 Mohamed Aly1*†
Mohamed Aly1*† Achraf Ammar2,3,4†
Achraf Ammar2,3,4† Khaled Trabelsi3,5,6
Khaled Trabelsi3,5,6 Liwa Masmoudi3Noha El-Gyar7
Liwa Masmoudi3Noha El-Gyar7 Amira M. Shalaby7
Amira M. Shalaby7 Osama Abdelkarim1
Osama Abdelkarim1- 1Faculty of Sport Sciences, Assiut University, Assiut, Egypt
- 2Department of Training and Movement Science, Institute of Sport Science, Johannes Gutenberg University Mainz, Mainz, Germany
- 3High Institute of Sport and Physical Education of Sfax, University of Sfax, Sfax, Tunisia
- 4Research Laboratory, Molecular Bases of Human Pathology, Faculty of Medicine of Sfax, University of Sfax, Sfax, Tunisia
- 5Research Laboratory Education, Motricity, Sport and Health, EM2S, High Institute of Sport and Physical Education of Sfax, University of Sfax, Sfax, Tunisia
- 6Department of Movement Sciences and Sports Training, School of Sport Science, The University of Jordan, Amman, Jordan
- 7Faculty of Medicine, Department of Pediatrics, Assiut University, Assiut, Egypt
Background: Physical inactivity among children is a growing public health concern, particularly in Mediterranean countries, where lifestyle changes have contributed to declining physical fitness levels. Structured school-based interventions have shown promise in improving children’s health-related physical fitness (HRF), but cross-cultural differences in intervention effectiveness remain understudied. This study, conducted within the DELICIOUS project, evaluates the impact of a standardized physical activity (PA) intervention on HRF components among children (8–10 years) and early adolescents (11–14 years) from five Mediterranean countries: Egypt, Italy, Lebanon, Portugal, and Spain.
Methods: A total of 937 participants aged 8–14 years took part in a six-month school-based PA program designed to enhance speed, agility, muscular strength, cardiovascular endurance, and coordination. Physical fitness was assessed using the International Physical Performance Test Profile (IPPTP) before and after the intervention. A three-way repeated measures ANOVA (Time × Age × Country) assessed intervention effects on anthropometric and fitness variables, while a two-way ANOVA (Age × Country) examined the percentage changes in these HRF across age groups and countries.
Results: Significant improvements were observed across multiple health-related fitness components, particularly in speed, lower-body power, coordination, muscular endurance, and cardiovascular endurance. Early adolescents (11–14 years) generally showed greater gains than younger children (8–10 years). The magnitude of improvement in fitness outcomes varied by country. Lebanon and Portugal recorded the most substantial gains in sprint, strength, and endurance. Spain and Italy showed relatively smaller improvements, especially among younger participants, whereas Egyptian students demonstrated notable gains in sprint performance and endurance, particularly among early adolescents, along with the most significant BMI reduction observed in the study. BMI remained stable across participants, suggesting that fitness improvements were achieved alongside healthy growth, without adverse changes in body composition.
Conclusion: A structured PA intervention can effectively improve HRF in children across Mediterranean countries, though outcomes vary by age and cultural context. These findings highlight the need for tailored, school-based PA programs that consider baseline fitness levels and regional factors. Implementing such interventions could play a crucial role in addressing physical inactivity and fostering long-term health benefits in children.
1 Introduction
Physical activity (PA) during childhood is a cornerstone of healthy development, offering physical, mental, and cognitive benefits (1, 2). Regular engagement in PA in children and adolescents improves cardiorespiratory fitness, muscular strength, bone health, coordination, and metabolic function. It also contributes to cognitive outcomes such as memory, attention, and academic performance (3–5). Conversely, insufficient activity increases the risk of obesity and related noncommunicable diseases (6) even from an early age (7, 8). The World Health Organization (WHO) reports that approximately 80% of adolescents globally fail to meet the recommended 60 min of moderate-to-vigorous PA per day (9). This inactivity crisis has contributed to a documented decline in youth physical fitness over the past few decades. For example, longitudinal analyses have revealed substantial drops in children’s cardiorespiratory endurance (a key indicator of aerobic fitness) since the 1980s, reflecting a worrying erosion in health-related fitness (HRF) levels across many countries (10–12). Recent evidence suggests that this inactivity crisis has been further exacerbated by the COVID-19 pandemic, which led to widespread school closures, increased sedentary behavior, and reduced access to structured PA for children and adolescents (13–15). These trends underscore the urgent need for effective interventions to promote PA and improve health-related fitness in young populations.
HRF in youth typically encompasses several fundamental components: muscular strength (including power and endurance), cardiorespiratory endurance, speed, agility, coordination, flexibility, and healthy body composition (16). Higher fitness levels during childhood are associated with healthier body weight, improved cardiovascular profiles, and better mental health outcomes in later life (17). Additionally, components such as speed and agility reflect motor skill development (18), while strength and endurance support functional independence (19, 20). Coordination enables complex movements and overall physical proficiency. Developing these skills early can influence lifelong adherence to active lifestyles and reduce the risk of chronic diseases (21, 22). To evaluate these fitness components in children, various standardized assessment protocols have been developed and validated in the pediatric population. These tools aim to provide comprehensive, age-appropriate measures of fitness across domains such as strength, speed, endurance, and coordination. One notable example is the ASSO Project, which proposed a Fitness Index model specifically designed for Italian adolescents living in Southern Italy and provided valuable normative data within that context (23). Such tools emphasize the importance of culturally adapted and validated assessments and highlight the value of comparing data across different populations using standardized instruments. These considerations reinforce the need for employing robust, cross-culturally applicable tools—such as the International Physical Performance Test Profile (IPPTP)—in multi-national studies.
Despite the known benefits of PA, many children, particularly in certain regions, are not achieving adequate fitness. In Mediterranean countries, historically associated with active lifestyles and healthy diets, recent data show high rates of childhood overweight and obesity (24). Sedentary behaviors and dietary shifts have led to declining activity levels and reduced physical fitness (25–27). For example, surveillance data show that about one-third of children aged 6 to 9 in Southern Europe are overweight, with prevalence particularly high in countries like Italy, Spain, Greece, and Cyprus (28). These trends present important public health challenges.
Structured interventions, particularly in school settings, have emerged as key strategies to counteract these negative trends. Numerous studies have shown that school-based PA programs can enhance various components of fitness, such as aerobic capacity, muscular strength, and motor coordination (29–32). Systematic reviews support the effectiveness of frequent physical education sessions in improving children’s health-related fitness (33). Multi-component programs that combine aerobic exercise, strength training, and skill-based activities have also proven effective, even within relatively short periods (34, 35). However, intervention outcomes may vary depending on baseline fitness levels and lifestyle factors. Children with lower initial fitness often show greater improvements, while those who are already active may experience smaller gains. Cultural and environmental factors also influence program effectiveness due to differences in school curricula, access to extracurricular sports, and general attitudes toward PA (36, 37). These findings suggest the need to test interventions in diverse settings, particularly in culturally heterogeneous regions like the Mediterranean.
This study is conducted within the framework of the DELICIOUS project—a multinational initiative aimed at promoting healthy Mediterranean diet and lifestyle (including regular PA) among children in Mediterranean countries (38). DELICIOUS (an acronym for “Diet and Eating habits, Lifestyle Interventions for Children In secOndary schools and primary schools to Upraise Mediterranean Sustainable food habits,” a hypothetical expansion) is a 3-year project supported by the EU PRIMA program, involving five countries: Egypt, Italy, Lebanon, Portugal, and Spain (39). A key objective of DELICIOUS is to counteract the decline in Mediterranean children’s fitness and dietary habits by implementing school-based interventions that encourage more active lifestyles and better nutrition.
In the present study, we present a comparative analysis of the effect of the DELICIOUS PA intervention on health-related fitness components in children from five Mediterranean countries. To our knowledge, this is one of the first multi-country studies to evaluate a unified PA program in a Mediterranean context, allowing cross-cultural comparisons of intervention effectiveness. The specific objectives of the study are: (1) to determine the extent to which the intervention improves each of the targeted fitness components (speed, agility, muscular strength, cardiovascular endurance, and coordination) in children; and (2) to compare the magnitude of these fitness changes across the five countries, and between two age groups (children aged 8–10 vs. early adolescents aged 11–14), enabling more tailored practical recommendations. We hypothesize that all participating countries will show improvements in most fitness measures after the intervention, but the degree of improvement may vary, with potentially larger gains in settings with lower baseline fitness or less prior exposure to organized PA. By addressing these aims, the study seeks to inform how school-based PA interventions can be adapted for diverse cultural settings, with implications for public health. Its findings would help guide strategies to improve youth fitness and reduce inactivity, ultimately supporting healthier adult populations and global health goals.
2 Materials and methods
2.1 Participants
The study sample was drawn from partner countries within the DELICIOUS consortium: Egypt, Italy, Lebanon, Portugal, and Spain. Primary goals and objectives of the DELICIOUS project, a comprehensive descriptive and intervention study aimed at promoting the Mediterranean diet and an active lifestyle among school children and adolescents, have been detailed elsewhere (38, 40). A formal sample size calculation was not performed prior to recruitment. Instead, a pragmatic approach was adopted, aiming to enroll the maximum number of eligible participants across the five participating Mediterranean countries. Schools were selected based on willingness and logistical feasibility, and the majority of eligible children within participating schools were invited to take part in the study. Thus, a convenience sampling strategy was employed to balance scientific rigor with practical constraints related to project timelines, resources, and field implementation across multiple countries. Accordingly, a total of 937 children and early adolescents aged 8 to 14 years were recruited from participating schools in urban areas across five Mediterranean cities: Assiut (Egypt), Lisbon (Portugal), Beirut (Lebanon), Cordoba (Spain), and Giugliano in Campania (Italy). To account for potential age-related differences in fitness levels, participants were stratified into two age groups: 8–10 years (children) and 11–14 years (early adolescents). Written informed consent was obtained from parents or legal guardians of all participants prior to the children’s participation. The study adhered to the ethical standards outlined in the Declaration of Helsinki and was approved by the ethics committee of Mondragon University (no. IEB-20230704).
2.2 Physical activity intervention program
A standardized, school-based physical activity intervention program was developed within the DELICIOUS project and implemented across all participating Mediterranean countries. Inspired by evidence-based models such as “Build Our Kids’ Success (BOKS)” (41), the program aimed to enhance key components of physical fitness—speed, agility, strength, endurance, and coordination—through structured, age-appropriate, and non-competitive activities that emphasize personal progress and inclusivity, particularly for children who are typically less active. The intervention was delivered over a six-month period and included a comprehensive series of activity plans targeting functional movement skills. Each session followed a standardized structure comprising a warm-up, skill instruction, movement-based exercises, and engaging games designed to reinforce the targeted skills. Sessions were conducted three times per week, with each lasting between 40 and 45 min. Implementing a uniform program across culturally distinct settings allowed for the examination of cross-cultural variability in outcomes and intervention effectiveness.
2.3 Measures
2.3.1 International Physical Performance Test Profile
The International Physical Performance Test Profile (IPPTP) is a standardized and validated test battery designed to assess HRF in children and adolescents. It provides a comprehensive evaluation of key fitness components, including speed, agility, strength, endurance, and coordination, making it particularly well-suited for cross-cultural studies (29, 42–45). Developed based on the methodologies of Bös and Mechling (46) and the German Motor Test 6–18 (47), the IPPTP comprises eight test items that encompass the five fundamental dimensions of physical fitness: endurance, strength, speed, coordination, and flexibility. These tests are widely recognized as valid and reliable field-based measures of core physical fitness components in pediatric populations. Prior research, including Bianco et al. (23), demonstrated strong correlations between these tests and other health-related fitness components in adolescents, confirming their suitability for large-scale youth fitness evaluations. For this study, six specific tests from the IPPTP were selected to target the core aspects of physical fitness relevant to children’s HRF. These tests were chosen for their high validity in measuring fitness components across culturally diverse populations and their robustness in cross-cultural applications. For this study, six tests were selected to target core aspects of children’s HRF: the 20 m Dash test assessed speed by recording sprint times over 20 meters; the Sideways Jumping (JSW) test measured agility and coordination through the number of lateral jumps in 15 s; the Push-Up (PU) test evaluated upper body strength and endurance by counting the total push-ups completed in 40 s; the Sit-Up (SU) test assessed core strength through the number of sit-ups performed in 40 s; the Standing Long Jump (SLJ) test measured lower body strength by the distance jumped from a standing position in centimeters; and the 6-Minute Run test assessed cardiovascular endurance by the total distance covered in meters. All tests were conducted under standardized conditions to ensure consistency and reliability across the diverse sample populations. The reproducibility and validity of the IPPTP have been established in previous research (29, 42). For additional details on these test items, readers are referred to the corresponding manuals (44).
2.3.2 Anthropometry
Height and weight were recorded before testing. Height was measured to the nearest 0.1 cm using a portable stadiometer (Seca 213, Seca GmbH & Co. KG, Hamburg, Germany), while weight was measured using a Tanita digital body composition scale (BF-350 Total Body Composition Analyzer, Amsterdam, the Netherlands), following standardized anthropometric protocols. Body mass index (BMI) was then calculated using the formula: BMI = weight (kg)/height (m2).
2.3.3 Statistical analysis
All statistical analyses were conducted using SPSS (version 25). The normality of the data was verified using the Shapiro–Wilk test. A three-way repeated measures ANOVA (2 levels for time: pre- and post-intervention × 2 levels for age groups: 8–10 years and 11–14 years × 5 levels for countries) was performed to evaluate the effects of the intervention program on body weight, height, BMI, and various physical fitness variables across different age groups and countries using pre- and post-intervention data. Additionally, a two-way ANOVA (2 levels for age groups × 5 levels for countries) was applied to assess the effects of the intervention program on the same parameters using percentage changes from pre- to post-intervention. Post-hoc differences were investigated using the Bonferroni test to identify pairwise comparisons between groups. Effect size was calculated using partial eta squared (ηp2) to evaluate the magnitude of change. Statistical significance was set a priori at p < 0.05 for all analyses.
3 Results
A total of 354 children (aged 8–10 years) and 583 early adolescents (aged 11–14 years) were included in the final analysis. Participants were distributed as follows: 204 from Egypt (49 children and 155 early adolescents), 200 from Lebanon (92 children and 108 early adolescents), 150 from Italy (111 children and 39 early adolescents), 202 from Spain (32 children and 170 early adolescents), and 181 from Portugal (70 children and 111 early adolescents).
3.1 Effects of the intervention program on body weight, height, and BMI across different age groups and countries
Table 1 presents the effects of time (pre- and post-intervention), age, and country of living on weight, height, and BMI. The three-way repeated measures ANOVA revealed significant Time × Age × Country interactions for weight, height, and BMI (p = 0.03, p < 0.01, and p = 0.02, respectively), as well as significant main effects of sex and country on all three variables (p < 0.001). A significant main effect of time was observed for weight and height (p < 0.001), but not for BMI (p = 0.08). Post-hoc analysis showed that weight increased significantly after the intervention in Lebanon and Portugal across both age groups (p < 0.05), in Italy only for the 8–10 years age group (p < 0.05), and in Spain only for the 11–14 years age group (p < 0.05). No significant weight changes were observed in any age group among Egyptian participants (p > 0.05). Height significantly increased from pre- to post-intervention in both age groups in most countries (p < 0.05), except in Italy, where this difference was significant only for the 8–10 years age group (p < 0.05). Participants aged 11–14 years showed significantly higher weight and height values compared to those aged 8–10 years (p < 0.05) in most countries, except in Italy. The highest weight and height values across both age groups were recorded in Spain.

Table 1. Body weight, height, and BMI at pre- and post-intervention categorized by age-group and countries.
For BMI, the intervention program significantly reduced BMI only in Egypt for the 11–14 years age group (p < 0.05), while BMI increased significantly in Lebanon across both age groups and in Italy for the 8–10 years age group (p < 0.05). Significantly higher BMI values at the older age were observed only in the Lebanese population (p < 0.05). The highest BMI values were recorded in Italy and Spain for the 8–10 years age group, showing significantly higher values than Lebanon and Portugal (p < 0.05). At the older age group (11–14 years), no significant differences in BMI were observed between countries.
Figure 1 illustrates the effect of age and country on the percentage change in body weight, height, and BMI. The two-way ANOVA revealed significant Age × Country interactions for height [F(4,910) = 11.45, p < 0.001, ηp2 = 0.05] and BMI [F (4,910) = 2.66, p = 0.03, ηp2 = 0.01]. Significant main effects of age were found for height [F(1,910) = 63.73, p < 0.001, ηp2 = 0.07] and BMI [F(1,910) = 5.04, p = 0.02, ηp2 = 0.01], while significant main effects of country were observed for weight [F(4,910) = 19.04, p < 0.001, ηp2 = 0.08], height [F(4,910) = 40.85, p < 0.001, ηp2 = 0.15], and BMI [F(4,910) = 24.17, p < 0.001, ηp2 = 0.10]. Post-hoc analysis revealed that the highest increase in body weight was recorded in Lebanon for both age groups (5.9 and 5.1%, respectively), with significantly higher percentage changes compared to Egypt and Spain in both age groups, and to Portugal in the 11–14 years group (p < 0.05). For height percentage change, the highest increase was observed among Portuguese children aged 8–10 years (2.1%), which was significantly higher than in Egypt, Lebanon, and Italy (p < 0.05). For BMI percentage change, only Egypt and Spain showed negative changes in both the 8–10 years group (−1.5% and −2.5%, respectively) and the 11–14 years group (−1.4% and −0.5%, respectively), indicating a decrease in BMI. Post-hoc analysis revealed significant differences in BMI percentage change between Egypt and Lebanon in both age groups, Egypt and Italy in children, and Egypt and Portugal, as well as Spain and Portugal, in early adolescent (p < 0.05).
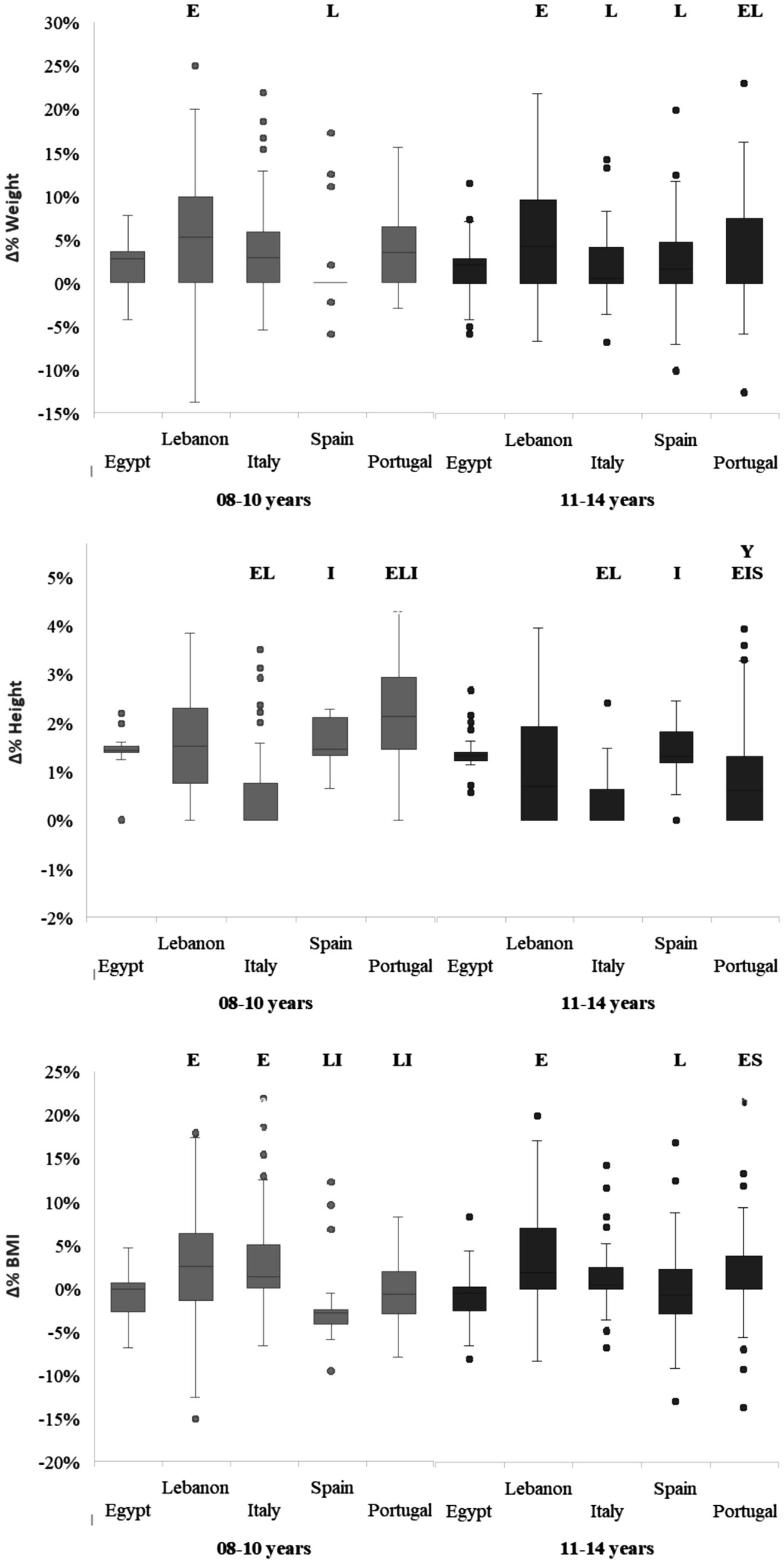
Figure 1. Percent change in body weight, Height, and BMI from pre- to post-intervention, categorized by age group and countries. Y, significant difference compared to younger age group (8–10 years); E, significant difference compared to Egypt; L, significant difference compared to Lebanon; I, significant difference compared to Italy; S, significant difference compared to Spain; at p < 0.05.
In terms of age effects, no significant differences were recorded between the two age groups in any country for both weight and BMI percentage changes. However, for height percentage change, only the Portuguese population showed a significant difference between age groups, with a higher change recorded in the 8–10 years group (p < 0.05).
3.2 Effects of the intervention program on physical fitness performances across different age groups and countries
Table 2 presents the effects of time, age, and country of living on physical fitness performance variables. The three-way repeated measures ANOVA revealed significant Time × Age × Country interactions for most variables (p < 0.001), except for JSW, which showed significant Time × Age and Time × Country interactions (p < 0.001). Significant main effects of time were observed for all variables (p < 0.001), and significant main effects of country were also recorded (p = 0.02 to p < 0.001). Significant main effects of age were found for most physical fitness performance variables (p = 0.03 to p < 0.001), except for the 6-min Run test.
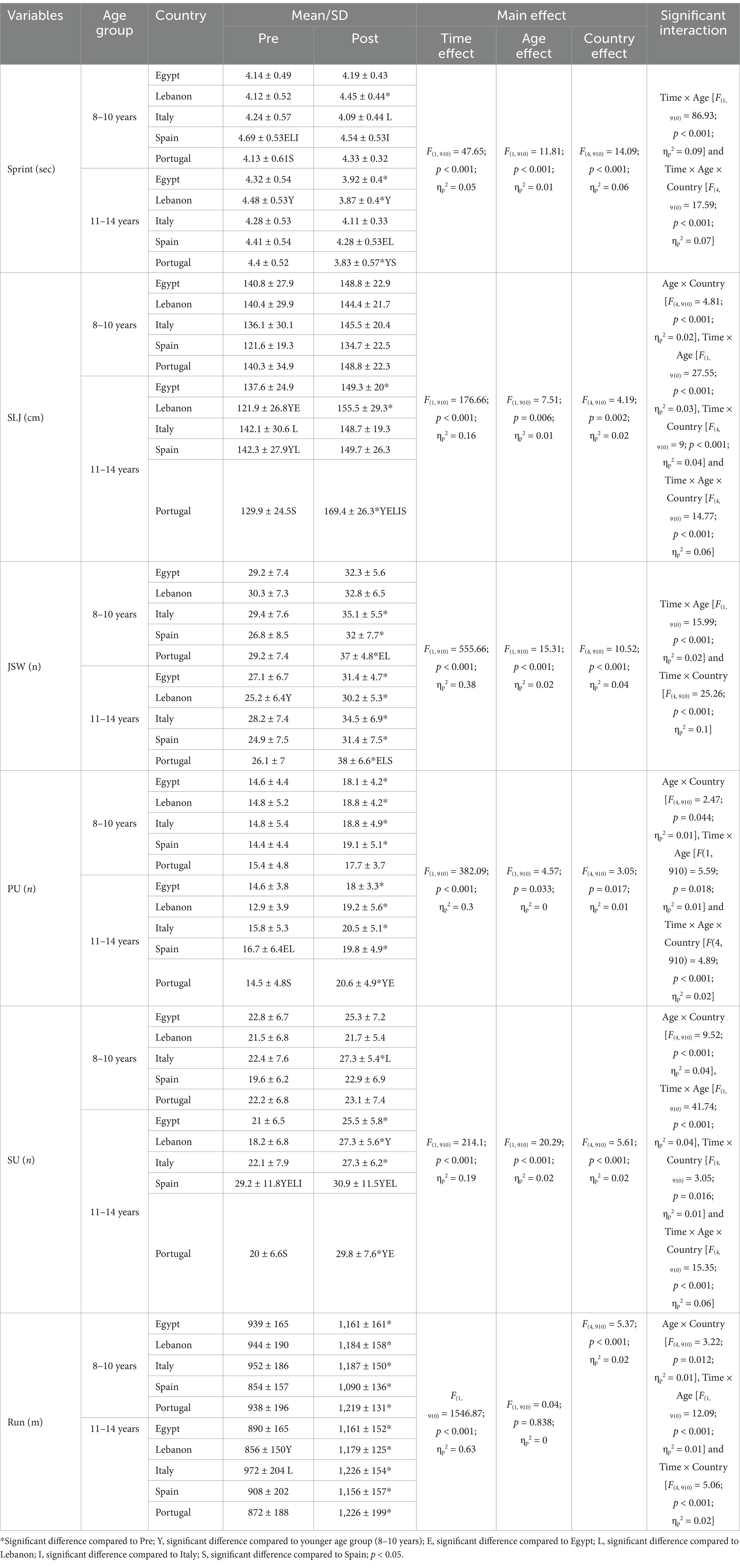
Table 2. Physical fitness performance.
Sprint performance significantly improved (decrease in time) after the intervention in most countries, except for Italy and Spain in the 11–14 years age group (p < 0.05), while no significant improvement was observed in any country for the 8–10 years age group. Better performance in the older age group was recorded only in Lebanon and Portugal (p < 0.05). At the younger age (8–10 years), Italian children outperformed Spanish participants, who also showed the worst performance in the older age group compared to those from Egypt, Lebanon, and Portugal.
SLJ performance improved significantly only in the 11–14 years age group, specifically in Egypt, Lebanon, and Portugal (p < 0.05). Overall, SLJ performance declined with older age, particularly in the Lebanese, Spanish, and Portuguese populations. Performance was comparable across countries in the younger age group (8–10 years), while Portugal showed significantly better performance post-intervention in the older age group (11–14 years; p < 0.05).
JSW performance improved significantly from pre- to post-intervention in most countries and age groups (p < 0.05), except in Egypt and Lebanon for the younger age group. The highest post-intervention performance was recorded in the Portuguese population across both age groups (p < 0.05), with generally comparable values between age groups in all countries.
PU performance improved significantly from pre- to post-intervention in most countries and age groups (p < 0.05), except in Portugal for the younger age group. Performance was generally comparable between age groups and countries, except for Portugal, which showed higher performance in the older age group and outperformed Egypt at this age (p < 0.05).
SU performance improved significantly only in Italy for the 8–10 years age group and in most countries for the 11–14 years age group (p < 0.05), except in Spain. Older age groups showed higher performance in Lebanon, Spain, and Portugal (p < 0.05). Post-intervention performance was higher in Italy compared to Lebanon for the younger age group and higher in Spain and Portugal for the older group (p < 0.05).
Endurance performance during the 6-min running test improved significantly in both age groups across all countries (p < 0.05), with generally comparable results between age groups and countries.
Figure 2 illustrates the effects of age and country on the percentage change in various physical fitness performance variables. The two-way ANOVA revealed significant Age × Country interactions for sprint, SLJ, PU, and SU, with p-values ranging from 0.003 to <0.001 and ηp2 values between 0.02 and 0.08. Significant main effects of age were found for most variables, except PU, with p < 0.001 and ηp2 values between 0.01 and 0.09. Significant main effects of country were observed for SLJ, JSW, SU, and the 6-min Run, with p-values ranging from 0.002 to <0.001 and ηp2 values between 0.02 and 0.06.
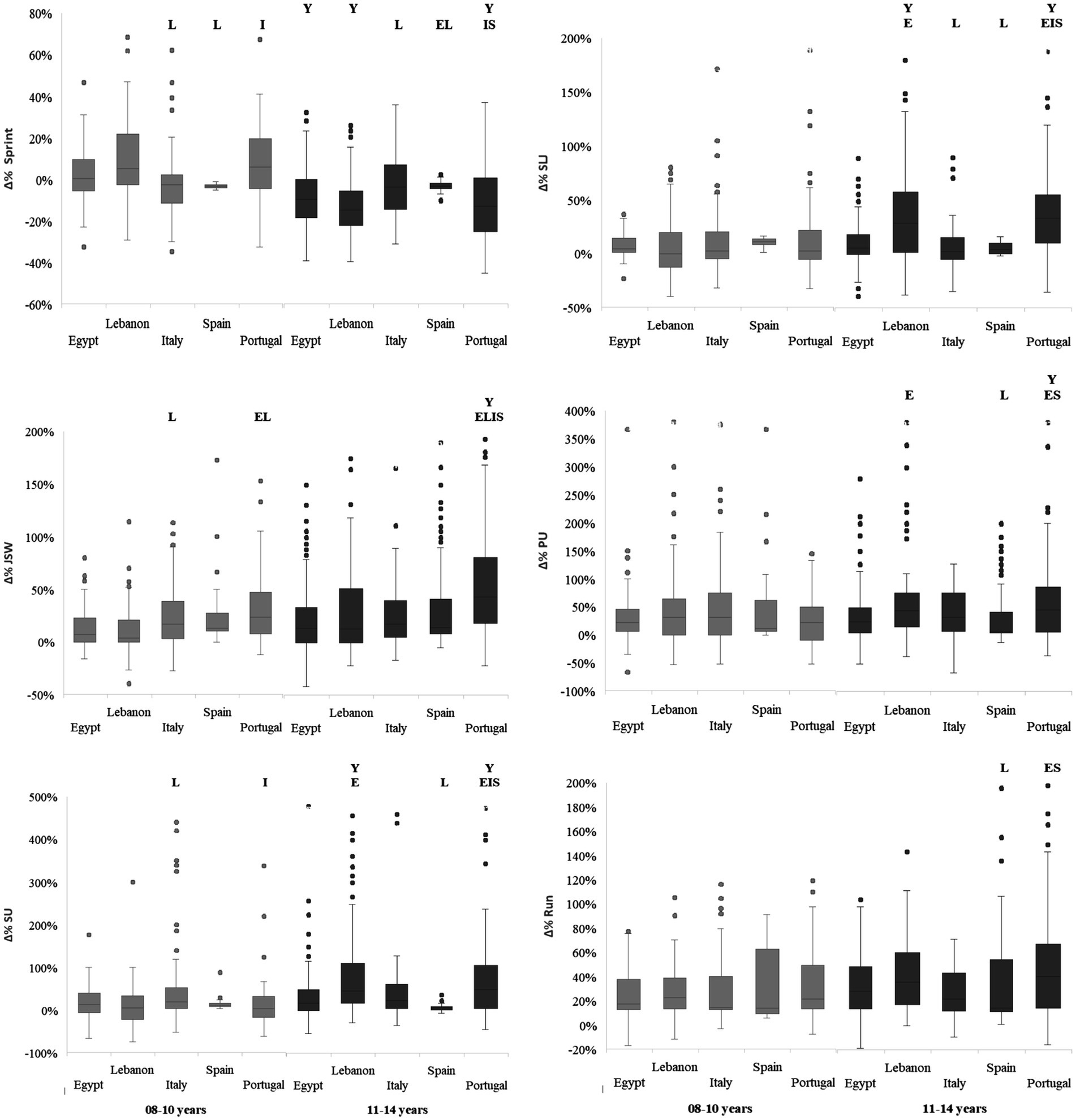
Figure 2. Percent change in physical fitness variables from pre- to post-intervention, categorized by age group and countries. Y, significant difference compared to younger age group (8–10 years); E, significant difference compared to Egypt; L, significant difference compared to Lebanon; I, significant difference compared to Italy; S, significant difference compared to Spain at p < 0.05.
Post-hoc analysis revealed that, for most studied parameters, the most significant differences between countries were observed in the 11–14 years age group. For sprint percentage change, the greatest improvements (largest decreases) were recorded in Lebanon (−13.7%) and Portugal (−12.9%), followed by Egypt (−9.3%) in the 11–14 years age group, with significant differences compared to Spain and Italy (p < 0.05). In contrast, improvements in the 8–10 years age group were minimal, not exceeding 3.4% (as observed in Italy and Spain), while the remaining countries showed worsened performance (positive percentage changes). For SLJ percentage change, the highest improvements were observed in Lebanon and Portugal (28–30%) in the 11–14 years age group, which were significantly higher than those in Spain and Italy (p < 0.05). However, in the younger age group (8–10 years), percentage changes were comparable across countries (p > 0.05).
JSW performance showed positive percentage changes across all countries in both age groups. In the 8–10 years age group, the highest improvement was recorded in Portugal (27%), followed by Italy and Spain (19%). In the 11–14 years age group, Portugal again exhibited the highest improvement (46%), which was significantly greater than the percentage changes observed in the other countries (p < 0.05).
PU performance followed a similar positive trend. In the 8–10 years age group, the highest improvement was observed in Spain (32.5%), followed by Lebanon and Italy (27%), with no significant differences between countries. In the 11–14 years age group, the highest improvements were recorded in Lebanon (49%) and Portugal (43%), which were significantly higher than those in Spain and Egypt (p < 0.05).
Positive percentage changes in SU performance were observed across all age groups and countries. In the 8–10 years age group, the highest improvement was recorded in Italy (22%), showing significant differences compared to Lebanon and Portugal (p < 0.05). In the 11–14 years age group, the greatest improvements were observed in Lebanon and Portugal (approximately 50%), which were significantly higher than those in Egypt, Italy, and Spain (p < 0.05).
Endurance performance registered positive percentage changes across all age groups and countries, with comparable improvements ranging from 24 to 30% in the 8–10 years age group (p > 0.05). In the 11–14 years age group, the highest values were recorded in Portugal (40.5%) and Lebanon (38%), which were significantly higher than those in Spain (p < 0.05) and Egypt (when compared to Portugal, p < 0.05).
In terms of age effects, significantly higher improvements at the 11–14 years age group compared to 8–10 years were primarily observed in Portugal across all physical fitness variables except Run (p < 0.05), in Lebanon for Sprint, SLJ, and SU (p < 0.05), and in Egypt for Sprint only (p < 0.05).
4 Discussion
4.1 Main findings and interpretations
Our findings demonstrate that the school-based PA intervention led to significant improvements in several components of health-related fitness—specifically speed, lower-body power, coordination, muscular endurance, and cardiovascular endurance—across all five Mediterranean countries. However, these improvements were not uniform. Early adolescents (11–14 years) generally experienced greater gains than younger children (8–10 years), and the magnitude of improvement varied between countries. For instance, early adolescents in Lebanon and Portugal exhibited notable improvements in sprint performance and endurance capacity, while younger children in those and other countries showed more modest changes. Some groups, particularly the younger age group, did not significantly improve in certain tests such as the 20 m sprint. This suggests that the intervention’s effects were moderated by developmental stage. This age-related disparity aligns with physiological evidence that prepubertal children typically show a reduced training response, achieving only about half the gains seen in postpubertal individuals under similar exercise conditions (48, 49). Therefore, the greater gains among early adolescents in our study may reflect their higher responsiveness to training, whereas younger children may benefit from longer or more intensive interventions. Additionally, the pronounced improvements observed in speed and strength are likely driven by rapid neuromuscular adaptations, such as enhanced motor unit recruitment, firing frequency, and coordination efficiency (50). In contrast, improvements in endurance capacity require more time, as they depend on adaptations of the cardiovascular and respiratory systems—including increased stroke volume, enhanced capillary density, and improved mitochondrial function—which involve more extensive tissue remodeling and slower physiological processes (51, 52). This difference in adaptation timelines helps explain why gains in speed and strength were more immediate, whereas endurance improvements were more gradual.
Cross-country differences in outcomes were also evident and align closely with our data, underscoring the influence of contextual factors on intervention effectiveness. For instance, Portugal and Lebanon not only had high baseline potential for improvement but also realized the greatest post-intervention gains in several fitness components (such as push-ups, sit-ups, and endurance run), whereas Spain and Italy showed smaller improvements in some measures. Countries with lower baseline fitness (e.g., Lebanon, Portugal) showed the greatest improvements, while fitter countries (e.g., Spain) exhibited smaller gains, possibly due to a ceiling effect. By the end of the intervention, previously observed fitness disparities between countries were somewhat altered: for example, Portuguese early adolescents showed the greatest improvements in endurance, followed by Lebanese and Spanish peers, with all three outperforming the younger groups. Our findings confirm that universal school-based programs may not yield uniform results, as differences in curricula, sports access, and initial fitness influence outcomes (36, 53). Factors such as variations in physical education curricula, extracurricular sports opportunities, and baseline fitness likely contributed to the differing country-specific responses (3). Moreover, the effectiveness of these interventions is significantly influenced by the implementation setting and fidelity. Elements such as school leadership, policies, workforce structure, program characteristics, and the overall school environment play critical roles in shaping outcomes (54). High fidelity and quality implementation, along with positive adaptations, have been shown to enhance intervention impact. For instance, schools that implemented interventions with high fidelity and quality demonstrated more favorable results (55). As prior cross-cultural research suggests, disparities in how children engage in organized PA (due to school systems or community sports) can influence fitness outcomes (36). Our results reinforce that notion, implying that culturally and contextually tailored approaches might be necessary to maximize the effectiveness of school-based fitness programs in each setting.
Importantly, the intervention’s effect on anthropometric measures was minimal. Weight and height increased with growth, but stable BMI indicates healthy, proportionate development. In other words, improved fitness did not come at the cost of unhealthy weight changes. This outcome is encouraging, as it suggests that participants’ weight gain was likely attributable to normal growth and possibly increased muscle mass rather than excess fat. Maintaining a stable BMI while improving fitness levels is a positive indicator that the program supported healthy development. It also aligns with the understanding that short-term interventions in children often do not drastically change BMI, especially when concurrent growth in stature is occurring. Our findings here mirror those of the Egyptian pilot study, which found no significant change in BMI alongside improvements in certain fitness components, underscoring that fitness gains can be achieved without immediate changes in body composition (29). This observation is consistent with prior research showing that while PA interventions can significantly enhance aerobic and anaerobic fitness, they often do not result in substantial changes in anthropometric indicators, particularly over shorter durations (56). This has important public health implications: a well-designed physical activity program can enhance functional fitness and health markers in children even if weight metrics remain constant in the short term.
4.2 Comparison with previous studies
The outcomes of our study align with previous research on school-based PA interventions and extend the literature by incorporating a multi-country, cross-cultural perspective. Numerous studies have shown that increased PA in school settings leads to improvements in children’s aerobic and muscular fitness (29–32). For example, interventions that increased the frequency of physical education classes reported significant gains in aerobic capacity and muscular strength (34). Our findings corroborate these results, with observed improvements in endurance (6-min run) and strength-based measures (standing long jump and push-ups) across many groups. That these gains were achieved through a relatively short-term program highlights children’s responsiveness to increased PA, consistent with findings from the Fit-4-Fun trial and similar school-based interventions (57). Furthermore, the intervention’s effectiveness across diverse populations supports the broader applicability of structured programs and reinforces calls for their wider implementation.
Beyond general intervention effects, our study contributes novel insights into how cultural and environmental factors might modulate outcomes. Prior work by Aly et al. (36) documented significant baseline differences in fitness levels among children from Egypt, Italy, Lebanon, Portugal, and Spain, attributing these disparities to variations in PA opportunities and lifestyles across countries (36). The current intervention study builds on those findings by showing that when a standardized PA program is applied, the relative improvements are inversely related to some of those baseline rankings. This suggests that children from countries with lower initial fitness (potentially due to fewer routine PA opportunities) can “catch up” to some degree when given equal access to structured exercise. For instance, Lebanese children—who had certain fitness disadvantages at baseline relative to peers from Spain—achieved among the highest gains in measures like sprint speed and muscular endurance during the intervention. Conversely, Spanish children, who on average started with superior performance in several tests, showed smaller proportional improvements. This inverse relationship between baseline fitness and improvement magnitude has been observed in other contexts and likely reflects a regression to the mean or greater room for improvement among initially less-fit groups (58). It also emphasizes the value of providing quality PA programs in regions where children’s habitual fitness may be lagging; these children stand to benefit substantially from interventions.
Our age-related findings are consistent with, and build upon, previous research showing that older children and adolescents typically experience greater gains in strength and aerobic capacity than prepubertal children, largely due to hormonal and developmental differences (59). The pronounced improvements in the early adolescence group—particularly in strength-oriented tests like push-ups and sit-ups in countries such as Lebanon and Portugal—support this trend. In contrast, the more modest gains among 8–10 year-olds mirror findings from short-term interventions where younger children demonstrate improvements, though less pronounced (48, 49). Nonetheless, the younger cohort in our study did achieve meaningful gains, especially in coordination and endurance, across several countries. This suggests that with well-designed programs, prepubescent children can still benefit from PA, albeit to a lesser extent. These insights are valuable for educators and practitioners, highlighting the potential of tailored, higher-intensity or play-based interventions to better engage younger children, as recommended by pediatric exercise guidelines.
In comparing specific fitness components, our multi-country results partly contrast with the single-country pilot study conducted in Egypt under the DELICIOUS project. That 6-week pilot intervention reported significant improvements primarily in coordination (jumping sideways) and lower-body power (standing long jump), with no significant changes in sprint speed, upper-body strength, or abdominal strength observed (29). In the present study, which spanned a longer duration and included a larger, more diverse sample, we observed significant improvements in nearly all those fitness domains (including sprint speed and muscle strength/endurance) in at least some subgroups, particularly among older children. This difference suggests that a longer or more comprehensive program can elicit broader fitness enhancements than a brief pilot, and that factors such as participant age and baseline fitness play a critical role in determining which fitness components improve. It’s worth noting that aerobic endurance improved markedly in our study across all countries (with 6-min run performance increasing ~24%–40% depending on group), whereas the pilot showed only marginal gains in endurance (perhaps due to its shorter timeframe). Thus, our findings provide stronger evidence that the “Be Fit” style school-based program can improve cardiovascular fitness when implemented at scale, while also confirming the pilot study’s implication that certain capacities (speed, strength) may require more time or intensity to change significantly. Overall, the consistency of our core outcomes with existing literature lends credibility to the effectiveness of school-based interventions, and the discrepancies (such as those with the pilot study) offer learning opportunities on how to optimize these programs.
4.3 Limitations and future directions
While this study offers valuable insights, several limitations must be acknowledged to ensure accurate interpretation of the findings. First, the absence of a control group in our design limits the ability to attribute improvements solely to the intervention, since natural growth and maturation over the study period could also enhance fitness measures. To address this limitation, we focused on age-specific changes within the broader context of cross-country comparisons. Notably, early adolescents—those approaching or undergoing puberty—demonstrated disproportionately greater improvements than younger peers, with the magnitude of change varying by country. This pattern cannot be fully attributed to natural growth alone, suggesting potential effects of both the training intervention and cultural context. While these findings provide meaningful insight, a future controlled trial would be necessary to establish stronger causal inferences. Second, there were inherent differences in sample characteristics between countries (e.g., baseline fitness levels, cultural attitudes toward PA, and perhaps slight variations in program implementation) that could have influenced the outcomes. We treated the intervention as a uniform exposure, but adherence and enthusiasm might have varied by site, introducing some bias. Although we believe that analyzing percentage change helps minimize the impact of baseline heterogeneity, future studies should assess program fidelity and possibly adjust for baseline fitness or use each country as its own control to better understand these context effects. Third, biological maturation (e.g., proximity to peak growth velocity) was not assessed. Future interventions should consider including maturity status estimations to better interpret changes in physical fitness and anthropometric outcomes across different developmental stages. A further limitation is that the intervention may have been insufficient for some fitness components, especially among younger children, to show full adaptation. Longer interventions or follow-up assessments would help determine whether gains are sustained or continue to increase. We also did not examine sex-based differences, which is a limitation given the developmental differences between boys and girls in this age group. Future work should explore gender-specific responses to the intervention in diverse culture contexts. Importantly, while this study focused on PA, other influential factors—such as nutrition and adherence to the Mediterranean diet (a focus of the broader DELICIOUS project)—were not analyzed. These factors likely interact with physical fitness outcomes and should be considered in future research. Finally, these findings highlight the need for supportive environments that enable children and adolescents to engage in regular PA. Beyond school-based interventions, broader policy initiatives are essential to promote sustainable PA habits. Policymakers should consider integrating PA into national education agendas, ensuring supportive school infrastructure, and prioritizing active lifestyles in youth development strategies. Creating such environmental and policy conditions is critical to addressing the inactivity crisis and promoting long-term public health. Another important consideration involves data privacy and ethical data sharing practices. Given the sensitive nature of collecting fitness and health data from children across culturally diverse settings, future research should incorporate rigorous safeguards for participant confidentiality. Recent methodological advancements, such as those described by Zhang et al. (60) offer useful frameworks for balancing open science practices with ethical data stewardship. Adopting such frameworks is essential to ensure that cross-national studies involving minors remain compliant with evolving standards of transparency and privacy protection.
Despite these limitations, the study’s strengths include its large, diverse sample and the cross-cultural comparative approach, which is uncommon in school-based fitness intervention research. By encompassing five countries, we could discern patterns that a single-country study might overlook, thereby providing a more holistic understanding of how context interacts with a PA program’s effectiveness.
5 Implications and conclusions
In summary, this study provides robust evidence that a structured, school-based PA program can significantly enhance children’s fitness across different domains (speed, strength, endurance, and coordination) in a variety of Mediterranean settings. The improvements observed, particularly among early adolescents, have meaningful implications for public health and education—healthier fitness profiles in youth are associated with numerous immediate and long-term benefits, including better cardiovascular health, muscular development, and even academic performance (1, 3, 7, 61–63). Our cross-country findings emphasize that while the foundational benefits of exercise are universal, programs may need to be tailored to account for age and cultural context to maximize their impact. Schools in regions where baseline fitness is low might expect especially large benefits from implementing such interventions, whereas those in settings with more active youth might focus on maintaining engagement and reaching the less-fit subgroup of students. The fact that BMI remained stable suggests that fitness improvements were achieved alongside healthy growth, without adverse changes in body composition.
Going forward, educators and policymakers should consider integrating regular PA sessions into school curricula as a strategy to improve youth fitness and combat sedentary lifestyle trends. Our results support recommendations for culturally adapted physical education strategies (36)—for instance, incorporating traditional games or locally favored activities to increase participation—and for paying special attention to motivating younger children who may not respond as readily. Furthermore, establishing international collaborations (like the DELICIOUS project) can facilitate knowledge exchange on effective practices and help develop guidelines that recognize both universal principles of child fitness and local needs. Ultimately, our findings affirm that investing in school-based PA programs is a viable and effective approach to enhance physical fitness among children, and they highlight the importance of refining these programs to ensure that all children, regardless of age or country, can achieve optimal benefits.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics committee of Mondragon University (no. IEB-20230704). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
MA: Funding acquisition, Investigation, Resources, Supervision, Writing – original draft, Writing – review & editing. AA: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. KT: Conceptualization, Data curation, Formal analysis, Validation, Visualization, Writing – review & editing. LM: Conceptualization, Data curation, Formal analysis, Validation, Visualization, Writing – review & editing. NE-G: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing. AS: Conceptualization, Methodology, Supervision, Writing – review & editing. OA: Writing – review & editing, Writing – original draft, Validation, Supervision, Resources, Project administration, Investigation, Funding acquisition, Data curation, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The DELICIOUS project is funded by the PRIMA program supported by the European Union [grant agreement no. 2131].
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Aly, M, and Kojima, H. Relationship of regular physical activity with neuroelectric indices of interference processing in young adults. Psychophysiology. (2020) 57:13674. doi: 10.1111/psyp.13674
2. Khan, NA, and Hillman, CH. The relation of childhood physical activity and aerobic fitness to brain function and cognition: a review. Pediatr Exerc Sci. (2014) 26:138–46. doi: 10.1123/pes.2013-0125
3. Aly, M, Ishihara, T, Torii, S, and Kamijo, K. Being underweight, academic performance and cognitive control in undergraduate women. Arch Womens Ment Health. (2024) 27:249–58. doi: 10.1007/s00737-023-01410-4
4. Aly, M, Sakamoto, M, and Kamijo, K. Grip strength, working memory, and emotion perception in middle-aged males. Prog. Brain Res. (2024) 286:89–105. doi: 10.1016/bs.pbr.2023.12.004
5. Hillman, CH, Erickson, KI, and Kramer, AF. Be smart, exercise your heart: exercise effects on brain and cognition. Nat Rev Neurosci. (2008) 9:58–65. doi: 10.1038/nrn2298
6. Ammar, A, Trabelsi, K, Hermassi, S, Kolahi, A-A, Mansournia, M, Jahrami, H, et al. Global disease burden attributed to low physical activity in 204 countries and territories from 1990 to 2019: insights from the global burden of disease 2019 study. Biol Sport. (2023) 40:835–55. doi: 10.1016/S1474-4422(24)00369-7
7. Aly, M, Hassan, MD, Hassan, MM, Alibrahim, M, and Kamijo, K. Association of aerobic fitness and grip strength with cognitive and academic performance in Arab children. Prog Brain Res. (2024) 286:107–28. doi: 10.1016/bs.pbr.2023.11.005
8. Bull, FC, and Bauman, AE. Physical inactivity: the “Cinderella” risk factor for noncommunicable disease prevention. J Health Commun. (2011) 16:13–26. doi: 10.1080/10810730.2011.601226
9. Bull, FC, Al-Ansari, SS, Biddle, S, Borodulin, K, Buman, MP, Cardon, G, et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
10. Dollman, J, and Olds, TS. Pediatric fitness: secular trends and geographic variability. J Sports Sci Med. (2007) 50:210–25. doi: 10.1159/isbn.978-3-318-01396-2
11. Fühner, T, Kliegl, R, Arntz, F, Kriemler, S, and Granacher, U. An update on secular trends in physical fitness of children and adolescents from 1972 to 2015: a systematic review. Sports Med. (2021) 51:303–20. doi: 10.1007/s40279-020-01373-x
12. Lovecchio, N, Vandoni, M, Codella, R, Rovida, A, Carnevale Pellino, V, Giuriato, M, et al. Trends in means and distributional characteristics of cardiorespiratory endurance performance for Italian children (1984–2010). J Sports Sci. (2022) 40:2484–90. doi: 10.1080/02640414.2023.2165007
13. Aly, M, AlMarzooqi, M, Mohamed, S, Alzahrani, TM, and Abdelkarim, O. Daily step counts before, during, and after COVID-19 pandemic: a smartphone-tracking study of university students in Egypt and Saudi Arabia. BMC Public Health. (2023) 23:1365. doi: 10.1186/s12889-023-16068-x
14. Ammar, A, Brach, M, Trabelsi, K, Chtourou, H, Boukhris, O, Masmoudi, L, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey. Nutrients. (2020) 12:1583. doi: 10.3390/nu12061583
15. Ammar, A, Trabelsi, K, Brach, M, Chtourou, H, Boukhris, O, Masmoudi, L, et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: insight from the ECLB-COVID19 multicenter study. Biol Sport. (2021) 38:9–21. doi: 10.5114/biolsport.2020.96857
16. Ruiz, JR, Castro-Piñero, J, Artero, EG, Ortega, FB, Sjöström, M, Suni, J, et al. Predictive validity of health-related fitness in youth: a systematic review. Br J Sports Med. (2009) 43:909–23. doi: 10.1136/bjsm.2008.056499
17. Ortega, FB, Ruiz, JR, Castillo, MJ, and Sjöström, M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes. (2008) 32:1–11. doi: 10.1038/sj.ijo.0803774
18. Fort-Vanmeerhaeghe, A, Romero-Rodriguez, D, Lloyd, RS, Kushner, A, and Myer, GD. Integrative neuromuscular training in youth athletes. Part II: strategies to prevent injuries and improve performance. Strength Cond J. (2016) 38:9–27. doi: 10.1519/SSC.0000000000000234
19. Ito, T, Sugiura, H, Ito, Y, Noritake, K, and Ochi, N. Relationship between the skeletal muscle mass index and physical activity of Japanese children: a cross-sectional, observational study. PLoS One. (2021) 16:e0251025. doi: 10.1371/journal.pone.0251025
20. Raghuveer, G, Hartz, J, Lubans, DR, Takken, T, Wiltz, JL, Mietus-Snyder, M, et al. Cardiorespiratory fitness in youth: an important marker of health: a scientific statement from the American Heart Association. Circulation. (2020) 142:e101–18. doi: 10.1161/CIR.0000000000000866
21. Catalano, RF, and Kellogg, E. Fostering healthy mental, emotional, and behavioral development in children and youth: a national agenda. J Adolesc Health. (2020) 66:265–7. doi: 10.1016/j.jadohealth.2019.12.003
22. Fernandes, RA, and Zanesco, A. Early physical activity promotes lower prevalence of chronic diseases in adulthood. Hypertens Res. (2010) 33:926–31. doi: 10.1038/hr.2010.106
23. Bianco, A, Mammina, C, Jemni, M, Filippi, AR, Patti, A, Thomas, E, et al. A fitness index model for Italian adolescents living in southern Italy: the ASSO project. J Sports Med Phys Fitness. (2015) 56:1279–88.
24. Musaiger, AO. Overweight and obesity in eastern mediterranean region: prevalence and possible causes. J Obes. (2011) 2011:407237. doi: 10.1155/2011/407237
25. Roditis, ML, Parlapani, ES, Tzotzas, T, Hassapidou, M, and Krassas, GE. Epidemiology and predisposing factors of obesity in Greece: from the second world war until today. J Pediatr Endocrinol Metab. (2009) 22:389–405. doi: 10.1515/jpem.2009.22.5.389
26. Sanmarchi, F, Esposito, F, Marini, S, Masini, A, Scrimaglia, S, Capodici, A, et al. Children’s and families’ determinants of health-related behaviors in an Italian primary school sample: the “seven days for my health” project. Int J Environ Res Public Health. (2022) 19:460. doi: 10.3390/ijerph19010460
27. Seral-Cortes, M, Sabroso-Lasa, S, Bailo-Aysa, A, Gonzalez-Gross, M, Molnar, D, Censi, L, et al. Mediterranean diet, screen-time-based sedentary behavior and their interaction effect on adiposity in European adolescents: the HELENA study. Nutrients. (2021) 13:474. doi: 10.3390/nu13020474
28. World Health Organization. Childhood obesity in European region remains high: new WHO report presents latest country data. Preuzeto, 26, 2023. (2022). Available online at: https://www.who.int/europe/news-room/08-11-2022-childhood-obesity-in-european-region-remains-high--new-who-report-presents-latest-country-data#:~:text=In%20the%20new%20COSI%20Round,Marino%20and%20girls%20in%20Malta (Accessed Janurary 6, 2025).
29. Abdelkarim, O, El-Gyar, N, Shalaby, AM, and Aly, M. The effects of a school-based physical activity program on physical fitness in Egyptian children: a pilot study from the DELICIOUS project. Children. (2024) 11:842. doi: 10.3390/children11070842
30. Kolle, E, Solberg, RB, Säfvenbom, R, Dyrstad, SM, Berntsen, S, Resaland, GK, et al. The effect of a school-based intervention on physical activity, cardiorespiratory fitness and muscle strength: the School in Motion cluster randomized trial. Int J Behav Nutr Phys Act. (2020) 17:154–64. doi: 10.1186/s12966-020-01060-0
31. Kriemler, S, Zahner, L, Schindler, C, Meyer, U, Hartmann, T, Hebestreit, H, et al. Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: cluster randomised controlled trial. BMJ. (2010) 340:c785. doi: 10.1136/bmj.c785
32. Meyer, U, Schindler, C, Zahner, L, Ernst, D, Hebestreit, H, van Mechelen, W, et al. Long-term effect of a school-based physical activity program (KISS) on fitness and adiposity in children: a cluster-randomized controlled trial. PLoS One. (2014) 9:e87929. doi: 10.1371/journal.pone.0087929
33. García-Hermoso, A, Alonso-Martínez, AM, Ramírez-Vélez, R, Pérez-Sousa, MÁ, Ramírez-Campillo, R, and Izquierdo, M. Association of physical education with improvement of health-related physical fitness outcomes and fundamental motor skills among youths: a systematic review and meta-analysis. JAMA Pediatr. (2020) 174:e200223–3. doi: 10.1001/jamapediatrics.2020.0223
34. Ardoy, DN, Fernandez-Rodriguez, JM, Ruiz, JR, Chillon, P, Espana-Romero, V, Castillo, MJ, et al. Improving physical fitness in adolescents through a school-based intervention: the EDUFIT study. Rev Esp Cardiol. (2011) 64:484–91. doi: 10.1016/j.recesp.2011.01.009
35. Gallotta, MC, Emerenziani, GP, Iazzoni, S, Iasevoli, L, Guidetti, L, and Baldari, C. Effects of different physical education programmes on children’s skill-and health-related outcomes: a pilot randomised controlled trial. J Sports Sci. (2017) 35:1547–55. doi: 10.1080/02640414.2016.1225969
36. Aly, M, El-Gyar, N, Shalaby, AM, and Abdelkarim, O. Health-related physical fitness in children among five Mediterranean countries: a cross-cultural study from the DELICIOUS project. Front Public Health. (2025) 12:1520096. doi: 10.3389/fpubh.2024.1520096
37. Rio, CJ, and Saligan, LN. Understanding physical activity from a cultural-contextual lens. Front Public Health. (2023) 11:1223919. doi: 10.3389/fpubh.2023.1223919
38. Grosso, G, Buso, P, Mata, A, Abdelkarim, O, Aly, M, Pinilla, J, et al. Understanding consumer food choices & promotion of healthy and sustainable Mediterranean diet and lifestyle in children and adolescents through behavioural change actions: the DELICIOUS project. Int J Food Sci Nutr. (2024) 75:527–35. doi: 10.1080/09637486.2024.2353065
39. Rosi, A, Scazzina, F, Giampieri, F, Abdelkarim, O, Aly, M, Pons, J, et al. Adherence to the mediterranean diet in 5 mediterranean countries: a descriptive analysis of the DELICIOUS project. Mediterr J Nutr Metab. (2024) 17:323–34. doi: 10.1177/1973798X24129644
40. Rosi, A, Scazzina, F, Giampieri, F, Álvarez-Córdova, L, Abdelkarim, O, Ammar, A, et al. Lifestyle factors associated with children’s and adolescents’ adherence to the mediterranean diet living in mediterranean countries: the DELICIOUS project. Nutrients. (2024) 17:26. doi: 10.3390/nu17010026
41. Whooten, RC, Perkins, ME, Gerber, MW, and Taveras, EM. Effects of before-school physical activity on obesity prevention and wellness. Am J Prev Med. (2018) 54:510–8. doi: 10.1016/j.amepre.2018.01.017
42. Abdelkarim, O, Aly, M, ElGyar, N, Shalaby, AM, Kamijo, K, Woll, A, et al. Association between aerobic fitness and attentional functions in Egyptian preadolescent children. Front Psychol. (2023) 14:1172423. doi: 10.3389/fpsyg.2023.1172423
43. Abdelkarim, O, Fritsch, J, Jekauc, D, and Bös, K. Examination of construct validity and criterion-related validity of the German motor test in Egyptian schoolchildren. Int J Environ Res Public Health. (2021) 18:8341. doi: 10.3390/ijerph18168341
44. Bös, K., Schlenker, L, Eberhardt, T, Abdelkarim, O, and Mechling, H. (2021). International physical performance test profile 6-18 (revised). Feldhaus Edition Czwalina: Hamburg.
45. Eberhardt, T, Bös, K, and Niessner, C. Changes in physical fitness during the COVID-19 pandemic in German children. Int J Environ Res Public Health. (2022) 19:9504. doi: 10.3390/ijerph19159504
46. Bös, K., and Mechling, H. (1983). Dimensionen sportmotorischer leistungen. Schorndorf: Hofmann. 335.
47. Bös, K, Schlenker, L, Büsch, D, Lämmle, L, Müller, H, Oberger, J, et al. Deutscher Motorik-Test 6-18 (DMT 6-18). Hamburg: Feldhaus (2009).
48. Matos, N, and Winsley, RJ. Trainability of young athletes and overtraining. J Sports Sci Med. (2007) 6:353–67.
49. McNarry, MA, Welsman, JR, and Jones, AM. Influence of training and maturity status on the cardiopulmonary responses to ramp incremental cycle and upper body exercise in girls. J Appl Physiol. (2011) 110:375–81. doi: 10.1152/japplphysiol.00988.2010
50. Zehr, EP, and Sale, DG. Ballistic movement: muscle activation and neuromuscular adaptation. Can J Appl Physiol. (1994) 19:363–78. doi: 10.1139/h94-030
51. Hellsten, Y, and Nyberg, M. Cardiovascular adaptations to exercise training. Compr Physiol. (2016) 6:1–32. doi: 10.1002/j.2040-4603.2016.tb00672.x
52. Nielsen, J, Gejl, KD, Hey-Mogensen, M, Holmberg, HC, Suetta, C, Krustrup, P, et al. Plasticity in mitochondrial cristae density allows metabolic capacity modulation in human skeletal muscle. J Physiol. (2017) 595:2839–47. doi: 10.1113/JP273040
53. Weatherwax, RM, Harris, NK, Kilding, AE, and Dalleck, LC. The incidence of training responsiveness to cardiorespiratory fitness and cardiometabolic measurements following individualized and standardized exercise prescription: study protocol for a randomized controlled trial. Trials. (2016) 17:601–12. doi: 10.1186/s13063-016-1735-0
54. Defever, E, and Jones, M. Rapid realist review of school-based physical activity interventions in 7-to 11-year-old children. Children. (2021) 8:52. doi: 10.3390/children8010052
55. Åvitsland, A, Ohna, SE, Dyrstad, SM, Tjomsland, HE, Lerum, Ø, and Leibinger, E. The process evaluation of a school-based physical activity intervention: influencing factors and potential consequences of implementation. Health Educ. (2020) 120:121–39. doi: 10.1108/HE-01-2020-0004
56. Thivel, D, Isacco, L, Lazaar, N, Aucouturier, J, Ratel, S, Doré, E, et al. Effect of a 6-month school-based physical activity program on body composition and physical fitness in lean and obese schoolchildren. Eur J Pediatr. (2011) 170:1435–43. doi: 10.1007/s00431-011-1466-x
57. Eather, N, Morgan, PJ, and Lubans, DR. Improving the fitness and physical activity levels of primary school children: results of the Fit-4-fun group randomized controlled trial. Prev Med. (2013) 56:12–9. doi: 10.1016/j.ypmed.2012.10.019
58. Pihlainen, K, Vaara, J, Ojanen, T, Santtila, M, Vasankari, T, Tokola, K, et al. Effects of baseline fitness and BMI levels on changes in physical fitness during military service. J Sci Med Sport. (2020) 23:841–5. doi: 10.1016/j.jsams.2020.02.006
59. Baquet, G, Guinhouya, C, Dupont, G, Nourry, C, and Berthoin, S. Effects of a short-term interval training program on physical fitness in prepubertal children. J Strength Cond Res. (2004) 18:708–13. doi: 10.1519/13813.1
60. Zhang, Y, Fan, S, Hui, H, Zhang, N, Li, J, Liao, L, et al. Privacy protection for open sharing of psychiatric and behavioral research data: ethical considerations and recommendations. Alpha Psychiatr. (2025) 26:38759. doi: 10.31083/AP38759
61. Aly, M, and Kojima, H. Acute moderate-intensity exercise generally enhances neural resources related to perceptual and cognitive processes: a randomized controlled ERP study. Ment Health Phys Act. (2020) 19:100363. doi: 10.1016/j.mhpa.2020.100363
62. Hillman, CH, Pontifex, MB, Raine, LB, Castelli, DM, Hall, EE, and Kramer, AF. The effect of acute treadmill walking on cognitive control and academic achievement in preadolescent children. Neuroscience. (2009) 159:1044–54. doi: 10.1016/j.neuroscience.2009.01.057
Keywords: physical fitness, exercise intervention, Mediterranean region, cross-cultural study, youth health promotion, early adolescents, children, anthropometrics
Citation: Aly M, Ammar A, Trabelsi K, Masmoudi L, El-Gyar N, Shalaby AM and Abdelkarim O (2025) School-based physical activity and health-related fitness in Mediterranean students: findings from the DELICIOUS project. Front. Public Health. 13:1603043. doi: 10.3389/fpubh.2025.1603043
Edited by:
Yibo Wu, Peking University, ChinaReviewed by:
Antonino Patti, University of Palermo, ItalyEui Jae Lee, Seowon University, Republic of Korea
Saima Kuu, Tallinn University, Estonia
Salvi Shah, SPB Physiotherapy College, India
Tiago Moreira, Polytechnic Institute of Maia, Portugal
Copyright © 2025 Aly, Ammar, Trabelsi, Masmoudi, El-Gyar, Shalaby and Abdelkarim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohamed Aly, bW9oYW1lZC5hbHlAYXVuLmVkdS5lZw==
†These authors have contributed equally to this work