 Pinto Francisco Impito
Pinto Francisco Impito José Azevedo
José Azevedo- 1Department of Arts and Humanities, Licungo University, Quelimane, Mozambique
- 2Department of Communication and Information Sciences, Laboratory for Integrative and Translational Research in Population Health (ITR), EPIUnit-Institute of Public Health, University of Porto, Porto, Portugal
- 3Faculty of Arts and Humanities, University of Porto, Porto, Portugal
Introduction: Health education is vital for empowering patients with knowledge about their health conditions, treatment options, and self-care, enabling them to make informed decisions. Video-based Health Education (VbHE) has proven to be a powerful tool for enhancing health literacy, often outperforming traditional methods in various circumstances. Previous research has focused on specific diseases in low-resource settings, but a broader understanding of video applications and implementation challenges remains necessary. This systematic review assessed the use of video for health education purposes in the least developed African countries from 2020 to 2024, exploring insights into the types of health content delivered through video, their effectiveness, and implementation obstacles.
Methods: We searched the ScienceDirect, PubMed, Scopus, Google Scholar, PLOS, and AJOL databases, limiting our review to the UN’s 33 least-developed African countries. Studies were evaluated based on country, participants, sample sizes, intervention methods, duration, video delivery, educational emphasis, objectives, outcomes, and findings. Adhering to PRISMA guidelines ensured a structured methodology.
Results: From the 218 records identified, 15 studies met our inclusion criteria. These studies highlighted video interventions with a focus on cancer (n = 5, 33.3%), HIV (n = 3, 20%), maternity care (n = 5, 33.3%), and other areas (n = 2, 13.3%, including COVID-19 and spinal anesthesia procedures). Most studies (n = 13, 86.6%) showed videos positively influenced knowledge retention and health outcomes, while the remaining two (n = 2, 13.3%) noted no significant difference from traditional methods. Video dissemination methods featured mobile devices, TV screens, and online platforms, with intervention durations ranging from 30 min to 36 months. Of the included studies, video has proven effective in enhancing health education in the least-developed African nations.
Discussion: Challenges including connectivity issues, cultural adaptation, and digital literacy remain significant. This review highlights the critical role of mobile video health communication in empowering underserved populations and informs future strategies to optimize health outcomes in resource-constrained African Contexts.
1 Introduction
The use of video for information and education has experienced substantial growth (Chatterjee et al., 2021). Among various digital formats, video has proven to be an effective medium for delivering health education due to its ability to enhance knowledge retention and accessibility. However, there are significant challenges; health professionals and ordinary web users often share health-related content within the same online spaces, raising concerns about the reliability of the information (Karlsen et al., 2013), and deviant behavior (Zhou et al., 2022). This is particularly concerning given the increasing trend of individuals posting self-produced health videos on social media, shifting responsibility onto the viewers if adverse outcomes happen. Despite these concerns, health professionals continue to rely on user-generated videos instead of producing original material, which impacts the quality and relevance of the education provided (Farrell et al., 2014; Snelson, 2018).
In recent years, research from the least-developed African countries has shown a shift toward health workers producing their video content for educational purposes (Ferla et al., 2023; Scott et al., 2022). This change signals a growing awareness of the significance of original video content in boosting patient education and involvement (Chatterjee et al., 2021; Adam SAM et al., 2019; WHO, 2024). This awareness became even more pronounced during the COVID-19 pandemic, further emphasizing the importance of digital health tools. During this period, many African nations have successfully utilized mobile devices to disseminate educational videos, illustrating the potential for enhanced health outcomes through digital innovation (Kinkade et al., 2022). However, while these tools have helped share information during the pandemic, they have also hosted rumors that led to misinformation, with traditional media being the only means capable of countering it by promoting critical thinking and limiting the spread of health-related rumors (Guo et al., 2023). Providing clear, credible information can foster more thoughtful engagement and increase user acceptance (Luo et al., 2021).
To encourage the use of digital health tools, the World Health Organization (WHO) has urged 47 countries in Africa to develop and implement digital health strategy plans (Alegana et al., 2023). While many of these nations acknowledge the benefits of such technologies and have started incorporating them into their health systems, a notable number (n = 14) still do not have comprehensive plans (Alegana et al., 2023). This initiative reflects a growing recognition across the continent of the value of digital technologies for various applications and emphasizes the need for their effective integration into health care. As part of the 2030 Agenda for the African region, WHO’s recommendations on digital health interventions support the pursuit of Universal Health Coverage (UHC) and disease prevention, reinforcing the digital health strategy for 2020–2025 (WHO, 2023). In the context of video utilization, the WHO advocates for mHealth based on initiatives such as ‘virtual care,’ ‘remote monitoring,’ ‘digital therapeutics’ (WHO, 2021), ‘video-based training,’ ‘video recordings,’ and leveraging YouTube for health videos (WHO, 2024) to improve health outcomes.
Recent reports highlight the constraints of video-based health education in the least developed African nations (Kabukye et al., 2021; Mamuye et al., 2022; Till et al., 2023), where some, if not many, local institutions struggle to maintain their promotion. Barriers such as limited access to affordable mobile data, low smartphone usage, and insufficient digital literacy contribute to a digital divide, hindering the reach and efficacy of video interventions. The WHO indicates that, although some countries have made significant strides in adopting digital health tools, many still require ‘institutional support’ for developing and strengthening their digital health strategies (WHO, 2021). Beyond infrastructure, emphasizing the usefulness of these tools and fostering attitudes through trust and engaging content can significantly enhance adoption (Zhang et al., 2014).
This systematic review aimed to assess the use of video-based health education in the least developed African countries, focusing on studies published from 2020 to 2024 and examining the impact, obstacles, and opportunities for improvement in under-resourced settings. Since African low-resource settings are often facing systemic barriers, such as underfunded health systems and a lack of trained professionals in using digital media tools for health education, traditional health education methods frequently fall short or are unsustainable. In this context, our study highlights these countries as a strategic and relevant area for evaluating the use of video-based health education as a cost-effective and scalable solution. The goal is not only to assess its applicability and impact but also to increase awareness of its potential and promote further research into integrating it into health training programs in similar environments.
2 Methods
2.1 Search strategy and database overview
A comprehensive literature review was conducted using the ScienceDirect, PubMed, Scopus, Google Scholar, PLOS, and AJOL databases. The search was limited to studies conducted in the 33 least-developed African countries as defined by the UN, and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). The keywords and search terms included combinations of: “Health videos,” “Educational videos,” “Video-based health education,” “Digital health,” “Health education,” and “Low-resource settings.” Boolean operators (AND, OR) were utilized to refine the search results, with filters applied to select studies published between 2020 and 2024, in English, and meeting the specified inclusion criteria.
During full-text review and data extraction, it became apparent that the included studies could be meaningfully categorized based on the primary population addressed by the interventions, namely, Patients and/or citizens (e.g., general public, disease-specific populations, adolescents, pregnant women, rural communities), and Health workers (e.g., doctors, nurses, community health workers, program managers, drug distributors). The latter group highlights the importance of multi-stakeholder approaches grounded in supportive policies to guide the development and promotion of digital health content (Zhang et al., 2017). In these situations, stakeholders are typically dedicated professionals who volunteer their time without pay, reflecting the realities of low-resource environments (Yang et al., 2021). Although the division between Patients and/or Citizens and Health workers was not an initial inclusion criterion, it was identified inductively due to apparent differences in intervention design, educational content, and reported outcomes. Consequently, after screening and extraction, studies were grouped according to the target population (patients/citizens vs. health workers). Subsequent synthesis and reporting were structured along these two categories to provide a more nuanced understanding of how video-based health education approaches differ according to the intended audience.
2.2 Ligibility and exclusion criteria
The review encompassed studies focused on enhancing, evaluating, designing, advocating for, testing, or investigating the use of video as a medium for health education. The eligibility criteria centered on studies published between 2020 and 2024 that examined Video-based Health Education in low-income or least-developed African nations. Studies lacking educational video content, those conducted outside the least-developed African countries, and those published outside the designated timeframe were excluded.
2.3 Data extraction and synthesis
Data extraction was performed using a predefined data extraction form to ensure uniformity across studies. Key information extracted included study characteristics (such as country, participants, sample size, intervention method, research duration, and video delivery approach) along with a performance summary (including educational contents, objectives, outcomes, and findings). To ensure the accuracy and integrity of all extracted data, two independent reviewers (PFI and JA) initially tested the extraction form on a random sample of included studies. They refined variable definitions until achieving an agreement of over 95%. Subsequently, each reviewer independently extracted data for all studies. Discrepancies were identified through systematic cross-checking in a shared spreadsheet and then resolved through discussion. Both reviewers adjudicated any remaining disagreements. Audit trails documented all changes, and the authors recalculated records to verify consistency. The gathered data were qualitatively synthesized, highlighting the effectiveness of Video-based Health Education interventions. A narrative synthesis was employed to summarize and interpret the results, with a focus on identifying observed patterns, differences, and common themes across the studies. The findings were then organized in tables, and key outcomes were discussed in relation to the research objectives (Table 1).

Table 1. The path followed on the method.
Following initial study selection, included studies were subsequently grouped by the population targeted by the intervention (patients/citizens vs. health workers) based on data extracted from the full texts.
3 Results
3.1 Study selection
The database search yielded 218 papers, of which 15 met our selection criteria after excluding duplicates (n = 3). We excluded 197 articles for the following reasons: (1) no use of educational video (n = 57), (2) research was not conducted in the least-developed African countries (n = 63), and (3) studies fell outside the 2020–2024-year range (n = 77). Participants’ demographics included health workers who received video training (n = 4), patients, and/or citizens (n = 11), all of whom were assessed for their responses to video-based health education (Figure 1).
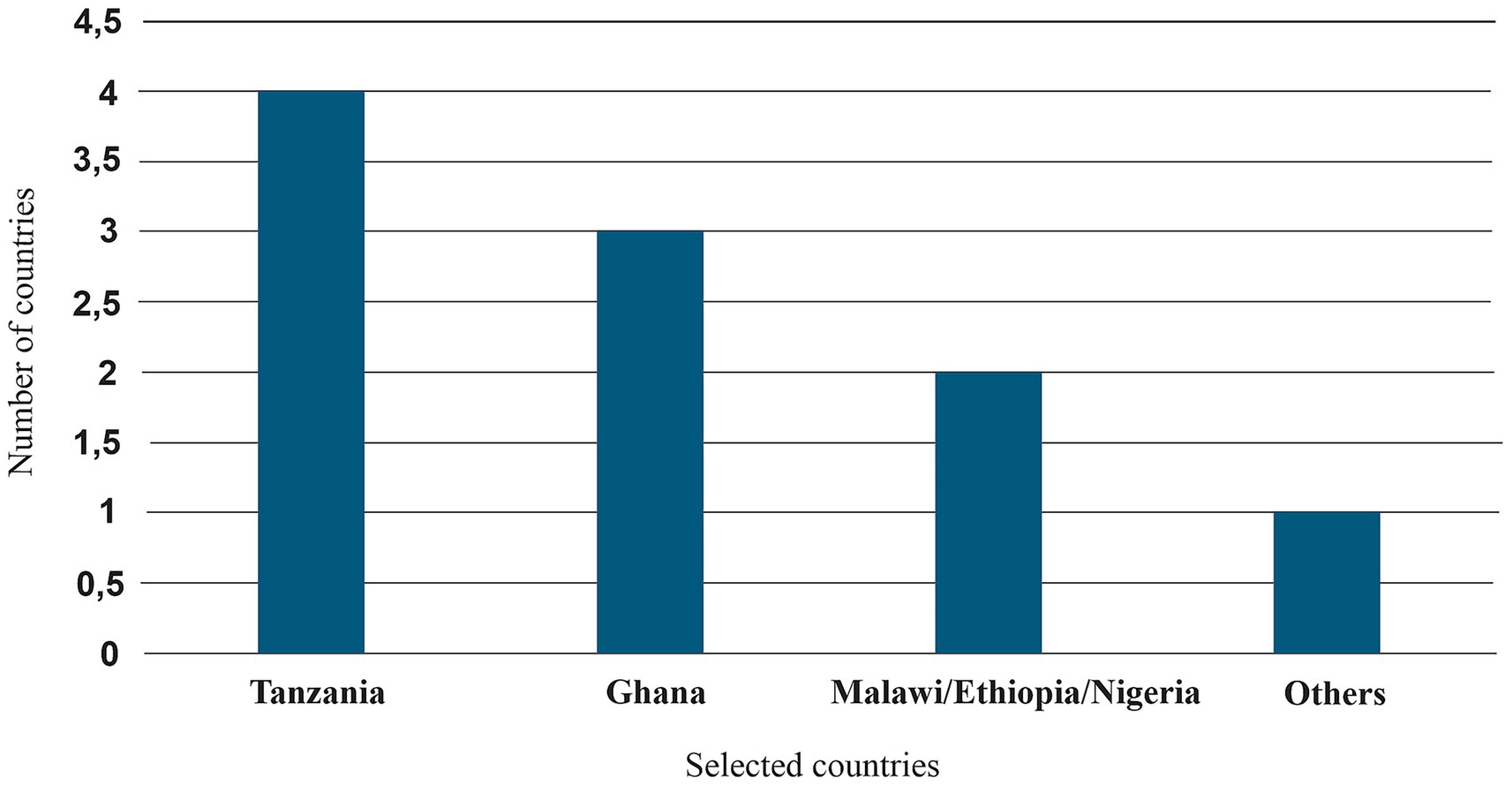
Figure 1. Number of studies per identified country.
3.2 Study characteristics
Only 24 countries were identified as implementing video-based health education. These include Tanzania (n = 4), Ghana (n = 3), Malawi (n = 2), Ethiopia (n = 2), Nigeria (n = 2), Kenya (n = 1), Botswana (n = 1), Uganda (n = 1), Rwanda (n = 1), Burundi (n = 1), Niger (n = 1), the Democratic Republic of the Congo (n = 1), São Tomé and Príncipe (n = 1), Benin (n = 1), Burkina Faso (n = 1), Gambia (n = 1), Guinea (n = 1), Guinea-Bissau (n = 1), Liberia (n = 1), Mali (n = 1), Mauritania (n = 1), Senegal (n = 1), Sierra Leone (n = 1), and Togo (n = 1). In this review, Tanzania and Ghana emerged as the countries with the most studies, followed by Malawi, Ethiopia, and Nigeria, as illustrated in Figure 2.
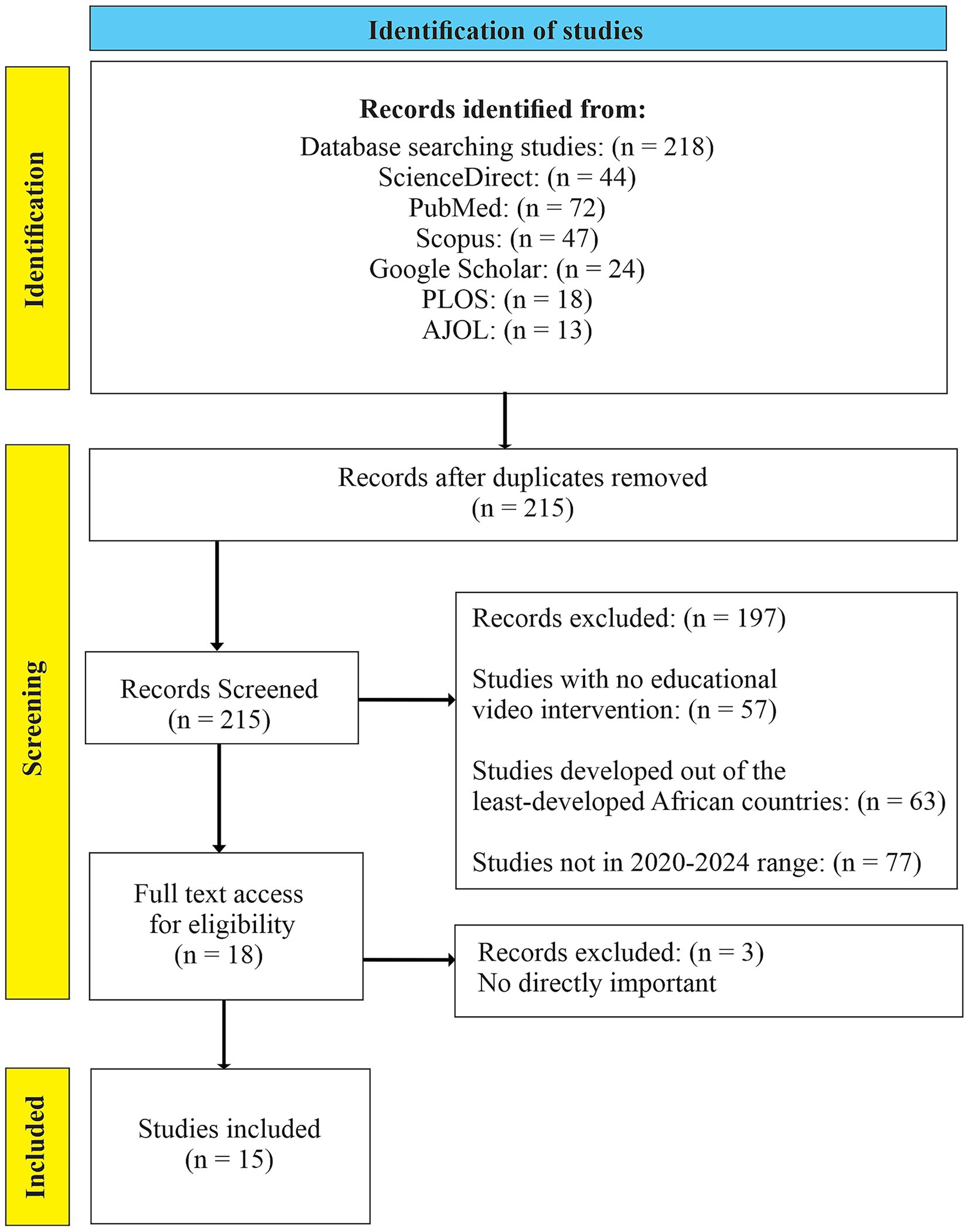
Figure 2. PRISMA flow diagram used in the study description.
3.2.1 Sample size
The study’s sample size varied from 9 to 7,648 participants. Four studies reported an average age range of 22–42 (Holst et al., 2021; Masiano et al., 2021; Godana Boynito et al., 2023; Obasola, 2021); three had an average age of 18 (Martei et al., 2024; Drokow et al., 2021; Kanyeki et al., 2022), while the remaining eight did not provide age data (Ferla et al., 2023; Scott et al., 2022; Tilly et al., 2022; Cooper et al., 2021; Ampofo et al., 2020; Mengistu et al., 2021; Holst et al., 2022; Ansari et al., 2024). The search exclusively targeted the least-developed African countries between 2020 and 2024. According to the UN classification, 33 countries are categorized as least developed (UN, 2024).
3.2.2 Dissemination, method, and duration
The studies utilized various media to present videos, including TV monitors or projectors (n = 6), mobile devices (n = 7) such as tablets, mobile phones, and portable projectors, online media (n = 1) through platforms such as YouTube, Web, and WhatsApp, and other formats (n = 1), such as TV, DVD, or compact disks. These video-based health education initiatives occurred in health facilities, schools, and occasionally in residential settings through door-to-door visits. The duration of the education programs varied from 30 to 40 min up to 36 months.
Three of the 15 studies reviewed employed true randomized control designs, assessing both control and intervention groups (Kanyeki et al., 2022; Holst et al., 2022; Ansari et al., 2024). The other 12 were single-group studies, often conducted in focus groups or with individuals, and utilized pre- and post-intervention assessments (Ferla et al., 2023; Scott et al., 2022; Holst et al., 2021; Masiano et al., 2021; Godana Boynito et al., 2023; Obasola, 2021; Martei et al., 2024; Drokow et al., 2021; Tilly et al., 2022; Cooper et al., 2021; Ampofo et al., 2020; Mengistu et al., 2021) (Table 2).
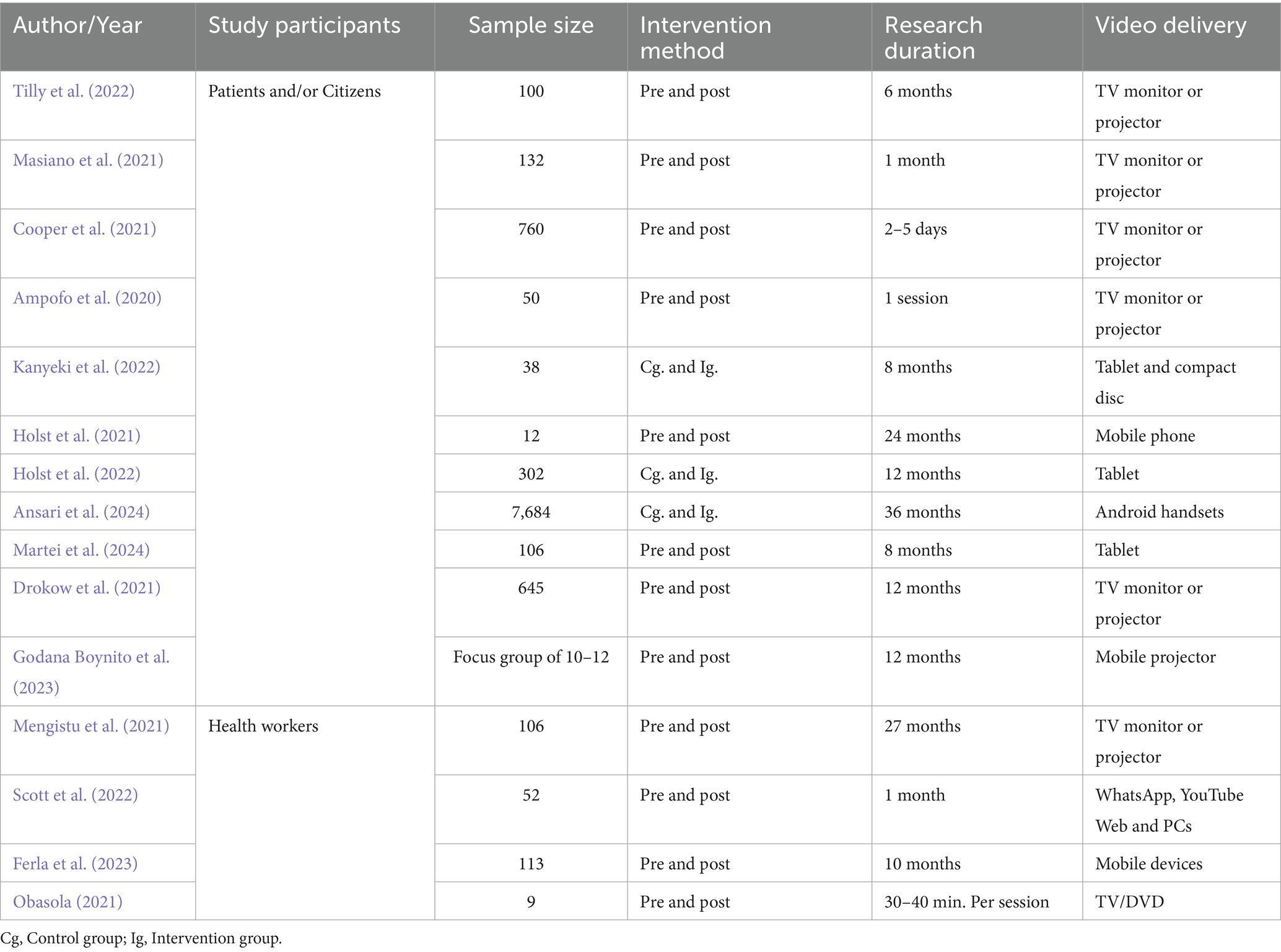
Table 2. Study characteristics.
3.3 Performance summary
3.3.1 Educational contents and outcomes
In general, the studies focused on video education initiatives covering topics such as cancer (n = 5, 33.3%; Martei et al., 2024; Drokow et al., 2021; Tilly et al., 2022; Cooper et al., 2021; Ampofo et al., 2020), HIV (n = 3, 20%; Holst et al., 2021; Masiano et al., 2021; Holst et al., 2022), maternity care (n = 5, 33.3%; Ferla et al., 2023; Godana Boynito et al., 2023; Obasola, 2021; Mengistu et al., 2021; Ansari et al., 2024), and other areas (n = 2, 13.3%, including COVID-19 and spinal anesthesia procedures; Scott et al., 2022; Kanyeki et al., 2022). In terms of preliminary outcomes, most studies (n = 13, 86.6%) found that the use of video proved effective, and in the remaining (n = 2, 13.3%), no significant differences were noted between video usage and no video.
The studies focusing on patients and/or citizens (n = 11) covered a range of topics. Of these, five (n = 5) focused on cancer-related subjects, using videos to discuss common myths, diagnostic procedures, bodily diseases, treatments, reactions to aftereffects, and quality of life (Martei et al., 2024). They aimed to raise awareness and knowledge about the screening and risks associated with human papillomavirus infection, the treatment and experiences of breast cancer survivors, and to promote vaccination, awareness, and counseling for the Pap smear test. Three studies (n = 3) addressed HIV-related issues (Holst et al., 2021; Masiano et al., 2021; Holst et al., 2022), through videos that highlighted the importance of antiretroviral therapy and addressed significant concerns regarding HIV/AIDS, tuberculosis, Taenia Solium (neuro) cysticercosis, taeniasis, and anthrax. Finally, the last three studies (n = 3) covered maternal and child health (Godana Boynito et al., 2023; Ansari et al., 2024), as well as spinal anesthesia procedures, including a video that reviews the pre-operative anxiety state (Kanyeki et al., 2022).
Similarly, studies focusing on health workers (n = 4) featured content related to maternity care topics that included testimonials from mothers (Mengistu et al., 2021), COVID-19 education, showcasing a video that guided handwashing, mask-wearing, and maintaining social distancing (Scott et al., 2022), motherhood, neonatal, and maternal child healthcare (Obasola, 2021), and finally, counselors offering guidance on nurturing care for caregivers (Ferla et al., 2023).
3.3.2 Finding summary
Eleven of the fifteen selected studies focused on patients and/or citizens, including students and women. Nine of these studies reported increased (1) knowledge (Holst et al., 2021; Drokow et al., 2021; Tilly et al., 2022; Cooper et al., 2021), (2) awareness and information retention (Masiano et al., 2021; Godana Boynito et al., 2023; Ampofo et al., 2020), and overall, (3) the video content was found to be acceptable, usable, and recommendable (Holst et al., 2021; Martei et al., 2024). Two studies reported “no statistical difference” in outcomes with or without video use, yet indicated increased knowledge (Ansari et al., 2024) and no discernible benefits (Kanyeki et al., 2022) (Table 3). Meanwhile, the remaining four studies, which involved health workers comprising health professionals, healthcare providers, program managers, and community health workers, showed improvements and clarity in understanding health content presented in video format (Ferla et al., 2023; Scott et al., 2022; Obasola, 2021; Mengistu et al., 2021). These studies recognized the potential of video for delivering effective health content, and overall, video-based health education interventions were reported to have a positive impact on the target audience (Table 4).
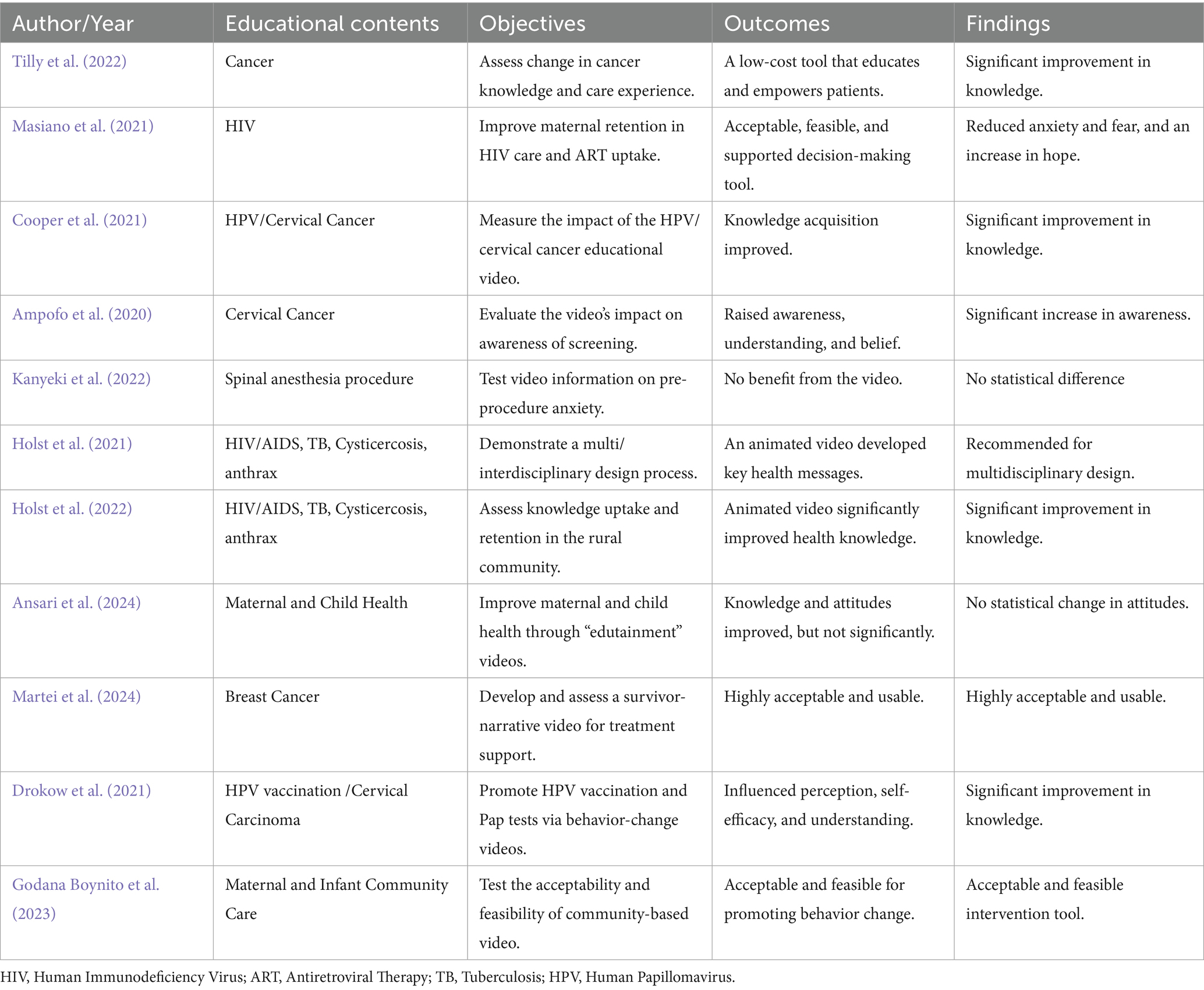
Table 3. Performance summary (patients and/or citizens).
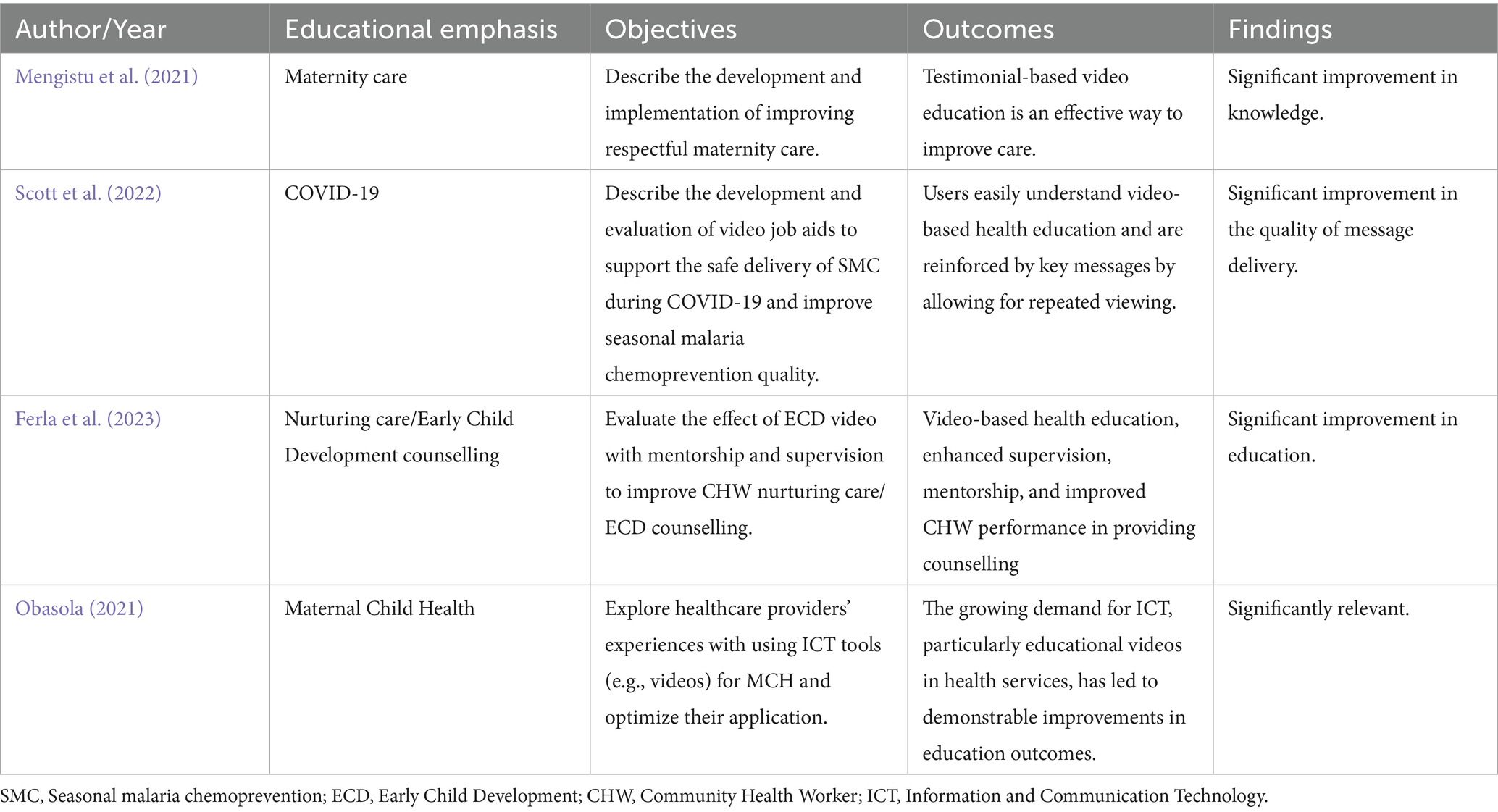
Table 4. Performance summary (health workers).
4 Discussion
This review systematically compiles evidence on video-based health education initiatives in the 24 least-developed African countries from 2020 to 2024. Among 15 eligible studies, most (13 out of 15, 86.6%) reported positive effects on knowledge, awareness, or self-efficacy among patients, citizens, and health workers. These results support global findings that multimodal media, such as video, can enhance understanding and memory (Ferguson, 2012; Robert et al., 2023; Yang et al., 2021), particularly in settings with low literacy levels (Ferguson, 2012; Liu et al., 2025).
4.1 Effectiveness and reach
Video-based health education is an impactful method for engaging patients effectively across various healthcare intervention sectors, including diagnosis, treatment, and self-care (Ploderer et al., 2022). Research conducted in some of the least-developed African nations highlighted this potential. Ansari et al. (2024) and Masiano et al. (2021) reported that video is a valuable tool for promoting health education among pregnant women regarding maternal and childbirth health (Ansari et al., 2024), and improving maternal retention in HIV care and the uptake of antiretroviral therapy (Masiano et al., 2021), respectively. Furthermore, Tilly et al. (2022) demonstrate that video is a cost-effective tool. Their study reveals that video-based health education saves patients time and money compared to traveling by bus or other means to attend awareness sessions at health centers. Patients can watch videos from home as often as they like using smartphones or other internet-enabled devices. The rapid sharing and widespread availability of health-related videos online have established them as a leading medium for health education and promotion (Ghozali, 2023).
Understanding health conditions helps diminish the barriers between doctors and patients, transforming doubt into informed dialogue. This improved understanding leads to higher patient satisfaction, whether it comes from real-time online support delivered by a physician (Tan et al., 2023), or from a pre-recorded health education video that engages both visual and auditory senses (Anasi, 2004). Further to the above, research from Tilly et al. (2022), Cooper et al. (2021), Holst et al. (2021), and Drokow et al. (2021) demonstrated how effective videos were in increasing knowledge among their audiences, primarily focusing on cancer, human papillomavirus infection, and HIV/AIDS. This increase in knowledge encourages patients to engage with the content anytime, anywhere, thereby enhancing comprehension retention (Naderyanfar et al., 2019; Gusdorf et al., 2023) and positively influencing memory, understanding, and emotions. These cognitive and emotional attitudes are primarily driven by how the information is tailored to the audience and how effectively it is delivered (Wang et al., 2018).
Numerous systematic reviews evaluating the effects of video-based health education in the least-developed African countries have shown steady growth in its application throughout the continent (Till et al., 2023). This approach has been shown to enhance knowledge among individuals with low literacy levels markedly (Mbanda et al., 2021); it acts as an effective decision-making tool (Mwase et al., 2022) and improves patients’ comprehension of health-related information (Boynito et al., 2024). Yet, several challenges hinder the implementation of video-based health education in these regions, which local governments need to tackle. These challenges include inadequate funding, limited technological literacy, a scarcity of technological resources (Kabukye et al., 2021), a lack of a health information exchange policy (Mamuye et al., 2022), and an overreliance on text-based communication (Till et al., 2023). Nevertheless, at least four studies from the least-developed African countries indicate that health institutions actively promote health education through videos: (1) Mengistu et al. conducted a survey with multidisciplinary health professionals, finding video-based education to be a powerful method for enhancing care (Mengistu et al., 2021), (2) Scott et al., through their study of program managers and drug distributors, discovered that educational videos with health content effectively reinforce messages and are easy to understand (Scott et al., 2022), (3) Ferla et al. explored video-based health education with community health workers, who reported improved counseling performance and enhanced mentorship (Ferla et al., 2023), and finally, (4) Obasola investigated healthcare providers’ perspectives, finding that implementing information and communication technology with video usage positively impacted health education interventions and received strong recommendations for its effectiveness (Obasola, 2021).
Compatibility issues with legacy devices, such as DVD players, outdated smartphones, and analog TVs, as well as the lack of standardized educational platforms in low-resource settings, continue to limit the adoption of AR/VR tools (Mondal and Mondal, 2025). Moreover, the rapid obsolescence of such devices, coupled with high maintenance costs, contributes to financial strain. Within this context, specialized outreach programs can capitalize on the widespread availability of smartphones, observed as early as 2015, by distributing smartphone-based VR kits like Google Cardboard. This strategy enables the delivery of immersive training experiences without requiring significant infrastructure investments (Mondal and Mondal, 2025). The Pragati study conducted in rural India demonstrates this approach by using Google Cardboard-mounted phones to train community health workers in maternal and child health (Sorathia et al., 2017). Adopting 360° guided audiovisual modules that simulated an Assamese home environment (Sorathia et al., 2017), participants experienced a training method distinct from those employed by Ferla and Obasola in training health workers across various African contexts (Ferla et al., 2023; Obasola, 2021).
Beyond the Google Cardboard approach, Neuwirth and Ros proposed the use of 180° video viewed through VR head-mounted displays (HMDs) or 3D-capable computer monitors (Neuwirth and Ros, 2021). These were deemed affordable and practical solutions, particularly suitable for training healthcare professionals in Africa. Compared to educational videos delivered via mobile phones, televisions, projectors, or DVDs, this approach is more effective in fostering engagement. Unlike the least-developed countries in Africa, more developed nations, including the United States, Europe, and parts of Asia, have successfully utilized VR-embedded video as a medium for health education (Costa et al., 2024; Jia et al., 2021). In the United States, for example, this broad application has led to the establishment of online public databases containing videos on various health education topics (Media GH, 2024; Plus, 2024), as well as VR websites dedicated to health education, such as medvr.education (USA), exr.education (England), SIMx (USA), among others.
4.2 Core findings
The assessment of selected studies in this systematic review was divided into two data subsets: “study design” and “performance summary” (Tables 2–4). These datasets were crucial for illustrating the role of video in health education in the least developed African countries from 2020 to 2024. The intervention methodologies employed in these studies to reach their audience were essential for evaluating the impact of videos designed for health education. Randomized controlled trial studies (n = 3) consisted of two groups (e.g., control group with no video and intervention group with video) to compare the effects of video-based health education versus traditional methods. Single-group studies (n = 12) assessed the effectiveness of video by examining a single group through pre- and post-intervention measures.
All included studies reported positive outcomes, although two (n = 2) found no significant difference between video-based methods and conventional practices. Research involving patients and citizens (n = 9) revealed increased knowledge, awareness, and retention of information related to cancer, HIV, human papillomavirus, and maternal and child health care. Furthermore, these studies indicated that video-based health education was deemed acceptable, feasible, and usable. Various sharing tools were employed to evaluate video effectiveness, including TV monitors, projectors, mobile phones, tablets, compact disks, PCs, and digital platforms such as WhatsApp, YouTube, and websites. Additionally, four studies (n = 4) involving health workers highlighted video as an effective educational tool due to its comprehensive nature. They reported understanding health content better when presented in video format, acknowledging its potential for effective health education delivery.
4.3 Future directions
Future research should focus on longitudinal studies to determine whether observed knowledge gains result in lasting behavioral changes, such as regular cancer screenings or consistent adherence to ART. Comparative studies assessing the cost-effectiveness of video versus traditional methods, as well as the level of engagement generated by live-action versus animated videos, are also recommended. Technological innovations, such as AI-driven adaptive videos and gamified features, could further enhance engagement and effectiveness. Equity-oriented research questions remain urgent, including how female participants respond and how to deliver health video education to nomadic and conflict-affected populations.
Ultimately, this review serves as a crucial reminder for the least-developed African nations about the efficacy of digital solutions in overcoming educational obstacles and enhancing health education strategies. Importantly, although limitations and challenges, this review concludes that significant attention is being given to the delivery of Video-based Health Education in most target countries (n = 24, 72.7%).
5 Conclusion
Video-based Health Education has demonstrated substantial potential in enhancing health literacy, knowledge retention, and patient engagement across various health issues in the least-developed African nations. This systematic review highlights the successful use of videos for educational health content, particularly in areas such as cancer, HIV, COVID-19, Human papillomavirus infection, spinal anesthesia procedures, and maternal health. The findings reveal that Video-based Health Education can help bridge gaps left by traditional healthcare delivery, offering a more accessible and engaging resource for patients, health workers, and the general public to enhance their understanding of health matters.
However, several challenges still need to be addressed, such as limited access to digital infrastructure, low levels of technological literacy, and inconsistent internet connectivity. These issues create a digital divide that hinders the broad adoption of video education approaches. Furthermore, the absence of institutional backing and inadequate incorporation of digital health strategies in many African nations restricts the full realization of its benefits. To address these challenges, further research is needed to assess the scalability, sustainability, and long-term effects of the Video-based Health Education initiative. For instance, comparing offline and online delivery methods in both rural and urban areas can help assess the health outcomes, such as knowledge acquisition and behavior change, alongside operational metrics like cost per user, training duration, and technology uptime. Incorporating formal cost-effectiveness and cost–benefit analysis into these studies will provide police makers with essential ROI (Return on investment) data to justify infrastructure investment. Longitudinal cohort studies that combine quantitative surveys and detailed qualitative interviews can also shed light on how digital literacy efforts for patients and healthcare workers influence engagement with video-based health education, as well as identify relevant facilitators or barriers in different contexts.
In conclusion, when carefully adapted and implemented, Video-based Health Education can substantially bridge knowledge and healthcare service gaps in marginalized African populations, empower patients, and provide scalable solutions for the development of health workers. Nevertheless, its effectiveness remains context-dependent, and continued evaluation is needed to maximize its transformative potential while addressing persistent challenges in resource-constrained settings.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
PI: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. JA: Data curation, Formal analysis, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The publication of this work was funded by the Doctoral Program – Digital Media, Faculty of Engineering, University of Porto. The sponsors did not play any role in the study design, data collection, analysis, decision to publish or preparation of the manuscript.
Acknowledgments
I appreciate Professor JA for collaborating with me on this scientific journey, which represents a significant contribution to health communication strategies.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Correction note
A correction has been made to this article. Details can be found at: 10.3389/fcomm.2025.1699250.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adam SAM, M., Prober, C., and Bärnighausen, T. (2019). Human-centered design of video-based health education: an iterative, collaborative, community-based approach. Adv. Digit. Health Open Sci. 21. doi: 10.2196/12128
Alegana, A., Victor LJF, A., Makubalo, L. E., Kalu, A. A., and Impouma, B. (2023). Digital health in the African region should be integral to the health system’s strengthening. Mayo Clin. Proc. Digit. Health 1, 425–434. doi: 10.1016/j.mcpdig.2023.06.003
Ampofo, A. G., SAGOpoku, N. S., Owusu, S. O., and Ibitoye, M. B. (2020). A pilot study of a video-based educational intervention and knowledge of cervical cancer among senior high school students in Ghana: a before-after study. J. Cancer Policy 24:6. doi: 10.1016/j.jcpo.2020.100220
Anasi, S. N. I. (2004). Audiovisual media capabilities and the dissemination of the health information. Libr. Focus 22. doi: 10.29087/2011.3.4.08
Ansari, U., Omer, K., Aziz, A., Gidado, Y., Mudi, H., Jamaare, I. S., et al. (2024). Added value of video edutainment on android handsets in home visits to improve maternal and child health in Bauchi state, Nigeria: secondary analysis from a cluster randomised controlled trial. Digit. Health 10:20552076241228408. doi: 10.1177/20552076241228408
Boynito, W. G., Pauwels, N. S., Otayto, K., De Henauw, S., and Abbeddou, S. (2024). Effects of community-based educational video interventions on nutrition, health, and use of health services in low- and middle-income countries: systematic review and meta-analysis. Nutr. Rev. 83, 201–216. doi: 10.1093/nutrit/nuae004
Chatterjee, A. G. S., Meinert, E., Milne-Ives, M., Halkes, M., and Wyatt-Haines, E. (2021). The use of video for patient information and education: a scoping review of the variability and effectiveness of interventions. Patient Educ. Couns. 104, 2189–2199. doi: 10.1016/j.pec.2021.02.009
Cooper, E. C., Maher, J. A., Naaseh, A., Crawford, E. W., Chinn, J. O., Runge, A. S., et al. (2021). Implementation of human papillomavirus video education for women participating in mass cervical cancer screening in Tanzania. Am. J. Obstet. Gynecol. 224, 105.e1–105.e9. doi: 10.1016/j.ajog.2020.07.018
Costa, JBD, Leyva, RGE, S, PHODF, and Souto, EJP, editors. (2024). “Enhancing virtual reality experiences through embedded 3D models in video content.” in 2024 IEEE International Conference on Consumer Electronics (ICCE); 6–8 Jan. 2024.
Drokow, E. K., Effah, C. Y., Agboyibor, C., Sasu, E., Amponsem-Boateng, C., Akpabla, G. S., et al. (2021). The impact of video-based educational interventions on cervical cancer, pap smear and HPV vaccines. Front. Public Health 9:3. doi: 10.3389/fpubh.2021.681319
Farrell, E. H., Phillips, K., Morgan, B., Savage, K., Lewis, V., Kelly, M., et al. (2014). Systematic review and meta-analysis of audio-visual information aids for informed consent for invasive healthcare procedures in clinical practice. Patient Educ. Couns. 94, 20–32. doi: 10.1016/j.pec.2013.08.019
Ferguson, L. A. (2012). Implementing a video education program to improve health literacy. J. Nurse Pract. 8, e17–e22. doi: 10.1016/j.nurpra.2012.07.025
Ferla, J. P., Gill, M. M., Komba, T., Abubakar, A., Remes, P., Jahanpour, O., et al. (2023). Improvement of community health worker counseling skills through early childhood development (ECD) videos, supervision and mentorship: a mixed methods pre-post evaluation from Tanzania. PLoS Glob. Public Health 3:e0001152. doi: 10.1371/journal.pgph.0001152
Ghozali, M. T. (2023). Is integrating video into tech-based patient education effective for improving medication adherence? A review. Paladyn J. Behav. Robot. 14:109. doi: 10.1515/pjbr-2022-0109
Godana Boynito, W., Tessema, G. Y., Temesgen, K., De Henauw, S., and Abbeddou, S. (2023). Acceptability and feasibility of video-based health education for maternal and infant health in Dirashe District, South Ethiopia: a qualitative study. PLoS Glob. Public Health 3:e0000821. doi: 10.1371/journal.pgph.0000821
Guo, F., Zhou, A., Zhang, X., Xu, X., and Liu, X. (2023). Fighting rumors to fight COVID-19: investigating rumor belief and sharing on social media during the pandemic. Comput. Hum. Behav. 139:107521. doi: 10.1016/j.chb.2022.107521
Gusdorf, R. E., Shah, K. P., Triana, A. J., McCoy, A. B., Pabla, B., Scoville, E., et al. (2023). A patient education intervention improved rates of successful video visits during rapid implementation of telehealth. J. Telemed. Telecare 29, 607–612. doi: 10.1177/1357633X211008786
Holst, C., Isabwe, G. M. N., Sukums, F., Ngowi, H., Kajuna, F., Radovanović, D., et al. (2021). Development of digital health messages for rural populations in Tanzania: multi- and interdisciplinary approach. JMIR Mhealth Uhealth 9:e25558. doi: 10.2196/25558
Holst, C., Stelzle, D., Diep, L. M., Sukums, F., Ngowi, B., Noll, J., et al. (2022). Improving health knowledge through provision of free digital health education to rural communities in Iringa, Tanzania: nonrandomized intervention study. J. Med. Internet Res. 24:e37666. doi: 10.2196/37666
Jia, F., Xu, S., and Huo, J. (2021). Embedded VR video image control system in the ideological and political teaching system based on artificial intelligence. Mob. Inf. Syst. 2021, 1–12. doi: 10.1155/2021/7839821
Kabukye, J. K., Kakungulu, E., Keizer, N., and Cornet, R. (2021). Digital health in oncology in Africa: a scoping review and cross-sectional survey. Int. J. Med. Inform. 158:104659. doi: 10.1016/j.ijmedinf.2021.104659
Kanyeki, T. V. M., Bal, R., and Odaba, D. (2022). Effect of video-based information on preoperative state trait anxiety inventory scores in adult patients presenting for elective caesarean section: a randomized controlled trial. Afr. Health Sci. 22, 117–124. doi: 10.4314/ahs.v22i3.14
Karlsen, R, Morell, JEB, Luque, LF, and Salcedo, VT editors. (2013). “A domain-based approach for retrieving trustworthy health videos from YouTube.” in 14th World Congress on Medical and Health Informatics (MEDINFO); 2013 Aug 20–23; Copenhagen, DENMARK.
Kinkade, C., Russpatrick, S., Potter, R., Saebo, J., Sloan, M., Odongo, G., et al. (2022). Extending and strengthening routine DHIS2 surveillance systems for COVID-19 responses in Sierra Leone, Sri Lanka, and Uganda. Emerg. Infect. Dis. 28, S42–S48. doi: 10.3201/eid2813.220711
Liu, X., Susarla, A., and Padman, R. (2025). Promoting health literacy with human-in-the-loop video understandability classification of YouTube videos: development and evaluation study. J. Med. Internet Res. 27:e56080. doi: 10.2196/56080
Luo, P., Ma, X., Zhang, X., Liu, J., and He, H. (2021). How to make money with credit information? Information processing on online accommodation-sharing platforms. Tour. Manag. 87:104384. doi: 10.1016/j.tourman.2021.104384
Mamuye, A. L., Yilma, T. M., Abdulwahab, A., Broomhead, S., Zondo, P., Kyeng, M., et al. (2022). Health information exchange policy and standards for digital health systems in africa: a systematic review. PLoS Digit. Health 1:e0000118. doi: 10.1371/journal.pdig.0000118
Martei, Y. M., Mokokwe, L., Ngwako, N., Kebuang, K., Setlhako, D. I., Gabaatlhole, G., et al. (2024). Development, acceptability and usability of culturally appropriate survivor narrative videos for breast cancer treatment in Botswana: a pilot study. BMJ Open 14:e073867. doi: 10.1136/bmjopen-2023-073867
Masiano, S., Machine, E., Mphande, M., Markham, C., Tembo, T., Chitani, M., et al. (2021). Video-based intervention for improving maternal retention and adherence to HIV treatment: patient perspectives and experiences. Int. J. Environ. Res. Public Health 18:1737. doi: 10.3390/ijerph18041737
Mbanda, N., Dada, S., Bastable, K., Ingalill, G. B., and Ralf, W. S. (2021). A scoping review of the use of visual aids in health education materials for persons with low-literacy levels. Patient Educ. Couns. 104, 998–1017. doi: 10.1016/j.pec.2020.11.034
Media GH. (2024). Our Videos. Available online at: https://globalhealthmedia.org/about-us/ (Accessed October 14, 2024).
Mengistu, B., Alemu, H., Kassa, M., Zelalem, M., Abate, M., Bitewulign, B., et al. (2021). An innovative intervention to improve respectful maternity care in three districts in Ethiopia. BMC Pregnancy Childbirth 21:541. doi: 10.1186/s12884-021-03934-y
Mondal, H., and Mondal, S. (2025). Adopting augmented reality and virtual reality in medical education in resource-limited settings: constraints and the way forward. Adv. Physiol. Educ. 49, 503–507. doi: 10.1152/advan.00027.2025
Mwase, C., Nkhoma, K., and Allsop, M. J. (2022). The role of digital health in palliative care for people living with HIV in sub-Saharan Africa: a systematic review. Digit. Health 8:205520762211337. doi: 10.1177/20552076221133707
Naderyanfar, F., Shahrakimoghadam, E., Heidari, M. A., and Soleimani, M. (2019). Evaluation of the effect of video-based education on self-care of patients with type II diabetes. J. Diabetes Nurs. 7, 672–682.
Neuwirth, L. S., and Ros, M. (2021). Comparisons between first person point-of-view 180° video virtual reality head-mounted display and 3D video computer display in teaching undergraduate neuroscience students stereotaxic surgeries. Front. Virtual Real. 2:706653. doi: 10.3389/frvir.2021.706653
Obasola, O. (2021). Experiences of health care providers using information and communications technology for maternal and child health care in selected health facilities in Nigeria. Libr. Philos. Pract. 2021, 1–22.
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. doi: 10.1136/bmj.n71
Ploderer, B., Rezaei Aghdam, A., and Burns, K. (2022). Patient-generated health photos and videos across health and well-being contexts: scoping review. J. Med. Internet Res. 24:e28867. doi: 10.2196/28867
Plus, M. (2024). Trusted health information for you. Available online at: https://medlineplus.gov/anatomyvideos.html (Accessed August 7, 2024).
Robert, H, Fernando, S, Kishanthini,, Tan, E, Jin, Y, Moe, S, et al. (2023). Effectiveness of video-based learning on students' memory: a randomized controlled trial.
Scott, S., Camara, B. S., Hill, M., Lama, E. K., Barry, L., Ogouyemi-Hounto, A., et al. (2022). The use of video job-aids to improve the quality of seasonal malaria chemoprevention delivery. PLoS Digit. Health 1:e0000165. doi: 10.1371/journal.pdig.0000165
Snelson, C. (2018). Video production in content-area pedagogy: a scoping study of the research literature. Learn. Media Technol. 43, 294–306. doi: 10.1080/17439884.2018.1504788
Sorathia, K., Sharma, K., Bhowmick, S., and Kamidi, P. (2017). “Pragati - a mobile based virtual reality (VR) platform to train and educate community health workers” in Human-computer interaction – INTERACT 2017 (Cham: Springer International Publishing).
Tan, H., Zhang, X., and Yang, Y. (2023). Satisfaction or gratitude? Exploring the disparate effects of physicians' knowledge sharing on patients' service evaluation in online medical consultations. Inf. Syst. J. 33, 1186–1211. doi: 10.1111/isj.12440
Till, S., Mkhize, M., Farao, J., Shandu, L. D., Muthelo, L., Coleman, T. L., et al. (2023). Digital health Technologies for Maternal and Child Health in Africa and other low- and middle-income countries: cross-disciplinary scoping review with stakeholder consultation. J. Med. Internet Res. 25:e42161. doi: 10.2196/42161
Tilly, A. E., Ellis, G. K., Chen, J. S., Manda, A., Salima, A., Mtangwanika, A., et al. (2022). Implementation and evaluation of educational videos to improve Cancer knowledge and patient empowerment. JCO Glob. Oncol. 8:e2100315. doi: 10.1200/GO.21.00315
UN. (2024). UN list of developed countries. Available online at: https://unctad.org/topic/least-developed-countries/list (Accessed October 8, 2024).
Wang, L., Wu, T., Guo, X., Zhang, X., Li, Y., and Wang, W. (2018). Exploring mHealth monitoring service acceptance from a service characteristics perspective. Electron. Commer. Res. Appl. 30, 159–168. doi: 10.1016/j.elerap.2018.06.003
WHO. (2021). Global strategy on digital health. Available online at: https://www.who.int/docs/default-source/documents/gs4dhdaa2a9f352b0445bafbc79ca799dce4d.pdf (Accessed July 25, 2024).
WHO. (2023). Vision, strategy and special initiatives, 2023–2030. Available online at: https://www.afro.who.int/sites/default/files/2023-09/Ending%20disease%20in%20Africa_ENDISA_ENG_0.pdf (Accessed July 31, 2024).
WHO. (2024). WHO compendium of innovative health technologies for low-resource settings Available online at: https://iris.who.int/bitstream/handle/10665/378235/9789240095212-eng.pdf?sequence=1 (Accessed July 25, 2024).
WHO. (2024). Tactics to apply to make your communications understandable: Make it visual. Available online at: https://www.who.int/about/communications/understandable/visuals.
Yang, Q., Wu, Z., Xie, Y., Xiao, X., Wu, J., Sang, T., et al. (2021). The impact of health education videos on general public’s mental health and behavior during COVID-19. Glob. Health Res. Policy 6:37. doi: 10.1186/s41256-021-00211-5
Yang, Y., Zhu, X., Song, R., Zhang, X., and Guo, F. (2021). Not just for the money? An examination of the motives behind physicians’ sharing of paid health information. J. Inf. Sci. 49:016555152199102. doi: 10.1177/0165551521991029
Zhang, X., Guo, X., Guo, F., and Lai, K. H. (2014). Nonlinearities in personalization-privacy paradox in mHealth adoption: the mediating role of perceived usefulness and attitude. Technol. Health Care 22, 515–529. doi: 10.3233/THC-140811
Zhang, X., Lai, K.-h., and Guo, X. (2017). Promoting China's mHealth market: a policy perspective. Health Policy Technol. 6, 383–388. doi: 10.1016/j.hlpt.2017.11.002
Keywords: VbHE, digital health, health education, educational video, African context
Citation: Impito PF and Azevedo J (2025) Assessing video-based health education in African contexts: a systematic review. Front. Commun. 10:1545306. doi: 10.3389/fcomm.2025.1545306
Edited by:
Xiaofei Zhang, Nankai University, ChinaReviewed by:
Lorenz S. Neuwirth, State University of New York at Old Westbury, United StatesShanshan Zhao, Capital Medical University, China
Panan Pichayapinyo, Mahidol University—Phayathai Campus, Thailand
Copyright © 2025 Impito and Azevedo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pinto Francisco Impito, cGludG9mcmFuY3NAZ21haWwuY29t