 Saen Fanai
Saen Fanai Eunice Okyere2†
Eunice Okyere2†- 1College of Medicine, Nursing and Health Science, Fiji National University, Suva, Fiji
- 2School of Public Health, College of Medicine, Nursing and Health Science, Fiji National University, Suva, Fiji
Objective: This systematic review aims to assess Behavior Change Interventions (BCIs) targeting dangerous driving behaviors (DDBs) in low- and middle-income countries (LMICs), evaluate their effectiveness, and explore the outcome measurement instruments employed in these contexts.
Method: A comprehensive search was performed across key databases such as Scopus, PubMed, CINAHL, Medline, ProQuest, Cochrane Library, and Research4life, focusing on studies published post-2015 on BCIs for DDB using randomized controlled trials (RCTs), quasi-experiments and mixed method designs. Data extraction centres on the types of intervention, theoretical frameworks, outcome measurement, and intervention effectiveness. The findings were analyzed through a narrative synthesis approach.
Results: Fifteen studies were analyzed in this review, which examined BCIs aimed at enhancing driver behavior. Some interventions included public awareness campaigns, peer mentorship programs, driving courses for skill enhancement, and in-vehicle monitoring systems for safety measures. The study results revealed that widely employed behavior change theories such as the Theory of Planned Behavior (TPB), along with Social Cognitive Theory (SCT) and the Health Belief Model (HBM), were prevalent in these interventions. Surveys like the Driver Behavior Questionnaire (DBQ) and assessments of road safety knowledge were frequently used to measure behavioral changes among participants. Objective criteria included the use of GPS tracking devices, as well as the examination of insurance claims and traffic violation reports to evaluate the interventions’ effectiveness. The study focused on methods like peer influence implementation and fear-based communication strategies paired with personalized feedback, which were identified as successful approaches in the review report. However, it emphasized a lack of uniformity in utilizing validated tools for outcome measurement across various socioeconomic contexts, particularly in LMICs.
Conclusion: Behavioral interventions informed by theories have demonstrated effectiveness in improving driving behaviors; nonetheless, recognized and validated measures for assessing results in lower—and middle-income settings remain unclear. In the future, research efforts should prioritize developing assessment tools that resonate with cultures and conducting studies to evaluate enduring changes in behavior. This systematic review may guide policymakers, and public health experts engaged in developing road safety programs.
Systematic review registration: www.crd.york.ac.uk/prospero, identifier 578081.
1 Introduction
Since the mid-20th century, reports have indicated some decline in road traffic deaths and injuries due to public health initiatives, preventive efforts, and technological improvements, including safer vehicles and roads, as well as improved emergency services and trauma care (1, 2). Despite these improvements, the issue remains important, particularly within health and social care and its escalating costs for health and welfare systems across the globe and in particular low and middle-income countries (LMICs) (3). Vehicle crashes and related injuries and deaths are not random incidents; Human behavior is the critical factor in more than 90% of crashes (1). It is essential to use a multi-disciplinary framework to understand the underlying psychological influences on driving behavior and the development and evaluation of interventions to achieve improvements in road user behavior (4). In recent years, there has been a growing focus on finding effective behavior change strategies to improve various forms of driver behavior across a wide range of road user-profiles and cultural contexts (5). Empirical findings show that successful behavior change strategies involve making drivers aware of the errors that lead to accidents using persuasive communications and penalty and reward systems while supporting them in adopting preventive strategies that maintain a certain driving quality during exposure (6). Nonetheless, the field of driving behavioral change holds several challenges. First, the definition of safe driving itself is far from clear and straightforward (4). Second, the readiness of individuals to adhere to driving quality can vary greatly depending on the context (7). Notable progress has been made in advancing empirical frameworks that effectively support the formulation of targeted actions. Information gathered from actual driving behaviors has enabled researchers to assemble detailed evidence regarding the impact of individual differences on changes in driver behavior (5).
1.1 Background and rationale
Traveling on the roads in our society poses a considerable health danger. Every year, traffic accidents result in around 1.24 million deaths worldwide, and between 20 to 50 million individuals sustain injuries or disabilities (2). The public health burden of traffic-related injuries is particularly pronounced in LMICs, where infrastructure, enforcement, and health system responses are often limited. This review focuses on these settings to assess context-specific challenges and intervention effectiveness. Despite a large body of research identifying a great deal of DDBs, which increases the risk of traffic crashes and other adverse outcomes, a relative lack of consensus about how to change such behavior effectively still exists (8). The complex nature of DDB may contribute to the diversity of its associated interventions, including policy and enforcement interventions, BCIs, and modifications of the driving environment (1). Earlier reviews on changing driver behavior mainly approach the field from a general road safety perspective, do not systematically focus on DDB, and do not specifically describe the extent to which studies included in those reviews employed intervention content derived from psychological theories, models, and insights (6). While previous research indicates that varying levels of cognitive constructs help to predict dangerous driving, these predictions should only serve as starting points for theory-based BCIs, as psychological theory tends to be abstract (5).
Previous research has highlighted that studies focusing on DDB often fail to incorporate relevant theories or models when developing interventions aimed at changing this behavior. For instance, one review of alcohol-related driving offenders was based on the characteristics of actual offenders rather than their risky driving behaviors (9), and another review classified various dangerous behavior characteristics based on a priori risk implications and then categorized some of these behavior characteristics into intervention types, either informational, technical, training, legal regulation, persuasion, rewards, sanctions, or combinations (10). Trying to change DDB in this manner has thus far met with mixed success. It might only contribute to mild effects because the BCIs are hypothesized based on identified risky driving-related behaviors and consequences. Still, no explicit theoretical framework was used to explain the nature of the predicted associations between the intervention content, behavioral determinants, and behavior (5). Commonly, individual-level BCIs neglect the broader contextual and cognitive factors influencing long-term change (7).
Previous reviews found that the most studied behavior change techniques included feedback and monitoring, goal setting and planning, social support, knowledge sharing, and natural consequences. All interventions proved somewhat effective in reducing DDB (5, 7). Goal setting, penalties, and vicarious experience were most frequently reported to create an overall change in driving Behavior (11). The most frequently reported outcome measures used to assess the effectiveness of the interventions were accidents and injuries, self-reported confidence, self-reported driving violations, behavior or sanctions, self-reported ability concerning driving, and self-reported behavioral change (4, 5).
1.2 Objective of the review
This review’s primary aim is to evaluate BCIs to reduce DDB in LMICs and synthesize context-specific evidence on their effectiveness and evaluation methods.
The findings of this review can assist policymakers and practitioners in creating innovative BCI tools that effectively address the needs of modern drivers (6).
1.3 Scope and definition of dangerous driving behavior
DDB consists of risky actions or patterns that significantly increase the likelihood of road accidents, resulting in injuries and fatalities. The definitions from the World Health Organization, Elander et al., and Reason et al. (2, 12, 13) inform our understanding of DDB, which includes at least the following behaviors:
• Speeding: Operating a vehicle above the legal speed limit or too fast for road or traffic conditions.
• Distracted driving: Activities that divert attention from driving, such as mobile phone use and interactions with passengers.
• Driving under the influence of psychoactive substances: Operating a vehicle while impaired by alcohol, drugs, or other substances.
• Fatigued driving: Driving while drowsy, often due to lack of sleep or prolonged hours on the road.
The established definition serves as our inclusion criteria for identifying relevant outcomes, intervention targets, and measurement instruments in the studies. Our analysis employs this definition to synthesize intervention effectiveness and the appropriateness of outcome measures across various contexts.
1.4 Significance of studying behavior change intervention
When appropriate BCI models and tools for measuring these interventions are developed, there can be a significant improvement in traffic safety, a reduction in the severity of DDB, and the prevention of traffic accidents before they occur (1, 4). BCIs that focus on reducing dangerous driving are crucial as they seek to modify social behaviors. These interventions promote social learning and experiential learning through various real-world tasks and simulations provided to participants. As alluded to, the findings of this review can assist policymakers and practitioners in creating innovative BCI tools that effectively address the needs of modern drivers (6).
2 Method
2.1 Information sources and search strategy
This systematic review was conducted and documented in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (14).
A comprehensive search strategy was developed using a combination of keywords and Medical Subject Headings (MeSH) terms related to dangerous driving BCIs, and outcome measurement instruments. The strategy was adapted for each database. The research supervisors, who are seasoned researchers who have led researchers on various health-related research projects, reviewed the strategy (15). The final search was conducted on September 14, 2024, and included seven electronic databases: Scopus, PubMed, CINAHL, Medline, ProQuest, Cochrane Library, and Research4life. Every database underwent an individual search, and the search approach for Medline, one of the databases, can be found in Table 1. The search strategy utilized a combination of controlled keywords and subject headings. An example of that used in Research4life and PubMed include: (“dangerous driving Behavior” OR “risky driving Behavior” OR “unsafe driving” OR “reckless driving”) AND (“Behavior change intervention” OR “Behavioral intervention” OR “educational program” OR “training program” OR “policy intervention”) AND (“outcome measurement” OR “evaluation” OR “assessment” OR “instrument”). The search was restricted to English-language publications involving human subjects and published from 2015. The search terms were aligned with MeSH headings whenever feasible. The reference lists of included studies and pertinent systematic reviews were also reviewed to identify additional eligible studies.
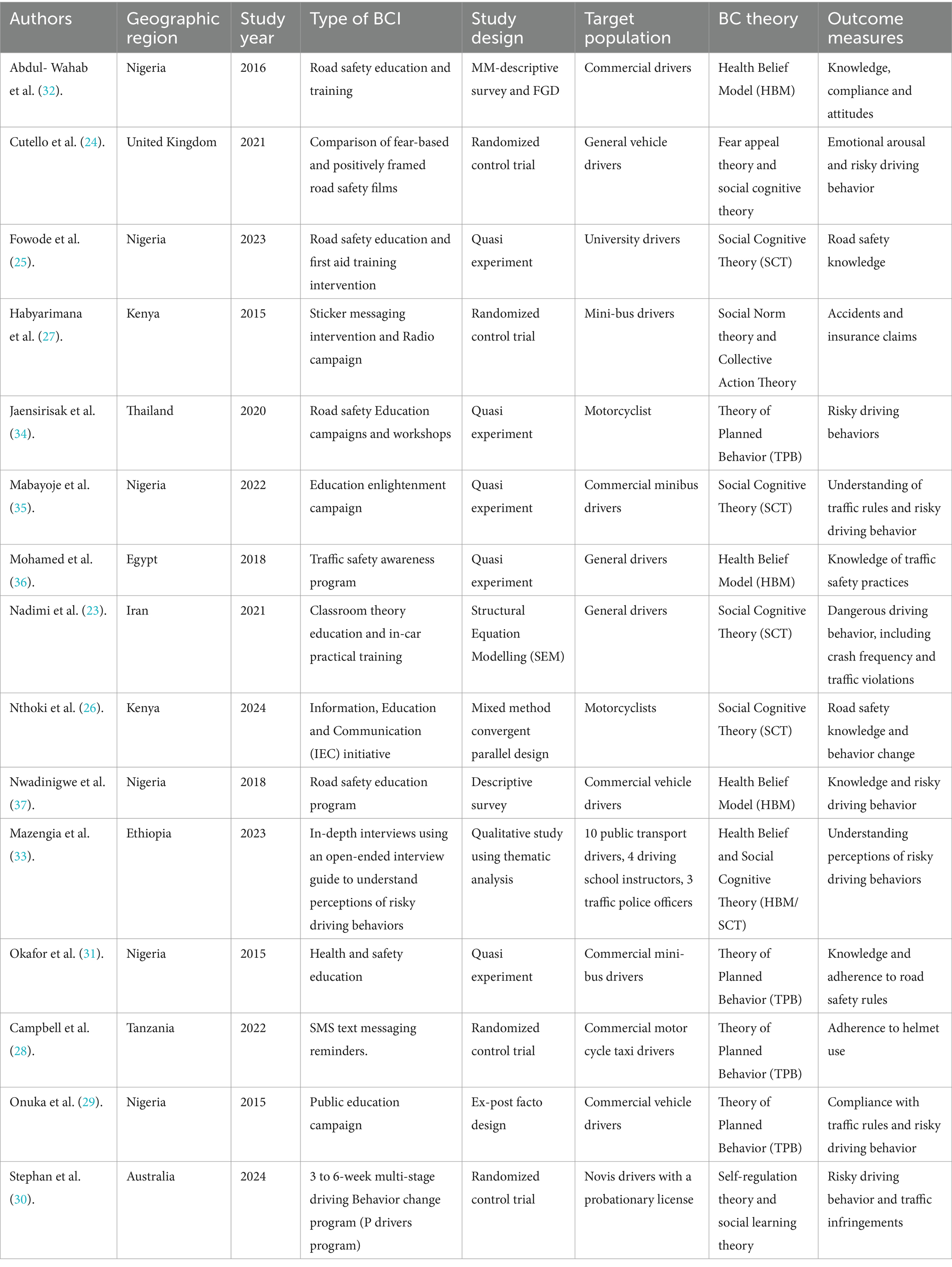
Table 1. Behavior change intervention study characteristics.
2.2 Study selection
Per the recommended approach for systematic reviews, three independent reviewers (Julianne Borugu, Clelia Raubebe and Susan Tavimele) assessed the eligibility of studies for inclusion in the review. The three reviewers (JB, CR, ST) were public health researchers with training in systematic review methodology. They used a standardized screening form to apply inclusion and exclusion criteria. Reliability was ensured by independent screening and resolution of disagreements through consensus discussion, enhancing consistency in study selection. Any disparities in their findings were addressed through discussion until a consensus was reached. Initially, the search results were evaluated based on the title and abstract. The full text was obtained if the eligibility was unclear or the abstract was not available. The eligibility criteria were then used to assess the inclusion of the full-text studies in the review (16, 17).
2.3 Eligibility criteria
2.3.1 Participants
Vehicle drivers of any age group and gender were included, regardless of health status (participants in good health or individuals with particular health issues or medical conditions).
2.3.2 Interventions
Studies that involved any BCIs aimed at reducing DDB, such as educational programs, technological aids, and media campaigns, were included. Any interventions that aim to raise awareness and improve knowledge about road safety among vehicle drivers, addressing traffic rules, the dangers of risky behaviors, and proper driving techniques are included. Interventions delivered through formal classroom settings, online modules, workshops, or seminars are included. The target audiences often include new drivers, commercial drivers, or offenders enrolled in remedial driving courses. The interventions must address at least one of the following DDB: speeding, aggressive driving, distracted driving, and impaired driving, which are the leading causes of traffic accidents globally.
2.3.3 Control or comparator
Studies with or without comparators (e.g., no intervention or alternative interventions) are acceptable.
2.3.4 Outcomes
The behavioral change intervention had to target one of the following individual modifiable health behaviors identified by the World Health Organization as leading risk factors for road traffic accidents and injuries (2): Speeding, aggressive driving, impaired driving, distracted driving, and driving when fatigued. For inclusion in the review, the study had to report data regarding the effectiveness of Behavior change. Additionally, studies were included if they reported variables closely related to Behavior change; this included potential mediators of Behavior change (e.g., health status or physical activity self-efficacy). Studies presenting secondary outcomes data, including Road traffic accidents, injuries, adherence to traffic rules, and other related behavioral and safety outcomes, are accepted.
2.3.5 Study design
The systematic review included RCTs, non-RCTs, Quasi-experimental studies, Cohort studies, Case–control studies, Cross-sectional studies, and including Qualitative studies that seek to explore insights into intervention mechanisms and contexts. Ecological studies and studies with small sample sizes (such as case studies) were considered for inclusion. Systematic reviews and Conference abstracts were not considered.
2.3.6 Data collection process and data items
Data was extracted using a standardized form created specifically for this review. Data extraction for each included study was done independently by the reviewers (JB, CR, ST), and any disagreements were resolved by checking and discussing the original study until a consensus was reached. The reviewers reached a 90% consensus on data extraction, with the primary discrepancies related to studies lacking clear outcomes. Information that was extracted included Study characteristics (e.g., authors, year, country, study design), Participant characteristics (e.g., age, gender, driving experience), Intervention details (e.g., type, duration, delivery method), Outcome measures (e.g., instruments used, primary and secondary outcomes), and Results (e.g., effectiveness of interventions, measured outcomes).
2.3.7 Risk of methodological Bias
The methodological quality of the included articles was assessed using the Cochrane Risk of Bias tool for RCTs (18), the ROBINS-I tool for non-randomized studies (19) and the Quality Assessment Tool for Quantitative Studies for observational studies (20). For randomized trials, the Cochrane Risk of Bias (RoB 2) tool was used; for non-randomized studies, we applied ROBINS-I; and for observational studies, we used the Quality Assessment Tool for Quantitative Studies. Two reviewers independently rated each study. Discrepancies were resolved through discussion with a third reviewer. We compiled the results from the subjective judgment matrix, which considered the authors’ conclusions, qualitative and quantitative data demonstrating statistically significant differences among participants and the BCI outcomes, and the methodological quality of the included articles. The protocol for this review overview was created before conducting the review. It was submitted to the PROSPERO International Prospective Register of Systematic Reviews. The reporting of this systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
2.3.8 Summary measures and synthesis of results
2.3.8.1 Summary measures
To assess how well BCI can help decrease DDBs, we will use summary measures to give a structured evaluation of the results achieved in this study. The changes in Behavior will be examined by assessing the tools such as self-reported surveys and observation of the DBQ, which looks at driving actions like speeding, traffic violations and close calls. We will also look at pre and post-evaluations to gauge any changes in drivers’ understanding of traffic regulations and their adherence to them. Depending on the studies, metrics, like GPS tracking for speed compliance and records of traffic violations, will be used to observe changes in behavior compared to self-reported information. Also, tools such as the Emotional Arousal Scale will be utilized to evaluate attitudinal shifts measuring responses to safety messages and interventions. These summarized measures will be gathered for comparison across studies to help assess the effectiveness of different BCIs intended to modify driver behavior and adherence.
2.3.8.2 Synthesis of results
To effectively compile and make sense of the results from the review, a narrative synthesis method involves looking at study designs and interventions while also considering the range of outcome measures used in each study. The initial categorization of BCI will be based on type, such as public awareness campaigns or driver improvement programs. This allows for comparisons between intervention approaches, like behavioral messaging and peer-supported mentoring initiatives. We will first examine the framework of each study with an emphasis on different health behavior change theories like TPB, HBM and SCT. We will gather effect sizes and other statistical indicators to assess changes in behavior resulting from different interventions. Additionally, we will consider factors like research methodologies (for example, RCTs and quasi-experiments), the specific groups being studied (such as professional drivers or new drivers), and the tools used for measurement in order to examine both the consistency and variations in outcomes. It is important to evaluate the research quality and potential biases while considering constraints, such as the absence of randomization and reliance on self-reported data collection methods.
3 Results
3.1 Study selection
The initial search retrieved 1,445 records. After deduplication and screening for title abstracts and full-text, using a predefined list of inclusion/exclusion criteria and assessment for risk of bias, 15 studies that reported information on BCIs and the instruments used to measure the results of these interventions were included in the systematic review (Figure 1).
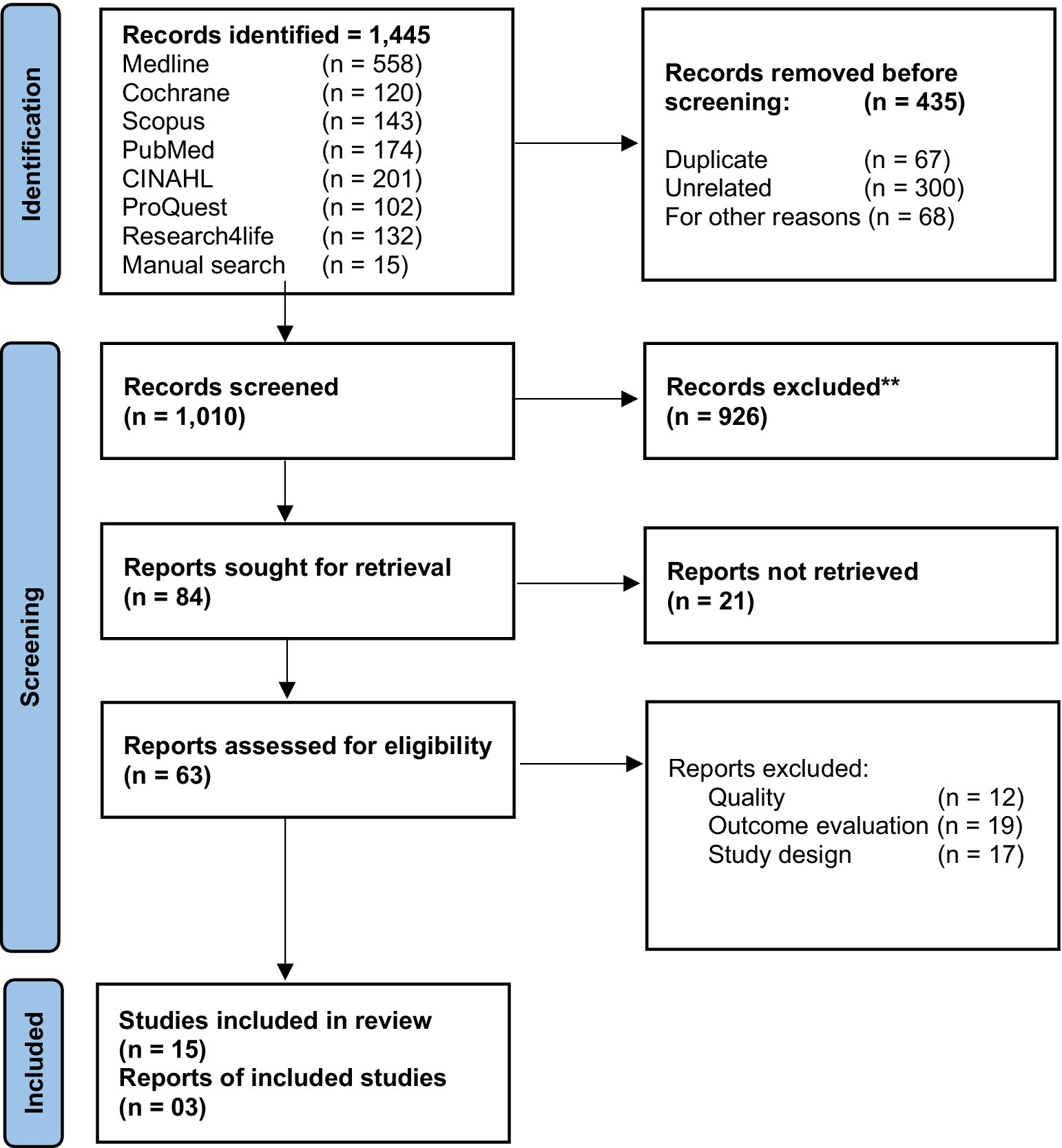
Figure 1. Flow diagram of selection of articles.
3.2 Study characteristics
The 15 included studies identified eighteen (n = 18) types of BCI and nine (n = 9) tools for measuring the effectiveness of BCI. The majority of the studies were from Nigeria (n = 6), Kenya (n = 2), and individual (n = 1) studies from Australia, the United Kingdom, Egypt, Iran, Tanzania, Thailand, and Ethiopia. Most studies (n = 10) used education and awareness as part of the BCI package. Instruments used to measure the outcome of the BCI vary, but of the eighteen identified, most of the studies (n = 7) used questionnaires and (n = 7) surveys. The characteristics of BCI are described further in Table 1; the intervention types and summary of outcomes are included in Table 2, and the BCI and Measurement Instruments Used are in Table 3.
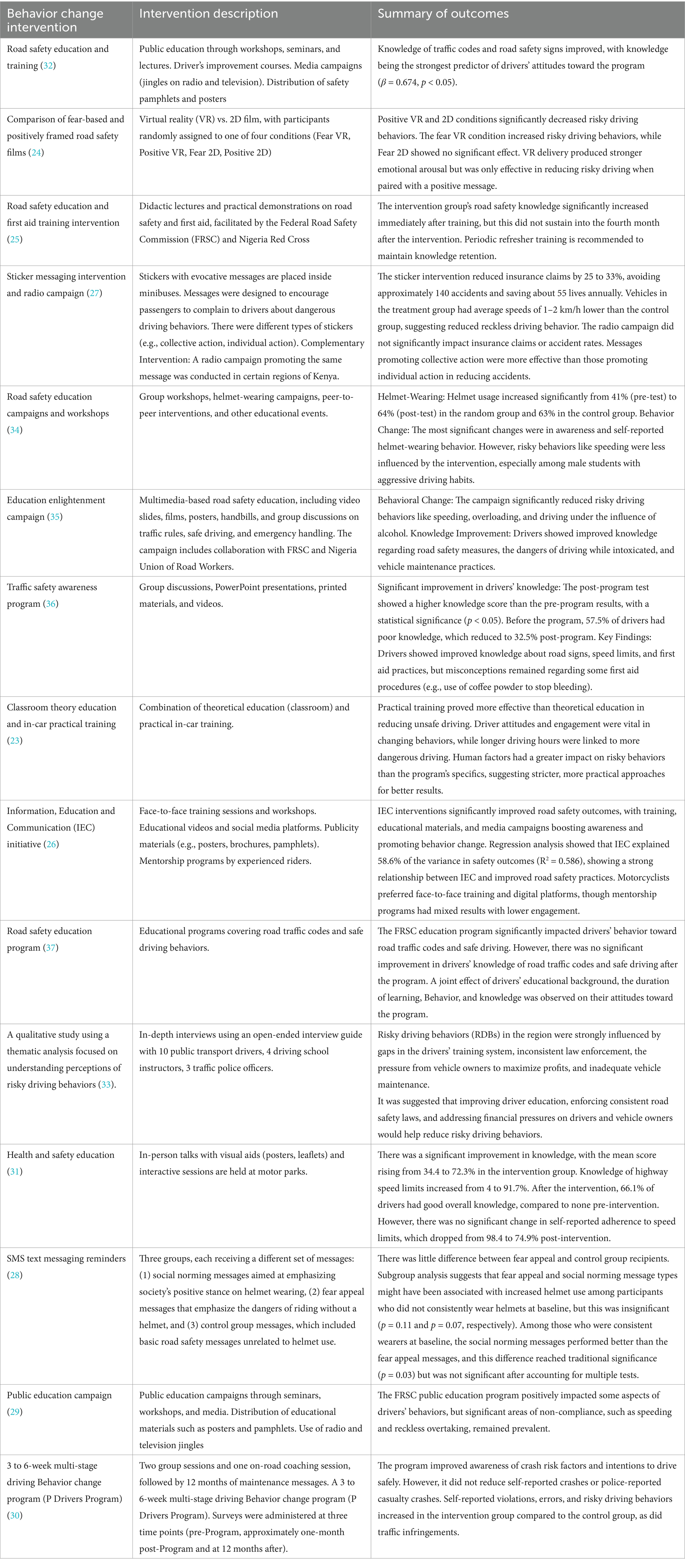
Table 2. Behavior change intervention and summary of outcomes.
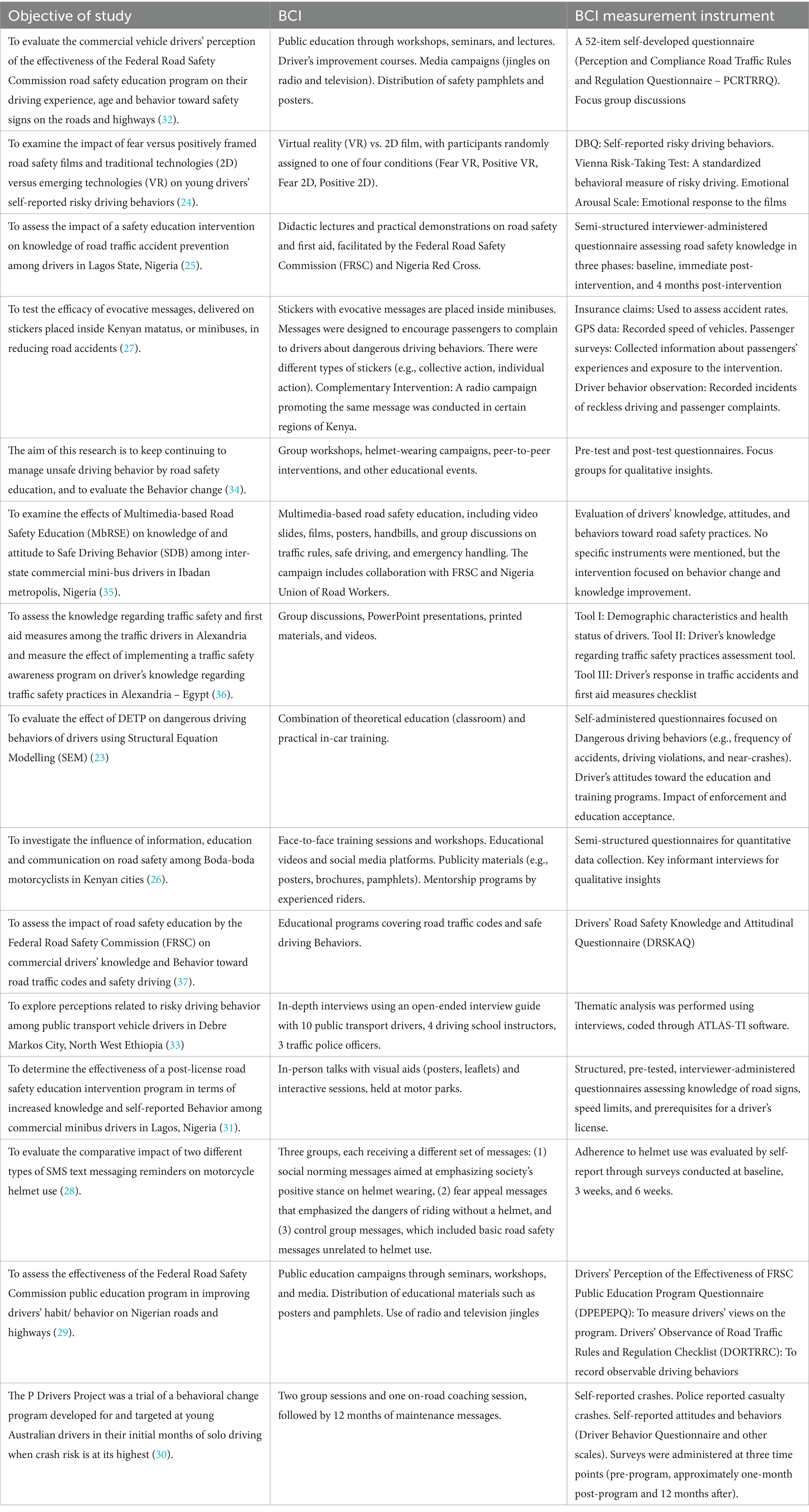
Table 3. Behavior change intervention and measurement instruments used.
3.3 Results of synthesis
3.3.1 Study designs
Of the 15 studies included in the systematic review, the majority (n = 5) used a quasi-experimental study design and (n = 4) used RCT. Two other studies used a mixed-method study design, one used an Ex Post Facto design, one used a descriptive survey study design, one used structural equation modelling (SEM), and one used a qualitative study design.
3.3.2 Behavior change intervention
The results showed that the majority of BCIs (n = 10) used driver’s educational programs and were conducted through various approaches alone or alongside other approaches like workshops or seminars (n = 4), printed materials (n = 4), media platforms (n = 3) and video slides or films (n = 3). One study conducted educational BCI alongside practical in-car training. Other studies (n = 2) assessed the effectiveness of driver’s educational programs that involve the attitudinal Behavior of drivers toward road signs, driving rules and management of road accident-free environment, which starts and ends in classrooms but did not specifically mention the educational approach. Other BCI that were conducted individually include SMS text messaging (n = 1), In-depth interviews (n = 1), Road safety films (n = 1), sticker messaging (n = 1) and Radio campaigns (n = 1). The BCIs are summarized in Table 2.
3.3.3 Behavior change theory used
The review result showed a range of behavior change theories used in the studies, either alone or in combination. The major behavior change theories were SCT (n = 4), TBP (n = 4) and HBM (n = 3). TPB focuses on the relationship between beliefs, attitudes, perceived behavioral control, and behavioral intention (21). The SCT emphasizes the influence of observational learning, social reinforcement, and self-efficacy on behavior (22). The HBM proposes that health behavior is influenced by perceived susceptibility, severity, benefits, barriers, and cues to action (21). Other studies (n = 4) used a combination of behavior change theories, including a combination of fear appeal theory and SCT (n = 1), a combination of social norm theory and collective action theory (n = 1), a combination of self-regulation theory and social learning theory (n = 1), and a combination of HBM and SCT (n = 1).
3.3.4 Outcome measures of behavior change intervention
The outcome measures of the BCI vary in the fifteen studies, with surveys (n = 7) and questionnaires (n = 8) making up most of the outcome measurement instruments. Other measurement tools include Focus Group Discussions (FGD) (n = 1), risk-taking tests, insurance claims (n = 1), recorded speed of vehicles (n = 1), driver behavior observation (n = 1) and self-report crashes (n = 1). These outcome measurement tools are used alone or in combination with other tools, particularly the two primary tools, surveys or questionnaires. Surveys used in these reviews include passenger surveys, Knowledge, Attitude and Behavior (KAB) surveys, demographic surveys, self-report surveys and drivers’ perceptions of BCI. Moreover, questionnaires that were used in these reviews include a self-developed questionnaire, a regulation questionnaire, a DBQ, a semi-structured interviewer-administered questionnaire, pre and post-test questionnaires, self-administered questionnaires, Driver’s Road Safety knowledge and Attitudinal Questionnaire (DRSKAQ) and self-reported attitudes and behavior questionnaire. The BCI measurement instruments are summarized in Table 3.
3.3.5 Comparative analysis across studies
This review reveals several patterns in the design, implementation, and effectiveness of BCIs aimed at DDBs across LMICs. While all included studies aimed to address risky behaviors such as speeding, distracted driving, and impaired driving, the methods employed, theoretical foundations, target groups, and contexts varied. This section synthesizes these variations to highlight meaningful comparisons and insights.
3.3.5.1 Intervention type and effectiveness
Educational programs were the most common BCIs used through seminars, campaigns, classroom training, or printed media. These interventions enhanced knowledge and awareness, but the actual behavior change results were not encouraging. Interventions that included practical aspects, such as in-car training (23) or simulation-based training (24) yielded better outcomes in actual driver behavior.
Interventions that included education, media outreach, and community engagement were the most promising (25, 26). These interventions were further reinforced by peer mentorship and social accountability. Single-medium approaches (e.g., standalone posters or brief SMS reminders) were less effective, particularly if they lacked cultural sensitivity or interactivity.
3.3.5.2 Theories used and behavioral outcomes
The review found that the TPB, SCT, and the HBM were the most commonly used behavior change theories. TPB-based interventions successfully changed intention-based behaviors such as wearing a helmet or following speed limits. SCT-based interventions utilized observational learning and social reinforcement (e.g., peer mentors, role modelling) and were effective in areas with strong community networks. HBM-based interventions focused on risk perception and compliance benefits, with results varying based on the content’s engagement level and cultural appropriateness.
The effectiveness of their implementation primarily determined the success of these theories. Interventions that depended solely on superficial constructs (e.g., benefits without action cues) had a reduced impact.
3.3.5.3 Measurement approaches and validity
Self-report surveys and questionnaires were the most commonly used measurement tools. However, social desirability bias and recall inaccuracies limited their effectiveness. Studies utilizing objective measures (e.g., insurance claims, GPS data, traffic records) provided more reliable evidence of behavioral change (23, 27).
Mixed-methods approaches that included surveys, FGDs, or observational tools were used to enhance the findings’ reliability and differentiate between self-reported and actual behavior.
A significant issue identified in all studies is the absence of standardized and validated tools that can be used in LMICs. This highlights a critical research gap in road safety in these countries.
3.3.5.4 Population and contextual constraints
Interventions for commercial drivers and motorcyclists (e.g., minibuses, boda-bodas) were typically tailored to their high-risk occupation. However, the success of these interventions depended on the following contextual factors: enforcement of traffic laws, economic pressures (e.g., incentives to maximize trips), cultural norms surrounding speed, masculinity, and alcohol use, and the availability of ongoing training and infrastructure. For instance, interventions in urban areas with visible law enforcement, such as Egypt and Kenya, had more tangible impacts than those in rural areas with informal transport systems.
In conclusion, this comparative analysis demonstrates that the success of BCIs in LMICs is influenced by the design of the intervention, the cultural environment, the level of theory employed, and the level of measurement used. Interventions that are theory-based, multi-modal, context-sensitive, and well-supported by sound evaluation techniques have a greater potential for enhancing road safety in LMICs.
3.4 Risk of bias
The risk of bias assessment revealed that most studies exhibited a low risk of bias across key domains (Selection Bias, Performance and detection bias, Incomplete outcome data attrition bias, Reporting bias, other bias, finance and confounding, and Study design bias). Minor concerns with selection bias, performance, and detection bias were identified in two studies, respectively (24, 28). Minor concerns for incomplete outcomes were also noted in two studies (29, 30). Minor concerns for reporting bias were observed in a few (n = 3) studies (28, 30, 31) and study design bias in a few (n = 3) other studies (31–33). The overall risk of bias for each study is low. No risks were observed in the majority of the studies (n = 8). The Risk of Bias summary is shown in Table 4. These findings indicate that the studies generally had a low risk of bias and thus may not affect the strength of the evidence.
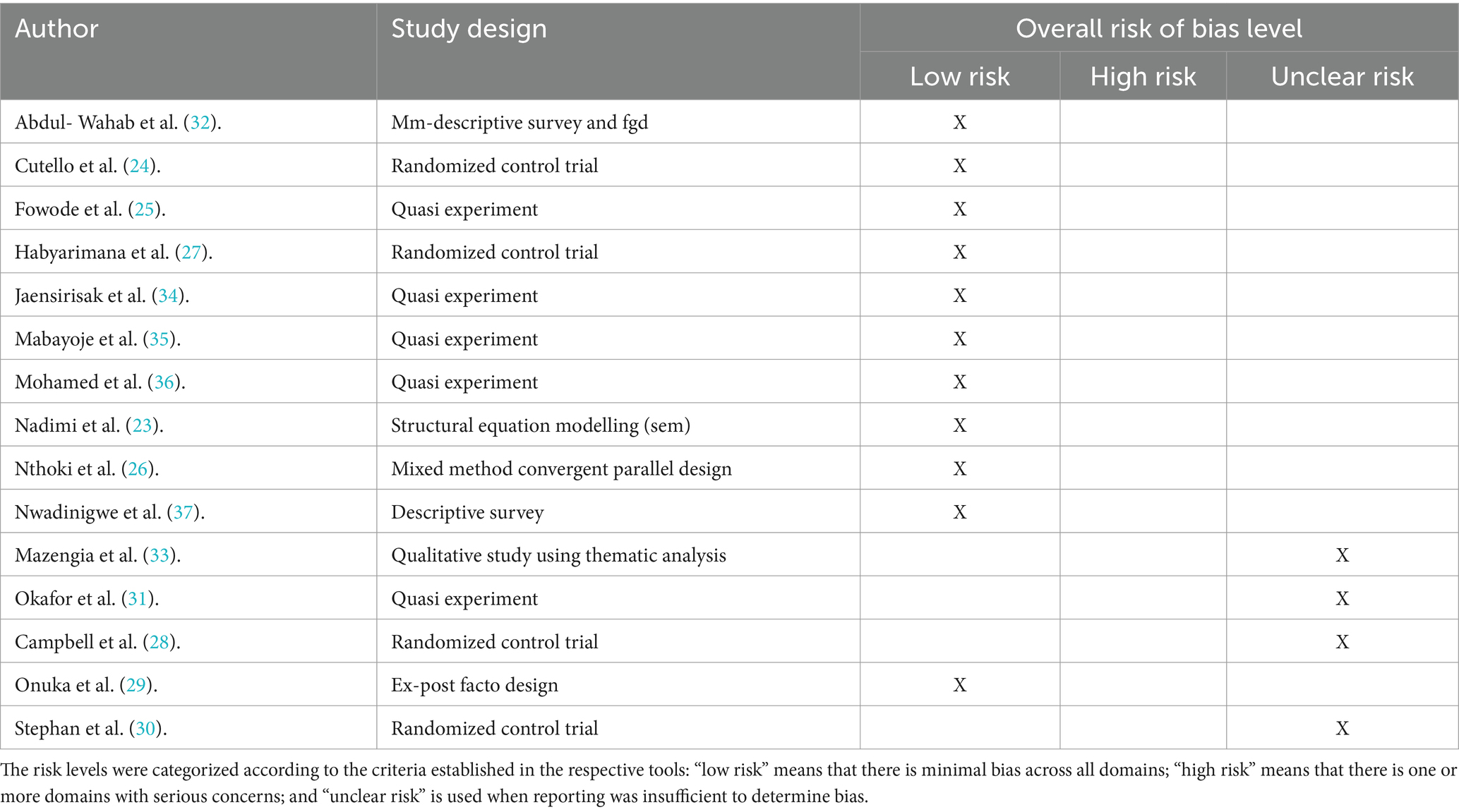
Table 4. Risk of bias summary.
4 Discussion
In synthesizing findings across studies, this review reveals that multiple contextual, theoretical, and methodological factors shape the effectiveness of BCIs. The following section evaluates intervention types, their theoretical foundations, implementation settings, and outcome assessment methods.
4.1 Behavior change intervention
The evaluation identified a range of methods to promote safer driving habits by addressing behaviors on the road through various approaches, each with differing levels of impact. Common strategies included public awareness campaigns, hands-on driver training programs, behavior-focused messaging, and peer mentoring initiatives.
Educational initiatives using workshops and media outreach, like radio and television ads, including posters and pamphlets, were prevalent approaches for promoting safe driving (25, 26, 29, 32, 34–37). These programs aimed to increase awareness and enhance understanding of driving practices. Multimedia-based road safety education utilizes films and group discussions in collaboration with road safety authorities. According to research studies, this method has proven effective in engaging a diverse audience (26, 28–30, 36).
The review indicated that most studies found success with a hands-on training method, which combined classroom learning and driving practice to improve skills behind the wheel and follow traffic rules (23, 25, 26, 30, 36). This interactive approach provided guidance and practical experience to help drivers become safer.
Psychological tactics such as using fear appeals and social norms are employed in messaging interventions to influence Behavior. Virtual reality (VR) and traditional 2D films delivered messages highlighting the dangers of risky driving behaviors. At the same time, sticker campaigns in minibuses encouraged passengers to take collective action against dangerous driving (24, 27, 28, 32). Fear-based messaging was also employed to promote helmet use among motorcyclists, highlighting non-compliance risks (26, 28, 34).
Furthermore, the review indicated that peer support initiatives played a role in influencing changes in driver behavior. Seasoned riders and drivers took on the role of mentors to guide and support others directly in influencing their behavior (23, 26, 30, 31, 34). Combining this method with awareness campaigns established a supportive environment to foster lasting behavioral changes (27, 29, 32, 35).
The analysis of included studies indicated that behavioral outcomes were stronger when interventions incorporated educational and interactive elements, such as practical in-car training and peer mentorship. Programs that utilized multiple channels, including theoretical approaches, real-world simulations, and community-based initiatives, produced more reliable results than single-channel methods like posters and SMS reminders. The results suggest that knowledge dissemination needs to be combined with behavior modelling and reinforcement mechanisms, especially when targeting high-risk groups such as commercial drivers and motorcyclists.
4.2 Measurement instruments for behavior change interventions
The review highlighted various measurement instruments used to effectively measure BCI’s impact on addressing risky driving habits. Those tools played a role in gauging drivers’ understanding, cognition, and conduct toward diverse BCI campaigns.
The DBQ was frequently used to assess driving behavior effectively by asking individuals to report their driving habits comprehensively. It has proven dependable in research studies and offers a standardized way to evaluate behaviors like speeding tickets and near-miss collisions (23, 25, 26, 30, 31). In addition to the DBQ is the Vienna Risk-Taking Test, which is a widely accepted method for gauging how inclined drivers are toward taking risks on the road (24). The self-reported and observed measures provided insights into how drivers perceive things and their real driving actions.
In addition to self-reports to assess the intervention’s impact on accident rates and driving behavior in real-life situations, researchers utilized objective measures such as insurance claims and GPS data as well (27). These tools enabled tracking vehicle speed and accident claims to gather data that effectively supplements subjective reports. Observed methods like the Driver behavior Observation Checklist captured instances of reckless driving and passenger complaints in real-time, providing direct insights into driving habits (24, 29, 35).
Various semi-structured questionnaires and interview-administered tools were used to evaluate people’s knowledge and opinions on road safety. One of these tools is the Drivers’ Road Safety Knowledge and Attitudinal Questionnaire (DRSKAQ) (23, 35, 37), which successfully measured how well drivers grasped road safety laws and norms throughout the intervention process from the assessment to the follow-up stages. Moreover, the questionnaire known as Drivers’ Perception of the Effectiveness of the FRSC Public Education Program Questionnaire (DPEPEPQ) assessed how drivers perceive the effectiveness of the public education program by the FRSC (29, 32). In contrast to this assessment tool is the Drivers’ Observance of Road Traffic Rules and Regulation Checklist (DORTRRC), which examines drivers’ adherence to road traffic regulations (29).
Additionally, valuable qualitative information was collected by engaging in focus group conversations and conducting interviews with individuals whose responses were organized and examined with the help of tools such as ATLAS TI (25, 31–34). These approaches offered context to the numerical data and shed light on the drivers’ perspectives on behavior change by investigating their attitudes and motivations.
Certain research studies included checklists focusing on health and safety practices, such as the Drivers Response in Traffic Accidents and First Aid Measures Checklist (36), which looked into how drivers were equipped and reacted in accident situations. Compliance with safety protocols, like wearing helmets, was evaluated through self-reports and surveys carried out at the beginning and end of the intervention periods (23–25, 28, 30, 32).
The studies reviewed used a combination of tools, such as surveys (such as DBQ and semi-formal questionnaires), concrete metrics (like GPS information and insurance records), and qualitative methods (like focus groups and interviews). These assessment tools offered a strategy that enabled the consideration of both personal perspectives and factual information in assessing the impact of interventions on improving road safety. The comparative analysis also showed that interventions using both subjective (e.g., surveys) and objective (e.g., GPS data, insurance claims) measures were more effective in assessing actual behavioral change. Programs relying solely on self-report instruments may have underestimated risky behaviors due to social desirability bias or recall bias. In LMIC contexts where access to administrative data may be limited, mixed-method approaches seem to provide a more balanced and credible evaluation of intervention outcomes.
4.3 Application of behavior change theories in road safety interventions
Various behavior change theories were used in the BCIs to address unsafe driving behaviors effectively. Many key behavior change theory frameworks guided the development and execution of these interventions by focusing on psychological and social factors that influence behavior change.
One of the most frequently applied theories was the TPB. The theory played a role in numerous initiatives, such as the ones carried out by the Federal Road Safety Commission (FRSC) in Nigeria and various public awareness campaigns aimed at drivers (28, 29, 31, 34). TPB focuses on three core components: attitudes, subjective norms, and perceived behavioral control, all of which influence an individual’s intentions to engage in safer driving practices (38). When interventions based on the TPB were implemented to alter drivers’ perceptions and motivations related to driving habits by addressing their beliefs about the outcomes of their actions and reinforcing social norms concerning road safety, they successfully promoted changes in behavior and compliance with traffic regulations (28, 29, 31, 34). This approach proved effective in initiatives targeting the enhancement of safe driving practices among drivers, as seen in studies like the Impact of Road Safety Education in Delta State and University Drivers in Ibadan research projects.
The HBM was frequently used in interventions aimed at raising drivers’ understanding of the risks of accidents and the advantages of practising safer driving habits (38). This model was involved in projects like the Federal Road Safety Commission Training in Jigawa State and the Traffic Safety Awareness Program in Alexandria. It also played a key role in media campaigns targeting Boda Boda motorcyclists in Kenya (32, 33, 36, 37). These initiatives sought to enhance drivers’ awareness of risks by highlighting the benefits of adhering to traffic rules for their safety and that of their communities. By addressing challenges and highlighting the advantages of applying the HBM (a model that helps predict health-related behaviors), these campaigns effectively motivated drivers to adopt habits such as wearing helmets and following speed limits (33, 36, 37).
The SCT has also been instrumental in developing programs that center on peer learning and mentorship initiatives, underscoring the value of observation learning, social influence and reinforcement mechanisms (38). BCIs, like the Media Campaign for Boda Boda Motorcyclists and the Adult Education Campaign for Mini Bus Drivers, used SCT by providing chances for drivers to witness and copy behaviors exhibited by their peers or seasoned riders (23–26, 33, 35). This approach promoted behavior change and fostered a supportive social environment in which safe driving practices could be reinforced. Similarly, Social Learning Theory (SLT), closely related to SCT, was employed in interventions like the P Drivers Program in Australia and the Driving Education Programs in Delta State (30, 37). The interventions based on SLT emphasized demonstrating role models and offering feedback to drivers so they could learn and modify their behaviors by observing and receiving reinforcement. These measures impacted novice drivers’ behavior, outlook, and road safety (30).
Some interventions use the Fear Appeal Theory to elicit reactions and prompt individual behavioral shifts. For instance, in research contrasting Virtual Reality with 2D Film presentations, fear-inducing messages emphasize the perils of unsafe driving habits, intending to encourage participants to avoid such behaviors (24). Nonetheless, the impact of fear appeal differed based on the framing of the messages and the setting in which they were presented (39, 40). Additionally, social norm theory and collective action theory were employed in Kenya’s Large-Scale BCI, which leveraged social norms and collective responsibility to influence passenger and driver behaviors (27). These theories emphasized the power of societal expectations and group action in promoting compliance with road safety rules.
Finally, the Self-Regulation Theory and aspects of the Transtheoretical Model (TTM) were applied to help individuals set goals and adjust their behaviors through self-observation and feedback mechanisms. This approach, though less commonly cited, has proven impactful in driving incremental improvement (30). They provided valuable frameworks for guiding behavior change through self-monitoring and gradual progression toward safer driving habits (38).
The effectiveness of TPB, SCT, and HBM appears to depend on the implementation depth. Interventions that extend beyond surface-level messaging and target behavioral intentions, self-efficacy, or perceived risk are more likely to influence real-world behavior. This suggests that merely referencing a theory is insufficient; instead, integrating theory into the design and delivery mechanisms of interventions is essential for effectiveness.
4.4 Predominant study designs and their relation to other vital variables
This review showed that different study designs were employed to assess BCIs to enhance road safety. RCTs, Quasi-Experimental Designs, Mixed Methods Approaches, and Qualitative Studies were the most common. The type of intervention and target population, alongside the intervention’s theoretical framework, underpinned each design choice, all of which played distinct roles in enhancing our understanding of behavior change outcomes.
RCTs were commonly employed to assess the effectiveness of interventions by comparing outcomes between randomized intervention and control groups. Cutello et al. in the UK (24), Habyarimana et al. in Kenya (27), Campbell et al. in Tanzania (28), and Stephan et al. in Australia (30) applied RCTs to test interventions rigorously. These research studies focused on populations ranging from everyday drivers to motorcycle taxi drivers and new drivers. Theories like Fear Appeal Theory, SCT, TPB and Self-Regulation Theory guided the interventions (24, 27, 28, 30), enabling researchers to evaluate outcomes such as risky driving behaviors, emotional responses, adherence to helmet use, and traffic violations.
RCTs have shown success in offering strong evidence of the effectiveness of interventions by evaluating theory-based strategies in controlled environments (41). Quasi-experimental designs, on the other hand, were commonly applied in situations where randomization was not feasible for community or educational initiatives (42). This approach was notably implemented in research conducted by authors like Fowode et al., Jaensirisak et al., Mabayoje et al., Mohamed et al., and Okafor et al. (25, 31, 34–36). These interventions mainly focused on university drivers, motorcyclists and commercial minibus drivers. The SCT, the HBM, and the TPB all focused on drivers’ understanding of road safety regulations and their adherence to them to reduce driving behaviors in society. For instance, research conducted by Mohamed et al. And Okafor et al. Examined individuals’ awareness of traffic safety regulations and willingness to follow road rules. These studies demonstrated how quasi-experiments could be effectively used to evaluate changes in behavior in real-life scenarios (31, 36).
Furthermore, Mixed methods designs were chosen in research where both quantitative and qualitative perspectives were necessary for comprehending behaviors and attitudes (43). For instance, Thoki et al. used a convergent design to assess the road safety habits of motorcyclists in Kenya (26). Mixed methods proved valuable for interventions based on SCT, emphasizing learning and reinforcement as critical elements in driving behavioral changes (43). These designs integrated data like road safety knowledge scores with drivers’ subjective viewpoints to offer a holistic understanding of behavioral shifts.
Mazengia et al. delved deeply into people’s thoughts and feelings about driving using qualitative approaches (33). These studies employed a combination of HBM and SCT to explore drivers’ motivations and beliefs about road safety. The thematic analysis brought out an understanding of the psychological aspects that influence risky driving behaviors, providing additional insights that complemented the numerical results (44).
The contextual challenges faced by LMICS, such as limited enforcement, economic pressures on drivers, and road infrastructure issues, emerged as critical factors influencing intervention success. Interventions located in urban areas with more robust regulatory frameworks tended to yield more quantifiable results. This underscores the importance of context-sensitive design and the integration of structural supports, such as enforcement partnerships or ongoing training programs, to enhance the impact of interventions.
4.5 Implications for policy and practice
The review indicates that BCIs in LMICs are most effective when they are theory-based, culturally adapted, and reinforced over time. Policymakers should invest in multi-component interventions, prioritize community engagement, and utilise validated outcome measurement tools. Additionally, integrating behavioral interventions into national road safety strategies could reduce traffic-related injuries and fatalities in resource-constrained settings.
4.6 Limitations
Some studies had flaws in the methods, such as lack of randomization, small sample sizes and uncertain bias levels in specific domains. Therefore, these limitations may affect the reliability and generalizability of the findings. Moreover, comparing the studies was made difficult by the level of variance in the types of intervention, the measurement tools and the outcomes evaluated. There was a lack of standardized measures for assessing changes in Behavior across different studies, which might affect result consistency. Finally, the evaluation could be affected by a bias in publication since research that yields negative results is less likely to be published.
5 Future research
For future studies, researchers should consider exploring a more comprehensive range of driver populations with diverse cultural and economic backgrounds to enhance the applicability and inclusiveness of results. Moreover, combining qualitative data through Mixed methods design provides valuable perspectives. It would be beneficial for research to adopt this method to capture both tangible impacts and environmental factors that impact changes in Behavior. Moreover, future studies should aim to develop and adopt standardized tools for measuring Behavior change outcomes to facilitate comparison across studies and improve data consistency.
6 Conclusion
This systematic review sought to identify the most common BCIs (BCIs) targeting DDBs and to examine the instruments used to measure these interventions’ outcomes. The review showed that public education campaigns, practical driver improvement programs, behavioral messaging interventions, and peer-to-peer mentorship were the most prevalent interventions applied across diverse driving populations. These BCI were usually based on established behavior change theories, such as the TPB, the HBM and the SCT. Different types of tools were used to measure these BCI, including self-reported instruments like the DBQ, guided surveys as well as objective data sources such as GPS tracking and insurance claims records to assess road safety aspects of BCIs effectiveness in various studies together with qualitative methods like focus groups and thematic analyses to gain a holistic perspective, on the subject.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
SF: Formal analysis, Methodology, Writing – review & editing, Investigation, Writing – original draft. EO: Conceptualization, Writing – review & editing, Supervision, Formal analysis, Visualization. KM: Writing – review & editing, Supervision, Methodology, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We extend our sincere gratitude to all individuals who contributed to the successful completion of this systematic review. We wish to express our appreciation to Fiji National University, notably the College of Medicine, Nursing and Health Science, for providing the necessary resources, access to research databases, and institutional support throughout this study. Thank you, especially to EO and KM, whose invaluable guidance, constructive feedback, and ongoing support significantly shaped this research. We also acknowledge the support of Dr. Julianne Borugu, Mrs. Clelia Raupepe, and Mrs. Susan Tavimele, whose contributions to data extraction, analysis, and manuscript review were essential in strengthening the study. Thank you all for your contributions to this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Peden, MM. World report on road traffic injury prevention. Geneva, Switzerland: World Health Organization (2004).
2. World Health Organization. Global status report on road safety 2018. Geneva, Switzerland: World Health Organization (2019).
3. Bishai, D, Asiimwe, B, Abbas, S, Hyder, AA, and Bazeyo, W. Cost-effectiveness of traffic enforcement: case study from Uganda. Injury Prev. (2008) 14:223–7. doi: 10.1136/ip.2008.018341
4. Evans, L. Traffic safety. Science serving society. Bloomfield Hills, MI: Science Serving Society. (2004). 179 p.
5. Michie, S, Van Stralen, MM, and West, R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. (2011) 6:1–12. doi: 10.1186/1748-5908-6-42
6. Fuller, R. Towards a general theory of driver behaviour. Accid Anal Prev. (2005) 37:461–72. doi: 10.1016/j.aap.2004.11.003
7. Conner, M, and Norman, P. Predicting health behaviour: a social cognition approach. Predict Health Behav. (2005) 2:1–27.
9. Babor, TF, McRee, BG, Kassebaum, PA, Grimaldi, PL, Ahmed, K, and Bray, J. Screening, brief intervention, and referral to treatment (SBIRT): toward a public health approach to the management of substance abuse. Alcohol Drug Screen Brief Interv. (2023) 28:7–30. doi: 10.1300/J465v28n03_03
10. Lonczak, HS, Neighbors, C, and Donovan, DM. Predicting risky and angry driving as a function of gender. Accid Anal Prev. (2007) 39:536–45. doi: 10.1016/j.aap.2006.09.010
11. Woods, D, Dekker, S, Cook, R, Johannesen, L, and Sarter, N. Behind human error. London, UK: CRC Press (2017).
12. Elander, J, West, R, and French, D. Behavioral correlates of individual differences in road-traffic crash risk: an examination of methods and findings. Psychol Bull. (1993) 113:279–94. doi: 10.1037/0033-2909.113.2.279
13. Reason, J, Manstead, A, Stradling, S, Baxter, J, and Campbell, K. Errors and violations on the roads: a real distinction? Ergonomics. (1990) 33:1315–32. doi: 10.1080/00140139008925335
14. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DG. PRISMA group* t. preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. (2009) 151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
15. Sampson, M, McGowan, J, Cogo, E, Grimshaw, J, Moher, D, and Lefebvre, C. An evidence-based practice guideline for the peer review of electronic search strategies. J Clin Epidemiol. (2009) 62:944–52. doi: 10.1016/j.jclinepi.2008.10.012
16. Higgins, JPT, and Green, S. (Eds.). Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0), Chichester, UK: John Wiley & Sons. (2011). Available at: https://handbook-5-1.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.htm (Cochrane Handbook)
17. Liberati, A, Altman, DG, Tetzlaff, J, Mulrow, C, Gøtzsche, PC, Ioannidis, JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. (2009) 151:W-65–94. doi: 10.7326/0003-4819-151-4-200908180-00136
18. Minozzi, S, Cinquini, M, Gianola, S, Gonzalez-Lorenzo, M, and Banzi, R. The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application. J Clin Epidemiol. (2020) 126:37–44. doi: 10.1016/j.jclinepi.2020.06.015
19. Igelström, E, Campbell, M, Craig, P, and Katikireddi, SV. Cochrane's risk of bias tool for non-randomized studies (ROBINS-I) is frequently misapplied: a methodological systematic review. J Clin Epidemiol. (2021) 140:22–32. doi: 10.1016/j.jclinepi.2021.08.022
20. Ma, L-L, Wang, Y-Y, Yang, Z-H, Huang, D, Weng, H, and Zeng, X-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Mil Med Res. (2020) 7:1–11. doi: 10.1186/s40779-020-00238-8
21. DiClemente, RJ, Salazar, LF, and Crosby, RA. Health behavior theory for public health: Principles, foundations, and applications. Burlington, USA: Jones & Bartlett Publishers (2013).
22. Luszczynska, A, and Schwarzer, R. Social cognitive theory. Fac Health Sci Publ. (2015) 2015:225–51.
23. Nadimi, N, Khalifeh, V, Khoshdel Sangdeh, A, and Mohammadian, AA. Evaluation of the effect of driving education and training programs on modification of driver's dangerous behaviors. Int J Transp Eng. (2021) 8:399–414. Available at: https://www.magiran.com/paper/2347893
24. Cutello, CA, Gummerum, M, Hanoch, Y, and Hellier, E. Evaluating an intervention to reduce risky driving behaviors: taking the fear out of virtual reality. Risk Anal. (2021) 41:1662–73. doi: 10.1111/risa.13643
25. Fowode, KV, Nwaogazie, IL, and Anyanwu, BO. Effect of safety education intervention on knowledge of road accident prevention among drivers in Lagos state, Nigeria. Open J Saf Sci Technol. (2023) 13:89–100. doi: 10.4236/ojsst.2023.133005
26. Nthoki, B, Biwott, C, and Kamau, A. Influence of information, education and communication on road safety amongst Boda-Boda motorcyclists in Kenyan cities. East Afr J Humanit Soc Sci. (2024) 3:120–30. doi: 10.58721/eajhss.v3i1.605
27. Habyarimana, J, and Jack, W. Results of a large-scale randomized behavior change intervention on road safety in Kenya. Proc Natl Acad Sci USA. (2015) 112:E4661–70. doi: 10.1073/pnas.1422009112
28. Campbell, B, Heitner, J, Amos Mwelelo, P, Fogel, A, Mujumdar, V, Adams, LV, et al. Impact of SMS text messaging reminders on helmet use among motorcycle drivers in Dar Es Salaam, Tanzania: randomized controlled trial. J Med Internet Res. (2022) 24:e27387. doi: 10.2196/27387
29. Onuka, AO, and Akinyemi, TF. The effectiveness of Frsc public education programme on drivers' road traffic habit in Lagos and Oyo state of Nigeria. British Journal of Arts and Social Sciences, British Journal Publishing, Inc.(ResearchGate). (2012) 6, 129–139. Available at: https://www.researchgate.net/publication/303345001_The_Effectiveness_of_FRSC_Public_Education_Programme_on_Drivers’_Road_Traffic_Habit_in_Lagos_and_Oyo_States_of_Nigeria(ResearchGate)
30. Stephan, K, Stephens, AN, Scully, M, Mitsopoulos-Rubens, E, and Newstead, SV. Outcome evaluation of the p drivers program: randomised controlled trial of a program to improve safe driving among novice drivers. Accid Anal Prev. (2024) 201:107569. doi: 10.1016/j.aap.2024.107569
31. Okafor, IP, Odeyemi, KA, Dolapo, DC, Ilika, AL, and Omosun, AO. Effectiveness of road safety education in Nigeria using a quasi-experimental trial: findings from the road safety intervention project. Afr Saf Promot. (2015) 12:1–17. Available at: https://www.ajol.info/index.php/asp/article/view/118305
32. Abdul-Wahab, I. Evaluating effectiveness of federal road safety commission training and education programmes for commercial vehicle drivers in Jigawa state, Nigeria. IFE Psychol. (2016) 24:127–39. doi: 10.10520/EJC192263
33. Mazengia, EM, Kassie, A, Zewdie, A, and Demissie, GD. A qualitative study of perception related to risky driving behavior in Debre Markos City, north West Ethiopia, 2021. BMC Public Health. (2023) 23:977. doi: 10.1186/s12889-023-15862-x
34. Jaensirisak, S, and Luathep, P. Evaluation of unsafe driving behaviour change by road safety education Asian Transp Res Soc Available online at: http://www.atransociety.com/resources/pdf/pdfResearchResources/2019/Project2019-001(Dr.Sittha).pdf (2020).
35. Mabayoje, ED. Multimedia-based road safety education and driving behaviour among interstate commercial mini-bus drivers in Ibadan metropolis. Nigeria: repository.pgcollege.ui.edu.ng. (2019).
36. Mohamed, AA, Mohammed, NY, and Mahmoud, A. Effect of implementing traffic safety awareness program on Driver’s knowledge regarding traffic safety practices in Alexandria-Egypt. Nurs Health Sci. (2018) 7:39–56. doi: 10.9790/1959-0704113956
37. Nwadinigwe, IP, Osarenren, NA, and Otuagoma, FA. Impact of road safety education on commercial drivers’ knowledge and behaviour towards road traffic codes and safety driving in Delta state. Int J Educ Res. (2018) 5:110–20. Available at: https://www.ajol.info/index.php/ijer/article/view/180880
38. Prestwich, A, Kenworthy, J, and Conner, M. Health behavior change: Theories, methods and interventions. London, UK: Routledge (2017).
39. Peters, G-JY, Ruiter, RA, and Kok, G. Threatening communication: a critical re-analysis and a revised meta-analytic test of fear appeal theory. Health Psychol Rev. (2013) 7:S8–S31. doi: 10.1080/17437199.2012.703527
40. Williams, KC. Fear appeal theory. Res Bus Econ J. (2012) 5:1–21. Available at: https://www.researchgate.net/publication/265807800_Fear_Appeal_Theory
41. Sibbald, B, and Roland, M. Understanding controlled trials. Why are randomised controlled trials important? BMJ. (1998) 316:201. doi: 10.1136/bmj.316.7126.201
42. Campbell, DT, and Stanley, JC. Experimental and quasi-experimental designs for research. Massachusetts, USA: Ravenio books (2015).
43. Creswell, JW, Fetters, MD, and Ivankova, NV. Designing a mixed methods study in primary care. Ann Fam Med. (2004) 2:7–12. doi: 10.1370/afm.104
44. Tenny, S, Brannan, JM, and Brannan, GD. Qualitative study. StatPearls Publishing (repository.ui.edu.ng) (2017) Available at: https://www.ncbi.nlm.nih.gov/books/NBK470395/.
Keywords: behavior change interventions, dangerous driving behavior, risky driving behavior, road safety, outcome measurement, randomized control trial
Citation: Fanai S, Okyere E and Marfoh K (2025) Behavior change interventions for dangerous driving behavior in low- and middle-income countries: a systematic review of interventions and outcome measurement instruments. Front. Public Health. 13:1597331. doi: 10.3389/fpubh.2025.1597331
Edited by:
Jaeyoung Jay Lee, Central South University, ChinaReviewed by:
Juneyoung Park, Hanyang University, Republic of KoreaJooyoung Lee, Hannam University, Republic of Korea
Copyright © 2025 Fanai, Okyere and Marfoh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Saen Fanai, c2ZhbmFpODBAZ21haWwuY29t
†ORCID: Eunice Okyere, orcid.org/0000-0003-3566-7561