 Regula Limacher
Regula Limacher Abderrazak Hajjioui
Abderrazak Hajjioui Maryam Fourtassi5
Maryam Fourtassi5 Christine Fekete
Christine Fekete- 1Swiss Paraplegic Research, Guido A. Zäch Institute, Nottwil, Switzerland
- 2Department of Health Sciences and Medicine, University of Lucerne, Lucerne, Switzerland
- 3Clinical Neuroscience Laboratory, Faculty of Medicine and Pharmacy, Sidi Mohamed Ben Abdallah University, Fez, Morocco
- 4Department of Physical and Rehabilitation Medicine, Hassan II University Hospital, Fez, Morocco
- 5Laboratory of Life and Health Sciences, Faculty of Medicine and Pharmacy of Tangier, Abdelmalek Essaadi University, Tangier, Morocco
- 6Work Mastery, Corporate Health Consulting, Lucerne, Switzerland
Background: Socioeconomic status (SES) and gender are well-known social determinants of health. However, their impact on health in populations with physical disabilities in low-resource countries is still lacking. Therefore, the objective of this study was to investigate associations of individual SES with health and the moderating effect of gender on this association in a Moroccan population with a physical disability, namely spinal cord injury.
Methods: Cross-sectional survey data from 385 participants with spinal cord injury living in Morocco were analyzed. SES was operationalized by education level, household income, financial hardship, and subjective social status. Health indicators included secondary conditions, pain, vitality, quality of life, and general health. Associations between SES and health indicators were investigated using linear and logistic regressions. To test the potential moderation of gender, interaction terms between SES and gender were introduced in regression models.
Results: Financial hardship and lower subjective social status were associated with poorer health outcomes in four out of five indicators in the total sample. In contrast, education and income were inconsistently associated with health. Overall, gender did not moderate the association between SES and health, except that educational inequalities in general health were more pronounced in women, and the observation of a trend for a stronger negative effect of subjective social status on men's than woman's health (p > 0.05).
Conclusion: This study revealed that subjective indicators of SES negatively impact on health, whereas evidence for the moderating role of gender in this association was weak. These findings underline the importance to reduce social marginalization and poverty in populations with disabilities in low-resource countries to reduce their double burden of living with a disability and encountering social disadvantages through low SES.
Introduction
Inequalities in health among groups with different socioeconomic status (SES) are among the most robust findings in socio-epidemiological research, existing with varying extent in both, within and between countries (1–3). Although economic, social, and health indicators in low-resource countries have improved in recent years, socially determined health inequalities may even have increased (4–6). Indeed, economic growth in Morocco has never been so strong as is has been since the early 2000s (7). However, the country is enduring serious difficulties in linking prosperity and social cohesion (7). Despite the marked reduction of poverty, Morocco has experienced persistent, if not greater, income inequalities and the ratio of the richest 10% to the poorest 10% is extremely high, indicating the presence of large social inequalities (6, 7). With only about two-third of the population being granted health insurance (8), healthcare is for many Moroccan people not affordable. Appropriate research is needed to narrow the health gap between different SES groups (5, 9, 10). Evidence on health inequalities in low-resource countries remains limited to the general population, and little is known about people living with health conditions (11–13). Research among this vulnerable group is often challenging and limited due to the widespread lack of resources and infrastructure for data collection.
The Moroccan spinal cord injury (MorSCI) cohort study collected data on people with spinal cord injury (SCI) in Morocco as part of an international community survey (8). SCI is a chronic health condition of varying degrees of complexity and severity. The traumatic or non-traumatic injury of the spinal cord leads to a complete or partial loss of sensory and motor function below the lesion level, and those affected are often severely physically impaired and suffer from secondary conditions (14, 15). Some studies have already documented social inequalities in the context of SCI in Western countries (11, 13, 16, 17), while evidence for low-resource countries is lacking. In less developed countries, people with disabilities are often marginalized and more likely to experience social exclusion and discrimination (18–21). Stigma and negative stereotypes and attitudes towards socially excluded groups can affect their health and create or even reinforce health inequalities (2, 10). To inform tailored interventions and health policies, it is of interest to investigate social inequalities in health in the context of SCI in Morocco.
In the study of health inequalities, it is of growing importance to go beyond the traditional SES indicators education, income, or occupation and examine how SES affects health in a more proximal way (22). Literature suggests that more subjective parameters, such as financial hardship (11, 23, 24) and subjective social status (SSS) (25–28) are important predictors for health beyond the traditional SES indicators, reflecting one's day-to-day lived experience. This study therefore includes a comprehensive set of SES indicators, including education, household income, financial hardship, and SSS. To gain a comprehensive picture of participants' health, a broad range of health indicators was used in this study. Along with quality of life (QoL) and general health as rather general assessments, emphasis is placed on physical health, which is measured by secondary conditions, pain intensity, and vitality.
Besides the main effect of SES on health, it is likely that gender moderates the association between individual SES and health. A moderating effect is present if the effect of the independent variable on the dependent variable depends on the value of a third variable, the so-called moderator variable (29). In this case, the effect of SES on health may differ depending on one's gender as another determinant of health (30). Gender differences in health outcomes are observed across the lifespan and contribute to inequalities in morbidity and mortality (31, 32). Social, cultural, economic, and biological factors have a more substantial negative effect on women's than on men's health (31, 32). The gender gap in Morocco has been reduced substantially over the past 30 years as the Gender Inequality Index dropped from 0.74 in 1990 to 0.43 in 2021 (the lower the number, the lower gender inequalities; average all countries worldwide in 2021: 0.46) (33). Still, gender disparities in Morocco are observable in different socioeconomic indicators. More specifically, women report lower school enrolment rates, lower literacy rates, lower labor income and a lower share of non-agricultural wage labor, which may lead to poorer overall health (6).
In summary, social inequalities in health in persons with SCI have not been studied in low-resource countries and so far, no research in the context of SCI has ever investigated whether health inequalities were moderated by gender. This original and novel study thus aims at expanding the current understanding on the interplay between SES, gender, and health in persons with disabilities from low-resource countries.
In light of these substantial research gaps, the aims of this study are twofold (see Figure 1):
(1) To investigate the association of SES (education, household income, financial hardship, and SSS) with health (secondary conditions, pain, vitality, QoL, and general health) for the total population and stratified by gender.
(2) To examine the potentially moderating role of gender in the association between SES and health.

Figure 1. Analytical framework for the study.
It is hypothesized that I) lower SES is associated with poorer health outcomes, and II) that social inequalities in health are more pronounced in women than in men.
Materials and methods
Design, setting and sample
Cross-sectional data from 385 participants of the population-based community survey of the MorSCI Cohort Study were analyzed (12). The MorSCI survey is part of the International Spinal Cord Injury (InSCI) Survey, a multi-country survey on people with SCI living in a community (8, 34, 35). Ethics committee approval was obtained prior to recruitment, and informed consent was provided by all participants after being informed of the study objectives (8, 34). The MorSCI sample was recruited from 20 institutions (8 rehabilitation facilities; 6 emergency and general hospitals; 3 patient organizations; 3 governmental agencies) using convenience sampling methods (8). The survey was mainly conducted by telephone or face-to-face interview while very few responded to the questionnaire online (8). The 125-item questionnaire was developed by the InSCI study group and was translated from English to Arabic (8, 34, 35). The MorSCI community survey was conducted between June 2017 and December 2018 (8). Persons with traumatic or non-traumatic SCI over 18 years old were included in the study, while people with congenital etiologies of SCI, neurodegenerative disorders, or Guillain Barré syndrome were excluded (8, 34).
Measures
Socioeconomic status
Education was assessed according to the International Standard Classification of Education as the highest completed level of education, combining general and vocational education (36). The categories post-secondary, short tertiary, bachelor or equivalent, and master or equivalent were combined to higher education as only few people indicated those education levels. Lower secondary and higher secondary education were merged into the category secondary education, thus resulting in four categories: no schooling, primary education, secondary education, and higher education.
Household income was used to assess the participants' income situation. It was measured by the total household income, weighted by the number of adults and children living in the household. The item for household income was based on the Model Disability Survey (Item H1017) (37). The response options were based on the guidelines of the European Social Survey and were categorized into ranges of deciles of current household income in Morocco (38). The criteria of the Organization for Economic Co-operation and Development (OECD) were applied for weighting (1.0 for the first adult; 0.5 for each additional adult over 14 years; 0.3 for children) (39, 40). Household income was classified into distribution-based quartiles for analyses.
Financial hardship was assessed with a 4-point Likert scaled item asking how much a problematic financial situation has influenced participation in society in the last four weeks. Response options included “not applicable”, “no influence”, “made my life a little harder”, and “made my life a lot harder”. The first two categories were combined into one, resulting in the three-categorical variable for the analysis: no financial hardship, some financial hardship, and massive financial hardship.
SSS. The Mac Arthur Scale of Subjective Social Status was used to assess the participants' SSS in society, visualized with a ten-step ladder (41, 42). Participants were asked to place themselves on the ladder representing the social hierarchy relative to other people living in Morocco. Due to a floor effect in the distribution of this variable, a categorical variable representing low (1,2), middle (3–5), and high (>5) SSS was created for analysis.
Health outcomes
Secondary conditions. The Spinal Cord Injury Secondary Condition Scale (SCI-SCS) was used to capture the prevalence and severity of secondary conditions in the last three months (43). The scale was modified by not recording the items on heterotopic bone ossification and diabetes mellitus but adding sleep problems. Since pain was measured as a separate health indicator, two items on pain were omitted. Therefore, the SCI-SCS used in this study included 13 items. The original 4-point Likert scale of the SCI-SCS was modified to a 5-point ordinal scale ranging from 1 (no problem) to 5 (extreme problem) following the Model Disability Survey (37). For analysis, the scale was recoded from 0 (no problem) to 4 (extreme problem), yielding a sum score ranging from 0 to 52, with a higher score indicating higher burden of secondary conditions.
Pain was assessed by asking participants to rate their pain as its worst in the last week on a numerical scale ranging from 0 (no pain) to 10 (pain as bad as you can imagine). The item was derived from the Brief Pain Inventory (44–46) and was used as a continuous variable in analysis.
Vitality was measured using the 4-item vitality index of the 36-item Short Form Health Survey (SF-36) (47). The items included the following questions: “How much of the time during the last 4 weeks did you feel full of life?” “…did you have a lot of energy?” “…did you feel worn out?” “…did you feel tired?”. The response options ranged from “all of the time” to “none of the time” and were coded with a 5-point scale from 1 to 5. Items three and four were recoded to 1, 2, 3.5, 5 and 6, and items one and two reversed to 6, 5, 3.5, 2 and 1 according to the SF-36 Manual and Interpretation Guide (47). The raw scale scores were transformed to a 0–100 scale, with a higher score indicating higher vitality.
Quality of life was assessed with the World Health Organization Quality of Life Assessment-5 (WHOQoL-5) (48). It consists of 5 items and enquires the overall quality of life and satisfaction with health, daily activities, relationships, and living conditions over the last 14 days (48). Each item was rated on a 5-point Likert scale from 0 (very dissatisfied) to 4 (very satisfied) and resulted in a global sum score ranging from 0 to 20, with a higher score indicating better QoL.
General health was assessed by single item “General health” of the 12-item Short Form Health Survey, rating their health in general as “excellent”, “very good”, “good”, “fair” or “poor” (49, 50). General Health was analyzed as a dichotomous variable, whereby “excellent”, “very good” and “good” were categorized as good health, and “fair” and “poor” were captured as poor health.
Control variables
Sociodemographic data (age, gender), lesion characteristics, and mobility status were included as potential confounders in the multivariable analysis, given their impact on health (14, 51). Lesion characteristics considered the injury level (paraplegia vs. tetraplegia), lesion completeness (complete vs. incomplete), time since injury, and etiology (traumatic vs. non-traumatic) (15, 52). Mobility status was included as a categorical variable and included the categories walking independently, manual wheelchair or supervision walking, and total assistance or electric wheelchair.
Statistical analysis
Statistical analysis was conducted using Stata version 16.0 for Mac (College Station, TX, USA). The distribution of all SES indicators, health outcomes, and control variables was described. The analysis was conducted for the total sample and stratified by gender. The data set is comprehensive, with only one missing data point reported for the variable vitality. To examine gender differences in SES and health variables, chi-square tests were conducted for categorical and binary variables and t-tests for continuous variables.
To investigate associations between SES and health, linear regressions were used for continuous outcomes secondary conditions, pain, vitality and QoL and logistic regression was used for the binary outcome general health. Two sets of regression models were calculated. First, health outcomes were separately regressed on each SES variable in an unadjusted model (Model 1; 5 models per outcome). Then, models were adjusted for all control variables and all SES indicators (Model 2; 1 model per outcome). The two models were performed for the total sample and stratified by gender. Coefficients and odds ratios (ORs), together with the 95% confidence intervals (CI), are reported for continuous and binary outcomes, respectively. Likelihood ratio tests were used to calculate the p-value for associations under investigation. Sensitivity analysis with a third model adjusted for all SES indicators was performed.
To test moderation, we followed the state-of-the-art approach to include an interaction term between the moderator variable (i.e., gender) and the SES indicators into regression models for each health outcome (53, 54). The interaction term was composed of gender and the individual SES indicators in order to test the interaction of these two variables in the association between SES and health (i.e., in respective regression models), with gender as the moderating factor being examined. The models were adjusted for all control variables. P-values were obtained from likelihood ratio tests using the contrast command. P-values of interaction terms <0.05 indicate a significant interaction or moderation of the variable gender. In other words, significant interaction terms indicate, that social inequalities in health differ between males and females.
Results
Sample characteristics and gender differences
Basic characteristics of the total sample and stratified by gender are displayed in Table 1. The majority of the sample was male (72.5%), the mean age was 38.7 years. The mean years since injury were 7.1 years, and most reported a traumatic cause of the SCI. Regarding education, 17.9% have never attended school, 21.3% have completed primary school, 39.2% had secondary education, and 21.6% had higher education. Two-thirds of the participants reported having massive financial hardship. 37.4% classified their social status as low and just over one out of ten considered themselves to be in the upper half of the social hierarchy. With regard to their health, participants reported on average 15.5 points on the secondary conditions scale (range 0–52), 4.2 on the pain intensity scale (range 0–10), 56.8 on the vitality scale (range 0–100) and 10.8 on the QoL scale (range 0–20) Less than one in four reported their general health to be good.

Table 1. Basic characteristics of the MorSCI population.
Significant gender differences were found for age, lesion characteristics, mobility, education, pain, and vitality. Men were younger, more often completely paralyzed and more frequently reported a traumatic cause of SCI. The proportion of participants who could walk was higher for women than for men. The gender difference in education was ambiguous. More women reported no schooling, however, the proportion of women in the highest level of education was higher than for men. Regarding self-reported health, men reported on average almost a 1-point lower pain intensity and 10% higher vitality than women.
Study aim 1: association of socioeconomic status with health
Results for the total sample
Results of bivariate and multivariable analyses of the total sample are presented in Table 2. Perceived financial hardship was associated with all health outcomes, i.e., more secondary conditions, increased pain intensity, reduced vitality, lower QoL, and higher odds for poor general health in model 1. Results were approved in model 2 (except for general health, p > 0.05). Association with SSS were significant for four out of five health outcomes (secondary conditions, vitality, QoL, and general health) in the unadjusted and adjusted model. Education and income were inconsistently associated with health and only three relevant associations were detected, whereby two of them were against the hypothesized direction (higher education—more secondary conditions; higher income—decreased pain intensity; higher income—decreased vitality).
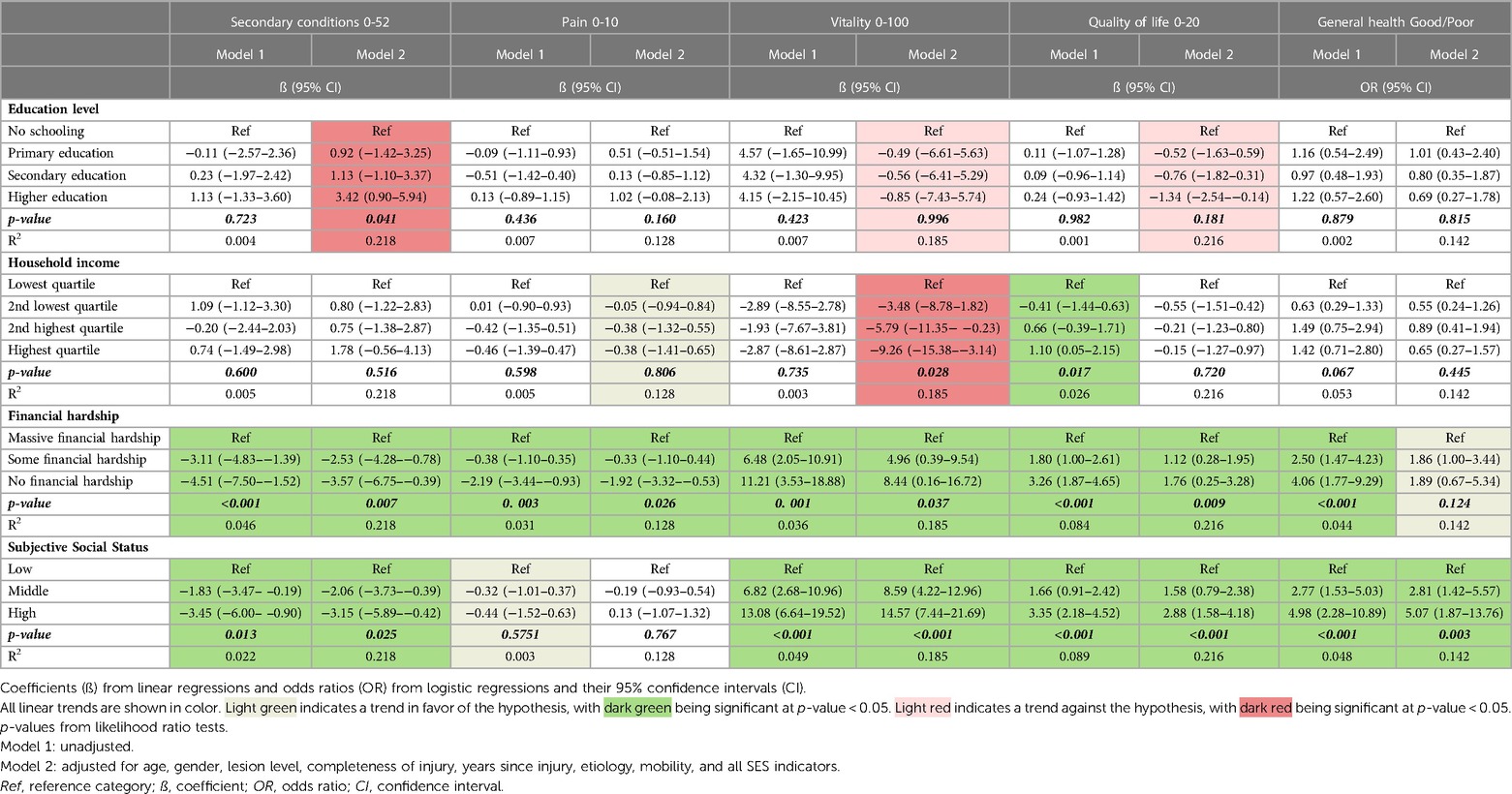
Table 2. Unadjusted and adjusted associations of socioeconomic status with health indicators for the total sample.
Results by gender
The results from the regression analysis for men and women are presented in Tables 3, 4, respectively. For men, financial hardship was associated with worse health in all outcomes under investigation but became insignificant for pain, vitality, and general health in model 2. Lower SSS was significantly associated with worse health in four (model 1) and three (model 2) health outcomes for men. The results for financial hardship and SSS generally showed similar results for women but were less linear and less robust. Only the association of SSS and general health differed from findings for men. Education was not associated with health, except that higher education was associated with higher odds of being in good general health in women (adjusted model). Income was inconsistently associated with health in any indicator, in both, men and women.
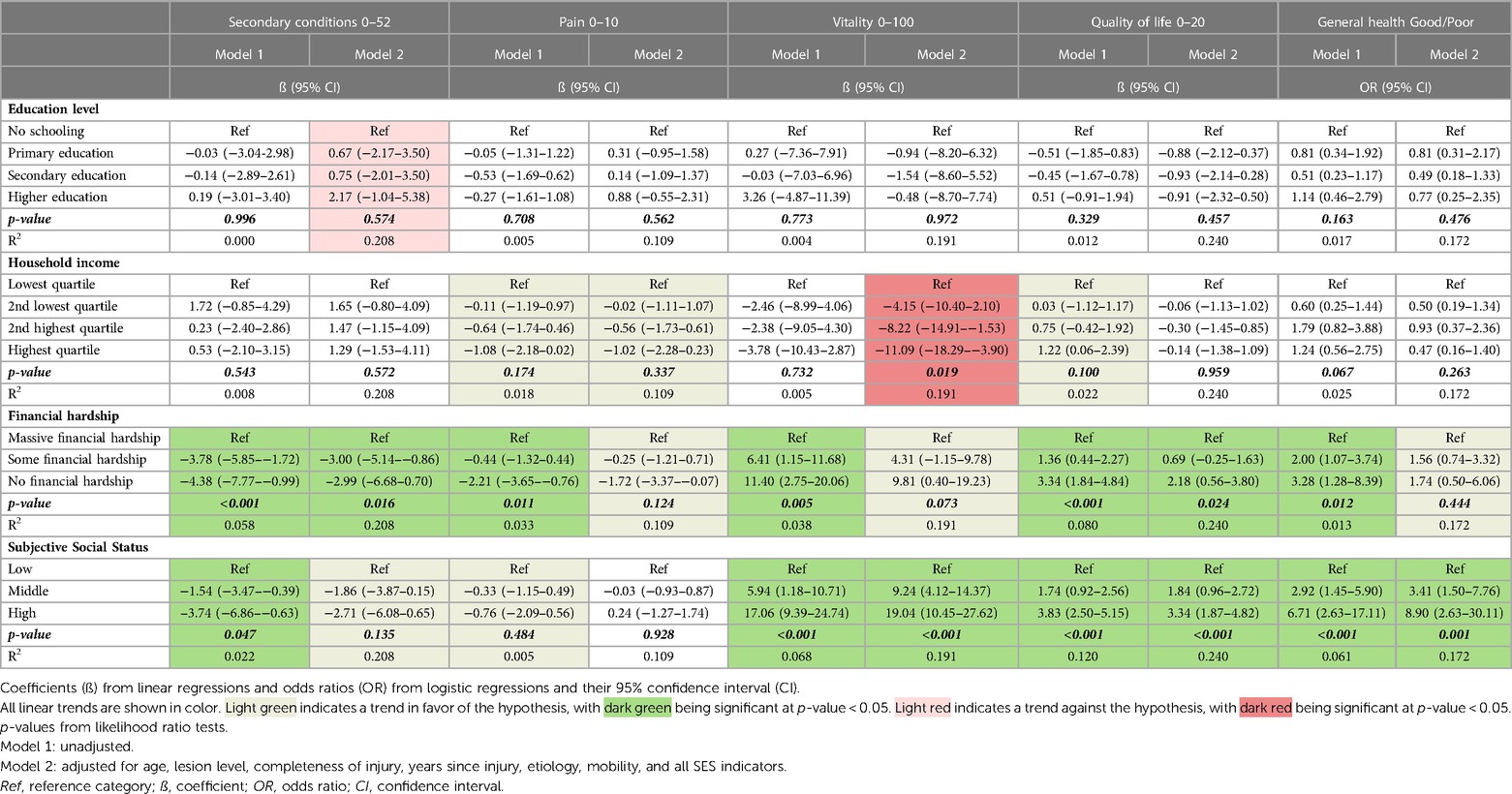
Table 3. Unadjusted and adjusted associations of socioeconomic status with health indicators for men.
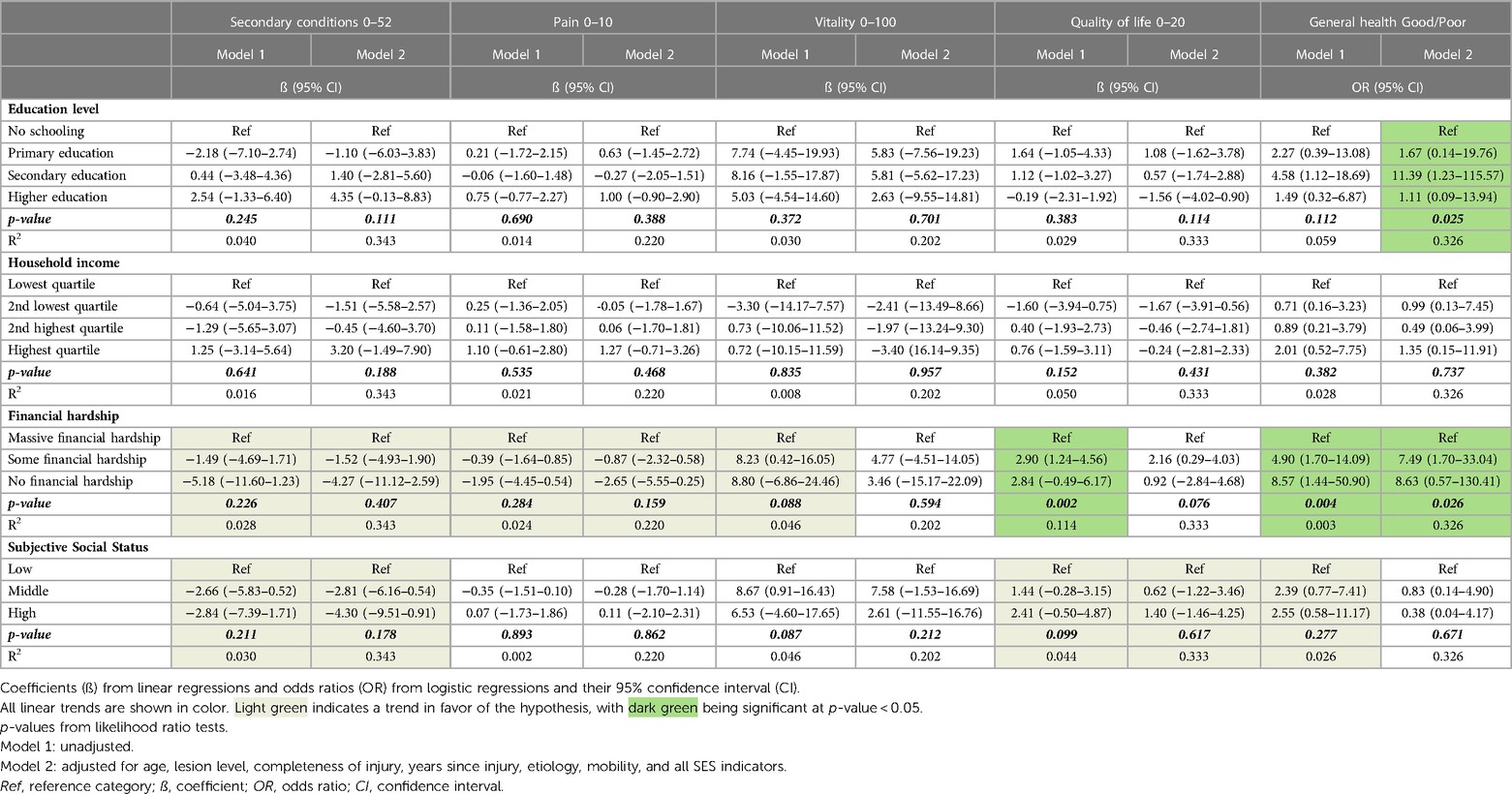
Table 4. Unadjusted and adjusted associations of socioeconomic status with health indicators for women.
Study aim 2: the moderating role of gender in the association between SES and health
The results of the interactions between SES and gender on health are displayed in Table 5. Results generally indicate that gender does not moderate the association between SES and health. However, a trend for moderation was observed for SSS (p > 0.05), as the impact of SSS was more pronounced for men than for women in four out of five health outcomes (secondary condition, pain, QoL, and general health). The interaction of education and gender on general health showed a significant result, indicating that the educational inequalities in women are larger than in men. No moderating effects of gender were found for income and financial hardship.
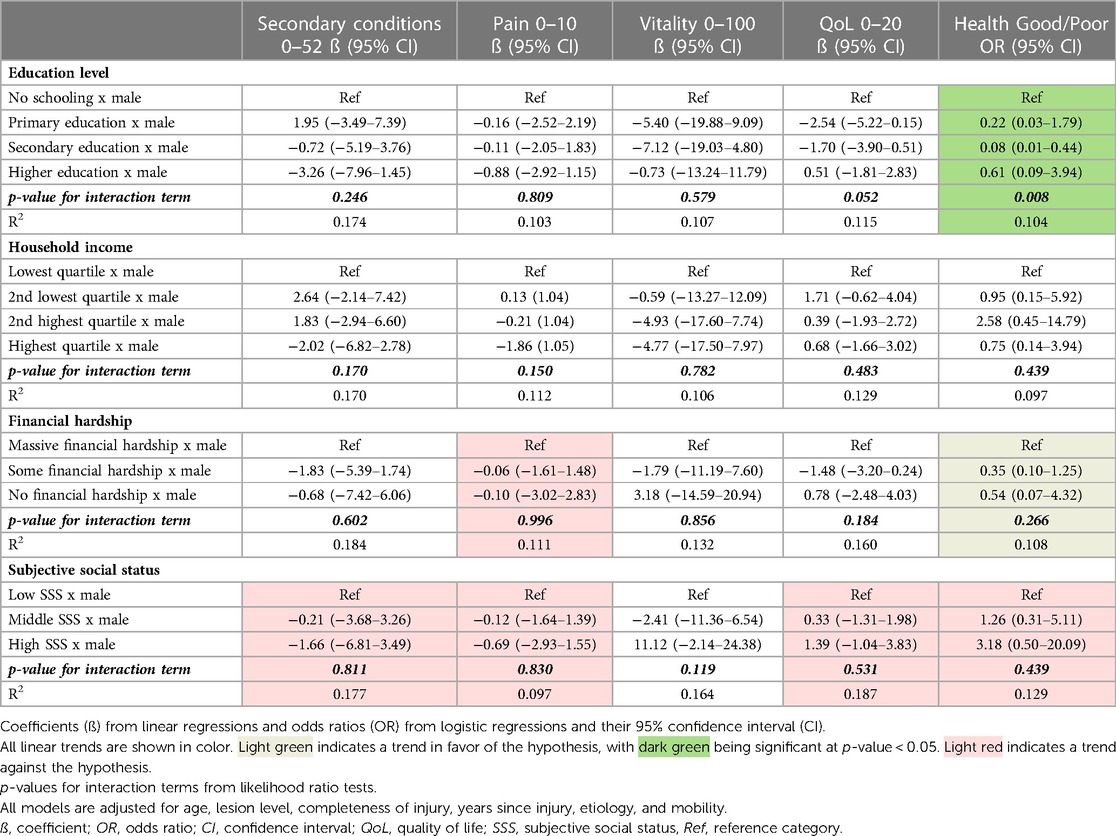
Table 5. Interactions of socioeconomic status and gender on health outcomes.
Discussion
This study of Moroccan men and women living with a disability indicates that subjective indicators of the SES (financial hardship and SSS) are consistently associated with health outcomes, whereas the association of education and income with health was inconsistent. Our hypothesis to find consistent health inequalities for a range of SES indicators was thus only confirmed for the more subjective indicators and less so for the traditional indicators education and income. Overall, the results did not support the moderating hypothesis stating that negative effects of socioeconomic status on health were amplified in women compared to men. Only the results of the interaction of education and gender on general health indicated educational inequalities to be larger in women than in men. A trend for moderation was observed for SSS (p > 0.05), as the impact of SSS on health was more pronounced for men than for women.
SES and health
The inconsistent results of the SES indicators for the association with health raise concerns about which SES indicators are crucial for explaining socioeconomic differences in health among persons with physical disabilities. In health inequalities research, objective measures such as education or income are traditional indicators to describe the relationship between SES and health, but associations with health were not observed in our study. One possible explanation could be that people with SCI are often marginalized due to their disability in low-resource countries such as Morocco and that this social disadvantage is better reflected in the more subjective measures, such as SSS, as it has already been reported for other SCI populations (11, 55). Objective measurements of SES are subsequently not as meaningful in this population. A closer look at the results reveals that the coefficients and ORs of income and education for all health outcomes, except the relationship between income and pain, generally weaken or reverse the assumed relationship after controlling for all confounders and SES indicators. This observation suggests that in the current study, the effects attributed to education or income in a simple model are driven by other factors such as age, lesion characteristics, mobility, and other SES indicators when the model is extended to include these additional variables. Conversely, results for financial hardship and SSS remained relatively robust after adjustment and are in line with previous findings (11, 25, 28).
The sensitivity analysis (see Supplementary Tables) showed that including the SES variables, in addition to all the confounding variables mentioned, had a stronger impact on associations of income and education on health than it was observed for SSS and financial hardship. Financial hardship and SSS have been found to mediate the association of income and education with health in previous studies (11, 28, 56). However, this cannot be explained conclusively in this study. Furthermore, as the study is based on cross-sectional data, it cannot be evaluated whether the subjective measures of SES cause poorer health or result from people's health problems.
There are multiple explanations for the constant associations of SSS and financial hardship with health. SSS might reflect a person's individual SES more comprehensively than more objective measures and therefore shows associations with health even when controlled for other SES measures (27), i.e., SSS has additional explanatory power over standard objective SES indicators like education or income. Additionally, the relative comparison of oneself in society can lead to subjective psychological consequences, negatively affecting physical and mental health (57). Similarly, financial hardship can create a sense of relative deprivation and lead to a heightened stress response, negatively impacting health (58). Financial hardship may further serve as a better indicator of the individual economic burden of people with disabilities due to their increased expenditure on health care and material deprivation such as lack of goods, opportunities, and resources may be adequately addressed (11, 59). Previous findings in high-income countries support the strong impact of financial hardship on the health of people with SCI (11).
Contrary to the hypothesis, education showed a significant positive association with secondary condition after adjustment for all confounders and other SES indicators. The coefficients for income showed a similar trend but were less pronounced and insignificant. Even when counterintuitive, these results can have several explanations. The literature confirms that lower education is associated with later referral among people with chronic health conditions (58), explaining that higher educated individuals are more likely to be diagnosed with secondary conditions. In countries where inequalities in health care services exist in favor of persons with higher SES (5, 6), income and education may play an essential role in detection of secondary conditions, as it reflects a person's access to health services (16). For persons with low SES, this may result in undiagnosed secondary conditions on one hand and untreated health conditions on the other. Comparing different countries showed that people with SCI in low-resource countries are more likely to die from preventable secondary conditions, while secondary conditions are no longer the leading cause of death for people with SCI in high-income countries (52).
Gender differences and moderation
The proportion of women and men among the study participants is representative, as the SCI prevalence is known to have a male-to-female ratio of at least 2:1 among adults (34, 52). The gender differences regarding age and lesion characteristics found in this study align with previous findings (34, 52). Women's ability to move around better and more independently may be attributed to their lower severity of the injury, as incomplete SCI preserves some sensory and motor functions below the lesion level (15). Previous results for the general Moroccan population indicate a gender difference in SES benefiting men (6, 60). The absence of these gender inequalities in SES in the present study population may be related to the general social exclusion of people affected by SCI in this country, equally valid for men and women (19, 20). The gender differences found in our study for pain (higher in females) and vitality (lower in females) are consistent with previous findings from studies conducted among populations with chronic or long-term disabilities (61, 62).
The fact that we did not observe a moderating effect of gender on the relationship between SES and health may be accompanied by methodological limitations when including interaction terms in a quantitative model. When main effects explain a large amount of the variance in an outcome, small but meaningful interactions between two variables can be difficult to detect (63). Nevertheless, a final point that needs to be discussed is the favorable but non-significant result of the moderating effect of SSS and gender on four out of five health outcomes, showing that inequalities in health are more pronounced in males than in females. This could be explained by the fact that lower SSS has an even more detrimental effect on health for men because they cannot fulfil the social norms of the gender role, e.g., by having a lower income and being unable to provide for the family.
Strengths and limitations
This is the first study examining the moderating role of gender on the association between SES and health among physically people with a physical disability and one of the first to examine health inequalities in a low-resource country and therefore contributes to health inequalities research in the setting of disability. A major strength of this study is the comprehensive set of SES indicators and health outcomes, allowing for a detailed analysis of key drivers for health inequalities. Validated measures for most of the constructs under investigation were used and the study population is based on a community sample including people from all country regions. The data meet high-quality standards with virtually no missing data.
This study has several limitations. Although the present study helps to understand the association between SES and health, the cross-sectional nature of data precludes the determination of causality and reverse causation (i.e., that poor health caused poor SES) cannot be excluded. Additionally, health is a complex construct that is determined by various factors. Therefore, other variables not included in the analysis may be important to fully understand the relationship between SES and the selected health indicators (e.g., psychosocial resources). The generalizability of results to the total population of individuals with SCI in Morocco might be limited due to sampling bias as convenience sampling was used. This recruiting strategy includes possible selection bias as the sample was based on 20 collaborating institutions. Also, it is worthwhile mentioning that the absence of statistical significance at the traditional level of p < 0.05 for analysis stratified for gender might be due to low sample size, especially in females. Those results still indicate a consistent trend for inequalities in the subjective SES indicators and absence of statistical significance should be interpreted with caution. It can further not be assessed whether self-report of SES and health indicators has led to biased responses. Information on SES might be prone to social desirability bias and people with lower SES might be reluctant to report themselves as being worse off because of stigmatization. Self-reported data might also result in a bias in health outcomes. People may not be aware of certain health conditions, as disadvantaged people often have poorer health literacy and less access to health services.
Conclusion
In this study on health inequalities in persons with a physical disability (SCI), financial hardship and lower SSS were consistently related to reduced health, whereas income and education were not associated with health. However, evidence for a moderation effect of gender was weak in our sample. Given the importance of subjective measures of SES on health, the results of this study provide evidence that the proximal social context and the lived experience of relative deprivation account most for health inequalities in this setting. These findings underline the importance to reduce social marginalization and poverty in populations with disabilities in low-resource countries to reduce their double burden of being stigmatized due to the disability and encountering social disadvantages through low SES.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by the Hospital and University Ethics Committee of Fez (03/17, approved July 20, 2017). The patients/participants provided their written informed consent to participate in this study.
Author contributions
RL: conceptualized the study, conducted data analysis, interpreted the results, drafted the initial manuscript and finalized the manuscript with contributions from all authors. CF: conceptualized the study, conducted data analysis, interpreted the results, and revised the manuscript. AH and MF: supervised data collection and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
Swiss Paraplegic Research and University of Lucerne, Faculty of Health Sciences and Medicine, funded the publication of this study.
Acknowledgment
We are grateful to all the participants of the MorSCI cohort study for their time and effort spent for responding to the questionnaire. Thank you to the following organizations, which have contributed to carrying out this survey: Ministry of Health and Social Protection (Directorate of Population), Mohammed VI National Centre for the Disabled, Moroccan association for the promotion of rehabilitation sciences and disability prevention and WHO office in Morocco. We also thank the following individuals, who have also contributed to carrying out this research project: Members of the MorSCI research team and collaborating centers, members of the national study group and stakeholders and members of the InSCI Steering Committee.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2023.1108214/full#supplementary-material.
Abbreviations
CI, confidence interval; InSCI, international spinal cord injury; IQR, interquartile range; MorSCI, moroccan spinal cord injury community survey; N, number of individuals; OECD, organization for economic co-operation and development; OR, odds ratio; QoL, quality of life; Ref, reference category; SCI, spinal cord injury; SCI-SCS, spinal cord injury secondary condition scale; SD, standard deviation; SES, socioeconomic status; SF-36, 36-item short form health survey; SSS, subjective social status; WHOQoL-5, world health organization quality of life assessment-5.
References
1. Mackenbach JP, Stirbu I, Roskam A-JR, Schaap MM, Menvielle G, Leinsalu M, et al. Socioeconomic inequalities in health in 22 European countries. N Engl J Med. (2008) 358(23):2468–81. doi: 10.1056/NEJMsa0707519
2. Marmot M, Allen J, Bell R, Bloomer E, Goldblatt P. WHO European review of social determinants of health and the health divide. Lancet. (2012) 380(9846):1011–29. doi: 10.1016/S0140-6736(12)61228-8
3. Marmot M. Social determinants of health inequalities. Lancet. (2005) 365(9464):1099–104. doi: 10.1016/S0140-6736(05)71146-6
4. Arcaya MC, Arcaya AL, Subramanian SV. Inequalities in health: definitions, concepts, and theories. Glob Health Action. (2015) 8(1):27106. doi: 10.3402/gha.v8.27106
5. Boutayeb A, Helmert U. Social inequalities, regional disparities and health inequity in north African countries. Int J Equity Health. (2011) 10(1):1–9. doi: 10.1186/1475-9276-10-23
6. Boutayeb A. Social inequalities and health inequity in Morocco. Int J Equity Health. (2006) 5(1):1–6. doi: 10.1186/1475-9276-5-1
7. Jaidi L. Economic and social change in Morocco: Civil society's Contributions and limits. The arab transitions in a changing world: building democracies in light of international experiences. Barcelona: Institute European de la Medditerrània (2016). 145–64.
8. Hajjioui A, Fourtassi M, Tachfouti N, Laaroussi Z, Boulman S, Boujraf S, et al. People with spinal cord injury in Morocco: results from the very first systematic data collection. Disabil Rehabil. (2021) 44(25):8054–65. doi: 10.1080/09638288.2021.2003451
9. Marmot M. Social justice, epidemiology and health inequalities. Eur J Epidemiol. (2017) 32(7):537–46. doi: 10.1007/s10654-017-0286-3
10. World Health Organization. Seventy-fourth world health assembly. Social determinants of health. World Health Organization (2021). Available at: https://apps.who.int/gb/ebwha/pdf_files/ WHA74/A74_R16-en.pdf (Accessed Feb 4, 2022).
11. Fekete C, Siegrist J, Reinhardt JD, Brinkhof MWG, SwiSCI Study Group Is financial hardship associated with reduced health in disability? The case of spinal cord injury in Switzerland. PLoS One. (2014) 9(2):e90130. doi: 10.1371/journal.pone.0090130
12. Krause JS, Broderick LE, Saladin L, Broyles J. Racial disparities in health outcomes after spinal cord injury: mediating effects of education and income. J Spinal Cord Med. (2006) 29(1):17–25. doi: 10.1080/10790268.2006.11753852
13. Saunders LL, Krause JS, Acuna J. Association of race, socioeconomic Status, and health care access with pressure ulcers after spinal cord injury. Arch Phys Med Rehabil. (2012) 93(6):972–7. doi: 10.1016/j.apmr.2012.02.004
14. Brinkhof M, Al-Khodairy A, Eriks-Hoogland I, Fekete C, Hinrichs T, Hund-Georgiadis M, et al. Health conditions in people with spinal cord injury: contemporary evidence from a population-based community survey in Switzerland. J Rehabil Med. (2016) 48(2):197–209. doi: 10.2340/16501977-2039
15. Bickenbach J, Biering-Sørensen F, Knott J, Shakespeare T, Stucki G, Tharion G, et al. Understading spinal cord injury. In: Bickenbach J, Bodine C, Brown D, Burns A, Campbell R, Cardenas D, et al. editors. International perspectives on spinal cord injury. Geneva: World Health Organization (2013). p. 3–10.
16. Oña A, Strøm V, Lee BS, Le Fort M, Middleton J, Gutenbrunner C, et al. Health inequalities and income for people with spinal cord injury. A Comparison Between and Within Countries. SSM—Population Health. (2021) 1(15):100854. doi: 10.1016/j.ssmph.2021.100854
17. Tough H, Brinkhof MWG, Siegrist J, Fekete C. Social inequalities in the burden of care: a dyadic analysis in the caregiving partners of persons with a physical disability. Int J Equity Health. (2020) 19(1):1–12. doi: 10.1186/s12939-019-1112-1
18. Wilkinson R, Marmot M, World Health Organization. The solid facts: social determinants of health. Copenhagen: World Health Organization (2003). Available at: https://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf (Accessed Feb 18, 2022).
19. Barbareschi G, Carew MT, Johnson EA, Kopi N, Holloway C. “When they see a wheelchair, they’ve not even seen me”—factors shaping the experience of disability stigma and discrimination in Kenya. Int J Environ Res Public Health. (2021) 18(8):4272. doi: 10.3390/ijerph18084272
20. Øderud T. Surviving spinal cord injury in low income countries. Afr J Disabil. (2014) 3(2):1–9. doi: 10.4102/ajod.v3i2.80
21. Sarfo FS, Nichols M, Qanungo S, Teklehaimanot A, Singh A, Mensah N, et al. Stroke-related stigma among west Africans: patterns and predictors. J Neurol Sci. (2017) 375:270–4. doi: 10.1016/j.jns.2017.02.018
22. Shavers VL. Measurement of socioeconomic Status in health disparities research. J Natl Med Assoc. (2007) 99(9):1013–23. doi: 10.13016/avw3-9cvx
23. Perry LM, Hoerger M, Seibert K, Gerhart JI, O’Mahony S, Duberstein PR. Financial strain and physical and emotional quality of life in breast cancer. J Pain Symptom Manage. (2019) 58(3):454–9. doi: 10.1016/j.jpainsymman.2019.05.011
24. Tucker-Seeley RD, Harley AE, Stoddard AM, Sorensen GG. Financial hardship and self-rated health among low-income housing residents. Health Educ Behav. (2013) 40(4):442–8. doi: 10.1177/1090198112463021
25. Singh-Manoux A, Adler NE, Marmot MG. Subjective social status: its determinants and its association with measures of ill-health in the whitehall II study. Soc Sci Med. (2003) 56(6):1321–33. doi: 10.1016/S0277-9536(02)00131-4
26. Euteneuer F. Subjective social status and health. Curr Opin Psychiatry. (2014) 27(5):337–43. doi: 10.1097/YCO.0000000000000083
27. Hoebel J, Lampert T. Subjective social status and health: multidisciplinary explanations and methodological challenges. J Health Psychol. (2020) 25(2):173–85. doi: 10.1177/1359105318800804
28. Demakakos P, Nazroo J, Breeze E, Marmot M. Socioeconomic status and health: the role of subjective social status. Soc Sci Med. (2008) 67(2):330–40. doi: 10.1016/j.socscimed.2008.03.038
29. Jaccard J, Turrisi R. Two-way interactions. In: Lewis-Beck MS, editors. Interaction effects in multiple regression. New York: Sage University Paper (2003) p. 16–43.
30. Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health: final report of the commission on social determinants of health. Geneva: World Health Organization (2008).
31. Hosseinpoor AR, Stewart Williams J, Amin A, Araujo de Carvalho I, Beard J, Boerma T, et al. Social determinants of self-reported health in women and men: understanding the role of gender in population health. PLoS One. (2012) 7(4):e34799. doi: 10.1371/journal.pone.0034799
32. Sen G, Östlin P. Gender inequity in health: why it exists and how we can change it. Glob Public Health. (2008) 3(S):11–12. doi: 10.1080/17441690801900795
33. Human Development Reports. Gender Inequality Index (GII). Available at: https://hdr.undp.org/data-center/thematic-composite-indices/gender-inequality-index#/indicies/GII (Accessed Mar 4, 2023).
34. Fekete C, Brach M, Ehrmann C, Post MWM, Stucki G, Middleton J, et al. Cohort profile of the international spinal cord injury community survey implemented in 22 countries. Arch Phys Med Rehabil. (2020) 101(12):2103–11. doi: 10.1016/j.apmr.2020.01.022
35. Fekete C, Post MWM, Bickenbach J, Middleton J, Prodinger B, Selb M, et al. A structured approach to capture the lived experience of spinal cord injury: data model and questionnaire of the international spinal cord injury community survey. Am J Phys Med Rehabil. (2017) 96(2):S5–16. doi: 10.1097/PHM.0000000000000622
36. UNESCO Institute for Statistics. International standard classification of education ISCED 2011. Montreal: United Nations Educational, Scientific and Cultural Organization (UNESCO) (2012). Available at: http://www.uis.unesco.org/Education/Documents/isced-2011-en.pdf (Accessed Sep 15, 2021).
37. World Health Organization. Model disability survey (MDS): survey manual. Geneva: World Health Organization (2017). Available at: http://apps.who.int/iris/bitstream/10665/258513/1/ 9789241512862-eng.pdf (Accessed Sep 15, 2021).
38. European Social Survey. ESS Round 8 source questionnaire. London: ESS ERIC Headquarters c/o City University London (2016). Available at: https://www.europeansocialsurvey.org/docs/round8/fieldwork/source/ESS8_source_questionnaires.pdf (Accessed Jan 3, 2022).
39. Hagenaars A, Vos Kd, Zaidi MA. Poverty statistics in the late 1980s: research based on micro-data. Luxembourg: Office for Official Publications of the European Communities (1994).
40. Directorate for Employment, Labour and Social Affairs, OECD Statistics Directorate. Quality review of the OECD database on household incomes and poverty and the OECD earnings database. Part I. (2012). Available at: https://www.oecd.org/els/soc/OECDIncomeDistribution QualityReview_PartI.pdf (Accessed Feb 4, 2022).
41. Ferreira WA, Giatti L, Figueiredo RC, Mello HR, Barreto SM. Concurrent and face validity of the MacArthur scale for assessing subjective social status: brazilian longitudinal study of adult health (ELSA-brasil). Cien Saude Colet. (2018) 23:1267–80. doi: 10.1590/1413-81232018234.16972016
42. Cundiff JM, Smith TW, Uchino BN, Berg CA. Subjective social Status: construct validity and associations with psychosocial vulnerability and self-rated health. Int J Behav Med. (2013) 20(1):148–58. doi: 10.1007/s12529-011-9206-1
43. Kalpakjian CZ, Scelza WM, Forchheimer MB, Toussaint LL. Preliminary reliability and validity of a spinal cord injury secondary conditions scale. J Spinal Cord Med. (2007) 30(2):131–9. doi: 10.1080/10790268.2007.11753924
44. Poquet N, Lin C. The brief pain inventory (BPI). J Physiother. (2016) 62(1):52. doi: 10.1016/j.jphys.2015.07.001
45. Cleeland CS, Ryan KM. Pain assessment: global use of the brief pain inventory. Ann Acad Med Singap. (1994) 23:129–38.8080219
46. Bryce TN, Budh CN, Cardenas DD, Dijkers M, Felix ER, Finnerup NB, et al. Pain after spinal cord injury: an evidence-based review for clinical practice and research. J Spinal Cord Med. (2007) 30(5):421–40. doi: 10.1080/10790268.2007.11753405
47. Ware JE, Snow KK, Kosinski M, Gandek B. SF36 Health survey: manual and interpretation guide. Lincoln, RI: Quality Metric Incorporated (1993).
48. Geyh S, Fellinghauer BA, Kirchberger I, Post MW. Cross-cultural validity of four quality of life scales in persons with spinal cord injury. Health Qual Life Outcomes. (2010) 8(1):1–6. doi: 10.1186/1477-7525-8-94
49. Huo T, Guo Y, Shenkman E, Muller K. Assessing the reliability of the short form 12 (SF-12) health survey in adults with mental health conditions: a report from the wellness incentive and navigation (WIN) study. Health Qual Life Outcomes. (2018) 16(1):1–8. doi: 10.1186/s12955-018-0858-2
50. Ware JE, Kosinski M, Keller SD. How to score SF-12 physical and mental health summary scales. 2nd ed. Boston, MA: The Health Institue, New Englang Medical Center (1995).
51. Sturm C, Gutenbrunner CM, Egen C, Geng V, Lemhöfer C, Kalke YB, et al. Which factors have an association to the quality of life (QoL) of people with acquired spinal cord injury (SCI)? A cross-sectional explorative observational study. Spinal Cord. (2021) 59(8):925–32. doi: 10.1038/s41393-021-00663-z
52. Bickenbach J, Boldt I, Brinkhof M, Chamberlain J, Cripps R, Fitzharris M, et al. A global picture of spinal cord injury. In: Bickenbach J, Bodine C, Brown D, Burns A, Campbell R, Cardenas D, et al. editors. International perspectives on spinal cord injury. Geneva: World Health Organization (2013). p. 13–41.
53. Mehmetoglu M, Jakobsen TG. Applied statistics using stata: a guide for the social sciences. London: Sage (2022).
54. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York: Guilford publications (2017).
55. Fekete C, Tough H, Leiulfsrud AS, Postma K, Bökel A, Tederko P, et al. Socioeconomic status, the countries’ socioeconomic development and mental health: observational evidence for persons with spinal cord injury from 22 countries. Int J Public Health. (2022) 67:278. doi: 10.3389/ijph.2022.1604673
56. Camacho EM, Verstappen SMM, Symmons DPM. Association between socioeconomic status, learned helplessness, and disease outcome in patients with inflammatory polyarthritis. Arthritis Care Res. (2012) 64(8):1225–32. doi: 10.1002/acr.21677
57. Mishra S, Carleton RN. Subjective relative deprivation is associated with poorer physical and mental health. Soc Sci Med. (2015) 147:144–9. doi: 10.1016/j.socscimed.2015.10.030
58. Lynch JW, Kaplan GA, Shema SJ. Cumulative impact of sustained economic hardship on physical, cognitive, psychological, and social functioning. N Engl J Med. (1997) 337(26):1889–95. doi: 10.1056/NEJM199712253372606
59. Butterworth P, Rodgers B, Windsor TD. Financial hardship, socio-economic position and depression: results from the PATH through life survey. Soc Sci Med. (2009) 69(2):229–37. doi: 10.1016/j.socscimed.2009.05.008
60. Boutayeb A. Evolution of rural–urban health gaps in Morocco: 1992–2011. BMC Res Notes. (2012) 5(1):1–6. doi: 10.1186/1756-0500-5-381
61. Thakral M, Lacroix AZ, Molton IR. Sex/gender disparities in health outcomes of individuals with long-term disabling conditions. Rehabil Psychol. (2019) 64(2):221–8. doi: 10.1037/rep0000248
62. Kefale B, Alebachew M, Tadesse Y, Engidawork E. Quality of life and its predictors among patients with chronic kidney disease: a hospital-based cross sectional study. PLoS One. (2019) 14(2):e0212184. doi: 10.1371/journal.pone.0212184
Keywords: disability, health inequalites, socioeconomic status, spinal cord injury, moderation, gender, Morocco
Citation: Limacher R, Hajjioui A, Fourtassi M and Fekete C (2023) Does gender moderate the association between socioeconomic status and health? Results from an observational study in persons with spinal cord injury living in Morocco. Front. Rehabil. Sci. 4:1108214. doi: 10.3389/fresc.2023.1108214
Received: 25 November 2022; Accepted: 14 March 2023;
Published: 4 April 2023.
Edited by:
Corneliu Bolbocean, University of Oxford, United KingdomReviewed by:
Paulo Moreira Silva Dantas, Federal University of Rio Grande do Norte, BrazilSungwook Kim, University of Oxford, United Kingdom
© 2023 Limacher, Hajjioui, Fourtassi and Fekete. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christine Fekete Y2hyaXN0aW5lLmZla2V0ZUB3b3JrbWFzdGVyeS5jaA==
Specialty Section: This article was submitted to Disability, Rehabilitation, and Inclusion, a section of the journal Frontiers in Rehabilitation Sciences