 Till Neuhaus1*
Till Neuhaus1* Friederike Gödecke2
Friederike Gödecke2- 1Faculty of Education, Bielefeld University, Bielefeld, Germany
- 2Independent Researcher, Bielefeld, Germany
The following article attempts to identify strategies, settings, and conditions which help children and adolescents with fetal alcohol spectrum disorder (FASD) to successfully attend educational institutions/ schools. FASD must be considered a profound and extensive disability which is the result of exposition of the unborn child to alcohol during pregnancy. The existing literature addressing FASD and schooling is comparatively sparse, therefore the following article attempts to generate insights based on expert interviews. In the course of the analysis, three themes – (1) improving teacher knowledge about FASD, (2) allowing for higher degrees of individualization within schooling, and (3) helping children and adolescents with FASD by partly externalizing structures and decisions – could be identified. Each of the themes will be sketched out and the specific findings will be compared to already existing research.
1 FASD and school – Introduction
Fetal alcohol spectrum disorder (FASD) is considered prenatal damage caused by exposition of the unborn child to alcohol (cf. Schmidt et al., 2016, p. 15). Due to the influence of further factors on the child's development during pregnancy – such as, but not limited to, genetic predisposition, length and intensity of alcohol exposure, additional lifestyle factors (cf. Kalberg and Buckley, 2007, p. 278/279) – FASD does not represent a fixed set of symptoms but, as the name suggests, a spectrum of potential impairments (cf. Betts et al., 2022). In addition, many of the impairments, which can be attributed to FASD, are not exclusively attributable to prenatal alcohol exposure alone but can also be found in alternative disorders (Andreu-Fernández et al., 2024). In that line of thought (Astley 2013, p. 417) concludes that “[i]ndividuals with prenatal alcohol exposure present with a wide range of outcomes, most of which are not specific to prenatal alcohol exposure and often manifest differently across the lifespan.” Despite the high degree of idiosyncrasy within the (sub-)population(s) of FASD affected people, attempts have been made to differentiate the spectrum (exemplarily, Hoyme et al., 2016). For example, Green et al. (2009, p. 688) propose the following division:
“FAS represents only a fraction (10–15%) of the children affected by prenatal exposure to alcohol, as it is more common for children to present with complex behavioral and neurological dysfunction related to their exposure, but in the absence some or all of the characteristic facial features. In these situations, the diagnostic terms partial FAS (pFAS) and alcohol-related neurodevelopmental disorder (ARND) have been used to describe individuals who do not meet all of the criteria for FAS.”
Regardless of the chosen division of the spectrum (for a refinement of the spectrum, see Coriale et al., 2013, p. 362), it can be stated that the affected children and adolescents—depending on the individual severity of the syndrome—are affected by cognitive, behavioral and, in more severe cases, physical impairments (cf. Gödecke and Neuhaus, 2024, p. 33). These impairments include behavioral problems—i.e. attention deficits, social behavior disorders, poor academic performance and poor social judgment (cf. Tsang et al., 2016, p. 2)—deficits in executive functions (cf. Green et al., 2009, p. 688), emotional dysregulation, memory problems, attention deficits, psychopathologies as well as secondary disabilities arising from interactions with their environment (cf. Coriale et al., 2013, p. 360; see also Andreu-Fernández et al., 2024). Additionally, physical and/or facial changes can be observed, at least in sub-populations of FASD-affected persons (cf. Landgraf and Hoff, 2018, p. 47/48; Blanck-Lubarsch et al., 2023). Further, studies suggest that the “group level cognitive profile in FASD [is] characterized by poor intelligence or intellectual functioning” (Kerdreux et al., 2024, p. 1109), so that those affected can exhibit IQ scores in the range of 55 to approximately 70 (cf. Juretko, 2007, p. 31; Spohr, 2014, p. 185; Kerdreux et al., 2024).
Due to dynamics of stigmatization (Roozen et al., 2022) but also the multifacetedness of the disorder (Ehrig et al., 2023), “many children with FAS and other FASD are neither detected nor referred for a diagnosis” (May et al., 2006, p. 1563)—a circumstance that has earned FASD the designation of a “hidden disability” (Tortorelli et al., 2023; Gibbs, 2025). As already stated, one central reasons for this dynamic may be the varied presentation of FASD which can complicate the diagnostic process (Ehrig et al., 2023), foster misdiagnosis (Burd, 2016, p. 325; Schlachtberger, 2020, p. 26), and ultimately result in ineffective therapy (Gödecke and Neuhaus, 2024, p. 33). Regarding an exemplary case, Dunbar Winsor (2021, p. 14) has outlined the difficulties of diagnosing FASD as following:
“Due to the differences or absence of physiological symptoms, the delay in noticing an issue among babies born exposed to alcohol vs. those exposed to drug use can result in years of passing before there is the detection of a child's behaviors or disclosure of alcohol use by the mother known or assessed.”
Even regarding the relatively standardized and well measurable metric of IQ-scores, the group of FASD affected people exhibits a relatively low degree of coherency as “[c]hildren with FASD showed a wide range of total IQ values, from moderate degree of mental retardation to very high intelligence” (Fadeeva and Nenasteva, 2022, p. 421). Such findings are supported by further studies suggesting that on average a decrease in cognitive ability can be observed in people affected by FASD while also acknowledging that sub-populations also feature regular or above average IQ-scores (Spohr, 2014, p. 151, see also Branton et al., 2022).
The characterization as an invisible disability becomes more comprehensible when looking at the available figures, as “[a]ll levels of FASD may affect 2–5%” (May et al., 2013, p. 503) of all newborns, making FASD the most common cause of non-genetic childhood malformations (Feldmann et al., 2007, p. 854/855). Consulting more recent statistics, Jacobsen et al. (2022, p. 297) cite the following numbers: “The estimated prevalence of an FASD diagnosis among minors in Europe is the highest in the world, with 19.8 per 1,000 population, whereas the global prevalence is 7.7 per 1,000” (cf. also Lange et al., 2017)1. However, “[a]s there is limited information available on the prevalence of FASD in many countries, the global prevalence rate may be significantly higher” (Brown et al., 2019, p. 169). For the specific case of Germany, it is estimated that roughly 2% of all newborns can be situated on the FASD spectrum (Zink, 2025a,b). At the same time, less than 2% of all newborn children in Germany are diagnosed with FASD which suggests that the diagnosis is underrepresented (cf. Landgraf et al., 2014, p. 903; Zink, 2025a). In absolute numbers, it is estimated that roughly 800,000 Germans can be placed on the FASD spectrum; of these 800,000 affected persons, 130,000 can be assigned to the category of children (Schecke, 2021). In a 2023 press release, Germany's Federal Center for Health Education (German: Bundeszentral für gesundheitliche Aufklärung, short BzgA) argues that each year 10,000 children, which fulfill the diagnostic criteria for FASD, are born (BzGA, 2023). Despite its numerical relevance (cf. also Feldmann et al., 2007, p. 854–855), FASD should and must still be considered a lesser known disorder even in the medical profession. As such, the number of undiagnosed or falsely diagnosed cases—subsumed under the umbrella term of undetected cases—can be estimated to be relatively high (Jewell et al., 2024), so that the absolute numbers of affected people are likely higher than the values cited in the available statistics (cf. Landgraf and Hoff, 2018, p. 24; Zink, 2025b).
The school environment seems to be of particular importance for children and adolescents with FASD. On the one hand, the diverse physical, cognitive and social impairments resulting from FASD are often only discovered and become relevant at school age (cf. Gödecke and Neuhaus, 2025), and on the other hand, schools do not seem to be particularly well adapted to the needs of this group of students (Neuhaus and Gödecke, 2024). The lack of adaption toward the needs of students affected by FASD can result—in a complex interplay with further factors and dynamics—in adverse outcomes, such as “a disrupted school experience and impacted academic achievement” (Lees et al., 2022, p. 797; Becker and Hantelmann, 2013). Taking these tentative observations seriously, children and adolescents affected by FASD can be considered a group that could certainly benefit from increased or more targeted inclusion-oriented efforts (cf. Neuhaus and Gödecke, 2024, n.p.). However, a lack of tried and tested educational strategies can be asserted and affected children and adolescents are therefore—referencing the sparse results of research on the issue for the German context—often taught at special schools with a focus on learning disability [German: Sonderschule Lernen] or intellectual impairment [German: Sonderschule Geistige Entwicklung] (cf. Minke, 2009). The lack of available strategies also manifests itself when looking at the available research: Duquette and Parr (2022), for example, were only able to identify eight studies globally that address the nexus of FASD and successful schooling as part of a scoping review; Neuhaus and Gödecke (2024) were able to identify 17 contributions in their scoping review on the same topic. In short: FASD and educational support strategies appears to be an under-researched and yet—given the number of learners affected as well as the impact the disorder can exert on people's lives—highly relevant complex of topics. Simultaneously, the nexus between FASD and educational support strategies seems to be under-researched but also under-represented in the academic discourse, despite clearly falling into the larger framework of inclusive education (Gödecke and Neuhaus, 2024, p. 41).
This article aims to partially address this lack of pedagogical strategies and support options by presenting results from expert interviews. This approach has been selected as a vast range of practical experience and expertise—for example practical experiences and professional observations in specialized institutions, care and support arrangements, etc.—could be retrieved by addressing professionals working in these fields and institutions. It is the aim of this study to excavate this highly specialized expert knowledge by conducting expert interviews (cf. Gläser and Laudel, 2010, p. 12). The research question guiding this endeavor is the following: which strategies, settings, measures and scenarios are conducive to supporting children and adolescents with FASD in the context of schooling and education? In order approximate this goal and answer the research question, this article follows the following structure: firstly, the method of the expert interview will be presented and reflected upon regarding its feasibility for this paper's aim; additionally, the process of data collection is sketched out and the data corpus will be described (Section 2). Following, the generated finding will be presented (Section 3) as well as linked to the existing state of research. The article concludes with a reflection of its limitations and shortcomings (section 4) as well as a summary of key findings and an outlook on worthwhile future research (section 5).
2 Method, sample, and analysis
2.1 Method—expert interviews
Regarding expert interview, it should be noted that this method can only be considered a scantly standardized method, which is primarily employed for exploratory purposes (cf. Meuser and Nagel, 2009, p. 465). As such, the expert interview can be pre-structured to varying degrees, conducted in different ways, and evaluated and interpreted divergently depending on the research interest and research question of the endeavor (cf. Bogner and Menz, 2002, p. 34). Despite the limited degree of standardization, expert interviews can be roughly divided into three categories:
(1) The exploratory expert interview, which aims to structure the field of investigation thematically and generate hypotheses (cf. Bogner and Menz, 2009, p. 64)
(2) The systematizing interview, in which holders of exclusive knowledge share their knowledge in order to answer questions for which there are no publications to date (cf. Meyen et al., 2011, p. 61/62)
(3) The theory-generating expert interview.
With regard to the subject matter discussed in this article as well as the associated research question—which pedagogical strategies or changes in setting are necessary in order to enable students with FASD to successfully learn in schools?—it can be stated that the following expert interviews should be understood as systematizing interview. As such, the expert interview is employed as an instrument of data collection that is related to a specific mode of knowledge, namely expert knowledge (cf. Meuser and Nagel, 2009, p. 466), which is then used to address and fill a gap in the current research landscape. As already hinted at in the introduction, the scoping reviews conducted by Duquette and Parr (2022) and Neuhaus and Gödecke (2024) were only able to identify eight and 17 relevant publications respectively.
Central to the method of an expert interview is the question of who is to be considered an expert and whose expertise is considered instructive for which subject area. In this regard, it can be stated that an expert is a person who possesses detailed and specialized knowledge (cf. Schütz, 1972). However, in order to support this definition, a clearly limited frame of reference must exist, which the expert is also aware of when making statements about his or her areas of knowledge (cf. Wassermann, 2015, p. 52). Taking these insights seriously, expertise must therefore be regarded as a domain- and context-specific phenomenon. The type of expertise or special knowledge (cf. Sprondel, 1979, p. 141) discussed here is usually acquired through activities in the relevant field, may it be professional or otherwise. Experts are therefore people who are active in a certain field, “regardless of their position in the social status system” (Gorden, 1975, p. 199). There are diverging answers regarding the length of time, which is required to acquire highly specialized expert knowledge and thereby to be considered an expert in a given field. For example, Chase and Simon (1973) cite the 10,000 h rule (see also Ericsson et al., 1993), (Neuhaus 2023, p. 50) speaks of ~10 to 15 years of professional activity and many other publications either do not specify a time frame (cf. Wright and Ayton, 1987) or primarily discuss very small sub-skills (i.e., learning of a single step of a surgical technique), which can of course be mastered in a shorter time (cf. Hetmański, 2018, p. 15). These statements indicate that a central problem in the definition and description of expert knowledge is the scope of application, which can range from ‘specific' to “global”. Expertise in a very specific domain—i.e. an isolated problem or a single task—is easy to identify, but the more global the expertise becomes, the more difficult it is to distinguish “real” experts from non-experts. Considerations of this kind have led critics to view some fields as so global (e.g., foreign policy, stock markets, etc.) that, strictly speaking, no real expertise can exist in these domains (see Tetlock, 2017).
Lastly, aims and quality of expert interviews should briefly be discussed. The central aim of an expert interview is to generate specialized knowledge that is as objective as possible. However, a central problem with that method is that interviewees—quasi by definition—only report on selective and subjective observations and insights. In other words, expert interview attempts to subsume subjective patterns of interpretation (cf. Ahlrichs, 2012, p. 105), which are then systematized and developed further into knowledge which is as objective as possible. This dynamic—subjective knowledge which is supposed to be the basis for more objective knowledge—is a central reason why, regarding quality assurance, it is considered advisable to interview several experts on an issue as subjective patterns are gradually straightened out by adding further expertise (cf. Wassermann, 2015, p. 55).
2.2 Sample recruitment and construction
With regard to the here discussed subject, the authors adhere to the definition of an expert outlined above, namely people who are/were professionally active or professionally interested in the relevant fields. In order to recruit relevant experts for the interviews, the authors compiled—based on registries, already existing lists of self-aid groups, as well as manual search—a comprehensive list of relevant institutions in Germany (N = 39). These 39 institutions—clinics, pediatric services, care facilities and therapy centers—have in common that they feature a pronounced focus regarding the diagnosis, counseling, treatment and/or therapy of children and adolescents with FASD. Despite this paper's educational focus, schools have not been addressed as we were explicitly searching for professionals with pronounced experiences regarding FASD. Arguably, this kind of experience can only be generated if institution have explicitly focused on the disorder. As to the knowledge of the authors, no specialized school regarding FASD exists in Germany; however, the lack of teacher perspectives is, without a doubt, a limitation of this study and should be addressed in future research endeavors.
These 39 institutions have been addressed via email, in which the authors explained their endeavor and aims—identifying strategies regarding the educational support of children and adolescents affected by FASD—and asked for the expertise of the institution on the matter. In the letter we sent out, the experts were asked to delineate their experience and best practices of how children and adolescents with FASD can be best supported at school. Also, we asked the experts to state their professional background and experience (i.e., years in the profession). The scope of the written response was left up to the expert.
The expertise was supposed to be handed in in written form, again via email. This approach was chosen for three reasons:
1) Firstly, institutions (i.e., therapeutic centers) often times feature a vast array of professionals, such as medical doctors, psychologists, or social workers. Despite working with children and adolescents affected by FASD, not all of these professionals necessarily have insights relevant for this study, namely educational support strategies in the context of schooling. By addressing the institution, the institution is forced to reflect which of its people is best suited to reply, which—in turn—increases the information quality.
2) As these 39 institutions are scattered throughout Germany, it would be extremely time intensive to schedule meetings and conduct in-person interviews; also, an actual interview approach (either live or through video-chat) could result in higher decline rates as interviews collide with work related tasks.
3) The written response also fosters two additional advantages: firstly, interviewees have the chance to deliberately think about their response (in advance but also while writing) and thereby actively and explicitly consult their expert knowledge (Menary, 2007). Further, such an approach allows the interviewees to talk to their colleagues before submitting their answer potentially increasing the expertise while also reducing the subjectivity of the replies. Secondly, a written reply is arguably easier to coordinate with the demands of a regular work day.
Being well aware of the fact that more than 39 institutions work in the field of FASD—yet, without explicitly stating that—, it was also pointed out in the cover letter that it is highly appreciated if the message is forwarded to other experts in the field—an approach known as the “snowball method” (cf. Gabler, 1992).
With regard to the professional background of the interviewees, it can be noted that five experts came from the field of social work, while one further expert each came from the fields of medicine and journalism, the latter having written a book on FASD and also being a parent of a FASD-affected child. Five of the interviewees also stated that they had acquired an additional qualification as an FASD specialist [German: FASD Fachkraft]. On average, the interviewees can look back on 9.75 years of experience regarding working with children and adolescents affected by FASD.
2.3 Analysis
A total of seven written expert opinions were acquired, varying in length and detail. The average length of the expert feedback was 683 words (standard deviation: 392 words). The collected responses were firstly anonymized and subsequently coded and analyzed by the two authors independently (see Mayring, 2019), the categories of analysis have been created inductively. The aim of the analysis was the establishment of themes, which were supposed to highlight different facets of educational support strategies for children and adolescents affected by FASD—ergo a context-focused analysis (Schreier, 2014, n.p.). After the first round of coding, the authors compared their themes and resolved coding conflicts by collaboratively discussing the scope and breath of the themes. Exemplary interview responses alongside the developed category are provided in the Table 1 below.
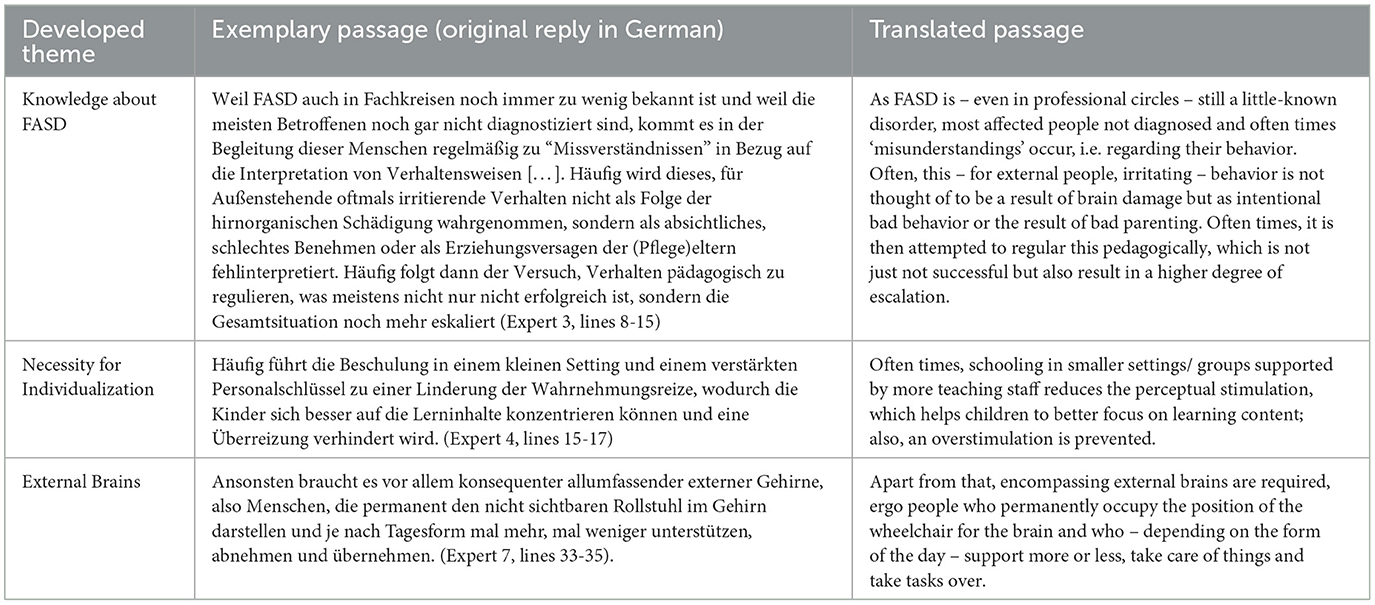
Table 1. Examples for coded segments and the codes developed out of them.
This step of the analysis—the content-focused coding (cf. Schreier, 2014)—was chosen with reference to Bogner et al. (2014, p. 73) as this study's aim is to uncover causal dependencies through the systematic analysis and comparison of the information provided by the experts; it is therefore primarily an evaluation for informational purposes and less about advancing theoretical considerations or concepts. Bogner et al. (2014, p. 72/73) therefore recommend the content analysis method for expert interviews such as the one conducted in this study. In the following sections, the categories generated are presented and key findings regarding the educational support of children and adolescents with FASD are presented.
3 Findings
The analysis identified three overarching themes—(1) knowledge about FASD, (2) the necessity for individualization and (3) External Brains—which are outlined below. Each topic consists of an extensive number of individual sub-aspects, which interact and/ or occur together. In this regard, it should be noted that topic 1 (knowledge about FASD) permeates several aspects and domains of schooling (diagnostics, school administration, pedagogical action, etc.), whereas topics 2 and 3 tend to be located within the school (classroom, breaks, etc.). In the following, an attempt will be made to identify the modes of action and dynamics addressed by the experts (section 3.1., 3.2., and 3.3.), as well as to compare these findings with existing findings (section 3.4.).
3.1 Knowledge about FASD
The first topic addressed by the experts deals with knowledge of and knowledge about the disorder FASD. This point represents the basis for addressing the successful schooling of children and adolescents with FASD and, as will be shown below, permeates various areas of school.
The lack of knowledge regarding FASD commences with special needs assessment procedures (German: AO-SF Verfahren), in which—according to the experts' experience—too much attention is paid to the intelligence/ IQ scores (Neuhaus, 2025) while simultaneously neglecting other diagnostic parameters, such executive functions. One result of the current approach is that children and young people with FASD are assessed but FASD is not actively considered a possibility. As such, these children and adolescents are subsequently educated in settings in which their needs cannot be met accordingly. One reason for this could be the primacy of special educators within such assessment procedures in the German context (Vogt and Neuhaus, forthcoming) (cf. Gasterstädt et al., 2021; cf. Vogt and Neuhaus, 2023; Debè et al., 2024), in which special educators can use various tests and diagnostic tools, yet these results are often subordinated to intelligence tests (Kottmann, 2006, p. 150; Neuhaus, 2025; Neuhaus and Vogt, 2025). “However, the intelligence quotient cannot be the sole indicator of what a person with FASD can achieve, as they cannot use it in many areas of life due to the damage to their executive functions” (ExInt42, lines 16–18). In addition, there is the observation that “even special education teachers are not familiar with the FASD issue” (ExInt1, line 96) and that FASD seems to be little present in teacher training (at university as well as in practical teacher training) and practice. Therefore, FASD is little known “even among teachers at special schools” (ExInt1, line 73). Another factor regarding the placement of children and adolescents with FASD appears to be the school administration's perspective as, according to the experts' assessment, German school authorities have the task of “promoting the idea of inclusion” (ExInt1, line 65) by less frequently removing pupils from mainstream school settings3. This administrative hesitancy—often caused by the fact that children and adolescents with FASD do not fall into clearly predefined administrative categories4—often results in a lack of support for and excessive demands toward the subgroup of those affected by FASD.
In addition to aspects of diagnosis and placement, knowledge of and about FASD is also—at least, according to the illustrations of the consulted experts—required in other education-related areas. On the one hand, knowledge about FASD helps at selecting and reflecting on educational support concepts, because when “what looks like a behavioral problem is actually an organic brain/neurological problem and that this cannot be solved with classical pedagogy, then this insight is the real game changer because it enables a different attitude” (ExInt3, lines 24–27). The change in attitude described here includes, for example, not taking undesirable behavior personally but rather interpreting misbehavior and strange social behavior as “overstrain and stress reactions to environmental conditions” (ExInt3, line 32). Reframing student behavior in such a fashion allows for “always being ready to make a new start” (ExInt3, line 76). Another game changer is the insight “to say goodbye to the concept of neurotypical ‘learning', ‘development' and ‘support”' (ExInt7, lines 18/19) and to engage with the idiosyncrasies of the pupil. On the other hand, knowledge about FASD also raises awareness for the student's (familial) history, because—as one expert states—“children who receive an FASD diagnosis have usually also had traumatic (early) childhood experiences” (ExInt6, line 47/48). In addition to traumatic early childhood experiences, it must also be considered that children and adolescents with FASD have generally had comparatively few positive experiences at school and therefore this place is often times associated with “anxiety and excessive demands” (ExInt5, line 3)—feelings of failure and truancy often seem to be observable patterns that result from this emotional state (cf. ExInt5, lines 3–8). The previous experiences, traumas and emotional states briefly outlined here must also be considered when working with children and adolescents with FASD; an endeavor that can only succeed if teachers, school counselors, social workers and others are fundamentally informed about the disorder (cf. ExInt6, lines 52–54).
3.2 The necessity for individualization
Following the more general observations from section 3.1, the second theme—the necessity for individualization—focuses on support options and strategies that can primarily be implemented in the classroom.
The experts identified the insight that the developmental age or stage of the child/ adolescent must be the primary point of reference for pedagogical endeavors (cf. e.g. ExInt6, line 45). This includes, above all, the (didactical) reduction of the subject matter into “smaller[...], more manageable chunks” (ExInt6, line 14), which should not only be worked on in small steps but also repeated frequently (cf. ExInt3, line 75), so that experiences of successful learning can be experienced (cf. ExInt5, line 8). As stated earlier, this student population is starved for positive experiences regarding school and learning, therefore this point cannot be stressed enough. The mantra referenced by several experts is “support instead of demand” and “strengthen strengths” (expressed particularly succinctly in ExInt6, lines 44–45). This can manifest itself, for example, in subjects such as music, arts, or sport being given more time and/or a higher priority (cf. ExInt6, line 42). The recalibration of educational contents and goals indicated here also goes hand in hand with a departure from existing goals and norms. For example, the experts argue that the schooling of children and adolescents with FASD should be based on “realistic expectations” (ExInt3, line 71) and should primarily aim to prepare this group of children and young people “as well as possible for their lives”; however, outside of “performance contexts” (ExInt5, line 6/7), primarily to reduce stress and pressure. Expert 7 outlines this particularly pointedly: “Away from laboriously achieved (regular) school qualifications5 toward radical reduction” (line 21). Due to the situation outlined so far, the interviewed experts recommend various alternative school models or concepts that can at least partially cater toward this degree of freedom. Montessori and Waldorf schools, home schooling and special schools were mentioned.
Moving away from the usual distribution of subjects or lessons and traditional educational goals (usually: educational qualifications) and the subsequent upgrading of subjects such as arts, music, or sport would also support the second aspect identified by the experts. For example, five out of seven experts were in favor of restructuring the school day by shortening learning intervals and increasing the number of breaks and physical activity (cf. ExInt5, line 11). For example, “frequent alternation (sometimes every 15 min) of concentration phases [...] and activity units” are suggested in order to enable children and adolescents to attend school successfully despite their “severely limited ability to concentrate” (ExInt3, line 55–57; cf. also ExInt6, line 39). In addition, the experts recommend “reducing school time to half days6” (ExInt3, line 58) to prevent excessive exhaustion. Homework should also be avoided “as the effort of a school day is completely sufficient” and “regeneration at home [...] is urgently needed” (ExInt5, line 13/14). In the case of overstimulation or overstressing a child/ young person, the experts observed that this not only has a negative effect on the child/ young person themselves (e.g. “high feeling of frustration”, ExInt4, line 27), but also manifests itself in “escalating behavior in the afternoon” (ExInt4, line 26) and would thus put additional strain on family life.
In addition to the enormous stress that a regular school day represents for children and adolescents with FASD, reference was also made to ways of limiting visual and sensory impressions, as the group discussed here often seems to have problems regulating sensory impressions (cf. ExInt6, line 20). Potential aids promising relief and being mentioned by the experts include noise canceling headphones, fidget toys, spatial separation (e.g., through movable partitions) and small classes (~4–5 children) (cf. ExInt3, line 10; ExInt4, line 16; ExInt6, lines 19–23). The aspect of focusing and processing visual stimuli was also raised with regard to the learning and teaching materials being used. In this regard, it was recommended that worksheets and other materials work with focusing aids and otherwise contain little distracting content (cf. ExInt4, line 49). The topics of reduction and individualization were also addressed in a second block, namely that of language/ instruction. Here, the experts explicitly point out to use “simple, clear language” (ExInt3, line 76), which is characterized by “short sentences, no negations” and uniformity (ExInt6, 16/17). Similarly, abstract language—metaphors, complex grammatical structures, hypothetical cases etc.—should be avoided.
3.3 External brains
The third topic identified in the experts' responses can be subsumed under the heading of externalization of (cerebral) structures. This means that children and adolescents with FASD need “all-encompassing[...] external[...] brains”, “i.e. people who permanently represent the invisible wheelchair in the brain and, depending on the demands of the day, support sometimes more, sometimes less support […]” (ExInt7, line 33–36). This seems to be particularly the case in “unstructured situations such as breaks and transitions” (ibid.). It should also be noted that these external brains do not necessarily have to be people, but can also be represented by structures, processes and non-personal aids. With their comments on external brains, the experts implicitly refer to the phenomenon of “transactive memory” (Wegner, 1987, p. 186). Transactive memory describe processes of memorization that lie between individuals (i.e., a couple managing its morning routines where each partner covers his/ her share; however, the actions result is a shared aim) and, in the case of children and adolescents with FASD, tend to be carried more by one side. Gladwell (2000) expanded the model of transactive memory to include the factor of structures and material aspects—a memory (i.e., of a process) can also be located between individuals and objects or structures (i.e., a coffee machine requiring certain motor actions which then become my standard morning routine with that machine; these processes/ habits remain invisible until something, i.e., my coffee machine, changes, for example a model requiring a different pattern).
For children and adolescents with FASD, the experts recommend a series of externalization strategies of these cerebral structures in order to enable a successful school day. For example, they recommend using “visual[...] aids such as timetables, diagrams and visual reminders” (ExInt6, line 15) for work phases or lessons. Timetables “with clear expectations” were identified as particularly helpful (ExInt6, line 26). However, the externalization of cerebral structures does not end with individual (learning) phases, but extends virtually throughout the entire (school) day. It was increasingly pointed out that “routines and structures” provide people with FASD security (ExInt6, line 24) and that these “stable everyday routines” are needed because “processes and rules [are] not internalized” and security must therefore be provided by external structures (ExInt 3, line 69/70). On the one hand, this includes a structured and, if possible, consistent daily routine, which should also be visualized (cf. ExInt3, line 74); on the other hand, children and adolescents with FASD need “clear rules” from which there should be no (or only very little) exceptions (ExInt3, line 68).
In addition to these structural measures, it is also recommended that children and adolescents with FASD are supported by special needs assistant7 (cf. ExInt3, line 63; ExInt4, 36; ExInt6, 40), who can provide relief in confusing situations and create structure when needed. With regard to cooperation with other professions (e.g., school support staff, social workers, teachers etc.), the point of networking is also emphasized, with a particular focus on coherence (cf. ExInt6, 30–32). This means that those involved should exchange strategies and, if possible, use the same or similar strategies in different settings (i.e., during school and outside of it) with the aim of creating a high degree of coherence for the child or adolescent and thus reducing complexity. In summary, it can be stated that the aspects discussed here can primarily be subsumed under the label of “reduction of complexity and ambiguity”. Children and young people with FASD should be able to fall back on transparent expectations regarding their behavior, activities, and goals at all times through visually available support, repetitive routines, and further externalized structures.
3.4 Comparison with existing research on FASD and schooling
Comparing the results outlined above with previous research findings, it can be observed that these appear to be quite compatible, yet the degree of resolution/detailedness is highly relevant.
For example, the first overarching theme (knowledge about FASD) has already been discussed in various places in research (cf. Millar et al., 2017; Opini, 2019, p. 78), so that Riggie and Xu (2013, p. 61/62), for example, state that “[a]dolescents with FASD have identified their best teachers as those who are knowledgeable about the disability and its impacts on learning and behavior”. The advantages of teacher knowledge about FASD listed in previous research include the aspects of relationship work (Neuhaus and Gödecke, 2024; Gödecke and Neuhaus, 2025), adjustment of expectations (cf. Mitašíková and Vodičková, 2022), a more holistic view of the student and their problems (cf. Poth et al., 2014, p. 254), and the focus on individualized strengths and weaknesses profiles. The latter often goes hand in hand with a detachment from institutional goals (cf. Duquette and Parr, 2022). Generally speaking, the first theme cannot just be supported by partial evidence from research on FASD and schooling but also, more generally, by insights generated in the field of neurodiversity and education (cf. Zahir et al., 2024; Dwyer, 2022). However, the study presented here was able to identify a German specificity with regard to (mis)diagnosis in special needs assessment procedures. In addition, it was also shown that a lack of knowledge regarding FASD is not only problematic for teachers, but can also have a counterproductive effect in (school) administrative contexts.
The results that were subsumed under the second topic (the necessity for individualization) can also be characterized as being applicable. For example, the reduction of teaching pace was advocated in various places (cf. Millians, 2015; Edmonds and Crichton, 2008); the same applies to shorter intervals of work and breaks as well as the expansion of movement components (cf. Millar et al., 2017). There are also recommendations to reduce class size (cf. Edmonds and Crichton, 2008), to limit sensory impressions (cf. Basaraba, 2016, p. 245), to use visual reminders and to keep the degree of ambiguity in verbal communication low (cf. Swart, 2012). A decidedly new aspect of the study presented here is the stress factor and the importance of regeneration at home, which can inform pedagogical action, for example by not assigning homework. Again, just as with the result subsumed under the first theme, the findings exhibit a pronounced similarity to findings from the field of neurodiversity research in the context of schooling.
With regard to the third topic (externalization of (cerebral) structures), it should be noted that the relevant research primarily points to the use of routines and rituals in everyday school life (cf. Van Schalkwyk and Marais, 2017; Duquette and Parr, 2022) in order to provide a high degree of external structure (cf. Basaraba, 2016, p. 228). The study presented here was able to confirm this and extends the previous findings by referring to interprofessional collaboration with the aim of creating coherence for children and adolescents with FASD beyond school boundaries.
In summary, it can therefore be stated that this study is in line with existing research, whereby selective extensions and refinements of results could be generated. Furthermore, the added value of this study is constituted by the transfer of previous insights to the German context with its national characteristics, exemplified in the context of special needs assessments, diagnostics, or school administrative contexts.
4 Limitations of the study and outlook on future research
Regarding the here presented study, certain limitations and weakness need to be discussed. Specifically, two aspects—one methodological and one conceptual—seem to require an in-depth reflection, namely the sample size and sample construction as well as the debate to what extent FASD can be integrated into the larger research frame of neurodiversity.
Regarding the sample size and sample construction, the following limitations, which in turn also affect the generalizability of the findings, can be observed:
- Despite having attempted to address all relevant institutions regarding diagnosis, counseling, and therapy in the field of FASD (N = 39), it still needs to be considered that the amount of participating institutions (N = 7) is relatively limited. Even though expert interviews operate on different grounds than other forms of interviews, the findings of this study—due to the limited sample size—should rather be understood as the result of a pilot endeavor which may guide future research with a larger sample size.
- Again, regarding the constitution of the sample and also limiting the generalizability of the findings, it should also be pointed out that the sample favored certain professions and backgrounds over others. While this may be explained due to inner-organizational responsibilities of the addressed institutions and the underlying design of the study, it can still be asserted that the perspective of social workers on the issue is overrepresented while other professions and backgrounds—such as, but not limited to, teachers, special educators, school counselors, school and/or educational psychologists, and parents—is left out. Future research should address this lack of diverse voices by actively recruiting interviewees from different fields of occupation.
Lastly, a conceptual remark should be pointed out. By taking a closer look at the findings of this study, it can be observed that a tremendous degree of the identified strategies dovetails with findings from the field of neurodiversity research in the context of schooling. Therefore, future research should explore to what extent the two fields overlap and to which degree already tried and tested strategies from one field could be transferred to the other. As pointed out, the last point is less of limitation of the here presented study but rather a point of reflection for future endeavors.
5 Summary of results and outlook
The aim of this article was to identify strategies, settings, procedures and/or measures that are conducive to the successful schooling of children and adolescents with FASD. As was shown at the outset, this is a group that, on the one hand, stands out from their peers due to their special needs profile and, on the other hand, this group has so far been treated—both in research and in (teaching) practice—as a subordinate group and would therefore benefit from more dedicated efforts. In order to approach this goal, expert interviews were conducted. The analysis of the experts' statements culminated in three main topics—knowledge about FASD, the need for expanded individualization and the externalization of decision processes—whose exact modes of action and factual connections are presented in more detail in sections 3.1., 3.2. and 3.3. and compared to existing research results in section 3.4.
As briefly discussed in the sections on limitations, future research should attempt to recruit and capture more and more diverse voices on the issues. Of particular interest could be the perspectives FASD-experienced teachers, school psychologists and counselors, parents, FASD-affected children and adolescents, as well as special educators.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
TN: Conceptualization, Investigation, Writing – review & editing, Writing – original draft, Data curation, Methodology. FG: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Data curation, Investigation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^The fact that Europe spearheads the numerical distribution can largely be attributed to the lack of reliable large-scale studies in other parts of the world. And while Europe's prevalence for FASD is cited with 19.8 per 1000, individual studies suggest much higher baselines in other parts of the world (i.e. 80.2 per 1000 in South Africa, cf. Louw et al., 2024).
2. ^The experts' responded in German and the authors of this paper then translated the replies.
3. ^Germany differentiates between the regular and the special school system. In order to be transferred to the special education system, an administratively organized assessment procedure must be conducted. The special school sector has – despite featuring smaller class sizes – usually been associated with a lack of opportunities as children graduating special schools only receive a diploma which qualifies for no further activities or trainings (cf. Neuhaus, 2025). Simultaneously, the degree of support a child can receive in a regular schooling setting is often times limited, especially when assigned to the administrative category of ‘learning disability'. For many observers, Germany's progress regarding inclusion is mainly dependent on the statistics regarding regular and special schooling (cf. Eckert, 2021; author 2025).
4. ^In the educational context, Germany differentiates between seven disability categories (German: Sonderpädagogische Förderschwerpunkte), which are administrative in nature. The categories are the following: (1) Learning, (2) social and emotional development, (3) seeing, (4) hearing, (5) speech, (6) physical development and motor skills, and (7) cognitive development.
5. ^Germany basically features three regular schooling degrees: Hauptschulabschluss (usually achieved after grade 9), Realschulabschluss (after grade 10), and Abitur (after 12 or 13 years of education), the latter being the standard requirement for entering university. Children who are operating outside this structure – i.e. being in the special education track – only receive a school certificate which comes with no further educational options.
6. ^The school day in Germany – at least for those learners who attend a Ganztagsschule [schools which basically cover the entire day] – usually starts between 7.30 and 8am goes until 3pm or 4pm. A half day would basically mean that students leave school between 12pm and 1pm.
7. ^Children who are diagnosed with severe enough special needs (i.e. social-emotional issues, physical handicap etc.) have the right to obtain a special needs assistant. The assistant accompanies the student the entire day and helps the students in times of need. However, such an assistant is not granted if the child falls into the administrative category of ‘learning'.
References
Ahlrichs, R. (2012). Zwischen sozialer Verantwortung und ökonomischer Vernunft: unternehmensethische Impulse für die Sozialwirtschaft. Wiesbaden: Springer-Verlag. doi: 10.1007/978-3-531-94355-8
Andreu-Fernández, V., La Maida, N., Marquina, M., Mirahi, A., García-Algar, O., Pichini, S., et al. (2024). Novel interventions on comorbidities in patients with fetal alcohol spectrum disorder (FASD): an integrative review. Biomedicines 12:496. doi: 10.3390/biomedicines12030496
Astley, S. J. (2013). Validation of the fetal alcohol spectrum disorder (FASD) 4-digit diagnostic code. J. Popul. Ther. Clin. Pharmacol. 20, 416–467.
Basaraba, D. (2016). FASD: from isolation to inclusion in Australian schools (doctoral dissertation). Victoria: Deakin University.
Becker, G., and Hantelmann, D. (2013). Fetales Alkoholsyndrom: Oft fehldiagnostiziert und falsch betreut. Deutsches Ärzteblatt 110, 1944–1945.
Betts, J. L., Eggins, E., Chandler-Mather, N., Shelton, D., Till, H., Harnett, P., et al. (2022). Interventions for improving executive functions in children with foetal alcohol spectrum disorder (FASD): a systematic review. Campbell Syst. Rev. 18:e1258. doi: 10.1002/cl2.1258
Blanck-Lubarsch, M., Dirksen, D., Feldmann, R., and Hohoff, A. (2023). A systematic review: facial, dental and orthodontic findings and orofacial diagnostics in patients with FASD. Front. Pediatr. 11:1169570. doi: 10.3389/fped.2023.1169570
Bogner, A., Littig, B., and Menz, W. (2014). Interviews mit Experten - Eine praxisorientierte Einführung. Wiesbaden: Springer VS. doi: 10.1007/978-3-531-19416-5
Bogner, A., and Menz, W. (2002). “Das theoriegenerierende experteninterview,” in Das Experteninterview - Theorie, Methode, Anwendung, eds. A. Bogner, B. Littig, W. Menz (Opladen: Leske+Budrich), 33–70. doi: 10.1007/978-3-322-93270-9
Bogner, A., and Menz, W. (2009). “Das theoriegenerierende Experteninterview,” in Experteninterviews (3. Auflage), eds. A. Bogner, B. Littig, W. Menz (Wiesbaden: VS Verlag für Sozialwissenschaften), 61–98.
Branton, E., Thompson-Hodgetts, S., Johnston, D., Gross, D. P., and Pritchard, L. (2022). Motor skills and intelligence in children with fetal alcohol spectrum disorder. Dev. Med. Child Neurol. 64, 965–970. doi: 10.1111/dmcn.15175
Brown, J. M., Bland, R., Jonsson, E., and Greenshaw, A. J. (2019). The standardization of diagnostic criteria for fetal alcohol Spectrum disorder (FASD): implications for research, clinical practice and population health. Can. J. Psychiatry 64, 169–176. doi: 10.1177/0706743718777398
Burd, L. (2016). FASD and ADHD: are they related and How?. BMC Psychiatry 16:325. doi: 10.1186/s12888-016-1028-x
BzGA (2023). Ohne Ausnahme: Kein Alkohol in der Schwangerschaft. Available online at: https://www.bundesdrogenbeauftragter.de/presse/detail/ohne-ausnahme-kein-alkohol-in-der-schwangerschaft/ (Accessed January 26, 2023).
Chase, W. G., and Simon, H. A. (1973). Perception in chess. Cognit. Psychol. 4, 55–81. doi: 10.1016/0010-0285(73)90004-2
Coriale, G., Fiorentino, D., Lauro, D. i., Marchitelli, F., Scalese, R., Fiore, M., et al. (2013). Fetal alcohol spectrum disorder (FASD): neurobehavioral profile, indications for diagnosis and treatment. Rivista di Psichiatria 48, 359–369. doi: 10.1708/1356.15062
Debè, A., Erşan, Ö., Neuhaus, T., Polenghi, S., Viteri Paredes, M. J., Vogt, M., et al. (2024). The influence of eugenic thinking on special needs assessment procedures. a historical and international-comparative study of Germany, Italy, and the United States. Espacio, Tiempo y Educación 11, 25–48. doi: 10.14516/ete.11202
Dunbar Winsor, K. (2021). An invisible problem: stigma and FASD diagnosis in the health and justice professions. Adv. Dual Diagn. 14, 8–19. doi: 10.1108/ADD-07-2020-0014
Duquette, C. A., and Parr, L. (2022). Students with fetal alcohol syndrome. Exceptionality Educ. Int. 32, 55–76.
Dwyer, P. (2022). The neurodiversity approach (es): what are they and what do they mean for researchers?. Hum. Dev. 66, 73–92. doi: 10.1159/000523723
Eckert, T. (2021). Eigenschaften der Indikatoren zum Montitoring von Inklusion. Bildungsforschung 1, 1–21. doi: 10.25656/01:22554
Edmonds, K., and Crichton, S. (2008). Finding ways to teach to students with FASD. Int. J. Spec. Educ. 23, 54–73. doi: 10.7459/ct/23.1.06
Ehrig, L., Wagner, A. C., Wolter, H., Correll, C. U., Geisel, O., Konigorski, S., et al. (2023). FASDetect as a machine learning-based screening app for FASD in youth with ADHD. NPJ Digit. Med. 6:130. doi: 10.1038/s41746-023-00864-1
Ericsson, K. A., Krampe, R. T., and Tesch-Römer, C. (1993). The role of deliberate practice in the acquisition of expert performance. Psychol. Rev. 100, 363–406. doi: 10.1037/0033-295X.100.3.363
Fadeeva, E., and Nenasteva, A. (2022). Diagnostic results of IQ-test in school-aged children with fetal alcohol syndrome and fetal alcohol spectrum of disorders. Eur. Psychiatry 65:421. doi: 10.1192/j.eurpsy.2022.1068
Feldmann, R., Löser, H., and Weglage, J. (2007). Fetales alkoholsyndrom (FAS). Monatsschr Kinderheilkd 155, 853–865. doi: 10.1007/s00112-007-1567-9
Gabler, S. (1992). Schneeballverfahren und verwandte Stichprobendesigns. Zuma Nachrichten 16, 47–69.
Gasterstädt, J., Kistner, A., and Adl-Amini, K. (2021). Die Feststellung sonderpädagogischen Förderbedarfs als institutionelle Diskriminierung? Eine Analyse der schulgesetzlichen Regelungen. Zeitschrift für Inklusion 4.
Gibbs, A. (2025). Using living experience and practitioner research to create unique programmes providing help for caregivers, professionals and students to increase support for children living with foetal alcohol spectrum disorder. Int. Social Work 68, 751–755. doi: 10.1177/00208728241288018
Gläser, J., and Laudel, G. (2010). Experteninterviews und qualitative Inhaltsanalyse. Wiesbaden: VS Verlag für Sozialwissenschaften. doi: 10.1007/978-3-531-91538-8
Gödecke, F., and Neuhaus, T. (2024). Das Fetale Alkoholsyndrom als pädagogische Herausforderung - Eruierung des Forschungsfeldes FASD und Desiderata erziehungswissenschaftlicher Forschung. Praxisforschung Lehrer*innenbildung - Zeitschrift für Schul- und Professionsentwicklung 6, 31–45.
Gödecke, F., and Neuhaus, T. (2025). Schulische Unterstützungsmaßnahmen für Kinder und Jugendliche mit FASD - Ergebnisse einer Expertenbefragung. Zeitschrift für Heilpädagogik 76, 105–112.
Green, C. R., Mihic, A. M., Nikkel, S. M., Stade, B. C., Rasmussen, C., Munoz, D. P., et al. (2009). Executive function deficits in children with fetal alcohol spectrum disorders (FASD) measured using the cambridge neuropsychological tests automated battery (CANTAB). J. Child Psychol. Psychiatry 50, 688–697. doi: 10.1111/j.1469-7610.2008.01990.x
Hetmański, M. (2018). Expert knowledge: its structure, functions and limits. Studia Humana 7, 11–20. doi: 10.2478/sh-2018-0014
Hoyme, H. E., Kalberg, W. O., Elliott, A. J., Blankenship, J., Buckley, D., Marais, A. S., et al. (2016). Updated clinical guidelines for diagnosing fetal alcohol spectrum disorders. Pediatrics 138:e20154256. doi: 10.1542/peds.2015-4256
Jacobsen, B., Lindemann, C., Petzina, R., and Verthein, U. (2022). The universal and primary prevention of foetal alcohol spectrum disorders (FASD): a systematic review. J. Prev. 43, 297–316. doi: 10.1007/s10935-021-00658-9
Jewell, E., Dunleavy, B., Faitakis, M., Pun, J. W., Moss, S., Pei, J., et al. (2024). Screening and identification of fetal alcohol spectrum disorder in criminal legal settings: a realist review. Crim. Behav. Mental Health 34, 208–270. doi: 10.1002/cbm.2336
Juretko, K. (2007). Das Muster kognitiver Funktionsstörungen bei Patienten mit fetalem Alkoholsyndrom und fetalen Alkoholeffekten Schwerpunkt: Die Intelligenz. Dissertation Universität Münster.
Kalberg, W. O., and Buckley, D. (2007). FASD: what types of intervention and rehabilitation are useful? Neurosci. Biobehav. Rev. 31, 278–285. doi: 10.1016/j.neubiorev.2006.06.014
Kerdreux, E., Fraize, J., Garzón, P., Chalain, E., Etchebarren, L., Sitbon, D., et al. (2024). Questioning cognitive heterogeneity and intellectual functioning in fetal alcohol spectrum disorders from the Wechsler intelligence scale for children. Clin. Neuropsychol. 38, 1109–1132. doi: 10.1080/13854046.2023.2281703
Kottmann, B. (2006). “Die Überweisung in die Sonderschule,” in Auf den Anfang kommt es an., eds. R. Hinz, and B. Schumacher (Hrsg.) (Wiesbaden: VS Verlag für Sozialwissenschaften), 145–152. doi: 10.1007/978-3-531-90429-0_14
Landgraf, M., Hilgendorff, A., and Heinen, F. (2014). Mütterlicher Alkoholkonsum in der Schwangerschaft und fetales Alkoholsyndrom. Monatsschr Kinderheilkd 162, 903–910. doi: 10.1007/s00112-014-3222-6
Landgraf, M. N., and Hoff, T. (2018). Fetale Alkoholspektrumstörungen: Diagnostik, Therapie, Prävention. Stuttgart: Kohlhammer Verlag. doi: 10.17433/978-3-17-024321-7
Lange, S., Probst, C., Gmel, G., Rehm, J., Burd, L., Popova, S., et al. (2017). Global prevalence of fetal alcohol spectrum disorder among children and youth: a systematic review and meta-analysis. JAMA Pediatr. 171, 948–956. doi: 10.1001/jamapediatrics.2017.1919
Lees, B., Riches, J., Mewton, L., Elliott, E. J., Allsop, S., Newton, N., et al. (2022). Fetal alcohol spectrum disorder resources for educators: a scoping review. Health Promot. J. Aust. 33, 797–809. doi: 10.1002/hpja.574
Louw, J. G., Broodryk, M., White, L., Acker, D., Viljoen, D. L., and Oliver, L. (2024). A multi-year, multi-site study of the prevalence of fetal alcohol syndrome in South Africa. Alcohol Clin. Exp. Res. 48, 867–879. doi: 10.1111/acer.15306
May, P. A., Blankenship, J., Marais, A-. S., Gossage, J. P., Kalberg, W. O., Joubert, B., et al. (2013). Maternal alcohol consumption producing fetal alcohol spectrum disorders (FASD). Drug Alcohol Depend. 133, 502–512. doi: 10.1016/j.drugalcdep.2013.07.013
May, P. A., Fiorentino, D., Gossage, P. J., Kalberg, W. O., Hoyme, E. H., Robinson, L. K., et al. (2006). Epidemiology of FASD in a province in Italy. Alcohol. Clin. Exp. Res. 30, 1562–1575. doi: 10.1111/j.1530-0277.2006.00188.x
Mayring, P. (2019). Qualitative content analysis. Qual. Soc. Res. 20. doi: 10.1007/978-3-658-18387-5_52-2
Meuser, M., and Nagel, U. (2009). “Das Experteninterview - konzeptionelle Grundlagen und methodische Anlage,” in Methoden der vergleichenden Politik- und Sozialwissenschaft, eds. S. Pickel, G. Pickel, H. J. Lauth, and D. Jahn (Hrsg.) (Wiesbaden: VS Verlag für Sozialwissenschaften), 465–479. doi: 10.1007/978-3-531-91826-6_23
Meyen, M., Löblich, M., Pfaff-Rüdiger, S., and Riesmeyer, C. (2011). Qualitative Forschung in der Kommunikationswissenschaft. Wiesbaden: VS Verlag für Sozialwissenschaften. doi: 10.1007/978-3-531-92829-6
Millar, J. A., Thompson, J., Schwab, D., Hanlon-Dearman, A., Goodman, D., Koren, G., et al. (2017). Educating students with FASD. J. Res. Spec. Educ. Needs 17, 3–17. doi: 10.1111/1471-3802.12090
Millians, M. N. (2015). Educational needs and care of children with FASD. Curr. Dev. Disord. Rep. 2, 210–218. doi: 10.1007/s40474-015-0055-5
Minke, M. (2009). Wissen und Kompetenzen von Lehrkräften an Förderzentren im Hinblick auf das Fetale Alkoholsyndrom (FAS). Forum Magazin 1–38.
Mitašíková, P., and Vodičková, B. (2022). Conditions and Barriers to School Inclusion for Children with Fetal Alcohol Spectrum Disorders - FASD. Int. J. Adv. Educ. 8, 60–69. doi: 10.51508/intcess.202257
Neuhaus, T. (2023). “Im Angesicht des Chaos - Die Geschichte zweier US-amerikanischer Anwaltskanzleien, ihrer Gründer sowie ihres Erfolges,” in Errungenschaften: Historische und psychologische Perspektiven auf eminente Leistungen, eds. F. Hutmacher, and R. Mayrhofer (Lengerich: Pabst Publishing), 47–59.
Neuhaus, T. (2025). Von Hilfsschulaufnahmeverfahren bis zur Feststellung sonderpädagogischen Unterstützungsbedarfs - Kritische Reflexionen von Überprüfungsprozessen im Feld des Lernens. Praxisforschung Lehrer*innenbildung - Zeitschrift für Schul- und Professionsentwicklung 7, 103–127. doi: 10.11576/pflb-8002
Neuhaus, T., and Gödecke, F. (2024). Schulische Unterstützungsmaßnahmen für Kinder und Jugendliche mit Fetaler Alkoholspektrum-Störungen (FASD) - Ein Scoping Review. Qualifizierung für Inklusion 6. doi: 10.21248/qfi.150
Neuhaus, T., and Vogt, M. (2025). “Intelligenzdiagnostik und der konzeptionelle Wandel des, Hilfsschulkindes' (ca. 1830–1930) - Eine historische Fallstudie,” in Historische und bildungshistorische Perspektiven auf Inklusion in Erziehung, Bildung und Schule, eds. M. Reichert, P. Gollub, S. Greiten, and M. Veber (Bad Heilbrunn: Julius Klinkhardt Verlag), 13–32. doi: 10.35468/6176-01
Opini, B. (2019). Inclusive education as exclusive practice. Exceptionality Educ. Int. 29, 72–90. doi: 10.5206/eei.v29i2.9403
Poth, C., Pei, J., Job, J. M., and Wyper, K. (2014). Toward intentional, reflective, and assimilative classroom practices with students with FASD. Teach. Educ. 49, 247–264. doi: 10.1080/08878730.2014.933642
Riggie, J. L., and Xu, T. (2013). Supporting individuals with fetal alcohol spectrum disorders. A summary of effective practices. Phys. Disabilities 32, 43–89. doi: 10.14434/pders.v32i2.12996
Roozen, S., Stutterheim, S. E., Bos, A. E., Kok, G., and Curfs, L. M. (2022). Understanding the social stigma of fetal alcohol spectrum disorders: from theory to interventions. Found. Sci. 27, 753–771. doi: 10.1007/s10699-020-09676-y
Schecke, H. (2021). Herausforderung FASD-Diagnostik im Erwachsenenalter. DNP-Der Neurologe Psychiater 22, 22–26. doi: 10.1007/s15202-021-4643-4
Schmidt, H., Fietzek, M., Holodynski, M., and Feldmann, R. (2016). FAS-Erste-Hilfe-Koffer. Idstein: Schulz-Kirchner-Verlag.
Schütz, A. (1972). “Der gut informierte Bürger,” in Gesammelte Aufsätze. Band 2, ed. A. Schütz (Den Haag: Nijhoff), 85–101. doi: 10.1007/978-94-010-2849-3_5
Spohr, H-. L. (2014). Das Fetale Alkoholsyndrom im Kindes- und Erwachsenenalter. Berlin/Boston: de Gruyter Verlag. doi: 10.1515/9783110287899
Sprondel, W. M. (1979). “Experte‘ und Laie',” in Alfred Schütz und die Idee des Alltags in den Sozialwissenschaften, eds. W. M. Sprondel, and R. Grathoff (Stuttgart: Ferdinand Enke Verlag), 140–154.
Swart, S. (2012). Intertwining to fit in: a grounded theory study of caregivers with school-aged children with FASD (doctoral dissertation), University of British Columbia, Vancouver, BC, Canada.
Tetlock, P. E. (2017). Expert Political Judgment. Princeton, NJ: Princeton University Press. doi: 10.1515/9781400888818
Tortorelli, C., Badry, D., Choate, P., and Bagley, K. (2023). “Ethical and social issues in FASD,” in Fetal Alcohol Spectrum Disorders, eds. O. A. Abdul-Rahman, and C. L. M. Petrenko (Cham: Springer), 363–384. doi: 10.1007/978-3-031-32386-7_14
Tsang, T. W., Lucas, B. R., Carmichael Olson, H., Pinto, R. Z., and Elliott, E. J. (2016). Prenatal alcohol exposure, FASD, and child behavior: a meta-analysis. Pediatrics 137, 1–20. doi: 10.1542/peds.2015-2542
Van Schalkwyk, I., and Marais, S. (2017). Educators' relational experiences with learners identified with fetal alcohol spectrum disorder. South Afr. J. Educ. 37, 1–9. doi: 10.15700/saje.v37n3a1278
Vogt, M., and Neuhaus, T. (2023). Der Wandel sonderpädagogischer Wissensordnungen in Überprüfungsverfahren - Ein Vergleich zwischen DDR und BRD (1959–1975). Zeitschrift für Pädagogik 69, 186–199. doi: 10.3262/ZP2302186
Vogt, M., and Neuhaus, T. (forthcoming). Die Diagnostik von Hilfsschulbedürftigkeit - Eine historische Analyse des und Kritik am Magdeburger Verfahren. Zeitschrift Inklusion.
Wassermann, S. (2015). “Das qualitative Experteninterview,” in Methoden der Experten- und Stakeholdereinbindung in der sozialwissenschaftlichen Forschung, eds. M. Niederberger, and S. Wassermann (Wiesbaden: Springer VS), 52–67. doi: 10.1007/978-3-658-01687-6_4
Wegner, D. M. (1987). “Transactive memory: a contemporary analysis of the group mind,” in Theories of Group Behavior, eds. B. Mullen, and G. R. Goethals (New York, NY: Springer), 185–208. doi: 10.1007/978-1-4612-4634-3_9
Wright, G., and Ayton, P. (1987). Eliciting and modelling expert knowledge. Decis. Support Syst. 3, 13–26. doi: 10.1016/0167-9236(87)90032-7
Zahir, R., Alcorn, A. M., McGeown, S., Mandy, W., Aitken, D., Murray, F., et al. (2024). Evaluation of wider community support for a neurodiversity teaching programme designed using participatory methods. Autism 28, 1582–1590. doi: 10.1177/13623613231211046
Zink, N. (2025a). “Fetale Alkoholspektrumstörung” wird viel zu selten erkannt: Aktualisierte Leitlinie stellt die vier diagnostischen Säulen vor. DNP-Die Neurologie Psychiatrie, 26, 23–26. doi: 10.1007/s15202-024-6388-3
Keywords: fetal alcohol spectrum disorder, inclusion, educational support, expert interviews, multiple disabilities
Citation: Neuhaus T and Gödecke F (2025) Educational support for learners with FASD—Results from German expert interviews. Front. Educ. 10:1623937. doi: 10.3389/feduc.2025.1623937
Received: 06 May 2025; Accepted: 15 October 2025;
Published: 30 October 2025.
Edited by:
Israel Kibirige, University of Limpopo, South AfricaReviewed by:
Jacobus Louw, Foundation for Alcohol Related Research, South AfricaNatalya Pasklinsky, Columbia University, United States
Copyright © 2025 Neuhaus and Gödecke. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Till Neuhaus, dGlsbC5uZXVoYXVzQHVuaS1iaWVsZWZlbGQuZGU=