 Amanda N. Gesselman1*
Amanda N. Gesselman1* Ellen M. Kaufman1
Ellen M. Kaufman1 Lee Y. S. Weeks1,2Zoe Moscovici1,2Margaret Bennett-Brown1,3
Lee Y. S. Weeks1,2Zoe Moscovici1,2Margaret Bennett-Brown1,3 Olivia R. Adams1,4
Olivia R. Adams1,4 Jessica T. Campbell1Malia Piazza1,5Lucy Bhuyan1,6Simon Dubé1,7Jessica J. Hille1
Jessica T. Campbell1Malia Piazza1,5Lucy Bhuyan1,6Simon Dubé1,7Jessica J. Hille1 Justin R. Garcia1,2
Justin R. Garcia1,2- 1Kinsey Institute, Indiana University Bloomington, Bloomington, IN, United States
- 2Department of Gender Studies, College of Arts and Sciences, Indiana University Bloomington, Bloomington, IN, United States
- 3Communication Studies, College of Media and Communications, Texas Tech University, Lubbock, TX, United States
- 4Department of Gender, Sexuality, and Women’s Studies, College of Liberal Arts and Sciences, University of Florida, Gainesville, FL, United States
- 5Department of Anthropology, College of Arts and Sciences, Indiana University Bloomington, Bloomington, IN, United States
- 6Department of Counseling and Educational Psychology, School of Education, Indiana University Bloomington, Bloomington, IN, United States
- 7Department of Psychology, Faculty of Arts and Science, Concordia University, Montreal, QC, Canada
Objective: The objective of this study is to examine mental health treatment utilization and interest among the large and growing demographic of single adults in the United States, who face unique societal stressors and pressures that may contribute to their heightened need for mental healthcare.
Method: We analyzed data from 3,453 single adults, focusing on those with possible mental health treatment needs by excluding those with positive self-assessments. We assessed prevalence and sociodemographic correlates of mental health treatment, including psychotherapy and psychiatric medication use, and interest in attending psychotherapy among participants who had never attended.
Results: 26% were in mental health treatment; 17% were attending psychotherapy, 16% were taking psychiatric medications, and 7% were doing both. Further, 64% had never attended psychotherapy, of which 35% expressed interest in future attendance. There were differences in current psychotherapy attendance and psychiatric medication use by gender and sexual orientation, with women and gay/lesbian individuals more likely to engage in both forms of mental health treatment. Additionally, interest in future psychotherapy among those who had never attended varied significantly by age, gender, and race. Younger individuals, women, and Black/African-American participants showed higher likelihoods of interest in psychotherapy.
Conclusion: Our research highlights a critical gap in mental health treatment utilization among single adults who may be experiencing a need for those services. Despite a seemingly higher likelihood of engagement in mental health treatment compared to the general population, only a minority of single adults in our sample were utilizing mental health treatment. This underutilization and the observed demographic disparities in mental health treatment underscore the need for targeted outreach, personalized treatment plans, enhanced provider training, and policy advocacy to ensure equitable access to mental healthcare for single adults across sociodemographic backgrounds.
Introduction
In recent years, the demographic landscape of the United States has witnessed a significant shift towards increased rates of singlehood (i.e., being romantically unpartnered), with a growing proportion of adults choosing to remain single or experiencing single life due to various circumstances (1–5). As a group, single adults face distinct social, psychological, and economic challenges, compared to romantically partnered adults. Single adults often navigate a complex social environment that prioritizes romantic relationships and their resulting familial relationships as indicators of personal success and happiness (6–8). As a result, single adults face societal stigma and pressures that can contribute to feelings of isolation, loneliness, and perceived inadequacy (9, 10). Further, singlehood introduces a set of unique stressors and life situations that may not be as prevalent among partnered individuals. These include making financial and living arrangements independently, providing extensive care to ill or aging family members, and managing one’s own physical health within a healthcare system that restricts in-person support to individuals who are legally or biologically related (4, 11). Particularly among those who are involuntarily single, singlehood may also prevent fulfillment of certain personal goals throughout the lifecycle (e.g., parenthood; long-term romantic companionship), exacerbating the negative mental health impact produced by other individual and societal factors unique to this population (12, 13). Taken together, these experiences could lead to a heightened need for mental health treatment among single adults.
Social causation theory (14, 15) offers a valuable lens through which to understand the increased need for mental health treatment among single adults. This theory suggests that social factors cause or worsen mental health issues. For example, investigations informed by this theory have shown that the stress and environmental adversity associated with having a low socioeconomic status contribute to higher probabilities for developing anxiety, depression, or other psychiatric disorders (16, 17). Reframed in the context of single adults, social causation theory might suggest that factors such as the presence or absence of supportive social relationships, societal expectations and pressures, and stigma associated with being single could evoke or exacerbate mental health issues. Considering that one-third of the adult population in the United States is currently single and that this population appears to be growing (2), it is important to understand how single adults utilize mental health treatment resources. Examining current uptake within single adults, and pinpointing demographic subgroups of single adults less likely to seek out resources when in need, is crucial for understanding how social structures and societal norms impact individual well-being.
Mental health disorders (e.g., anxiety, depression) affect millions worldwide, with rates rising in recent years, and further intensified by the COVID-19 pandemic (18–22). Mental health issues can severely impact personal, economic, and social well-being [(e.g., 23–25)], which are known to further exacerbate existing mental health difficulties (26). In the U.S., mental health treatment primarily consists of psychotherapy and/or prescribed psychiatric medications (27, 28). Psychotherapy involves talking with a trained therapist, with techniques ranging from cognitive-behavioral to psychodynamic approaches (29, 30). Psychiatric medications, like antidepressants and anxiolytics, alter neurotransmitter activity to address mental health issues (31, 32). Despite the need for mental health treatment, reports suggest that treatment may be underutilized (33–38).
Largescale reports of mental health treatment utilization in the United States are sparse. However, the U.S. Centers for Disease Control (CDC) reports that around one in five American adults receive mental health treatment annually, with prescription psychiatric medication use more common than psychotherapy (32). According to their study, 17% of U.S. adults were receiving mental health treatment in the form of prescription psychiatric medication while 10% of U.S. adults were receiving psychotherapy/counseling (32). It should be noted that Terlizzi and Norris’ (32) study did not account for participants’ need for mental health treatment. Instead, results are derived from a nationally representative household survey of adults in the U.S., which may have included many adults without a need for these services. As such, it is difficult to accurately estimate the percentage of U.S. adults who should be seeking mental health treatment. However, studies conducted in other countries suggest that adults in the U.S. are underutilizing mental healthcare. While mental health treatment utilization was between 10 and 17% for U.S. adults (32), other countries reported that between 32 and 71% of the adult population had accessed mental health treatment (39–41). Further national studies are crucial to understand U.S. adults’ need for mental health treatment and pursuit of those services.
In the current study, we focus on single adults with self-reported suboptimal mental health—excluding those with higher self-assessments—to investigate their uptake or interest in mental health treatment. Singles are a heterogeneous group, however; to avoid viewing this group monolithically, it is important to investigate how demographic factors aligning with different identities and/or lived experiences contribute to their uptake and interest in mental health treatment. In particular, research conducted in the U.S. and elsewhere has shown that factors like gender, age, socioeconomic status, and race influence mental health treatment-seeking behavior. Women are more likely to be receiving mental health treatment compared to men (32, 42–44). This gender effect between men and women has been found consistently across sampled countries, but no further investigations into gender identity and mental health treatment-seeking are found in the literature. In particular, while gender identity is clearly impactful on treatment-seeking, only studies conducted with adolescent participants have examined differences in mental health treatment as a function of transgender or cisgender identities (45). We do know, however, that transgender and genderqueer individuals are exposed to more societal and structural risks that increase their need for mental health services (46). This disparity in exposure to risks is a reflection of “minority stress”—high levels of stress endured by members of stigmatized minority groups—a factor that exacerbates challenges to mental health for many people, including those with minoritized gender, racial/ethnic, and sexual orientation identities (47–50).
With regards to age, most studies have found that younger people are more likely than older people to be in psychotherapy (32, 43, 44), although Terlizzi and Norris’ (32) sample of U.S. adults found a reversed pattern of results for psychiatric medication use—older age was associated with more use. Further, there appears to be a robust effect for socioeconomic standing, but with a different direction of effect depending on country and type of mental health treatment assessed. In Brazil and Finland, higher education level and occupational status were associated with seeking mental health treatment [(42, 43); but see Suokas et al. (51)]. Conversely, in Spain, people with lower education and income levels were more likely to seek mental health treatment (44). There are no known studies examining the association between income and mental health treatment utilization in a U.S. sample. However, in line with social causation theory, lower income levels are associated with higher prevalence of mental illness in the U.S. (52). Reflecting the systemic bias inherent in the U.S.’s societal hierarchy, people with minoritized identities or demographic backgrounds often have the lowest income (53). Taken together, these findings would suggest that people engaged in mental health treatment are more likely to have lower income and to hold a minority identity. However, in their CDC study, Terlizzi and Norris (32) found that people who identified their race/ethnicity as non-Hispanic white—a majoritized identity—were more likely to have received mental health treatment than Hispanic, non-Hispanic Black, and non-Hispanic Asian adults. Further research is needed to understand how mental health treatment uptake and interest varies by income and race in U.S adults.
Amassed, the small existing literature suggests that within a population of single adults who may need mental health treatment, mental health treatment uptake and interest is more likely for people who identify as women (vs. men); younger in age (vs. older); potentially white, non-Hispanic (vs. other races/ethnicities); and potentially higher (vs. lower) in income. In addition to these, there are a few key demographic factors that have not yet been investigated but may drive differences in mental health treatment utilization and interest. For example, research indicates that non-heterosexual (e.g., gay or lesbian, queer) individuals are exposed to a multitude of societal and structural risks that predispose them to a greater need for mental health services (54–56), yet there’s insufficient exploration into how these pressures translate into actual mental health treatment engagement compared to heterosexual individuals. Further, because this investigation takes place in the single adult population, it is important to assess the impact of single parenthood on mental health treatment. In addition to increased stress, parenthood evokes hormonal changes, interpersonal stress, and sleep disturbances that may subsequently challenge mental well-being (57–61). Single parents might experience these challenges more acutely than partnered parents, as a result of the added responsibilities and limited support (62, 63). In the current study, we investigate differences in mental health treatment uptake and interest by age, gender, income, and race, as prior studies have done. Further, we undertake the first known investigation into differences in mental health treatment uptake and interest by sexual orientation and parenthood.
In the current study, we conducted a secondary data analysis on an existing national dataset of single adults in the United States. Selecting only those who self-rated their mental health over the last year as “poor,” “fair,” or “good”—and omitting those who self-rated their mental health as “very good” or “excellent”—we examined engagement and interest in mental health treatment among 3,453 single adults to answer the following research questions. Among single adults who may need mental health treatment:
1. How many were undergoing mental health treatment at time of survey? We examined mental health treatment in the form of attending psychotherapy/counseling, using psychiatric medications, or both.
2. What sociodemographic characteristics of singles are associated with undergoing mental health treatment (i.e., psychotherapy/counseling, psychiatric medication use, or both)?
3. Of those who had never attended psychotherapy, how many were interested in attending psychotherapy in the future, and what sociodemographic characteristics are most associated with interest?
Methods
Below we report how we determined our sample size, all data exclusions, and all measures used in the current study. This study did not employ manipulations.
Participants
The initial sample included 5,001 single adults. We restricted the sample to only those who reported their mental health as “poor,” “fair,” or “good” on a 5-point Likert scale ranging from poor (1) to excellent (5). Participants who rated their mental health as “very good” (n = 1,012) or “excellent” (n = 536) were removed from the sample. We report descriptive statistics below for mental health treatment utilization and interest among a sample of 3,453 single adults (see Table 1 for demographic distributions). However, further sample restrictions were required before we could investigate comparisons by gender, sexual orientation, or race/ethnicity, resulting in an analytic sample of 2,902 participants; see the Data Analysis Plan section below for details.
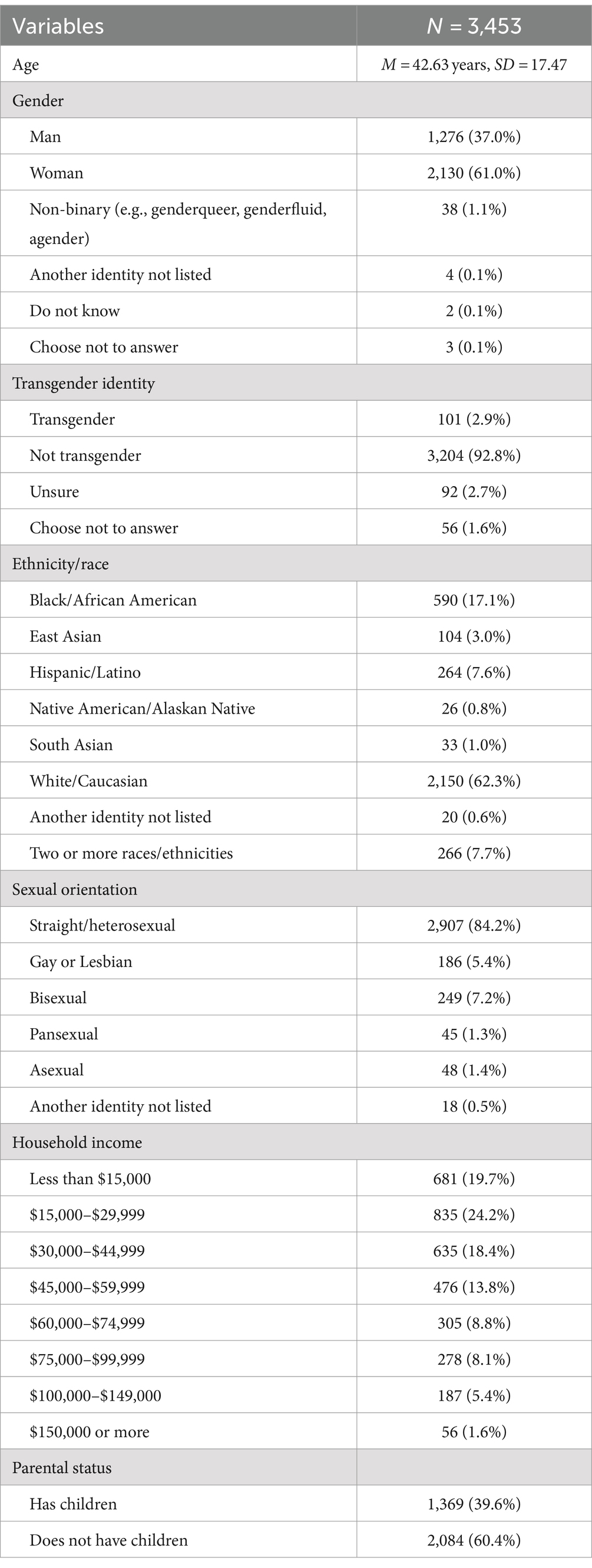
Table 1. Demographic distributions for the sample of participants who may need mental health treatment.
Procedure
Data were collected as part of the annual Singles in America (SIA) study. The current study was conducted as a secondary data analysis of de-identified market research data collected by an outside party. The authors of this manuscript have not interacted with participants and have access only to a de-identified dataset. Based on the nature of these secondary analyses of anonymized data, the current research is exempt from the federal regulations at 45 CFR part 46 (64). Participants must have been at least 18 years old, fluent in English, and single (i.e., romantically unpartnered). Singlehood was defined for participants as being unmarried and not in a committed romantic relationship. There were no requirements for the length of singlehood. Participants were recruited by Dynata (Dallas, TX, United States), using independent opt-in Internet research panels for quota-based cross-sectional surveying. Panelists were drawn from a diverse pool of participants who have been recruited over several years from many venues, including paper and electronic mailings and internet recruitment. Recruitment was balanced in real-time so that demographic distributions (i.e., age, gender, ethnicity, region, income) in the sample were closely aligned with demographic distributions published in the most recent Current Population Survey conducted by the U.S. Bureau of the Census.
Participants received a recruitment message from Dynata inviting participation for financial remuneration (~$5 USD). Panelists were screened to ensure survey engagement, with those straight-lining responses or moving too quickly through panels removed. Participants completed the full survey; there is no missing data due to participants opting to skip questions. All data were collected over the Internet. SIA is sponsored by the relationship company Match; however, participants were not recruited or drawn from the Match population or subsidiary sites. No a priori power analyses were conducted; the Singles in America survey aims to collect a sample of 5,000 respondents yearly. This study was not pre-registered.
Measures
Demographics
Participants reported their age, gender and transgender identity, income, parenting status, sexual orientation (straight/heterosexual; gay/lesbian; bisexual; other), and race/ethnicity (White; Black/African-American; Hispanic/Latino; South Asian; East Asian; North American Indian/Alaska Native/Pacific Islander; other). Measures of gender were based on Haupert et al. (65) for inclusive measurement. First, participants selected gender identity from this list: man, woman, non-binary (e.g., genderqueer, genderfluid), agender, another identity not listed, do not know, choose not to answer. Next, they answered, “‘Transgender’ describes people whose gender identity or expression is different, at least part of the time, from the sex assigned to them at birth. Do you consider yourself to be transgender?” with one of the following options: yes, no, do not know, and choose not to answer. Regarding race/ethnicity, note that participants were allowed to select all identities that applied; however, for analytic purposes, we recoded participants who identified with multiple racial/ethnic identities into their own category.
Self-reported mental health
Participants responded to the following question, “How would you rate your average mental health over the last year?” Responses were, “poor” (1), “fair” (2), “good” (3), “very good” (4), and “excellent” (5). Note that this question was used to restrict the final analytic sample, such that participants who selected “very good” or “excellent” were removed.
Mental health treatment
Participants responded to a question assessing broader medication use: “Are you currently taking/using any of the following? Select all that apply.” The list included 15 options (e.g., hormonal birth control, testosterone, prescription painkillers). Of note, the list included four options relevant to mental health treatment. These were, “SSRI (e.g., Lexapro, Prozac, Zoloft)”; “SNRI (e.g., Pristiq, Cymbalta, Effexor)”; “MAOI (e.g., Marplan, Nardil)”; and “Wellbutrin.”
Participants also responded to: “Have you been in therapy, counseling, or some form of mental healthcare in the last 3 years?” Response options were Yes, currently; Yes, in the past but not now; No, but I’m interested in seeking therapy/treatment; and No, and I’m not interested in seeking therapy/treatment.
Data analysis plan
Within the sample of participants who may need mental health treatment (i.e., who rated their mental health as poor, fair, or good), we first examined descriptive statistics for demographics and mental health treatment variables. Next, we conducted three binary logistic regressions. However, due to cell size restrictions, a number of adjustments were made prior to regression modeling. First, we recoded the gender and transgender identity variables. People who did not identify as a man or woman (n = 47), or did not select “yes” or “no” for the transgender identity question (n = 138), were removed from the analytic sample. Second, we restricted the analyses to compare participants who identified their race/ethnicity as white, Black/African-American, or Hispanic/Latino. Due to small cell sizes—and particularly due to low engagement with either form of mental health treatment or interest in psychotherapy—we could not analytically compare mental health treatment engagement or interest for East or South Asian participants (n = 33 and 104, respectively), Native American or Alaskan Native participants (n = 26), participants who identified as another race or ethnicity not listed (n = 20), or participants who identified as two or more races/ethnicities (n = 266). Likewise, we could not compare mental health treatment or interest for people identifying their sexual orientation as pansexual (n = 45), asexual (n = 48), or another orientation not listed (n = 18); instead, we compare participants identifying their sexual orientation as heterosexual, gay/lesbian, and bisexual. Finally, we did not have adequate statistical power to compare transgender and cisgender participants, as only 101 participants identified as transgender. However, we did not remove these individuals from the sample unless they specified their gender as being an identity other than man or woman.
The final analytic sample for demographic comparisons in regression models was 2,902 single adults. In the regression models, the dependent variables were whether participants were attending psychotherapy (model 1), whether they were taking psychiatric medications (model 2), and among participants who had not been in psychotherapy, whether they were interested in psychotherapy in the future (model 3; all 0 = no, 1 = yes). Predictor variables were: age (mean-centered); income; gender (0 = men, 1 = women; in regression models, men served as the comparison group); two sexual orientation dummy codes (0 = heterosexual, 1 = gay/lesbian, bisexual; in regression models, heterosexual served as the comparison group); parent status (0 = does not have children, 1 = has children); and two dummy codes for race/ethnicity (0 = White, 1 = Black/African-American, Hispanic/Latino, White served as comparison). Because these analyses include multiple comparisons of the same individuals, we implemented a Bonferroni correction. Only effects reaching significance at p ≤ 0.001 are interpreted below. All data and analytic codes can be found at https://osf.io/zh3kd/?view_only=725060e1f96546f5ad5acdf9c5881aab.
Results
Prevalence of singles in mental health treatment
Within the sample of participants who may need mental health treatment, 26.2% (n = 902) of the sample were in mental health treatment at the time of the survey (i.e., psychotherapy or psychiatric medication use): 16.5% were in psychotherapy, 16.3% were taking psychiatric medications, and 6.7% were doing both. Additionally, 19.1% had attended psychotherapy previously but not currently. In total, 35.6% of the sample had experience with psychotherapy; 64.4% had not been in psychotherapy before, of which 35.4% were interested in attending psychotherapy in the future.
Sociodemographic associations with current mental health treatment
We examined associations between age, income, gender, race, sexual orientation, and parental status with attending psychotherapy, taking psychiatric medications, and interest in pursuing psychotherapy. We report percentages of engagement and interest in mental health treatment by demographics in Table 2 (psychotherapy attendance) and Table 3 (psychiatric medication use). Regression coefficients can be found in Tables 4–6.
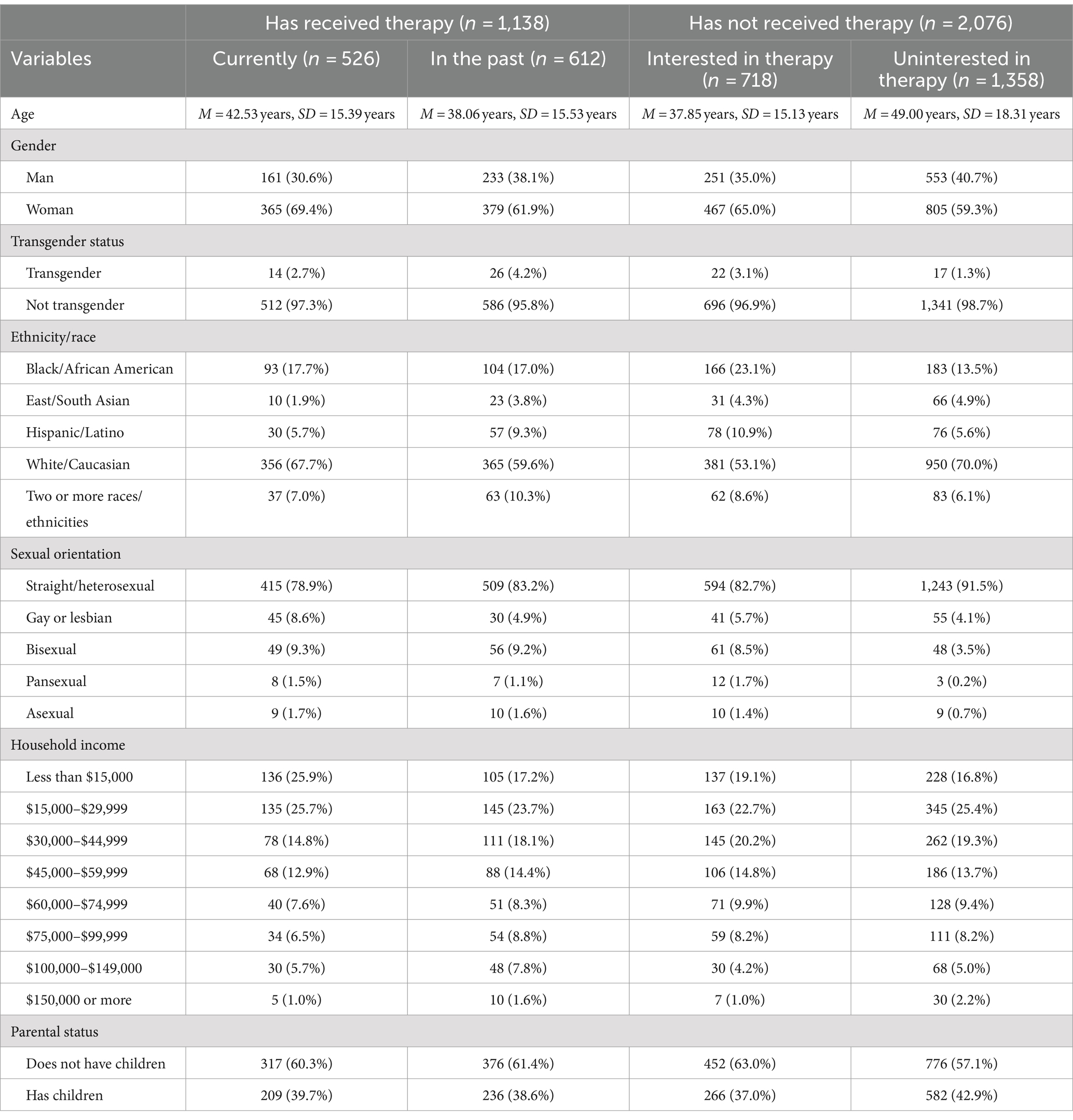
Table 2. Sample demographics by therapy attendance and interest in pursuing therapy.
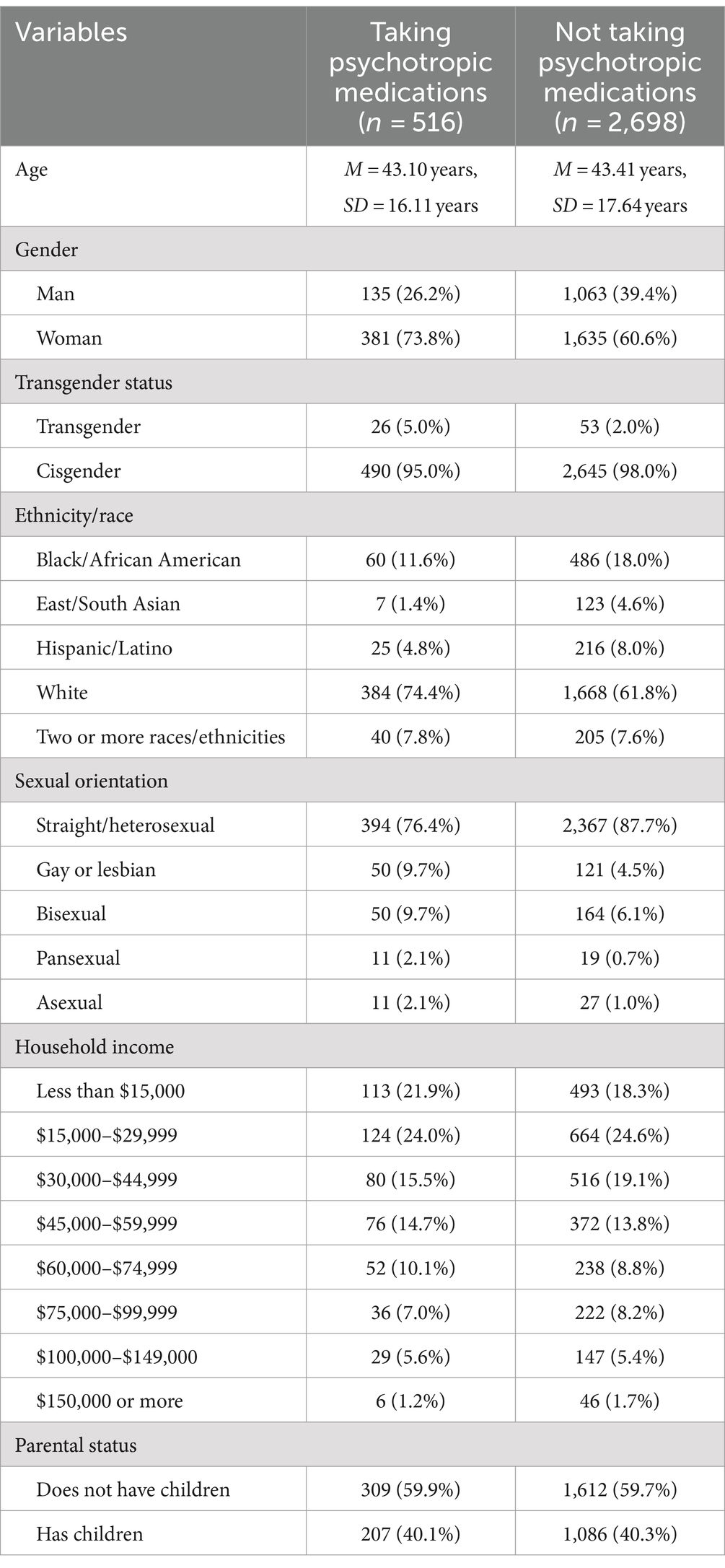
Table 3. Sample demographics for participants who were and were not taking psychiatric medications.
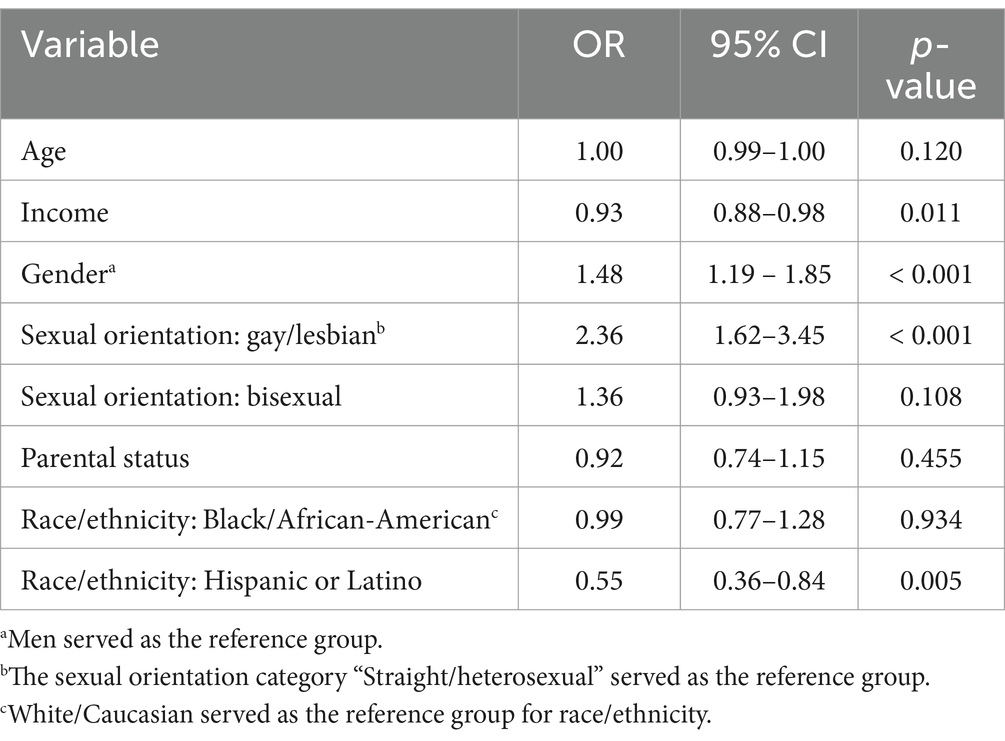
Table 4. Demographic characteristics predicting current psychotherapy attendance.
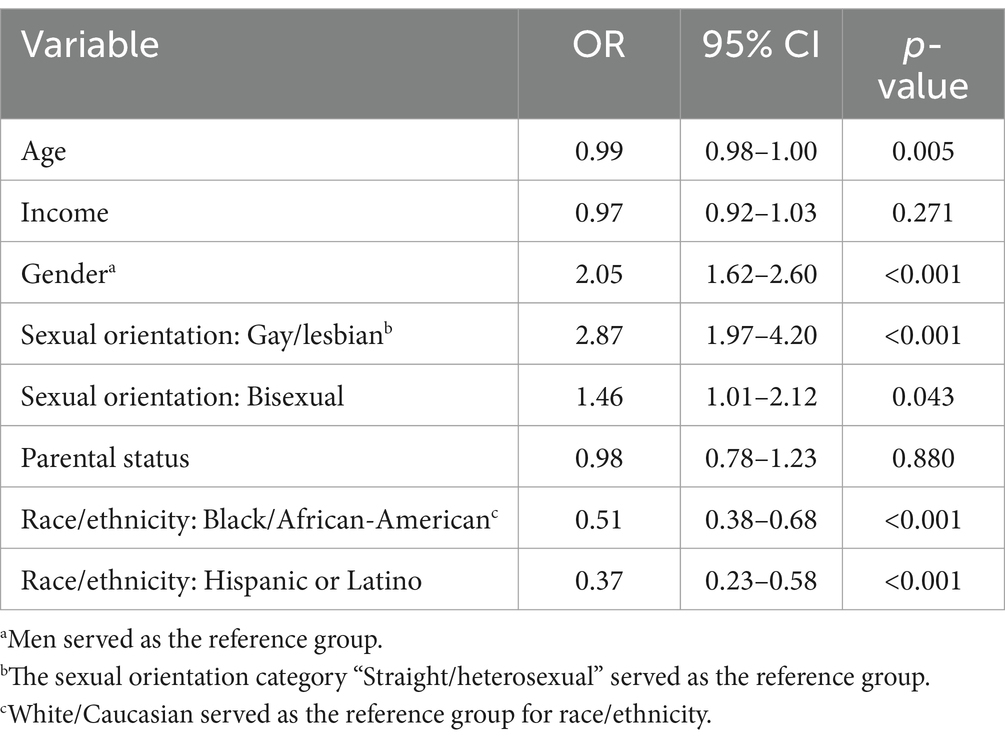
Table 5. Demographic characteristics predicting psychiatric medication use.
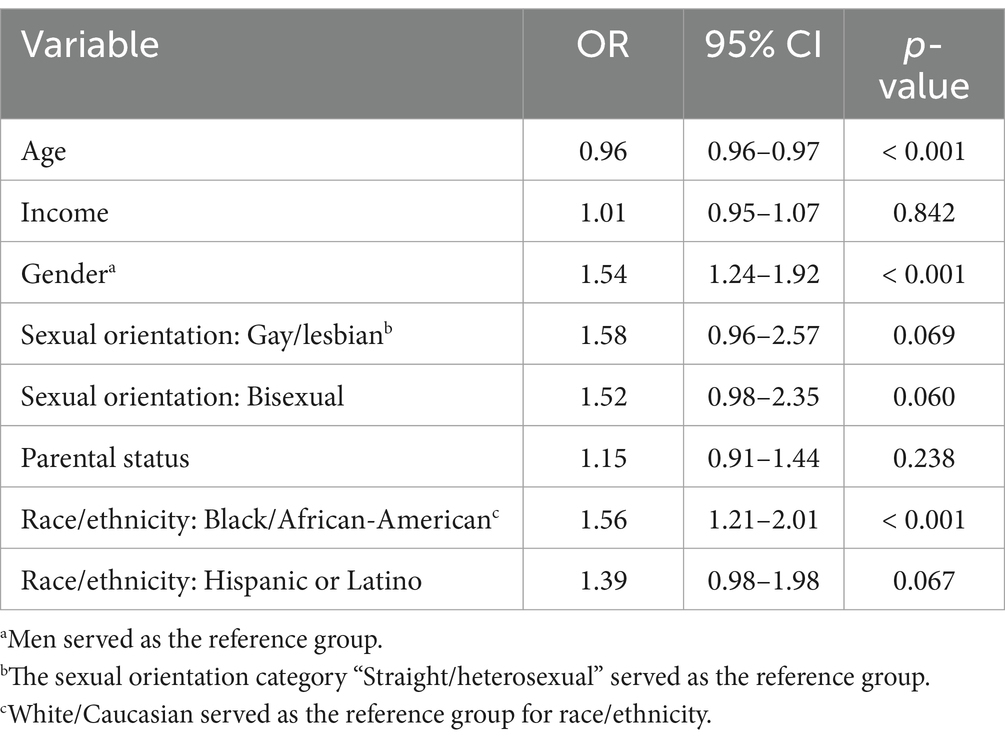
Table 6. Demographic characteristics predicting interest in future psychotherapy attendance, among those who had never attended psychotherapy.
Current psychotherapy attendance
In the regression model, there were significant differences in current psychotherapy attendance by gender and sexual orientation. Results suggest that women are more likely than men, and gay/lesbian individuals are more likely than heterosexual individuals, to be currently engaged in psychotherapy. Age, income, parenthood, and race/ethnicity were not significant predictors of psychotherapy attendance at p ≤ 0.001. See Table 4 for regression coefficients.
Current psychiatric medication use
There were significant differences in the odds of currently using psychiatric medication use by gender, sexual orientation, and race. Results suggest that women are more likely than men, gay/lesbian individuals are more likely than heterosexual individuals, and both Black/African-American and Hispanic/Latino individuals are more likely than white individuals to be currently taking psychiatric medications. Age, income, and parenthood were not significant predictors of psychotherapy attendance at p ≤ 0.001. See Table 5 for regression coefficients.
Interest in attending psychotherapy in the future
Among the subgroup of participants who had never attended psychotherapy, there were significant differences in the odds of being interested in future psychotherapy attendance by age, gender, and race. Results suggest that younger participants are more likely than older participants, women are more likely than men, and Black/African-American participants are more likely than white participants to be interested in attending psychotherapy in the future. Income, sexual orientation, and parenthood were not significant predictors of psychotherapy attendance at p ≤ 0.001. See Table 6 for regression coefficients.
Discussion
Single adults face a variety of unique societal stressors, including social stigma, a lack of systemic support, and increased financial and social obligations compared to partnered peers (4). These experiences may produce negative mental health outcomes throughout the lifespan, subsequently producing a need for mental health treatment (9, 10). In our study, we estimated mental health treatment rates among single American adults, who comprise around one-third of the adult population (2, 66–68). Among those who self-reported their mental health as suboptimal, we identified demographic subgroups who have higher likelihoods of utilizing mental health treatment resources and who may be more receptive to mental health treatment in the future. Our findings shed light on the extent to which single adults in the U.S. are currently engaging in mental health treatment and helps to pinpoint areas of need based on demographic background.
At the time of the survey, in August 2022, more than one-quarter (26%) of single adults in our sample were using mental health resources. In particular, 17% were currently engaged in psychotherapy and 16% were taking psychiatric medications (SSRIs, SNRIs, MAOIs, or Wellbutrin). The prevalence of mental health treatment in this sample of single adults was more substantial than reports generated from the general population [i.e., 10% in psychotherapy, 17% using psychiatric medications; (32)]. This suggests that single adults may seek out mental health treatment to a greater extent than the average population, and perhaps more than romantically partnered individuals. Future research should investigate this comparison.
With regards to demographic differences, we found that women were more likely than men to receive or be interested in mental health treatment. Further, we found that age was unassociated with current psychotherapy attendance or psychiatric medication use, but younger individuals were more likely to be interested in attending psychotherapy in the future, compared to older individuals. Gendered risk factors, societal influences, stigma around male help-seeking, and normalization of mental health conversations among younger audiences on social media platforms could contribute to these patterns (69–72). The COVID-19 pandemic has also had a profound impact on mental health and well-being across populations; younger individuals with less life experience may be less equipped to adapt to pandemic stressors and thus more interested in professional mental health treatment (73).
We found racial and ethnic differences in mental health treatment and interest. Although there were no racial/ethnic differences in the likelihood of current psychotherapy attendance, Black/African-American and Hispanic/Latino singles were less likely than White singles to report psychiatric medication use. There is no prior empirical literature to explain these differences. However, because psychiatric medications are procured through visits with a healthcare provider with the ability to prescribe medications, people who have experienced discrimination in healthcare settings may be less inclined to pursue mental health treatment via this route (74–77). Of note, Black/African-American participants were more likely than white participants to be interested in attending psychotherapy in the future. This suggests a nuanced understanding of mental health treatment preferences among racial and ethnic groups, highlighting the importance of considering historical and systemic factors that influence these preferences. It underscores the need for culturally sensitive approaches in mental health treatment provision, which can address and mitigate barriers to accessing treatment, particularly in the context of psychiatric medication.
In terms of sexual orientation, gay and lesbian participants were more likely to be currently engaged in psychotherapy or using psychiatric medications than were heterosexual participants. These findings align with prior work showing that people identifying as a sexual minority are more likely to seek out mental health treatment [(e.g., 78, 79)]. Further, these findings demonstrate the impact of minority stress on the need for mental health treatment (55): gay and lesbian participants likely experience a number of stressors related to their around their sexual identity and minoritized societal standing, which could increase their need for mental health services compared to heterosexual peers.
Finally, we did not find any differences in mental health treatment utilization or interest with respect to parenthood status or income. Although the transition to parenthood can bring about immense stress (57–61), and single parenthood may exacerbate that stress (e.g., 63), we did not observe differences in current mental health treatment uptake or interest as a function of whether or not participants had children. Our dataset did not account for the age of children or whether participants had full custody of their children, which would dictate whether the child(ren) resided with the participant. These factors have the potential to create substantial differences in the stress resulting from parenting, as well as in the amount of time one has to pursue treatment. Future research should investigate these discrepancies.
Prior literature suggests that lower income would be associated with greater mental health treatment uptake (52, 53), but income was not a meaningful factor in our study. Mental health treatment is often privatized and potentially costly in the U.S. (80). However, lower incomes have been linked to greater use of mental health resources offered as free services (81, 82). Further, one in five U.S. adults are enrolled in the Medicaid program for people with low income (83), which offers some financial coverage for a range of behavioral health conditions [e.g., substance use disorder; Medicaid.gov (84)]. Taken together, our lack of significant results for income may be explained by the ability of higher-income participants to afford treatment, and the accessibility of mental health treatment for lower-income participants. Future research is needed to understand how socioeconomic status dictates mental health treatment utilization and interest.
Limitations
The current research has several limitations. First, it relies on self-report data which requires participants to be honest and open. As the survey dealt with the stigmatized topic of mental health treatment, some participants may have answered in a manner more socially desirable than truthful [(e.g., 85)]. Relatedly, online survey research studies must acknowledge a self-selection bias, in which participants who are more interested in a topic may be more likely to take the survey. This bias violates probability theory; therefore online quota-based samples like the one used in the current study cannot be considered a random sample (86). This limits generalizability of our findings. Future research should employ random sampling techniques to help reduce self-selection bias. Future researchers could also cross-verify self-reported data about engagement in mental health treatment with healthcare records, to ensure that participants are accurately reporting their mental health treatment uptake.
This study is also limited by the ways in which the survey assessed psychotherapy attendance and psychiatric medication use. There was a lack of specificity regarding types of psychotherapy in which participants were engaged or interested. We assumed that participants understood the term “therapy/counseling” to mean sessions with a licensed mental health professional. However, participants might have considered alternative forms of care as psychotherapy, which would not be recognized as psychotherapy by the academic/scientific community. Future research should assess the specific types of therapeutic support that are sought after and preferred. Additionally, the survey did not include the full range of available psychiatric medications or assess interest in future use of such psychiatric medications. Consequently, the study may have unintentionally excluded participants using other types of psychiatric medications, providing an incomplete view of psychiatric medication use among singles. In future studies, it is essential to include all available forms of psychiatric medication to prevent unintentional exclusions and possible oversights. Relatedly, the survey may inadequately represent individuals with severe mental illness. There is often a co-occurrence of poverty and severe mental illness, including homelessness and joblessness (87). People with severe mental illness may be underrepresented in this research due to barriers to accessing online surveys.
After restricting our analytic sample to only participants who self-rated their mental health in the past year as suboptimal (i.e., those who did not report “very good” or “excellent” mental health), we were unable to report any findings on engagement or interest in mental health treatment for singles who identified as transgender, or for those who identified as Asian, Native American/American Indian, or as another racial/ethnic group not listed in survey item. Given that the study data stems from a 2022 survey, the exclusion of Asian participants from analyses is particularly noteworthy due to associations observed in the research literature between mental health, race, and the COVID-19 pandemic. For example, Lee and Howard (88) reported increases in the probability of Asian Americans receiving an anxiety or depression diagnosis between 2019 and 2020, and suggest this may be in part due to increased anti-Asian hate crimes stoked by inaccurate media coverage regarding the origins of the COVID-19 virus. As a result, our inability to comment on Asian singles’ engagement in mental health treatment or their interest in attending psychotherapy in the future is an important limitation of this study.
Additionally, the small cell size for Native American/American Indian participants also limited our analysis of their engagement and interest in mental health treatment. Mental health burden is high for this population group. In an analysis of data from the 2012 Behavioral Risk Factor Surveillance System Survey, Asdigian et al. (89) reported that Native American and American Indian adults rated their mental health as “poor” for around 6–7 days out of the past month. Importantly, this study compared the mental health burden of multiracial and single race Native American/American Indian participants and found that multiracial-identified individuals reported worse mental health compared to single-race identified individuals. These findings suggest not only the need for research attention on Native American and American Indian mental health and engagement in treatment, but also intentional targeted recruitment to allow for comparison of multiracial and single race individuals, as over 40% of Native American/American Indian people identify as multiracial (90).
Finally, we lacked information on participants’ education level or area of residency (i.e., urban or rural). Previous research indicates that those with higher levels of education and those living in urban areas are more interested in accessing mental health treatment (34, 91). Future research should take these factors, and those mentioned prior, into account for a more comprehensive understanding of mental health attitudes and preferences.
Clinical implications and conclusion
Our study on mental health treatment utilization and interest among single adults reveals a complex picture of both high and low levels of engagement with mental health services. Despite a greater propensity among single adults to engage in mental health treatment compared to the general U.S. population, as indicated in Terlizzi and Norris’ (32) study, most participants in our sample were not engaged in mental health treatment at the time of the survey—even though everyone in the final analytic sample self-evaluated their mental health over the last year as being less than “very good” or “excellent”. This underutilization of mental health resources highlights a critical gap in the provision and accessibility of mental healthcare for single adults. Furthermore, our findings reveal demographic disparities in the interest and uptake of mental health treatment based on gender, sexual orientation, and race, pointing to systemic barriers that may influence these trends.
These insights call for a multifaceted approach to address the therapeutic and clinical implications of our findings. Targeted outreach and education are imperative to raise awareness about the benefits of mental health treatment and to reduce stigma, especially in communities with identified disparities in mental health treatment engagement (e.g., Black/African-American and Hispanic/Latino individuals compared to white individuals). Personalized treatment plans that account for the individual’s demographic background and preferences may improve engagement in mental health treatment as well as treatment outcomes.
Moreover, enhancing provider training to better understand and cater to the specific needs and barriers encountered by single adults seeking mental health treatment is crucial. This includes comprehending the impact of systemic discrimination on mental health and implementing strategies to engage underrepresented groups effectively. Collaborating with community organizations can serve as a bridge to reach individuals who are in need of mental health treatment but are currently unengaged, promoting a more inclusive approach to mental healthcare. Finally, these findings underscore the importance of advocacy for policy changes aimed at ensuring equitable access to mental health services for all individuals, regardless of their relationship status, gender, sexual orientation, race, or other factors. By integrating these strategies, we can work towards a more inclusive and effective mental healthcare system that addresses the disparities and underutilization identified in this study, ultimately fostering a supportive environment for the mental well-being of single adults.
Data availability statement
The data reported in this manuscript were collected as part of a larger data collection. The larger data collection is cross-sectional and has been collected annually since 2010 (except 2018). There are published manuscripts including data from older waves of the survey, but not including the current participants, research topics, or target variables. There are no other manuscripts—published or in preparation—using the data included in the current manuscript. The 2022 wave is the only wave thus far to ask about therapy attendance or interest. Psychiatric medication use has been assessed in prior waves of the survey, but this data has never been reported in any publications. The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics statement
Ethical approval was not required for the studies involving humans because the Singles in America survey is conducted as market research by Match Group; only a de-identified dataset is provided to the researchers. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements because due to the nature of the secondary de-identified data, the present research falls under the category of exempt according to federal regulations at 45 CFRP part 46, paragraph d, number four, item ii (Office for Human Research Protections, 2021).
Author contributions
AG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. EK: Formal analysis, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing. LW: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. ZM: Data curation, Formal analysis, Investigation, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. MB-B: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. OA: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. JC: Conceptualization, Formal analysis, Investigation, Project administration, Writing – original draft, Writing – review & editing. MP: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft. LB: Data curation, Conceptualization, Validation, Investigation, Writing – original draft. SD: Conceptualization, Formal analysis, Investigation, Writing – original draft. JH: Conceptualization, Investigation, Writing – original draft. JG: Funding acquisition, Methodology, Project administration, Resources, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The annual Singles in America study is funded by Match. No financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
AG and JG received funding from Match Group as statistical consultant and scientific advisor, respectively, on the Singles in America project.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Apostolou, M. Why people stay single: an evolutionary perspective. Personal Individ Differ. (2017) 111:263–71. doi: 10.1016/j.paid.2017.02.034
2. Brown, A. (2020). A profile of single Americans. Pew Research Center’s Social & Demographic Trends Project. Available at: https://www.pewresearch.org/social-trends/2020/08/20/a-profile-of-single-americans/ (Accessed May 20, 2022)
4. DePaulo, BM. Singled out: How singles are stereotyped, stigmatized, and ignored, and still live happily ever after New York: Macmillan (2006).
5. Fry, R., Igielnik, R., and Patten, E. (2023) How millennials today compare with their grandparents 50 years ago. Pew Research Center. Available at: https://www.pewresearch.org/short-reads/2018/03/16/how-millennials-compare-with-their-grandparents/
6. DePaulo, BM, and Morris, WL. Singles in society and in science. Psychol Inq. (2005) 16:57–83. doi: 10.1207/s15327965pli162&3_01
7. Gesselman, AN, Franco, CY, Brodgon, EM, Gray, PB, Garcia, JR, and Fisher, HE. Perceptions of married life among single never-married, single ever-married, and married adults. Pers Relat. (2019) 26:586–601. doi: 10.1111/pere.12295
8. Greitemeyer, T. Stereotypes of singles: are singles what we think? Eur J Soc Psychol. (2009) 39:368–83. doi: 10.1002/ejsp.542
9. Apostolou, M, Alexopoulos, S, and Christoforou, C. The price of being single: an explorative study of the disadvantages of singlehood. Personal Individ Differ. (2023) 208:112208. doi: 10.1016/j.paid.2023.112208
10. Morris, WL, Sinclair, S, and DePaulo, BM. No shelter for singles: the perceived legitimacy of marital status discrimination. Group Process Intergroup Relat. (2007) 10:457–70. doi: 10.1177/1368430207081535
11. DePaulo, B. Single, no children: who is your family? In: A Vangelisti, editor. Handbook of family communication. 2nd ed. New York: Routledge (2012). 190–204.
12. Adamczyk, K. Voluntary and involuntary singlehood and young adults’ mental health: an investigation of mediating role of romantic loneliness. Curr Psychol. (2017) 36:888–904. doi: 10.1007/s12144-016-9478-3
13. Lechner, L, Bolman, C, and van Dalen, A. Definite involuntary childlessness: associations between coping, social support and psychological distress. Hum Reprod. (2007) 22:288–94. doi: 10.1093/humrep/del327
15. Hollingshead, AB, and Redlich, FC. Social class and mental illness: Community study Hoboken, New Jersey: John Wiley & Sons Inc. (1958).
16. Dodge, KA, Pettit, GS, and Bates, JE. Socialization mediators of the relation between socioeconomic status and child conduct problems. Child Dev. (1994) 65:649–65. doi: 10.2307/1131407
17. Johnson, JG, Cohen, P, Dohrenwend, BP, Link, BG, and Brook, JS. A longitudinal investigation of social causation and social selection processes involved in the association between socioeconomic status and psychiatric disorders. J Abnorm Psychol. (1999) 108:490–9. doi: 10.1037/0021-843X.108.3.490
18. Daniali, H, Martinussen, M, and Flaten, MA. A global meta-analysis of depression, anxiety, and stress before and during COVID-19. Health Psychol. (2023) 42:124–38. doi: 10.1037/hea0001259
19. Goodwin, RD, Dierker, LC, Wu, M, Galea, S, Hoven, CW, and Weinberger, AH. Trends in U.S. depression prevalence from 2015 to 2020: the widening treatment gap. Am J Prev Med. (2022) 63:726–33. doi: 10.1016/j.amepre.2022.05.014
20. National Collaborating Centre for Mental Health (UK). (2011). Common mental health disorders: Identification and pathways to care. Leicester (UK): British Psychological Society (UK). (NICE Clinical Guidelines, No. 123.) Available at: https://www.ncbi.nlm.nih.gov/books/NBK92266/
21. Wang, D, Zhao, J, Ross, B, Ma, Z, Zhang, J, Fan, F, et al. Longitudinal trajectories of depression and anxiety among adolescents during COVID-19 lockdown in China. J Affect Disord. (2022) 299:628–35. doi: 10.1016/j.jad.2021.12.086
22. World Health Organization (2022). COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide. Available at: https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide (Accessed July 27, 2023).
23. Byrom, NC. Supporting a friend, housemate or partner with mental health difficulties: the student experience. Early Interv Psychiatry. (2019) 13:202–7. doi: 10.1111/eip.12462
24. Chen, H, Cohen, P, Kasen, S, Johnson, JG, Berenson, K, and Gordon, K. Impact of adolescent mental disorders and physical illnesses on quality of life 17 years later. Arch Pediatr Adolesc Med. (2006) 160:93–9. doi: 10.1001/archpedi.160.1.93
25. Virgolino, A, Costa, J, Santos, O, Pereira, ME, Antunes, R, Ambrósio, S, et al. Lost in transition: a systematic review of the association between unemployment and mental health. J Ment Health. (2022) 31:432–44. doi: 10.1080/09638237.2021.2022615
26. Knifton, L, and Inglis, G. Poverty and mental health: policy, practice and research implications. BJPsych Bulletin. (2020) 44:193–6. doi: 10.1192/bjb.2020.78
27. Corponi, F, Anmella, G, Verdolini, N, Pacchiarotti, I, Samalin, L, Popovic, D, et al. Symptom networks in acute depression across bipolar and major depressive disorders: a network analysis on a large, international, observational study. Eur Neuropsychopharmacol. (2020) 35:49–60. doi: 10.1016/j.euroneuro.2020.03.017
28. Jing, E, and Straw-Wilson, K. Sexual dysfunction in selective serotonin reuptake inhibitors (SSRIs) and potential solutions: a narrative literature review. Mental Health Clinician. (2016) 6:191–6. doi: 10.9740/mhc.2016.07.191
29. American Psychological Association (2009). Different approaches to psychotherapy. Available at: https://www.apa.org/topics/psychotherapy/approaches (Accessed July 27, 2023).
30. U.S. Department of Health and Human Services (2023). Psychotherapies. National Institute of Mental Health. Available at: https://www.nimh.nih.gov/health/topics/psychotherapies
31. National Institute of Mental Health. (2022). Mental health medications. Available at: https://www.nimh.nih.gov/health/topics/mental-health-medications (Accessed July 27, 2023).
32. Terlizzi, E. P., and Norris, T. (2021). Mental health treatment among adults: United States, 2020. CDC.gov. Available at: https://www.cdc.gov/nchs/products/databriefs/db419.htm (Accessed July 27, 2023).
33. Burkett, CA. Obstructed use: reconceptualizing the mental health (help-seeking) experiences of black Americans. J Black Psychol. (2017) 43:813–35. doi: 10.1177/0095798417691381
34. Gamm, L, Stone, S, and Pittman, S. Mental health and mental disorders—a rural challenge: a literature review. Rural Healthy People. (2010) 2:97–114.
35. Gavrilovic, JJ, Schützwohl, M, Fazel, M, and Priebe, S. Who seeks treatment after a traumatic event and who does not? A review of findings on mental health service utilization. J Trauma Stress. (2005) 18:595–605. doi: 10.1002/jts.20068
36. Kessler, RC, Demler, O, Frank, RG, Olfson, M, Pincus, HA, Walters, EE, et al. Prevalence and treatment of mental disorders, 1990 to 2003. N Engl J Med. (2005) 352:2515–23. doi: 10.1056/nejmsa043266
37. McChesney, GC, Adamson, G, and Shevlin, M. Service use patterns and mental health symptoms among adolescents exposed to multiple types of trauma. J Adolesc. (2015) 40:1–10. doi: 10.1016/j.adolescence.2015.01.003
38. Smith, TB, and Trimble, JE. Mental health service utilization across race: a meta-analysis of surveys and archival studies In: TB Smith and JE Trimble, editors. Foundations of multicultural psychology: Research to inform effective practice : Washington, DC: American Psychological Association (2016). 67–94.
39. Kovess-Masfety, V, Alonso, J, Brugha, TS, Angermeyer, MC, Haro, JM, and Sevilla-Dedieu, C. Differences in lifetime use of services for mental health problems in six European countries. Psychiatr Serv. (2007) 58:213–20. doi: 10.1176/ps.2007.58.2.213
40. NHS. (2009). Adult psychiatric morbidity in England – 2007, results of a household survey. Adult Psychiatric Morbidity Study. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/adult-psychiatric-morbidity-survey/adult-psychiatric-morbidity-in-england-2007-results-of-a-household-survey
41. Olfson, M, and Marcus, SC. National trends in outpatient psychotherapy. Am J Psychiatry. (2010) 167:1456–63. doi: 10.1176/appi.ajp.2010.10040570
42. Blay, SL, Fillenbaum, GG, da Silva, PFR, and Peluso, ET. Use of psychotherapy in a representative adult community sample in São Paulo, Brazil. J Nerv Ment Dis. (2014) 202:688–94. doi: 10.1097/nmd.0000000000000181
43. Leppänen, H, Kampman, O, Autio, R, Karolaakso, T, Näppilä, T, Rissanen, P, et al. Socioeconomic factors and use of psychotherapy in common mental disorders predisposing to disability pension. BMC Health Serv Res. (2022) 22:983–12. doi: 10.1186/s12913-022-08389-1
44. Sora, B, Nieto, R, Montesano, A, and Armayones, M. Usage patterns of telepsychology and face-to-face psychotherapy: clients’ profiles and perceptions. Front Psychol. (2022) 13:821671. doi: 10.3389/fpsyg.2022.821671
45. Stewart, SL, Van Dyke, JN, and Poss, JW. Examining the mental health presentations of treatment-seeking transgender and gender nonconforming (TGNC) youth. Child Psychiatry Hum Dev. (2023) 54:826–36. doi: 10.1007/s10578-021-01289-1
46. Lefevor, GT, Boyd-Rogers, CC, Sprague, BM, and Janis, RA. Health disparities between genderqueer, transgender, and cisgender individuals: an extension of minority stress theory. J Couns Psychol. (2019) 66:385–95. doi: 10.1037/cou0000339
47. Meyer, I. H. “Minority stress and mental health in gay men.” Journal of health and social behavior (1995): 38–56.
48. Cyrus, K. Multiple minorities as multiply marginalized: applying the minority stress theory to LGBTQ people of color. J Gay Lesbian Ment Health. (2017) 21:194–202. doi: 10.1080/19359705.2017.1320739
49. Parra, LA, and Hastings, PD. Integrating the neurobiology of minority stress with an intersectionality framework for LGBTQ-Latinx populations. New Dir Child Adolesc Dev. (2018) 2018:91–108. doi: 10.1002/cad.20244
50. Williams, SL, Job, SA, Todd, E, and Braun, K. A critical deconstructed quantitative analysis: sexual and gender minority stress through an intersectional lens. J Soc Issues. (2020) 76:859–79. doi: 10.1111/josi.12410
51. Suokas, K, Koivisto, A, Hakulinen, C, Kaltiala, R, Sund, R, Lumme, S, et al. Association of income with the incidence rates of first psychiatric hospital admissions in Finland, 1996-2014. JAMA Psychiatry. (2019) 77:274–84. doi: 10.1001/jamapsychiatry.2019.3647
52. Marcotte, D, and Wilcox-Gök, V. Estimating the employment and earnings costs of mental illness: recent developments in the United States. Soc Sci Med. (2001) 53:21–7. doi: 10.1016/S0277-9536(00)00312-9
53. Connor, P, Sarafidis, V, Zyphur, MJ, Keltner, D, and Chen, S. Income inequality and white-on-black racial Bias in the United States: evidence from project implicit and Google trends. Psychol Sci. (2019) 30:205–22. doi: 10.1177/0956797618815441
54. McConnell, EA, Janulis, P, Phillips, G II, Truong, R, and Birkett, M. Multiple minority stress and LGBT community resilience among sexual minority men. Psychol Sex Orientat Gend Divers. (2018) 5:1–12. doi: 10.1037/sgd0000265
55. Meyer, IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. (2003) 129:674–97. doi: 10.1037/0033-2909.129.5.674
56. Rivas-Koehl, M, Rivas-Koehl, D, and McNeil Smith, S. The temporal intersectional minority stress model: reimagining minority stress theory. J Fam Theory Rev. (2023) 15:706–26. doi: 10.1111/jftr.12529
57. Banker, JE, and LaCoursiere, DY. Postpartum depression: risks, protective factors, and the couple’s relationship. Issues Ment Health Nurs. (2014) 35:503–8. doi: 10.3109/01612840.2014.888603
58. Paavonen, EJ, Saarenpää-Heikkilä, O, Pölkki, P, Kylliäinen, A, Porkka-Heiskanen, T, and Paunio, T. Maternal and paternal sleep during pregnancy in the child-sleep birth cohort. Sleep Med. (2017) 29:47–56. doi: 10.1016/j.sleep.2016.09.011
59. Reid, KM, and Taylor, MG. Social support, stress, and maternal postpartum depression: a comparison of supportive relationships. Soc Sci Res. (2015) 54:246–62. doi: 10.1016/j.ssresearch.2015.08.009
60. Saxbe, D, Rossin-Slater, M, and Goldenberg, D. The transition to parenthood as a critical window for adult health. Am Psychol. (2018) 73:1190–200. doi: 10.1037/amp0000376
61. Schiller, CE, Meltzer-Brody, S, and Rubinow, DR. The role of reproductive hormones in postpartum depression. CNS Spectr. (2015) 20:48–59. doi: 10.1017/s1092852914000480
62. Bemiller, M. Non-custodial mothers: thematic trends and future directions. Sociol Compass. (2008) 2:910–24. doi: 10.1111/j.1751-9020.2008.00117.x
63. Gray, PB, Franco, CY, Garcia, JR, Gesselman, AN, and Fisher, HE. Romantic and dating behaviors among single parents in the United States. Pers Relat. (2016) 23:491–504. doi: 10.1111/pere.12139
64. Office for Human Research Protections (OHRP). (2021). Exemptions (2018 requirements). U.S. Department of Health and Human Services. Available at: https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/common-rule-subpart-a-46104/index.html (Accessed May 1, 2023).
65. Haupert, ML, Pope, AR, Garcia, JR, and Smith, ER. An inclusive gender identity measure In: RR Milhausen, JK Sakaluk, TD Fisher, CM Davis, and WL Yarber, editors. Handbook of sexuality-related measures. 4th ed. New York: Routledge (2019). 353–5.
66. Fry, R., and Parker, K. (2021). Rising share of U.S. Adults are living without a spouse or partner, pew research Center’s Social & Demographic Trends Project. United States of America. Available at: https://policycommons.net/artifacts/1846178/rising-share-of-us/2591786/ (Accessed July 27, 2023). CID: 20.500.12592/snmn6m.
67. Girme, YU, Park, Y, and MacDonald, G. Coping or thriving? Reviewing intrapersonal, interpersonal, and societal factors associated with well-being in singlehood from a within-group perspective. Perspect Psychol Sci. (2022) 18:1097–120. doi: 10.1177/17456916221136119
68. Ta, VP, Gesselman, AN, Perry, BL, Fisher, HE, and Garcia, JR. Stress of singlehood: marital status, domain-specific stress, and anxiety in a national U.S. sample. J Soc Clin Psychol. (2017) 36:461–85. doi: 10.1521/jscp.2017.36.6.461
69. Kearl, H., Johns, N. E., and Raj, A. (2019). Measuring# MeToo: A national study on sexual harassment and assault. UC San Diego Center on Gender Equity and Health. Available at: https://gehweb.ucsd.edu/wp-content/uploads/2019/05/2019-metoo-national-sexual-harassment-and-assault-report.pdf
70. Liddon, L, Kingerlee, R, and Barry, JA. Gender differences in preferences for psychological treatment, coping strategies, and triggers to help-seeking. Br J Clin Psychol. (2018) 57:42–58. doi: 10.1111/bjc.12147
71. Patalay, P, and Demkowicz, O. Debate: don’t mind the gap–why do we not care about the gender gap in common mental health difficulties? Child Adolesc Mental Health. (2023) 28:341–3. doi: 10.1111/camh.12647
72. Pattyn, E, Verhaeghe, M, and Bracke, P. The gender gap in mental health service use. Soc Psychiatry Psychiatr Epidemiol. (2015) 50:1089–95. doi: 10.1007/s00127-015-1038-x
73. Bhattacharjee, B, and Acharya, T. The COVID-19 pandemic and its effect on mental health in USA – a review with some coping strategies. Psychiatry Q. (2020) 91:1135–45. doi: 10.1007/s11126-020-09836-0
74. Kim, G, Aguado Loi, CX, Chiriboga, DA, Jang, Y, Parmelee, P, and Allen, RS. Limited English proficiency as a barrier to mental health service use: a study of Latino and Asian immigrants with psychiatric disorders. J Psychiatr Res. (2011) 45:104–10. doi: 10.1016/j.jpsychires.2010.04.031
75. Segal, SP, Bola, JR, and Watson, MA. Race, quality of care, and antipsychotic prescribing practices in psychiatric emergency services. Psychiatr Serv. (1996) 47:282–6. doi: 10.1176/ps.47.3.282
76. Thomeer, MB, Moody, MD, and Yahirun, J. Racial and ethnic disparities in mental health and mental health care during the COVID-19 pandemic. J Racial Ethn Health Disparities. (2023) 10:961–76. doi: 10.1007/s40615-022-01284-9
77. Williams, D. Stress and the mental health of populations of color: advancing our understanding of race-related stressors. J Health Soc Behav. (2018) 59:466–85. doi: 10.1177/0022146518814251
78. Baams, L, De Luca, SM, and Brownson, C. Use of mental health services among college students by sexual orientation. LGBT Health. (2018) 5:421–30. doi: 10.1089/lgbt.2017.0225
79. Ward, BW, Dahlhamer, JM, Galinsky, AM, and Joestl, SS. Sexual orientation and health among U.S. adults: national health interview survey, 2013. Natl Health Stat Rep. (2014) 77:1–10.
80. Geyman, J. COVID-19 has revealed America’s broken health care system: what can we learn? Int J Health Serv. (2021) 51:188–94. doi: 10.1177/0020731420985640
81. Ali, MM, West, K, Teich, JL, Lynch, S, Mutter, R, and Dubenitz, J. Utilization of mental health Services in Educational Setting by adolescents in the United States. J Sch Health. (2019) 89:393–401. doi: 10.1111/josh.12753
82. Farmer, EM, Stangl, DK, Burns, BJ, Costello, EJ, and Angold, A. Use, persistence, and intensity: patterns of care for children’s mental health across one year. Community Ment Health J. (1999) 35:31–46. doi: 10.1023/a:1018743908617
83. Kaiser Family Foundation (2021). Health insurance coverage of the Total population: 2021. Available at: https://www.kff.org/other/state-indicator/total-population/ (Accessed July 27, 2023).
84. Medicaid.gov (2023). Behavioral health services. Medicaid.org. Available at: https://www.medicaid.gov/medicaid/benefits/behavioral-health-services/index.html (Accessed July 27, 2023).
85. Latkin, CA, Edwards, C, Davey-Rothwell, MA, and Tobin, KE. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict Behav. (2017) 73:133–6. doi: 10.1016/j.addbeh.2017.05.005
86. Bethlehem, J. Selection bias in web surveys. Int Stat Rev. (2010) 78:161–88. doi: 10.1111/j.1751-5823.2010.00112.x
87. Elbogen, EB, Lanier, M, Wagner, HR, and Tsai, J. Financial strain, mental illness, and homelessness: results from a national longitudinal study. Med Care. (2021) 59:S132–8. doi: 10.1097/mlr.0000000000001453
88. Lee, J, and Howard, JT. Increased self-reported mental health problems among Asian-Americans during the COVID-19 pandemic in the United States: evidence from a nationally representative database. J Racial Ethn Health Disparities. (2023) 10:2344–53. doi: 10.1007/s40615-022-01414-3
89. Asdigian, NL, Bear, UR, Beals, J, Manson, SM, and Kaufman, CE. Mental health burden in a national sample of American Indian and Alaska native adults: differences between multiple-race and single-race subgroups. Soc Psychiatry Psychiatr Epidemiol. (2018) 53:521–30. doi: 10.1007/s00127-018-1494-1
90. Parker, K., Horowitz, J. M., and Lopez, M. H. (2015). Multiracial in America. Pew Research Center’s Social & Demographic Trends Project. Available at: https://www.pewresearch.org/social-trends/2015/06/11/multiracial-in-america/
Keywords: mental health treatment-seeking, client characteristics, gender identity, ethnic/racial identity, psychotherapy
Citation: Gesselman AN, Kaufman EM, Weeks LYS, Moscovici Z, Bennett-Brown M, Adams OR, Campbell JT, Piazza M, Bhuyan L, Dubé S, Hille JJ and Garcia JR (2024) Exploring patterns in mental health treatment and interests of single adults in the United States: a secondary data analysis. Front. Public Health. 12:1292603. doi: 10.3389/fpubh.2024.1292603
Edited by:
Christos Theleritis, National and Kapodistrian University of Athens, GreeceReviewed by:
Aikaterini Arvaniti, Democritus University of Thrace, GreeceDonna Mcalpine, University of Minnesota Twin Cities, United States
Copyright © 2024 Gesselman, Kaufman, Weeks, Moscovici, Bennett-Brown, Adams, Campbell, Piazza, Bhuyan, Dubé, Hille and Garcia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amanda N. Gesselman, YWdlc3NlbG1AaW5kaWFuYS5lZHU=