 Maria Gudbrandsen
Maria Gudbrandsen Michelle Jayman
Michelle Jayman- Centre for Research in Psychological Wellbeing (CREW), School of Psychology, University of Roehampton, London, United Kingdom
Children and young people with 22q11.2 deletion syndrome (22q) face unique educational and wellbeing challenges that are often poorly understood in mainstream schools. This participatory action research (PAR) aimed to produce a practical, school-based toolkit to support the needs of pupils with 22q with a focus on wellbeing and inclusive practice. Participants included educational professionals (N = 7), young people with 22q and their parents (N = 9), and staff in schools (N = 3). Data were collected through questionnaires, a co-production workshop, and a focus group, and analyzed thematically. Participants collaboratively designed three resources; an infographic poster, a pocket guide for staff, and a short, animated video aimed at peers. Survey findings identified key gaps in staff knowledge, inconsistent provision, especially for transition, and limited wellbeing support, in line with the authors’ previous research. These findings helped to inform the development of the resources, which were praised by staff in schools for clarity, adaptability and alignment with existing practices. This study demonstrated how co-produced, low-cost resources can enhance awareness, promote inclusion and support the holistic wellbeing of pupils with 22q. This approach offers a scalable model for addressing similar gaps across wider SEND.
1 Introduction
Children with special educational needs and disabilities (SEND) represent a significant proportion of the school community. There are approximately 9 million pupils in England, and over 1.7 million have SEND (GOV.UK, 2005). Evidence suggests significant variability in the quality, availability, and type of support and resources offered to pupils with SEND across different settings, with many experiencing unmet learning and wellbeing needs due to inadequate provision and limited specialist support (Children’s Comissioner, 2022; GOV.UK, 2023). In line with evidence supporting the benefits of promoting both mental and physical wellbeing in education (Well Schools, 2023), a genuinely inclusive, holistic approach must tackle the full spectrum of needs experienced by pupils with SEND. Current challenges, intensified by systemic pressures, have contributed to rising levels of alternative provision referrals and exclusions among the SEND population (Thomson, 2023). Despite legislation supporting inclusive education (Children and Families Act 2014), evidence from research with children and young people (CYP) strongly suggests that their voices often go unheard; especially those with SEND (House of Commons Education Committee, 2019). Nonetheless, studies have shown that pupils with SEND can actively contribute to positive change and drive more inclusive practice in schools (Dimitrellou and Male, 2020). The current participatory action research (PAR) is underpinned by this ethos and focused on supporting the holistic wellness of a subpopulation of SEND pupils: CYP with 22q11.2 deletion syndrome (22q).
1.1 Characteristics and challenges associated with 22q
Children with 22q face unique educational challenges and support needs due to a combination of overlapping factors. They have complex developmental challenges, including cognitive, language and motor delays (Swillen and McDonald-McGinn, 2015), and face socio-emotional difficulties (Cohen et al., 2017). These overlapping challenges highlight the importance of integrated support systems that consider not only academic progress but also emotional resilience, social inclusion and physical components of wellness. The 22q condition affects approximately 1 in 2148 individuals (Blagojevic et al., 2021) and presents with a highly variable profile, distinct facial features such as a small mouth, wide-set eyes, drooping eyelids, and a rounded nasal tip, as well as physical health complications, such as palatal abnormalities, congenital heart disease, immunodeficiency, and low muscle tone (McDonald-McGinn et al., 2015; McDonald-McGinn et al., 2022). In the UK, the socio-emotional needs of CYP with this condition are largely overlooked in the classroom due to lack of staff knowledge, or the focus of support being directed primarily on academic progress (Cohen et al., 2017). A recent study highlighted the importance of parental perspectives in shaping inclusive planning.
Communication difficulties are common among the 22q population (Solot et al., 2019). Many also have a mild- to-moderate intellectual disability (Fiksinski et al., 2022) and may attend either a mainstream or special school depending on severity. UK data is limited, but one study suggested that 76% of CYP with 22q attend mainstream schools, and overall, 74% had a statement of special educational needs (Reilly and Stedman, 2013). However, international studies suggest a trend toward special education during secondary schooling and beyond, when the curriculum demands higher cognitive skills and more abstract understanding (Mosheva et al., 2019; Cutler-Landsman, 2020). In addition, physical challenges hinder participation in activities like physical education (PE) and group sports, and CYPs often have numerous appointments with health professionals due to the range of medical issues which leads to frequent absence (Reilly and Stedman, 2013). Combined with learning challenges, this can greatly impact CYP’s educational journey (McDonald-McGinn et al., 2015) and consequently, result in feelings of inadequacy and a lack of belonging.
In addition to medical and educational challenges, CYP with 22q are at increased risk of neurodevelopmental and psychiatric conditions, including autism, attention deficit hyperactivity disorder (ADHD) and phobias (Schneider et al., 2014). Mood and anxiety disorders are particular common and linked to developmental milestones that demand greater independence and social integration. These difficulties may be exacerbated by low self-esteem and a growing awareness of their differences (Fabbro et al., 2012; Tang et al., 2015). Moreover, daily challenges with social cognition can make it difficult to form and maintain peer relationships and many CYP with 22q experience bullying or exclusion by peers which can lead to anxiety and social withdrawal (Angkustsiri et al., 2014). Combined, these cognitive, behavioral and socio-emotional difficulties significantly affect the educational experiences of CYP with 22q.
1.2 Gaps in support for learning and wellbeing
Lack of awareness of 22q among school staff often results in variation in the level of provision, poor communication between educators and families, and a failure to address individual needs (Cohen et al., 2017). A recent co-production study echoed these concerns, highlighting that schools prioritized academic performance over holistic support while CYP’s socio-emotional needs were often ignored (Jayman et al., 2025). Moreover, the authors reported several triggers for poor mental health, including bullying, peer rejection and social isolation (Jayman et al., 2025). Despite these challenges, CYP with 22q can thrive when provided with appropriate learning and socio-emotional support as shown by data from the US (Cutler-Landsman, 2020). Jayman et al.’s (2025) research identified a range of protective school factors including strong relationships with knowledgeable staff, supportive peers, and inclusive environments. Building on this evidence, further co-production research is needed to tackle the existing gaps in holistic wellbeing support in the UK education system.
1.3 Championing co-production and inclusion in education and research
The current study aligns with educational priorities that champion inclusive, health-promoting environments (GOV.UK, 2021; Schuelka, 2018) where all pupils can thrive academically, socially, and emotionally. Key to this is authentic collaboration with CYP, their families and other key stakeholders. As such, this study aimed to bridge knowledge gaps and facilitate more inclusive practice by designing an educational toolkit comprised of practical resources. Crucially, development was led by young people with 22q and their families. Their voices and experiences were prioritized throughout the research process.
2 Methodology
This study used a participatory action research approach (PAR), involving educational professionals, young people with 22q11.2DS, and their parents. Data were collected through questionnaires, a co-production workshop, and a focus group, and analyzed thematically to inform toolkit development.
2.1 Design
The study design was participatory-action research (PAR) (James et al., 2007) (see Figure 1). PAR recognizes participants as active collaborators throughout the research journey (Kindon et al., 2009). Any health evaluation, either physical, mental, or other, should involve the individuals whose health is being addressed (Fetterman et al., 1996). Thus empowering participants to have greater control over their lives (Baum et al., 2006).
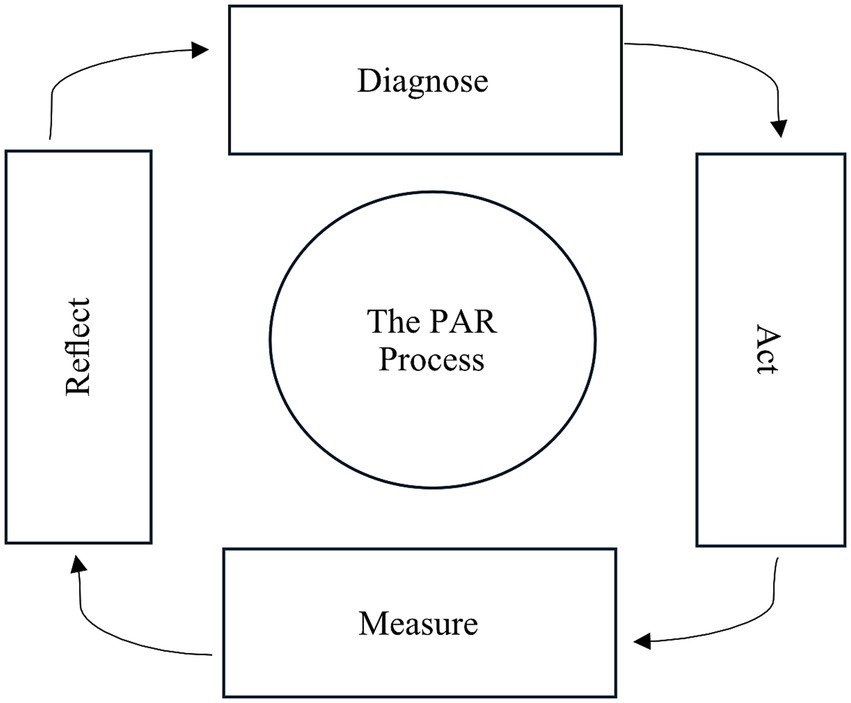
Figure 1. The PAR design process (adapted from James et al., 2007).
PAR aims to be democratic, reducing the top-down, expert-driven nature of traditional evaluation research (Kindon et al., 2009), and is particularly suitable for research involving marginalized groups such as CYP with 22q and the wider SEND population. PAR principles were embedded throughout the research process (see Table 1).
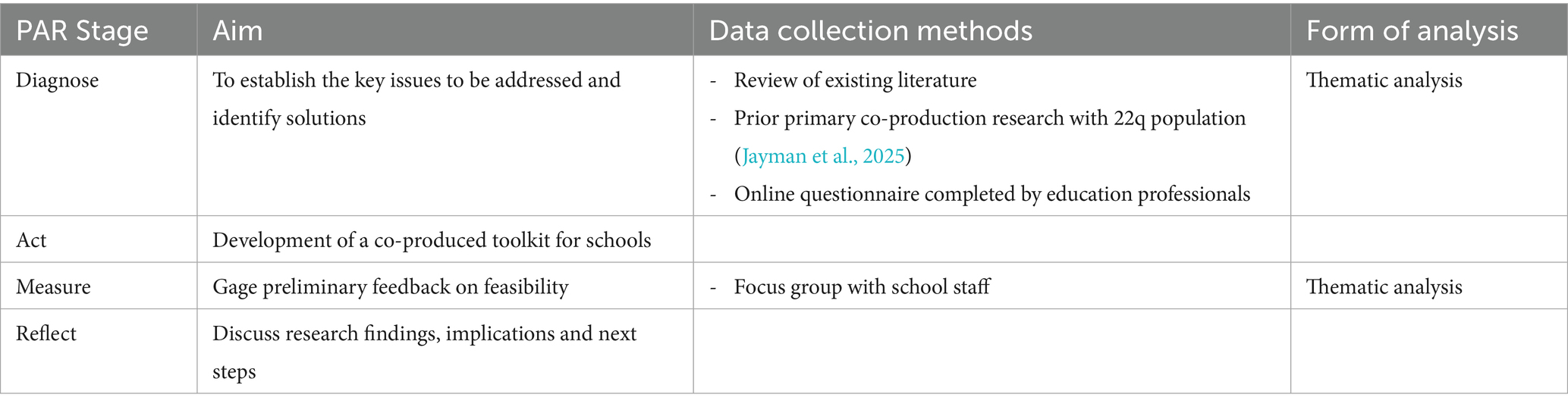
Table 1. Summary of the PAR research process.
2.2 Participants
The coproduction team comprised: Educational professionals (questionnaire respondents); CYP with 22q and parents, Educators (focus group participants); and researchers from the University (see Table 2). Purposive sampling was used to recruit professionals and CYP with 22q and their families.
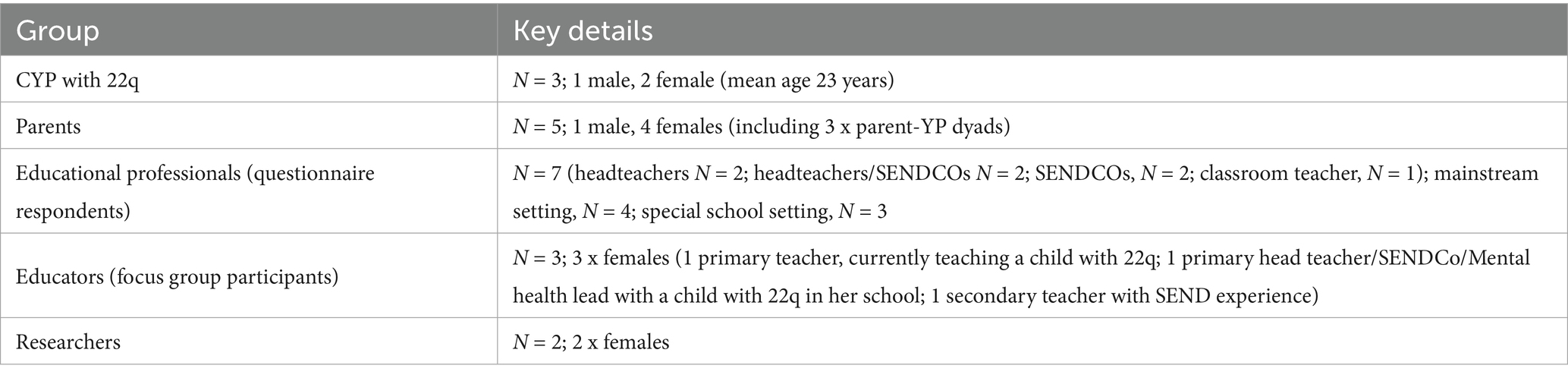
Table 2. The co-production team.
2.3 Procedures
Ethical approval was provided by the University ethics board before the study commenced (PSYC 24–493). An online questionnaire was distributed to educational professionals from across the UK. Questions pertained to: Staff sources of knowledge around 22q and wider SEND; knowledge and provision of support; barriers to supporting students with 22q and wider SEND; and transition and induction. Ten educational professionals responded; three were excluded due to missing data and seven were included in the analysis.
A total of nine participant-researchers (three young people with 22q and six parents) took part in designing and developing the toolkit resources. A one-day workshop was hosted at the University and took place in a comfortable room arranged for group work. Resources including large paper, colored pens, sticky notes and Blu Tak were provided to facilitate workshop activities. The session was facilitated by author 1 and author 2. The co-production team agreed the aims of the workshop. Participant-researchers brainstormed ideas for tackling existing poor understanding and lack of support in schools for CYP with 22q. Through a collaborative, iterative process, three resource types were selected to comprise an educational toolkit for schools (primarily aimed at secondary schools, where evidence suggests CYP struggle the most): an infographic poster targeted at the whole school community; a pocket guide for support staff, and a short video aimed at peers without 22q. Three smaller groups were formed (with one young person and two parents in each), to work on developing the individual resources, with researchers facilitating but not directing discussion. At the end, each group presented their ideas, and feedback was shared across the group to inform further development. The workshop lasted approximately 4 hours with lunch and refreshment breaks added. CYP and parent dyads were paid £50 each for their time and reimbursed travel/accommodation expenses. Following the workshop, the designs for the resources were refined in collaboration with participant-researchers via online communications until final approval was agreed.
Three educators from across the UK took part in an online focus group to provide preliminary feedback. Qualitative data on the toolkit’s practical application in schools were gathered. Each educator was provided with a £50 book voucher for their school. Feedback was used to refine the toolkit and revised versions were shared with all stakeholders for final sign-off. A set of sample resources was produced by external professional services.
2.4 Researcher reflexivity
The researchers acknowledged traditional power imbalances in research and actively stepped back from leading, instead prioritizing the voices of CYP with 22q and their families throughout. Participants were treated as co-researchers, and member checking was regularly used to ensure authentic representation of their views.
2.5 Data collection and analysis
Questionnaire data were integrated with evidence from the wider literature and prior research findings. Deductive thematic analysis was conducted to identify key gaps in understanding and support needs for CYP with 22q which informed the development of an educational toolkit. Focus group data from educators was thematically analyzed to establish preliminary evidence of feasibility and inform ongoing development.
3 Findings
Findings are presented in accordance with the first three stages of the participatory action research cycle: 1. Diagnose – establish the key issues to be targeted for action and identify solutions; 2. Act – develop a practical toolkit solution; 3. Measure – implement a process to evaluate the potential value of the toolkit.
3.1 Thematic analysis findings from PAR stage 1: diagnose
Integrated findings from the extant literature, prior co-production research with the 22q population (Jayman et al., 2025) and questionnaire data collected from educational professionals, identified specific gaps in understanding and support for pupils with 22q as well as factors promoting good practice and inclusion. Two thematic categories and nine subthemes were elicited (see Table 3).
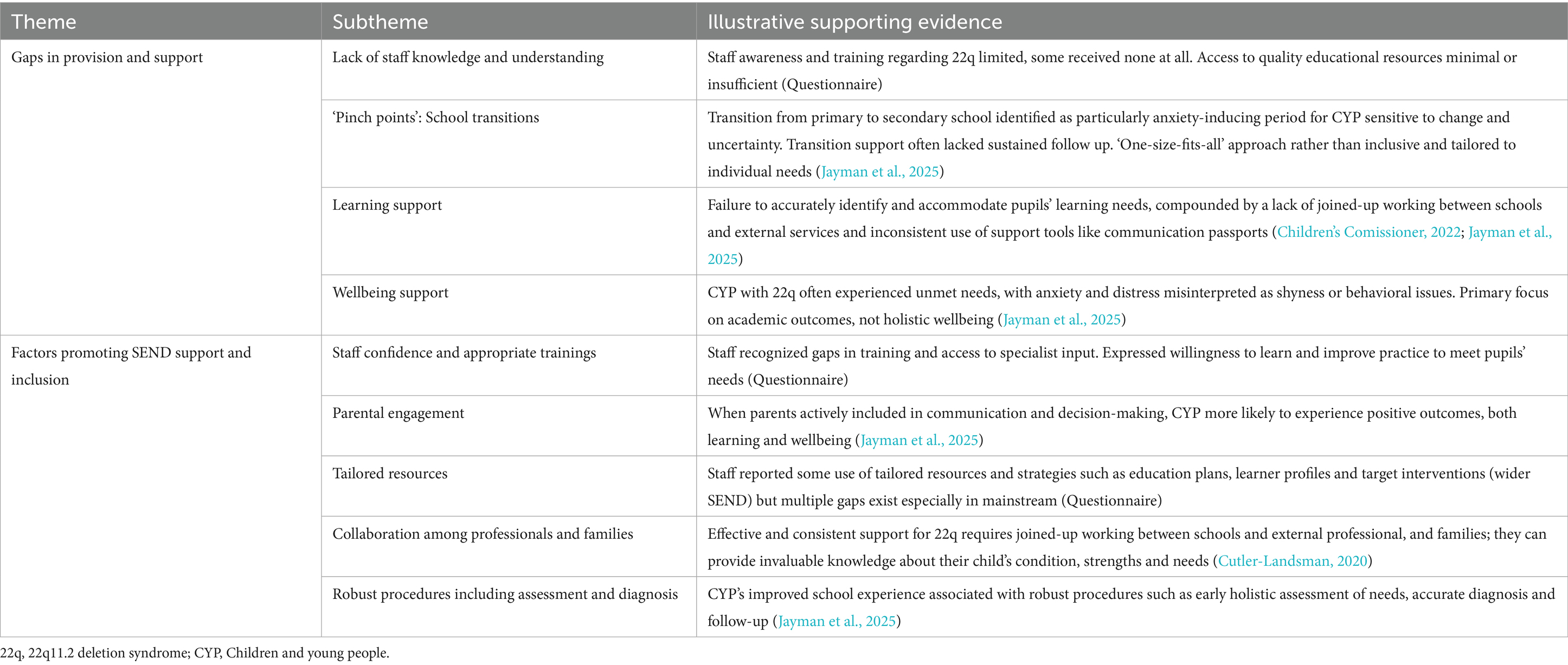
Table 3. Table of theme: gaps and factors to promote good practice in schools for CYP with 22q.
Findings revealed that the majority of staff in schools (85%) had little awareness of 22q, and limited knowledge had been acquired informally, via parents, staff’s own research or the MaxAppeal (22q) charity. Little formal training around 22q was identified and support staff lacked confidence in their ability to provide tailored support. Families reported feeling dismissed or misunderstood by professionals and often felt excluded from planning the support for their CYP which contributed to knowledge gaps. Education, Health and Care Plans (EHCPs) were largely completed without parental or CYP input and with targets often vague, poorly set, and consequently unachievable.
School transitions were periods when CYP and families felt more support was needed as school-related stressors were intensified. The transition from primary to secondary school was a pivotal ‘pinch point’, that is, a critical stage in a pupil’s educational journey when challenges and support needs are heightened. For young people with 22q11.2DS, such transitions often bring increased stress and risk of unmet needs, highlighting the importance of targeted support at these times. Transition planning was often inconsistent and lacked follow-up across settings. While some tailored support was reported, a fragmented picture was revealed with insufficient support in place, particularly around socioemotional needs.
Multiple gaps were identified in timely and appropriate support for CYP’s unique learning needs. For example, with regard to speech, language and communication, support was often variable, and a lack of joined up working between schools and speech and language services was a common challenge. While ‘communication passports’ designed to share information between professionals were underutilized.
Similarly, gaps in mental wellbeing support were revealed with CYP’s needs often being overlooked or misinterpreted as behavioral issues. Several school-related factors associated with diminished wellbeing such as peer rejection, disrupted routines and lack of belonging were commonly reported. Due to the lack of formal or accessible support pathways (e.g., targeted socio-emotional interventions), some CYP used avoidance coping strategies. As Kate reflected, “I think I mostly just blocked out my time at secondary school from my mind.” Whereas Emma took a more direct approach: “Her way of dealing with it is to get out of the situation, so she’ll tell the teachers that she’s not feeling…her aim from that is that somebody will come and pick her up and take her home” (parent of Emma). Conversely, protective factors included positive relationships with trusted adults, peer support and structured routines. Kate’s parent described the primacy of her daughter’s relationship with one of her teacher’s: “Her German teacher was so good with her and so nurturing, he worked with her one-to-one.” While Callum extolled the benefits of having someone to call a friend, “Abel [my friend] looked after me and helped me.”
Despite the substantial barriers that CYP encountered, some pockets of good practice were flagged which relate not only to CYP with 22q but the broader SEND population. School staff were generally committed to supporting all CYP under their care given appropriate training and support themselves. Factors promoting better provision and an improved school experience for pupils with SEND included good relationships between staff and parents with strong parental involvement, robust and consistent procedures, tailored resources, and collaboration among all key stakeholders including CYP. Pertinently, however, these exemplars overwhelmingly emanated from specialist providers, exposing a disproportionate gap in support and good practice found in mainstream settings.
Collectively, these findings indicated a widespread lack of whole school awareness of 22q and accessible resources to support pupils in mainstream schooling. To address these gaps, the co-production team agreed an action plan which constituted the next stage of the PAR cycle.
3.2 Outputs from the co-production workshop PAR stage 2: ACT
YP and their parents designed a toolkit primarily targeted at secondary schools. This comprised three unique resources: 1. An infographic poster, targeted at the whole school community for display in public areas to raise general awareness of the condition. 2. A pocket guide aimed at individuals working on a 1–1 basis with CYP, and who may have little or no specialist training or prior experience. 3. A short, animated video aimed at peers without 22q. See Figure 2 documenting the design and development process for the infographic poster.
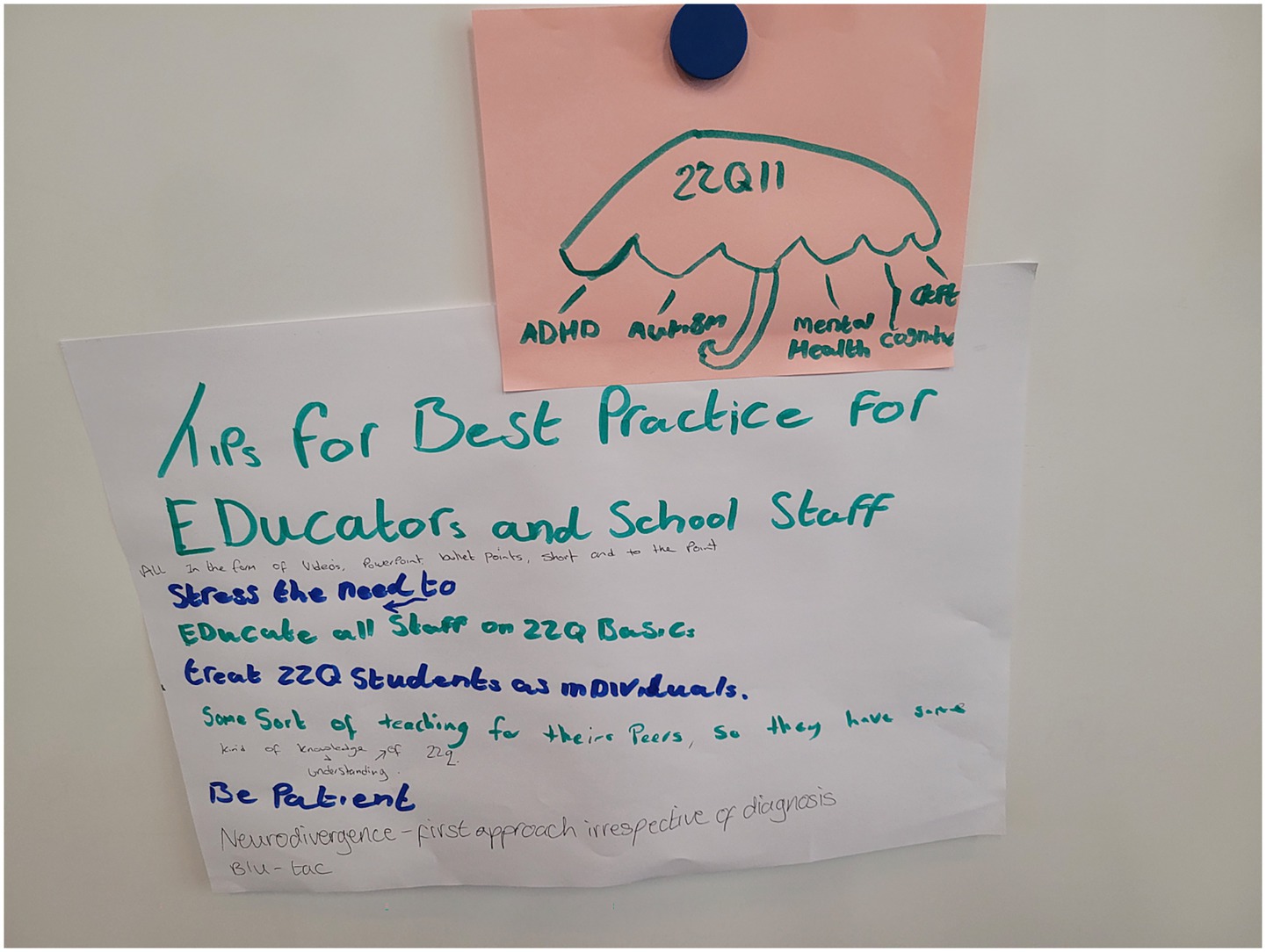
Figure 2. Initial brainstorming ideas for the infographic poster.
Following the workshop, the authors worked closely with YP and their families over several weeks to refine and finalize the first iterations of the three resources for stage 3 of the PAR cycle.
3.3 Thematic analysis findings from PAR stage 3: measure
Overall, feedback from the three educators who participated in the focus group was highly positive. All three resources were perceived as useful and feasible for implementation in mainstream school settings. The video was still under development at the time of writing and evaluation not included here Key findings are organized under thematic categories: Practicality and alignment with existing practice; Value to multiple stakeholder groups; and Ongoing development and enhancement.
3.3.1 Theme 1: practicality and alignment with existing practice
Educational professionals appreciated the clarity, simplicity, and visual design of the materials which aligned well with existing school practices such as transition packs and SEND awareness initiatives. The resources were seen as easily integrated into routine processes: “I’d be using that as part of class transitions [line 128]… also sharing it in staff meetings where SEND is a standard agenda item [line 133].” The infographic poster was praised as a means of raising general awareness among staff and school visitors. The format and layout were seen as conducive to initiating conversations about individual pupil needs and potential wider application in the classroom was proposed: “I can easily print this out and then talk to the specific pupil and put actions onto those bubbles [lines 192–193]… really useful as a framework to have those conversations” [lines 195–96]. Others described how the poster could be widely displayed in public areas or circulated via email “There could be posters displayed in staff rooms [line 175] … my principal might just attach it to an e-mail for all staff to look at” [lines 179–180].
3.3.2 Theme 2: value to multiple stakeholder groups
The pocket guide was described as useful for a range of stakeholders, including teaching assistants and inclusion teams. Its concise, actionable format was appreciated for offering practical strategies, easily implemented with limited prior knowledge of 22q: “Documents like this… give staff more to go on… looking through those actions, some of those would work” [lines 715–716]. Crucially, the guide was seen as promoting a holistic understanding of pupil needs, encompassing physical health, emotional wellbeing, and learning profile: “It gives you an idea that it’s not just a learning need… there’s the physical, then their wellbeing, and then about how they learn” [lines 840–842].
The ‘My Support Needs’ section was seen as particularly valuable for planning: “I could see it working when doing teacher transitions and handovers [line 694]. Furthermore, “I can present these points to anyone who joined in new inclusion team [line 878] … a great starting point… slowly build up to include more strategies to support that student” [lines 886–887].
3.3.3 Theme 3: ongoing development and enhancement
Educators offered suggestions to enhance the accessibility and impact of the resources. One recommendation was to bold key phrases to ensure important messages were not overlooked: “Just putting some of the phrases that they [young people] felt were most important in bold… so you are going to catch it quickly at a glance” [lines 404–406]. Another suggestion was to provide a blank version of the poster to allow for personalized use in the classroom, for example, when pupils arrive in a new setting and may feel anxious with unfamiliar staff. As one educator explained “If there is like a blank version that we can [individually] update… that would be really helpful [line 218–220]… especially when they are quite anxious, quite shy when they transition into year 7” [line 234].
Suggestions for improving the pocket guide included clarifying that the introduction was written by a young person with 22q – “I only realised it was written by a young person when I got to the end… maybe make it clearer” [line 651–653]. Adding a blank notes page at the back of the guide was also recommended, so it could be used as a continuous working document with individual pupils.
Based on educator feedback, the resources were revised, and final versions were signed off by all stakeholders (see Figure 3). See a link to the full toolkit (Centre for Research in Psychological Wellbeing (CREW), University of Roehampton’s website: https://www.roehampton.ac.uk/research/research-and-knowledge-exchange-centres/centre-for-research-in-psychological-wellbeing/. Also, see video aimed at peers at: https://www.youtube.com/watch?v=XPTR5odnJJw).
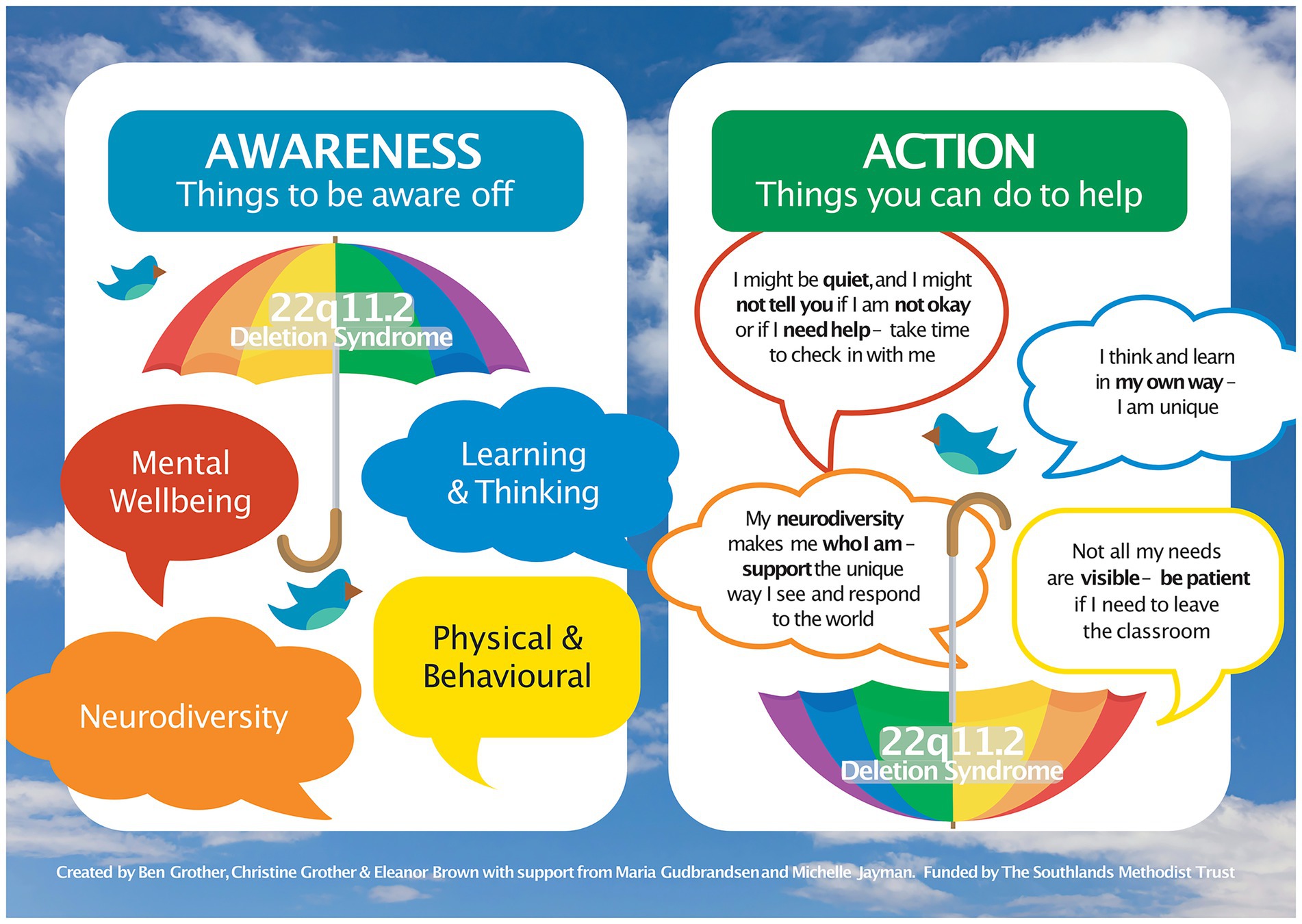
Figure 3. Final version of the infographic poster.
4 Discussion
This study aimed to address a significant gap in educational awareness and support for CYP with 22q in mainstream schools. Extant evidence (Jayman et al., 2025) has highlighted the unique educational challenges and elevated risk of poor holistic wellbeing these pupils face. Effective school strategies are urgently needed to address current gaps in provision and ensure inclusive learning environments and tailored support for every pupil. Collaborative working and co-production with all key stakeholders is at the heart of effective and meaningful change (Jordan et al., 2022). Through PAR, an educational toolkit was designed with young people with 22q and their families, ensuring their authentic voices and experiences shaped its development.
Previous literature highlights complex and multifaceted needs of CYP with 22q, spanning cognitive, physical, and socio-emotional social domains (Cutler-Landsman, 2020; Angkustsiri et al., 2014; Tang et al., 2014). Current findings confirmed limited awareness of 22q, lack of formal training for educational professionals, and inconsistent school provision, aligning with broader literature on inadequate provision for the general SEND population (Children’s Comissioner, 2022). Findings also identified school-level factors that promote better support for pupils with SEND and more inclusive practice. Good relationships between staff and parents and strong parental involvement in decision-making around educational planning were pivotal to ensuring genuine, rather than assumed, needs were met. Worryingly, in line with wider research, parents of CYP with 22q often struggled to have their voices heard (Cohen et al., 2017). A recent study highlighted the importance of parental perspectives in shaping inclusive educational planning, finding that parents often faced significant challenges in advocating for their child’s needs, particularly in navigating inconsistent provision and limited staff understanding (Roche et al., 2024). This reinforce the current study’s emphasis on strong parental involvement and the need for collaborative approaches to educational support. As such, this study adds to growing evidence (Dimitrellou and Male, 2020) showing the vital contribution of CYP, including those with SEND, for developing effective and meaningful interventions and initiatives targeted at them.
The educational toolkit created from this study focuses on both mental wellbeing (i.e., anxiety and peer-relationships) as well as physical health (i.e., fatigue and medical needs), reflecting a holistic approach to supporting the needs of pupils with 22q in mainstream schools. Crucially, the toolkit embodies the heterogenous experiences and voices of its main beneficiaries (Ackermann, 2021). As well as enhancing relevance and usability for the target population, it champions the commitment to inclusive practice and empowerment of marginalized groups (Baum et al., 2006). Preliminary feedback from educators was overwhelmingly positive and toolkit resources were rated highly for clarity, accessibility, and adaptability across educational settings. The infographic poster was seen as an effective tool for raising awareness at the school-wide level, while the pocket guide provided actionable strategies for those working directly with pupils. The inclusion of a video aimed at peers’ further supports fostering inclusive school environment, as peer-led interventions have been shown to improve understanding and empathy among pupils (Dodd et al., 2022). Importantly, educators noted that the toolkit complimented some existing SEND support practices, suggesting it could be integrated into current provision. Ease of implementation and educator buy-in are imperative considerations in proposing any new school-based initiative (Turnbull, 2002; Nellis and Fenning, 2023).
It is important to acknowledge some limitations of this study. Due to relatively small sample sizes, transferability of the findings is limited. However, it is possible that the small sample size combined with our PAR approach, encouraged tailored and creative resources that may not have emerged in a larger or less focused study. Also, the small sample size fostered close collaboration between researchers, participants and stakeholders, deepening engagement and ownership of the research outcome. While there is potential for self-selection bias in this study, as those with a particular interest or experience with 22q may have been more likely to participate, informal feedback suggested non-participation was mainly due to practical constraints. Further, toolkit focused primarily on early secondary school application; therefore adaptations are required to optimize use across different levels of education. Future studies should also consider sustained use of the toolkit in schools and implementation processes according to local needs.
This study had several strengths. It utilized a PAR design, empowering CYP with 22q and their families to take an active role in shaping the research process and driving real-world outcomes. The co-production team also included educators from both mainstream and specialist settings, ensuring that all stakeholder perspectives were incorporated. Finally, the study produced a scalable, low-cost resource for schools to help enhance staff confidence and competence in supporting pupils with 22q.
The overall study findings contribute to the growing body of work advocating for a holistic, inclusive, educational environment, supporting all pupil needs, whether academic, socio-emotional or physical (GOV.UK, 2021; Schuelka, 2018). Specifically, it highlights a clear need for improved training and awareness for 22q, particularly for mainstream education. The toolkit can be integrated into staff training and transition planning and contributes to engendering an overall more inclusive school environment for CYP with 22q.
In conclusion, this co-production study addresses gaps in educational provision for CYP with 22q. By prioritizing the voices of young people and their families, a practical, evidence-informed toolkit was developed, with potential to improve awareness, promote inclusivity, and enhance holistic support in schools. This PAR model can be used to guide improved support for other specific conditions, as well as the wider SEND population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the ethical approval for the study was provided by the University of Roehampton ethics board before the study commenced (PSYC 24-493). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MG: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing, Investigation. MJ: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was supported by the Southlands Methodist Trust under Grant Number PSY-2024-20. The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
The authors would like to express their heartfelt thanks to the young people with 22q11.2 Deletion Syndrome and their parents who generously shared their time, experiences, and insights as co-researchers in this study. Your voices were central to every stage of this project and have been invaluable in shaping its direction and findings. We are also grateful to the educators who contributed their perspectives and to those who provided thoughtful feedback throughout the research process. Our sincere thanks to the Southlands Methodist Trust for their financial support which made this research possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. Microsoft Copilot, powered by OpenAI’s GBT-4 model (version GBT-4-turbo) was used to assist with rephrasing and improving clarity of text originally written by MG. All AI-assisted edits were reviewed and approved by MG to ensure accuracy and integrity.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ackermann, T. (2021). Co-production approaches in social research with children and young people as service users-challenges and strategies. Soc. Work Soc. 18, 1–17. Available at: https://www.researchgate.net/publication/349395020
Angkustsiri, K., Goodlin-Jones, B., Deprey, L., Brahmbhatt, K., Harris, S., and Simon, T. (2014). Social impairments in chromosome 22q11.2 deletion syndrome (22q11.2DS): autism spectrum disorder or a different endophenotype? J. Autism Dev. Disord. 44, 739–746. doi: 10.1007/s10803-013-1920-x
Baum, F., Macdougall, C., and Smith, D. (2006). Participatory action research. J. Epidemiol. Community Health 60, 854–857. doi: 10.1136/jech.2004.028662
Blagojevic, C., Heung, T., Theriault, M., Tomita-Mitchell, A., Chakraborty, P., Kernohan, K., et al. (2021). Estimate of the contemporary live-birth prevalence of recurrent 22q11.2 deletions: a cross-sectional analysis from population-based newborn screening. CMAJ Open 9:E802-e809. doi: 10.9778/cmajo.20200294
Children’s Comissioner,. (2022). Beyond the labels: A SEND system which works for every child, every time. Available at: https://assets.childrenscommissioner.gov.uk/wpuploads/2022/11/cc-beyond-the-labels-a-send-system-which-works-for-every-child-every-time.pdf (Accessed May 4, 2025).
Cohen, W., Mccartney, E., and Crampin, L. (2017). 22q11 deletion syndrome: parents’ and children’s experiences of educational and healthcare provision in the United Kingdom. J. Child Health Care 21, 142–152. doi: 10.1177/1367493516686203
Cutler-Landsman, D. (2020). Educating children with Velo-cardio-facial syndrome, 22q11.2 deletion syndrome, and DiGeorge syndrome. San Diego: Plural Publishing, Inc.
Dimitrellou, E., and Male, D. (2020). Understanding what makes a positive school experience for pupils with SEND: can their voices inform inclusive practice? J. Res. Spec. Educ. Needs 20, 87–96. doi: 10.1111/1471-3802.12457
Dodd, S., Widnall, E., Russell, A. E., Curtin, E. L., Simmonds, R., Limmer, M., et al. (2022). School-based peer education interventions to improve health: a global systematic review of effectiveness. BMC Public Health 22:2247. doi: 10.1186/s12889-022-14688-3
Fabbro, A., Rizzi, E., Schneider, M., Debbane, M., and Eliez, S. (2012). Depression and anxiety disorders in children and adolescents with velo-cardio-facial syndrome (VCFS). Eur. Child Adolesc. Psychiatry 21, 379–385. doi: 10.1007/s00787-012-0273-x
Fetterman, D., Kaftarian, S., and Wandersman, A. (1996). Empowerment evaluation: Knowledge and tools for Self-Assessment & Accountability. Thousand Oaks, California: SAGE Publications, Inc.
Fiksinski, A. M., Bearden, C. E., Bassett, A. S., Kahn, R. S., Zinkstok, J. R., Hooper, S. R., et al. (2022). A normative chart for cognitive development in a genetically selected population. Neuropsychopharmacology 47, 1379–1386. doi: 10.1038/s41386-021-00988-6
GOV.UK. (2021). Promoting and supporting mental health and wellbeing in schools and colleges. Available at: https://www.gov.uk/guidance/mental-health-and-wellbeing-support-in-schools-and-colleges (Accessed May 4, 2025).
GOV.UK. (2023). Academic year 2022/23: Special educational needs in England. Available at: https://explore-education-statistics.service.gov.uk/find-statistics/special-educational-needs-in-england/2022-23/data-guidance (Accessed May 10, 2025).
GOV.UK. (2005). Academic year 2024/25: Special educational needs in England. Available at: https://explore-education-statistics.service.gov.uk/find-statistics/special-educational-needs-in-england/2024-25/data-guidance (Accessed May 10, 2025).
House of Commons Education Committee. (2019). Special educational needs and disabilities: Government response to the committee’s first report of session 2019. Available at: https://committees.parliament.uk/publications/2067/documents/19714/default/ (Accessed May 10, 2025).
James, E. A., Milenkiewicz, M. T., and Bucknam, A. (2007). Participatory action research for educational leadership: Using data-driven decision making to improve schools. Thousand Oaks, CA: SAGE Publications.
Jordan, A., Jones, E., Horter, S., and Snape, D. (2022). Educational experiences of young people with special educational needs and disabilities in England: February to May 2022. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/educationandchildcare/bulletins/educationalexperiencesofyoungpeoplewithspecialeducationalneedsanddisabilitiesinengland/februarytomay2022 (Accessed May 6, 2025).
Jayman, M., Edmonds, S., and Gudbrandsen, M. (2025). Driving innovation to support pupils with SEND through co-production in education and research: participatory action research with 22q11.2 deletion syndrome families in England. Behav. Sci. 15:22. doi: 10.3390/bs15010022
Kindon, S., Pain, R., and Kesby, M. (2009). “Participatory action research” in International encyclopedia of human geography. ed. R. T. Kitchin (Amsterdam, Netherlands: Elsevier).
McDonald-McGinn, D. M., Hoffman, E., Lairson, L. A., Mcginn, D. E., and Zackai, E. H. (2022). “22q11.2 deletion syndrome: setting the stage” in The chromosome 22q11.2 deletion syndrome. ed. D. M. McDonald-McGinn (New York: Academic Press).
Mcdonald-Mcginn, D. M., Sullivan, K. E., Marino, B., Philip, N., Swillen, A., Vorstman, J. A. S., et al. (2015). 22q11.2 deletion syndrome. Nat. Rev. Dis. Primers 1:15071. doi: 10.1038/nrdp.2015.71
Mosheva, M., Pouillard, V., Fishman, Y., Dubourg, L., Sofrin-Frumer, D., Serur, Y., et al. (2019). Education and employment trajectories from childhood to adulthood in individuals with 22q11.2 deletion syndrome. Eur. Child Adolesc. Psychiatry 28, 31–42. doi: 10.1007/s00787-018-1184-2
Nellis, L. M., and Fenning, P. A. (2023). “Connecting implementation science and school-based initiatives: considerations for practice” in Systems consultation and change in schools: integrating implementation science into practice. eds. L. M. Nellis and P. A. Fenning (Cham: Springer International Publishing).
Reilly, C., and Stedman, L. (2013). Supporting children with genetic syndromes in the classroom: the example of 22q deletion syndrome. Support Learn. 28, 115–121. doi: 10.1111/1467-9604.12029
Roche, L., Flynn, T., and Campbell, L. (2024). Exploring education for children with 22q11. 2 deletion syndrome: A qualitative study of mothers perspectives. OBM Genetics 8, 1–36. doi: 10.21926/obm.genet.2401217
Schneider, M., Debbane, M., Bassett, A. S., Chow, E. W. C., Fung, W. L. A., van den Bree, M. B. M., et al. (2014). Psychiatric disorders from childhood to adulthood in 22q11.2 deletion syndrome: results from the international Consortium on Brain and behavior in 22q11.2 deletion syndrome. Am. J. Psychiatry 171, 627–639. doi: 10.1176/appi.ajp.2013.13070864
Schuelka, M. J. (2018). Implementing inclusive education. Available at: https://k4d.ids.ac.uk/resource/implementing-inclusive-education/ (Accessed May 10, 2025).
Solot, C. B., Sell, D., Mayne, A., Baylis, A. L., Persson, C., Jackson, O., et al. (2019). Speech-language disorders in 22q11.2 deletion syndrome: best practices for diagnosis and management. Am. J. Speech Lang. Pathol. 28, 984–999. doi: 10.1044/2019_AJSLP-16-0147
Swillen, A., and McDonald-McGinn, D. (2015). Developmental trajectories in 22q11.2 deletion syndrome. Am. J. Med. Genet. C Semin. Med. Genet. 169, 172–181. doi: 10.1002/ajmg.c.31435
Thomson, D. (2023). Risk factors of permanent exclusion. Available at: https://ffteducationdatalab.org.uk/2023/09/risk-factors-of-permanent-exclusion/ (Accessed May 4, 2025).
Tang, K. L., Antshel, K. M., Fremont, W. P., and Kates, W. R. (2015). Behavioral and psychiatric phenotypes in 22q11.2 deletion syndrome. J. Dev. Behav. Pediatr. 36, 639–650. doi: 10.1097/DBP.0000000000000210
Tang, S. X., Yi, J. J., Calkins, M. E., Whinna, D. A., Kohler, C. G., Souders, M. C., et al. (2014). Psychiatric disorders in 22q11.2 deletion syndrome are prevalent but undertreated. Psychol. Med. 44, 1267–1277. doi: 10.1017/S0033291713001669
Turnbull, B. (2002). Teacher participation and buy-in: implications for school reform initiatives. Learn. Environ. Res. 5, 235–252. doi: 10.1023/A:1021981622041
Keywords: special educational needs, 22q11.2 deletion syndrome, inclusive education, mental wellbeing, participatory action research, co-production, educational toolkit
Citation: Gudbrandsen M and Jayman M (2025) Fostering healthy schools for students with SEND through co-production: creating an educational toolkit to support young people with 22q11.2 deletion syndrome. Front. Educ. 10:1655848. doi: 10.3389/feduc.2025.1655848
Edited by:
Darren Moore, University of Exeter, United KingdomReviewed by:
Ben Morris, Leeds Trinity University, United KingdomJulie Milner, Long Island University - Post Campus, United States
Copyright © 2025 Gudbrandsen and Jayman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Gudbrandsen, bWFyaWEuZ3VkYnJhbmRzZW5Acm9laGFtcHRvbi5hYy51aw==