A multivariate logistic regression analysis was used to control potential confounding factors and to determine the association. Among 660 (100%) respondents, 330 (50%) of them experienced low back pain after starting weaving. Out of the respondents with low back pain through their job career, 291 (44.1%) of them experienced low back pain during the last 12 months. Working greater than 8 h per day (AOR = 4.60, 95%CI: 2.35, 8.87), working with frequent bending (AOR = 3.32, 95%CI: 1.49, 7.40), job stress (AOR = 1.68, 95%CI: 1.18, 2.40) were among factors significantly associated with the occurrence of low back pain. This study has shown a high prevalence of low back pain among traditional cloth weavers which indicates the need for immediate public health action. However, very small improvements in the working condition, weaving tools design, working methods can potentially lead to large benefits.
Introduction
Musculoskeletal disorders are injuries and disorders of the soft tissues and nervous system. They can affect almost any tissue, but the arms and back are the most commonly affected. Musculoskeletal disorders are one of the most common public health issues in today’s world, and they are caused by a variety of risk factors (1). It is common in many professions and the second leading cause of transient work injury after the common cold (2), as well as a source of workplace accidents and impairments in developing countries (3). Work-related musculoskeletal disorders (WMSDs) have long been recognized as a leading cause of nonfatal accidents and work-related absences in manufacturing communities (4).
Lower back pain (LBP) is the most common musculoskeletal disorder (MSD) affecting adults, with a lifetime prevalence of up to 84% (5). Symptoms can arise from a variety of anatomical sources, including nerve roots, muscles, fasciae, bones, joints, intervertebral discs (IVDs), and organs within the abdominal cavity (6). Previous research has found that LBP is responsible for an estimated 21.8 million disability adjusted life years (DALYs) in 2010. LBP affects approximately 60–80% of people at some point in their lives (7). In 2015, low back and neck pain were ranked as the fourth leading cause of DALYs worldwide. DALYs for low back and neck pain increased by 59.5% between 1990 and 2015. Low back and neck pain were the leading causes of disability in the majority of countries in 2015 (the second leading cause of DALYs in high-income countries after ischemic heart disease) (8).
Furthermore, lower back pain (LBP) is a leading cause of disability globally (1). It is one of the most common chronic disorders and has a significant economic impact worldwide (9). The pathophysiological causes of LBP are frequently unknown (10). This may lead to skepticism or dismissal of the seriousness and legitimacy of the disability associated with LBP (11). In addition to the physical effects that LBP patients experience, the condition has personal, societal, and psychological ramifications (12). Furthermore, chronic LBP is frequently accompanied by increased work absenteeism, lower productivity, status loss, and depressive symptoms (13).
A variety of factors influence the occurrence of chronic low back pain in various professions. Working postures are influenced by the shape, arrangement, size, and placement of the tools used as well as their operating methods. Unnatural body positions and non-ergonomic ways of working for an extended period of time can result in a variety of health issues for employees. Working in the same position for an extended period of time whether standing or sitting will cause discomfort (14). Working postures such as sitting for an extended period of time without any adjustment can soften the abdominal muscles, causing spine curvature and causing respiratory and digestive organ disorders (15).
Furthermore, a poor ergonomic workstation has been shown to increase muscular load and activity, resulting in an increase in MSD (16). Physical factors or loads on the biomechanical system are thought to cause tissue damage and inflammation, leading to MSD (17). Quantifying a workstation’s ergonomic risk is a method to cost-effectively implement and manage MSD in the workplace (18). However, there is still conflicting evidence that there is no link between workstation configuration and MSD (1, 19).
In developing countries such as Iran, China, Turkey, India, Pakistan, Russia, Egypt, Nepal, and Afghanistan, weaving is a common industry (20). The back is a vulnerable area in humans due to the mechanisms of the human body and the various types of tissue and structures that comprise the spine (21). Weavers weave in a variety of sitting postures, including forward flexion, upright posture, and side bending (22). During weaving, weavers sit continuously on a hard floor or a hard wooden bench with no back support. It stresses their lower limbs, calf muscles, and back. Throughout the weaving process, throwing shuttles and moving reed frames necessitate repetitive movements with no breaks. This could have long-term health implications. Weavers lean forward to avoid the effort required for rolling operations and maintain this posture for as long as weaving is possible, resulting in severe back pain. Furthermore, as raw material prices rise, the survival of the industry becomes increasingly difficult; as a result, weavers work long hours on the loom to complete tasks in order to earn more money (23, 24).
For centuries, Ethiopians have practiced traditional cotton weaving using both endogenous and exogenous technology. Cotton weavers work in small, cramped spaces under appalling working conditions. People working in the weaving industry are extremely vulnerable due to a lack of occupational safety and health services and poor working conditions because they are not supported by occupational safety and health services (25). Even in modern times, weaving has cultural value, and weavers must be properly cared for and valued as artisans. This research is critical not only for the health of weavers, but also for the esthetic and cultural value of the weaving profession. Traditional cloth weaving is still practiced in many parts of Ethiopia. The occupation has contributed significantly to the economies of both the workers in the sector and the country as a whole. There is, however, a scarcity of information about the health issues that weavers face at work. As a result, the purpose of this study was to determine the extent of low back pain and its associated factors among traditional cloth weavers in the Gulele sub-city of Addis Ababa, Ethiopia.
Materials and methods
Study setting and design
A descriptive cross-sectional study with internal comparison was conducted between June 1, 2022, and August 30, 2022, G.C. Weaving has long been a significant rural and urban home industry activity in Ethiopia. According to a handlooms cluster report, there are over 330,341 weavers’ nationwide and 66,068 weavers in Addis Abeba, with more than 60% (39,640) of them located in the Gulele sub-city of the Addis Ababa Administration. Weavers can be found at home, in sheds, and in cooperatives. Shiromeda, a sub-district on Addis Ababa’s northern outskirts near the Entoto Hills, is home to some of Ethiopia’s most celebrated weavers. Over the last 60 years, several weavers have migrated from southern Ethiopia to Shiromeda. Shiromeda and Addisu Gebeya are the traditional weaving hotspots in Addis Ababa (26). The study participants were drawn from Gulele, one of Addis Ababa’s 10 sub-cities.
Sample size and sampling procedures
This study included all traditional cloth weavers from Addis Ababa’s Gulele sub-city who work in both individual households and cooperatives. The study subjects were weavers with more than 1 year of experience to determine the 12-month prevalence of low back pain among weavers. Because no similar studies in this sector had been conducted in Ethiopia or any other African country, the sample size was calculated using a single proportion formula with a prevalence of 50% since we could not get study conducted in Ethiopia and other similar countries in Africa on this topic. Furthermore, we calculated sample size for factors that contribute for the occurrence of low back pain among different professions in Ethiopia. Finally we used the larger sample size for the study since it is recommended to use the larger sample size to increase the representativeness of this study. The total sample size for this study was 660 weavers who worked in both individual households and government-established cooperatives.
The total sample size required for this study was proportionally allocated to each of the woredas and cooperatives found in Gulele sub city according to their weight (Figure 1).
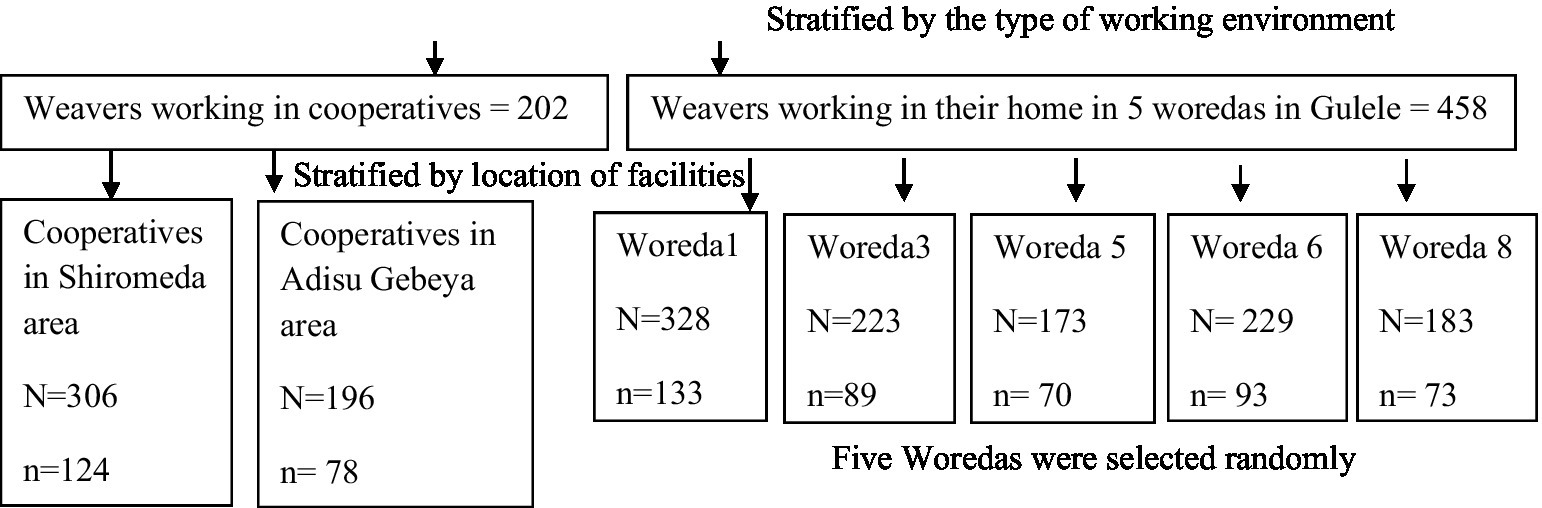
Figure 1. Sampling chart of weaving facilities.
The total sample size was stratified into individual households and cooperatives. A systematic random sampling method was used to select participants in Adisu Gebeya from 306 weavers organized into 11 cooperatives; 196 weavers organized into 7 cooperatives in the Shiromeda area; and individual households in 5 woredas in Gulele sub-city. The total sample size required for this study was proportionally allocated to each of the woredas and cooperatives found in the Gulele sub-city based on their weight.
Data collection procedures
A structured questionnaire was used to collect data from traditional cloth weavers who work in both individual households and cooperatives. The questionnaire was designed using the Nordic standard musculoskeletal questionnaire and was structured to include both the responses of the respondents and the observations of the interviewers. The data collectors and supervisor were given 2 days of training on how to conduct interviews, study subjects’ rights, and ethical issues such as confidentiality. Following data collector training, the questionnaire was pretested with 5% of the sample in areas that were unable to be included in the actual study, and the data collection process was supervised by two supervisors to ensure data quality and validity.
Data quality management and analysis
The collected data was checked for errors before being transferred to SPSS 26 software for analysis and data management. The data were analyzed using the SPSS statistical package for percentage calculations, and Univariate analysis was used to describe the data using percentages, and bivariate and multivariate analysis to determine the presence of association. In the bivariate analysis, variables with a 0.25 probability of association with the outcome variable were entered into a multivariate logistic regression to control for potential confounding factors. An odds ratio with a 95% confidence interval and a p-value of 0.05 was used to determine the presence of a significant association.
Ethical consideration
The University of Gondar’s ethical review board provided approval and clearance, as did the Gulele sub-city Small Scale Enterprise Development Agency. Furthermore, each study participant provided verbal informed consent. Respondents were informed that they could skip or end the interview process at any time. Furthermore, the study participants were informed that any information obtained from them would be kept confidential and used solely for research purposes.
Result
Socio-demographic characteristics of traditional cloth weavers
A total of 660 (100%) respondents took part in this study, with a response rate of 100%. Among the study participants, 591 (89.5%) were males, while only 69 (10.5%) were females. The majority of respondents, 256 (38.8%), were between the ages of 30 and 41, with a mean (±SD) age of 35.2(±11.921) years. The majority of study participants [341 (51.7%) had a high school (7–10) education, while the remaining 69 (10.5%) were uneducated (Table 1)].
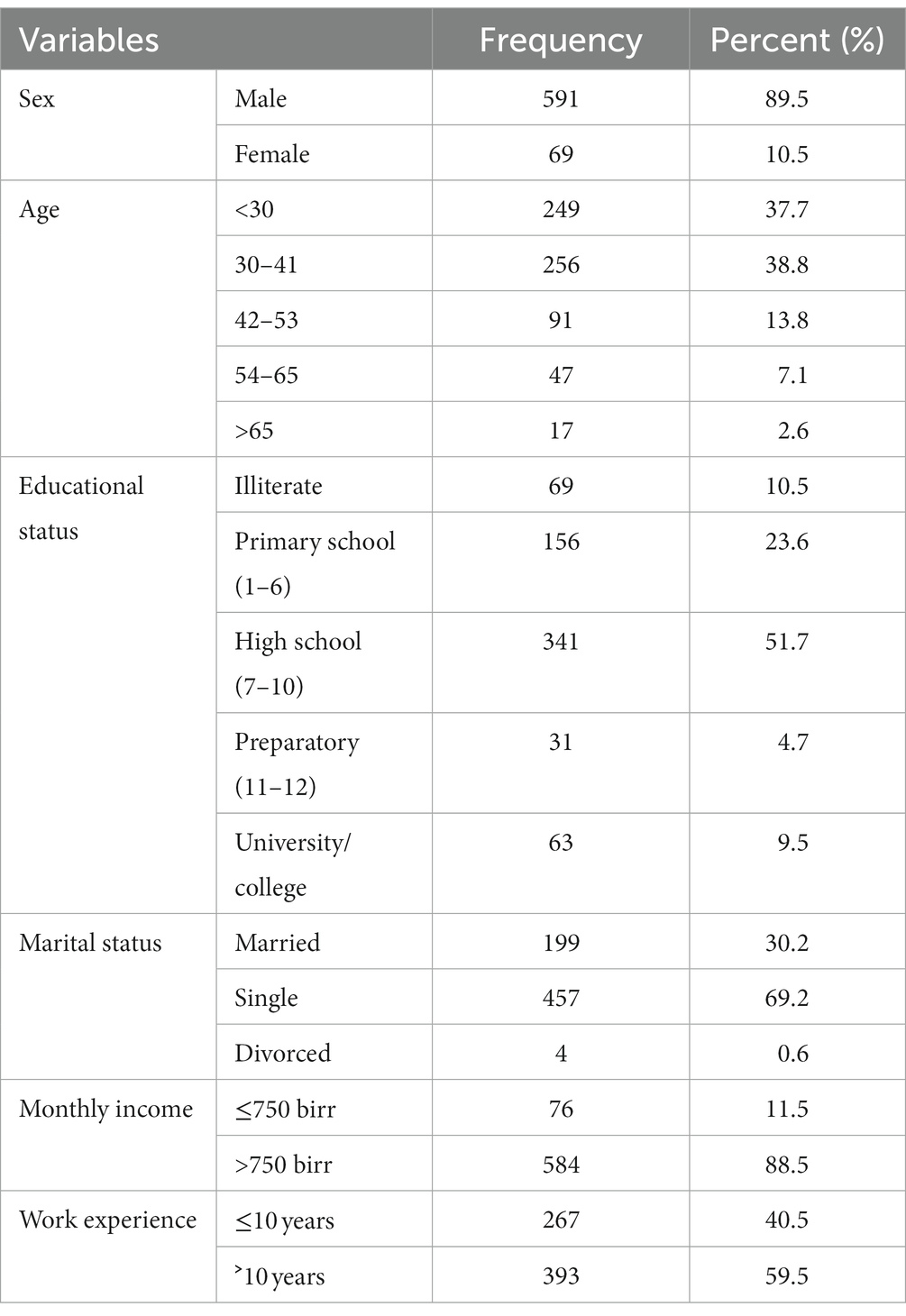
Table 1. Socio-demographic characteristics of traditional cloth weavers in the Gulele sub-city, Addis Ababa, Ethiopia, 2022.
Prevalence of low back pain among traditional cloth weavers
Among 660 respondents, 330 (50%) reported low back pain after beginning to weave (95%CI: 46.2, 53.9%). About 291 (44.1%) of respondents with low back pain during their job career experienced low back pain in the previous 12 months (95%CI: 40.3, 47.7%). Among weavers who reported having low back pain in the previous 12 months, 68 (10.3%) of them felt low back pain during the last 7 days. In terms of work absenteeism, 212 (32.1%) of the respondents were absent due to low back pain, with 102 (48.1%), 59 (27.8%) of the weavers were absent for 1–7 and more than 30 working days consecutively during the previous 12 months (Table 2).
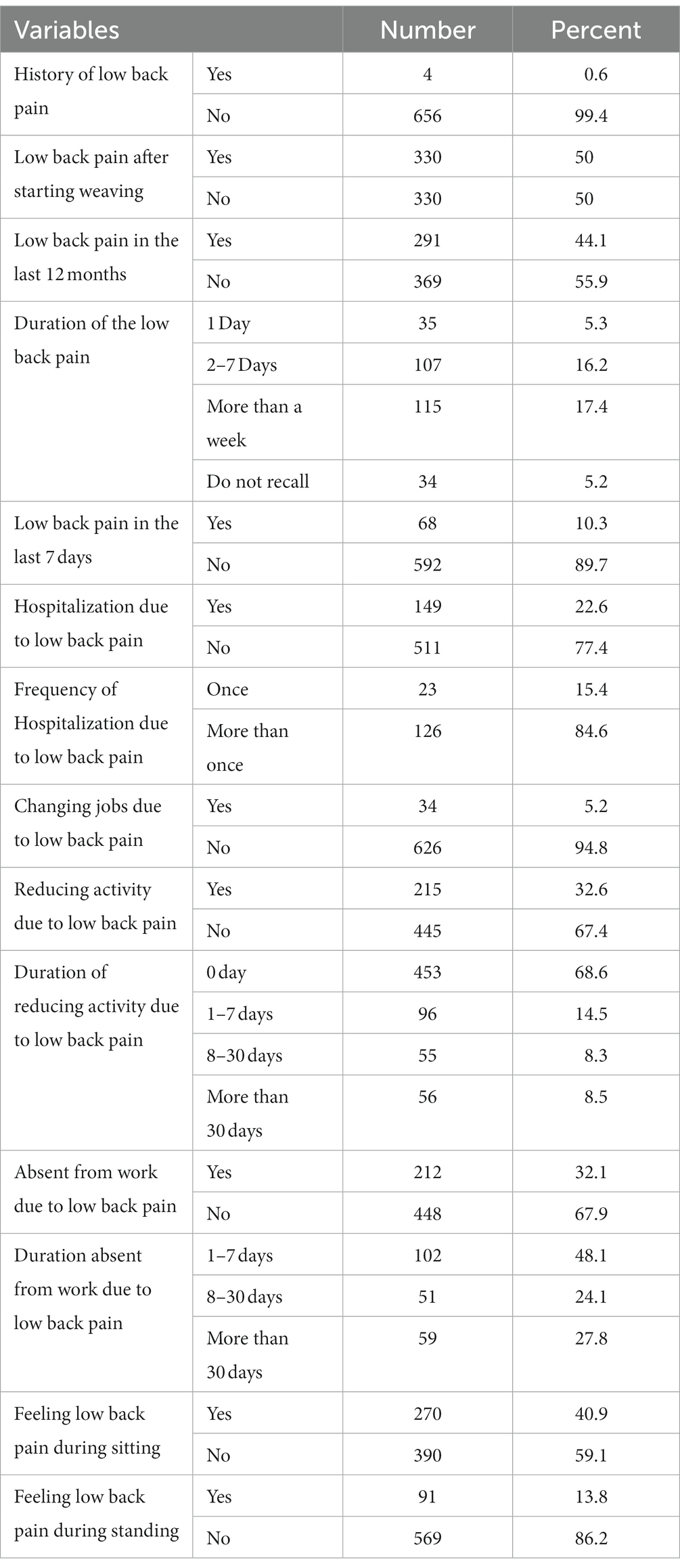
Table 2. Prevalence of low back pain among traditional cloth weavers in the Gulele sub-city, Addis Ababa, Ethiopia, 2022.
Socio-demographic determinants
Bivariate and multivariate analyses of socio-demographic determinants were performed using the logistic regression model. The bivariate logistic regression analysis revealed a statistically significant association between age group, educational status, monthly income, work experience, and low back pain. In the multivariate logistic regression analysis, low back pain was significantly associated only with lower monthly income (AOR 1.73, 95%CI 1.01, 2.95) and illiteracy (AOR 3.10, 95%CI 1.33, 7.20; Table 3).
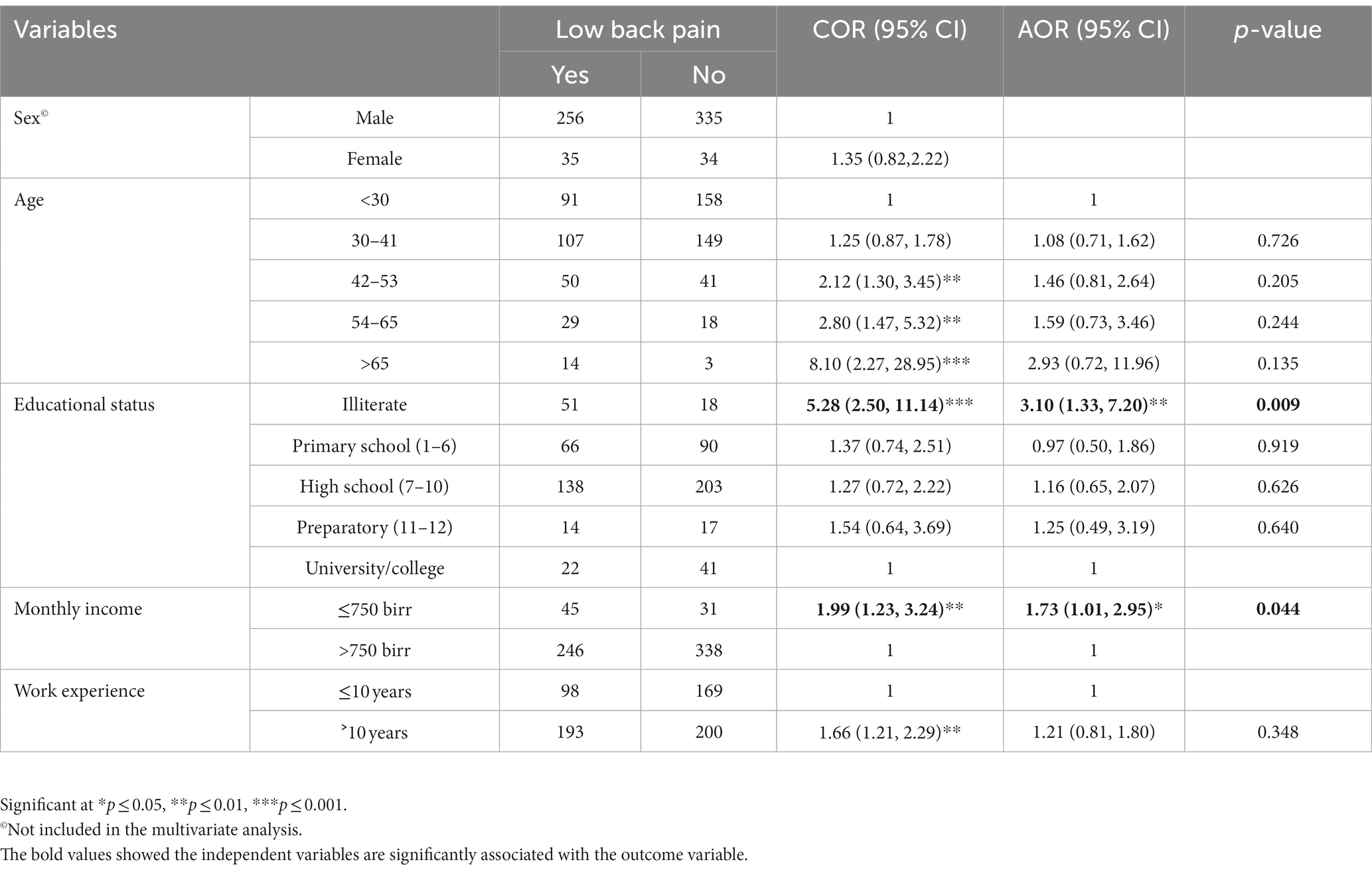
Table 3. Association between socio-demographic determinants and low back pain among traditional cloth weavers in the Gulele sub-city, Addis Ababa, Ethiopia, 2022.
Working condition and environmental determinants
Among working condition and environmental determinants, working for more than 8 h per day (AOR = 4.60, 95%CI 2.35, 8.87), working with frequent bending (AOR = 3.32, 95%CI 1.49, 7.40), working with uncomfortable posture (AOR =2.07, 95%CI 1.23, 3.49) and tasks creating pressure on the back (AOR = 4.41, 95%CI 1.87, 10.41) remained significant in the multivariate analysis (Table 4).
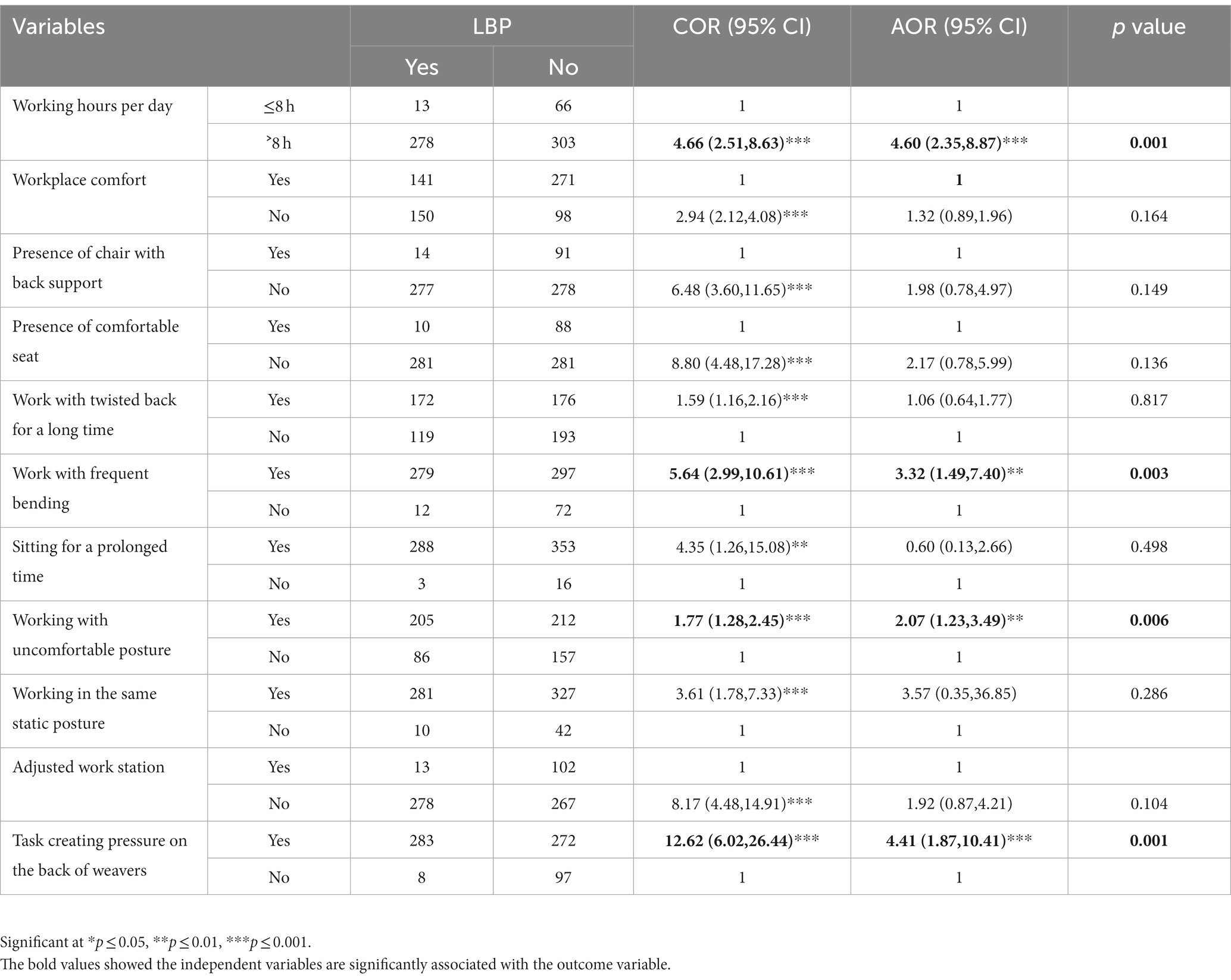
Table 4. Association between working condition and environment determinants and low back pain among traditional cloth weavers in the Gulele sub-city, Addis Ababa, Ethiopia, 2022.
Behavioral and psychosocial determinants
Among behavioral and psychosocial determinants, taking a break and resting time during the workday did not show a significant association with the occurrence of low back pain in the bivariate analysis. However, practicing regular physical activities (AOR = 1.77, 95%CI 1.21, 2.57), knowledge about the causes of low back pain (AOR = 4.49, 95%CI 3.14, 6.41), job stress (AOR = 1.68, 95%CI 1.18, 2.40), and job dissatisfaction (AOR = 1.63, 95%CI 1.13, 2.36) were significantly associated with the occurrence of low back pain (Table 5).
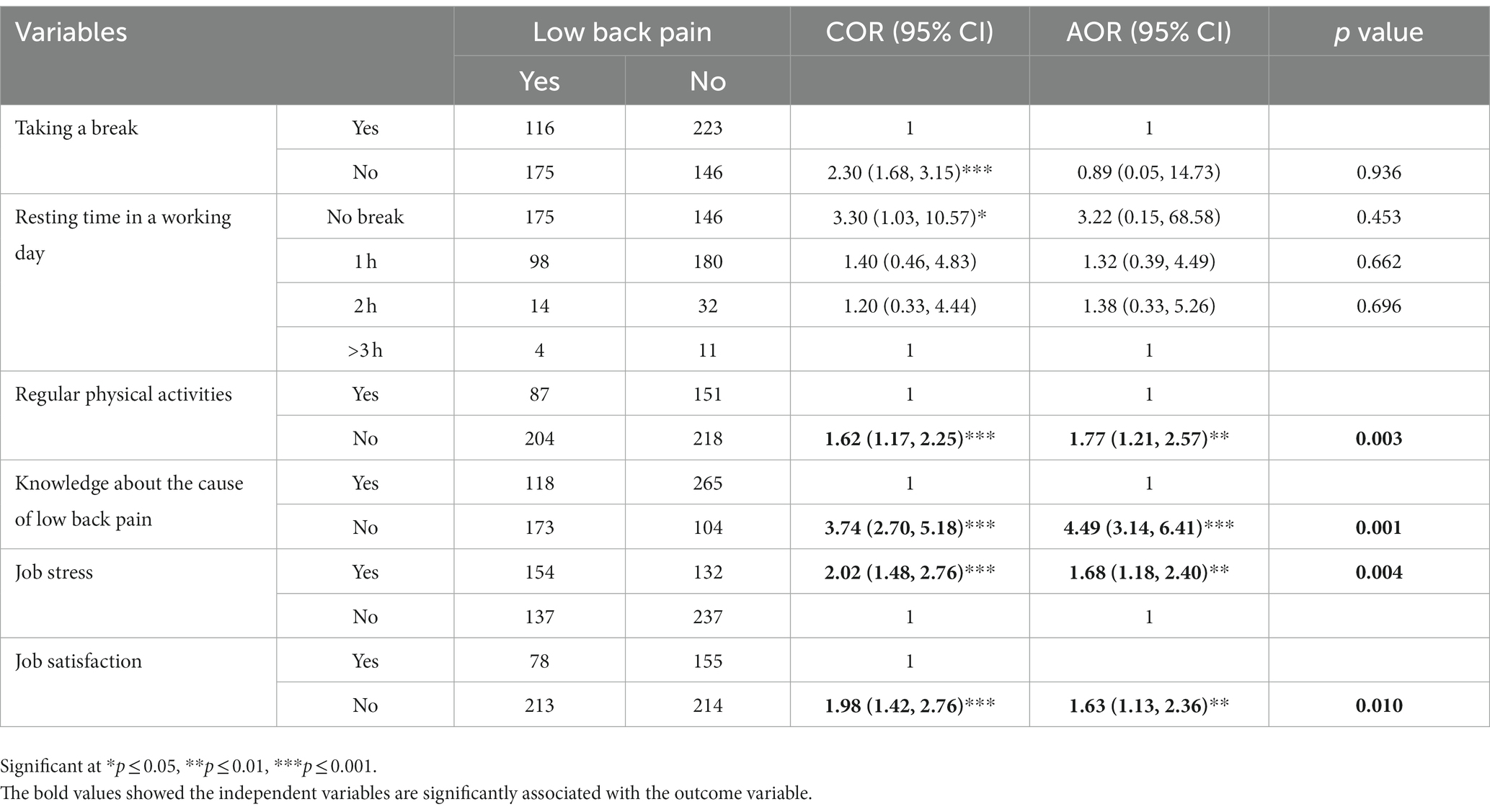
Table 5. Association between behavioral and psychosocial determinants and low back pain among traditional cloth weavers in the Gulele sub-city, Addis Ababa, Ethiopia, 2022.
Discussion
Weavers in small-scale industries and informal sectors had significantly higher rates of low back pain (27). Furthermore, traditional cloth weaving is one of the informal sectors that contribute significantly to the Ethiopian economy and its workers. However, the health issues associated with this sector did not receive the attention they deserved, and no research was conducted. As a result, the goal of this study was to determine the prevalence of low back pain and its associated factors among traditional cloth weavers in Addis Ababa’s Gulele sub-city.
According to the study’s findings, the prevalence of low back pain among traditional cloth weavers was 330 (50%) after they began weaving (95% CI: 46.2, 53.9%). The 12-month prevalence among study participants was 291 (44.1%) (95% CI: 40.3, 47.7%), which is comparable to studies done among Ethiopian young traditional cloth weavers (48.9%) and women weavers working with handlooms in Samarinda, Indonesia (28, 29). However, the prevalence of LBP is lower than in studies conducted in the weaving industries of Uttarakhand, Arunachal Pradesh, and Varanasi in India and Northern Thailand, where the prevalence of LBP was 67.19, 79.2, 82.91, and 81%, respectively (22, 24, 30, 31). The difference in the prevalence of LBP in these two studies could be attributed to differences in the working conditions of weavers. The Indian study focused on well-organized workshops with a poor working environment, whereas this study focused on individual households and cooperatives with less organized workshops. Furthermore, working conditions differ between handloom and power loom weaving in India and traditional cloth weaving in Ethiopia.
Weavers suffer from musculoskeletal disorders for a variety of reasons, the most important of which is the prolonged use of a constrained sitting posture (Figure 2). LBP was the most common complaint among those suffering from musculoskeletal disorders. According to research, weavers frequently experience pain in their lower back (32–35). Multiple factors may contribute to the occurrence of low back pain among weavers. According to this study, one of the factors that may contribute to the occurrence of LBP is illiteracy. According to this study, illiterate weavers were 3.10 times more likely than those with a college education or higher to develop LBP (AOR = 3.10, 95% CI: 1.33, 7.20). This finding was consistent with previous research conducted among Iranian petrochemical industry workers and women weavers using handlooms in Samarinda, Indonesia (28, 36). This study, on the other hand, contradicted a study conducted among textile factory workers in Amhara regional state, which discovered that educational status was not significantly associated with LBP (37).

Figure 2. Sampling chart of weaving facilities.
The number of working hours per day was another factor that could contribute to the occurrence of LBP among traditional cloth weavers. Weavers working more than 8 h per day were 4.60 times more likely to develop LBP than those working less than or equal to 8 h per day (AOR = 4.60, 95% CI: 2.35, 8.87). Furthermore, this study was consistent with previous research conducted among weavers in Varanasi, India, LetmafoInduk Village, Insana Tengah District, Indonesia, and women weavers working with handlooms in Samarinda, Indonesia, which discovered that daily working time had a positive association with LBP among weavers (28, 30, 34). The reason for this could be that daily working hours in the weaving industry are not usually fixed; they vary depending on the situation and workload, and the desire to earn more money drives weavers to work longer hours. Furthermore, the long working hours cause fatigue of the physical endurance of the muscles and bones, resulting in low back pain (32). This study, however, contradicted previous research conducted among textile industry workers in Pakistan, weavers in Varanasi, India, and weavers in Pathrail union in Tangail district, Bangladesh, which discovered that working hours were not significantly associated with the occurrence of low back pain (30, 38, 39).
Several occupational risk factors are associated with the weaving method, including the requirement to sit for long periods of time with the trunk forward bent (Figure 3), as well as activities such as pulling, pushing, lifting tools, working while bent or twisted at the waist, and repetitive motions with hands/wrists and gripping (22, 24). Similarly, weavers who worked with frequent bending were found to be 3.32 times more likely to report LBP than those who did not (AOR = 3.32, 95%CI: 1.49, 7.40). This is because frequent bending involves the same joints and muscle groups, and when workers perform the same motion too frequently, too quickly, and for too long, frequent bending becomes dangerous to the weavers’ backs (22, 23, 40).

Figure 3. Working with the trunk bent for longer duration.
Weavers typically work while seated (Figure 4). Weavers’ use a variety of sitting postures while weaving, including forward flexion, upright posture, and side bending (22). Several studies in various professions, including weaving, have revealed that working in an awkward posture contributes to the occurrence of musculoskeletal problems in various body regions (21, 41). Similarly, weavers who worked in an uncomfortable posture were about 2.07 times more likely than those who did not work in an uncomfortable posture to report LBP (AOR = 2.07, 95% CI: 1.23, 3.49). Given that weavers used to weave for long periods of time while seated, with a stretched, extended body and repeatable movement, the outcome is not surprising. Furthermore, several studies among weavers discovered that bending, twisting, and static postures that put pressure on the back were risk factors for LBP (22, 24, 42). Weaving looms, for example, have a sitting arrangement with no cushion or back support, which weavers have reported as uncomfortable. It strains the lower limbs, calf muscles, and back (40, 42).

Figure 4. Working using a variety of posture including forward flexion and side bending.
The perception of weaving as stressful, physically and mentally demanding, a lack of adequate breaks, and the presence of long working hours have all contributed to weavers’ stress levels. Weavers who were stressed were 1.68 times more likely to complain of LBP than their counterparts (AOR = 1.68, 95% CI: 1.18, 2.40). A study of textile factory workers in Ethiopia’s Amhara regional state, as well as a study of young weavers in Ethiopia, who reported working under pressure and emotional abuse and were nearly twice as likely to develop LBP, backed up this finding (29, 37).
Finally, satisfaction with the working environment, current job, income from current job, and community status all played a role in the occurrence of LBP. Weavers who were dissatisfied were 1.63 times more likely than their counterparts to experience LBP (AOR = 1.63, 95% CI: 1.13, 2.36). A study conducted among weavers in Varanasi, supports this finding (30).
Conclusion
This study discovered a high prevalence of low back pain among traditional cloth weavers, indicating the need for immediate public health action to improve Ethiopian traditional cloth weavers’ health. Having a higher income, taking breaks, engaging in regular physical activity, and having a job that you enjoy were all factors that could reduce your risk of LBP. Furthermore, working for more than 8 h per day, frequent bending, working in an uncomfortable posture, tasks that put pressure on the weaver’s back, and job stress were all linked to an increased risk of LBP. As a result, ergonomically oriented weaving workstations are required because the majority of WRMSDs are caused by poorly designed workstations. Even minor changes in working conditions, weaving tool design, and working methods can result in significant benefits, such as reduced bending, uncomfortable posture, and tasks that put strain on weavers’ backs. As a result, concerned stakeholders must act to improve working conditions in the traditional weaving sector in order to improve both weavers’ health and productivity of the weaving sector.
Limitation of the study
The Nordic Musculoskeletal Disorder Questionnaire cannot determine the risk level of low back pain symptoms, which is a limitation of this study. This study did not analyze the risk of low back pain symptoms among traditional cloth weavers because it was not the study’s goal. As a result, other researchers can investigate Musculoskeletal Disorder Symptom Risk Levels using methods other than the NMQ.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by University of Gondar review committee. The patients/participants provided their written informed consent to participate in this study.
Author contributions
AT has been contributed to idea inception, design methodology, data entry, data analysis, and manuscript preparation for publications. TJ and TW has been contributed to data collection, data entry, data analysis, and manuscript preparation for publications. All authors contributed to the article and approved the submitted version.
Acknowledgments
We are grateful to all of the data collectors, supervisors, study participants, and the Gulele sub-city micro and small-scale enterprise development agency office for their assistance in completing this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Vos, T, Allen, C, Arora, M, Barber, RM, Bhutta, ZA, Brown, A, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. (2016) 388:1545–602. doi: 10.1016/S0140-6736(16)31678-6
2. Shahijani, G, Karimi, A, Tavakol, R, Gharahzade, A, Mousavi, E, Tahernezhad, S, et al. Prevalence of musculoskeletal disorders among the surgical and anesthesia technologists in selected hospitals of Isfahan in 2018. J Adv Biomed Sci. (2020) 10:1943–50.
3. Heydari, M, Ghantab Pour, T, Zadi, O, Mahdavinoor, SMM, and Nasiri, E. Correlation between work-related musculoskeletal disorders and medical errors in surgical technologists of Mazandaran educational hospitals, Iran (2019). J Occup Health Epidemiol. (2020) 9:18–26. doi: 10.29252/johe.9.1.18
4. Huang, C, Kim, W, Zhang, Y, and Xiong, S. Development and validation of a wearable inertial sensors-based automated system for assessing work-related musculoskeletal disorders in the workspace. Int J Environ Res Public Health. (2020) 17:6050. doi: 10.3390/ijerph17176050
5. Allegri, M, Montella, S, Salici, F, Valente, A, Marchesini, M, Compagnone, C, et al. Mechanisms of low back pain: a guide for diagnosis and therapy. F1000Research. (2016) 5:F1000 Faculty Rev-1530. doi: 10.12688/f1000research.8105.2
6. Garland, EL. Pain processing in the human nervous system: a selective review of nociceptive and biobehavioral pathways. Prim Care. (2012) 39:561–71. doi: 10.1016/j.pop.2012.06.013
7. Hoy, D, Bain, C, Williams, G, March, L, Brooks, P, Blyth, F, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. (2012) 64:2028–37. doi: 10.1002/art.34347
8. Hurwitz, EL, Randhawa, K, Yu, H, Côté, P, and Haldeman, S. The global spine care initiative: a summary of the global burden of low back and neck pain studies. Eur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc. (2018) 27:796–801. doi: 10.1007/s00586-017-5432-9
9. Mutubuki, EN, Luitjens, MA, Maas, ET, Huygen, FJPM, Ostelo, RWJG, van Tulder, MW, et al. Predictive factors of high societal costs among chronic low back pain patients. Eur J Pain Lond Engl. (2020) 24:325–37. doi: 10.1002/ejp.1488
10. Hartvigsen, J, Hancock, MJ, Kongsted, A, Louw, Q, Ferreira, ML, Genevay, S, et al. What low back pain is and why we need to pay attention. Lancet Lond Engl. (2018) 391:2356–67. doi: 10.1016/S0140-6736(18)30480-X
11. Dima, A, Lewith, GT, Little, P, Moss-Morris, R, Foster, NE, and Bishop, FL. Identifying patients’ beliefs about treatments for chronic low back pain in primary care: a focus group study. Br J Gen Pract J R Coll Gen Pract. (2013) 63:e490–8. doi: 10.3399/bjgp13X669211
12. Froud, R, Patterson, S, Eldridge, S, Seale, C, Pincus, T, Rajendran, D, et al. A systematic review and meta-synthesis of the impact of low back pain on people’s lives. BMC Musculoskelet Disord. (2014) 15:50. doi: 10.1186/1471-2474-15-50
13. Nolet, PS, Kristman, VL, Côté, P, Carroll, LJ, and Cassidy, JD. Is low back pain associated with worse health-related quality of life 6 months later? Eur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc. (2015) 24:458–66. doi: 10.1007/s00586-014-3649-4
14. Oakman, J, Clune, S, and Stuckey, R. Work-related musculoskeletal disorders in Australia. Canberra: Safe Work Australia. (2019).
15. Sun, Y, Nimbarte, AD, and Motabar, H. Physical risk factors associated with the work-related neck/cervical musculoskeletal disorders: a review. Ind Syst Eng Rev. (2017) 5:44–60. doi: 10.37266/ISER.2017v5i1.pp44-60
16. Bruno Garza, JL, and Young, JG. A literature review of the effects of computer input device design on biomechanical loading and musculoskeletal outcomes during computer work. Albin TJ, editor. Work. (2015) 52:217–30. doi: 10.3233/WOR-152161
17. Qibtiyah, M. Ergonomic risk analysis and musculoskeletal disorders (MSDs) on operator uniformity final inspection. (2022) 3.
18. Coelho, DA, Tavares, CSD, Lourenço, ML, and Lima, TM. Working conditions under multiple exposures: a cross-sectional study of private sector administrative workers. Arezes P, editor. Work. (2015) 51:781–9. doi: 10.3233/WOR-152025
19. Lima, TM, and Coelho, DA. Ergonomic and psychosocial factors and musculoskeletal complaints in public sector administration – a joint monitoring approach with analysis of association. Int J Ind Ergon. (2018) 66:85–94. doi: 10.1016/j.ergon.2018.02.006
20. Naidoo, RN, and Haq, SA. Occupational use syndromes. Best Pract Res Clin Rheumatol. (2008) 22:677–91. doi: 10.1016/j.berh.2008.04.001
21. Mallapiang, F, Azriful, N, Syarfaini, MM, and Adriansyah,. The relationship of posture working with musculoskeletal disorders (MSDs) in the weaver West Sulawesi Indonesia. Gac Sanit. (2021) 35:S15–8. doi: 10.1016/j.gaceta.2020.12.005
22. Naz, H, Kwatra, S, and Ojha, P. Prevalence of musculoskeletal disorders among handloom weavers of Uttarakhand: an ergonomic study. J Appl Nat Sci. (2015) 7:102–5. doi: 10.31018/jans.v7i1.571
23. Pandit, S, Kumar, P, and Chakrabarti, D. Ergonomic problems prevalent in handloom units of north East India (2013) 3:7.
24. Pavana,, and Mica, N. Work-related musculoskeletal disorders among traditional weavers of districts of Arunachal Pradesh - a cross sectional study. Indian J Physiother Occup Ther-Int J [Internet]. (2021) 15:71–80. doi: 10.37506/ijpot.v15i3.16165
25. Muchiri, F, and Seblework, D. Traditional women weavers in Addis Ababa, Ethiopia: Occupational safety, health and working conditions [special topic:] small-scale enterprises and informal sector - International Labour Organization [internet]. (2012). Available at: https://labordoc.ilo.org/discovery/fulldisplay/alma994784943402676/41ILO_INST:41ILO_V2 (Accessed January 31, 2023).
26. Alemayehu, W. “Unleashing the potential of MSMEs in Ethiopia” CDP-handlooms cluster diagnostic study report. [internet]. (2006). Available at: http://backonline.apswiss.ch/6001/dsr_guellele_handlooms.pdf (Accessed February 18, 2022).
27. Nazari, J, Mahmoudi, N, Dianat, I, and Graveling, R. Working conditions in carpet weaving workshops and Muscu-loskeletal complaints among Workers in Tabriz-Iran. Health Promot Perspect. (2012) 2:265–73. doi: 10.5681/hpp.2012.032
28. Muhamad Ramdan, I, Candra, KP, and Rahma, FA. Factors affecting musculoskeletal disorder prevalence among women weavers working with handlooms in Samarinda. Indonesia Int J Occup Saf Ergon. (2018) 26:507–13. doi: 10.1080/10803548.2018.1481564
29. Tefera Zele, Y, Ahmed, AN, Wondie, Y, Yilma, TM, Gebreegziabher, HW, Weldegebreal, MK, et al. Prevalence of low back pain and associated factors among young workers in traditional weaving of the informal sectors, central and southern Ethiopia. Vulnerable Child Youth Stud. (2020) 15:48–59. doi: 10.1080/17450128.2019.1683926
30. Siddiqui, LA, Banerjee, A, Chokhandre, P, and Unisa, S. Prevalence and predictors of musculoskeletal disorders (MSDs) among weavers of Varanasi, India: a cross-sectional study. Clin Epidemiol Glob Health. (2021) 12:100918. doi: 10.1016/j.cegh.2021.100918
31. Chantaramanee, N, Taptagaporn, S, and Piriyaprasarth, P. The assessment of occupational ergonomic risks of handloom weaving in northern Thailand. Science & Technology Asia (2015) 20:29–37.
32. Suryati, Y, and Nggarang, BN. Analysis of working postures on the low Back pain incidence in traditional Songket weaving craftsmen in Ketang Manggarai Village. NTT J Epidemiol Public Health. (2020) 5:469–76. doi: 10.26911/jepublichealth.2020.05.04.09
33. Datta, DB, Sarkar, B, and Biswas, A. Effectiveness of self-care training module for work-related musculoskeletal disorders among handloom weavers at Udaynarayanpur. West Bengal SMS J Entrep Innov. (2022) 8:46–55.
34. Ruliati, LP, Limbu, R, and Sopbaba, A. Ergonomic risks associated with musculoskeletal disorders in ikat weaving Workers in Letmafo Induk Village. Insana Tengah District: Timor Tengah Utara Regency (2021).
35. Meenaa, ML, Singhb, AK, and Dangayach, GS. Measuring Quality of Work Life among Workers in Carpet Industries of Jaipur. Available at: http://nebula.wsimg.com/8dfbbd8eac24fd32d829d6684f3519b5?AccessKeyId=5F3CC2159ACF9F0B97B9&disposition=0&alloworigin=1 (Accessed January 29, 2023).
36. Choobineh, AR, Daneshmandi, H, Aghabeigi, M, and Haghayegh, A. Prevalence of musculoskeletal symptoms among employees of Iranian petrochemical industries: October 2009 to December 2012. Int J Occup Environ Med. (2013) 4:195–204.
37. Aderaw, Z, Engdaw, D, and Tadesse, T. Determinants of occupational injury: a case control study among textile factory Workers in Amhara Regional State. Ethiopia J Trop Med. (2011) 2011:1–8. doi: 10.1155/2011/657275
38. Khan, UA, Usama, M, Ahmad, A, and Gillani, SA. Frequency of neck and low Back pain and its associated risk factors among textile industry workers. J Riphah Coll Rehabili Sci. (2020) 8:1. doi: 10.5455/JRCRS.202008SI03
39. Rahman, AM, Khan, MH, Hossain, I, and Bari, S. Musculoskeletal problems among handloom workers. Texila Int J Public Health. (2017) 5.
40. Badanayak, P, and Kulloli, SD. Socio-economic status and associate health problems of Guledgudda Khana weavers. Int J Curr Microbiol Appl Sci. (2018) 12:378–81. doi: 10.15740/HAS/AJHS/12.2/378-381
41. Durlov, S, Chakrabarty, S, Chatterjee, A, Das, T, Dev, S, Gangopadhyay, S, et al. Prevalence of low back pain among handloom weavers in West Bengal. India Int J Occup Environ Health. (2014) 20:333–9. doi: 10.1179/2049396714Y.0000000082
Keywords: low back pain, weavers, prevalence, musculoskeletal—disorders, factors
Citation: Terfe A, Jemal T and Waqkene T (2023) Prevalence of low back pain and its associated factors among traditional cloth weavers in Gulele sub-city, Addis Ababa, Ethiopia. Front. Public Health. 11:1181591. doi: 10.3389/fpubh.2023.1181591
Edited by:
Loveness Anila Nkhata, University of Zambia, ZambiaReviewed by:
Emma Sala, Civil Hospital of Brescia, ItalyReza Tavakkol, Mashhad University of Medical Sciences, Iran
Copyright © 2023 Terfe, Jemal and Waqkene. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amare Terfe, YW1hcmV0ZXJmZUBnbWFpbC5jb20=; YW1hcmV0ZXJmZTJAZ21haWwuY29t