 Fidelia Cascini1,2
Fidelia Cascini1,2 Andrea Gentili1*Andriy Melnyk1
Andrea Gentili1*Andriy Melnyk1 Flavia Beccia1
Flavia Beccia1 Francesco Andrea Causio1Vincenzo Solimene1Serena Battilomo2Simona Paone3Alice Borghini3Michelangelo Bartolo4Emilio Chiarolla2
Francesco Andrea Causio1Vincenzo Solimene1Serena Battilomo2Simona Paone3Alice Borghini3Michelangelo Bartolo4Emilio Chiarolla2 Walter Ricciardi1
Walter Ricciardi1- 1Section of Hygiene, Department of Life Sciences and Public Health, Università Cattolica del Sacro Cuore, Rome, Italy
- 2General Directorate of Health Information System and Statistics, Ministero della Salute, Rome, Italy
- 3Italian National Agency for Regional Healthcare Services (Agenas), Rome, Italy
- 4Telemedicine Department, San Giovanni Addolorata Hospital, Rome, Italy
Introduction
Telemedicine is the remote delivery of healthcare services using information and communication technologies for the exchange clinical data for diagnosis, treatment and prevention of diseases (1). Telemedicine has historically been used to provide healthcare to rural or underserved areas. Still, in recent years it has grown in popularity as a way to improve access to healthcare, increase care quality level and, in some cases cost reduction was proved (2). However, the regulatory landscape for telemedicine varies across countries and regions, with some having more developed and supportive frameworks than others (3). The use of telemedicine in the National Health Service (NHS) in Italy peaked during the COVID-19 pandemic, which resulted in the development of the Italian National Recovery and Resilience Plan (“Piano Nazionale di Ripresa e Resilienza”, PNRR) (4). The PNRR is part of the Next Generation EU (NGEU) programme, namely the €750 billion package that the European Union negotiated in response to the pandemic crisis with the goal of strengthening local prevention and health services, modernizing and digitalizing the health system and ensuring equal access to care.
Those objectives will be achieved through:
• the creation of Community Health Houses (“Case delle Comunità”) and Community Hospitals (“Ospedali di comunità”) for proximity healthcare;
• new Territorial Coordination Centers (“Centrale Operativa Territoriale”, COT) for remote healthcare; and
• technological and digital upgrading including diagnostic imaging machinery.
The new healthcare delivery model is based on patient access and continuity of care in a multi-stakeholder process. The patient's home is the first and main place of health delivery, and COT will act as a trait-d'union between healthcare services and professionals, playing the role of transitional care following patient through different settings of care. The implementation of telemedicine is pivotal: within Mission 6 of the PNRR (“Health”), the component “Territorial assistance and telemedicine” has the goal of reaching out to at least 10% of the older adult population (over 65 years of age) to tackle the issue of patients with chronic conditions lost to follow-up and who only access the healthcare system when developing acute complications. In order to do so, it is planned to assist through telemedicine at least 200 000 people by the end of 2025. The main objective of the National Portal for Telemedicine is to establish a fundamental level of interoperability that ensures common standards for telemedicine services developed by the regions, enhancing what is already available in the landscape of local contexts while complementing or completing the portfolio of services. In particular, it aims to connect all healthcare providers and patients in Italy, and the dissemination of electronic prescriptions and Electronic Health Records (EHRs) (5).
This paper aims to describe the technical, structural, and operational characteristics of the new Italian Integrated Home Care (IHC) digital model, as described in the most recently operational manual published by the Ministry of Health. These features will be discussed and analyzed in order to identify strengths, weaknesses, and future implications, as well as to assess how the proposed model fits into the European context, and possibly comparing it to other highly advanced international ones.
Description of technical, structural features
The National Digital Health Agency (“Agenzia Nazionale per la Sanità Digitale”) is charged with ensuring the provision of telemedicine services through the cloud-based Network Time Protocol. The Network Time Protocol is a national infrastructure which contains the “Enabling Services” (data gathering, management of telemedicine solutions, policy role management and workflow solutions) and all the connected regional infrastructures which provide “Basic Telemedicine Services” (healthcare professionals' teleconsultation, telemonitoring, teleassistance, patient's teleconsultation known as “televisita”) (6). Communication between different services, infrastructures and local health authorities (Aziende Sanitarie Locali—ASL) is guaranteed by a modular interoperability layer in which various pathways ensure data standards and quality, smoothing data governance. Finally, a national telemedicine dissemination portal (“Portale Nazionale per la Diffusione della Telemedicina”), controlled directly by the Ministry of Health will contain data on all telemedicine solutions provided (Figure 1).
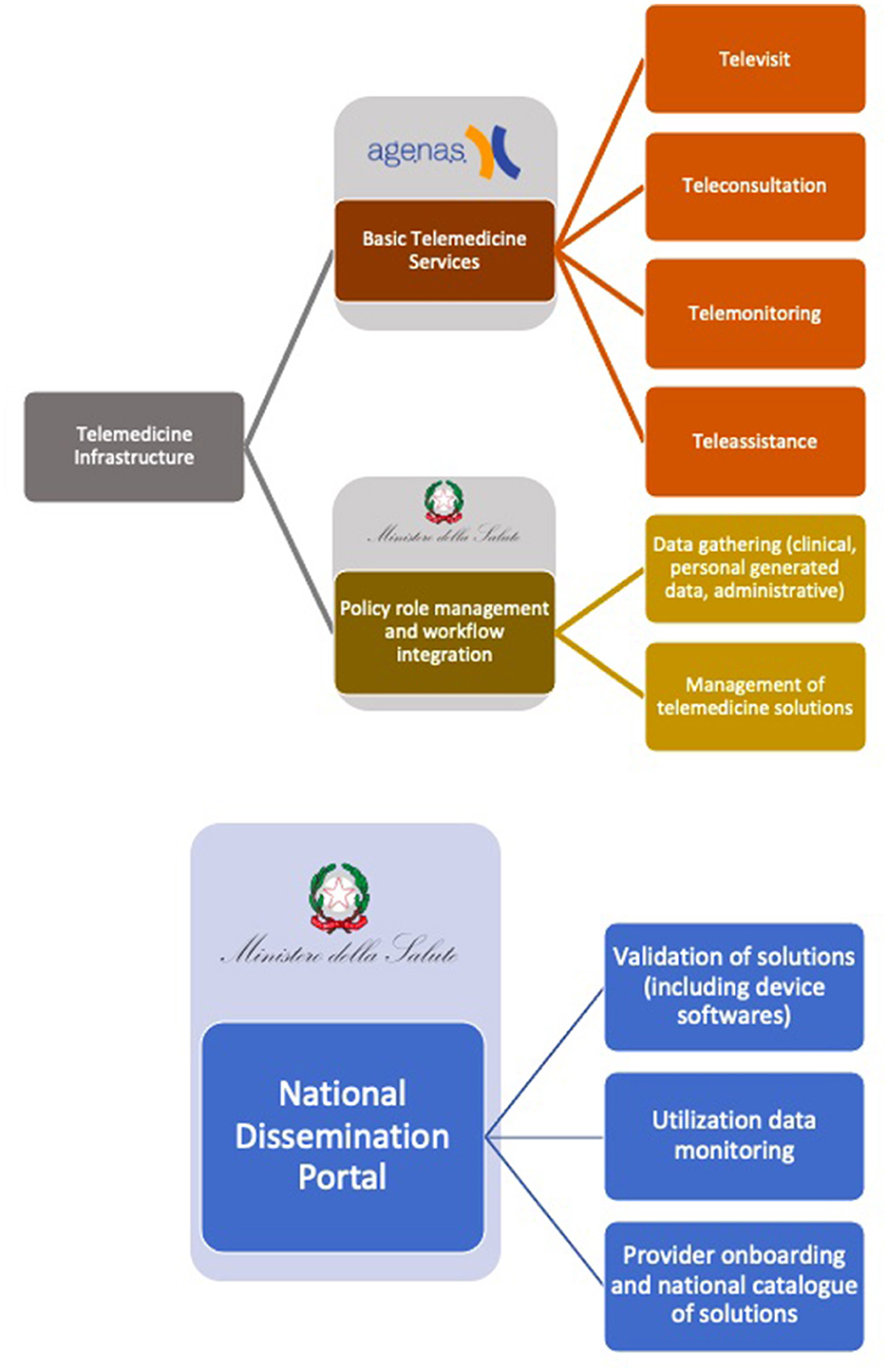
Figure 1. Description of the main services provided by each infrastructure in the national telemedicine model and the entities responsible for their development.
Operational and organizational aspects of the new digital home care guidance
In Table 1, four main use cases (patients' teleconsultation, healthcare professional teleconsultation, telemonitoring, teleassistance) will be examined and structured following the newly published ministerial guidance for the implementation of digital home care (7, 8). In each use case, it will go through the prescriber, the activation and provision service, and the technical support and shared information.
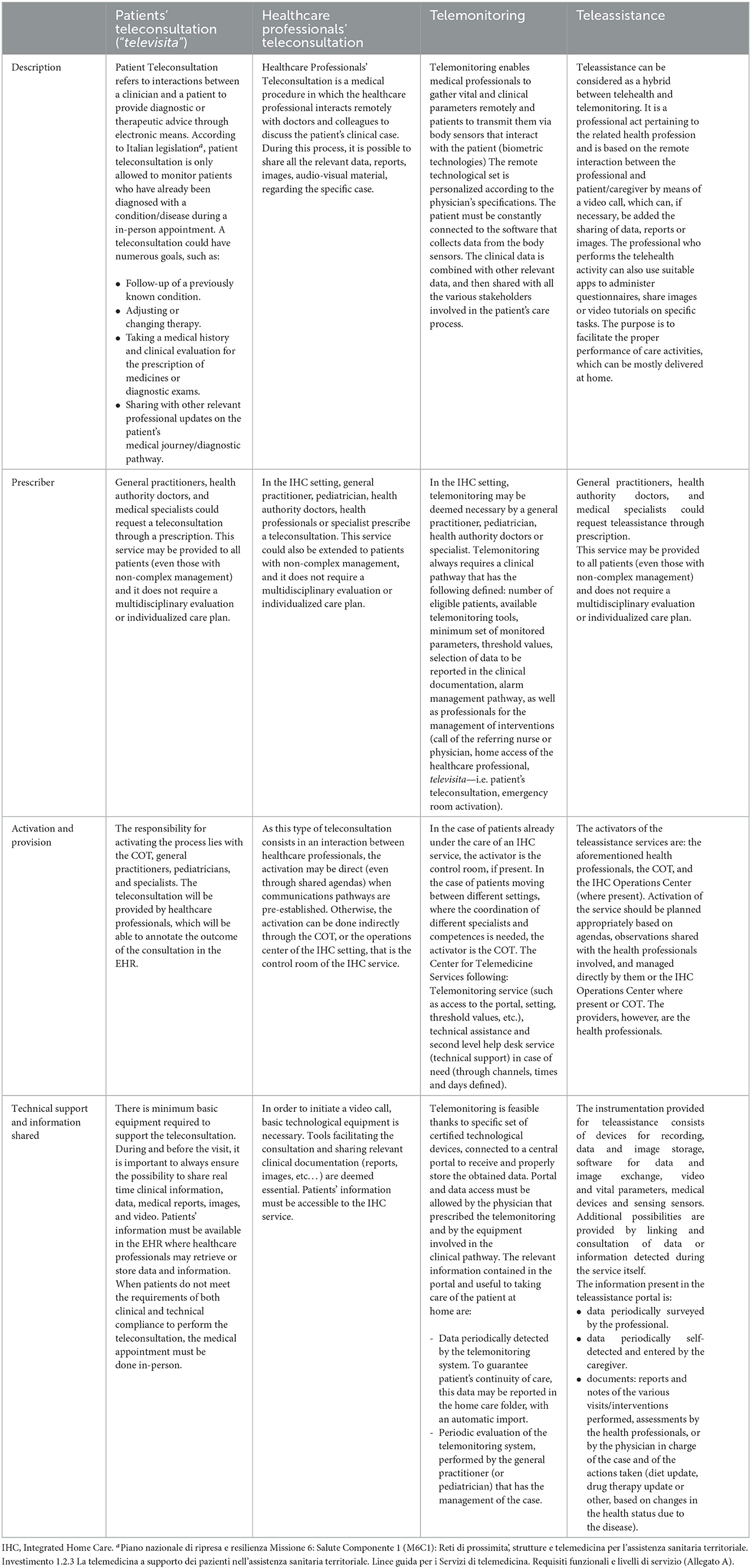
Table 1. Organizational aspects of the 4 main use cases (patients' teleconsultation, healthcare professional teleconsultation, telemonitoring, teleassistance).
Discussion
Strengths
Similar to many other European countries, Italy is expected a strong decline in population (especially in the rural areas) within the next 10 years (9). One of the most immediate and pronounced effects of a declining population is an aging demographic. As the proportion of older adult individuals increases, there will be a strain on healthcare systems and pensions. As rural areas depopulate, they may face challenges related to maintaining infrastructure, schools, and healthcare services.
Several countries have implemented telemedicine as an effort to improve healthcare for residents of rural or underserved areas, where healthcare facilities and specialists may be hard to reach (10, 11). The new IHC model has the potential to change the way healthcare is delivered in Italy drastically. Telemedicine can assist in providing care at the patient's home, increase access to healthcare services, and improve patients' health through continuous and dedicated care delivery.
The implementation of this IHC new digital model, in fact, is aimed at strengthening the territorial primary care, in line with the principle of proximity of care: it can reduce waiting times and prevent patient health conditions from worsening by guaranteeing prompt access to the healthcare system, in the form of patient's teleconsultation (televisita), healthcare professionals' teleconsultation, or similar (12). Given the increase in chronic morbidity prevalence, addressing these conditions timely can have a positive impact on hospital admissions (13) by reducing their number and leading to cost optimization and resource savings. This task can be accomplished by the prompt activation of the COT, that can drastically reduce the “near-misses” and the need for excessive follow-up care.
The intent of this new model is to transform the telemedicine as a routine practice. As nearly every doctor could request a teleconsultation from every patient, the opportunity to have a not-in-person visit has been seen to positively impact queuing and waitlists. As seen in other developed countries, such as Australia or the USA, telemedicine adoption leads to shorter waiting lists for specialized outpatient services (14) and the number of waitlisted patients in general (15, 16). Additionally, patients have claimed time savings from less commuting and waiting in queues (17).
Cost-effectiveness of telemedicine should also be considered: available literature on the economics of telemedicine implementation is scarce, but it notes that despite initial set-up expenses could be a significant obstacle to the implementation of telemedicine, they will likely be compensated in the long run (18). Some studies, however, noted that telehealth brings down healthcare system costs in the short- to medium-term, particularly when either patient or clinician traveling was minimized or avoided. Moreover, telemedicine demonstrated enhanced care even when costs were not decreased. For instance, research shows that remote patient monitoring is currently ineffective at cutting costs, but it is good at enhancing general health and lowering morbidity and hospitalization (18). This is in line with the goal of reaching remote areas of the territory, potentially supplying the shortages (both of funds and staff) that primary care has in these areas. Also, these points can help convince the stakeholders to invest and take care of primary care, since very poor efforts have been made toward the latter in recent years (19). In this context, the PNRR has allocated 4 billion euros to strengthen IHC and telemedicine implementation in Italy (20), and it has been estimated there will be a total of 1.2 billion euros in savings due to the new plan's implementation (21).
Barriers
Some drawbacks should be pointed out in this context.
First, even if conspicuous investments have been made, the Italian technical infrastructural capacity is still very poor, particularly in the areas where telemedicine is needed the most: only around 18% of rural households are reached by Very High Capacity Networks (22). Poor network coverage can limit access to essential services, including emergency services, telemedicine, and online education. This can be especially critical in times of crisis or when remote services are needed.
Furthermore, it should be mentioned that rural systems and older adult population are typically reluctant to change, making the process more difficult (11). In some nations, the lack of computer or digital health literacy was identified as the biggest obstacle to the use of telemedicine (23, 24), so it is possible to expect similar problems in Italy, as it is still below the mean European threshold for digital skills (22). So, if it is evident that adequate infrastructure and sufficient digital literacy is needed to carry out a televisita or a teleconsultation, it is worth mentioning that both doctors and patients must receive an adequate training: according to the latest Report of the Digital Health Innovation Observatory, only 60% of primary care physicians have basic digital skills and only about 38% of the Italian population had heard about the EHR, so there's still a long way to go (25).
Additionally, the Italian NHS is highly fragmented at regional level (26), so different outcomes stemming from different resources could be expected. Regions with the highest funding may invest more, not only on digital tools and technical support, but also on infrastructure: broadband connection, updated operative systems, latest hardware, etc (27). Italy is a diverse country, and each region has its unique strengths and challenges. However, there are regions that face specific socio-economic difficulties and are often considered less prosperous in certain respects (for example, southern regions of Italy). It will be important to support less virtuous regions, in order to guarantee the principle of equity of care, and to avoid a “health journey” (the migration of people, usually from southern regions to northern regions, seeking for better healthcare standards).
Finally, it is worth mentioning that Italy is facing a severe challenge related to the shortage of doctors and healthcare professionals. The implementation and sustenance of this new digitally based healthcare model will require the support of trained and skilled medical and technical personnel. If future health care planning will not include a plan for recruitment and adequate professional education, it will be complicated to govern the vast change that the new model will cause on a regional and national scale.
Future implications
In 1995, Pisanelli et al. predicted that telemedicine would play a major role in Italy, improving the quality of health care and reducing costs (28). More than 20 years later, despite the epidemic input, records show that telemedicine is still only seldomly used (29). Italy is still far behind other nations where COVID has made a strong push (as in the US) (30), but this gap can be addressed by improving acceptance by end-users (31, 32). For this reason, it is important that health professionals, the media, and institutions promote clear, accurate and transparent communication and information on the new model, to involve the population and let them know the benefit of this approach.
Another aspect to consider is the role of COT and the introduction of the EHR. Compared to the current situation, it will be possible to see greater communication, not only between the territory and the patient, but also between the territory and the Community Health Houses, or between the territory and the hospital structure belonging to that district. All of this can happen both with the introduction of a new organization responsible for coordinating these elements (the COT), and with the unification of health data with the EHR. The possibility of having such uniformity will make both accessibility and decision making easier and faster in the transfer of patients between one structure and another, as well as in acute and chronic management, always in an integrated vision.
It is important to address the challenge posed by the “inverse care law”: people who need health assistance the most, will be the ones to have bigger difficulties to access digital healthcare or engage with digital platforms, e.g., disadvantaged groups suffering from poverty, language diversity, or disability. A crucial point is age: some studies found that telemedicine use was decreased as people aged (33, 34). Since 34.9% of the Italian population will be 65 or older by 2050 (9), policymakers and healthcare professionals will need to address the technology gap in older adult patients when implementing telemedicine and telehealth. When it comes to consulting a medical report, engaging in a patient's teleconsultation (televisita), or employing a telemonitoring smart bracelet, education and communication is the key to make things run smoothly. Formal programs and updated courses will be needed to embrace the digital illiterate and to prevent the already present gap from expanding further.
That said, strengthening communication of the benefits that telemedicine can bring to healthcare will be crucial to avoid frustration and ensure a smooth adoption by end-users (35). Policymakers and other stakeholders should address factors that might affect implementation, such as fostering teamwork and involving and supporting frontline employees, in order to ensure a successful application (36). In this sense, the Italian pace has been slow, but it is important to run toward the equality of access and the full integration at the national level of telemedicine services (37).
Although various tools and technologies are used for the provision of digitally integrated home care services within the various European countries, it is difficult to identify a nationally approved operational plan which regulates the use of remote home care technologies in a practical and definitive manner, such as the one just published in Italy.
One of the countries at a global level that has shown great commitment to the development of a digital ecosystem in the field of home care assistance is Australia. The government has included a specific plan on this area in its national agenda (“Australia's National Digital Health Strategy”) that implements digitally enabled models of care. The successful implementation of this Strategy is contingent on overcoming challenges related to data security, privacy, interoperability, and the engagement of both healthcare professionals and patients. Nevertheless, it also has the potential to improve the patient care, to enhance efficiency (administrative processes, reduce paperwork, and minimize redundant tests and procedures), to guarantee a better access to health records, to increase interoperability of the health system, and to provide telehealth and remote monitoring.
Author contributions
FC: Investigation, Supervision, Visualization, Writing—original draft, Writing—review & editing. AG: Investigation, Methodology, Writing—original draft, Writing—review & editing. AM: Investigation, Writing—original draft. FB: Investigation, Writing—original draft. FAC: Methodology, Writing—review & editing. VS: Writing—original draft. SB: Conceptualization, Writing—review & editing. SP: Writing—review & editing. AB: Supervision, Writing—review & editing. MB: Writing—review & editing. EC: Writing—original draft. WR: Visualization, Writing—review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The publication of this paper has been supported by the Joint Action 1011280885, entitled Xt-EHR_ Extended EHR@EU Data Space for Primary Use.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Consolidated Telemedicine Implementation Guide. Geneva: World Health Organization (2022). Available online at: https://www.who.int/publications/i/item/9789240059184 (accessed February 22, 2023).
2. Services B on HC Medicine I of. The Evolution of Telehealth: Where Have We Been and Where Are We Going. (2012). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK207141/ (accessed May 12, 2023).
3. Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth. Vol. 2, Global Observatory for eHealth series - Volume 2. (2010). Available online at: https://apps.who.int/iris/handle/10665/44497 (accessed February 22, 2023).
4. Razzano G. La missione salute del PNRR: le cure primarie, fra opportunità di una “transizione formativa” e unità di indirizzo politico e amministrativo. Corti supreme e salute (2022).
5. Agenzia Nazionale per i Servizi Sanitari Regionali. Gazzetta Ufficiale 5a Serie Speciale - Contratti Pubblici n.33 del 20-3-2023. Available online at: https://www.agenas.gov.it/comunicazione/primo-piano/2149-piattaforma-nazionale-di-telemedicina-pubblicato-bando-di-gara (accessed February 22, 2023).
6. Decreto Legge 21 settembre 2022. Approvazione delle linee guida per i servizi di telemedicina - Requisiti funzionali e livelli di servizio. (22A06184). Gazzetta Ufficiale Anno 163° - Numero 256. Available online at: https://www.gazzettaufficiale.it/eli/gu/2022/11/02/256/sg/pdf (accessed February 22, 2023).
7. PNRR Mission 6: Salute Componente 1 (M6C1). La telemedicina a supporto dei pazienti nell'assistenza sanitaria territoriale. Indicazioni metodologiche per la perimetrazione delle proposte di ppp per la piattaforma nazionale di telemedicina. Available online at: https://www.gazzettaufficiale.it/atto/serie_generale/caricaArticolo?art.versione=1&art.idGruppo=0&art.flagTipoArticolo=1&art.codiceRedazionale=22A06184&art.idArticolo=1&art.idSottoArticolo=1&art.idSottoArticolo1=10&art.dataPubblicazioneGazzetta=2022-11-02&art.progressivo=0 (accessed March 1, 2023)
8. PNRR MISSIONE 6-SALUTE Piano Nazionale di Ripresa e Resilienza Missione 6: Salute Componente 1 (M6C1): Reti di prossimità, strutture e telemedicina per l'assistenza sanitaria territoriale Investimento, 1,.2.1 Assistenza Domiciliare Linee guida organizzative contenenti il modello digitale per l'attuazione dell'assistenza domiciliare (Milestone EU M6C1-4, DM 29 aprile 2022). Gazzetta Ufficiale (2022). available online at: https://www.gazzettaufficiale.it/eli/id/2022/05/13/22A02808/sg (accessed July 1, 2023)
9. Previsioni della popolazione residente e delle famiglie 2 Popolazione in calo progressivo. Statistiche Report ISTAT. Available online at: https://www.istat.it/it/files/2022/09/REPORT-PREVISIONI-DEMOGRAFICHE-2021.pdf (accessed July 1, 2023).
10. Rao B, Lombardi A. Telemedicine: current status in developed and developing countries. J Drugs Dermatol. (2009) 8:371–5.
11. Beheshti L, Kalankesh LR, Doshmangir L, Farahbakhsh M. Telehealth in primary health care: a scoping review of the literature. Perspect Health Inf Manag. (2022) 19:1n.
12. Nesbitt TS, Cole SL, Pellegrino L, Keast P. Rural Outreach in Home Telehealth: Assessing Challenges Reviewing Successes. (2006). Available online at: https://www.liebertpub.com/doi/10.1089/tmj.2006.12.107 (accessed March 2, 2023).
13. Groom LL, McCarthy MM, Stimpfel AW, Brody AA. Telemedicine and telehealth in nursing homes: an integrative review. J Am Med Dir Assoc. (2021) 22:1784. doi: 10.1016/j.jamda.2021.02.037
14. Caffery LJ, Farjian M, Smith AC. Telehealth interventions for reducing waiting lists and waiting times for specialist outpatient services: a scoping review. J Telemed Telecare. (2016) 22:504–12. doi: 10.1177/1357633X16670495
15. Pfeil JN, Rados D V., Roman R, Katz N, Nunes LN, Vigo Á, et al. A telemedicine strategy to reduce waiting lists and time to specialist care: a retrospective cohort study. J Telemed Telecare. (2020) 29:10–7. doi: 10.1177/1357633X20963935
16. Gioia G, Salducci M. Medical and legal aspects of telemedicine in ophthalmology. Rom J Ophthalmol. (2019) 63:197–207.
17. Aashima A, Nanda M, Sharma R. A review of patient satisfaction and experience with telemedicine: a virtual solution during and beyond COVID-19 pandemic. Telemed e-Health. (2021) 27:1325–31. doi: 10.1089/tmj.2020.0570
18. Eze ND, Mateus C, Hashiguchi TCO. Telemedicine in the OECD: AN umbrella review of clinical and cost-effectiveness, patient experience and implementation. PLoS ONE. (2020) 15:e0237585. doi: 10.1371/journal.pone.0237585
19. Gentili A, Failla G, Melnyk A, Puleo V, Tanna GL Di, Ricciardi W, et al. The cost-effectiveness of digital health interventions: a systematic review of the literature. Front Public Heal. (2022) 10:2656. doi: 10.3389/fpubh.2022.787135
20. Cascini F, Gentili A. National recovery and resilience plan and health: qualitative analysis on the sustainability of the interventions on healthcare. Ann Ig. (2023) 35:602–610. doi: 10.7416/ai.2023.2561
21. 7° R. A cura di NNA Network Non Autosufficienza L'ASSISTENZA AGLI ANZIANI NON AUTOSUFFICIENTI IN ITALIA Punto di non ritorno Rapporto promosso dalla Fondazione Cenci Gallingani. (2020). Available online at: www.maggiolieditore.it (accessed May 12, 2023).
22. 2030 Digital Decade - Report on the state of the Digital Decade 2023. Catalogue number KK-04-23-958-EN-C. doi: 10.2759/999709
23. Scott Kruse C, Karem P, Shifflett K, Vegi L, Ravi K, Brooks M. Evaluating barriers to adopting telemedicine worldwide: a systematic review. J Telemed Telecare. (2018) 24:4. doi: 10.1177/1357633X16674087
24. Cascini F, Altamura G, Failla G, Gentili A, Puleo V, Melnyk A, et al. Approaches to priority identification in digital health in ten countries of the Global Digital Health Partnership. Front Digit Heal. (2022) 4:186. doi: 10.3389/fdgth.2022.968953
25. Osservatorio Sanità Digitale: la Ricerca 2022-2023. La sanità digitale in italia: gli ambiti di innovazione e il ruolo dei dati. (2023). Available online at: https://www.osservatori.net/it/ricerche/osservatori-attivi/sanita-digitale (accessed May 12, 2023).
26. Gazzetta, Ufficiale Serie Generale n,.4 del 07-01-1994 - Suppl. Ordinario n. 3. Available online at: https://www.gazzettaufficiale.it/eli/id/1994/01/07/094A0049/sg (accessed March 2, 2023).
27. Luo J, Tong L, Crotty BH, Somai M, Taylor B, Osinski K, et al. Telemedicine adoption during the COVID-19 pandemic: gaps and inequalities. Appl Clin Inform. (2021) 12:836. doi: 10.1055/s-0041-1733848
28. Pisanelli DM, Ricci FL, Maceratini R. A survey of telemedicine in Italy. J Telemed Telecare. (1995) 1:125–30. doi: 10.1177/1357633X9500100301
29. Parretti C, La Regina M, Tortu C, Candido G, Tartaglia R. Telemedicine in Italy, the starting point. Intern Emerg Med. (2022) 18:949–51. doi: 10.1007/s11739-022-03176-6
30. Tarazi WW, Finegold K, Sheingold SH, Wong Samson L, Zuckerman R, Bosworth A. COVID-19-related deaths and excess deaths among medicare fee-for-service beneficiaries. Health Aff . (2021) 40:879–85. doi: 10.1377/hlthaff.2020.02521
31. Harst L, Lantzsch H, Scheibe M. Theories predicting end-user acceptance of telemedicine use: systematic review. J Med Internet Res. (2019) 21:e13117. doi: 10.2196/13117
32. Mirone V, Celentano G, Ruvolo CC, Cirillo L, Fusco GM, Abate M, et al. Perceptions and attitudes toward the use of telemedicine for the postoperative outpatient urological care during the COVID-19 pandemic in an Academic Hospital in Southern Italy. Arch Ital di Urol e Androl. (2022) 94:375–9. doi: 10.4081/aiua.2022.4.375
33. Eberly LA, Kallan MJ, Julien HM, Haynes N, Khatana SAM, Nathan AS, et al. Patient characteristics associated with telemedicine access for primary and specialty ambulatory care during the COVID-19 pandemic. JAMA Netw Open. (2020) 3:e2031640. doi: 10.1001/jamanetworkopen.2020.31640
34. Davies AR, Honeyman M, Gann B. Addressing the digital inverse care law in the time of COVID-19: potential for digital technology to exacerbate or mitigate health inequalities. J Med Internet Res. (2021) 23:e21726. doi: 10.2196/21726
35. Sinsky CA, Jerzak JT, Hopkins KD. Telemedicine and team-based care: the perils and the promise. Mayo Clin Proc. (2021) 96:429. doi: 10.1016/j.mayocp.2020.11.020
36. Xyrichis A, Iliopoulou K, Mackintosh NJ, Bench S, Terblanche M, Philippou J, et al. Healthcare stakeholders' perceptions and experiences of factors affecting the implementation of critical care telemedicine (CCT): qualitative evidence synthesis. Cochrane Database Syst Rev. (2021) 2:CD012876. doi: 10.1002/14651858.CD012876.pub2
37. DECRETO-LEGGE 27 gennaio 2022 n. 4 Misure urgenti in materia di sostegno alle imprese e agli operatori economici, di lavoro, salute e servizi territoriali, connesse all'emergenza da COVID-19, nonche' per il contenimento degli effetti degli aumenti dei prezzi nel settore elettrico. GU Serie Generale n.21 del 27-01-2022. Available online at: https://www.gazzettaufficiale.it/eli/id/2022/01/27/22G00008/sg (accessed February 22, 2023).
Keywords: digital health, teleassistance, telemonitoring, televisit, telehealth, home assistance
Citation: Cascini F, Gentili A, Melnyk A, Beccia F, Causio FA, Solimene V, Battilomo S, Paone S, Borghini A, Bartolo M, Chiarolla E and Ricciardi W (2023) A new digital model for the Italian Integrated Home Care: strengths, barriers, and future implications. Front. Public Health 11:1292442. doi: 10.3389/fpubh.2023.1292442
Received: 11 September 2023; Accepted: 30 October 2023;
Published: 14 November 2023.
Edited by:
Kerstin Denecke, Bern University of Applied Sciences, SwitzerlandReviewed by:
Jerrald Lau, National University of Singapore, SingaporeCopyright © 2023 Cascini, Gentili, Melnyk, Beccia, Causio, Solimene, Battilomo, Paone, Borghini, Bartolo, Chiarolla and Ricciardi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Gentili, YW5kcmVhLmdlbnRpbGkxOTg5QGdtYWlsLmNvbQ==