 Mekdes Mengesha Jemberie1
Mekdes Mengesha Jemberie1 Meseret Zewdu
Meseret Zewdu Bayew Kelkay Rade
Bayew Kelkay Rade- 1Tibebe Gihon Specialized and Comprehensive Hospital, Bahir Dar University, Bahir Dar, Ethiopia
- 2Department of Gender and Developmental Studies, Faculty of Social Science, Bahir Dar University, Bahir Dar, Ethiopia
- 3Department of General Midwifery, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Background: Sexual and reproductive health rights (SRHRs) are integral elements of the rights of everyone to the highest attainable standard of physical and mental health, but they are the most underdeveloped and least understood sphere of rights, especially in Africa, including the country of Ethiopia. The implementation of women’s SRHRs is essential for achieving gender equality and promoting women’s rights. Husbands’ knowledge and involvement play a significant role in improving women’s practice of their SRHRs. However, there is limited information/data about the level of husbands’ knowledge and involvement in Northwest Ethiopia, including Bahir Dar City. Therefore, this study aimed to assess husbands’ knowledge, involvement, and factors influencing their involvement in women’s SRHRs.
Methods: Community-based cross-sectional study design was conducted from March 20 to April 5, 2023, in Bahir Dar City, Northwest Ethiopia, among 391 husbands. Multi-stage sampling and simple random sampling technique were applied to select kebeles and study participants, respectively. Participants were interviewed face-to-face using structured and pretested questionnaire. Binary logistic regression was applied to identify associated factors, and a p-value of <0.05 was a cutoff point to declare statistical significance.
Results: In this study, 50.6% (198/391) of the husbands had good knowledge about their wives’ SRHRs and 44.2% (173/391) (95% CI, 39.3–49.1%) of the husbands were involved when their wives practiced their SRHRs. Access training/education about sexual health [AOR = 5.99; 95% CI (2.7–13.2)], husbands’ advance educational level [AOR = 8.81; 95% CI (2.04–38)], good knowledge about SRHRs [AOR = 7.94; 95% CI (4.3–14.4)], low monthly income (<4,600 birr) [AOR = 9.25; 95% CI (4.2–20.5)], and had open discussion with family members and friends about SRHRs [AOR = 1.92; 95% CI (1.01–3.6)] were found to have significant association with husbands’ involvement.
Conclusion: Husbands’ level of knowledge on SRHRs of women and their involvement remain low. Therefore, responsible concerned bodies need to work on the strategies that help to improve men involvement and knowledge, and tackle the above-mentioned factors influencing their involvement.
Introduction
The global maternal mortality rate (MMR) in 2020 was estimated 223 per 1,000,000 live births, and sub-Saharan African region have reported extremely high MMR, which was over 1,000 (1). According to mini-2019-Ethiopian Demographic Health Survey (EDHS) report, MMR accounts 412 per 100,000 live births (2). This is because polices, programs, and strategies were not giving special attention to women and their roles for improving reproductive health rights; result high maternal morbidities and mortalities. Women sexual and reproductive rights need special attention since the violation occurred worldwide and have serious consequence on women’s health (3, 4).
Sexual and reproductive health rights (SRHRs) are defined as “these are the rights of sexual and reproductive health, that includes the right to freely control and responsibly decide on matters related to sexuality, including sexual and reproductive decision-making and the ability to seek sexual and reproductive healthcare; information, counseling, and care related to sexual function and satisfaction; prevention, detection, and management of sexual and gender-based violence and coercion; a choice of safe and effective contraceptive methods; safe and effective antenatal, childbirth and postnatal care; safe and effective abortion and post-abortion care services; prevention, management and treatment of infertility, sexual transmitted infections (STIs), including human immunodeficiency virus (HIV) infection; and prevention, screening, and treatment of reproductive cancers like cervical cancer” (5, 6). About 4.3 billion of reproductive age women globally have inadequate SRH services for their lives, and there is relatively low access in the low- and middle-income countries (LMICs) (7). In history, men focused almost exclusively on women’s fertility, and family planning program policies were implemented with limited male involvement (8). Evidence revealed that knowing husband’s understanding of his wife’s reproductive rights can aid in planning and intervening on maternal healthcare needs during pregnancy, childbirth, and afterward (9). Moreover, male involvement related to the practice of maternal healthcare service uptake and nutritional health has a positive association in reducing maternal and child morbidity and mortality (10). The large body of evidence said that women’s practice of their SRHRs is low without explaining men’s involvement because the source of data was only from women (11). In Nigeria, husbands’ involvement on safe motherhood was 26.3%-antenatal care (ANC), 19%-nutrition, and 4.6%-involved in family planning. Nearly, three-fourths (74.8%) of the husbands had poor knowledge of safe motherhood initiative practices (12). Husbands’ lack of knowledge on wives’ reproductive health right is the public health concern in Ghana, and 53.8% had poor knowledge about human rights and 66.7% denial of SRHRs services (13). The study carried out in Harar revealed that the level of husbands’ involvement in women SRHRs was 40.1% (14). Study among university students in Ethiopia also highlighted that 45.5% of them have no adequate knowledge on sexual and reproductive rights (9). Some literatures revealed that media exposure, high level of education, positive attitude, good knowledge and awareness, good sociocultural factors, and good policies play important roles in improving male involvement in women sexual and reproductive health rights (15–17). Generally, women are facing a challenge in exercising their SRHRs because they have less power in relationship due to their economic, political and sociocultural status that results gender disparities which strongly affect SRHRs of women (18). Husbands are the main household decision-makers in various cultures of many countries, including Ethiopia, which affect wives to exercise their reproductive health rights and cause morbidity and mortality of women (9, 13).
Husbands and wives in Ethiopia are openly communicating on different issues in life, but not focused on reproductive health rights (RHRs). Past studies determined women’s knowledge and their practice of SRHRs and reported that male dominance in women’s decision-making on sexual reproductive health rights (SRHRs) was proximal factor for poor practice of SRHRs. The implementation of proper and effective promotion of men involvement in the protection of women’s reproductive rights needs a baseline data of husbands’ knowledge, involvement, and related factors. However, little is known about the issue in Ethiopia at large and in Bahir Dar city specifically. Therefore, this study aimed to assess husband’s knowledge on women SRHRs, husbands’ involvement when their wives practice their SRHRs and to identify factors associated with husbands’ involvement in Bahir Dar City, Northwest Ethiopia.
Methods
Study, setting, design, and period
Community-based cross-sectional study design was employed in Bahir Dar city, Ethiopia. Bahir Dar is the capital of Amhara administrative regional state, located 563 km away from Addis Ababa. According to the Bahir Dar City Municipality office 2019\2020 report, Bahir Dar city has 6 sub-cities and 26 kebeles with a total population of 312,410; of these, 145,579 are male individuals. According to Bahir Dar sub-cities’ administrative 2021/22 report, 99, 238 married male households are living in the city. As per Bahir Dar City administrative health department report, there are 23 governmental health facilities and four private hospitals and few more private clinics. From 23 governmental health facilities: three hospitals, ten health centers, and ten health posts. The health facilities provide various reproductive health services based on the capacity of health facilities in terms of available human resources and equipment including essential drugs. The services are including counseling and provision of contraception, STIs including HIV/AIDS testing and management, safe motherhood service (antenatal, intrapartum and postnatal), cervical cancer screening and treatment, infertility screening and treatment, safe abortion and post-abortion care services, and effective referral linkage. The data were collected from March 20 to April 5, 2023.
Source and study population
All men who were married and had at least one child in Bahir Dar city were the source population, while all men who fulfilled the above criteria and lived in randomly selected sub-cities were the study population.
Inclusion criteria
Those husbands, who were married, lived in the city at least for the past 6 months preceding the survey and had at least one child included in this study.
Sample size determination and sampling procedure
The sample size (n) for this study was calculated using single Kothari formula
and this formula used for finite population, considered; proportion (p) 40.1% which was husbands’ level of involvement in Harar, East Ethiopia (14), 95% level of confidence (1.96), and 5% margin of error.
By considering a 10% non-response rate, the final sample size for this study was 403.
Regarding sampling procedure, Bahir Dar City has six sub-cities, and three sub-cities were selected by lottery method. The total sample size was allocated proportionally to each sub-city based on the total married men living in each sub-city (Figure 1).
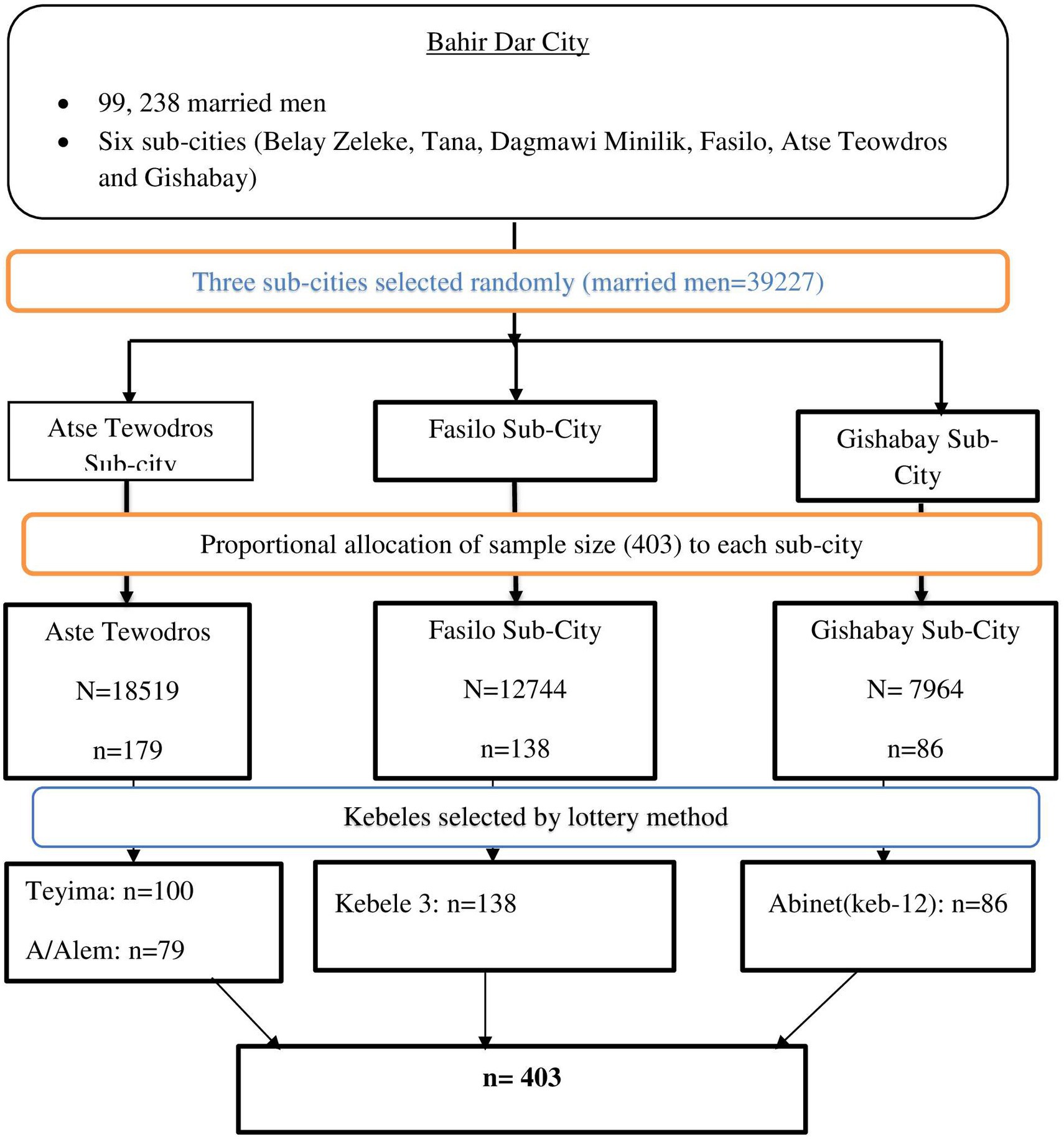
Figure 1. Schematic presentation of sampling procedure in Bahir Dar city, 20,223.
Sampling techniques
A multi-stage sampling technique was used to select sub-cities from six sub-cities. In the first stage, three sub-cities were selected from Bahir Dar city using a lottery method by considering the rule of thumb of 30% coverage of representative of the study population. In the second stage; four kebeles were selected from three sub-cities using lottery method. The total calculated sample husbands were allocated proportionally to each kebeles based on the total number of households. In the third stage, total numbers of married households were taken from each kebele administration using simple random sampling method until the allocated sample size was reached. When each selected household had more than one respondent (study unit), one person was selected by the lottery method at the time of data collection. In non-response after the repeated visit (two times), the individual was considered non-response.
Study variables
Husband involvement in their wives’ SRHRs was the outcome variable; while socio-demographic and economic-related variables (age, income, husband’s father raised up, educational level, occupation, religion, and types of marriage); source of information-related variables (exposure to media, training/education on SRHR, open discussion with family members and friends); and Knowledge on SRHRs were independent variables.
Data collection tool and procedure
The data collection tool for this study was adapted from prior published international literatures (9, 14, 17, 19–22). The primary source of information/data for this study was husbands. The data were collected using translated to local language (Amharic) and pretested structured questionnaire through face-to-face interview. One-day training was given for two male data collectors and one supervisor who had data collection and supervision experiences. The data collection procedure was done in private rooms/areas since the topic was sensitive.
Definition of terms
Reproductive right
It is the right of an individual to decide and choose about reproduction free of discrimination, coercion, and violence (23).
Reproductive health
It is a state of complete physical, mental, and social wellbeing not merely the absence of diseases and infirmity in all matters of relating to the reproductive system and its functions and process (24, 25).
Sexual health
It is a positive approach to human sexuality, and the purpose of sexual healthcare should be to enhance life and personal relations, counseling and care related to reproduction and sexually transmitted diseases (25).
Sexual rights
Embrace human rights that are already recognized in national laws, international human rights documents, and other consensus documents. These include the right of all persons, to be free of coercion, discrimination, and violence, to live to the highest attainable standard of health in relation to sexuality, including access to sexual and reproductive healthcare services; seek, receive, and impart information in relation to sexuality; sexuality education; respect for bodily integrity; choice of partner; decide to be sexually active or not; consensual sexual relations; consensual marriage; decide whether or not, and when to have children; and pursue a satisfying, safe, and pleasurable sexual life (25).
Sexuality
It is a central aspect of being human throughout life and encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy, and reproduction. Sexuality is experienced and expressed in thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships. It can be influenced by the interaction of biological, psychological, social, economic, political, cultural, ethical, legal, historical, religious, and spiritual factors (25).
Sexual and reproductive health
It is a state of physical, mental, emotional, and social wellbeing about sexuality and reproduction (24).
Sexual and reproductive health rights
These are the rights of sexual and reproductive health, which includes the right to freely control and responsibly decide on matters related to sexuality, including sexual and reproductive decision-making and the ability to seek sexual and reproductive healthcare that is free of coercion, discrimination, violence, the number of babies, and spacing (6).
Operational definition
Discussion with family members and friends
Refers to a discussion on sexual and reproductive health issues with husband/male involvement and initiated by himself or friends or any family members including women, reproductive aged daughters, or/and sons,
Measurements
Knowledge of husband
It was measured using 22 standard reproductive right questions, each scored 1 or 2 (1 = no and 2 = yes). Those who scored above the total mean (>1.73) value of knowledge-measuring questions were considered knowledgeable; otherwise, they were considered not knowledgeable (14, 26).
Husband’s involvement
It is husband’s activity or support in his wife’s SRHRs when the wife practices her SRHRs at home and workplace. The outcome variable was coded as 1 = No, 2 = Yes of husband’s involvement after computing thirteen (13) involvement Likert scale questions were used to assess husbands’ level of involvement when their wives’ practice their SRHRs and each item scored 1 to 5(1 = never, 2 = rarely, 3 = sometimes, 4 = often, and 5 = always). The study participants’ minimum and highest possible score were 13 and 65, respectively (14, 26, 27). Husbands’ who scored above median (>2) of involvement-measuring questions were categorized as having good involvement (Yes = 2) in their wives’ sexual and reproductive rights.
Data analysis and presentation
The data were coded and entered Epi-data version 4.6 and exported to the Statistical Package for Social Sciences (SPSS) version 25 software for analysis. Descriptive data analysis (frequency and percentage) was used to extract values from the raw data. Both bivariate and multivariate logistic regression models were done to estimate the association between independent variables and outcome variable (husbands’ involvement). Independent variables with p-value of less than 0.25 in the bi-variable analysis were entered into the multivariable logistic regression analysis and p-value <0.05 was cutoff point to declare statistical significance in the final regression model. Backward elimination (Backward LR) was applied in multivariable analysis to control confounding variables. Hosmer–Lemeshow model test with p-value >0.05 showed fitted model with this study p-value of 0.121. Finally, adjusted odd ratio (AOR) with 95% CI was used to show the strength of association between the outcome and independent variables.
Data quality control
The quality of data was assured by different mechanisms. The questionnaire was first prepared in English and translated into Amharic (local language) and retranslated to English to check its consistence. Then, the questionnaire was pretested among 5% (21 participants) of the sample size in kebel-7, Bahir Dar before the start of actual data collection, and we made minor modifications to its content. One-day training was provided for data collectors and supervisors. The data collection process was supervised closely, and the completeness of each questionnaire was checked by the investigator and supervisor on a daily basis. The content and technical aspect of the tool was reviewed by experts. Internal consistency of Likert scale category of variables was checked using the Cronbach alpha value of 0.849.
Results
Socio-demographic and economic characters of participants
A total of 391 out of 403 husbands participated in this study with a response rate of 97.02%. In total, 241 (61.1%) of the study participants’ father grew up in rural area, and 161 (41.2%) of study participants’ fathers were unable to read and write due to their educational status. The mean age of the study participants was 41.77 years with (SD ± 11.68), and 115 (29.4%) of the study participants were with age range of 40–49 years. More than half (59.8%) of the study participants lived together with their wives between 5 and 25 years. Nearly, one-fourth (24%) of the study participants were first degree by educational level, and more than two-thirds (67%) of the study participants were orthodox Christian religion followers. Regarding occupation, 183(46.8%) of the study participants were engaged in personal business activity, and more than one-thirds (37.3%) of the study participants had arranging marriage by type. Lastly, six in ten (59.3%) of the study participants’ monthly income was > or = 4,600 Ethiopian birr (Table 1).
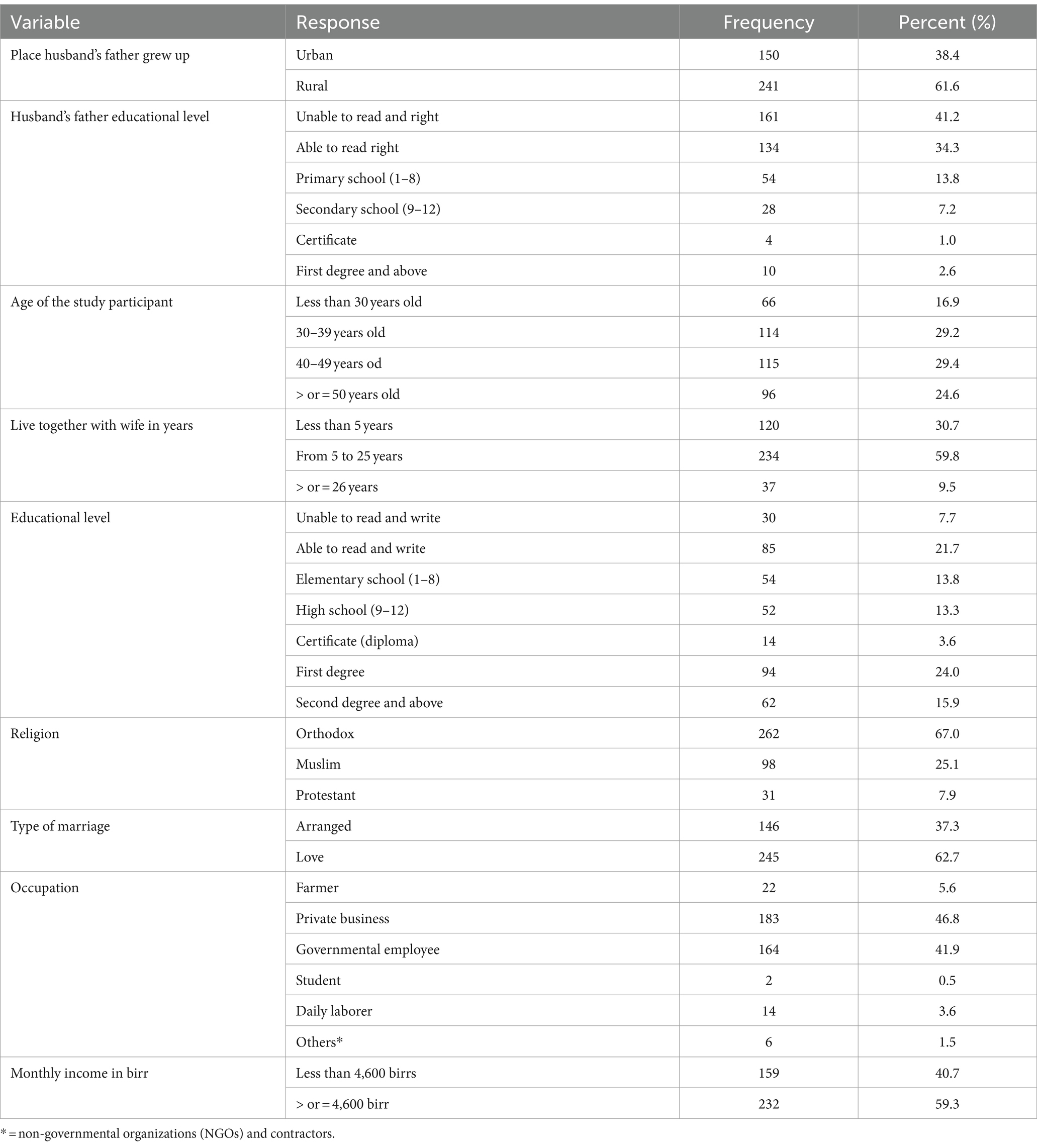
Table 1. Socio-demographic and economic-related factors of the study participants and their extended families in Bahir Dar city, Ethiopia, 2023 (N = 391).
Source of information and husbands’ knowledge on SRHRs-related characteristics
Nearly, three-fourths (73.4%) of the study participants did not access any training/education opportunity about reproductive health, and almost two-thirds (63.9%) of the study participants did not discuss with their friends and/or family members about SRHRs.
Regarding husbands’ knowledge on SRHRs, 198 (50.6%) of them had good knowledge after computing knowledge assessment questions. More than three-forth (76.7%) of the respondents replied that they aware about women SRHRs without verified the components. Among those who aware about women SRHRs, health institutions (72.3%) were the leading source of information followed by 182(60.7%) mainstream media (radio and Television). Of the total 370 husbands who knew that their wives have the right to use their choice of family planning methods, 281 (75.9%) knew injectable type of family planning method. Almost one-fifth (23.8%) of the study participants did not know that their wives have the right to receive screening and treatment of STIs including HIV/AIDS and urinary tract infections (UTIs). More than three-fourth (77.2%) of the study participants knew that they and their wives have equal reproductive health rights and 177 (45.3%) of the husbands did not know about their wives have the right to enjoy and control their sexual and reproductive life. Almost half (48.8%) of the study participants did not know that having sex whenever they want irrespective of their wives’ will be punishable by the law. More than half (57.8%) of the husbands did not know that forced marriage and/or abusive sexual language is punishable by law. Finally, three-fourth (73.1%) of the study participants did not aware about safe abortion with certain conditions is legal by law in Ethiopia (Table 2).
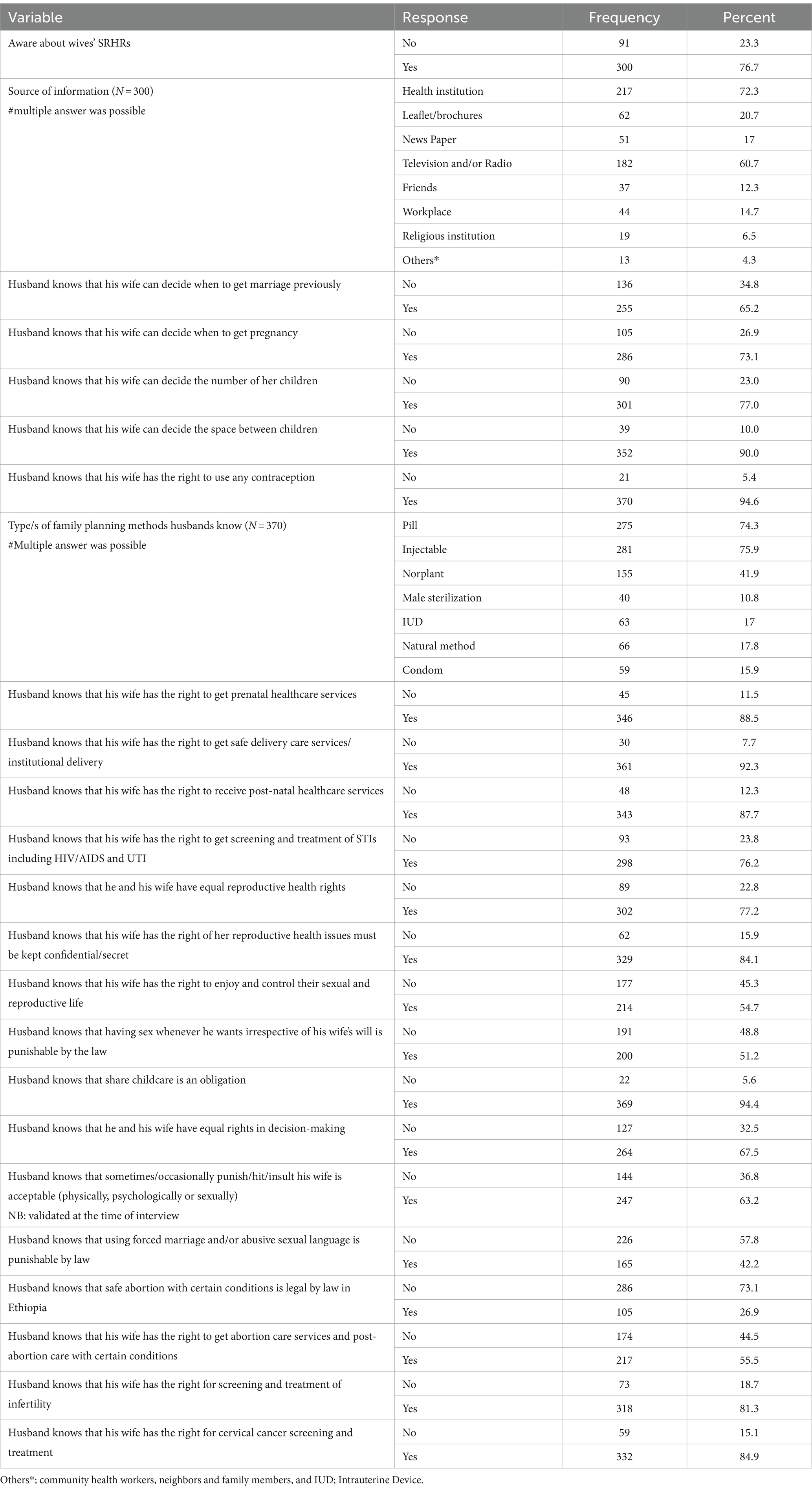
Table 2. Source of information and knowledge of study participants on SRHRs, Bahir Dar city, Ethiopia, 2023 (N = 391).
Husbands’ involvement in wives SRHRs
Of the overall respondents, 173(44.2%) were involved in their wives SRHRs (Figure 2).
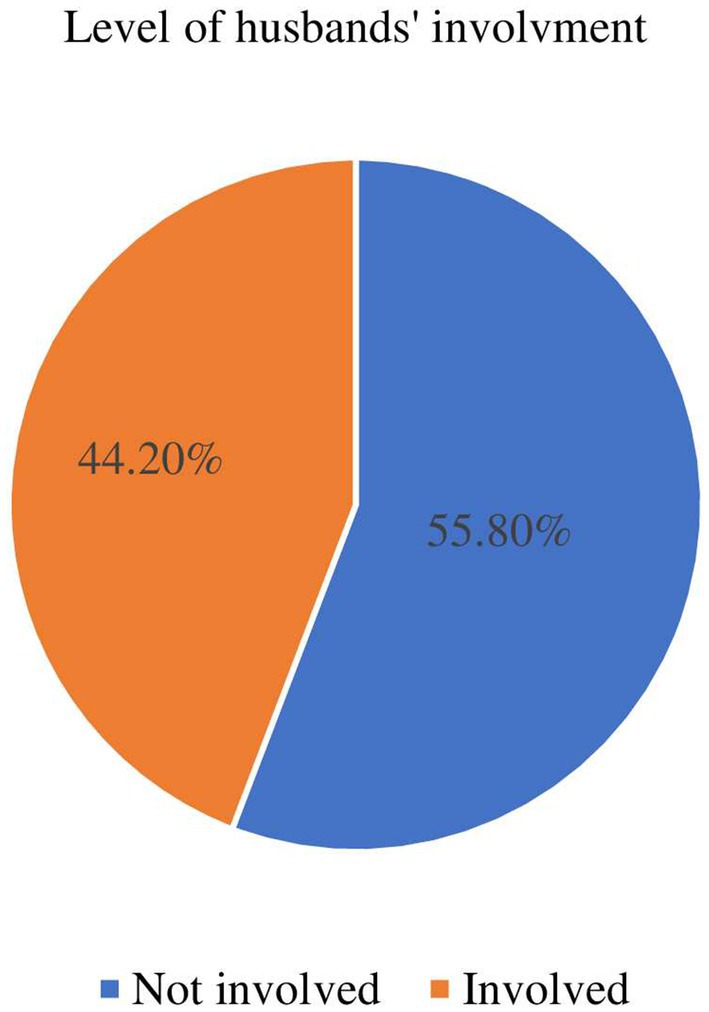
Figure 2. Husbands’ level of involvement in their wives SRHRs in Bahir Dar City, Ethiopia, 2023 (N = 391).
From Likert scale questions, a total of 192 (49.1%) study participants were not reminding where and when family planning services are needed for their wives. More than half (57.6%) of the participants never had sex whenever they need irrespective of wives’ interest. Half (50.6%) of the husbands were not encouraging their wives to get reproductive health-related information/education. Regarding antenatal visit, more than one-thirds (38.6%) of husbands had never gone with their wives for ANC follow-up; of these, 60 (39.7%) mentioned that havening ANC follow-up is females’ job as a reason for not involved. In total, 118 (30.8%) of the husbands did not go with their wives for institutional childbirth service ever and 91 (23.3%) were not involved in PNC follow-up. A promising finding in this study was that 138 (35.3%) husbands often supported their wives when they breastfed. Sixty-two (15.9%) of the husbands did not involve in their wives screening/testing for STIs, including HIV/AIDS and of these, 26 (41.9%) respondents mentioned busy for other duties as a reason for not being involved. More than half (51.9%) of the husbands never discussed openly with their wives about sexual desire and when to have sex and only 92 (23.5%) study participants were always ready to go with their wives if they need cervical cancer screening and treatment (Table 3).
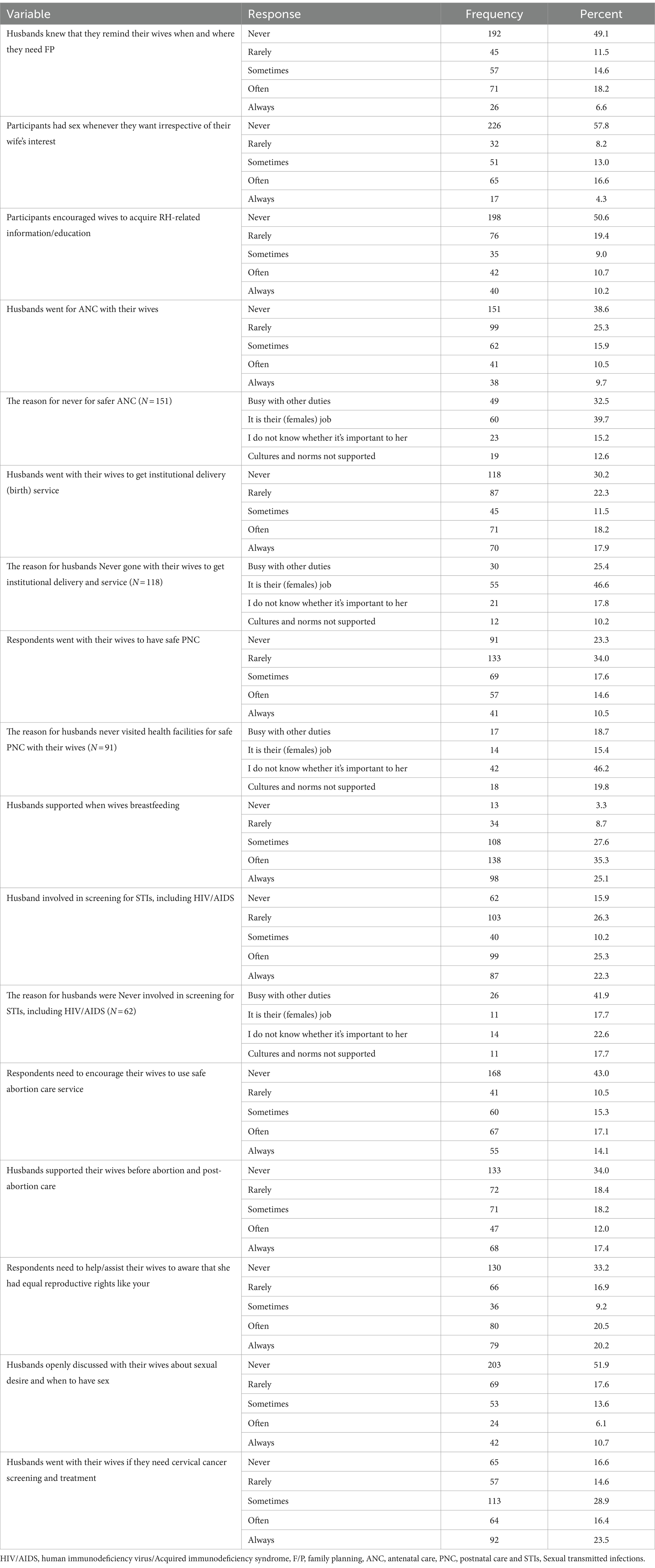
Table 3. Husbands’ involvement by each Likert scale measurement items in Bahir Dar City, Northwest Ethiopia, 2022/23(N = 391).
Factors affecting husbands’ involvement in their wives SRHRs
Binary (bivariate and multivariate) logistic regression was run to identify factors associated with the outcome variable. In bivariate logistic regression, six variables were associated with p-value less than 0.25. After controlling confounding factors, five variables were significantly associated with outcome variable in multivariate logistic regression at p-value <0.05. Those who had a monthly income of <4,600 Ethiopian birrs were 9.25 times more likely to involve in their wives SRHRs compared to those who had > or = 4600birr monthly income with [AOR = 9.25; 95% CI (4.17–20.5)]. Study participants who had second degree and above by educational level were 8.8 times more likely to involve in their wives SRHRs compared with those who were unable to read and write husbands [AOR = 8.8; 95% CI (2.04–38)]. The odds of study participants involvement in their wives SRHRs were almost 6 times higher among those who accessed training/education opportunity about reproductive health compared to those who did not with [AOR = 5.99; 95% CI (2.71–13.2)]. The study participants who had open discussion about SRHRs with family members and/or friends were 1.92 times more likely to involve in their wives SRHRs compared with those who had not get discussion with [AOR = 1.92; 95% CI (1.01–3.63)]. Finally, the odds of involvement were 7.9 times higher among those who had good knowledge on SRHRs issue compared with their counterparts with [AOR = 7.9; 95% CI (4.28–14.4)] (Table 4).
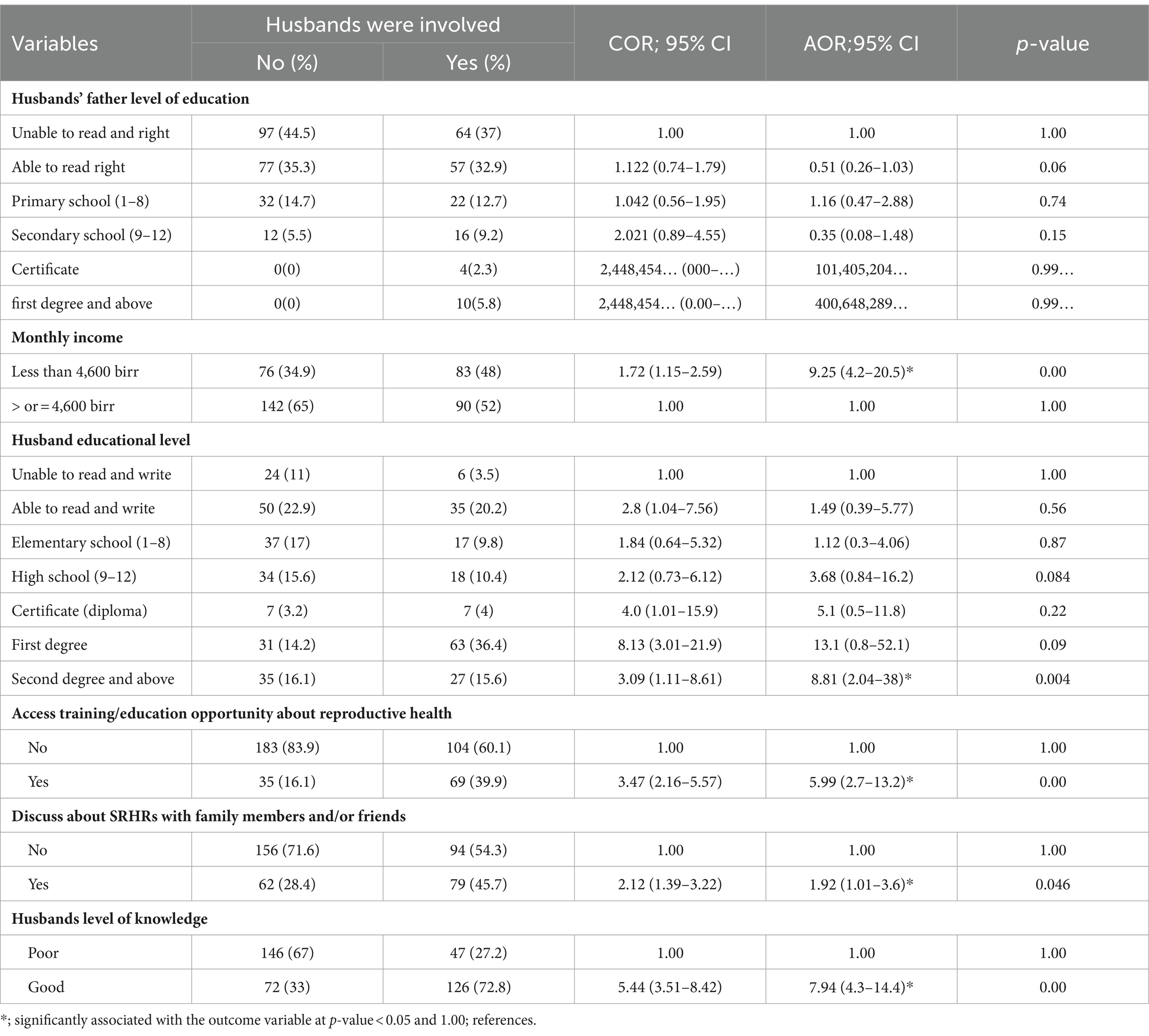
Table 4. Regression table shows the association between independent and dependent variables, Bahir Dar City, 2023.
Discussion
This study was conducted using a quantitative study approach that intended to assess husbands’ knowledge and involvement and factors influencing husbands’ involvement in their wives sexual and reproductive health rights in Bahir Dar city, Northwest Ethiopia. The level of husbands’ involvement and knowledge was 44.2% (95% CI; 39.3–49.1%) and 50.6% (95%CI, 48.07–53.13%), respectively. Husbands’ level of education, monthly income, access of training/education opportunity about reproductive health, had open discussion about SRHRs with family members and/or friends, and husbands’ level of knowledge were the factors significantly associated with husbands’ involvement.
The level of knowledge in this study is in line with the study conducted in Harar, Eastern, Ethiopia (48.3%) (14). These similarities might be due to short time gap, similar study population (urban resident), and the study participants were married husbands in both studies. However, this study is lower than the study conducted in Wolaita Sodo, Ethiopia (54.5%) (9), Gondar, Ethiopia (57.7%) (28), Adet Tana Haik (59.6%) (29), Debre Markos, Ethiopia (67%) (30), and Ghana (80%) (13). The difference might be due to variation of study population socio-demographic profile, gender of study participants, and study design. The study conducted in Gondar, Wolaita Sodo, Debre Markos, and Adet was among university and college students who aimed to assess their knowledge on female SRHRs. College/university students usually participated or members in reproductive health clubs, which may give more opportunity to understand girls/women’s SRHRs. Moreover, students may have SRHRs information exposure from their class courses, life skill trainings and communication/discussion with their friends/peers. The difference with Ghana might be due to study design and study population, both sexes of adolescent students were involved in the study. On other hand, the level of knowledge in this study is higher than the study conducted in Sri Lanka (24.4%) (20), Nepal (37%) (23), India (9.1%) (26), Nigeria (45.2%) (17), and shire town, Northern Ethiopia (47.1%) (31). This might be because of cultural, socio-demographic profile of the study population, study area, and year of study differences.
Level of husbands’ involvement in this study is in line with the study conducted in Bangladesh (40%) (32), Bale zone, Southern Ethiopia (41.4%) (16), Afar, Ethiopia (42.2%) (21), and Harar, Eastern Ethiopia (40.1%) (14). The plausible reason for the similarity might be due to the same socio-economic background of study population, and all studies were conducted in recent years. However, the level of involvement in this study is lower than studies conducted in Nepal (57.6%) (33), Debre Markos, Northwest Ethiopia (60%) (34) and Tanzania (69%) (35). The probable reasons for the difference might be sociocultural and economic status, husbands’ level of education, time/year of study, the accessibility and implementation of SRHRs components. The study conducted in Debre Markos; Northwest Ethiopia was not evaluated all components of SRHRs rather specific on family planning involvement, while the study conducted in Nepal and Tanzania are better in implementation of laws and regulation and done on single component of SRHRs which was antenatal follow-up. Probably religious norms are also the barriers for low involvement of husbands in SRHRs. In this study, more than two-thirds (67%) of the study participants were orthodox Christian religion followers. One study in Afar, Ethiopia revealed that religious leader husbands were 30% less likely to involve during their wife’s family planning service uptake compared with husbands who were not religious leaders (21). Beside this, poor health system and not having a health policy that encourages the practice of SRHRs in Ethiopia may be another reason for low husbands’ involvement. On the other side, this study is higher than the study conducted in Ghana (20%) (19) and Harar, Eastern Ethiopia (19.7%) (36). The probable reason for the discrepancy might be due to cultural differences, quality and availability of healthcare service infrastructures, sample size, and component of SRHRs were assessed. The study conducted in Ghana was on husbands’ involvement in postnatal care service utilization which is one component of SRHRs. One study highlighted that cultural standards were identified as a barrier for male involvement (37).
The regression analysis showed that husbands who had <4,600 Ethiopian birr monthly income were more likely to involve in their SRHRs compared with those who had monthly income of > or = 4,600 birr. This study agrees with qualitative study conducted in Nepal (38) that showed; “mostly males are involved in income generation, they do not have enough time and no concerns about wives SRHRs.” The likely reason for the association might be that husbands with better monthly income could be busy with different duties/responsibilities and give their time for generating money over helping their wives.
Education is an important instrument/strategy to know about something and to change the mind set of human behavior. Husbands who had advanced educational level were 8.8 times more likely to be involved in their wives SRHRs when compared to their counterparts. This finding is supported with the study conducted in Nepal (33) and Tanzania (35). One study reported that adequate information on SRHRs directly impacts the involvement of sexual and reproductive rights, changing attitude, and overcoming some sociocultural-related barriers (21).
Those husbands who accessed training/education opportunities about reproductive health were 6 times more likely to be involved in their wives SRHRs compared with their counterparts. This finding is supported with study conducted in Myanmar, Nepal and Malawi (39, 40). The plausible reason for the association could be the more the husbands have knowledge on SRHRs would have the better involvement. The study participants who had open discussion about SRHRs with family members and/or friends were 1.92 times more likely to involve in their wives SRHRs compared with who did not have discussion, which agrees with studies conducted in Harar, Ethiopia (14), Bangladesh (32), and India (41). The probable reason could be those who had an open discussion with their friends and/or family about SRHRs may boost their knowledge and then yield good involvement in their wives SRHRs. One study proved that an open discussion between husbands and wives resulted good knowledge and involvement of the husbands on women reproductive issues (28). Another study also proved that poor communication between husband and their female partners was associated with poor male involvement (34). Finally, in this study, the odds of involvement were 7.9 times higher among those who had good knowledge on SRHRs issue compared to their counterparts. This finding is agreed with the study conducted in Afar, Ethiopia (21), Nigeria (17), Nepal (38) and Myanmar (39). It is obvious that when the level of husbands’ knowledge increased, the possibility their involvement in their wives SRHRs could be also increased.
Implication of the study
National and International conventions recommend husband involvement is necessary in women’s SRHRs; however, more efforts are needed to implement different international conventions. At community level; community leaders should create awareness about traditional, cultural practice norms and barriers affecting husbands’ involvement in wives SRHRs. Finally, legal affairs and women federation must adopt policies and strategies that sustained the presence of husband involvement in SRHRs through education/trainings. The government needs to develop a male involvement strategy to encourage and support men and boys to take responsibility of their sexual and reproductive behavior and to abstain from all forms of discrimination against women and girls. Husbands’ knowledge and involvement in their wives SRHRs increase their awareness, acceptance and support to their partner’s needs, choices, and rights. Men participation in women SRHRs encourages prompt care in wives’ safe motherhood services. An engaged father who feels responsible for and behaves responsibly toward his child, is emotionally engaged and physically accessible, involved in childcare, rearing provides material and support to sustain the children’s needs.
Limitations of the study
This study has some limitations. The study setting was urban; therefore, the finding could not be generalizable for rural husbands. Moreover, the study did not show a real cause-and-effect relationship due to the nature of the study design, which was a cross-sectional study. Finally, due to the nature of the topic sensitivity, this study might introduce reporting bias despite all efforts to minimize it.
Conclusion
In this study, the level of husbands’ knowledge and involvement in their wives’ SRHRs were low. Access training/education about sexual health, husbands’ advance educational level, having good knowledge about SRHRs, low monthly income (<4,600 birr), and open discussion with family members and friends about SRHRs were significantly associated with husbands’ involvement when their wives exercise SRHRs. Therefore, responsible concerned bodies need to work on the strategies that help to improve men involvement and knowledge, and tackle the above-mentioned factors influencing their involvement.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The ethical approval letter for this study was obtained from the Ethical Review Committee of the Bahir Dar University (reference number: GDS-25/15). Permission letters were received from each selected sub-cities. The study was conducted in accordance with local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MJ: Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. MZ: Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. BR: Data curation, Formal analysis, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We acknowledge Bahir Dar city for the permission they gave to conduct the study and providing all necessary information/data such as household numbers. We would also like to thank data collectors, supervisors, and study participants.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ANC, Antenatal Care; AOR, Adjusted Odds Ratio; COR, Crude Odds Ratio; HIV/AIDS, Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome; PNC, Postnatal Care; SPSS, Statistical Package for Social Sciences; SRHRs, Sexual and Reproductive Health Rights; STIs, Sexual Transmitted Infections.
References
1. World Health Organization. Trends in maternal mortality 2000 to 2020: Estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/population division. Geneva: World Health Organization (2023) Licence: CC BY-NC-SA 3.0 IGO.
2. Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF. Ethiopia mini demographic and health survey 2019: Final report. Rockville, Maryland, USA: EPHI and ICF (2021).
3. UNFPA. ICPD beyond 2014; high-level global commitments. Implementing the population and development agenda. UNFPA (2016).
4. UNDP. National Human Development Report 2018: Ethiopia UNDP (Ethiopia: United Nations Development Programme) (2018).
5. UNFPA. Sexual and reproductive health and rights: An essential element of universal health coverage. New York, NY: United Nations Population Fund (2018).
6. IPPF. The men and boys collection: stories of gender justice and sexual and reproductive health and rights. London: United Kingdom (2014).
7. Ravindran, TKS, and Govender, V. Sexual and reproductive health services in universal health coverage: a review of recent evidence from low- and middle-income countries. Sex Reprod Health Matters. (2020) 28:1779632. doi: 10.1080/26410397.2020.1779632
8. Greene, ME, and Biddlecom, AE. Absent and problematic men: demographic accounts of male reproductive roles. Popul Dev Rev. (2000) 26:81–115. doi: 10.1111/j.1728-4457.2000.00081.x
9. Adinew, YM, Worku, AG, and Mengesha, ZB. Knowledge of reproductive and sexual rights among university students in Ethiopia: institution-based cross-sectional. BMC Int Health Hum Rights. (2013) 13:12. doi: 10.1186/1472-698X-13-12
10. Tokhi, M, Comrie-Thomson, L, Davis, J, Portela, A, Chersich, M, and Luchters, S. Involving men to improve maternal and newborn health: a systematic review of the effectiveness of interventions. PLoS One. (2018) 13:e0191620. doi: 10.1371/journal.pone.0191620
11. Nath, DC, Land, KC, and Goswami, G. Effects of the status of women on the first-birth interval in Indian urban society. J Biosoc Sci. (1999) 31:55–69. doi: 10.1017/S0021932099000553
12. Sokoya, MR, Farotimi, AR, and Ojewole, FR. Women’s perception of husbands’ support during pregnancy, labour and delivery. IOSR J Nurs Health Sci. (2014) 3:45–50. doi: 10.9790/1959-03314550
13. Yendaw, E, Martin, E, and Bagah, DA. Knowledge and perception of adolescents on sexual and reproductive health rights in Ghana: a case study of Yamoransa in the Mfantseman municipality. Br J Educ Soc Behav Sci. (2015) 8:147–58. doi: 10.9734/BJESBS/2015/16098
14. Mohammed, A, Alemayehu, T, Desalew, A, Debela, A, Sema, A, Belay, Y, et al. Knowledge and involvement of husbands in the reproductive rights of women in Harar, eastern Ethiopia. SAGE Open Med. (2021) 9:205031212110384. doi: 10.1177/20503121211038456
15. Hassan, II, Hussain, NHN, Sulaiman, Z, Kadir, AA, and Nor, MZM. Menopausal women’s experiences of husband’s support: a negative view. Enferm Clin. (2020) 30:190–3. doi: 10.1016/j.enfcli.2019.07.075
16. Kassahun, F, Worku, C, Nigussie, A, and Ganfurie, G. Prevalence of male attendance and associated factors at their partners antenatal visits among antenatal care attendees in bale zone, south East Ethiopia. Int J Nurs. (2018) 10:109–20. doi: 10.5897/IJNM2018.0323
17. Makinde, OA, and Adebayo, AM. Knowledge and perception of sexual and reproductive rights among married women in Nigeria. Sex Reprod Health Matters. (2020) 28:1–14. doi: 10.1080/26410397.2020.1731297
18. ICRW. What would a feminist foreign policy mean for sexual and reproductive health and rights? Suite 500 north. Washington: International Center for Research on Women (2020).
19. Craymah, JP, Oppong, RK, and Tuoyire, DA. Male involvement in maternal health Care at Anomabo, central region. Ghana Int J Reprod Med. (2017) 2017:1–8. doi: 10.1155/2017/2929013
20. Perera, U, and Abeysena, C. Knowledge, attitudes and perceptions of sexual and reproductive health rights among undergraduates in state universities in Sri Lanka. (2022).
21. Chekole, MK, Kahsay, ZH, Medhanyie, AA, Gebreslassie, MA, and Bezabh, AM. Husbands' involvement in family planning use and its associated factors in pastoralist communities of Afar, Ethiopia. Reprod Health. (2019) 16:33. doi: 10.1186/s12978-019-0697-6
22. Berhe, ET, Ayene, M, Gebregyorgis, T, Hagos, MG, and Gebremeskel, TG. Low-level knowledge and associated factor of sexual and reproductive health rights among Aksum university students, Aksum Ethiopia. Front Public Health. (2022) 10:860650. doi: 10.3389/fpubh.2022.860650
23. Kumar Yadav, R, Ram Gahatraj, N, Kumar Yadav, D, and Marahatta, SB. Knowledge and practice on reproductive heath rights among married women in Nepal. J Health Allied Sci. (2019) 5:53–7. doi: 10.37107/jhas.36
24. IPPF and UNFPA. Global sexual and reproductive health service package for men and adolescent boys. London and New York City: IPPF and UNFPA (2017).
25. WHO. Defining sexual health—Report of a technical consultation on sexual health 28–31 January 2002, Geneva. Sexual Health Document Series. Geneva: World Health Organization (2006).
26. Bhattarai, M, and Dhakal, R. Knowledge regarding reproductive rights among undergraduate students. Sch J Appl Med Sci. (2015) 3:2461–5.
27. Joshi, A, Kale, S, Chandel, S, and Pal, D. Likert scale: explored and explained. Br J Appl Sci Technol. (2015) 7:396–403. doi: 10.9734/BJAST/2015/14975
28. Gebresilassie, KY, Boke, M, Kindie, M, and Baraki, A. Knowledge level and associated factors about sexual and reproductive health rights among University of Gondar students, Gondar Ethiopia. Int J Sex Reprod Health Care. (2019) 2:016–20. doi: 10.17352/ijsrhc.000006
29. Ayalew, M, Nigatu, D, Sitotaw, G, and Debie, A. Knowledge and attitude towards sexual and reproductive health rights and associated factors among Adet tana Haik college students, Northwest Ethiopia: a cross-sectional study. BMC Res Notes. (2019) 12:80. doi: 10.1186/s13104-019-4116-4
30. Abajobir, AA, and Seme, A. Reproductive health knowledge and services utilization among rural adolescents in east Gojjam zone, Ethiopia: a community-based cross-sectional study. BMC Health Serv Res. (2014) 14:138. doi: 10.1186/1472-6963-14-138
31. Gebretsadik, GG, and Weldearegay, GG. Knowledge on reproductive and sexual rights and associated factors among youths, Shire town, Tigray, Northern Ethiopia. Int J Res Pharm Sci. (2016) 6:30–7.
32. Bishwajit, G, Tang, S, Yaya, S, Ide, S, Fu, H, Wang, M, et al. Factors associated with male involvement in reproductive care in Bangladesh. BMC Public Health. (2017) 17:3. doi: 10.1186/s12889-016-3915-y
33. Bhusal, CK, and Bhattarai, S. Social factors associated with involvement of husband in birth preparedness plan and complication readiness in Dang District, Nepal. J Commun Med Health Educ. (2018) 8:8. doi: 10.4172/2161-0711.1000636
34. Kassa, M, Abajobir, AA, and Gedefaw, M. Level of male involvement and associated factors in family planning services utilization among married men in Debremarkos town, Northwest Ethiopia. BMC Int Health Hum Rights. (2014) 14:33. doi: 10.1186/s12914-014-0033-8
35. Mapunda, B, August, F, Mwakawanga, D, Mhando, I, and Mgaya, A. Prevalence and barriers to male involvement in antenatal care in Dar Es Salaam, Tanzania: a facility-based mixed-methods study. PLoS One. (2022) 17:e0273316. doi: 10.1371/journal.pone.0273316
36. Fekede, A, Ayele, G, and Yadeta, D. Male partners involvement in maternal ANC care: the view of women attending ANC in Hararipublic health institutions, eastern Ethiopia. Sci J Public Health. (2014) 2:182–8. doi: 10.11648/j.sjph.20140203.17
37. Reece, M, Hollub, A, Nangami, M, and Lane, K. Assessing male spousal engagement with prevention of mother-to-child transmission (pMTCT) programs in western Kenya. AIDS Care. (2010) 22:743–50. doi: 10.1080/09540120903431330
38. Sharma, S, Kc, B, and Khatri, A. Factors influencing male participation in reproductive health: a qualitative study. J Multidiscip Healthc. (2018) 11:601–8. doi: 10.2147/JMDH.S176267
39. Wai, KM, Shibanuma, A, Oo, NN, Fillman, TJ, Saw, YM, and Jimba, M. Are husbands involving in their Spouses' utilization of maternal care services?: a cross-sectional study in Yangon, Myanmar. PLoS One. (2015) 10:e0144135. doi: 10.1371/journal.pone.0144135
40. Osuafor, GN, Akokuwebe, ME, and Idemudia, ES. Male involvement in family planning decisions in Malawi and Tanzania: what are the determinants? Int J Environ Res Public Health. (2023) 20:5053. doi: 10.3390/ijerph20065053
Keywords: involvement, sexual health, sexual rights, reproductive health, reproductive rights
Citation: Jemberie MM, Zewdu M and Rade BK (2024) Husbands’ knowledge and involvement in sexual and reproductive health rights of women in Bahir Dar City, Northwest Ethiopia: a community-based study. Front. Public Health. 12:1359756. doi: 10.3389/fpubh.2024.1359756
Edited by:
Graça S. Carvalho, University of Minho, PortugalReviewed by:
Triphonie Nkurunziza, World Health Organization - Regional Office for Africa, Republic of CongoElias Amaje, Bule Hora University, Ethiopia
Copyright © 2024 Jemberie, Zewdu and Rade. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bayew Kelkay Rade, YmF5ZWtlbGtheUB5YWhvby5jb20=