 Inés González Casanova1*Delia Lilian Martínez Rodriguez2
Inés González Casanova1*Delia Lilian Martínez Rodriguez2 Julissa Ortiz Brunel3María Gudelia Rangel Gómez4Mary de Groot5
Julissa Ortiz Brunel3María Gudelia Rangel Gómez4Mary de Groot5 Alicia Fernández6
Alicia Fernández6- 1Department of Applied Health Science, School of Public Health, Indiana University Bloomington, Bloomington, IN, United States
- 2Oaxaca Ministry of Health, Oaxaca, Oaxaca, Mexico
- 3Department of Sciences of Human Movement, University Center for Health Sciences, Universidad de Guadalajara, Guadalajara, Guadalajara, Jalisco, Mexico
- 4Comision de Salud Fronteriza Mexico-Estados Unidos, Tijuana, Baja California, Mexico
- 5Division of Internal Medicine, Indiana University School of Medicine, Indianapolis, IN, United States
- 6San Francisco General Hospital, University of California, San Francisco, San Francisco, CA, United States
Introduction: Mental health promotion and screenings are recommended as part of standard preventive care. Mexican immigrants in the U.S. are at high risk for mental health illness especially after the COVID-19 pandemic, however access to mental health prevention for this population has been limited, which results in important implementation and equity gaps. The Ventanilla de Salud (VDS) program provides preventive services through Mexican consulates in the U.S.
Objective: The objective of this study was to assess capability, opportunity, and motivation for promotores to implement mental health programming through the VDS, leveraging early experiences of ongoing mental health prevention efforts.
Methods: This was a qualitative study using the Capability, Opportunity, and Motivation for Behavior Change model (COM-B). We conducted 9 focus groups with 40 VDS promotores and 6 semi-structured interviews with program stakeholders. Data were analyzed using inductive and deductive coding.
Results: We found high levels of interest from the leadership, partners, and promotores to provide mental health services through the VDS. Early implementation of a mental health strategy that included training sessions for promotores and mental health promotion, screenings and referrals for VDS users was ongoing. We identified facilitators and barriers that could affect capability, opportunity, and motivation to provide mental health services. Facilitators included promotores’ extensive knowledge about the importance of mental health, promotores service mindset and commitment to provide services to VDS users, and general support from the VDS network and partners. Barriers included promotores’ turnover, need for additional economic compensation, burnout, competing priorities, and lack of mental health professionals to provide clinical services or supervision. Additional investments are recommended to support promotores’ well-being.
Conclusion: The main lesson learned from this study was that investing in VDS promotores’ training, resources, and well-being is key to their capability, opportunity and motivation to provide mental health services for Mexican immigrants in the US. Results from this study can be applied to improve the ongoing VDS mental health strategy and increase its impact on the mental health of Mexican immigrants.
Introduction
Mental illness is the leading cause of disability worldwide (1). Mexican immigrants, the largest foreign-born group in the United States, are at higher risk of developing depressive and anxiety disorders compared to non-migrant Mexicans and to their US-born counterparts (2). It is estimated that almost 40% suffer from anxiety disorders and almost 15% have been diagnosed with depressive disorders, which is probably an underestimation due to the high prevalence of undiagnosed mental illness in this population (3). Hence, it is essential to implement evidence-based interventions to prevent mental disorders among Mexican immigrants.
The World Health Organization has identified mental health promotion and screening for mental disorders as essential for the prevention of mental illness (4). However, Mexican immigrants in the US face barriers in access to mental health preventive services and care (3). For instance, Mexican immigrants are less likely to receive health screenings for mental disorders or seek mental health treatment compared to other Hispanics in the US (5). National US data show Mexican immigrants have, on average, fewer years of education, lower income, and are less likely to have health insurance than US-born individuals, other Hispanics and immigrants from other countries (6–8). Language and structural barriers also complicate access to preventive care in this population (9). To address these many barriers, a promising approach is to incorporate mental health promotion and screening into existing health prevention initiatives that already reach this at-risk population (10, 11).
The Ventanilla de Salud (VDS), implemented through the network of Mexican consulates, is an initiative that already reaches a large number of Mexican immigrants throughout the US. The VDS plays a critical role in the preventive care of recent immigrants, providing health education, cardiometabolic risk screenings, and referrals to community resources or healthcare to millions of Mexican and other Latino immigrants that would otherwise not have ready access to these services (12). According to the latest evaluation of the program in 2020, the VDS provided screenings for cardiometabolic risk factors (hypertension, hyperglycemia, dyslipidemia, and overweight) to more than 500,000 Latino immigrants in 2019 (13). While the specific impact of the VDS screening program on health outcomes has not been evaluated, screening for cardiometabolic risk factors in combination with appropriate referrals is an evidence-based intervention has been shown to increase preventive behaviors, improve quality of life, and linkage to care (14). Taken together, this evidence supports an important contribution of the VDS to the cardiometabolic health of Latino immigrants in the US.
Since 2018, the VDS began implementing a strategy to integrate mental health promotion into their existing services through basic training for promotores. More recently, during the COVID pandemic, this effort was expanded to include screenings and referrals (3). We conducted this study to evaluate existing efforts to provide mental health prevention services through the VDS network and to identify barriers and opportunities for additional mental health programming (screening and services) through the VDS.
Methods
Study design
This was a qualitative study aimed at assessing the implementation of mental health strategies through the VDS program. It followed the capability, opportunity, and motivation to affect behavior (COM-B) model and the Theoretical Domains Framework (TDF) (See a more detailed description of COM-B and TDF below). A description of the study following the consolidated criteria for reporting qualitative studies (COREQ) (15) is presented next.
The VDS program
The VDS is a program funded by the government of Mexico and implemented in the US to facilitate access to primary and preventive health services to Mexican immigrants. There are currently 49 VDS and two mobile units operating in the Mexican consular network in the US (13). According to information from the Mexican Ministry of Health, between 2013 and 2018, the VDS program served over 9 million people, providing more than 25 million individual services (8). More recently, in the period from January 2019 to June 2021, 14 million services were provided to 5 million people (13).
The VDS program is implemented through a health promotores model, where each Ventanilla has a team of one to four promotores and a coordinator, as well as a local non-for-profit partner responsible for managing each site. This team works together at a VDS to provide high quality health information, health education, advice, and referrals in a safe environment, with the goal of improving the health and quality of life of Mexican immigrants (16). Promotores background and education varies but some of the qualifications for the job include college education preferably in a health related field, or training as community health worker, community outreach worker, or health promotor; experience working with Latino families; basic knowledge about the health care system and social services; experience conducting outreach in diverse settings; and experience providing community education. There is also a national coordination center based in San Diego that is responsible for establishing partnerships in the US and for overall program management and evaluation. The coordination center works closely with the Mexican Ministry of Health and the Mexican Institute for Mexicans in the Exterior, which are the two governmental organizations responsible for the program in Mexico.
Existing mental health services implemented through the VDS
A VDS mental health strategy is already underway where training sessions in the WHO mental health Gap Action Programme (mhGAP) intervention guide, which is an integrated package of mental health interventions, the development and implementation of a COVID-mental health screening questionnaire, and a telephone line to provide psychological services in Spanish to people who completed the screening questionnaire and were deemed at risk. In addition, VDS promotores developed a database to generate a network of local partners in mental health.
Training in the WHO mental health Gap Action Programme was conducted in collaboration with the Mexican section of the United States-Mexico Border Health Commission (CSFMEU) and the Pan American Health Organization (PAHO) and targeted VDS health personnel and community promotores. This was done to strengthen technical capacities in mental health through basic training for detecting and referring patients with mental health problems. Forty-two health promotores were initially trained in 2018, and some updates were made available as new promotores joined the VDS.
In 2020, as a response to the COVID-19 pandemic, the screening questionnaire and the psychological services phone line were implemented through a collaboration between the Mexican Ministry of Foreign Affairs, the Mexican Ministry of Health, the Mexican Section of the CSFMEU, the Migrant Clinicians Network (MCN), and the National Autonomous University of Mexico (UNAM) with the objective of providing remote mental health services in Spanish. At the time of this qualitative study, sixty-one Mexican immigrants had been given a questionnaire to determine if they had mental health needs. Among those, forty-two people consented to be contacted by professionals from the Faculty of Psychology of UNAM. The problems identified mainly were anxiety and depression, followed by substance abuse and stress (3).
Theoretical framework
This study was guided by the Capability, Opportunity, and Motivation behavioral change model (COM-B), that recognizes behavior as a part of an interacting system involving all these components (8, 17). The target behavior in this case was for promotores to conduct mental health screening, education, and/or referrals during VDS visits. We also used the Theoretical Domains Framework (TDF) (18) to operationalize the COM-B model. The TDF is an implementation framework developed by behavioral and implementation scientists. It operationalizes behavior into 14 theoretical constructs that can be mapped to capability, opportunity, and motivation (see Table 1). The use of COM-B and TDF has been recommended to collect information about barriers and opportunities that then can lead to the development and implementation of individual behavioral change interventions (17). In this study, we used the COM-B and TDF to develop the data collection instruments following the process recommended by Michie et al. Similarly, deductive codes were based on the TDF framework (Table 1).
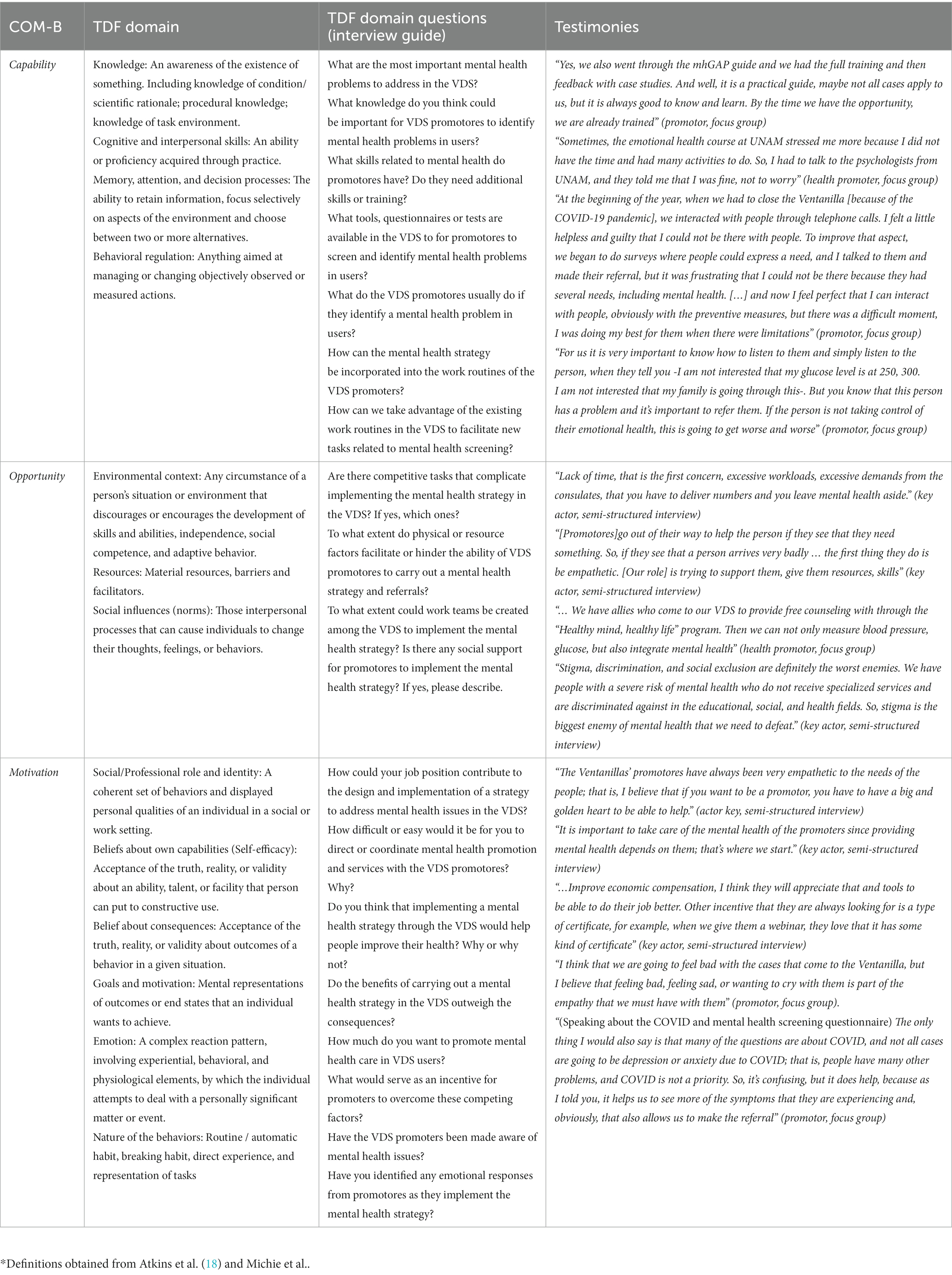
Table 1. TDF domain definitions*, questions, and testimonies from VDS promotores and key actors.
Data collection
The qualitative data collection was conducted between July and December of 2021 through interviews with key actors and focus groups with health promotores. The semi-structured interview and focus group guides were developed based on the COM-B model and the TDF framework (Table 1) and pilot-tested with former and current VDS employees (n = 3). All data collection activities were conducted in Spanish by native Spanish speakers.
The field psychologist (DLMR) conducted six semi-structured interviews with key actors from the VDS program including the national VDS coordinator, other program administrators, and collaborators from the National Autonomous University of Mexico (UNAM) who had been responsible for implementing mental health strategies through the VDS. Information obtained from key actor interviews was complemented with bibliographic research and available publications (often suggested by the stakeholders) to better understand the context and previous efforts to provide mental health services through the VDS program.
In addition, nine focus groups were conducted (led by DLMR, with IGC or JOB present for support and note-taking) with promotores who worked in VDS throughout the United States. Focus groups were divided by the following regions: East [2], West [2], Center [1] and Border [2]. Additionally, two groups with promotores from any region who could not attend the scheduled groups were conducted. The number of participants in each group varied between 3 and 6.
Study participants
We used intentional selection to choose the key actors who were interviewed (VDS strategy coordinators and administrators and UNAM collaborators). For the focus groups, an e-mail was sent to all VDS health promotores and site coordinators inviting them to participate in the study. Calendly was used to allow promotores to sign up to their preferred groups. Participants were compensated for their participation with a 25 US dollar gift card. The criteria used were being 18 or older, working as promotores or coordinators in a VDS, and giving their verbal consent to participate in the study.
Data analysis
We performed content analysis with inductive and deductive coding. Audio recordings of the interviews and focus groups were transcribed by JOB. The coding guide was developed by IGC based on TDF domains and refined through several discussions with DMLR, and JOB. We used inductive coding by looking at emerging patterns, and deductive coding guided by COM-B and the TDF framework. An initial subset of an interview and a focus group was coded for reliability purposes and the coding guide was refined until a kappa of 0.82 was reached. NVivo 14 qualitative data analysis software was used. Analyses were conducted in Spanish by native speakers and then the results and quotes were translated into English while writing this manuscript. Quote translations were reviewed for meaning by bilingual (Spanish and English) speakers.
Results
In total six VDS key actors participated in the semi-structured interviews and 40 promotores participated in the focus groups. Promotores were on average 46 years, had been working in the VDS for almost 5 years, and were primarily women (Table 2).
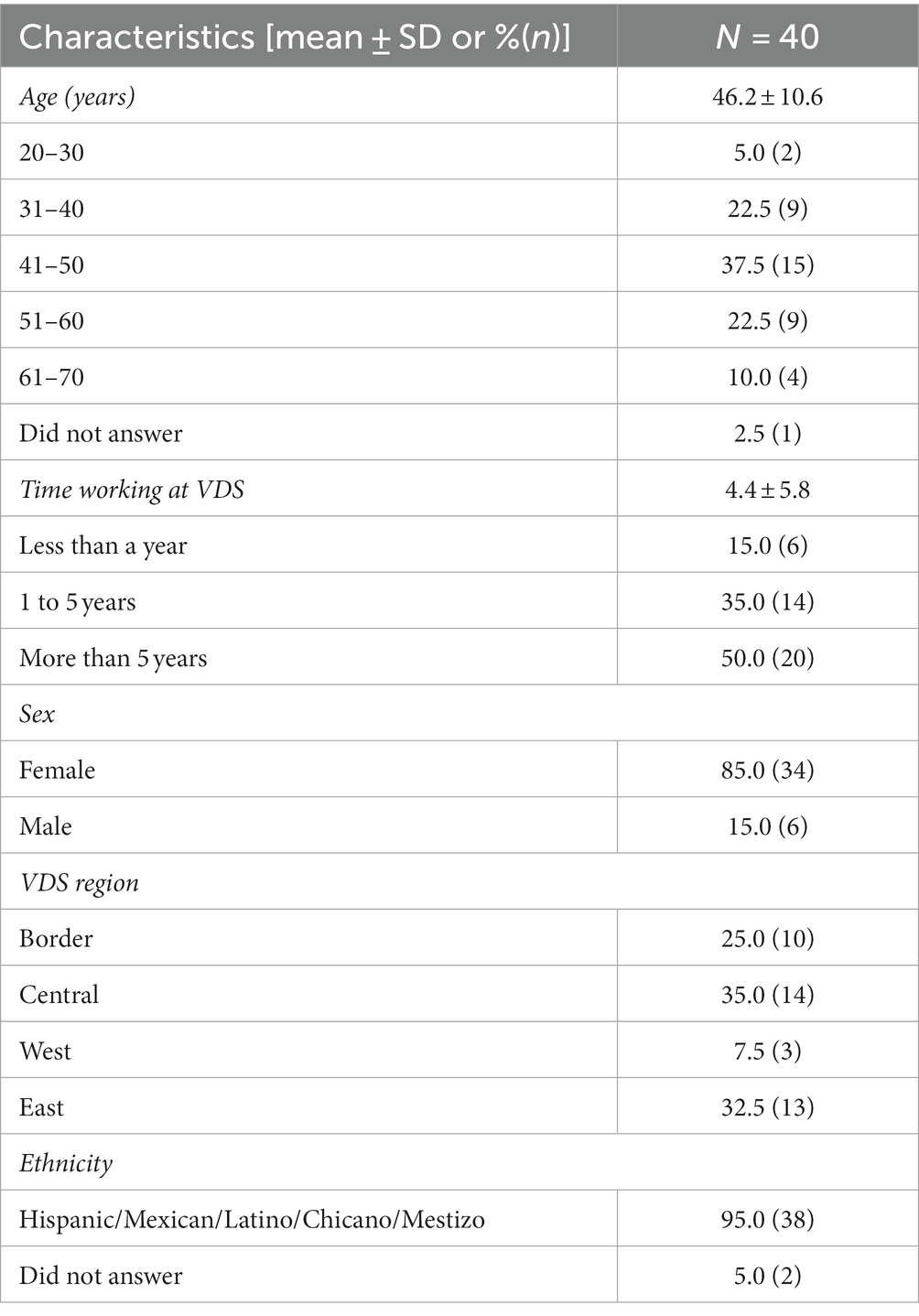
Table 2. Sociodemographic characteristics of Ventanilla de Salud promotores who participated in focus groups (n = 40).
Capability, opportunity and motivation to provide mental health services through the VDS
The main findings for the capability opportunity and motivation domains are summarized in Figure 1. The detailed explanation by TDF domains, sample interview questions, and quotes are included in Table 1.
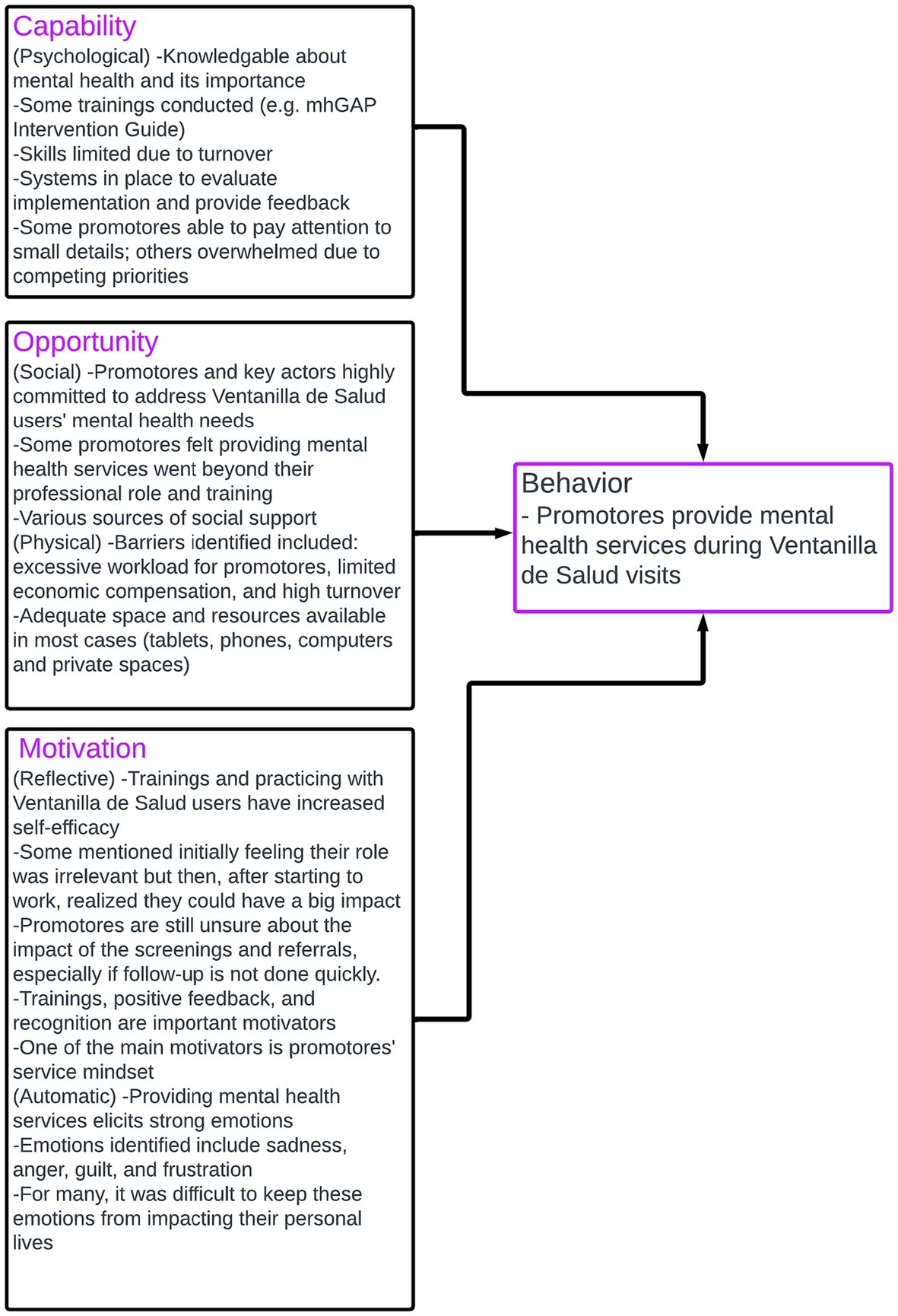
Figure 1. Summary of main results for capability, opportunity, and motivation of Ventanillas de Salud promotores to provide mental health services.
Psychological capability
For psychological capability, promotores expressed basic knowledge about mental health and its importance, especially for VDS users. The promotores repeatedly expressed their goal of providing mental healthcare to VDS users from a holistic perspective.
“To me, mental health is an integral part of our health. Many times, we focus on physical [health] and leave mental health behind because we see it as a taboo. Then, what we talk with the community is that mental health is part of our wholesome health.” (Promotor, focus group).
This was potentially due to the ongoing training opportunities provided by the VDS leadership team, as well as to their interactions with VDS users in need of these services.
“Yes, we also went through the mhGAP guide and had the whole training and then feedback with practical cases. And well, is a practical guide, maybe not all the cases are applicable for us, but it is always good to know and learn. For whenever we get an opportunity, we are already trained.” (Promotora, focus group).
However, despite these training sessions, there was a general perception that skills needed to conduct mental health screenings and referrals remained limited due to the high turnover in promotores.
Ongoing supervision and feedback were potential factors that can improve the implementation of mental health screenings and referrals through providing behavioral regulation.
In terms of attention and decision processes, many promotores mentioned that they were able to listen attentively to users and to pay attention to small details, however, some promotores said that they felt overwhelmed due to competing priorities, and sometimes were not able to provide these services.
Social opportunity
For social opportunity, promotores expressed mixed feelings related to the question if providing mental health services was part of their professional role. Some saw themselves as highly empathetic, with great commitment to and interest in providing these services that they see as a priority for VDS users. However, others felt that the training sessions went beyond their role of promotores because they included information about the diagnosis and treatment of mental health illnesses and most promotores do not have formal training or credentials in mental health.
“My concern when I heard what they were doing was exactly what (person 1) was talking about. I do not think it is adequate that the promoters of the Ventanillas, who do not have professional training in mental health, are the ones who lead this type of situation.” (promotora, focus group).
Similarly, the promotores identified several sources of social support for them including the network of external organizations and partners to the VDS, as well as the collaboration with the National Autonomous University of Mexico, their fellow promotores, and the national managers of the VDS program.
Stigma and discrimination associated with mental illness were identified as social norms that need to be addressed, and promotores already started to work on some initiatives. Similarly, gender roles were also identified as an important consideration, including the problem of machismo.
Physical opportunity
Regarding opportunity, the promotores expressed that resources are generally adequate to provide mental health services. However, they also identified various environmental stressors including excessive workload, lack of time, high turnover of promotores, increased workload without increased compensation, time consuming data entry requirements into a monitoring system, lack of support from mental health professionals, and the need to shift activities online during the COVID-19 pandemic.
“Lack of time, that is the first issue, excessive workloads, excessive demands, that you have to report numbers, and you leave mental health aside. … that could mean that they do not have time to do this” (key actor, semi-structured interview).
Reflective motivation
For reflective motivation, we found that most promotores felt increasingly capable of listening to mental health concerns, providing general information and referring VDS users as needed. They explained that this increase of self-efficacy has been built through the training sessions and the practice of these skills with users.
In general, promotores and stakeholders feel that the actions they take providing mental health services through the VDS will positively impact the well-being of the VDS users. However, a challenge they have found witnessing the impact of their actions is that often VDS users do not return to the VDS for years and promotores never know if they are adequately linked to mental health services. Even when promotores referred users to VDS programs, such as the phone line staffed with psychologists from the National University of Mexico, they never know if the users received the call backs as planned or if the connection was lost. Some promotores expressed concern that maybe the psychologists are not being able to connect with the users, and they never received the mental health care they needed. This concern sometimes affected their motivation to conduct the screenings.
Both stakeholders and promotores identified the latter’s attitude towards service as the most important motivation for incorporating mental health services. However, stakeholders also highlighted the importance of improving economic incentives, giving recognition to the promotores’ work and providing constant feedback as motivators for promotores to continue providing the services.
“We need to provide economic motivation[to the promotores], I think they will appreciate that and tools to be able to do their job better, they are always looking for that and that these tools have a type of certificate, for example, when we give them a webinar, they love that it has some kind of certificate that they took an hour to practice this and this” (key actor, semi-structured interview).
Automatic motivation
Regarding automatic motivation, a theme that was constantly highlighted by promotores was the strong emotional response that they experience when providing mental health services. They identified sadness, anger, guilt, and frustration as the main emotions felt when providing mental health services through the VDS. They mentioned feeling afraid of the magnitude of the responsibility that helping users with their mental health problems represents. In some instances, the stress related to providing these services started during the training. Others described how the COVID-19 pandemic also generated a mental health emergency in the VDS users, and promotores were left to address it with limited tools. In some cases, this led to compassion fatigue in the promotores, where they started to take on the users’ emotions. To address this, VDS leadership and mental health partners implemented some self-care workshops that the promotores described as very helpful. In terms of habits done automatically and routinely, promotores identified that there was a setback during the COVID-19 pandemic because all the normal procedures had to be adapted to fit the new reality. They were able to adjust some of the procedures to continue to provide mental health information, screenings, and referrals to some users.
“I think that we are going to feel bad with the cases that come to the Ventanilla, but I believe that feeling bad, feeling sad, or wanting to cry with them is part of the empathy that we must have with them” (health promoter, focus group).
Emerging codes
The following sections describe codes that were identified inductively during the data analysis phase.
Mental health activities independently designed and implemented by promotores
Besides the strategies designed by the VDS in partnership with the Mexican National Autonomous University (UNAM) psychology team, promotores designed, adapted and implemented diverse approaches to provide mental health services, in response to the specific needs of the VDS users in their consulates. Some of these approaches included: providing mental health education through videos, WhatsApp messenger, Facebook lives, virtual and face to face talks; following up with users through text messaging or phone calls to see if they had received the care that they needed; agreements with local organizations or with volunteer mental health professionals; virtual Zumba dance, yoga or other fitness classes; and having a box with different stress balls, plush toys and other trinkets to release anxiety or stress. Some VDS relied on psychology students doing their internships to provide mental health preventive services.
“It would take all the publicity in the world. Right now, we have a poster that says mental health support; come to your Ventanilla. This, I think, could be educational videos. I think that what works the most are social networks so that videos can be handy, and posts on social networks, on Facebook Live, on the Facebook of the Mexican consulate, of the Ventanilla de Salud.” (promotor, focus group).
Self-care strategies employed by health promotores
Self-care was a recurring topic that was mentioned by both key actors and promotores as essential to sustaining the mental health strategy and supporting promotores. Key actors introduced the context of self-care through formal training and virtual sessions during the COVID-19 pandemic. The promotores quickly adopted these strategies and used them to deal with the emotional load of providing mental health services to the VDS users. Self-care strategies mentioned by the promotores included using oils, aromatherapy, lime and chamomile tea, Himalayan salts, music, yoga classes, mindfulness, psychotherapy, relaxation exercises, and activities such as going out for coffee and walking around. They mentioned the need to create an emotional support group for them.
“I went to therapy after so many deaths with COVID, dead and dead and dead, and obviously, you were referring people with families to support groups or psychologists back then, but it was too much. So, I said ‘I needed to look for a professional’, and I was in therapy to take away the emotional pressure of having to provide solutions all the time, all the time, 24 h, because people were left alone, women without families, cases of children where all the older relatives died. So, there were extreme cases. And yes, I did raise my hand and looked for a therapist because I said, ‘it’s too much, I cannot’. And yes, it works! It really is something good and recommendable” (promotora, focus group).
Specific characteristics of the training sessions that could help support promotores
Key actors and promotores provided suggestions and requests to improve the ongoing mental health training sessions. Topics suggested by key actors included communication skills, active listening, interviewing techniques, developing new partnerships, and identifying mental health risks of users, as well as training sessions that included clinical practice opportunities.
“I was just telling you about these skills that are priorities that have to do with awareness, and later essential skills, communication and listening, establishing this environment of trust, so that the person feels heard, and shares with us what is happening” (key actor, semi-structured interview).
Promotores suggested crisis response, suicide prevention, schizophrenia, child rearing styles, and gender violence.
“Maybe schizophrenia or suicide. These two, because we almost always focus on what is very common: anxiety, depression, bipolar disorder. I have been at the Ventanilla de Salud for 8 years, and I have taken all the courses that UNAM has offered. So it’s been excellent. I mean, I congratulate them; they have been terrific, but it seems to me that suicide and schizophrenia have been left a little to the side. Personally, I have not had many of these cases, but yes, it’s not like none have ever appeared, and I would like to be a little more prepared to deal with them in case I need to help someone” (health promoter, group focal).
They requested additional training in self-care and additional support tools for themselves as providers. They mentioned that activities such as group and individual self-care guided sessions provided by psychologists, counselors, or other mental health professionals for promotores would be very beneficial for their mental health. The most frequently suggested training session frequency for these activities was every 15 days, although others mentioned that, because their time is limited, once a month or every 2 months would be better. Also, they highlighted that sessions should be preferably online during VDS working hours (because many promotores have other jobs) or as lunch and learns. However, some promotores expressed concerns that the high flow of people in their VDS would not allow them to attend the sessions.
Discussion
In this study, we explored capability, opportunity, and motivation for promotores to provide mental health services during the ongoing health promotion and prevention programming that they routinely conduct through the network of Mexican Consulates in the US. We found that the leadership of the VDS had already implemented some mental health programming, had established partnerships in Mexico with the psychology school of UNAM, and provided training and support for promotores. Through the interviews with key actors and the focus groups with promotores, we identified strengths of the ongoing program and opportunities to improve it and to fully integrate mental health promotion and prevention into the current services provided through the VDS.
The main strengths found in terms of capability were that promotores have at least basic knowledge of the importance of mental health as part of overall health and well-being, and that there are systems in place to monitor the implementation of the mental health strategy and provide feedback. Conversely, there is high staff turnover, which has resulted in many promotores without all the skills that have been taught through the training sessions. Also, some promotores feel overwhelmed with all the tasks required of them and are not able to pay attention to detail when providing mental health services. Interventions that can help improve capability in this context include additional training, role modeling from more experienced promotores, and adding prompts or cues to remind the promotores to conduct the mental health questionnaires (19).
Social opportunity was identified as an important area to strengthen the implementation of the intervention. Promotores identified different sources of social support including other promotores, the VDS leadership, and psychologist form UNAM; however, they also expressed the importance of channeling that support through official and structured channels. They requested periodic support groups where they can talk to each other, express their feelings, and exchange ideas and approaches. This is in line with recommendations from a recent review of health provider mental health during the COVID-19 pandemic that found that healthcare workers relied on social support and contact to address mental health problems (20).
Another important aspect of social opportunity was the big sense of commitment among promotores to provide mental health services. They have witnessed firsthand the difficulties faced by VDS users and have a service mindset that compels them to provide these mental health services. However, some participants questioned if the proposed activities go beyond the professional role and training of the promotores who are not licensed mental health professionals. Recommendations to address this issue include increasing the partnerships with trained mental health professionals who can provide treatment, and delineating very clearly what is expected from the promotores during the VDS work, which is primarily health promotion, screenings, and referrals.
Under certain circumstances, being able to provide support has been deemed positive for providers’ mental health and well-being (21, 22). Inagaki and Orehek identified two conditions that need to be met for providing support to be beneficial for the provider: that support is given by choice and that the individual giving support believes the support is effective (23). In the case of VDS promotores, the first condition is met. However, a challenge identified for reflective motivation was that, even though providers feel that their work can have a big impact, they often do not know what happens to the VDS users they refer: whether they are ever contacted by the psychologists and receive the attention they need. This not only could decrease the benefits that they get as providers of support, but also dampens their motivation to conduct screenings and referrals.
Perhaps the most important challenge identified for automatic motivation was the emotional burden that promotores experienced while providing mental health services, especially during the COVID-19 pandemic when the mental health vulnerable Latino groups was particularly impacted (24). Promotores described experiencing strong emotions while providing mental health services to VDS users, including anxiety, sadness, and frustration, and that sometimes, these emotions and concerns persisted at home and affected their personal lives. Self-care training was implemented by the VDS leadership and the UNAM psychology team as a response to this situation. Self-care was described as extremely helpful by promotores, which is consistent with other studies that have improved emotional burnout of community health workers with self-care interventions (25, 26).
High turnover was identified as an important challenge for capability, opportunity, and motivation to implement the mental health services in the VDS. This challenge is potentially related to the emotional burnout associated with proving services to a highly minoritized population, (27, 28) as well as to the limited economic compensation and high demands the VDS promotores face. Recommendations are to continue supporting and addressing the mental health needs of the promotores, to find additional economic resources and improve economic compensation as much as possible, and to innovate to try to reduce competing tasks and demands. In this sense, most recommendations identified through this study relate to the importance of investing in the well-being of VDS promotores. The VDS is a unique program reaching and addressing the preventive needs of thousands of Mexican immigrants in the US and, within this program, promotores are a unique workforce that is essential to achieving the goals of the program.
Limitations of this study include that some key actors and promotores were not able to participate in the study due to the demanding nature of their jobs, and that all data collection was conducted online which can affect the way people interact, especially in focus groups. However, we were able to collect qualitative data from a diverse group of key actors and promotores describing different aspects of the VDS mental health strategy. The use of the COM-B model to explore barriers and opportunities is also a strength of this study, which will allow us to translate the results into actionable solutions that improve the implementation of the VDS mental health strategy and improve mental health prevention for Mexican immigrants.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Indiana University Bloomington Institutional Review Board (2009002576). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Research was considered exempt as part of a program evaluation. Verbal assent was provided by participants.
Author contributions
IG: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Project administration, Supervision, Writing – original draft. DM: Data curation, Formal analysis, Investigation, Writing – original draft. JO: Data curation, Formal analysis, Investigation, Writing – original draft. MR: Conceptualization, Resources, Supervision, Writing – review & editing. MG: Investigation, Supervision, Writing – review & editing. AF: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the National Heart, Lung and Blood Institute (NHLBI) as part of Programs to Increase Diversity Among Individuals Engaged in Health-Related Research (PRIDE). Research in Implementation Science for Equity small research project (5R25HL126146). IG was supported by NHLBI supplement to support diversity 3R01HL137338-03S1.
Acknowledgments
The authors would like to thank all promotores and key actors that contributed their time and opinions, and who work tirelessly to improve the health of Mexicans in the United States. The authors are especially grateful to Leslie Martinez who was the national VDS coordinator at the time of the study, and was instrumental in the implementation of this research project.
Conflict of interest
At the time of the study MR worked at the Border Health Commission and was responsible for overseeing the Ventanilla de Salud program.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Global Burden of Disease Study 2013 Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. (2015) 22:743–800. doi: 10.1016/S0140-6736(15)60692-4
2. Breslau, J , Borges, G , Tancredi, D , Saito, N , Kravitz, R , Hinton, L, et al. Migration from Mexico to the United States and subsequent risk for depressive and anxiety disorders: a cross-national study. Arch Gen Psychiatry. (2011) 68:428–33. doi: 10.1001/archgenpsychiatry.2011.21
3. Ministry of Health, Ministry of Foreign Affairs, Institute for Mexicans Abroad, & Mexican Section of the United States-Mexico Border Health Commission . Executive report. VDS Strategy. Results of strategic projects 2020-June 2021. (2021). Available at: https://ventanillasdesaludums.org/wp-content/uploads/2021/12/Informe-ejecutivo-VDS-2020-jun2021.pdf
4. World Health Organization . World mental health report: transforming mental health for all [internet] World health Organization (2022) (Accessed July 1, 2023). Available at: https://www.who.int/publications/i/item/9789240049338
5. Alegría, M , Álvarez, K , and DiMarzio, K . Immigration and mental health. Curr Epidemiol Rep. (2017) 4:145–55. doi: 10.1007/s40471-017-0111-2
6. Kuehn, B . Better risk assessment tools needed for Hispanic or Latino patients. Circulation. (2019) 139:2186–7. doi: 10.1161/CIRCULATIONAHA.119.040938
7. Zhen-Duan, J , Jacquez, F , and Vaughn, L . Demographic characteristics associated with barriers to health care among Mexican and Guatemalan immigrants in a nontraditional destination area. Fam Community Health. (2017) 40:101–11. doi: 10.1097/FCH.0000000000000141
8. Rangel Gomez, M , López Jaramillo, A , Svarch, A , Tonda, J , Lara, J , Anderson, E, et al. Together for health: an initiative to access health Services for the Hispanic/Mexican population living in the United States. Front Public Health. (2019) 7:273. doi: 10.3389/fpubh.2019.00273
9. Koniak-Griffin, D , and Brecht, M-L . Awareness of cardiovascular disease and preventive behaviors among overweight immigrant Latinas. J Cardiovasc Nurs. (2015) 30:447–55. doi: 10.1097/JCN.0000000000000181
10. Mensah, G , and Collins, P . Understanding mental health for the prevention and control of cardiovascular diseases. Glob Heart. (2015) 10:221–4. doi: 10.1016/j.gheart.2015.08.003
11. Lichtman, J , Bigger, TJ , Blumenthal, J , Frasure-Smith, N , Kaufmann, P , Lespérance, F, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association prevention Committee of the Council on cardiovascular nursing, council on clinical cardiology, council on epidemiology and prevention, and interdisciplinary council on quality of care and outcomes research: endorsed by the American Psychiatric Association. Circulation. (2008) 118:1768–75. doi: 10.1161/CIRCULATIONAHA.108.190769
12. Rangel Gomez, M , Tonda, J , Zapata, G , Flynn, M , Gany, F , Lara, J, et al. Ventanillas de Salud: a collaborative and binational health access and preventive care program. Front Public Health. (2017) 5:151. doi: 10.3389/fpubh.2017.00151
13. Rangel Gómez, MG , Salazar, S , López Jaramillo, AM , Lira Chávez, IA , Romero Rangel, A , Caballero Abraham, ML, et al. Ventanillas de Salud (VDS) and Mobile health units (MHU): a binational collaborative models. Front Public Health. (2022) 10:976941. doi: 10.3389/fpubh.2022.976941
14. Søgaard, R , Diederichsen, A , and Lindholt, J . The impact of population screening for cardiovascular disease on quality of life. Eur Heart J Open. (2023) 3:oead055. doi: 10.1093/ehjopen/oead055
15. Tong, A , Sainsbury, P , and Craig, J . Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual health care. Int J Qual Health Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
16. Government of Mexico . Ventanilla de Salud [internet]. Instituto de los Mexicanos en el Exterior. (2016) Available at: https://www.gob.mx/ime/acciones-y-programas/ventanilla-de-salud (Accessed July 1, 2023).
17. Michie, S , Atkins, L , and West, R . The behaviour change wheel: A guide to designing interventions. vol. 1003. 1st ed. Great Britain: Silverback Publishing (2014). 1010 p.
18. Atkins, L , Francis, J , Islam, R , O’Connor, D , Patey, A , Ivers, N, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. (2017) 12:77. doi: 10.1186/s13012-017-0605-9
19. Michie, S , van Stralen, M , and West, R . The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. (2011) 6:42. doi: 10.1186/1748-5908-6-42
20. Muller, A , Hafstad, E , William Himmels, J , Smedslund, G , Flottorp, S , Stensland, S, et al. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: a rapid systematic review. Psychiatry Res. (2020) 293:113441. doi: 10.1016/j.psychres.2020.113441
21. Kim, H , Sherman, D , and Taylor, S . Culture and social support. Am Psychol. (2008) 63:518–26. doi: 10.1037/0003-066X
22. Brown, S , Nesse, R , Vinokur, A , and Smith, D . Providing social support may be more beneficial than receiving it: results from a prospective study of mortality. Psychol Sci. (2003) 14:320–7. doi: 10.1111/1467-9280.14461
23. Inagaki, T , and Orehek, E . On the benefits of giving social support: when, why, and how support providers gain by caring for others. Curr Dir Psychol Sci. (2017) 26:109–13. doi: 10.1177/0963721416686212
24. Gomez-Aguinaga, B , Dominguez, M , and Manzano, S . Immigration and gender as social determinants of mental health during the COVID-19 outbreak: the case of US Latina/os. Int J Environ Res Public Health. (2021) 18:6065. doi: 10.3390/ijerph18116065
25. Sultana, A , Sharma, R , Hossain, M , Bhattacharya, S , and Purohit, N . Burnout among healthcare providers during COVID-19: challenges and evidence-based interventions. Indian J Med Ethics. (2020) V:1–6. doi: 10.20529/IJME.2020.73
26. Kravits, K , McAllister-Black, R , Grant, M , and Kirk, C . Self-care strategies for nurses: a psycho-educational intervention for stress reduction and the prevention of burnout. Appl Nurs Res. (2010) 23:130–8. doi: 10.1016/j.apnr.2008.08.002
27. Willard-Grace, R , Knox, M , Huang, B , Hammer, H , Kivlahan, C , and Grumbach, K . Burnout and health care workforce turnover. Ann Fam Med. (2019) 17:36–41. doi: 10.1370/afm.2338
Keywords: mental health promotion, mexican immigrants, Latino mental health, depression screening, implementation science, health disparties, COM-B, Theoretical Domains Framework
Citation: González Casanova I, Martínez Rodriguez DL, Ortiz Brunel J, Rangel Gómez MG, de Groot M and Fernández A (2023) Barriers and facilitators to mental health promotion for Mexican immigrants in the U.S. through the Ventanillas de Salud program. Front. Public Health. 11:1268253. doi: 10.3389/fpubh.2023.1268253
Edited by:
Mechelle Sanders, University of Rochester, United StatesReviewed by:
Francisco Cartujano-Barrera, University of Rochester Medical Center, United StatesFelicia Mata-Greve, University of Washington, United States
Copyright © 2023 González Casanova, Martínez Rodriguez, Ortiz Brunel, Rangel Gómez, de Groot, and Fernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Inés González Casanova, aW5lZ29uemFAaXUuZWR1