 Jesús Calderón-Moreno1
Jesús Calderón-Moreno1 María Jesús Delgado-Rodriguez1
María Jesús Delgado-Rodriguez1 Raúl Juárez-Vela2,3Clara Isabel Tejada-Garrido2
Raúl Juárez-Vela2,3Clara Isabel Tejada-Garrido2 Regina Ruiz de Viñaspre-Hernández2,3
Regina Ruiz de Viñaspre-Hernández2,3 Amaya Burgos-Esteban2*
Amaya Burgos-Esteban2* Pilar Sánchez-Conde4,5Vicente Andreu-Fernández6
Pilar Sánchez-Conde4,5Vicente Andreu-Fernández6 Vicente Gea-Caballero6Jose Angel Santos-Sanchez4
Vicente Gea-Caballero6Jose Angel Santos-Sanchez4 Manuel Quintana-Diaz3,7
Manuel Quintana-Diaz3,7 Eva María Andrés-Esteban1
Eva María Andrés-Esteban1- 1Business Economics Department, University of Rey Juan Carlos, Madrid, Spain
- 2Department of Nursing, GRUPAC, University of La Rioja, Logroño, Spain
- 3Research Group Blood Patient Management, IDI-Paz Research Institute, Madrid, Spain
- 4Faculty of Medicine, University of Salamanca, Salamanca, Spain
- 5Anesthesia and Resuscitation Service, University Healthcare Complex, Salamanca, Spain
- 6Faculty of Health Sciences, International University of Valencia, Valencia, Spain
- 7Intensive Care Unit, Hospital La Paz, La Paz, Spain
Introduction: Many researchers have focused their studies on hypertension due to its over-representation among COVID-19 patients. Both retrospective and observational studies conducted close to the Wuhan area have reported that hypertension is the most common comorbidity observed in patients affected by COVID-19.
Objective: Our objective is that patients with arterial hypertension have a worse prognosis in terms of evolution leading to higher costs.
Methods: A retrospective cross-sectional study was conducted. A total of 3,581 patients from La Paz University Hospital (LPUH) during the period between 15 July 2020 and 31 July 2020 were included in this study.
Results: It should be noted that 40.71% of the patients were hypertensive. As expected, hypertension was associated with men, among whom we observed a higher prevalence and a higher age (median age of 77 years (IQI: 65–85) versus 52 years (IQI: 37–64), p-value < 0.001). Hypertensive patients had a higher prevalence of dyspnea (52.14% vs. 47.15%, p-value = 0.004) and altered awareness (14.89% vs. 4.30%, p-value <0.001). The non-parametric Kaplan–Meier curve estimates the survival of patients in the two study groups. We can see how patients with hypertension have a higher associated mortality, with the difference being statistically significant, p-value (log-rank) = 0.004. Only for the appearance of complications during hospitalization, the group of hypertensive patients reached the figure of €1,355,901.71 compared to the total of 421,403.48 € for normotensive patients.
Conclusion: Our study shows the worse clinical evolution of patients with COVID-19 in terms of associated morbidity and mortality. It also shows that the cost of managing patients with hypertension is greater than that of managing normotensive patients.
Introduction
Many researchers have focused their studies on hypertension due to its over-representation among COVID-19 patients (1). Both retrospective and observational studies conducted close to the Wuhan area have reported that hypertension is the most common comorbidity observed in patients affected by COVID-19, ranging between 15 and 30% (2–4). In one of the largest studies conducted in Wuhan with data collected from 1,099 COVID-19 patients, 165 patients (approximately 15% of the total sample) had high blood pressure (5). The same study also reported that a total of 23.7% of hypertensive patients had higher disease severity than 13.4% of normotensive subjects. However, 35.8% of hypertensive patients experienced worst outcomes in terms of intensive care unit (ICU) admission, mechanical ventilation, or death compared to just 13.7% of normotensive patients (5).
Another study conducted in China, which investigated 138 COVID-19 patients, found a similarly high prevalence of hypertension among the patients (31.2%) (2). The researchers also affirmed that 58.3% of hypertensive patients with COVID-19 infection were admitted to ICU compared to 21.6% of patients with normal blood pressure. Guan et al. studied a cohort of 1,590 patients from 575 hospitals and found that hypertension was independently associated with severe COVID-19 (hazard ratio 1.575; 95% CI: 1.07–2.32). All these findings indicate that hypertensive patients have a higher risk of developing severe outcomes from COVID-19.
These early results were similar to those subsequently found in other countries. Thus, JAMA published data on 1,591 patients admitted to intensive care units in Italy (6). Arterial hypertension (49%) and cardiovascular disease (21%) were the most frequent comorbidities, above other respiratory diseases. The study stratified the cohort by the presence or absence of hypertension and hypertensives finding that patients with arterial hypertension had higher mortality (65% vs. 40%, p < 0.001).
The Spanish National Health System (SNS) is based on a Beveridge-type public model (7). It is a decentralized national health system, with competencies transferred to 17 Spanish autonomous communities (regions), under the control of the Ministry of Health. The SNS coverage gradually spread until 100% of citizens were covered in 1989. Currently, care is financed by taxes, and services are accessed by health cards. There are not many studies related to the cost of managing patients infected with the SARS-CoV-2 virus. In Spain, Calderon et al. reported that the cost of managing patients with COVID-19 without hospitalization is €729.79, and the cost of hospitalized patients ranges between €4294.36 and €14440.68, if there is an ICU admission (8).
If we focus on the worse evolution of hypertensive patients, they have a higher incidence of complications, longer hospital stays, or stays in intensive care units than normotensive patients, and all this translates into higher healthcare costs for the management of hypertensive patients when infected with the SARS-CoV-2 virus. Therefore, our working hypothesis is that patients with arterial hypertension have a worse prognosis in terms of evolution leading to higher costs.
Methods
Design
A retrospective cross-sectional study was carried out.
Data collection
Given the avalanche of patients in the emergency department, wards, and the ICU and the lack of knowledge of the disease during the initial months of the pandemic, the Hospital Universitario La Paz created a specific data collection notebook for all those who came to the hospital with clinical manifestations compatible with SARS-CoV-2 virus infection. This database was created by several experts in epidemiology at the hospital with the aim of learning more about the disease known as COVID-19.
Population and sample
A total of 3,581 patients from the La Paz University Hospital (LPUH) during the period between 15 July 2020 and 31 July 2020 were included in this study. The database included sociodemographic data, clinical status, laboratory findings, and clinical management of patients admitted with a respiratory infection caused by SARS-CoV-2 since the outbreak of the current pandemic.
Variables
Patient demographic data were collected prior to admission. Total costs were categorized based on care settings (admission to the hospital ward, admission to the ICU, and length of hospital stay) and the occurrence of most frequent complications (such as respiratory infection, pneumonia, acute respiratory distress syndrome, pneumothorax, pleural effusion, meningitis, convulsions, stroke, heart failure, endocarditis, arrhythmia, cardiac ischemia, cardiac arrest, coagulation problems, anemia, renal failure, pancreatitis, hepatic failure, psychiatric illness, and gastrointestinal bleeding). Additionally, variables associated with chronic health problems (such as smoking, diabetes, hypertension, chronic cardiac diseases, asthma, and chronic bronchitis) were considered. These variables have been linked to complications in COVID-19.
The cost data used were provided by the accounting department of the hospital, which allowed more precise estimates to be made.
Statistical analysis
Quantitative variables were described using robust statistics, such as median and interquartile interval, whereas for qualitative variables, frequency distribution was used. For the comparison of quantitative variables that were not normally distributed among frailty groups, the Kruskal–Wallis non-parametric H test was used, based on the Shapiro–Wilk test. Finally, the chi-squared test was used to compare qualitative variables.
The survival estimate was assessed using the Kaplan–Meier method comparing the survival curve between the groups with the log-rank test. The multivariate analysis was carried out by means of Cox regression, with the forward conditional method, introducing as independent variables the variables that obtained statistical significance in the bivariate analysis or that could have a clinically plausible implication. The results of the multivariate model were presented as a hazard ratio (95% CI).
The statistical analysis was performed using STATA v16.0, and a p-value of 5% was considered statistically significant.
Ethical considerations
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki (2008 update, available on the World Medical Association website).1 Additionally, it adhered to the standards of good clinical practice as described in the ICH Harmonized Tripartite Guidelines for Good Clinical Practice (2001) and the Guidelines for Good Epidemiological Practice.2 The study was approved by the Clinical Research Ethics Committee of LPUH, Madrid, with the LPUH code: PI-4155. It was not necessary to provide a formulary of informed consent as the anonymized database was used for data extraction. This study was conducted in accordance with European and Spanish regulations for the protection of personal data (Organic Law 3/2008).
Results
Description of the sample
The patients were stratified according to the diagnosis of hypertension. Table 1 shows the demographic characteristics of these patients. It should be noted that 40.71% of the patients were hypertensive. As expected, hypertension was associated with men, among whom we observed a higher prevalence and a higher median age [median of 77 years (IQI: 65–85) vs. 52 years (IQI: 37–64), p-value <0.001].
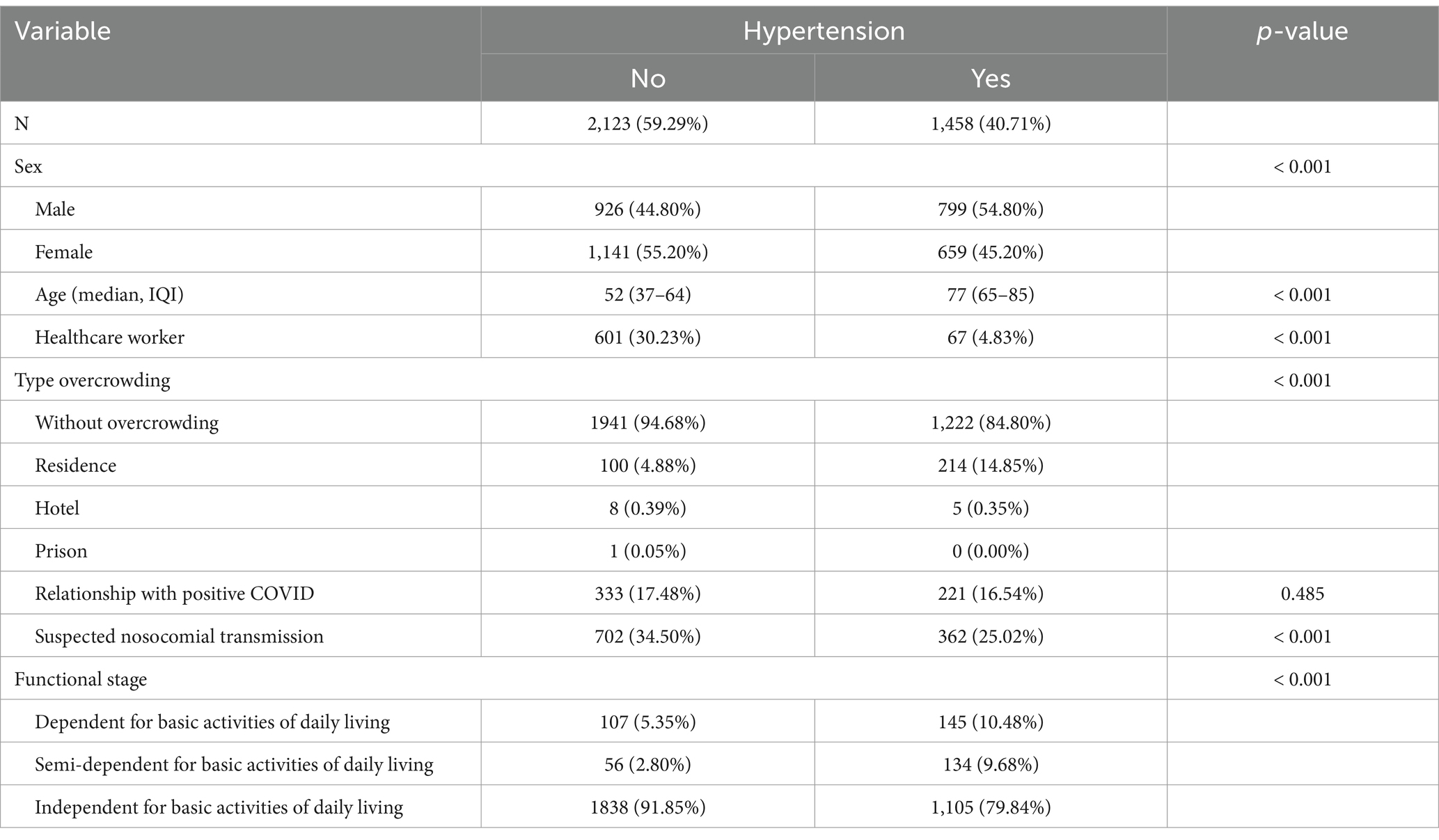
Table 1. Description of demographic variables in patients with and without arterial hypertension admitted for COVID-19.
The clinical presentation of COVID-19 symptomatology was also very different between patients with hypertension and normotensive patients, as shown in the following Table 2. Notably, hypertensive patients exhibited a higher prevalence of dyspnea (52.14% vs. 47.15%, p-value = 0.004) and altered awareness (14.89% vs. 4.30%, p-value <0.001).

Table 2. Clinical symptomatology at hospital admission.
Regarding the complications presented by patients with hypertension, we observed a significant difference in most of them. Acuate Respiratory Syndrome by COVID-19, much more present in patients with HT (31.37% vs. 12.00%, p-value <0.001), pneumothorax (6.73% vs. 0.67%, p-value = 0.007), cardiac arrest (15.38% vs. 0.00%, p-value <0.001), acute confusional syndrome (29.81% vs. 4.67%, p-value <0.001), and clotting alteration or sharp failure as shown in Table 3. In addition, hypertensive patients have a higher in-hospital mortality rate than normotensive patients (Tables 4, 5).
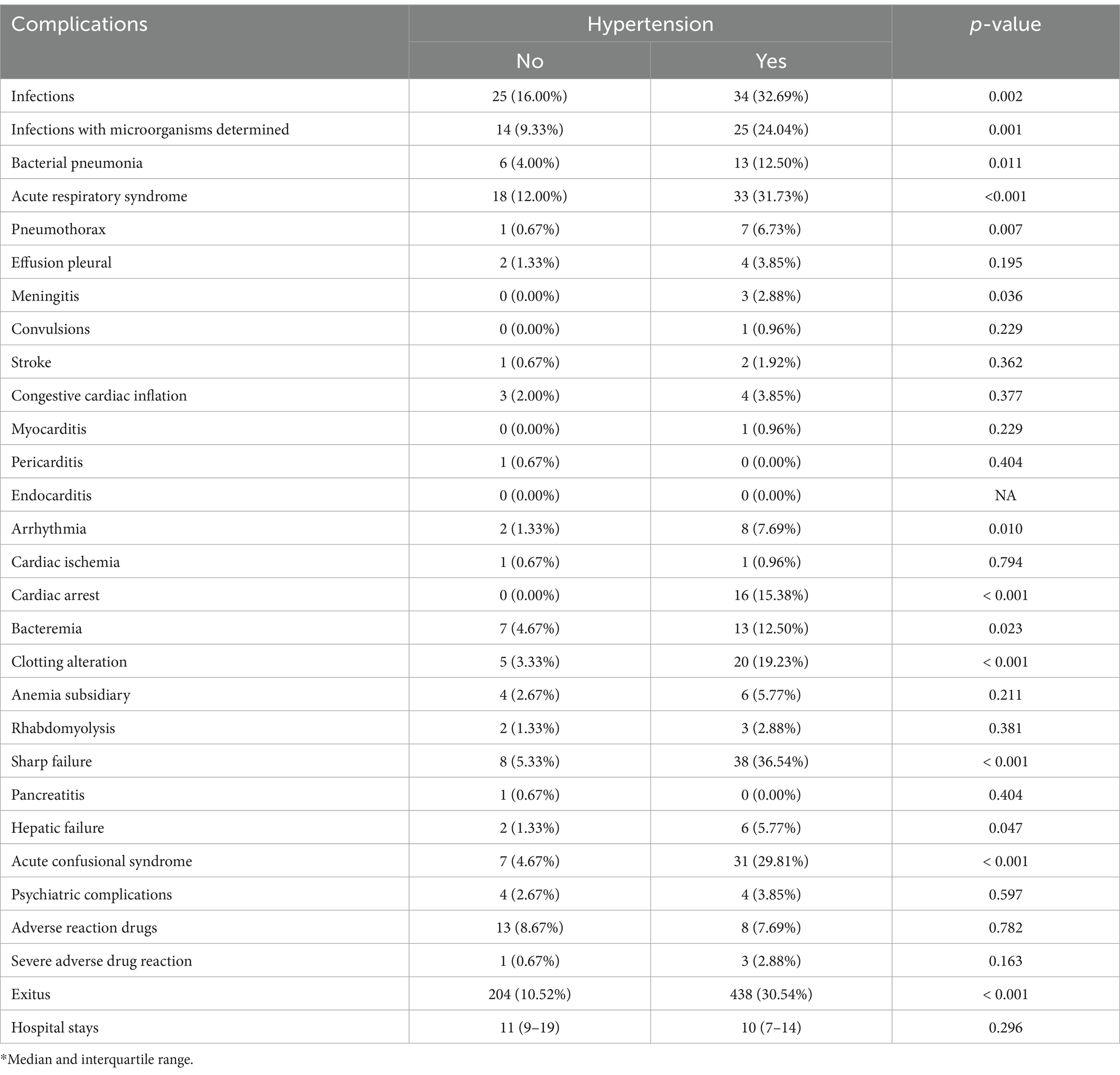
Table 3. Incidence of complications during hospital stay.
Figure 1 shows the non-parametric Kaplan–Meier curve, which estimates the survival of patients in the two study groups. We can see how patients with hypertension have a higher associated mortality, with the difference being statistically significant, p-value (log-rank) = 0.004.
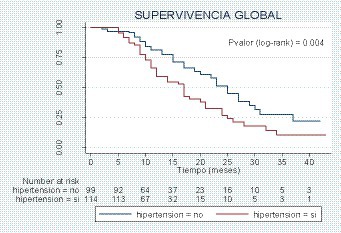
Figure 1. Kaplan–Meier estimator.

Table 4. Cox regression model to predict COVID-19 mortality.
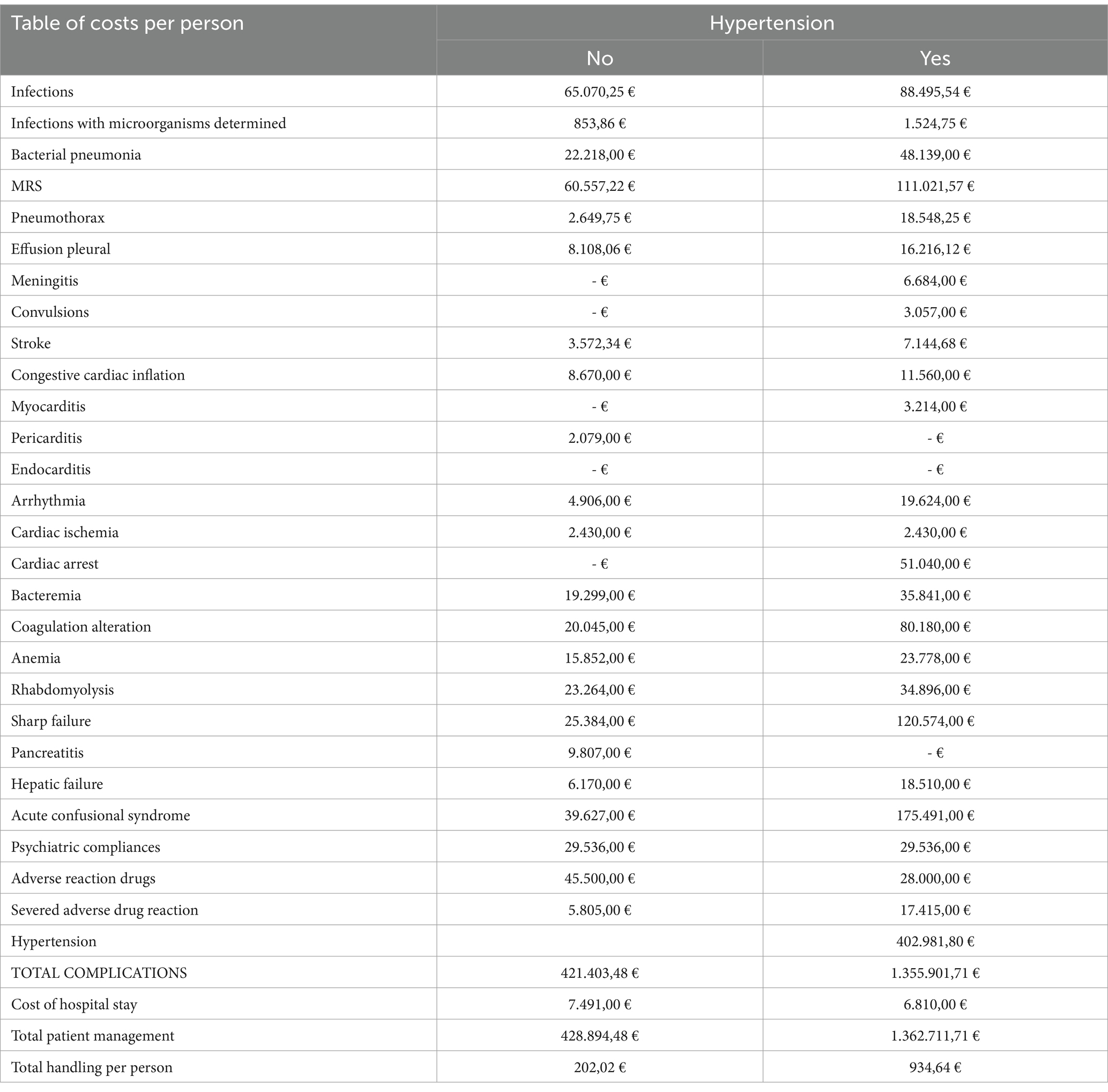
Table 5. Costs associated with the management of COVID-19 patients with and without hypertension.
In the Cox regression model, we observed that chronic cardiac disease (HR = 1.70, 95% CI: 1.05–2.75), chronic kidney disease (HR = 2.08, 95% CI: 1.13–3.80), and arterial hypertension (HR = 1.67, 95% CI: 1.07–2.35) were associated with in-hospital mortality.
Finally, to conclude the analysis, we include the cost of managing complications. We have already seen that hypertensive patients have more complications compared to normotensive patients, and this increases the healthcare costs of these patients. Specifically, only for the appearance of complications during hospitalization, the group of hypertensive patients reached the figure of €1,355,901.71 compared to the total of €421,403.48 for normotensive patients. This difference in figures means that the cost of managing the complications observed in hypertensive patients is 3.2 times higher than in normotensive patients. However, there was no significant difference in hospital stay between the two groups.
Discussion
Our data show that the group of hypertensive patients studied are older and more frequently men. These two characteristics, male sex and advanced age, are considered as highly relevant conditions associated with a worse prognosis in the evolution of COVID-19. Furthermore, older age is related to higher incidence of comorbidities other than hypertension, such as diabetes, cardiovascular disease, cerebrovascular disease, or obesity, which also increase susceptibility to infection and worsen disease progression. Consequently, the impact of hypertension on COVID-19 is not well defined. However, findings of some studies suggest that hypertension alone may not increase the risk of infection and complications of COVID-19 including death (9).
Many studies show that the cost of managing hypertensive patients is double that of normotensive patients. Our studies are in line with the findings of Badia et al. (10) and it is important to establish an evaluation of interventions and services aimed at the management of hypertension with special emphasis on complications. Numerous studies, such as the analyses presented in The Lancet (11), focus on improvements in detection and treatment with the aim, precisely, of reducing prevalence through early diagnosis, thereby reducing complications, which our study has quantified. For example, obesity is an important aspect to take into account in the development of arterial hypertension. Different studies have quantified that, if managed at an aggregate level, the savings in healthcare costs would amount to between €1,859 and €1,926 per person, and the return on investment would be between 3.3 and 7.0%. (12)
However, if we take a global view of hypertension, we know precisely that several studies (13) reflect the comorbidity of patients with hypertension together with other pathologies, such as dyslipidemia, diabetes, ischemic heart disease, and even stroke, which is also reflected in our study when discussing associated comorbidities. Precisely in the field of stroke, hypertension is the main driver of cerebral small vessel disease (CSVD) leading to cognitive impairment and lacunar stroke (14). On the other hand, the COVID-19 pandemic has also highlighted the worse evolution of patients with COVID-19 and the associated costs (8). Precisely, the association between cardiovascular pathology and poor evolution of SARS-CoV-2 infection is striking in terms of costs. With respect to comorbidities and COVID-19 and its associated costs, studies published in different countries (14) show that hypertension, diabetes, cerebrovascular disease, and ischemic heart disease are markedly more frequent in patients who require critical care or die from COVID-19, establishing a causal link between an underlying pathology, such as hypertension, and other factors, such as myocardial dysfunction produced by SARS-CoV-2.
Continuing with myocardial dysfunction, special interest should alert us to the relationship between hypertension and heart failure. It is precisely in the development of left ventricular hypertrophy and consequently heart failure (15) that hypertension is a key factor, and early diagnosis and treatment are necessary. Hypertensive heart disease describes a spectrum of diseases ranging from uncontrolled hypertension to the final development of heart failure, being mainly among others, the triggering event of left ventricular hypertrophy a hypertensive heart disease, something that can be reversible if recognized early and treated aggressively. Regarding heart failure, a study in the United States (16) found that the mean total cost ± SD was $13,807 ± 24,145, with mean total costs of $15,618 ± 25,264 for patients with 30-day readmission and $11,845 ± 22,710 for patients without readmission. These findings are consistent with our study, which also found both the higher costs associated with hypertension and readmission.
Another aspect to be addressed is the complications that end in fatal consequences. We have already mentioned the relationship between hypertension and stroke, stroke being a major public health problem and a problem that accounts for 10% of all deaths (17) Different studies (18, 19) established that approximately half of the patients analyzed had hypertension.
There are many factors to take into account when discussing hypertension and its associated costs. It has been well established that patients with hypertension have greater associated comorbidities, are admitted to hospital more often, and have higher morbidity and mortality rates.
Limitations
This study has limitations: first, inherent to the type of study, it cannot evaluate cause and effect relationships. Another limitation is that the study was a single-center study mainly due to the imminent need to know the evolution of the disease, and the costs in different autonomous communities or regions may vary. However, as they are public hospitals, the prices are usually subject to the Official State Gazette; therefore, we state that these variations are slight.
Finally, the creation of a specific The Electronic Data Collection Notebook (CRD) for the hospital itself and for this disease in particular means that we cannot compare it with other types of infections such as Influenza.
Conclusion
The results obtained provide evidence that tends to support our initial hypothesis that hypertensive patients admitted for SARS-CoV-2 respiratory infection would have a worse prognosis in terms of outcomes compared to normotensive patients, leading to higher healthcare costs for the hypertensive patient group. Our study shows the worse clinical evolution of patients with COVID-19 in terms of associated morbidity and mortality. It also shows that the cost of managing the complications observed in hypertensive patients is 3.2 times higher than in normotensive patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Clinical Research Ethics Commitee of LPUH, Madrid, with LPUH code: PI-4155. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
JC-M: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Writing – original draft, Writing – review & editing. MD-R: Investigation, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. RJ-V: Funding acquisition, Methodology, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing. CT-G: Validation, Visualization, Writing – original draft. RV-H: Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. AB-E: Funding acquisition, Project administration, Writing – original draft. PS-C: Investigation, Supervision, Validation, Writing – original draft. VA-F: Data curation, Investigation, Validation, Writing – original draft. VG-C: Data curation, Writing – original draft. JS-S: Writing – original draft, Investigation. MQ-D: Project administration, Supervision, Writing – original draft, Writing – review & editing. EA-E: Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Schiffrin, EL, Flack, JM, Ito, S, Muntner, P, and Webb, RC. Hypertension and COVID-19. Am J Hypertens. (2020) 33:373–4. doi: 10.1093/ajh/hpaa057
2. Wang, D, Hu, B, Hu, C, Zhu, F, Liu, X, Zhang, J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061–9. doi: 10.1001/jama.2020.1585
3. Zhang, J-J, Dong, X, Cao, Y-Y, Yuan, Y-D, Yang, Y-B, Yan, Y-Q, et al. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy. (2020) 75:1730–41. doi: 10.1111/all.14238
4. Zhou, F, Yu, T, Du, R, Fan, G, Liu, Y, Liu, Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
5. Guan, W-J, Ni, Z, Hu, Y, Liang, W, Ou, C-Q, He, J, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
6. Onder, G, Rezza, G, and Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. (2020) 323:1775–6. doi: 10.1001/jama.2020.4683
7. Boscá, JE, Doménech, R, Ferri, J, and García, JR. Shifts in the beveridge curve in Spain and their macroeconomic effects. Revista de Economía Aplicada. (2017) 25:5–27.
8. Calderón-Moreno, J, Juárez-Vela, R, Delgado-Rodríguez, MJ, Quintana-Díaz, M, Magallón-Botaya, R, Olivan-Blázquez, B, et al. Approximation to the consumption of healthcare resources and the economic cost of SARS-CoV-2 patient management: a retrospective study. Front Public Health. (2022) 10:751. doi: 10.3389/fpubh.2022.843751
9. Gallo, G, Calvez, V, and Savoia, C. Hypertension and COVID-19: current evidence and perspectives. High Blood Press Cardiovasc Prev. (2022) 29:115–23. doi: 10.1007/s40292-022-00506-9
10. Badía, X, Rovira, J, Tresserras, R, Trinxet, C, Segú, JL, and Pardell, H. The cost of arterial hypertension in Spain. Med Clin (Barc). (1992) 99:769–73.
11. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. (2021) 398:957–80. doi: 10.1016/S0140-6736(21)01330-1
12. Drozdz, D, Alvarez-Pitti, J, Wójcik, M, Borghi, C, Gabbianelli, R, Mazur, A, et al. Obesity and Cardiometabolic risk factors: from childhood to adulthood. Nutrients. (2021) 13:4176. doi: 10.3390/nu13114176
13. Lee, JH, Kim, KI, and Cho, MC. Current status and therapeutic considerations of hypertension in the elderly. Korean J Intern Med. (2019) 34:687–95. doi: 10.3904/kjim.2019.196
14. Salazar, M, Barochiner, J, Espeche, W, and Ennis, I. COVID-19, hipertensión y enfermedad cardiovascular [COVID-19 and its relationship with hypertension and cardiovascular disease]. Hipertens Riesgo Vasc. (2020) 37:176–80. doi: 10.1016/j.hipert.2020.06.003
15. Slivnick, J, and Lampert, BC. Hypertension and heart failure. Heart Fail Clin. (2019) 15:531–41. doi: 10.1016/j.hfc.2019.06.007
16. Kwok, CS, Abramov, D, Parwani, P, Ghosh, RK, Kittleson, M, Ahmad, FZ, et al. Cost of inpatient heart failure care and 30-day readmissions in the United States. Int J Cardiol. (2021) 329:115–22. doi: 10.1016/j.ijcard.2020.12.020
17. Mozaffarian, D, Benjamin, EJ, Go, AS, Arnett, DK, Blaha, MJ, Cushman, M, et al. Heart disease and stroke statistics-2015 update: a report from the American Heart Association. Circulation. (2015) 131:e29–e322. doi: 10.1161/CIR.0000000000000152
18. Holloway, RG, Benesch, CG, Burgin, WS, and Zentner, JB. Prognosis and decision making in severe stroke. JAMA. (2005) 294:725–33. doi: 10.1001/jama.294.6.725
Keywords: healthcare economics and organizations, economics, hospital, COVID-19, public health administration, cost of illness
Citation: Calderón-Moreno J, Delgado-Rodriguez MJ, Juárez-Vela R, Tejada-Garrido CI, de Viñaspre-Hernández RR, Burgos-Esteban A, Sánchez-Conde P, Andreu-Fernández V, Gea-Caballero V, Santos-Sanchez JA, Quintana-Diaz M and Andrés-Esteban EM (2024) Approximation to the economic cost of healthcare for hypertensive patients diagnosed with COVID-19. Front. Public Health. 12:1333081. doi: 10.3389/fpubh.2024.1333081
Edited by:
Hai Fang, Peking University, ChinaReviewed by:
Eduardo Gutiérrez-Abejón, Universidad de Valladolid, SpainStyliani A. Geronikolou, National and Kapodistrian University of Athens, Greece
Copyright © 2024 Calderón-Moreno, Delgado-Rodriguez, Juárez-Vela, Tejada-Garrido, de Viñaspre-Hernández, Burgos-Esteban, Sánchez-Conde, Andreu-Fernández, Gea-Caballero, Santos-Sanchez, Quintana-Diaz and Andrés-Esteban. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amaya Burgos-Esteban, YW1heWEuYnVyZ29zQHVuaXJpb2phLmVz