 Bernadetta Repka1,2
Bernadetta Repka1,2 Grzegorz Bejda3†
Grzegorz Bejda3† Agnieszka Kułak-Bejda4*†Damian Czarnecki5†Marcin Ziółkowski5†Anna Mosiołek6†
Agnieszka Kułak-Bejda4*†Damian Czarnecki5†Marcin Ziółkowski5†Anna Mosiołek6† Agata Szulc6†Napoleon Waszkiewicz4†Anna Ślifirczyk7†Wojciech Kułak8
Agata Szulc6†Napoleon Waszkiewicz4†Anna Ślifirczyk7†Wojciech Kułak8 Elżbieta Krajewska-Kułak9†
Elżbieta Krajewska-Kułak9†- 1Medical College of the Universal Education Society, Łomża, Poland
- 2MindHealth Mental Health Center, Białystok, Poland
- 3The School of Medical Science in Białystok, Białystok, Poland
- 4Department of Psychiatry, Medical University, Białystok, Poland
- 5Department of Preventive Nursing, Nicolaus Copernicus University, Toruń, Poland
- 6Department of Psychiatry, Faculty of Health Sciences, Medical University of Warsaw, Warszawa, Poland
- 7Siedlce University of Natural Sciences and Humanities, Siedlce, Poland
- 8Department of Pediatric Rehabilitation and Center of Early Support for Handicapped Children “Give a Chance”, Medical University of Białystok, Białystok, Poland
- 9Department of Integrated Medical Care, Medical University of Białystok, Białystok, Poland
Introduction: Homelessness is considered to be a global problem, independent of the material situation of a given country and occurring in most societies around the world.
Aim of the study: Assessment of the preferred health behaviors of homeless people.
Materials and methods: The study covered 153 men who are homeless and 312 men who are not homeless. The original questionnaire of homeless, and validated the Satisfaction with Life Scale (SWLS), the Health Behavior Inventory (HBI), the General Self-Efficacy Scale (GSES) and the Multidimensional Health Locus of Control (MHLC) Scale were used. The research covered fully completed questionnaires from 153 homeless men staying in Białystok and Gdańsk homelss centers.
Results: On average, the homeless men assessed their health at 6.0 ± 2.7 points, and the non-homeless at 7.8 ± 2.2 points (p < 0.001). Significant differences were found between people experiencing a homelessness crisis and the control group in selected aspects concerning the everyday life hygiene of the respondents, health self-assessment, declarations of visits to a specialist and carrying out check-ups, level of satisfaction with life, coping with difficult situations, preferred pro-health behaviors and dimensions of health control. In the used scales, SWLS, HBI, GES, and MHCL, the majority of homeless men obtained average scores. They were rather dissatisfied with their lives, with a low level of effectiveness in coping with difficult situations and obstacles, a low level of health behaviors, and in the scope of health, control increasing the impact of chance.
Conclusion: The level of the presented health behaviors showed statistically significant diversification with all dimensions of the health locus of control, and its internal dimension with age, homelessness phase, the respondents’ criminal history, being under constant medical care, and self-assessment of health.
Introduction
Homelessness is considered to be a global problem, independent of the material situation of a given country and occurring in most societies around the world. The population of homeless people is internally very diversified, although it is possible to observe in it some life situations typical for this group, most often of a social, economic, psychological, legal or health nature (1). However, the literature on the subject lacks a consensus as to the exact definition of homelessness and a consensus as to whether people living in conditions described as ‘homeless’ consider themselves as such (2). In general, homelessness is defined as ‘the state of a lack of a home’ (3), which does not reflect the actual scope of the problem. Homelessness is living without a home and the inability to satisfy basic needs. Therefore, the definition of homelessness should not exclude people living in inadequate housing conditions or temporary accommodation. The UN report, after Brannon (4), distinguishes the following types of homelessness: rough sleeping (sleeping on the street, under a bridge, or in a public place–temporary, seasonal, short-or long-term); living on the sidewalk (use of the ‘pitch’ and shelter under cardboard, fabric or plastic–short- or medium-term); squatting (regularly staying in the same abandoned building for a short or medium period); living in poor, often unsafe accommodation (on boats or other floating platforms without protection or services, which do not pass all adequacy tests–long-term or permanent) and refugee camps (life without the possibility of returning home–long-term or permanent). Based on ETHEOS 2008, the Polish Typology of Homelessness was developed (5, 6); it distinguishes rooflessness (living without a roof over their head in public spaces), houselessness (staying in facilities for the homeless, in shelters, temporary and transitional accommodation, medical and penitentiary institutions without a residential address); unsecured accommodation (living in unsecured/insecure accommodation temporarily with family/friends); inappropriate/inadequate accommodation (living in temporary/unconventional, fragile constructions/structures – mobile homes, unconventional buildings, temporary structures).
Nearly 155 million people are thought to be homeless and stay in temporary shelters, refugee camps, and other transitional conditions, with another billion living without adequate shelter. It is estimated that by 2050, this number will reach 3 billion. The largest increase in the homelessness rate was recorded in Iceland (by 168% from 2009 to 2017, although the homelessness rate remained low, at 0.1% of the total population). In turn, Norway and Finland recorded the largest decreases in the homelessness rate (in Norway, it fell by 40% in 2012–2016, and in Finland by 39% in 2010–2018). In such countries as Austria, Canada, Denmark, Poland, Slovenia, and Sweden, the homelessness rate has remained relatively stable in recent years (7). In Israel, in 2018–2020, the homeless population almost doubled, from about one person to almost 800 people (7).
At this point, it is worth noting that compared to the countries of Western Europe and other developed countries of the world, where the issue of homelessness has been the subject of systematic reflection in social sciences for many decades, this phenomenon was scientifically diagnosed in Poland very late (8) and it is a problem that is still not fully diagnosed. A relatively new phenomenon in Poland is the increase in the group of homeless foreigners, who often stay illegally, and the so-called ‘homeless by choice’ who wander from city to city (free birds, ‘giants’, vagabonds), who reject all applicable norms and consciously remain on the margins of social life (1).
Homelessness is associated with poorer health status and affects men, women, children, and veterans (9).
Several recent studies indicated that 20–31% of homeless adults endorse such alcohol related problems (10, 11). Compared with housed populations, alcoholism, anemia, and growth problems are more common among homeless persons.
In this study, we tried to evaluate the health behaviors in a group of men experiencing a homelessness crisis in Poland.
Health behaviors have been defined as ‘overt behavioral patterns, actions, and habits that relate to health maintenance, to health restoration, and to health improvement’ (12). A variety of behaviors fall within such a definition, including smoking, alcohol use, diet, physical activity, sexual behaviors, physician visits, medication adherence, screening, and vaccination. Four widely studied health behaviors that are a regular focus of attention are smoking, binge drinking and physical activity (13, 14).
Many health psychology research has examined the psychological determinants of health behaviors (15). Several general models of such determinants have been developed including the health belief model; protection motivation theory, self-determination theory, theory of reasoned action/theory of planned behavior; and social cognitive theory. These models contain several common determinants: intentions, self-efficacy, outcome expectancies, perceived susceptibility, and perceived severity.
Medical anthropology studies how health and illness are shaped, experienced, and understood in the context of cultural, historical, and political forces. Perhaps anthropology’s greatest contribution to our knowledge of homelessness has been a description and understanding of the methods of adaptation and survival in life on the streets and in the shelters (16). The thick, ethnographic descriptions of the daily rounds of the homeless have brought the concept of “the street” to life in these studies. As a group, anthropologists see the street (in its full metaphoric sense) as one of the sites for the kinds of adaptations to contemporary life that some homeless people make.
Understanding the experiences, practices, and perceptions of homeless people in health behaviors is essential to perform effective interventions to improve health outcomes. Furthermore, there are few studies on health behaviors in homeless people.
We wanted to explore selected aspects of mental health including health behaviors, self-efficacy, and locus of control in homeless men. The detailed aims included the assessment of selected health behaviors, need for health care and education, life satisfaction, the strength of the general conviction of the respondents as to the effectiveness of coping with difficult situations and obstacles, sense of the health locus of control and the dependence of the above on the phase of homelessness in the group of people experiencing homelessness crisis compared to those who do not experience it.
Materials and methods
The research performance received the consent of the Bioethics Committee, R-I- 449/2013. The main research was preceded by a pilot study in each group of 50 people, which made it possible to verify the clarity of the statements formulated in the questionnaires and to finally develop the original questionnaire. The research covered fully completed questionnaires from 153 homeless men staying in Białystok at the St. Brother Albert Home for the homeless of Caritas of the Archdiocese of Białystok, Men’s Night Shelter of Caritas of the Archdiocese of Białystok, Women’s Night Shelter of Caritas of the Archdiocese of Białystok, Emergency Help Point of the ELEOS Orthodox Mercy Center of the Białystok-Gdańsk Diocese and 312 people who do not experience a homelessness crisis (control group). The selection of the groups was purposeful, and the research was carried out with the diagnostic survey method with the use of:
Instruments
The original questionnaires (version for the homeless and those who are not homeless) consisting of 40 particular questions and questions concerning various aspects of homelessness was used. This survey was not validated. It consists of three parts.
PART I
1. Gender.
2. Age.
3. Marital status.
4. Do you have any children?
5. If so, do you keep in touch with them?
6. Last place of permanent residence:
7. Last place of work.
8. Education.
9. Have you ever had a criminal record?
10. Do you have an ID card?
11. Do you have permanent registration?
12. What are your current sources of income?
13. Are you ready to start work in the coming days if possible?
14. Do you think it is possible to get out of homelessness?
PART II
1. What phase of homelessness are you in?
2. Why did you become homeless?
3. Please indicate where you have been staying in the last year.
4. Do you have health insurance?
5. Do you have a certified disability group or degree of disability?
6. Do you use social assistance?
7. What forms of social assistance do you use?
8. What social assistance facilities do you know for the homeless?
PART III
1. On a scale of 0 to 10, how would you rate your current health?
2. When were you last hospitalized, and why?
3. How often do you use medical care?
4. Are you under constant medical supervision?
5. How often did you use medical services during the last year?
6. Do you follow the doctor’s recommendations?
7. What do you usually do when you feel sick, in pain, or have any ailments?
8. What medications have you used in the last year?*.
9. What are the most important diseases that currently affect you?
10. How often do you have a bath during the week?
11. When you last visited physician or dentist, he had an x-ray of the lungs.
12. How often do you eat the following meals - first breakfast, second breakfast, lunch, afternoon tea, dinner.
13. Do you smoke cigarettes? If so, since when, how much per day, how often.
14. Do you drink alcohol? If so, since when, how much per day, how often.
15. Which ailments do you feel Headaches, Lumbar spine pain, Cervical spine pain, Abdominal pain, Pain in lower limbs, Physical fatigue, Mental fatigue, Susceptibility to stress, Insomnia, Other, what.
16. Do you have any difficulties in performing the following daily activities, such as washing, dressing, moving around, preparing meals.
17. Do you have access to health services?
18. Where is access to health services for the homeless hindered?
19. Which doctor do you have the most difficult access to?
The standardized Satisfaction with Life Scale (SWLS), Diener, Emmons, Larsen, Griffin, in Polish Juczyński, version for other professionals who are not psychologists, to assess the extent to which the respondent relates to their current life was used (17). The Satisfaction With Life Scale (SWLS) consists of five statements. The subjects assessed the degree to which the statements describe their lives so far: 1 meant “I strongly disagree,” 2 – “I disagree,” 3 – “I somewhat disagree,” 4 – “I neither agree nor disagree,” 5 – “I somewhat agree,” 6 – “I agree” and 7 – “I strongly agree.” The scores were summed up, and the general result described the level of satisfaction with one’s life. The scores could range from 5 to 35 points, where higher values corresponded to higher satisfaction with life: 5–9 points – for a person extremely dissatisfied with his life, 10–14 points – for a person dissatisfied with his life, 15–19 points – a person slightly dissatisfied with his life, 20 points – a person neither satisfied nor dissatisfied with his life, 21–25 points – a person slightly satisfied with his life, 26–30 points – a person satisfied with his life, 31–35 points – a person delighted with his life. In the interpretation of the results, the specificity of the sten scale was also taken into account. 1–4 sten scores were considered low, 7–10 sten scores were considered high, and 5–6 sten scores were considered average. The Cronbach’s α values start at 0.86 (15).
The standardized Health Behavior Inventory (HBI) according to Juczyński – containing 24 questions describing various types of health-related behaviors (eating habits, preventive behaviors, positive mental attitudes, health practices) in the last 12 months (17). The answers to these questions were graded using a five-point scale where one corresponds to nearly never and five to nearly always. Based on this point system, the mean level of health behaviors was calculated for each category. The total HBI was calculated as the sum of all points gathered. Theoretically, the total HBI could range from 24 points (all answers graded 1) to 120 points (all answers graded 5). These values are presented and interpreted using the standard 10 scale (women: low 24–77 pts., moderate 78–91 pts., high 92–120 pts.; males: low 24–71 pts., moderate 72–86 pts., high 87–120 pts). Cronbach’s reliability index (alpha index) of HBI was calculated to be 0.85, ranging from 0.60 to 0.65 depending on the analyzed category of health behaviors.
The General Self-Efficacy Scale (GSES)–R. Schwarzer, M. Jerusalern, Z. Juczyński–measuring the strength of an individual’s general conviction as to the effectiveness of coping with difficult situations and obstacles (17). The respondent chooses one of four possible responses: no −1, rather no - 2, rather yes - 3, yes - 4. The total score presents a general indicator of self-efficacy, which can vary from 10 to 40 points. High scores represent a high sense of self-efficacy. The general indicator was transformed into standardized units and was interpreted according to the characteristics of the sten score. 1–4 sten scores were considered low, 7–10 sten scores were considered high, and 5–6 sten scores were considered average. The Cronbach’s α of the scale is high – 0.85.
The Multidimensional Health Locus of Control (MHLC-B) Scale version B of B. Wallston, B. S. Wallston, R. DeVellis, in the Polish adaptation of Juczyński – assessing generalized expectations of the respondents in three dimensions of the health locus of control: internal (conviction that control over my own health depends on me); the impact of others (conviction that the state of my health is the result of the impact of others, mainly medical personnel) and chance (the state of health depends on chance or other external factors). The results obtained allow the classification of the respondents into the following types: Strong Internal, Strong External, Decreasing the Impact of Others; Increasing the Impact of Others; Decreasing the Impact of Chance; Increasing the Impact of Chance, Undifferentiated-Strong and Undifferentiated-Weak (17).
Statistical analysis
The Statistica 13.0 PL program was used for statistical calculations. The Chi2 test was used to compare response rates between groups. Statistical relationships between satisfaction with life, health behaviors, coping with difficult situations and dimensions of the health locus of control in the surveyed group of homeless men and age, phase of homelessness and criminal record calculated with the use of multiple regression analysis. Statistical significance was evaluated at p < 0.05.
Characteristics of the study group
In the study group of 153 homeless men, the largest number was in the age range from 51 to 60 (36.6%), divorced men (55.5%), having children (59.5%), but not maintaining contact with them (53.6%). Most frequently, the respondents had a permanent address of residence in a city with a population over 200,000 (59.6%) and vocational education (52.3%), Details are shown in Table 1.
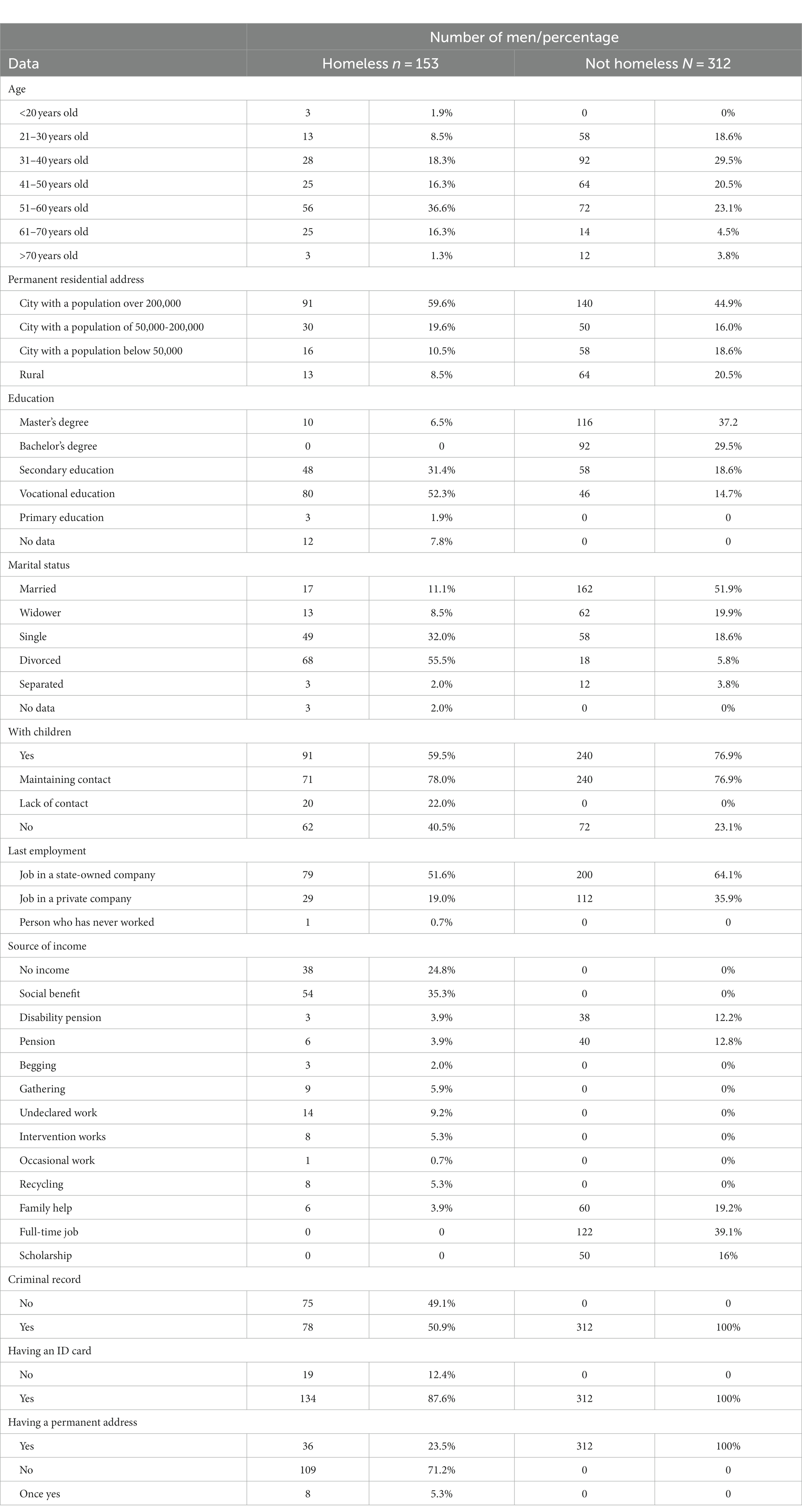
Table 1. Characteristics of the study group.
Results
The most common reasons for homelessness were eviction, residence address deregistration (41.8%), family conflicts (30.7%), unemployment, lack of work and lack of sources of income (22.2). Details are shown in Table 2.
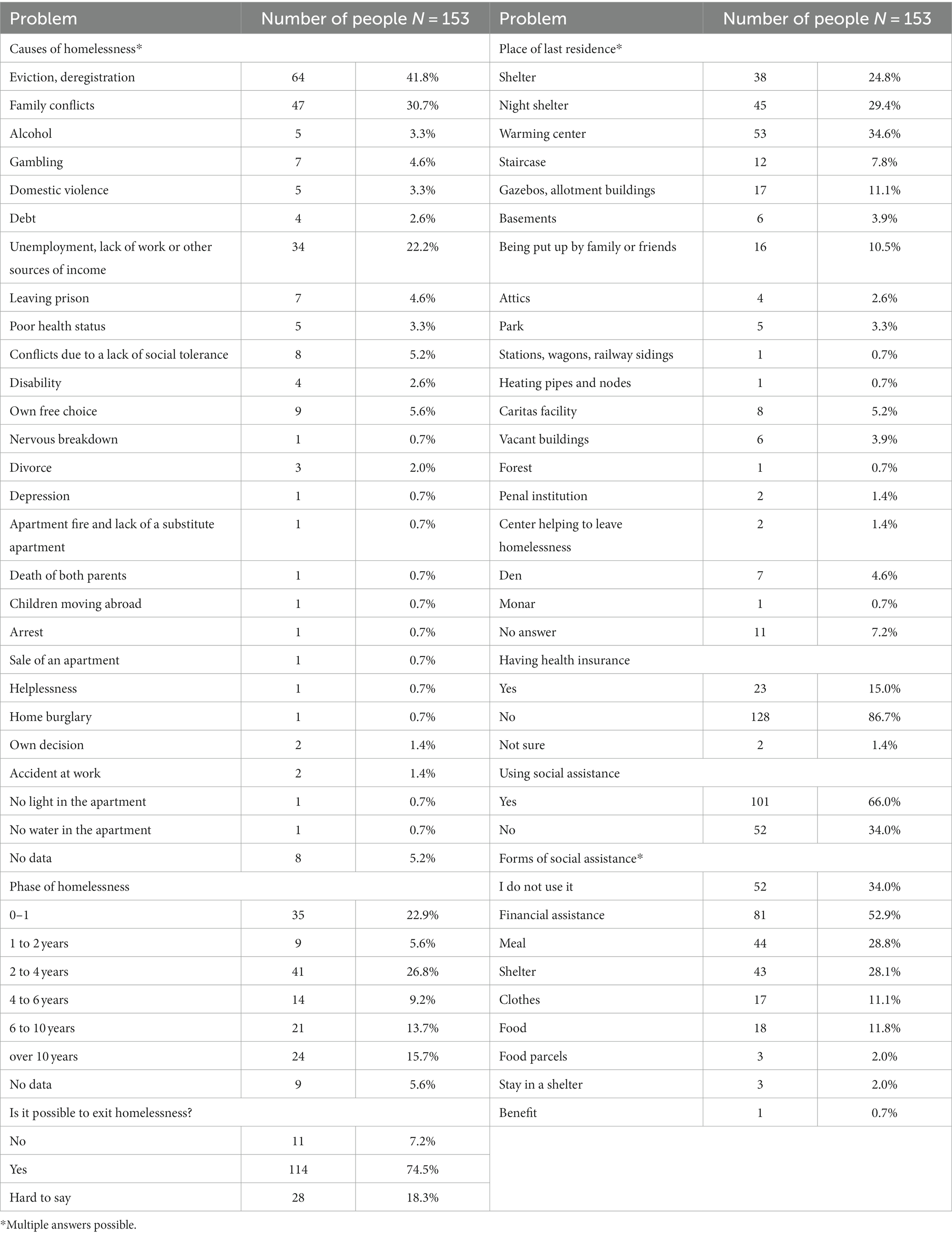
Table 2. Selected aspects of homelessness in the group of respondents.
The respondents indicated numerous social welfare facilities for the homeless, including night shelters (65.9%), warming centers (44.4%), and other shelters (people – 36.6%).
In the next part of the study, the health habits of the respondents were assessed. 92.2% of the surveyed homeless people and none of the men from the control group did not wash every day. The largest number of the homeless and men from the control group declared that they eat lunch (71.2 and 64.7% respectively) and dinner (77.1 and 58.3% respectively) every day. More than half (55%) of homeless drunk alcohol. Details are shown in Table 3.
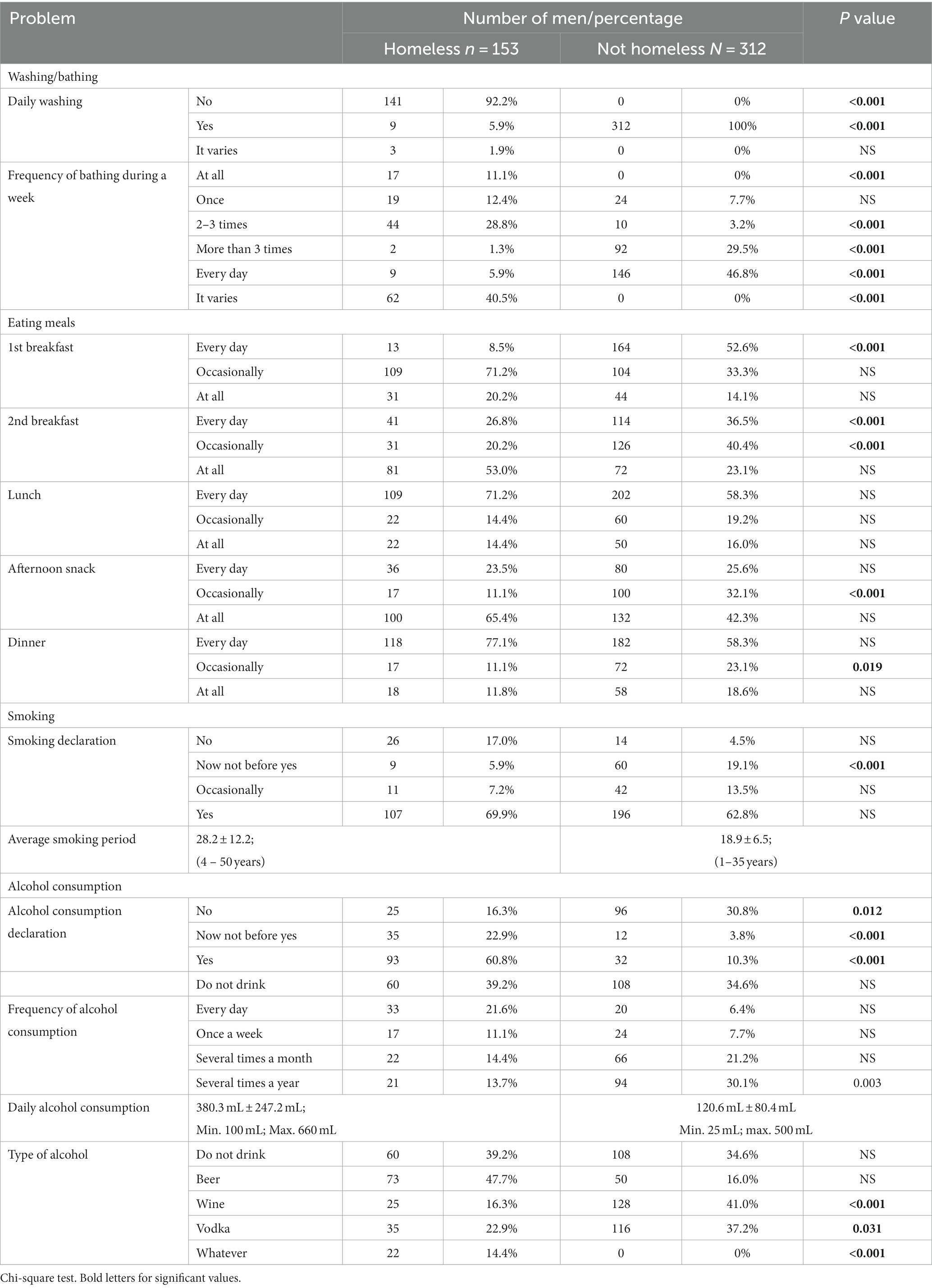
Table 3. Selected aspects concerning the everyday life hygiene of the respondents.
The respondents were asked to rate their health from 0 to 10 on a scale. Most frequently, the homeless chose 5 points in their health self-assessment (33 people–21.6%), and men from the control group chose 7 points (23.3%). The homeless men assessed their health poorer (6.0 ± 2.7 points) than the non-homeless (7.8 ± 2.2 points)(p < 0.001).
In the homeless group, 98 (64.1%) and 312 (91.0%) in the control group did not have a disability degree certificate.
The respondents declared that:
• they use professional medical assistance when necessary: the homeless–60 (39.2%) and the non-homeless – 80 (25.6%)–p = 0.030
• they did not use it at all: the homeless–39 (25.5%) and the non-homeless–10 (3.2%)–(p < 0.001)
• several times a year: the homeless–12 (7.8%) and the non-homeless–62 (19.9%)–p = 0.005
• several times a month: the homeless–7 people (4.6%) and the non-homeless–32 (10.3%)–NS
In a situation where they feel pain, any ailments:
• they immediately went to the doctor and used medicines prescribed by them–49 (32%) homeless people and 130 (41.7%) men from the NS control group
• they only used their own tested methods – 48 (31.4%) homeless people and 72 (23.1%) men from the NS control group
• they did nothing and tried to wait out the ailments–28 (18.3%) homeless people and 50 (16%) men from the NS control group
• they did not go to the doctor because they could not afford it–25 (16.3%) homeless people and 20 (6.4%) men from the control group p = 0.004
• 3 (2%) homeless people and 40 (12.8%) men from the control group had problems with the declaration on this issue p < 0.001
21 (13.7%) homeless people and 214 (68.6%) people from the control group (p < 0.001) used the help of the general practitioner.
In the last year, 48 (31.4%) surveyed homeless men and 70 (22.4%) from the control group did not use medical assistance–NS.
In the last year, 62 (40.5%) surveyed homeless men and 284 (91%) from the control group were not in hospital–p < 0.001.
In the last year they took antibiotics–50 (32.7%) homeless men and 139 (44.6%) from the control group–NS; vitamins–47 (30.7%) homeless men and 176 (56.4%) from the control group–p = 0.0019, analgesics–33 (21.6%) homeless men and 11 (3.5%) from the control group–p < 0.001; sedatives–31 (20.3%) homeless men and 36 (11.5%) from the control group–p = 0.034. No medications were taken by 34 (22.2%) homeless men and 56 (17.9%) from the control group–NS.
During the study, 74 (48.4%) homeless men and 112 (35.9%) from the control group reported they did not suffer from any disorders. Others most often complained about hypertension–14 (9.2%) homeless men and 116 (37.1%) from the control group–p < 0.001; back pain–10 (6.5%) homeless men and 18 (5.8%) from the control group–NS, asthma/allergy–8 (5.2%) homeless men and 48 (15.4%) from the control group–p = 0.007, heart problems–6 (3.9%) and 34 (10.9%) from the control group p = 0.031, diabetes–5 (3.3%) homeless men and 41 from the control group p < 0.001, epilepsy, gastric ulcer–4 (2.6%) homeless men alcoholism. In the control group, anemia was also reported–4 (1.3%) people, headaches/migraine–18 (5.8%) people, thyroid diseases–18 (5.8%) people, ophthalmological diseases–21 (6.7%) people, joint degeneration–19 (6.1%) people and lower limb varicose veins–6 (1.9%) people.
The respondents were asked about the declaration of visits for the internist, dentist and lung x-rays. Most often, the homeless claimed that they did not remember the last time they had visited an internist (53.6%), dentist (52.3%) and when they had a lung x-ray (51%). Details are shown in Table 4.
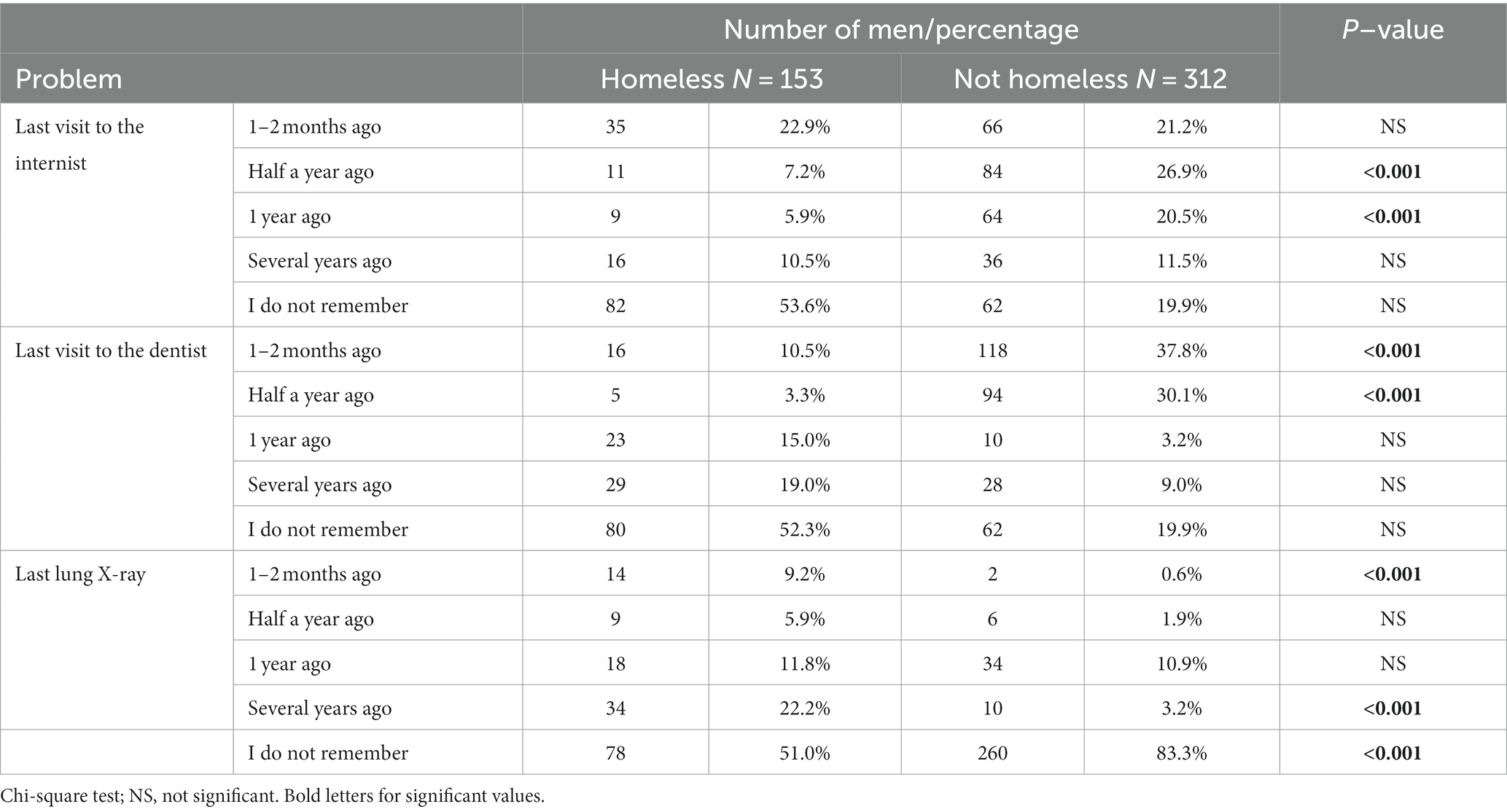
Table 4. Declaration of visits to the internist, the dentist, and for a lung X-ray.
Homeless men reported, sometimes they have a headache (34%), stomachache (32.7%), physical fatigue (36.6%), mental fatigue (34. 6%), stress (33.3%), insomnia (32%), and, every day, lower back pain (30.7%), and lower limb pain (36.6%). Men from the control group most often had a headache (39.1%), stomachache (31.4%), mental fatigue (33.3%), stress (35.9%), insomnia (42.9%), lower back pain (42.9%), lower limb pain (40.4%), neck pain (37.8%), and, every day, physical fatigue (30.1%). The results are shown in Table 5.
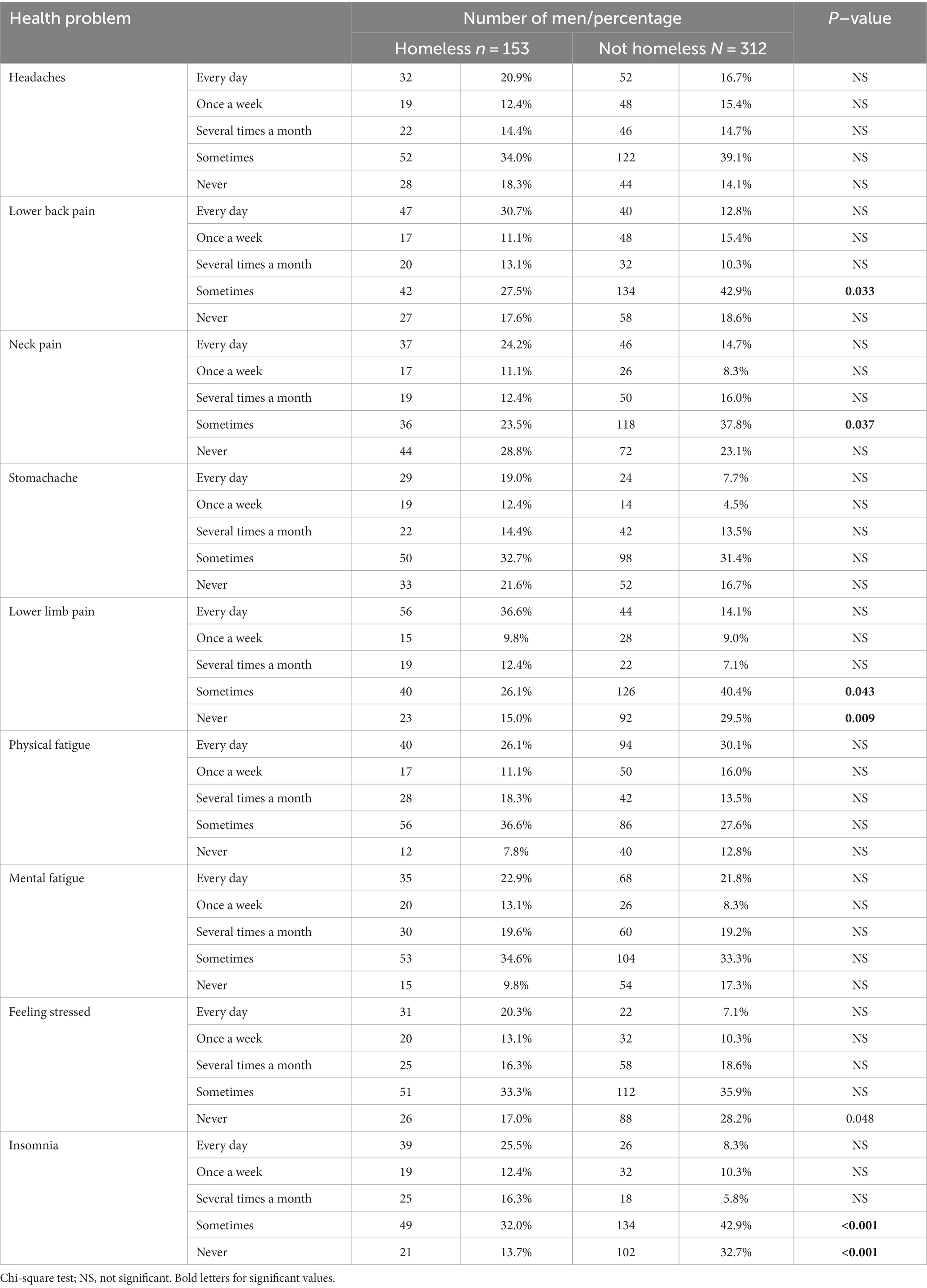
Table 5. Declaration of the frequency of experiencing selected ailments.
In the assessment of satisfaction with life (SWLS), the homeless men obtained 15.4 ± 8.1 points on average (people rather dissatisfied with their lives), and in the control group – 23.2 ± 5.5 on average (people rather satisfied with their lives). In assessing the effectiveness of coping with difficult situations and obstacles, the homeless men obtained 18.5 ± 5.7 points, and the control group obtained 29.1 ± 1.2 points. The homeless in the point scale in the assessment of health behaviors (HBI) obtained 62.4 ± 21.9 points on average, and the control group obtained 82.1 ± 10.8 points. The homeless obtained the highest average values for positive mental attitude (2.9 ± 1.1 points on average), and the control group for health practices (3.9 ± 0.7). The homeless and the control group obtained the lowest mean values for proper eating habits (2.3 ± 1.0 and 3.5 ± 0.9, respectively). In assessing the dimensions of the health locus of control, the homeless obtained the highest average values in the dimension of chance – 19.2 ± 9.1 points on average, and the control group in the internal dimension (26.0 ± 5.2). Details are shown in Table 6.
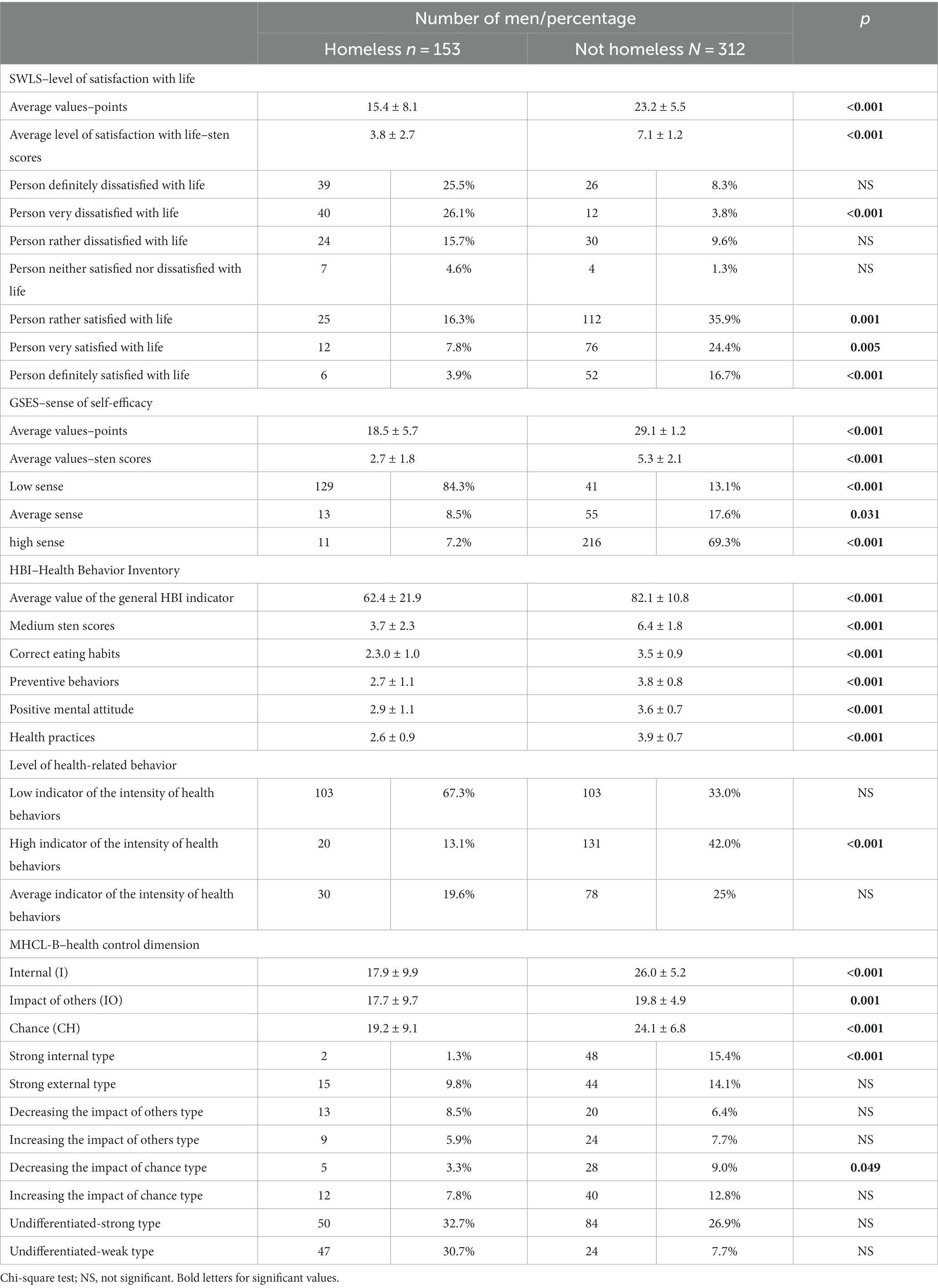
Table 6. Results of the analysis using SWLS, GSES, HBI and MHCL-B scales.
Statistically significant correlations were found between the internal dimension of health behavior control and age, homelessness phase, criminal history of the respondents, being under constant medical care and health self-assessment. The ‘Impact of others’ dimension showed significant statistical differences with the level of health behaviors, and the ‘chance’ dimension with the criminal record of the respondents. The level of the presented health behaviors showed statistically significant differences with all dimensions of the health locus of control (Table 7).
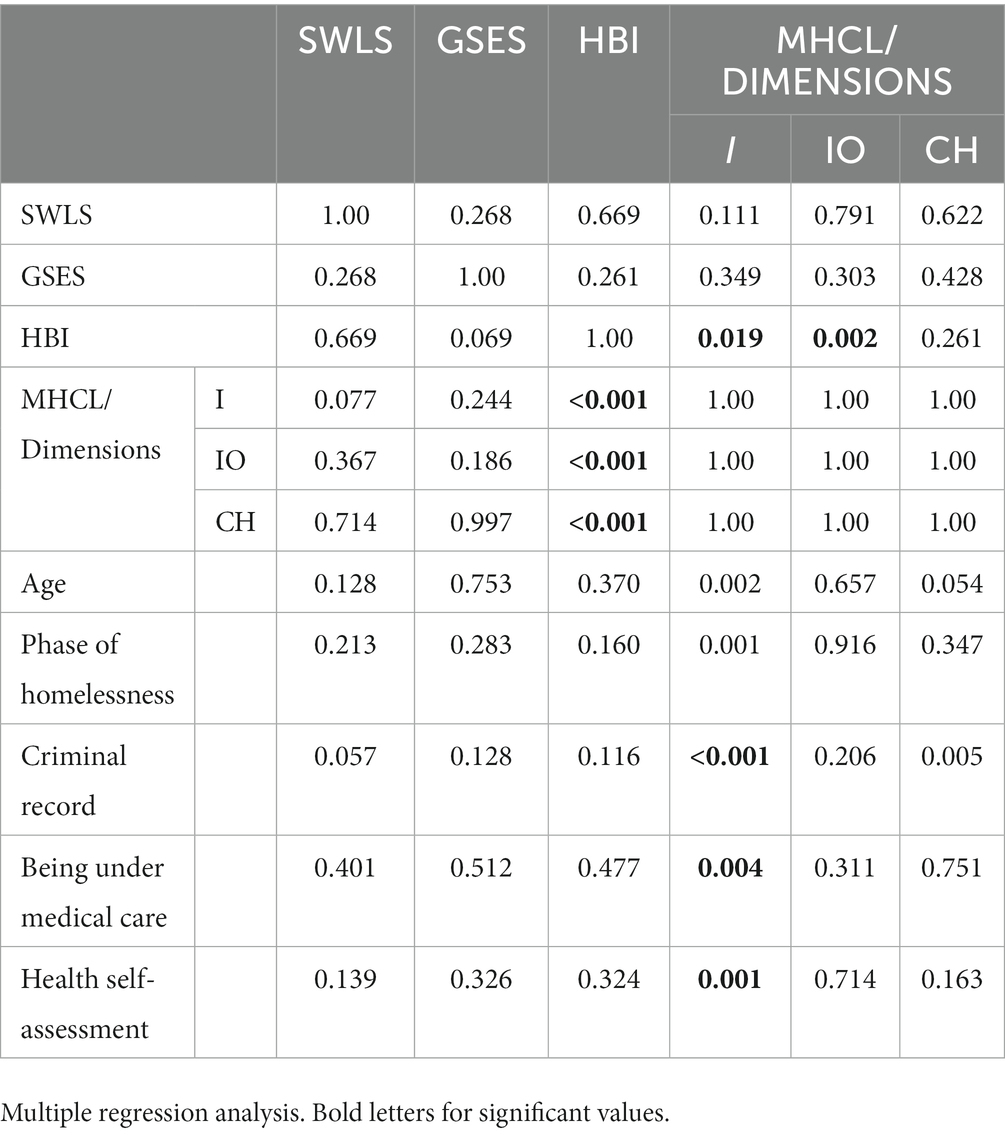
Table 7. Statistical relationships between satisfaction with life, health behaviors, coping with difficult situations and dimensions of the health locus of control in the surveyed group of the homeless and age, homelessness phase and criminal record.
Discussion
In the present study, health behaviors of homeless men showed statistically significant diversification with all dimensions of the health locus of control, and its internal dimension with age, homelessness phase, the respondents’ criminal history, being under constant medical care, and self-assessment of health. We found significant differences between the homeless men and controls in selected aspects concerning the everyday life hygiene, health self-assessment, declarations of visits to a specialist and carrying out check-ups, level of satisfaction with life, coping with difficult situations, preferred pro-health behaviors and dimensions of health control.
In the study by Baranowski (18), which covered 91 homeless people, 80.2% were men and people aged 51 to 60 (37.4%) and 41 to 50 (34.1%). This was confirmed by research conducted by Pindral (7), which also showed a much higher percentage of men in the homeless group (on average four times); research conducted by Śledzianowski (19)–in which he also found the dominance of men (90.7%) and the research from 2019, in which it was shown that the largest number of homeless people were aged 41–60 (45.5% of people) (20). The above was also confirmed in the current study, in which the largest number, i.e., 36.6%, of men were in the age range from 51 to 60.
In the study by Baranowski (18), 46.2% of the homeless declared vocational education, 24.1%–primary or incomplete primary education, 17.6%–secondary education, 7.7%–general secondary education, and 2.2%–lower secondary education or higher education. In the group Pindral [7] studied, 75% of homeless people had post-primary education, a 34% higher indicator than the homeless population. In the study by Śledzianowski (19), 50.8% of homeless people had vocational education, 23.5% had primary education, 21.2% had secondary or incomplete secondary education, and 3.9% had higher education.
The literature data show that the homeless population is also dominated by singles, divorcees, people in separation, children, and wives fleeing from home due to violence by their fathers or husbands (20). The homeless people in the 2011 study in Białystok, Suwałki (21) were most often (44%) divorcees; almost 30% of the respondents were unmarried, 15%–married, and 10% were widowed. This has been confirmed in the current study, where divorced people accounted for 55.5% of all homeless people and singles for 32%.
In the literature on homelessness (22, 23), there are certain levels of isolation of the homeless which make it difficult to get out of homelessness: economic level (failure to meet needs), social level (lack of interpersonal relationships), individual level (emotional disorders, low self-esteem) and institutional level (confusion in institutional support mechanisms). In the research of Baranowski (11), the most frequently indicated factors causing homelessness were family problems (42.9%) and addictions (41.8%). Inhabitants of Łódź studied by Bartczak et al. (22) indicated addictions (86.5%), eviction from the apartment (78.6%), and loss of a job (62.0%) or being abandoned by the closest family (48.1%) as reasons for becoming homeless. According to a 2019 study, the main cause of homelessness was family conflict (32.2%), addiction (28%), eviction, deregistration (26.3%) and relationship breakdown (18.4%) (22). This has also been confirmed in our research because, in the case of our respondents, the homelessness crisis was most often caused by eviction, deregistration (41.8%), and family conflicts (30.7%).
In the research by Baranowski (18), 62.6% of the homeless stayed in various institutions such as hostels, centers for the homeless, or social emergency centers, while the remaining 37.4% occasionally used the offers of eateries and came to various centers for food and clothes. The homeless surveyed by Olech (24), rarely used the services of facilities providing them with shelter, and during the last year, only 7% occasionally lived in a facility for homeless people. According to the 2019 study, 80.2% of the homeless stayed in institutional facilities, such as shelters, while the remaining 19.8% lived outside (20). Contrary to the above data, in the present study, only 24.8% indicated a shelter as the place of their last stay; the respondents most often indicated warming centers (34.6%) and night shelters (29.4%).
In the literature (21, 24, 25), there is a division of the typology of homeless people into homeless by choice, homeless by force, actually homeless at risk of homelessness, homeless by force, temporarily homeless by choice; shallowly homeless deeply homeless and permanently homeless temporarily homeless. Also (26) five stages of homelessness are distinguished: 1. breakdown of the life plan and breakdown of the family; 2. material poverty, cultural poverty, and social poverty; 3. different dimensions of becoming homeless; 4. adaptation to homelessness; 5. actual, chronic homelessness, when full adaptation to the state of homelessness takes place, lasting 6 to 10 years. The largest group in the 2019 study was people experiencing a homelessness crisis for more than 5 to 10 years–(27.8%) and homeless people for up to 2 years (23.4%) (20). In the current study, there were significantly more homeless people in the phase up to years (28.5%) and fewer in the group from 5 to 10 (21.9%). In the study of Baranowski (18) only 8.8% of homeless persons had a permanent legal job,
The main sources of income for the others were: occasional work (15.4% each), social assistance (12.1%), charitable organizations’ assistance (8.8%), disability pension/pension (17.6%), and collecting and selling scrap (5.5%).
Buciński et al. (26) emphasize that the health condition of homeless people is worse than that of the community leading a normal life, and the above depends on many factors and does not allow the treatment of homeless people in a universal way. Basically, the health problem of the homeless is affected by age, length of homelessness, place of stay of the homeless person, aging of the homeless community, and staying in public spaces that increase the risk to health and even life. The issue of homeless people’s health should be of key importance for social policy and the system of helping homeless people.
People without a roof over their heads, more often than others, do not have health insurance or an ID card (27). In the research carried out by Śledzianowski (19), 78.7% of women and 60.3% of men had health insurance. The current studies have also confirmed this, as most (86.7%) of our respondents did not have health insurance.
In the study of Śledzianowski (19), 28.7% had a disability degree certificate, usually moderate (64%). In the group of homeless people from the study conducted in 2011 in Białystok, Suwałki (21), 47% had a moderate disability degree, and 30% had a light disability degree. In contrast to the above, in the current study, 64.1% of homeless people did not have a disability certificate.
Heszen (28) emphasizes that health consists of four main dimensions: mental, social, somatic, and spiritual. In the context of homelessness, every aspect of health is important. 77.4% of homeless people from the Śledzianowski study (19) reported good health. In the current study, the respondents assessed their health as average.
The assessment of the health of the homeless in a shelter in Poznań city (29), showed that the most common diseases they had were parasitic and infectious skin diseases, alcoholism, tuberculosis, hypertension, diseases of the spine and musculoskeletal system, nervous system, and gastrointestinal tract. According to the study (21) conducted in 2011 in Białystok, Suwałki, 50% of the homeless reported feeling unhealthy. In the present study, 48.4% of the homeless claimed they did not suffer from any disorders.
While examining the health of the homeless in a shelter for homeless men in Poznań, Przymeński (29) stated that the homeless usually did not treat their diseases. Śledzianowski (19) demonstrated that 57.1% of the homeless people used medical services last year. In the current study, 31.4% of the respondents did not use medical assistance in the last year.
Przymeński (29) closely connects the poor health of the homeless to their living conditions, including poor hygiene, malnutrition, lack of adequate protection against low temperatures, constant stress, lack of satisfaction with basic mental and emotional needs, and addiction to drugs and alcohol. According to Tędzialgolska et al. (30), the daily functioning of homeless people was hindered by the lack of possibility to care for hygiene due to the lack of intimacy, basic toiletries, access to water, and clean clothes. This is also confirmed by our research, because as many as 92.2% of the respondents did not wash every day.
Błażej and Bartosz (26) think that excessive alcohol consumption is a very special feature of homeless people. In a Polish study (24), about 70–80% of adult homeless men are addicted to alcohol. In a French study (31), one in five homeless people was alcohol-dependent. In the current study, the respondents reported that they most often consume alcohol occasionally (55.5%).
Doctors who care for homeless people notice the following health problems: cardiological problems, the digestive, respiratory, urinary, and hormonal systems, cancers, skin diseases, frostbite, dental deficiencies, and HIV/AIDS (24, 32). In the study by Śledzianowski (19), 16.4% of the homeless suffered from congenital diseases, 3.5% from respiratory diseases, 3.3% from mental and neurological diseases, 2.7% from heart and circulatory system diseases, and 3% from musculoskeletal system diseases. In the current research, the respondents most often complained about hypertension (9.2%), back pain (6.5%), asthma (5.2%), heart problems (3.9%), diabetes, colds, pneumonia (3.3% each), epilepsy, gastric ulcer (2.6% each), alcoholism, prostatic hypertrophy, atherosclerosis, and hernia (2% each).
Homelessness brings such emotional effects as loneliness, powerlessness, fear, and anxiety (26, 33). On the other hand, 63.2% of the homeless people from the Śledzianowski study (19) believed they were valuable, and 61.5% did not lose self-confidence. Homeless people from the study by Bodys-Cupak et al. (34) declared a sense of external control over their health and a low sense of effectiveness. Similarly, in the current study, homeless people showed a low level of effectiveness in coping with difficult situations and obstacles but a high level of internal control, indicating the belief that control over their health lies with them. Unfortunately, the homeless respondents also showed a low level of satisfaction with life and a low level of health behaviors, the highest for the sphere of a positive mental attitude and the lowest for proper eating habits.
In conclusion, it is worth emphasizing once again that the problem of homelessness is a broad and extremely complicated phenomenon (35–37). The struggle for survival and the necessity to satisfy basic needs preclude focusing on one’s health and taking care of its good condition and often contributes to its deterioration. Therefore, several actions should be taken to protect health. Unfortunately, health for people in the homeless crisis is no longer a value and a determinant of action; hence, problems may arise in complying with the basic principles of treatment and in remission diseases. However, in the current study, as many as 60.1% of the respondents claimed that they always follow medical recommendations, 39.2% did it sometimes or never, and 74.5% were not under constant medical care. The above shows that medical assistance for the homeless requires considering several different variables, including the entire social context. Our results suggest that the groups of men whom special measures should cover are those in the homelessness phase up to 4 years and people with a criminal record.
Study limitations
The small size of the group and the lack of evaluation in the group of women can be considered as limitations of the study.
Practical implications
Homeless people should be provided with free health care.
Homeless people should have access to specialist doctors.
It is advisable to monitor the health behaviors of the homeless to get to know them better.
Future research directions
The research should be carried out on a larger population in different country regions.
Research should also include homeless women.
Conclusion
1. The level of the health behaviors showed statistically significant diversification with all dimensions of the health locus of control and its internal dimension with age, phase of homelessness, criminal history of the respondents, being under constant medical care, and self-assessment of health.
2. Significant differences were found between people experiencing a homelessness crisis and the control group in selected aspects concerning the everyday life hygiene of the respondents, health self-assessment, declarations of visits to a specialist and carrying out check-ups, level of satisfaction with life, coping with difficult situations, preferred pro-health behaviors and dimensions of health control.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without under reservation.
Ethics statement
The studies involving humans were approved by the Bioethics Committee of the Medical University of Bialystok, R-I- 449/2013. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
BR, DC, MZ, AM, AS, and AŚ collected the epidemiological and clinical data. NW processed statistical data. BR, GB, and AK-B drafted the manuscript. BR, GB, and NW revised the final manuscript. WK and EK-K is responsible for summarizing all epidemiological and clinical data. All authors contributed to the article and approved the submitted version.
Funding
Work carried out as part of a research project − /ST/ZB/15/009/3310; 153–196 48P.
Acknowledgments
We would like to express our sincere thanks to all participants of the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer KK declared a shared affiliation with the authors GB, AK-B, NW, WK, and EK-K to the handling editor at the time of review.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fransham, M, and Dorling, D. Homelessness and public health. BMJ. (2018) 360:k214. doi: 10.1136/bmj.k214
2. Rajpari, A Czym jest bezdomność i dlaczego jest problemem? (2023). Available at: https://sites.uab.edu/humanrights/2020/03/09/what-is-homelessness-and-why-is-it-an-issue/ (Accessed March 30, 2023).
3. Brannon, A. Homelessness statistics reveal a problem that’s bigger than us, but not beyond solving. (2023). Available at: https://newstoryhomes.org/homelessness-statistics/ (Accessed March 30, 2023).
4. Gruszka, J. Badania nad bezdomnością w Polsce. Wytyczne ogolnopolskich badan nad bezdomnościa. Stud Humanist AGH. (2012) 11:75–87. doi: 10.7494/human.2012.11.4.75
5. Gruszka, J. Wykluczenie społeczne osób bezdomnych w Polsce In: Z Badań, A Kłonkowska, and M Szulc, editors. Społecznie wykluczeni. Niewygodni, nienormatywni, nieprzystosowani, nieadekwatni. Gdańsk: Uniwersytetu Gdańskiego (2013). 233–50.
6. OECD. HC3.1. Homeless Population. Available at: https://www.oecd.org/els/family/HC3-1-Homeless-population.pdf (Accessed March 30, 2023).
7. Pindral, A. Definicje i typologie bezdomności In: A Dębski, editor. Problem bezdomności w Polsce. Wybrane aspekty. Gdańsk: Wyd. w ramach Projektu systemowego 1.18 (2010). 31–52.
8. Basińska, MA. Oso by bezdomne In: JH Block and J Block, editors. Psychologiczne aspekty ich funkcjonowania. Bydgoszcz: Fundacja Salvus (2014)
9. Weber, JJ. A systematic review of nurse-led interventions with populations experiencing homelessness. Public Health Nurs. (2019) 36:96–106. doi: 10.1111/phn.12552
10. Iwundu, CN, Chen, TA, Edereka-Great, K, Businelle, MS, Kendzor, DE, and Reitzel, LR. Mental Illness and Youth-Onset Homelessness: A Retrospective Study among Adults Experiencing Homelessness. Int J Environ Res Public Health. (2020) 17:28295. doi: 10.3390/ijerph17228295
11. Neisler, J, Shree, S, Reitzel, LR, Chen, TA, Kendzor, DE, Obasi, EM, et al. Characterizing Alcohol Use Behaviors among Homeless Men and Women. Am J Health Behav. (2019) 43:37–49. doi: 10.5993/AJHB.43.1.4
13. Lynch, AD, Coley, RC, Sims, J, Lombardi, CM, and Mahalik, JR. Direct and interactive effects of parent, friend, and schoolmate drinking on alcohol use trajectories. Psychol Health. (2015) 30:1183–205. doi: 10.1080/08870446.2015.1040017
14. Elbert, S, Dijkstra, A, and Rozema, A. Effects of tailoring ingredients in auditory persuasive health messages on fruit and vegetable intake. Psychol Health. (2017) 32:781–97. doi: 10.1080/08870446.2017.1300259
15. Conner, M, and Norman, P. Health behaviour: Current issues and challenges. Psychol Health. (2017) 32:895–906. doi: 10.1080/08870446.2017.1336240
16. Glasser, I, and Rae, B. Surviving the Streets In: B Rae, editor. Braving the Street: The Anthropology of Homelessness. 1st ed. New York: Berghahn Books (1999). 58–89.
17. Juczyński, Z. Narzędzia pomiaru w promocji i psychologii zdrowia. Warszawa: Wyd. Pracownia Testów Psychologicznych (2011).
18. Baranowski, M. Raport na temat osób bezdomnych. (2023). Available at: http://www.depot.ceon.pl/itstream/handle/123456789/680/baranowski_raport_na_temat_osob_bezdomnych.pdf?sequence=1 (Accessed March 30, 2023).
20. Wyniki Ogólnopolskiego Badania Liczby osób Bezdomnych–Edycja. (2019). Available at: https://www.gov.pl/web/rodzina/wyniki-ogolnopolskiego-badania-liczby-osob-bezdomnych-edycja-2019 (Accessed March 30, 2023).
21. Obserwatorium Integracji Społecznej. Socjodemograficzny Portret Zbiorowości Ludzi Bezdomnych Województwa Podlaskiego, Regionalny Ośrodek Polityki Społecznej w Białymstoku. Białystok: Obserwatorium Integracji Społecznej. (2012). Available at: https://rops-bialystok.pl/downloads/Socjodemograficzny%20portret%20bezdomnosci%202012.pdf (Accessed March 30, 2023).
22. Chwaszcz, J. Osobowościowe i społeczne wyznaczniki funkcjonowania bezdomnych mężczyzn. Lublin: Towarzystwo Naukowe Katolickiego Uniwersytetu Lubelskiego Jana Pawła II (2008).
23. Bartczak, J., Bernacka, A., Janik, J., Kulczyńska, A, and Kwiatkowska, A. Postawy łodzian wobec bezdomnych, pp. 1–41. Available at: https://www.eksoc.uni.lodz.pl/is/lodzianie-o-bezdom.pdf (Accessed March 30, 2023).
24. Olech, O. Bezdomność–bezdachowość i bezmieszkaniowość, Agenda Bezdomności–Standard Aktywnego Powrotu na Rynek Pracy, e-przewodnik streetworkingu. Available at: http://www.ab.org.pl/e-przewodnik/fr_index.html (Accessed March 30, 2023).
26. Błażej, E, and Bartosz, B. O doświadczaniu bezdomności. Warszawa: Wydawnictwo Naukowe Scholar (1995).
27. Oliwa-Ciesielska, M. Piętno nieprzypisania. Studium o wyizolowaniu społecznym bezdomnych. Poznań: Wydawnictwo UAM (2005).
28. Heszen, I. Zmienność wymiarów zdrowia na przestrzeni życia człowieka In: D Kubacka-Jasiecka and TM Ostrowski, editors. Psychologiczny wymiar zdrowia, kryzysu i choroby. Kraków: Wydawnictwo Uniwersytetu Jagiellońskiego (2005). 21.
30. Tędzialgolska, M, Gola, W, Rżanek, K, and Wożniakowska, P. Problem bezdomności młodzieży i młodych dorosłych w Warszawie. Warszawa: Diagnoza sytuacji. Raport z badania. Stacja. (2015). Available at: https://programstacja.org.pl/wp/wp-content/uploads/2015/07.
31. Laporte, A, Vandentorren, S, Détrez, MA, Douay, C, Le Strat, Y, Le Méner, E, et al. Prevalence of Mental Disorders and Addictions among Homeless People in the Greater Paris Area, France. Int J Environ Res Public Health. (2018) 15:20241. doi: 10.3390/ijerph15020241
33. Hemberg, J, Nyqvist, F, and Näsman, M. "Homeless in life" - loneliness experienced as existential suffering by older adults living at home: a caring science perspective. Scand J Caring Sci. (2019) 33:446–56. doi: 10.1111/scs.12642
34. Bodys-Cupak, I, Róg, K, Majda, A, and Kózka, M. Samoocena stanu zdrowia a zasoby osobiste i zachowania zdrowotne bezdomnych. Pielegniarstwo Opiece Długoterminowej. (2020) 1:17–29. doi: 10.19251/pwod/2020.1(2)
35. Buciński, A, Romaszko, J, Kaliszan, R, et al. Czy bezdomność może być traktowana jako zdefiniowany czynnik ryzyka chorób układu krążenia? Zdrowie Publ. (2007) 117:324–9.
36. Raport CBOS. Badania pt: Sytuacja osób bezdomnych w Warszawie - opinie osób bezdomnych i pracowników socjalnych zostały zrealizowane na zlecenie Miasta Stołecznego Warszawy. (2005). Available at: https://www.bezdomnosc.edu.pl/images/PLIKI/Raporty/sytuacja%20osob%20bezdomnych%20w%20warszawie%20badanie%20cbos.pdf (Accessed March 30, 2023).
Keywords: homeless, health promoting behaviors, men, mental health, Poland health behaviors, health problems, Poland the homeless
Citation: Repka B, Bejda G, Kułak-Bejda A, Czarnecki D, Ziółkowski M, Mosiołek A, Szulc A, Waszkiewicz N, Ślifirczyk A, Kułak W and Krajewska-Kułak E (2023) Health behaviors and problems in Polish homeless men. Front. Public Health. 11:1208877. doi: 10.3389/fpubh.2023.1208877
Edited by:
M. Barton Laws, Brown University, United StatesReviewed by:
Matthew Anderson, Eastern Washington University, United StatesMahboubeh Dadfar, Iran University of Medical Sciences, Iran
Karol Konaszewski, University of Białystok, Poland
Cecilia Colunga-Rodriguez, University of Guadalajara, Mexico
Copyright © 2023 Repka, Bejda, Kułak-Bejda, Czarnecki, Ziółkowski, Mosiołek, Szulc, Waszkiewicz, Ślifirczyk, Kułak and Krajewska-Kułak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Agnieszka Kułak-Bejda, YWduaWVzemthLmt1bGFrLmJlamRhQGdtYWlsLmNvbQ==
†ORCID: Grzegorz Bejda, https://orcid.org/0000-0002-4829-0292
Agnieszka Kułak-Bejda, https://orcid.org/0000-0001-6334-9371
Damian Czarnecki, https://orcid.org/0000-0003-3474-5927
Marcin Ziółkowski, https://orcid.org/0000-0001-7707-7290
Anna Mosiołek, https://orcid.org/0000-0001-6999-2309
Agata Szulc, https://orcid.org/0000-0003-0059-9861
Napoleon Waszkiewicz, https://orcid.org/0000-0003-0059-9861
Anna Ślifirczyk, https://orcid.org/0000-0002-2495-025X
Elżbieta Krajewska-Kułak, https://orcid.org/0000-0002-9425-2430