 Christian R. Mejia1
Christian R. Mejia1 Víctor Serna-Alarcón2,3
Víctor Serna-Alarcón2,3 Martín A. Vilela-Estrada2,3
Martín A. Vilela-Estrada2,3 Jose Armada4Milward Ubillus1Jose Beraún-Barrantes1Aldo Álvarez-Risco5*
Jose Armada4Milward Ubillus1Jose Beraún-Barrantes1Aldo Álvarez-Risco5* Shyla Del-Aguila-Arcentales6Neal M. Davies7,8Jaime A. Yáñez9
Shyla Del-Aguila-Arcentales6Neal M. Davies7,8Jaime A. Yáñez9- 1Universidad de Huánuco, Huánuco, Peru
- 2Universidad Privada Antenor Orrego, Piura, Peru
- 3Hospital Regional José Cayetano Heredia, EsSalud, Piura, Peru
- 4Universidad Continental, Lima, Peru
- 5Universidad Tecnológica del Perú, Lima, Peru
- 6Escuela de Posgrado, Universidad San Ignacio de Loyola, Lima, Peru
- 7Faculty of Pharmacy and Pharmaceutical Sciences, University of Alberta, Edmonton, AB, Canada
- 8Asociación Médica de Investigación y Servicios en Salud, Lima, Peru
- 9Universidad Peruana de Ciencias Aplicadas, Facultad de Educación, Carrera de Educación y Gestión del Aprendizaje, Lima, Peru
Introduction: Latin America was the region most affected by COVID-19 in the second quarter of 2020, and consequently, the impact on mental health requires evaluation. The aim of this study was to assess the risk of post-traumatic stress disorder (PTSD) caused by bereavement due to COVID-19 in 12 countries in Latin America.
Methods: The current study was an analytical cross-sectional study. Validated tests were applied for PTSD, depression, anxiety, and stress (DASS-21), questions about the respondent’s condition or their environment, and demographic questions, as well as the length of the mourning period of suffering.
Results: The outcomes demonstrated that the PTSD risk increased for women (p < 0.001), when a friend or acquaintance had COVID-19 (p = 0.002), when a close relative died from COVID-19 (p = 0.010), having severe depression (p <0.001), severe anxiety (p <0.001), severe stress (p <0.001), residing in Chile (p <0.001), Paraguay (p <0.001), Bolivia (p <0.001), Costa Rica (p <0.001) or El Salvador (p = 0.005). On the other hand, there was less risk of PTSD at an older age (p <0.001) or if respondents had a sentimental partner (p = 0.025). In the case of severe PTSD, there was a greater gender risk for women (p <0.001), a close relative dying from COVID-19 (p = 0.017), having severe depression (p <0.001), severe anxiety (p <0.001), severe stress (p <0.001), residing in Chile (p <0.001), Paraguay (p <0.001), Bolivia (p <0.001) and Costa Rica (p = 0.002). It was also observed that there was less risk of severe PTSD at an older age demographic (p <0.001).
Discussion: It can be concluded that the percentages of PTSD are high in its clinical presentation as severe, especially among Latin American women.
Introduction
COVID-19 is an infectious illness caused by the SARS-CoV-2 virus. Most infected people with the virus present mild to moderate respiratory symptoms and recover without treatment requiring hospitalization. However, many people can also become severely ill and require medical attention (1). COVID-19 has been a major global socioeconomic and health problem comparable to what could be caused by a large-scale war (2). The beginning of this pandemic arose at the end of 2019 (3, 4), having a significant effect on Europe during the first quarter of 2020 (5) and affecting the North American continent in the subsequent months (6–8). The pandemic caused significant morbidity and mortality in millions of patients, as well as social and economic repercussions such as isolation, restrictions, and a host of additional problems and sequelae (9, 10). In addition, through mainstream and social media, additional fear and panic were generated and exacerbated in the populations (11–13).
There is evidence that several illnesses, such as hypertension (14), diabetes (15, 16), Ebola (17–19), SARS (20), dengue (21), H7N9 (22), and H1N1 (23), can generate post-traumatic stress disorder (PTSD). PTSD has been defined as a mental health condition that can affect people who have experienced or witnessed a traumatic event, series of events, or set of circumstances. Such an event can be emotionally or physically harmful or life-threatening, which can lead to symptoms that affect the mental, physical, social, and/or spiritual well-being of an individual (24).
The measurement of PTSD using DASS-21 (25–28) has previously been undertaken. However, there have been few studies linking PTSD and COVID-19 with survivors (29, 30) and healthcare workers (31, 32).
The possible effect of the COVID-19 pandemic on population mental health (33), especially for those who suffered from the disease and those who had relatives who were infected or even died, has been addressed (34). The COVID-19 pandemic was characterized by some relevant features that increase the risk of PTSD, such as an often-unpredictable course of the disease, high mortality rates (35–37), lack of knowledge and preventive practices (38), and lack of effective treatment, treatment guidelines, and the appearance of viral variants (39). PTSD related to COVID-19 has been reported in healthcare workers (31, 32) and the general public (40, 41), including perinatal women (30).
Recent studies have highlighted the significant occurrence of PTSD among individuals affected by COVID-19, with health professionals on the front lines facing heightened risks due to intense and prolonged exposure to trauma. The nature of one’s vocation, such as the specific health profession and the unit of work within the healthcare system, plays a crucial role in determining susceptibility to PTSD. The prevalence of PTSD among healthcare workers during the COVID-19 pandemic has been reported to be 13.52% globally (42). A study comparing Italian healthcare professionals to a control group of the general population found that the prevalence of self-reported PTSD symptoms caused by the COVID-19 pandemic was high (43). Another study reported that the prevalence of PTSD among intensive care unit (ICU) professionals increased to 73.3% following the COVID-19 health crisis (44). A review of the literature highlighted the high prevalence of PTSD, especially among healthcare professionals who work in COVID-19 wards (45). A multi-centered cross-sectional study in Northwest Ethiopia found the prevalence of PTSD among healthcare providers during the COVID-19 pandemic to be 55.1% (46).
These findings highlight the significant effect of the COVID-19 pandemic on the mental health of healthcare professionals, emphasizing the need for standardized and culturally sensitive measures to assess the true extent of PTSD in different populations. The nature of one’s work and geographical location have been identified as key factors influencing susceptibility to PTSD. Additionally, age emerges as a key moderator, with younger individuals often exhibiting different vulnerability patterns compared to their older counterparts. The geographical aspect is also crucial, as PTSD prevalence can vary across continents, reflecting diverse cultural and contextual factors. The choice of assessment tools can influence reported prevalence rates, emphasizing the importance of standardized and culturally sensitive measures to capture the true extent of PTSD in different populations. PTSD varies widely, with a lifetime prevalence ranging from 6.1 to 9.2% in national samples (42, 47, 48). In the United States, the 1 year prevalence of PTSD was estimated at 6.7% among male veterans and 11.7% among female veterans, and the lifetime prevalence was reported to range from 3.4 to 26.9% among civilians.
Factors, such as female sex, lower income, younger age, and behavioral health conditions, were identified as risk factors for PTSD (47, 48). These findings highlight the importance of understanding significant moderators of PTSD prevalence for tailoring interventions and support strategies for those at risk of or experiencing PTSD.
In highly affected populations, such as Peru, which became the country with the world’s highest per-capita COVID-19-related mortality (49, 50), significant mental health issues have arisen. In addition, other Latin American countries have also been significantly affected (51–53). However, to the best of our knowledge, there has not been any published study that addressed early PTSD in a large Latin American population that could serve as a baseline of PTSD levels at the different stages of the pandemic: surge of infodemic, early quarantine, various waves, and prior to the massive distribution of vaccines (54, 55).
The objective of this study was to evaluate the risk of PTSD according to the immediate environment’s suffering or grief after exposure to COVID-19 in 12 countries in Latin America.
Materials and methods
Study design
We conducted an online cross-sectional multicenter survey in Spanish-speaking countries (Peru, Chile, Paraguay, Mexico, Colombia, Bolivia, Panama, Ecuador, Costa Rica, El Salvador, Honduras, and Guatemala) between June 7, 2021 and August 30, 2021, which were the pandemic months with the most significant effect in Latin America. The design was based on the fact that each respondent was approached only once and that descriptive and analytical results were generated. It was determined that a minimum sample size of 3,204 was necessary to achieve a minimum percentage difference of 2.5% (49.0% vs. 51.5%), a statistical power of 80%, and a confidence level of 95% (data not shown). The sample size was calculated using power analysis (56) and based on a previous study in Peru that assessed PTSD after a natural phenomenon (57). Residents of the countries in question were included who reported that they remained in those territories during the time of the pandemic and who agreed to participate in the research. Duplicate responses were excluded, as were those who did not answer all the questions on the measured scales, those who did not have complete personal information, or those who presented anomalous response patterns (more than 4,000 surveys were excluded for all these reasons). The survey consisted of an online questionnaire in Google Surveys that was sent via WhatsApp, Messenger, and Facebook, and it was configured to enable the submission of an email at the end of the survey so that the investigation group could ensure that individual data were submitted. The survey was generated only online because, at the time of sampling, there were still individual restrictions on circulating freely in public places. In addition, online sampling was selected to prevent the surveyors from becoming infected and spreading the disease even further. The shared questionnaire was made anonymous, ensuring data confidentiality and reliability; each participant was informed in the first part of the questionnaire that they were free to participate, that they were free to withdraw if they liked, and that, by not asking for identifying data, we would not be able to know or divulge their identity. This survey was undertaken in the Spanish language since we surveyed only Spanish-speaking countries in Latin America in laboratory-confirmed cases. The survey was performed from June 7, 2021 to August 30, 2021, after approximately 3–5 months of lockdown and social distancing measures in Latin America due to the COVID-19 outbreak. At the beginning of the survey (June 7, 2021), the number of confirmed COVID-19 cases in the surveyed countries totaled 625,495 and the number of confirmed deaths was 36,287, while, at the end of the survey (August 30, 2021), the number of confirmed cases increased to 2,685,447 and the deaths increased to 136,068. We surveyed the public with adults (over 18 years old) in all countries that participated in the survey (Peru, Chile, Paraguay, Mexico, Colombia, Bolivia, Panama, Ecuador, Costa Rica, El Salvador, Honduras, and Guatemala). Participants were recruited through the FELSOCEM-ASOMEDISS COVID-19 Latam (which is an organization of physicians and medical students from almost every country in Latin America), a network of investigators that includes physicians, health professionals, and students performing COVID-19 social epidemiological studies in Peru and Latin America. Each collaborator verified that the contact to whom they sent the virtual survey could answer it adequately and that they were willing to resolve the doubts of the participants.
Outcomes and covariates
The survey (Annex 1) included 46 questions, of which 13 were demographic, 21 were from the DASS-21 test, and 12 were related to suffering from post-traumatic stress and also having this pathology, but in a severe stage (with suicidal ideation), both by applying the Short Post-traumatic Stress Disorder Rating Interview (SPRINT-E) created in 2001 to measure the symptoms of this pathology (58). The instrument has been used in Chile, where it obtained a value of 0.92 for Cronbach’s alpha (59); in the current study, a Cronbach’s alpha of 0.93 was obtained. For anxiety, stress, and depression, the DASS-21 test was used, which has been validated and used in multiple settings (60), where the severe category was used for each case and a Cronbach’s alpha of 0.96 was obtained.
There were multiple exposure variables as follows: (a) if a friend or close acquaintance was afflicted with COVID-19; (b) if a friend or acquaintance died from COVID-19; (c) if someone at home was sick from COVID-19; (d) if a family member was not home, they became ill from COVID-19; (e) if a close relative died from COVID-19; (f) if a distant relative died from COVID-19; and (g) if it was suspected or it was very likely that someone had COVID-19 (according to the report of having symptoms, but not a confirmatory test) and had or became ill with COVID-19 (confirmed with rapid or molecular test). The demographic questions included the gender (male or female), age (in completed years), if they had a romantic partner (yes or no), job status, type of job, level of education (university / postgraduate or a lower academic level), and the country of residence (of the 12 countries already mentioned). There were multiple exposure variables as follows: if a friend or close acquaintance became sick from COVID-19, if a friend or acquaintance died from COVID-19, if someone at home fell ill from COVID-19, if a family member who was not at home became ill from COVID-19, if a close relative died from COVID-19, if a distant relative died from COVID-19 if it was suspected or it was very likely that they had contracted COVID-19 (according to the report of having symptoms, but not a confirmatory test) and had or became ill with COVID-19 (confirmed with rapid or molecular test).
Ethics approval
The research has the approval of the Universidad Privada Antenor Orrego (UPAO) Bioethics Committee, a human ethics committee in Peru (Resolution of the Bioethics Committee No. 0240-2020-UPAO). The same endorsement could not be made in other countries since the pandemic generated the closure of most institutions that housed researchers during the pandemic. After obtaining approval in Peru, we proceeded with the respondents in the various countries; in each one, a non-random sample was obtained (due to the difficulty of having official lists). The participants remained anonymous and could finish the survey at any time, and their information was kept confidential. All the survey participants were well-versed in the study intentions and were required to consent before enrollment. The participants were not involved in any of the planning, execution, or reporting stages of the study.
Statistical analysis
Data analysis was done in STATA version 14 (Stata Corp.) with a significance level of p < 0.05. The instrument validity was assessed with the known-groups validity approach by fitting multivariate analysis. Univariate statistics were represented with frequencies and percentages for categorical variables. A description of the variables was made in each country, showing the percentages of the dependent variables and anxiety, depression, and stress (in their severe form). Then, the bivariate models were carried out, where each independent variable was crossed with the two dependent variables, from which they were statistically significant (p < 0.05), and they were entered into the multivariate model. For analytical statistics, adjusted prevalence ratios (aPR) and 95% confidence intervals (CIs) were obtained using generalized linear models (GLM), with the Poisson family, log-link function, and models for robust variances to adjust for the large sample size.
Results
Sociodemographic characteristics of the respondents
The survey was sent to 9,000 people in Peru, Chile, Paraguay, Mexico, Colombia, Bolivia, Panama, Ecuador, Costa Rica, El Salvador, Honduras, and Guatemala to achieve the minimum sample size of 3,204 calculated based on power analysis. Out of the 9,000 surveys sent online, we received 8,194 responses indicating a 91.0% response rate. Most participants were women (4,854 [59.2%]), were those aged 18–89 years, were single (6,699 [81.8%]), had some university studies or higher (5,750 [70.2%]), and had a romantic partner (3,669 [44.8%]). The country evaluated with the highest response was Peru, with 4,026 surveys, and it had the most deaths/infections (120). The population was also evaluated in Chile (738), Mexico (647), Paraguay (583), Colombia (435), Bolivia (385), Panama (374), Ecuador (279), Costa Rica (256), El Salvador (199), Honduras (162), and Guatemala (110).
Of the 8,194 respondents in Latin America, there was a higher frequency of severe episodes of anxiety (Chile 17%, Peru 14%, and Bolivia 14%), stress (Chile 19% and Costa Rica 14%), and depression (Chile 15% and Ecuador 14%). In addition, there was a high frequency of PTSD (Chile 37%, Paraguay 30%, and Bolivia 30%) and severe PTSD (Chile 22%, Costa Rica 16%, and Bolivia 16%; Figure 1).
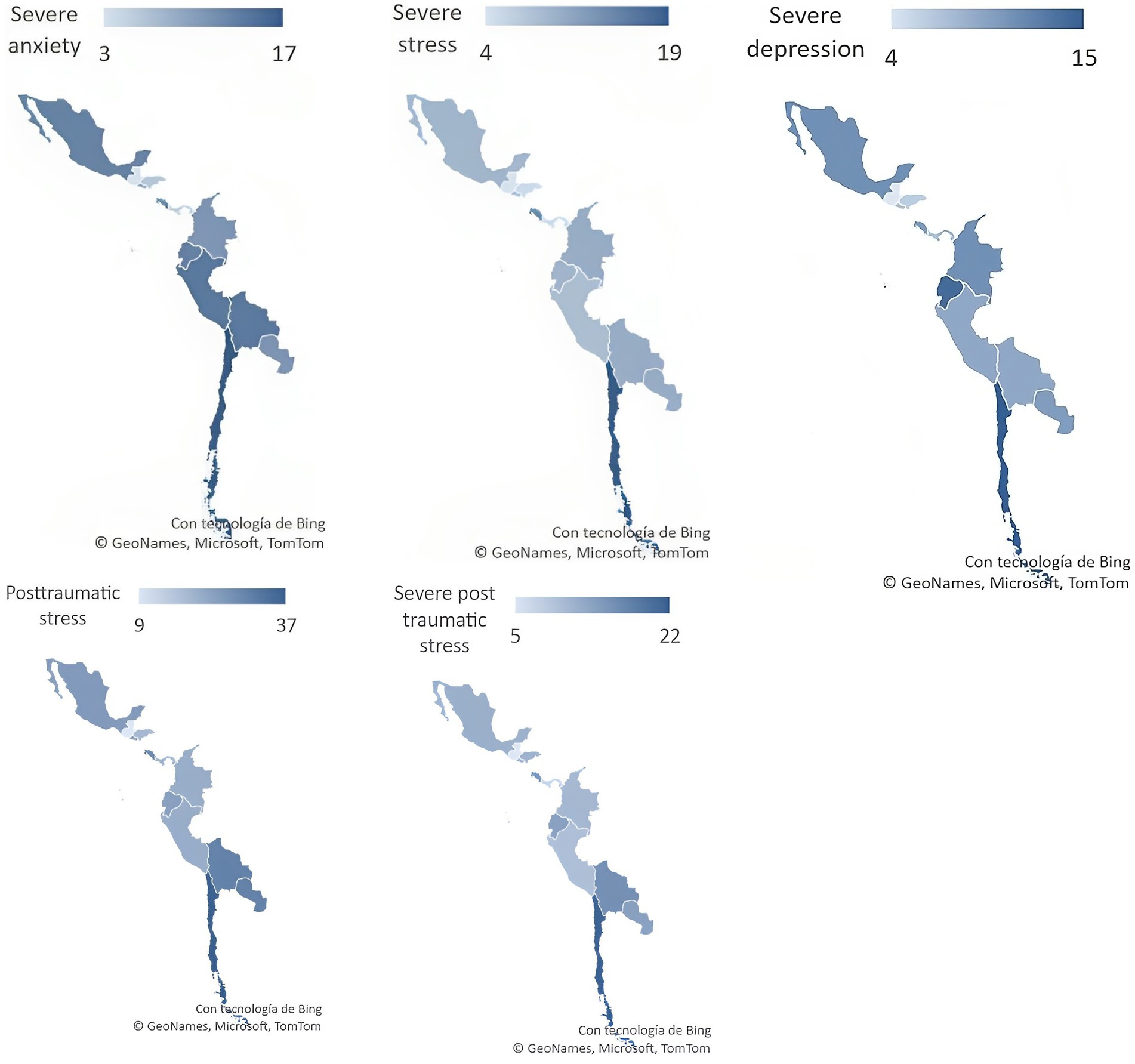
Figure 1. Severe anxiety, severe stress, severe depression, PTSD, and severe PTSD in 12 Latin American countries during the COVID-19 pandemic.
In the bivariate analysis, it was determined that more PTSD or severe PTSD was observed among women (p < 0.001 for both), among those who had a friend or acquaintance with the diagnosis of COVID-19 (p < 0.001 for both), among those who had a relative outside the home with COVID-19 (p < 0.035 for both), among those who had a close relative who died from COVID-19 (p < 0.002 for both), among those whose distant relative died from COVID-19 (p < 0.001 for PTSD), if the respondent suspected COVID-19 (p = 0.002 for both), and if the respondent confirmed that they had COVID-19 (p = 0.008 for severe PTSD). Additionally, respondents who confirmed their own COVID-19 diagnosis had severe depression (p < 0.001 for both), severe anxiety (p < 0.001 for both), or severe stress (p < 0.001 for both). Similarly, compared to Peru, there was greater prevalence among those who resided in Chile (p < 0.001 for both), Mexico (p = 0.019 for PTSD), Paraguay (p < 0.002 for both), Bolivia (p < 0.001 for both), Costa Rica (p < 0.008 for both), or Guatemala (p = 0.005 for PTSD). On the contrary, the risk was reduced with advanced age (p < 0.001 for both) and by having a romantic partner (p < 0.001 for EPT) (Table 1).
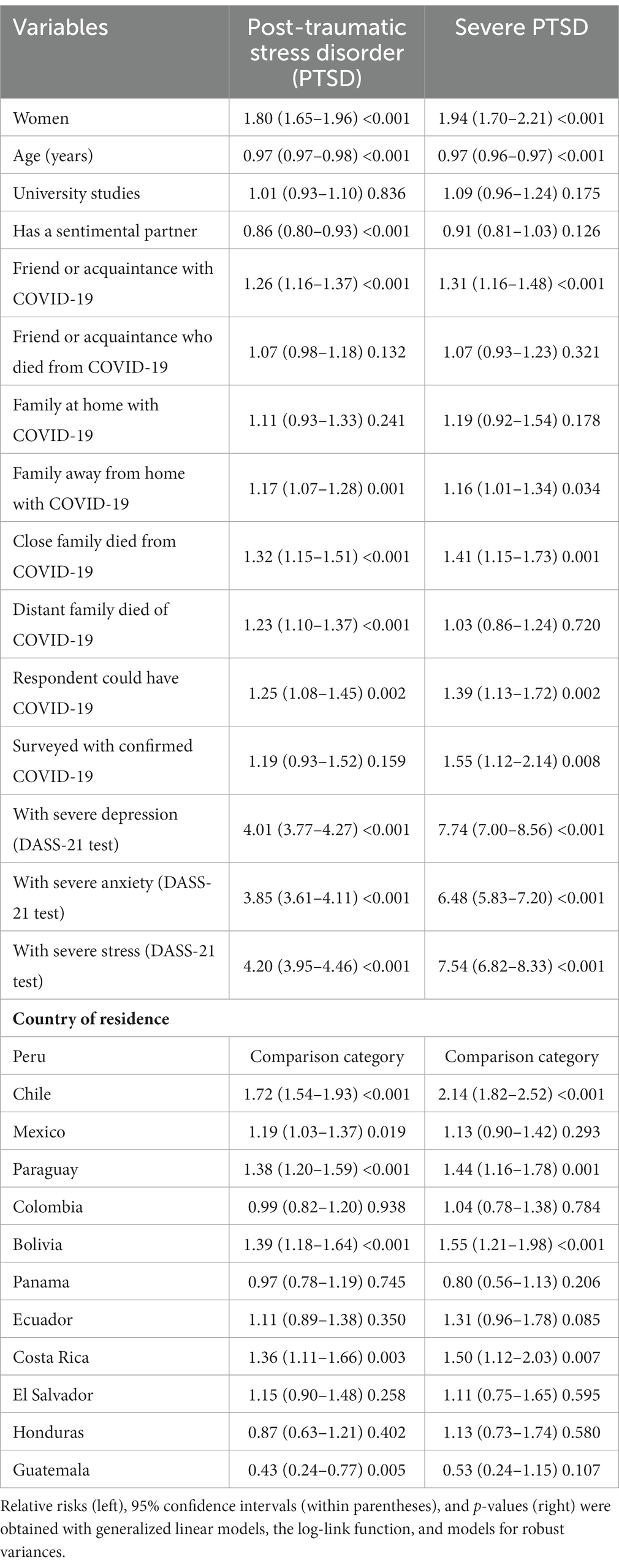
Table 1. Bivariate analysis of risk factors for post-traumatic stress disorder (PTSD) and severe PTSD in 12 Latin American countries during the COVID-19 pandemic (n = 8,194).
Multivariate analysis was performed, and a higher risk of PTSD was found among women (p < 0.001), among those who had a friend or acquaintance with a diagnosis of COVID-19 (p = 0.002), among those whose close relative died from COVID-19 (p = 0.010), among those who had severe depression (p < 0.001), severe anxiety (p < 0.001), or severe stress (p < 0.001) at the time of the survey, and among those who resided in Chile (p < 0.001), Paraguay (p < 0.001), Bolivia (p < 0.001), Costa Rica (p < 0.001), or El Salvador (p = 0.005). On the other hand, there was lower risk of PTSD at an advanced age (p < 0.001) or if the respondent had a sentimental partner (p = 0.025), adjusted for three variables (Table 2).
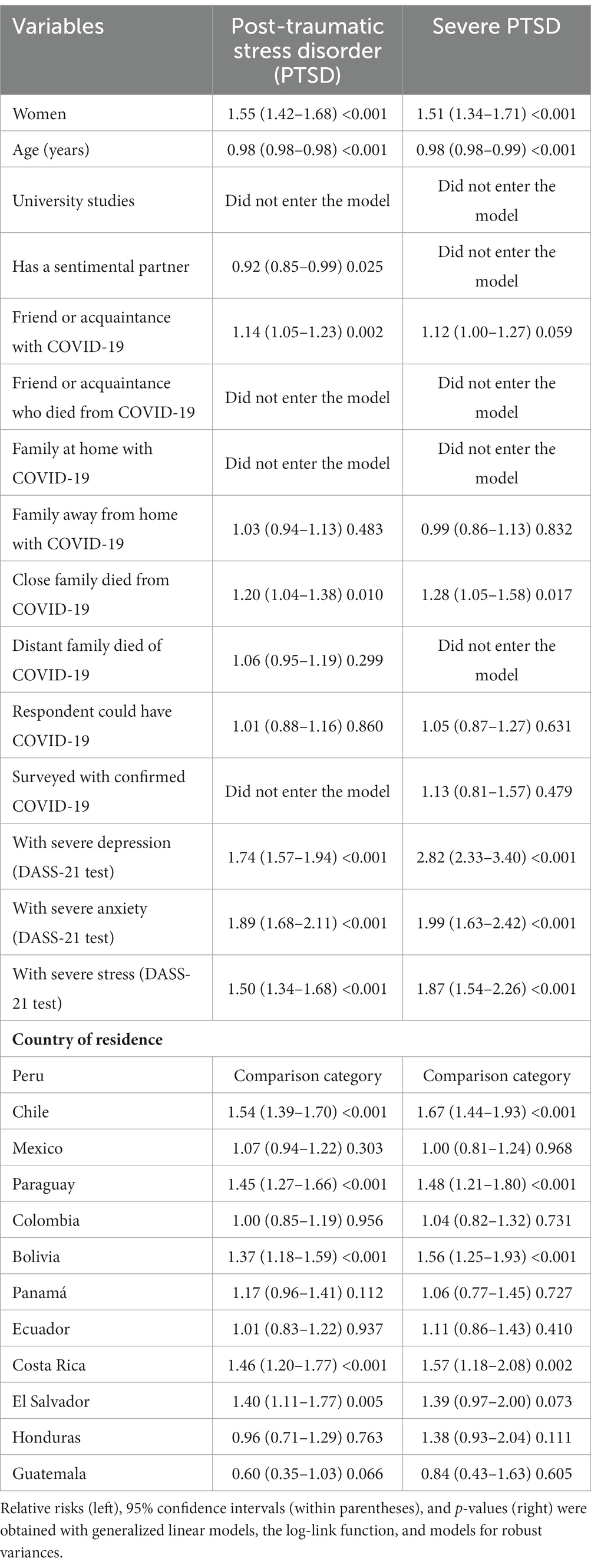
Table 2. Multivariate analysis of risk factors for PTSD and severe PTSD in 12 Latin-American countries during the COVID-19 pandemic (n = 8,194).
For severe PTSD, there was a higher risk among women (p < 0.001), among those who had a close relative who died from COVID-19 (p = 0.017), among those who had severe depression (p < 0.001), severe anxiety (p < 0.001), and severe stress (p < 0.001), among those who resided in Chile (p < 0.001), Paraguay (p < 0.001), Bolivia (p < 0.001), and Costa Rica (p = 0.002); on the other hand, there was a lower risk of severe PTSD at an older age (p < 0.001), adjusted by four variables (Table 2).
Discussion
Frequencies of PTSD and severe PTSD were found in up to one in three and one in five respondents, respectively. Despite not being able to extrapolate the results to the rest of the continent, these results are alarming due to the high number of people with an alteration in the mental health plane, without counting the large percentage of respondents who have thought about committing suicide. The findings of PTSD are approximately equivalent to those previously reported in other geographical locations; this is consistent with a meta-analysis of more than 60 studies published in different circumstances in countries of Europe, Asia, and North America, where a clinically significant prevalence of PTSD of 32% was recorded (61). Furthermore, the findings related to severe PTSD are striking since, even in China, the epicenter of the pandemic, and Italy, one of the countries initially most affected by COVID-19 (62), a much lower prevalence of PTSD was reported, and there have been very few cases of severe PTSD (40, 63). The timing of the measurement, access to information about the severity of the virus, and the educational level affected the results since it is evident that those with a lower level of education have a greater risk of psychological distress (64). All these variables should be further studied, as this is a fairly accurate approximation of the circumstances reflecting occurrences in the Latin-American population’s mental health arena.
Women were at increased risk of PTSD and severe PTSD, as observed in previous research (63, 65), which shows that women have been more susceptible to alterations caused by the coronavirus. In parts of Latin America, women are still associated with significant domestic work and caring for the home and its members, which also increased with the “lockdown” families had in their homes. In addition, women historically have occupied the roles of caregivers of the home, which, in some similar situations, translates into symptoms, such as insomnia, fatigue, anxiety, stress, and depression. Finally, it is often assumed that, in addition to their salaried jobs (66), women are subject to changes due to the crisis. Finally, cases have been reported of women who, due to the pandemic’s effects and measures, were forced to return to live with their domestic partner abusers, further increasing their access to support networks (67). This paragraph highlights the null gender perspective in the general measures taken during the pandemic, often overlooking their direct effects on the health of women.
At an older age, there was a lower risk of PTSD and severe PTSD. These results are striking since they are contrasted with other articles that present this age group as one of the highest risk groups. This difference can be explained by concerns about health complications for older adults and their close family members, along with comorbidities, the decrease in controls for chronic diseases during the pandemic, and the infantilization of their decisions in this same context (68). However, our study results can be further explained because older adults have already lived with these daily concerns and have been able to cope with a series of uncertain events, such as other epidemics (21). In addition to this, they tend to have limited access to social networks, which is considered a protective factor because they would avoid being affected by news that could cause anxiety, depression, and stress (69). The previous explanation does not mean that this is a group that must be in constant analysis to be able to detect the appearance of alarming symptoms, such as isolation, anxiety, excessive worries about the disease, excessive thinking about death, and other typical signs, which tend to go unnoticed due to the global contingency.
Those respondents who had a romantic partner were at lower risk of developing PTSD in the context of the COVID-19 pandemic. Our results are similar to those found in other studies applied to the general population of China (70, 71), Italy (72), Mexico (64), and Spain (73). The underlying factors that may explain this protective effect are real or perceived satisfaction, stability, understanding, attention, support, and emotional security. In turn, this effect depends on the quality of romantic relationships and communication (virtually or remotely in the first month and in person when the quarantines were lifted), the degree of alliance and commitment of the couple, mutual trust, and well-being generated (74). On the contrary, the marital status of widowed, separated, or divorced people has been reported as a risk factor for suffering from severe PTSD (75).
Severe stages of anxiety, depression, or stress have a higher risk of PTSD and severe PTSD, which can be rationalized as a determinant because each individual experiences and faces the same event differently (76). PTSD is a chronic mental illness that generally develops after being exposed to severe trauma, intrusive memories, distressing dreams, and a negative mood. It is estimated that approximately 6% of people exposed to psychological trauma go on to develop PTSD (57); according to this data and other references, it is considered that severe stages of anxiety, depression, or stress are risk factors for having PTSD and severe PTSD. These results are related to gender differences since it has been shown that women with some susceptibilities have a higher risk of being affected by PTSD (77).
Residing in different countries generated an increased risk of PTSD or severe PTSD compared to those who lived in Peru, which is the country with the most significant effect worldwide, showing that mental health could be impaired in multiple realities. These outcomes have been shown in studies of the area in different countries across several continents (78–84). Therefore, it is suggested that mental health measurement campaigns be generated in various settings as a baseline so that measures can be implemented that facilitate recovery, especially among the populations identified as being the most affected.
Some additional recommendations for future research and interventions to address the mental health concerns of people during pandemics or other high-stress situations include additional social and practical support. Literature reviews have concluded that social and practical support are important mechanisms for alleviating psychological distress and may be preferred to professional psychological support. This highlights the need for interventions that focus on providing social and practical support to individuals affected by pandemics (85). Furthermore, research on the effectiveness of mental health interventions during pandemics is growing. Future research should continue to evaluate the effectiveness of various interventions, including psychosocial interventions and the implementation of existing or new training programs, to address the mental health sequelae of pandemics (86). Moreover, addressing the psychological response of healthcare workers to medical pandemics is complicated. Future research should focus on developing interventions that specifically address the unique psychological challenges faced by healthcare workers during pandemics, including the effect of the pandemic on their personal, professional, and relational levels (87).
Additionally, when designing and implementing mental health interventions, it is important to consider cultural adaptations and the mental health workforce. Future research should explore the cultural and geographical constraints that may affect the effectiveness of mental health interventions during pandemics and the role of the mental health workforce in providing support to those most in need (86). Our recommendations highlight the need for future research and interventions that focus on providing social and practical support, evaluating the effectiveness of interventions, addressing the psychological response of healthcare workers, and considering cultural adaptations and the mental health workforce during pandemics.
The main implications of this research were, in general, the fact that we contributed to filling a gap that existed in terms of the immediate consequences in mental health to cause PTSD in a large population in Latin America as well as the main factors associated with it. The effects of the COVID-19 pandemic on other aspects of mental health in the medium and long term in Latin America have been reported (88–91).
All of these implications should serve the health sector, as well as the governing and academic institutions of each country. To evaluate the mental health of the population continuously, an investigation is recommended. Post-traumatic stress in various populations can cause medium- to long-term effects and can be linked with an increase in suicides (92, 93). Therefore, it highlights the importance of generating early detection, intervention, and treatment programs.
The study had an information bias because it was based on the respondents’ information, especially those who suffered (or had suspicions) if someone in their environment became ill or died due to COVID-19. It is possible that some cases did not occur, but this issue is not crucial because we intended to capture the thoughts and mental effects of respondents. One limitation was a small sample size in some countries, which requires a situational analysis to extrapolate the results. Our objective was to show the reality of a time period related to the significant mortality peaks in each country during the pandemic. This can be considered the main strength of the research because it evaluates the incidence of PTSD early on in the pandemic in a large population in multiple Latin American countries with different socioeconomic realities and various mental health coping mechanisms. Further research is warranted to determine the current incidence of PTSD and how it might be a further detriment to the overall mental health of the Latin American population.
Conclusion
It can be concluded that, in this cross-sectional survey, the prevalence percentages of PTSD risk are high in its severe presentation post-COVID-19 in 12 countries in Latin America. This risk increased among women if they had a friend or acquaintance who suffered from COVID-19 or a close relative who died from COVID-19; it also increased among those who had severe anxiety, depression, or stress and resided in Latin American countries. On the contrary, older age or having a romantic partner appears to reduce the risk of PTSD, as determined in this cross-sectional survey.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Universidad Privada Antenor Orrego (No. 0240-2020-UPAO). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CM: Conceptualization, Formal analysis, Investigation, Methodology, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. VS-A: Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. MV-E: Conceptualization, Investigation, Supervision, Visualization, Writing – original draft, Writing – review & editing. JA: Investigation, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing. MU: Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. JB-B: Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. AÁ-R: Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. SD-A-A: Formal analysis, Visualization, Writing – original draft, Writing – review & editing. ND: Resources, Visualization, Writing – original draft, Writing – review & editing. JY: Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. WHO . (2022). "Coronavirus disease (COVID-19)." Available at: https://www.who.int/health-topics/coronavirus#tab=tab_1 (Accessed Nov 11, 2023).
2. Humphries, MO . Paths of infection: the first world war and the origins of the 1918 influenza pandemic. War Hist. (2014) 21:55–81. doi: 10.1177/0968344513504525
3. Chan, JF-W, Yuan, S, Kok, K-H, Kelvin Kai-Wang To, Chu, H, Yang, J, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. (2020) 395:514–23. doi: 10.1016/S0140-6736(20)30154-9
4. Petzold, MB, Bendau, A, Plag, J, Pyrkosch, L, Maricic, LM, Betzler, F, et al. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. (2020) 10:e01745. doi: 10.1002/brb3.1745
5. Alifano, M, Attanasi, G, Iannelli, F, Cherikh, F, and Iannelli, A. COVID-19 pandemic: a European perspective on health economic policies. J Behav Econ Pol. (2020) 4:35–43.
6. Burki, T . COVID-19 in Latin America. Lancet Infect Dis. (2020) 20:547–8. doi: 10.1016/S1473-3099(20)30303-0
7. Garcia, PJ, Alarcón, A, Bayer, A, Buss, P, Guerra, G, Ribeiro, H, et al. COVID-19 response in Latin America. Am J Trop Med Hyg. (2020) 103:1765–72. doi: 10.4269/ajtmh.20-0765
8. Kirby, T . South America prepares for the impact of COVID-19. Lancet Respir Med. (2020) 8:551–2. doi: 10.1016/S2213-2600(20)30218-6
9. Hiscott, J, Alexandridi, M, Muscolini, M, Tassone, E, Palermo, E, Soultsioti, M, et al. The global impact of the coronavirus pandemic. Cytokine Growth Factor Rev. (2020) 53:1–9. doi: 10.1016/j.cytogfr.2020.05.010
10. Zhang, SX, Sun, S, Jahanshahi, AA, Alvarez-Risco, A, Ibarra, VG, Li, J, et al. Developing and testing a measure of COVID-19 organizational support of healthcare workers – results from Peru, Ecuador, and Bolivia. Psychiatry Res. (2020) 291:113174. doi: 10.1016/j.psychres.2020.113174
11. Bendau, A, Petzold, MB, Pyrkosch, L, Maricic, LM, Betzler, F, Rogoll, J, et al. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur Arch Psychiatry Clin Neurosci. (2021) 271:283–91. doi: 10.1007/s00406-020-01171-6
12. Naeem, M . Do social media platforms develop consumer panic buying during the fear of Covid-19 pandemic. J Retail Consum Serv. (2021) 58:102226. doi: 10.1016/j.jretconser.2020.102226
13. Sasaki, N, Kuroda, R, Tsuno, K, and Kawakami, N. Exposure to media and fear and worry about COVID-19. Psychiatry Clin Neurosci. (2020) 74:501–2. doi: 10.1111/pcn.13095
14. Sumner, JA, Kubzansky, LD, Roberts, AL, Gilsanz, P, Chen, Q, Winning, A, et al. Post-traumatic stress disorder symptoms and risk of hypertension over 22 years in a large cohort of younger and middle-aged women. Psychol Med. (2016) 46:3105–16. doi: 10.1017/S0033291716001914
15. Agyemang, C, Goosen, S, Anujuo, K, and Ogedegbe, G. Relationship between post-traumatic stress disorder and diabetes among 105 180 asylum seekers in the Netherlands. Eur J Pub Health. (2012) 22:658–62. doi: 10.1093/eurpub/ckr138
16. Trief, PM, Ouimette, P, Wade, M, Shanahan, P, and Weinstock, RS. Post-traumatic stress disorder and diabetes: co-morbidity and outcomes in a male veterans sample. J Behav Med. (2006) 29:411–8. doi: 10.1007/s10865-006-9067-2
17. Bah, AJ, James, PB, Bah, N, Sesay, AB, Sevalie, S, and Kanu, JS. Prevalence of anxiety, depression and post-traumatic stress disorder among Ebola survivors in northern Sierra Leone: a cross-sectional study. BMC Public Health. (2020) 20:1391. doi: 10.1186/s12889-020-09507-6
18. Cénat, JM, Felix, N, Blais-Rochette, C, Rousseau, C, Bukaka, J, Derivois, D, et al. Prevalence of mental health problems in populations affected by the Ebola virus disease: a systematic review and meta-analysis. Psychiatry Res. (2020) 289:113033. doi: 10.1016/j.psychres.2020.113033
19. Vyas, KJ, Delaney, EM, Webb-Murphy, JA, and Johnston, SL. Psychological impact of deploying in support of the U.S. response to Ebola: a systematic review and meta-analysis of past outbreaks. Mil Med. (2016) 181:e1515–31. doi: 10.7205/MILMED-D-15-00473
20. Alberque, B, Laporte, C, Mondillon, L, Baker, JS, Mermillod, M, Brousse, G, et al. Prevalence of post-traumatic stress disorder (PTSD) in healthcare workers following the first SARS-CoV epidemic of 2003: a systematic review and meta-analysis. Int J Environ Res Public Health. (2022) 19:13069. doi: 10.3390/ijerph192013069
21. Khan, S, Akbar, SMF, and Nishizono, A. Co-existence of a pandemic (SARS-CoV-2) and an epidemic (dengue virus) at some focal points in Southeast Asia: pathogenic importance, preparedness, and strategy of tackling. Lancet Reg Health Southeast Asia. (2022) 4:100046. doi: 10.1016/j.lansea.2022.100046
22. Tang, L, Pan, L, Yuan, L, and Zha, L. Prevalence and related factors of post-traumatic stress disorder among medical staff members exposed to H7N9 patients. Int J Nurs Sci. (2017) 4:63–7. doi: 10.1016/j.ijnss.2016.12.002
23. Elizarrarás-Rivas, J, Vargas-Mendoza, JE, Mayoral-García, M, Matadamas-Zarate, C, Elizarrarás-Cruz, A, Taylor, M, et al. Psychological response of family members of patients hospitalised for influenza a/H1N1 in Oaxaca, Mexico. BMC Psychiatry. (2010) 10:104. doi: 10.1186/1471-244X-10-104
24. American Psychiatric Association . (2022). "What is posttraumatic stress disorder (PTSD)?" Available at: https://www.psychiatry.org/patients-families/ptsd/what-is-ptsd (Accessed Nov 11, 2023).
25. Chudzicka-Czupała, A, Hapon, N, Chiang, S-K, Żywiołek-Szeja, M, Karamushka, L, Lee, CT, et al. Depression, anxiety and post-traumatic stress during the 2022 Russo-Ukrainian war, a comparison between populations in Poland, Ukraine, and Taiwan. Sci Rep. (2023) 13:3602. doi: 10.1038/s41598-023-28729-3
26. Guest, R, Tran, Y, Gopinath, B, Cameron, ID, and Craig, A. Prevalence and psychometric screening for the detection of major depressive disorder and post-traumatic stress disorder in adults injured in a motor vehicle crash who are engaged in compensation. BMC Psychol. (2018) 6:4. doi: 10.1186/s40359-018-0216-5
27. Kok, T, de Haan, HA, van der Meer, M, Najavits, LM, and De Jong, CAJ. Screening of current post-traumatic stress disorder in patients with substance use disorder using the depression, anxiety and stress scale (DASS-21): a reliable and convenient measure. Eur Addict Res. (2014) 21:71–7. doi: 10.1159/000365283
28. Li, X, Li, S, Xiang, M, Fang, Y, Qian, K, Jiawei, X, et al. The prevalence and risk factors of PTSD symptoms among medical assistance workers during the COVID-19 pandemic. J Psychosom Res. (2020) 139:110270. doi: 10.1016/j.jpsychores.2020.110270
29. Kaseda, ET, and Levine, AJ. Post-traumatic stress disorder: a differential diagnostic consideration for COVID-19 survivors. Clin Neuropsychol. (2020) 34:1498–514. doi: 10.1080/13854046.2020.1811894
30. Liu, CH, Erdei, C, and Mittal, L. Risk factors for depression, anxiety, and PTSD symptoms in perinatal women during the COVID-19 pandemic. Psychiatry Res. (2021) 295:113552. doi: 10.1016/j.psychres.2020.113552
31. Blekas, A, Voitsidis, P, Athanasiadou, M, Parlapani, E, Chatzigeorgiou, AF, Skoupra, M, et al. COVID-19: PTSD symptoms in Greek health care professionals. Psychol Trauma Theory Res Pract Policy. (2020) 12:812–9. doi: 10.1037/tra0000914
32. Carmassi, C, Foghi, C, Dell'Oste, V, Cordone, A, Bertelloni, CA, Bui, E, et al. PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: what can we expect after the COVID-19 pandemic. Psychiatry Res. (2020) 292:113312. doi: 10.1016/j.psychres.2020.113312
33. Sakib, N, Akter, T, Fatematuz Zohra, AKM, Bhuiyan, I, Mamun, MA, and Griffiths, MD. Fear of COVID-19 and depression: a comparative study among the general population and healthcare professionals during COVID-19 pandemic crisis in Bangladesh. Int J Ment Heal Addict. (2023) 21:976–92. doi: 10.1007/s11469-020-00477-9
34. Torales, J, O’Higgins, M, Castaldelli-Maia, JM, and Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int J Soc Psychiatry. (2020) 66:317–20. doi: 10.1177/0020764020915212
35. Haider, N, Hasan, MN, Guitian, J, Khan, RA, McCoy, D, Ntoumi, F, et al. The disproportionate case–fatality ratio of COVID-19 between countries with the highest vaccination rates and the rest of the world. IJID Reg. (2023) 6:159–66. doi: 10.1016/j.ijregi.2023.01.011
36. Haider, N, Yavlinsky, A, Chang, Y-M, Hasan, MN, Benfield, C, Osman, AY, et al. The Global Health security index and joint external evaluation score for health preparedness are not correlated with countries' COVID-19 detection response time and mortality outcome. Epidemiol Infect. (2020) 148:e210. doi: 10.1017/S0950268820002046
37. Hasan, MN, Haider, N, Stigler, FL, Khan, RA, McCoy, D, Zumla, A, et al. The global case-fatality rate of COVID-19 has been declining since may 2020. Am J Trop Med Hyg. (2021) 104:2176–84. doi: 10.4269/ajtmh.20-1496
38. Rahman, MM, Marzo, RR, Chowdhury, S, Qalati, SA, Hasan, MN, Paul, GK, et al. Knowledge, attitude and practices toward coronavirus disease (COVID-19) in southeast and South Asia: a mixed study design approach. Front Public Health. (2022) 10:875727. doi: 10.3389/fpubh.2022.875727
39. Islam, M, Aminul, SS, Al Marzan, A, Amin, MR, Hasan, MN, Nazmul Hoque, M, et al. Variant-specific deleterious mutations in the SARS-CoV-2 genome reveal immune responses and potentials for prophylactic vaccine development. Front Pharmacol. (2023) 14:1090717. doi: 10.3389/fphar.2023.1090717
40. Forte, G, Favieri, F, Tambelli, R, and Casagrande, M. COVID-19 pandemic in the Italian population: validation of a post-traumatic stress disorder questionnaire and prevalence of PTSD symptomatology. Int J Environ Res Public Health. (2020) 17:4151. doi: 10.3390/ijerph17114151
41. Liu, CH, Zhang, E, Wong, GTF, Hyun, S, and Hahm, HC. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: clinical implications for U.S. young adult mental health. Psychiatry Res. (2020) 290:113172. doi: 10.1016/j.psychres.2020.113172
42. Asnakew, S, Legas, G, Liyeh, TM, Belete, A, Haile, K, Yitbarek, GY, et al. Prevalence of post-traumatic stress disorder on health professionals in the era of COVID-19 pandemic, Northwest Ethiopia, 2020: a multi-centered cross-sectional study. PLoS One. (2021) 16:e0255340. doi: 10.1371/journal.pone.0255340
43. Carmassi, C, Dell’Oste, V, Bui, E, Foghi, C, Bertelloni, CA, Atti, AR, et al. The interplay between acute post-traumatic stress, depressive and anxiety symptoms on healthcare workers functioning during the COVID-19 emergency: A multicenter study comparing regions with increasing pandemic incidence. Journal of Affective Disorders. (2022) 298, 209–216. doi: 10.1016/j.jad.2021.10.128
44. Deltour, V, Poujol, A-L, and Laurent, A. Post-traumatic stress disorder among ICU healthcare professionals before and after the Covid-19 health crisis: a narrative review. Ann Intensive Care. (2023) 13:66. doi: 10.1186/s13613-023-01145-6
45. Sahebi, A, Yousefi, A, Abdi, K, Jamshidbeigi, Y, Moayedi, S, Torres, M, et al. The prevalence of post-traumatic stress disorder among health care workers during the COVID-19 pandemic: an umbrella review and meta-analysis. Front Psych. (2021) 12:764738. doi: 10.3389/fpsyt.2021.764738
46. Andhavarapu, S, Yardi, I, Bzhilyanskaya, V, Lurie, T, Bhinder, M, Patel, P, et al. Post-traumatic stress in healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. (2022) 317:114890. doi: 10.1016/j.psychres.2022.114890
47. Schein, J, Houle, C, Urganus, A, Cloutier, M, Patterson-Lomba, O, Wang, Y, et al. Prevalence of post-traumatic stress disorder in the United States: a systematic literature review. Curr Med Res Opin. (2021) 37:2151–61. doi: 10.1080/03007995.2021.1978417
48. Yang, Y, Liu, D, Liu, B, Weiyan, O, Wang, L, Ma, Y, et al. Prevalence of post-traumatic stress disorder status among healthcare workers and its impact on their mental health during the crisis of COVID-19: a cross-sectional study. Front Public Health. (2022) 10:904550. doi: 10.3389/fpubh.2022.904550
49. Dyer, O . Covid-19: Peru’s official death toll triples to become world’s highest. BMJ. (2021) 373:n1442. doi: 10.1136/bmj.n1442
50. Mas-Ubillus, G, Ortiz, PJ, Huaringa-Marcelo, J, Sarzo-Miranda, P, Muñoz-Aguirre, P, Diaz-Ramos, A, et al. High mortality among hospitalized adult patients with COVID-19 pneumonia in Peru: a single Centre retrospective cohort study. PLoS One. (2022) 17:e0265089. doi: 10.1371/journal.pone.0265089
51. Andrus, JK, Evans-Gilbert, T, Santos, JI, Guzman, MG, Rosenthal, PJ, Toscano, C, et al. Perspectives on battling COVID-19 in countries of Latin America and the Caribbean. Am J Trop Med Hyg. (2020) 103:593–6. doi: 10.4269/ajtmh.20-0571
52. Rodriguez-Morales, AJ, Gallego, V, Escalera-Antezana, JP, Méndez, CA, Zambrano, LI, Franco-Paredes, C, et al. COVID-19 in Latin America: the implications of the first confirmed case in Brazil. Travel Med Infect Dis. (2020) 35:101613. doi: 10.1016/j.tmaid.2020.101613
53. Sakellariou, D, Malfitano, APS, and Rotarou, ES. Disability inclusiveness of government responses to COVID-19 in South America: a framework analysis study. Int J Equity Health. (2020) 19:131. doi: 10.1186/s12939-020-01244-x
54. Carvalho, S, Coelho, CG, Kluwe-Schiavon, B, Magalhães, J, and Leite, J. The acute impact of the early stages of COVID-19 pandemic in people with pre-existing psychiatric disorders: a systematic review. Int J Environ Res Public Health. (2022) 19:5140. doi: 10.3390/ijerph19095140
55. Li, Y, Chen, B, Hong, Z, Sun, Q, Dai, Y, Basta, M, et al. Insomnia symptoms during the early and late stages of the COVID-19 pandemic in China: a systematic review and meta-analysis. Sleep Med. (2022) 91:262–72. doi: 10.1016/j.sleep.2021.09.014
56. Schmidt, SAJ, Lo, S, and Hollestein, LM. Research techniques made simple: sample size estimation and power calculation. J Investig Dermatol. (2018) 138:1678–82. doi: 10.1016/j.jid.2018.06.165
57. Iglesias-Osores, S, Acosta-Quiroz, J, Iglesias-Osores, S, and Acosta-Quiroz, J. Estrés postraumático en trabajadores de la salud y COVID-19. Arch Prev Riesgos Labor. (2020) 23:363–5. doi: 10.12961/aprl.2020.23.03.06
58. Connor, KM, and Davidson, JRT. SPRINT: a brief global assessment of post-traumatic stress disorder. Int Clin Psychopharmacol. (2001) 16:279–84. doi: 10.1097/00004850-200109000-00005
59. Bianchi, L, Cristian, M, and Cuadra, IG. Validación de la escala breve para diagnosticar estrés post-traumático (SPRINT-E) en una muestra de personas afectadas por el terremoto y tsunami del 27-F en Chile. An Psychol. (2013) 29:328–34. doi: 10.6018/analesps.29.2.130681
60. Gloster, AT, Rhoades, HM, Novy, D, Klotsche, J, Senior, A, Kunik, M, et al. Psychometric properties of the depression anxiety and stress Scale-21 in older primary care patients. J Affect Disord. (2008) 110:248–59. doi: 10.1016/j.jad.2008.01.023
61. Rogers, JP, Chesney, E, Oliver, D, Pollak, TA, McGuire, P, Fusar-Poli, P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:611–27. doi: 10.1016/S2215-0366(20)30203-0
62. Lazzerini, M, and Putoto, G. COVID-19 in Italy: momentous decisions and many uncertainties. Lancet Glob Health. (2020) 8:e641–2. doi: 10.1016/S2214-109X(20)30110-8
63. Liu, N, Zhang, F, Wei, C, Jia, Y, Shang, Z, Sun, L, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. (2020) 287:112921. doi: 10.1016/j.psychres.2020.112921
64. Ramírez, G, Patricia, L, Arriaga, RJM, Hernández-Gonzalez, MA, and De la Roca-Chiapas, JM. Psychological distress and signs of post-traumatic stress in response to the COVID-19 health emergency in a Mexican sample. Psychol Res Behav Manag. (2020) 13:589–97. doi: 10.2147/PRBM.S259563
65. Wang, C, Pan, R, Wan, X, Tan, Y, Linkang, X, Ho, CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
66. Martínez Pizarro, S . Síndrome del cuidador quemado. Revista Clínica de Medicina de Familia. (2020) 13:97–100.
67. Lorente-Acosta, M . Violencia de género en tiempos de pandemia y confinamiento. Rev Esp Med Leg. (2020) 46:139–45. doi: 10.1016/j.reml.2020.05.005
68. Lloyd-Sherlock, P, Ebrahim, S, Geffen, L, and McKee, M. Bearing the brunt of covid-19: older people in low and middle income countries. BMJ. (2020) 368:m1052. doi: 10.1136/bmj.m1052
69. Mejia, CR, Rodriguez-Alarcon, JF, Garay-Rios, L, Enriquez-Anco, MD, Moreno, A, Huaytan-Rojas, K, et al. Percepción de miedo o exageración que transmiten los medios de comunicación en la población peruana durante la pandemia de la COVID-19. Rev Cuba Investig Bioméd. (2020) 39:698.
70. Cai, X, Xiaopeng, H, Ekumi, IO, Wang, J, An, Y, Li, Z, et al. Psychological distress and its correlates among COVID-19 survivors during early convalescence across age groups. Am J Geriatr Psychiatry. (2020) 28:1030–9. doi: 10.1016/j.jagp.2020.07.003
71. Liang, L, Ren, H, Cao, R, Yueyang, H, Qin, Z, Li, C, et al. The effect of COVID-19 on youth mental health. Psychiatry Q. (2020) 91:841–52. doi: 10.1007/s11126-020-09744-3
72. Rossi, R, Socci, V, Talevi, D, Mensi, S, Niolu, C, Pacitti, F, et al. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front Psych. (2020) 11:790. doi: 10.3389/fpsyt.2020.00790
73. González-Sanguino, C, Ausín, B, Castellanos, MÁ, Saiz, J, López-Gómez, A, Ugidos, C, et al. Mental health consequences during the initial stage of the 2020 coronavirus pandemic (COVID-19) in Spain. Brain Behav Immun. (2020) 87:172–6. doi: 10.1016/j.bbi.2020.05.040
74. Pieh, C, O’Rourke, T, Budimir, S, and Probst, T. Relationship quality and mental health during COVID-19 lockdown. PLoS One. (2020) 15:e0238906. doi: 10.1371/journal.pone.0238906
75. Serrano-Ripoll, MJ, Meneses-Echavez, JF, Ricci-Cabello, I, Fraile-Navarro, D, Fiol-deRoque, MA, Pastor-Moreno, G, et al. Impact of viral epidemic outbreaks on mental health of healthcare workers: a rapid systematic review and meta-analysis. J Affect Disord. (2020) 277:347–57. doi: 10.1016/j.jad.2020.08.034
76. Quintana Díaz, H, and Lozano Lesmes, L. Estrés y ansiedad como respuestas a la cuarentena en época de coronavirus. Rev Neuronum. (2020) 6:442–52.
77. Lozano-Vargas, A . Impacto de la epidemia del Coronavirus (COVID-19) en la salud mental del personal de salud y en la población general de China. Rev Neuropsiquiatr. (2020) 83:51–6. doi: 10.20453/rnp.v83i1.3687
78. Grech, P, and Grech, R. COVID-19 in Malta: the mental health impact. Psychol Trauma Theory Res Pract Policy. (2020) 12:534–5. doi: 10.1037/tra0000925
79. Ibanez, A, Santamaria-Garcia, H, Barragan, AG, Kornhuber, A, Ton, AMM, Slachevsky, A, et al. The impact of SARS-CoV-2 in dementia across Latin America: a call for an urgent regional plan and coordinated response. Alzheimers Dement. (2020) 6:e12092. doi: 10.1002/trc2.12092
80. Llibre-Guerra, JJ, Jiménez-Velázquez, IZ, Llibre-Rodriguez, JJ, and Acosta, D. The impact of COVID-19 on mental health in the Hispanic Caribbean region. Int Psychogeriatr. (2020) 32:1143–6. doi: 10.1017/S1041610220000848
81. Marazziti, D, Pozza, A, Di Giuseppe, M, and Conversano, C. The psychosocial impact of COVID-19 pandemic in Italy: a lesson for mental health prevention in the first severely hit European country. Psychol Trauma Theory Res Pract Policy. (2020) 12:531–3. doi: 10.1037/tra0000687
82. Mukhtar, S . Pakistanis’ mental health during the COVID-19. Asian J Psychiatr. (2020) 51:102127. doi: 10.1016/j.ajp.2020.102127
83. Tandon, R . COVID-19 and mental health: preserving humanity, maintaining sanity, and promoting health. Asian J Psychiatr. (2020) 51:102256. doi: 10.1016/j.ajp.2020.102256
84. Thome, J, Deloyer, J, Coogan, AN, Bailey-Rodriguez, D, da Cruz e Silva, OAB, Faltraco, F, et al. The impact of the early phase of the COVID-19 pandemic on mental-health services in Europe. World J Biol Psychiatry. (2021) 22:516–25. doi: 10.1080/15622975.2020.1844290
85. American Psychological Association . (2023). "COVID-19 information and resources." Available at: https://www.apa.org/topics/covid-19 (Accessed Nov 11, 2023).
86. Soklaridis, S, Lin, E, Lalani, Y, Rodak, T, and Sockalingam, S. Mental health interventions and supports during COVID-19 and other medical pandemics: a rapid systematic review of the evidence. Gen Hosp Psychiatry. (2020) 66:133–46. doi: 10.1016/j.genhosppsych.2020.08.007
87. Saladino, V, Auriemma, V, and Campinoti, V. Healthcare professionals, post-traumatic stress disorder, and COVID-19: a review of the literature. Front Psych. (2022) 12:795221. doi: 10.3389/fpsyt.2021.795221
88. Forrester, A, Aboaja, A, Beigel, L, Mundt, AP, Rivera, G, and Torales, J. Mental health in prisons in Latin America: the effects of COVID-19. Med Sci Law. (2023) 63:89–92. doi: 10.1177/00258024221149932
89. González-Ortiz, M, Castro, P, Vergara-Barra, P, Huerta, P, and Escudero, C. COVID-19 on pregnancy outcomes, mental health and placenta: focus in Latin America In: M Gonzalez-Ortiz , editor. Advances in maternal-fetal biomedicine: cellular and molecular mechanisms of pregnancy pathologies. Cham: Springer International Publishing (2023). 269–85.
90. de Miranda, KG, Rodrigues da Silva, IC, Fonseca, RMAM, and Gallassi, AD. Effects of working in vulnerable contexts on the mental health of primary healthcare professionals during the COVID-19 pandemic: a mixed-methods study. BMJ Open. (2023) 13:e073472. doi: 10.1136/bmjopen-2023-073472
91. Moya-Salazar, J, Jaime-Quispe, A, Cañari, B, Moya-Espinoza, JG, and Contreras-Pulache, H. A systematic review of mental health in rural Andean populations in Latin America during the COVID-19 pandemic. Front Psych. (2023) 14:1136328. doi: 10.3389/fpsyt.2023.1136328
92. Collins, RA, Herman, T, Snyder, RA, Haines, KL, Stey, A, Arora, TK, et al. Unspoken truths: mental health among academic surgeons. Ann Surg. (2023). doi: 10.1097/SLA.0000000000006159
93. Shaff, J, O'Keefe, VM, Atkin, AL, Wang, X, and Wilcox, HC. Examining the unique impacts of potentially traumatic experiences (PTE) and discrimination events on post-traumatic stress disorder (PTSD) and suicidal thoughts and behaviors among multiracial/ethnic adults in the United States. J Affect Disord. (2024) 347:51–6. doi: 10.1016/j.jad.2023.11.035
Keywords: COVID-19, Latin America, mental health, Peru, post-traumatic stress disorder, PTSD
Citation: Mejia CR, Serna-Alarcón V, Vilela-Estrada MA, Armada J, Ubillus M, Beraún-Barrantes J, Álvarez-Risco A, Del-Aguila-Arcentales S, Davies NM and Yáñez JA (2024) Prevalence of post-traumatic stress disorder risk post-COVID-19 in 12 countries in Latin America: a cross-sectional survey. Front. Public Health. 11:1302694. doi: 10.3389/fpubh.2023.1302694
Edited by:
Samer El Hayek, Erada Center for Treatment and Rehab, United Arab EmiratesReviewed by:
Mohammad Nayeem Hasan, Shahjalal University of Science and Technology, BangladeshAnna Maria Cybulska, Pomeranian Medical University in Szczecin, Poland
Copyright © 2024 Mejia, Serna-Alarcón, Vilela-Estrada, Armada, Ubillus, Beraún-Barrantes, Álvarez-Risco, Del-Aguila-Arcentales, Davies and Yáñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aldo Álvarez-Risco, YzI3NDA4QHV0cC5lZHUucGU=