 Nicole Quodling
Nicole Quodling Norman Hoffman
Norman Hoffman Frederick Robert Carrick
Frederick Robert Carrick Monèm Jemni
Monèm Jemni- 1The Carrick Institute, FL, United States
- 2Coelevate Chiropractic, Adelaide, SA, Australia
- 3College of Medicine, University of Central Florida, Orlando, FL, United States
- 4Burnett School of Biomedical Science, University of Central Florida, Orlando, FL, United States
- 5MGH Institute for Health Professions, Boston, MA, United States
- 6Centre for Mental Health Research in Association with the University of Cambridge, Cambridge, United Kingdom
- 7Faculty of Physical Education, Ningbo University, Ningbo, China
Chronic pain is inherently multifactorial, with biological, psychological and social factors contributing to neuropathic pain (NP) and central sensitization (CS) syndromes. Comorbidity between functional disorders and the lack of clinical biomarkers adds to the challenge of diagnosis and treatment, leading to frustration for healthcare professionals and patients. The main objective of this review is to investigate the association between NP, CS syndromes and sensory processing disorders. A structured search was conducted on the PubMed database using the keywords Central Sensitization, Fibromyalgia, Complex Regional Pain Syndrome, and Neuropathic Pain, combined with the keywords Vision, Audition, Olfaction, Touch, Taste, and Proprioception. PubMed was chosen because it is accessible and user-friendly. Articles within the last five years, from 2018 to 2023, have been included. 380 studies on conditions of CS and sensory processing were identified. After applying inclusion and exclusion criteria, the number of retained papers was 78. There were a few emerging themes. Reduced sensory thresholds were found to be comorbid with chronic pain conditions, particularly those with a component of CS. Both cranial nerve and sensory evaluation examinations may prove helpful as potential biomarkers for diagnosis and for potential treatments.
Introduction
Chronic pain represents one of the most critical public health problems, accounting for significant personal, social, and economic burdens (1). Chronic pain is inherently multifactorial, with biological, psychological and social factors contributing to NP and CS syndromes with considerable comorbidity between the different functional disorders (2, 3).
NP, as defined by the International Association for the Study of Pain (IASP), is “pain caused by a lesion or disease of the somatosensory nervous system” (4). This pain arises when a health condition impacts the nerves responsible for transmitting sensations to the brain, making it distinct from other types of pain. It can affect any nerve in the body, with some nerves more commonly impacted than others. Notably, diabetes-related neuropathy accounts for about 30% of all nerve pain cases. NP can vary in intensity, ranging from mild to severe, and may be persistent or fluctuate over time, affecting any part of the body (5).
The IASP further elaborates that NP requires “a demonstrable lesion or disease that satisfies established neurological diagnostic criteria” (6). It involves complex processes such as sensitization and alterations in brain connectivity (7, 8), initiated by various pathophysiologies including peripheral nerve injury, central nervous system injury, viral infections, tumours, and metabolic disorders (9, 10). This condition persists for at least three months or beyond the expected healing time (11–14).
NP syndromes are notably refractory to treatment and cause significant suffering (10, 15). The prevalence of NP is estimated to be between 6% and 20%, leading to high costs at both individual and societal levels (6, 10, 15, 16) and a decline in quality of life (17).
CS occurs when the patient's nervous system is persistently in a high-activity state, leading to an exaggerated response to pain stimuli. This condition, also known as centralized pain, central pain, or widespread/diffuse pain, is a syndrome influenced by both genetic and environmental factors (18). CS involves the amplification of neural signalling and dysfunction in neurophysiological mechanisms that increase neuronal responses to both noxious and non-noxious stimuli. It is a critical mechanism in chronic pain maintenance (7, 19–21). The underlying factors contributing to CS are complex, individualized, and poorly understood (21). CS is characterized by hypersensitivity to mechanical stimuli, a lowered pain threshold, prolonged pain after the stimulus has been removed, and significant increases in the excitability of nociceptive neurons (21, 22).
CS is inferred from symptoms like allodynia or hyperalgesia without a clear pattern of aggravating or relieving factors and is not in a dermatomal distribution (7, 14, 23). Centralized pain is associated with mood changes, fatigue, cognitive disturbances, sleep changes, catastrophizing, and often comorbid major depressive disorder or generalized anxiety disorder (24). Centralized pain affects between 5% and to 30% of the general population, with fibromyalgia (FM) or migraine being common conditions within this group (25).
Pain severity is often measured through subjective reports, while objective biomarkers that may guide diagnosis and treatment are lacking (15). This leads to ambiguity in diagnosis, difficulties in quantification, reliability and comparability, and uncertainty in understanding its physiopathology (26). There is significant interest in the field, as the biopsychosocial contribution, the lack of biomarkers and ineffective treatments frustrate clinicians and patients alike (14, 27). The clinical description is based on subjective report, history taking, clinical examination, and quantitative sensory testing (QST) (6, 28). Patients with CS syndromes report multiple sensory hypersensitivities, yet environmental sensitivity is not measured as part of the diagnostic process (27, 28). Pre-morbid or baseline sensory processing disorders seem to be a factor in developing CS pain in individuals with chronic musculoskeletal pain and may have been present from a young age (7). Assessing sensory function may prove helpful as diagnostic or predictive criteria and provide insight into potential treatment protocols. Only one paper utilized the SPQ to examine the relationship between FM and sensory processing disorder (27). No review was found to have extensively examined the potential link between chronic pain syndromes in general and sensory processing disorders.
The main objective of this review is to investigate the association between NP, CS syndromes and sensory processing disorders. This paper aims to explore simple definitions of how sensation works, progressing beyond the five traditional senses, to delve into newly recognized senses such as proprioception and equilibrioception.
Method
Following the PRISMA framework, a structured search was conducted on the PubMed database using the keywords Central Sensitization, Fibromyalgia, Complex Regional Pain Syndrome, and Neuropathic Pain, combined with the keywords Vision, Audition, Olfaction, Touch, Taste, and Proprioception. PubMed was chosen because it is accessible and user-friendly. Articles within the last five years, from 2018 to 2023, have been included. 380 studies on conditions of CS and sensory processing were identified. After title and abstract screening, 138 studies were identified as meeting inclusion. These papers were then sorted into two categories—those primarily discussing sensory processing in pain syndromes and those discussing treatment options. The number of papers discussing sensory processing was 78. Papers were excluded if they were animal studies, investigated tissue damage, disease processes or addiction, were conference proceedings or non-English. Only a few relevant reviews that add specific details on the condition have been retained, to summarise evidence from different outcomes, conditions and populations. As this study is a systematic review of previously published research rather than a clinical trial or experimental investigation, the risk of bias was assessed independently by at least two reviewers. Discrepancies were resolved through discussion or adjudication by a third reviewer. A colour-coded system was used to visually flag studies based on their risk level (e.g., low, moderate, or high), supporting transparent identification of studies warranting further discussion.
Results and discussion
380 studies on conditions of CS and sensory processing were identified. After title and abstract screening, 78 studies were identified as meeting inclusion in this paper (Figure 1).
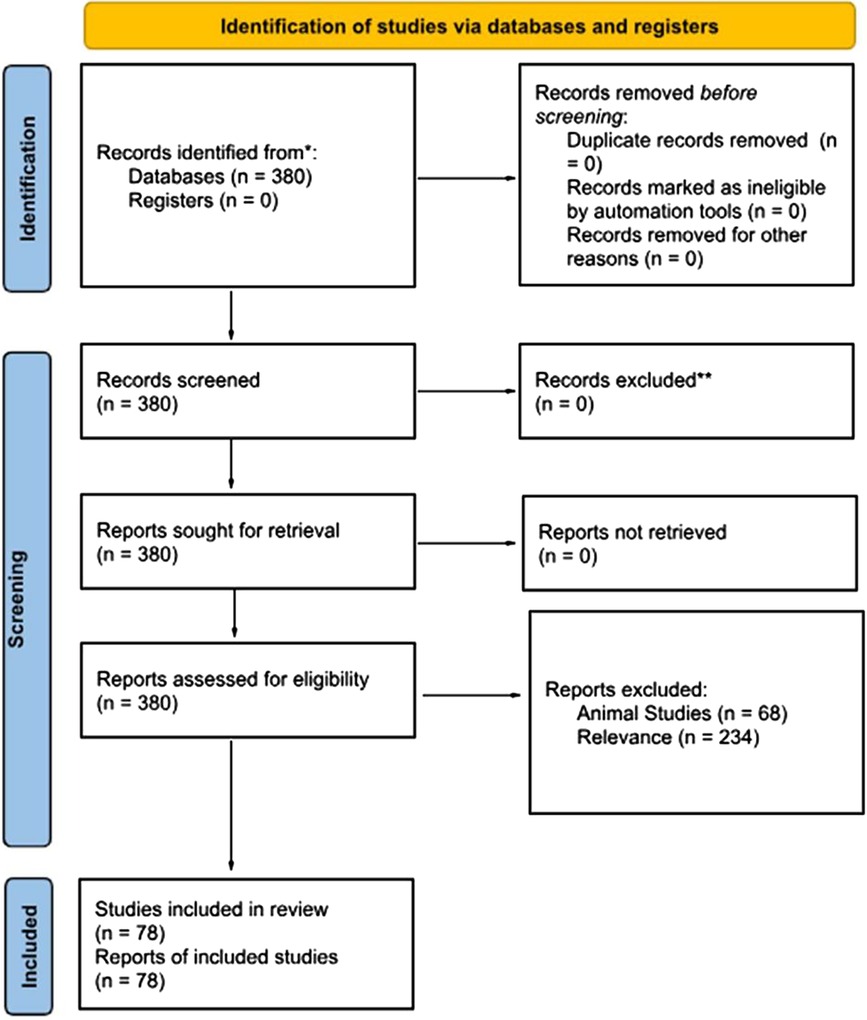
Figure 1. PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only. For more information, visit http://www.prisma-statement.org/.
Findings are summarized in Table 1.
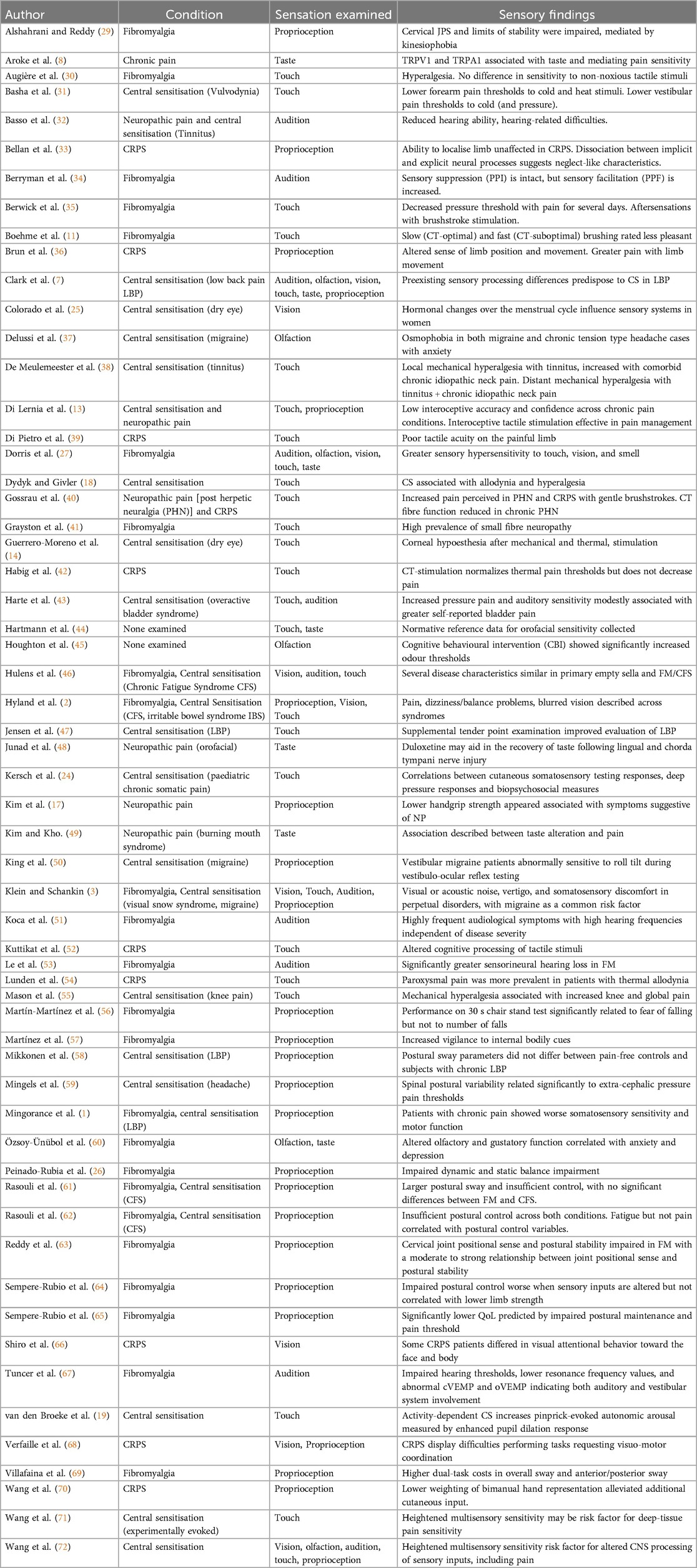
Table 1. Sensory findings by condition.
Neuropathic pain syndromes
Nociplastic pain is associated with dysfunction of the somatosensory nervous system and may result in complex alterations in cognitive and emotional neural functions. Disrupted interoceptive processing is associated with the perception and maintenance of pain (13, 48), paraesthesia, and dysesthesia (16, 49). Since no pain biomarkers exist, the physical examination can only provide supporting evidence for a neurological lesion or disorder that could cause pain (6, 15).
Synaptic plasticity, underlying learning and memory, is a particular component of CS. Syndromes include FM, whiplash, temporomandibular disorders, non-specific low back pain (7, 21), vulvodynia (31) and migraine (25). Centralized pain is associated with mood changes, fatigue, cognitive disturbances, sleep changes, catastrophizing, and often comorbid major depressive disorder or generalized anxiety disorder (24).
Individuals with pain syndromes may experience proprioceptive and balance impairments, gait alteration, sensorimotor deficits and distortions of body representation, which could be caused by alterations in sensory processing (3, 21, 26, 28–30, 34, 60, 61, 64, 73) and a compromised habituation response to repeated stimulus exposures (74).
Dysfunction of the central, autonomic and peripheral nervous systems, alteration of neurotransmitters, endocrine and immune systems, oxidative stress, external stressors and psychological aspects have been implicated (28, 41, 46, 51, 53, 65, 67, 75, 76).
The Complex regional pain syndrome (CRPS)
The complex regional pain syndrome (CRPS) is an example of a NP syndrome. It is characterized by spontaneous or regional pain arising in one or more limbs, usually the upper limb, disproportionate to an inciting event and associated with trophic changes and sensory, motor, and autonomic dysfunction (39, 40, 42, 52, 54, 66, 68, 70, 77). Cognitive difficulties have been reported to affect the ability to represent, perceive and use the affected limb (52, 57, 68). Motor disturbances of the affected limb sometimes spread to the unaffected limb(s) associated with maladaptive “inter-limb coupling” (77). CRPS usually develops from a peripheral event, but its maintenance relies on neuroplastic changes within the central nervous system (39, 40, 52, 54, 66, 77). These deficits implicate distortions in body representation and are corroborated by the evidence of cortical reorganization associated with inflammation, autoimmunity, and genetic, structural and functional changes, although much remains unclear (40, 54, 70). The estimated incidence of CRPS is 5.5–26.2 cases per 100,000 people per year, with females affected more than males. CRPS occurs in approximately 2%–7% of patients who experience limb fractures, injuries or surgery (42).
Fibromyalgia
FM is a complex multifactorial condition of unknown aetiology characterized by chronic widespread pain, hyperalgesia and allodynia (28, 34, 41, 46, 51, 56, 57, 67, 73), leading to significant disability and reduced health-related quality of life (27–29, 41, 53, 56, 63, 64). Patients present with multiple sites of pain or tender points, fatigue, cognitive impairment, sleep impairment, and emotional or mood fluctuations (1–3, 26, 27, 35, 41, 53, 56, 57, 60, 61, 63, 67, 69, 78). Individuals with FM may experience proprioceptive and balance impairments, gait alteration, sensorimotor deficits and distortions of body representation, which could both be caused by alterations in sensory processing (3, 21, 26, 28, 30, 34, 41, 60, 61, 64, 73) Alshahrani & Reddy and a compromised habituation response to repeated stimulus exposures (74). Dysfunction of the central, autonomic and peripheral nervous systems, alteration of neurotransmitters, endocrine and immune systems, oxidative stress, external stressors and psychological aspects have been implicated (1, 28, 41, 46, 51, 53, 65, 67, 75, 76, 78). FM has also been reported to develop as a result of cervical spine injury but, the relationship between spine injury and FM remains unclear (78). The total prevalence of FM in the general population ranges from 0.2% to 11% and is most frequent in women (1, 3, 26, 30, 34, 35, 41, 51, 53, 56, 57, 63, 67, 73, 78).
Diagnosis and assessment
An adequate diagnostic method is required to determine functional deficiencies and achieve adequate therapy objectively (44). Several tests were utilized in the literature and included painDETECT (17, 35), The Central Sensitization Inventory (CSI) (21, 72), Quantitative Sensory Testing (QST) (6, 28, 30, 35, 40, 44, 48, 54, 55, 71), The Sensory Perception Quotient (SPQ) (27), the Fibromyalgia Impact Questionnaire (FIQ) (26, 79), the Body Perception Questionnaire (BPQ) (57) pain drawings (80) and the Tampa Scale for Kinesiophobia (TSK) (77). Pre-morbid assessments of high sensory sensitivity using QST is a predictor of CS (71).
The role of biomarkers
The National Institutes of Health (NIH) defines biomarkers as: “characteristics that can be objectively measured and evaluated as an indication of normal or pathogenic processes or pharmacological responses to a therapeutic intervention” (81). Research into potential biomarkers for medically unexplained pain, including chronic NP (82–84), CRPS (52, 85), FM (34, 86), and CS (81), is ongoing. The pursuit of pain biomarkers has mostly followed two general directions: serum markers (84, 86) and brain neuroimaging (15, 81, 83, 85). However, none of the analysed metabolites have been shown to be sufficiently reliable to create valid and reproducible testing (81, 86). The development of imaging provides objectivity and connects structural changes and potentially therapeutic or diagnostic information by highlighting the involved area of dysfunction. However, structural and functional changes in the neuraxis do not always correlate with pain perception (83). Neuroimaging is also expensive and currently unavailable for routine clinical use (81). Exploiting possible sensory processing issues within the clinical environment may provide screening biomarkers for further investigation (27, 28) and provide viable targets for non-opioid interventions and the development of mechanistic approaches to pain management (84). The approval of composite serological, imaging and clinical biomarkers, emerges as the way forward to improve diagnosis, subtyping, predictive and prognostic evaluation and the development of therapeutic options (15, 81, 83, 85, 86).
Few potential clinical biomarkers were examined in the literature. Vestibular migraine patients were proposed to be abnormally sensitive to roll tilt during vestibular ocular testing, potentially providing a biomarker that allows individual patients to be subtyped as vestibular or non vestibular migraineurs and facilitating individualised treatment (50). Compared with healthy controls, altered but highly variable tactile discrimination performance was shown across CRPS patients. Late latency responses could provide convenient biomarkers of abnormal perceptual decision-making mechanisms in CRPS to aid clinical detection and treatment (52). FM patients were shown to have similar startle responses to healthy controls but reacted more strongly to subsequent sound, demonstrating increased prepulse facilitation. This suggests that the reaction to new or surprising stimulation is overactive, indicating high sympathetic nervous system activity. It was suggested that, as prepulse inhibition was intact, therapies that calm the nervous system, such as vagus nerve stimulation, mindfulness, or music therapy, could be helpful for FM (34).
Objective biomarkers and classification by sensory profiles have been suggested to further understanding of underlying mechanisms, prognosis and validation of therapeutic efficiency for chronic pain conditions (15, 44, 54). The rationale for treatment aims to modulate central nervous system plasticity (34).
Neuropathic pain mechanisms
Central sensitization and sensory processing
Functional disorders are diagnosed by symptoms after other biomedical causes of these symptoms are ruled out (2). Pain hypersensitivity involves multiple mechanisms, including CS, conditioned pain modulation, reward and motivation, epigenetic mechanisms and neuroinflammation, including microglial activation (24). Triggers such as stress, trauma, or environmental changes are associated with the onset, maintenance and exacerbation of the syndrome (3). NP and CS syndromes are characterized by spontaneous pain and almost always by sensory loss and sensory gain (11, 71). Patients display hypersensitivities to internal and external stimuli (22, 27, 28, 30, 34, 35, 45) so that daily life sensations, including noise, light, touch and smell, become aversive (3, 22, 72). Reduced sensory thresholds often exceed the predominantly affected sensory modality, including touch, visual or acoustic noise, odors, and proprioception (3, 28, 43, 71) to a degree that is distressing and painful (45, 67, 71, 72). Furthermore, generalized sensory sensitivity is associated with the presence of chronic overlapping pain conditions (72).
Interoception, sensory processing and associated brain changes
Pain is inherently interoceptive. Such differences also extend to the processing of interoceptive signals (13). FM patients are less able to perceive inner bodily sensations accurately, with interoceptive accuracy correlated with pain intensity, anxiety and depression. Intact unimodal processing of sensory information is essential for integrating these signals with other information, which is at the core of body representation and motor control (30).
The thalamus is a central component of all sensory networks implemented in filtering sensory input. Thalamocortical dysrhythmia has been discussed as the neuronal correlate of several syndromes of pain syndromes (3), most notably FM (30, 41) and CRPS (39). FM patients have demonstrated decreases in grey matter in the prefrontal cortex (11) which has reciprocal connections with the anterior cingulate cortex, amygdala, insula and ventral striatum, to make it well positioned to influence pain perception, including interindividual variability in negative affective responses to multimodal stimuli (15). The insula cortex integrates the forebrain structure involved in sensory perception, learning, and memory (76), playing a crucial role in evaluating and prioritizing stimuli and perceptual decision-making (3) and the psychosocial components of pain (76). Hypervigilance may not be limited to external sensory input but also involves an enhanced awareness of internal bodily cues (57).
Additionally, CS patients show higher activation in motor cortices and rate stimulation as more painful with reduced connectivity between the somatosensory cortex and medial frontal and prefrontal cortices, parahippocampal gyri, thalamus, and pons (3). These cortical areas are influenced by cognitive processing, which includes attentional demands and movement complexity (77). Pain-related central disturbances affect postural control, synergistic muscle activation and recruitment to maintain joint stability and movement in conditions of CS, including FM (1) and CRPS (70). Interestingly, these areas are not dedicated to the reception of the senses (11).
Transient receptor potential (TRP) channels
Two primary types of nerves can detect and transmit painful signals: unmyelinated C-fibers and myelinated Aδ- fibers, which depend on electrical signals generated by ion channels, such as Transient Receptor Potential (TRP) channels (8). TRP are non-selective ion channels mediating the fluxes of various cations across the cell membrane. They are widely expressed in the nervous system including in the substantia nigra, hippocampal pyramidal neurons, hypothalamus, locus coeruleus and cortex to function as cellular sensors (22). Various cellular environmental stimuli such as chemicals, temperature (54), stretch/pressure, osmolarity, and pH (8, 75), activate TRPs to play a significant role in the five primary senses as well as the sense of pain (8, 22). Repeated, chronic activation of TRPA1 (22), TRPM8 and TRPV1 receptors can lead to upregulation and sensitization (22, 54, 75), which may result in a more robust cellular response to an activating substance.
Sensitization involves receptor hyperexcitability and perceiving an input as noxious, even from a standard or subthreshold, generally innocuous stimulus (22). As the role of TRPs in chronic pain and pain modulation emerges, many TRP channels have been examined as potential therapeutic targets for pain management (8, 14, 22, 75).
Comorbidities of neuropathic pain
Vision
CS and concomitant sympathetic nervous system disorders have been associated with retinal nerve fiber thinning, decreased optic disc perfusion, blurred vision, visual field defects and diplopia (46, 78), dry eye (20, 25), photoallodynia, increased visual attention to symptomatology and decreased visual attention to other areas (3, 29, 66). CS can induce an exaggerated pain response when faced with visual illusions that involve sensory incongruence (33). Pinprick stimulation of areas of peripheral hypersensitivity elicits an increased pupil dilation response, making pupil size a possible sensitive measure for detecting the presence of CS (19, 41).
Audition
Audiovestibular complaints are often attributed to central hypersensitivity, despite standard hearing evaluations (28, 30, 34, 51, 64, 67, 73). Central nervous system gain leads to a greater risk for debilitating perceptual consequences, including hyperacusis, auditory hallucinations (3) or tinnitus, with or without vestibular symptoms (3, 50, 73, 79). Tinnitus can be associated with various physical and mental conditions, including chronic pain, depression and anxiety disorders (3, 32, 53, 79, 87). Patients with CS and nociplastic pain conditions can also demonstrate more significant rates of hearing loss (3, 28, 30, 43, 51, 53, 67), which is the most crucial predictor of tinnitus presence (79, 87). There is also preliminary evidence demonstrating that chronic neck pain and tinnitus correlates with findings of CS (38).
Anxiety is not only a predisposing factor for tinnitus but also a consequence of it, which can, in turn, impede habituation (32, 79). A more significant number of patients with tinnitus had chronically elevated cortisol levels. Glucocorticoid receptors are present in the inner ear so that cortisol can exert a direct influence on hearing detection thresholds with aberrant links between limbic and auditory system structures (79). The limbic and auditory systems interact at the thalamic level and modulate the perception of auditory signals. The conscious perception and distress of tinnitus seem to be influenced by connectivity patterns in the anterior cingulate cortex and left precuneus, the posterior cingulate cortex, and the right medial prefrontal cortex (3). The hearing and balance systems function interchangeably and should be evaluated in systemic conditions (67).
Olfaction
Olfactory hypersensitivity, anxiety and pain share common neural pathways and area activation and a possible functional association (3, 11, 30, 37, 60). Osmophobia, defined as fear, aversion, or psychological hypersensitivity to odors, is related to a broader sensorial hypersensitivity and symptoms of CS, such as greater chronicity, elevated anxiety and allodynia (30, 37). Conversely, olfactory loss is an early sign in diagnosing neurodegenerative disorders (22). Patients with FM can be hypersensitive to olfactory stimulations or show reduced olfactory bulb volume associated with decreased olfactory and gustatory function scores (30, 60).
Taste
Most individuals with altered taste function have primarily smell disorder, so smell and taste must be assessed concurrently (60). Neuropathic taste changes have been attributed to peripheral processing, central processing and microglial responses (48). TRP channels are located in nerve terminals, dorsal root ganglion, and taste buds, which play an essential role in pain and taste perception. TRP channelopathies have been associated with NP, inflammation, and reduced taste perception (8). Duloxetine has been shown to facilitate the recovery of partial nerve damage, helping to retrieve sensation and taste and providing evidence of a CS mechanism (48).
Touch
A pathognomic feature of CS is hypersensitivity to somatosensory stimulations (30, 34), which results in allodynia and hyperalgesia (27, 35, 88, 89). Other tactile misperceptions include decreased two-point discrimination and temperature detection (39, 52). Tactile allodynia, especially when accompanied by after-sensations, suggests likely CS (10, 16, 24) and is often reported in FM (27), NP and CRPS (54, 88). Blunt pressure pain thresholds are typically reduced as static mechanical allodynia, but in some cases, gentle brushstroke alone can induce dynamic mechanical allodynia (31, 35). At the cortical level, the anticipation of pain influences brain activity and increases sensitivity to somatosensory stimuli and a reduced ability to habituate to somatosensory stimuli (74).
Pain-sensitized patients characteristically show nociceptive system augmented responsiveness as a common feature (42, 73). Localized or diffuse hyperalgesia signifies regional or diffuse CS (24, 47). Hyperalgesia is often accompanied by allodynia (41). It is not restricted to tender points (30), although tender point examination may be used as a supplementary clinical test (47). Secondary hyperalgesia that is not associated with tender points is thought to result from CS (23). Pain after blunt pressure, tender point examination, pressure pain threshold, brushstroke and thermal assessment typically lingers for several days in FM and is correlated with clinical pain intensity (24, 35). Tender point examination in symptomatic patients can regularly cause long-lasting discomfort and is no longer required for diagnosis (35).
Persons with FM are hypersensitive to thermal stimulation, and show decreased rates of habituation (30, 74). Patients with chronic pain conditions can report more painful and longer-lasting painful aftersensations following exposure to noxious thermal stimuli (35), possibly indicating a pathology of small-diameter nerve fibers (42). There is a significant correlation between thermal allodynia and allodynia to light touch, as underlying hyperexcitability is likely to explain both phenomena (10, 54).
Poor tactile acuity has been observed in people with CRPS (33, 52) and reported to coincide with the distribution of pain (39). Poor tactile acuity could be related to aberrant perceptual representation of the environment or altered somatotopic mapping (52). Social touch is essential for interpersonal interaction and physical and social well-being (11) but, many patients with chronic pain conditions find generally pleasant stimuli intolerable, often inducing wind-up and increasing allodynia and hyperalgesia (11, 70). Uncomfortable aftersensations after brushstroke are associated with reports of reduced pleasantness in FM (11, 35). Mapping cortical activity during brush stroking reveals an inverted pattern of insula activity, inferring that anhedonia might be related to aberrant central nervous system evaluative processing. However, the finding of anhedonia does not exclude the possibility of abnormal signal processing of input from sensory afferents associated with small-fiber pathology (35). Small-fiber neuropathy is a disorder that selectively affects thinly myelinated Aδ and unmyelinated C fibers that mediate pain, heat, and cold sensations (10, 41, 46) and affective aspects and rewarding aspects of touch (35, 40, 42). Social touch is essential for physical and social well-being, and its loss, tactile anhedonia, is an unmistakable feature of FM (11, 35). C Tactile (CT) stimulation can reduce experimental pain in healthy individuals; however, in patients with a reduced intraepidermal nerve fiber density, gentle stroking loses its pain-modulating properties as the pain modulating capacities of CT fibers might be too weak, or the feeling of chronic pain simply overrules normal CT fiber function (13, 42). Many chronic pain conditions show altered C-fiber innervation density, sensory loss, and pain sensitization (40), including FM (11, 41) and CRPS (54). Negative expectations and experiences towards the touch, such as in allodynia, could negatively affect touch perception (40).
Proprioception and vestibular symptoms
Vestibular symptoms of vertigo and unsteadiness are prevalent in CS (21), including migraine (50) and FM (26, 46) and probably result from an overreliance on visual and postural stimuli and reduced input from the central vestibular system (3). Impairment of proprioceptive processing has been observed in people with a range of persistent pain states (88). Proprioception is required for precise and synchronized action planning, joint stability, preserving static and dynamic balance, optimal posture maintenance (63, 64), and to perform tasks requiring visuomotor coordination (68). Body representations are blurred in pain, with alterations shown in motor and sensory cortical areas in CRPS (36, 68) and FM (29, 34, 73). Sensorimotor integration is crucial for planning our movements and their online monitoring and correction, but also to build a unified representation of our body (76, 90). Moreover, alterations in position sense have been associated with the severity of motor deficits (36).
Cervical joint position sense significantly contributes to functional balance mediated by the integrated function of proprioceptors present in the muscles, capsules, joints, and vestibular and visual stimuli. Changes in the proprioceptive signals are associated with cervicogenic dizziness in cervical disc degeneration (90) and FM (29, 63, 73). Cervical injury, pain and muscle fatigue can alter cervical proprioception from muscle spindles (63, 78), resulting in a sensory mismatch of vestibular and visual information, leading to dizziness and instability (89). Cervicogenic dizziness may also be caused by circulatory failure of the vertebral artery or cervical sympathetic nervous system disorders (78). Hand grip force (17), postural sway (61, 69) and cervical joint position sense (63) are reliable methods to measure physical capacity and muscle strength, the lack thereof being a good predictor for functional disability (73).
Posture and balance
Attention and sensory integration of visual and vestibular afferents are essential to produce appropriate motor output, including balance control (26, 57, 69). Alterations to vestibular, visual and somatosensory input could modulate the appropriate neuromuscular response where there is cervical disc degeneration (89) or in patients with FM (64). Alternatively, pain may force a patient to adopt a protective posture to protect the painful or threatened part of the body by constraining movement in the case of cervicogenic headache (59) or neuropathic pain (17), or the impact of pain on γ motor neuron activity can create long-term neurological adaptations of postural and motor behavior (1, 63).
Additionally, impaired postural stability has been linked to reduced muscle strength and stamina, decreased cognitive function, somatosensory integration, and pain processing (63, 64). Postural control impairment can affect balance, thus negatively affecting their quality of life (26, 29, 65). Poor balance has been considered a predictor of widespread musculoskeletal pain (1, 26, 29, 64, 69). The perceived lack of balance is related to the fear of falling, while objective balance is associated with the number of falls (56).
Tone
There is reduced muscle strength in FM and NP symptoms, primarily in female patients (17), both in grip strength, linked to a state of sarcopenia, weakness or dystonia, and in upper limb strength, linked to functional limb capacity (57, 65). Patients with muscle weakness have decreased muscle mass, incomplete muscle activation, decreased muscle spindle sensitivity, fewer sensory units, and fewer mechanoreceptors, all of which can affect the limits of stability (29). Hypermobility is significantly more frequent in FM than in control groups (73). Low handgrip strength is a clinically relevant predictor of poor patient outcomes, such as more extended hospitalization, impaired functional status, mental health problems, poor quality of life, and mortality (17).
Kinesiophobia
The fear of pain following movement or physical activity in patients with musculoskeletal pain can predispose to the development and aggravation of loss of muscle strength and mass (17). Soreness results in avoidance behaviors similar to those with other types of chronic pain (75). Pain is a highly salient signal of bodily harm and, thus, a strong motivator for learning (88). Poor physical fitness or fear of falling may also create avoidance of motor activities of daily living (56).
Kinesiophobia refers to the fear of movement brought on by activity or exercise and the catastrophic belief that such activity would result in damage or re-injury (29) and is frequent in patients with chronic musculoskeletal pain (17). Delayed onset muscle soreness (DOMS) usually leads to hyperalgesia, allodynia and ongoing muscle pain. Kinesiophobia may serve as a protective mechanism against discomfort and the worsening of pain by encouraging the avoidance of movement and the restriction of movement (29, 68). Protective behaviors are helpful in the case of acute pain because they avoid engagement with the pain. However, in chronic pain, this avoidance of interaction increases impairment (29). Fear of movement could impose additional cognitive demands, placing an extra burden on executing a movement task (77). This type of pain-related fear is less stimulus-bound and manifests itself instead as sustained anticipatory anxiety, which is prototypical for widespread pain disorders (88).
Kinesiophobia can cause mobility restriction in individuals with chronic pain and can change motor activation patterns, resulting in muscular weakening and atrophy (17, 59). These modifications can significantly alter the afferent proprioceptive input, affecting joint position sensation and stability limits (29, 36, 61) leading to further deterioration of postural control and fear of falling with a negative impact on endurance, muscle strength, flexibility, coordination, and quality of life (1, 29, 62, 69, 73).
Body image and neglect
Body image is a conscious representation of the body's appearance and our attitudes and feelings towards it, but is not used for action. Body schema is an unconscious representation with sensorimotor integration and is used for motor planning and execution, but may inform body image (36). Maintenance of the body schema depends on multisensory bodily inputs and may be altered in patients suffering from chronic pain (1, 21, 30, 33, 51, 52, 59, 62, 70). The severity of body perception disturbance has been linked to the reorganization of the primary and secondary cortical maps (66). Body image and schema are both tied to activity in the somatosensory and parietal areas, however, only body image is processed in the insula (36). Cortical changes in chronic pain conditions may cause alterations in spatial attention, leading to neglect-like symptoms (66). CRPS patients often describe their affected limb as feeling disconnected from their bodies, with difficulty initiating movements and performing actions consistent with the symptomatology of hemispatial neglect (68). Diminished interoceptive accuracy has been associated with depression and alexithymia (57), CRPS, FM, and NP disorders (13). Sensorimotor integration is crucial for planning movements and building a unified representation of our body (73). Individuals with acute or chronic pain report higher sensory disturbances in the presence of sensorimotor conflicts compared to pain-free individuals (12, 33, 61, 62). This may relate to the inability of incoming sensory inputs to adequately update somatic long-term memory (57).
Clinical applications
Premorbid contexts may be related to the onset of CS. CS pain often develops in the context of sensory processing differences related to learning difficulties, sensitivities and trauma, and personal characteristics of low confidence and control (7). Sensory overload can significantly impact the quality of life (27). Although various aetiologies can cause CS, the symptoms and characteristics of pain are influenced by pathophysiological mechanisms rather than aetiology, with important therapeutic implications for personalized treatment (1). With the recognition that healthcare professionals consistently underestimate pain compared to patients, there is an increasing movement toward person-centered assessment of chronic pain conditions (27). The persistence of symptoms and refractoriness to treatment could be due to the central changes not sufficiently influenced by conventional approaches. Interventions integrating somatic, physical, and emotional factors should be considered when developing clinical programs (1), although the effect of most therapies is modest (34). There is an unmet need to characterize chronic pain patients regarding underlying mechanisms to aid early detection and treatment (52).
Limitations
Despite the structured search strategy and specific eligibility criteria and goals, this review has limitations, related to methodological inconsistencies, study heterogeneity, low subject numbers and the reliance on self-reported data. Although this review was based on an extensive literature review, the study was limited by the selectivity of searches and databases. The findings of all conditions were assessed concurrently, with an assumption of a central origin, however a large proportion of studies examined CS, particularly FM, and proprioceptive deficits, and results may not be generalisable. The lack of biomarkers in medically unexplained pains leads to lack of consistency in measurement, assessment and reporting, further complicating comparison. Further studies are required with large study numbers, subgrouping of pain syndromes and homogenized methodology.
Conclusion
The objective of this review was to investigate the association between NP, CS syndromes and sensory processing disorders. Objective biomarkers for medically unexplained pain syndromes are sadly lacking, thwarting reliable diagnosis and treatment strategies. Multiple sensory hypersensitivities are often reported and in conditions of CS, and could contribute to the diagnostic process and assessment of treatment success. Pre-morbid sensory processing disorders may be a risk factor for the development of chronic pain syndromes. Assessing sensory function through cranial nerve and other neurological examinations may prove helpful as diagnostic or predictive criteria and provide insight into potential treatment protocols.
Recommendations and future directions
Considering the above limitations, the scientific community can move closer to developing more precise diagnostic markers and tailored treatment strategies for individuals suffering from NP and CS syndromes by pursuing the following:
Development of standardized protocols
To enhance comparability and reproducibility, future research should adopt standardized methodologies for assessing NP, CS, and sensory processing (e.g., consistent inclusion/exclusion criteria, uniform pain assessment scales, and validated sensory evaluation tools).
Integration of objective biomarkers
Given the limitations of subjective reporting, studies should explore and validate objective measures—such as cranial nerve evaluations, quantitative sensory testing (QST), and neuroimaging techniques—to identify and confirm the presence of CS and NP mechanisms.
Longitudinal and interventional studies
Further longitudinal research is needed to clarify the natural progression of CS syndromes and to establish causal relationships. Interventional trials that incorporate both pharmacological and non-pharmacological approaches (e.g., sensory re-education, cognitive-behavioral therapy, neuromodulation) could provide deeper insights into effective management strategies.
Personalized medicine approaches
Recognizing the heterogeneous nature of NP and CS syndromes, future efforts should focus on personalized treatment plans that account for individual differences in sensory processing, comorbidities, and psychosocial factors.
Collaborative, multidisciplinary research
Scientists, clinicians, and specialists from fields such as neuroscience, psychology, physiotherapy, and pain medicine should collaborate to develop comprehensive models of chronic pain. This interdisciplinary approach can improve diagnostic accuracy and therapeutic outcomes.
Focused investigation of high-risk groups
Targeted studies of populations underrepresented in the current literature—such as pediatric, geriatric, or culturally diverse groups—would help clarify how central sensitization and sensory processing manifest across different demographics.
Author contributions
NQ: Conceptualization, Formal analysis, Methodology, Project administration, Writing – original draft, Writing – review & editing. NH: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. FC: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. MJ: Formal analysis, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors want to thank the Carrick Institute Admin staff members and Coelevate Chiropractic for their continuing support along the way.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mingorance JA, Montoya P, Miranda JGV, Riquelme I. An observational study comparing fibromyalgia and chronic low back pain in somatosensory sensitivity, motor function and balance. Healthcare (Basel, Switzerland). (2021) 9(11):1533. doi: 10.3390/healthcare9111533
2. Hyland ME, Bacon AM, Lanario JW, Davies AF. Symptom frequency and development of a generic functional disorder symptom scale suitable for use in studies of patients with irritable bowel syndrome, fibromyalgia syndrome or chronic fatigue syndrome. Chronic Dis Transl Med. (2019) 5(2):129–38. doi: 10.1016/j.cdtm.2019.05.003
3. Klein A, Schankin CJ. Visual snow syndrome, the spectrum of perceptual disorders, and migraine as a common risk factor: a narrative review. Headache. (2021) 61(9):1306–13. doi: 10.1111/head.14213
4. International Association for the Study of Pain (IASP). Terminology. Available online at: https://www.iasp-pain.org/resources/terminology/ (accessed July 24, 2024).
5. Healthdirect Australia. Nerve pain (neuralgia) (2024). Available online at: https://www.healthdirect.gov.au/ (accessed July 24, 2024).
6. Timmerman H, Wilder-Smith OH, Steegers MA, Vissers KC, Wolff AP. The added value of bedside examination and screening QST to improve neuropathic pain identification in patients with chronic pain. J Pain Res. (2018) 11:1307–18. doi: 10.2147/JPR.S154698
7. Clark JR, Goodwin PC, Yeowell G. Exploring the pre-morbid contexts in which central sensitization developed in individuals with non-specific chronic low back pain. A qualitative study. Braz J Phys Ther. (2019) 23(6):516–26. doi: 10.1016/j.bjpt.2018.10.012
8. Aroke EN, Powell-Roach KL, Jaime-Lara RB, Tesfaye M, Roy A, Jackson P, et al. Taste the pain: the role of TRP channels in pain and taste perception. Int J Mol Sci. (2020) 21(16):5929. doi: 10.3390/ijms21165929
9. Nagarajan E, Kang SA, Holmes C, Govindarajan R. Clinical features with anti fibroblast growth factor receptor 3 (FGFR3) antibody-related polyneuropathy: a retrospective study. BMC Neurol. (2021) 21(1):74. doi: 10.1186/s12883-021-02090-2
10. Stucky CL, Mikesell AR. Cutaneous pain in disorders affecting peripheral nerves. Neurosci Lett. (2021) 765:136233. doi: 10.1016/j.neulet.2021.136233
11. Boehme R, van Ettinger-Veenstra H, Olausson H, Gerdle B, Nagi SS. Anhedonia to gentle touch in fibromyalgia: normal sensory processing but abnormal evaluation. Brain Sci. (2020) 10(5):306. doi: 10.3390/brainsci10050306
12. Brun C, McCabe CS, Mercier C. The contribution of motor commands to the perturbations induced by sensorimotor conflicts in fibromyalgia. Neuroscience. (2020) 434:55–65. doi: 10.1016/j.neuroscience.2020.03.017
13. Di Lernia D, Lacerenza M, Ainley V, Riva G. Altered interoceptive perception and the effects of interoceptive analgesia in musculoskeletal, primary, and neuropathic chronic pain conditions. J Pers Med. (2020) 10(4):201. doi: 10.3390/jpm10040201
14. Guerrero-Moreno A, Baudouin C, Melik Parsadaniantz S, Réaux-Le Goazigo A. Morphological and functional changes of corneal nerves and their contribution to peripheral and central sensory abnormalities. Front Cell Neurosci. (2020) 14:610342. doi: 10.3389/fncel.2020.610342
15. Shirvalkar P, Prosky J, Chin G, Ahmadipour P, Sani OG, Desai M, et al. First-in-human prediction of chronic pain state using intracranial neural biomarkers. Nat Neurosci. (2023) 26(6):1090–9. doi: 10.1038/s41593-023-01338-z
16. Peirs C, Dallel R, Todd AJ. Recent advances in our understanding of the organization of dorsal horn neuron populations and their contribution to cutaneous mechanical allodynia. J Neural Trans (Vienna, Austria: 1996). (2020) 127(4):505–25. doi: 10.1007/s00702-020-02159-1
17. Kim HJ, Ban MG, Yoon KB, Jeon W, Kim SH. Neuropathic-like pain symptoms and their association with muscle strength in patients with chronic musculoskeletal pain. J Clin Med. (2022) 11(18):5471. doi: 10.3390/jcm11185471
18. Dydyk AM, Givler A. Central Pain Syndrome. Treasure Island, FL: StatPearls Publishing LLC (2024).
19. van den Broeke EN, Hartgerink DM, Butler J, Lambert J, Mouraux A. Central sensitization increases the pupil dilation elicited by mechanical pinprick stimulation. J Neurophysiol. (2019) 121(5):1621–32. doi: 10.1152/jn.00816.2018
20. McMonnies CW. Could contact lens dryness discomfort symptoms sometimes have a neuropathic basis? Eye Vis (London, England). (2021) 8(1):12. doi: 10.1186/s40662-021-00236-4
21. Mikkonen J, Luomajoki H, Airaksinen O, Neblett R, Selander T, Leinonen V. Cross-cultural adaptation and validation of the finnish version of the central sensitization inventory and its relationship with dizziness and postural control. BMC Neurol. (2021) 21(1):141. doi: 10.1186/s12883-021-02151-6
22. Molot J, Sears M, Marshall LM, Bray RI. Neurological susceptibility to environmental exposures: pathophysiological mechanisms in neurodegeneration and multiple chemical sensitivity. Rev Environ Health. (2021) 37(4):509–30. doi: 10.1515/reveh-2021-0043
23. Torta DM, Filbrich L, Van Den Broeke EN, Legrain V. No perceptual prioritization of non-nociceptive vibrotactile and visual stimuli presented on a sensitized body part. Sci Rep. (2018) 8(1):5359. doi: 10.1038/s41598-018-23135-6
24. Kersch A, Perera P, Mercado M, Gorrie A, Sainsbury D, McGrath T, et al. Somatosensory testing in pediatric patients with chronic pain: an exploration of clinical utility. Children (Basel, Switzerland). (2020) 7(12):275. doi: 10.3390/children7120275
25. Colorado LH, Edwards K, Dinh L, Ha S, Liu D, Luu A, et al. Associations between the menstrual cycle, lifestyle factors and clinical assessment of the ocular surface: a prospective observational study. BMC Women’s Health. (2020) 20(1):23. doi: 10.1186/s12905-020-0894-z
26. Peinado-Rubia A, Osuna-Pérez MC, Rodríguez-Almagro D, Zagalaz-Anula N, López-Ruiz MC, Lomas-Vega R. Impaired balance in patients with fibromyalgia syndrome: predictors of the impact of this disorder and balance confidence. Int J Environ Res Public Health. (2020) 17(9):3160. doi: 10.3390/ijerph17093160
27. Dorris ER, Maccarthy J, Simpson K, McCarthy GM. Sensory perception quotient reveals visual, scent and touch sensory hypersensitivity in people with fibromyalgia syndrome. Front Pain Res (Lausanne, Switzerland). (2022) 3:926331. doi: 10.3389/fpain.2022.926331
28. Staud R, Godfrey MM, Robinson ME. Fibromyalgia patients are not only hypersensitive to painful stimuli but also to acoustic stimuli. J Pain. (2021) 22(8):914–25. doi: 10.1016/j.jpain.2021.02.009
29. Alshahrani MS, Reddy RS. Mediation effect of kinesiophobia on the relationship between cervical joint position sense and limits of stability in individuals with fibromyalgia syndrome: a cross-sectional study using mediation analysis. J Clin Med. (2023) 12(8):2791. doi: 10.3390/jcm12082791
30. Augière T, Desjardins A, Paquette Raynard E, Brun C, Pinard AM, Simoneau M, et al. Tactile detection in fibromyalgia: a systematic review and a meta-analysis. Front Pain Res (Lausanne, Switzerland). (2021) 2:740897. doi: 10.3389/fpain.2021.740897
31. Basha ME, Kellogg-Spadt S, Burrows LJ, Ruberu MS, Wallach AS, Nazar AM, et al. Thermal and mechanical pain thresholds of women with provoked localized vulvodynia: a pilot study. J Am Osteopath Assoc. (2019) 119(3):164–72. doi: 10.7556/jaoa.2019.027
32. Basso L, Boecking B, Brueggemann P, Pedersen NL, Canlon B, Cederroth CR, et al. Gender-specific risk factors and comorbidities of bothersome tinnitus. Front Neurosci. (2020) 14:706. doi: 10.3389/fnins.2020.00706
33. Bellan V, Braithwaite FA, Wilkinson EM, Stanton TR, Moseley GL. Where is my arm? Investigating the link between complex regional pain syndrome and poor localisation of the affected limb. PeerJ. (2021) 9:e11882. doi: 10.7717/peerj.11882
34. Berryman C, Wallwork SB, Heredia-Rizo AM, Knight E, Camfferman D, Russek L, et al. Are you listening? Facilitation of the auditory blink response in people with fibromyalgia. J Pain. (2021) 22(9):1072–83. doi: 10.1016/j.jpain.2021.03.141
35. Berwick RJ, Andersson DA, Goebel A, Marshall A. Aftersensations and lingering pain after examination in patients with fibromyalgia syndrome. Pain Med (Malden, Mass.). (2022) 23(12):1928–38. doi: 10.1093/pm/pnac089
36. Brun C, Giorgi N, Pinard AM, Gagné M, McCabe CS, Mercier C. Exploring the relationships between altered body perception, limb position sense, and limb movement sense in Complex regional pain syndrome. J Pain. (2019) 20(1):17–27. doi: 10.1016/j.jpain.2018.07.008
37. Delussi M, Laporta A, Fraccalvieri I, de Tommaso M. Osmophobia in primary headache patients: associated symptoms and response to preventive treatments. J Headache Pain. (2021) 22(1):109. doi: 10.1186/s10194-021-01327-2
38. De Meulemeester K, Meeus M, De Pauw R, Cagnie B, Keppler H, Lenoir D. Suffering from chronic tinnitus, chronic neck pain, or both: does it impact the presence of signs and symptoms of central sensitization? PLoS One. (2023) 18(8):e0290116. doi: 10.1371/journal.pone.0290116
39. Di Pietro F, Lee B, Henderson LA. Altered resting activity patterns and connectivity in individuals with complex regional pain syndrome. Hum Brain Mapp. (2020) 41(13):3781–93. doi: 10.1002/hbm.25087
40. Gossrau G, Klimova A, Lapp HS, Frost M, Peschel E, Weidner K, et al. C-tactile touch perception in patients with chronic pain disorders. Pain Reports. (2021) 6(2):e941. doi: 10.1097/PR9.0000000000000941
41. Grayston R, Czanner G, Elhadd K, Goebel A, Frank B, Üçeyler N, et al. A systematic review and meta-analysis of the prevalence of small fiber pathology in fibromyalgia: implications for a new paradigm in fibromyalgia etiopathogenesis. Semin Arthritis Rheum. (2019) 48(5):933–40. doi: 10.1016/j.semarthrit.2018.08.003
42. Habig K, Lautenschläger G, Maxeiner H, Birklein F, Krämer HH, Seddigh S. Low mechano-afferent fibers reduce thermal pain but not pain intensity in CRPS. BMC Neurol. (2021) 21(1):272. doi: 10.1186/s12883-021-02304-7
43. Harte SE, Wiseman J, Wang Y, Smith AR, Yang CC, Helmuth M, et al. Experimental pain and auditory sensitivity in overactive bladder syndrome: a symptoms of the lower urinary tract dysfunction research network (LURN) study. J Urol. (2022) 207(1):161–71. doi: 10.1097/JU.0000000000002147
44. Hartmann A, Welte-Jzyk C, Schmidtmann I, Geber C, Al-Nawas B, Daubländer M. Somatosensory and gustatory profiling in the orofacial region. Diagnostics (Basel, Switzerland). (2022) 12(12):3198. doi: 10.3390/diagnostics12123198
45. Houghton DC, Uhde TW, Borckardt JJ, Cortese BM. Exploratory investigation of a brief cognitive behavioral intervention and transcranial direct current stimulation on odor sensitivity. Psychosom Med. (2019) 81(4):389–95. doi: 10.1097/PSY.0000000000000679
46. Hulens M, Dankaerts W, Rasschaert R, Bruyninckx F, De Mulder P, Bervoets C. The link between empty sella syndrome, fibromyalgia, and chronic fatigue syndrome: the role of increased cerebrospinal fluid pressure. J Pain Res. (2023) 16:205–19. doi: 10.2147/JPR.S394321
47. Jensen OK, Nielsen CV, Stengaard-Pedersen K. Diffuse central sensitization in low back patients: a secondary analysis of cross-sectional data including tender point examination and magnetic resonance imaging of the lumbar spine. Medicine (Baltimore). (2020) 99(38):e22198. doi: 10.1097/MD.0000000000022198
48. Junad K, Ruchika S, Moin A, Mythili K. Duloxetine for the management of sensory and taste alterations, following iatrogenic damage of the lingual and chorda tympani nerve. Scand J Pain. (2020) 21(1):194–9. doi: 10.1515/sjpain-2020-0066
49. Kim MJ, Kho HS. Understanding of burning mouth syndrome based on psychological aspects. Chin J Dent Res. (2018) 21(1):9–19. doi: 10.3290/j.cjdr.a39914
50. King S, Priesol AJ, Davidi SE, Merfeld DM, Ehtemam F, Lewis RF. Self-motion perception is sensitized in vestibular migraine: pathophysiologic and clinical implications. Sci Rep. (2019) 9(1):14323. doi: 10.1038/s41598-019-50803-y
51. Koca TT, Seyithanoglu M, Sagiroglu S, Berk E, Dagli H. Frequency of audiological complaints in patients with fibromyalgia syndrome and its relationship with oxidative stress. Niger J Clin Pract. (2018) 21(10):1271–7. doi: 10.4103/njcp.njcp_95_18
52. Kuttikat A, Noreika V, Chennu S, Shenker N, Bekinschtein T, Brown CA. Altered neurocognitive processing of tactile stimuli in patients with Complex regional pain syndrome. J Pain. (2018) 19(4):395–409. doi: 10.1016/j.jpain.2017.11.008
53. Le TP, Tzeng YL, Muo CH, Ting H, Sung FC, Lee SD, et al. Risk of hearing loss in patients with fibromyalgia: a nationwide population-based retrospective cohort study. PLoS One. (2020) 15(9):e0238502. doi: 10.1371/journal.pone.0238502
54. Lunden LK, Kleggetveit IP, Schmelz M, Jorum E. Cold allodynia is correlated to paroxysmal and evoked mechanical pain in complex regional pain syndrome (CRPS). Scand J Pain. (2022) 22(3):533–42. doi: 10.1515/sjpain-2021-0208
55. Mason KJ, O'Neill TW, Lunt M, Jones AKP, McBeth J. Psychosocial factors partially mediate the relationship between mechanical hyperalgesia and self-reported pain. Scand J Pain. (2018) 18(1):59–69. doi: 10.1515/sjpain-2017-0109
56. Martín-Martínez JP, Collado-Mateo D, Domínguez-Muñoz FJ, Villafaina S, Gusi N, Pérez-Gómez J. Reliability of the 30 s chair stand test in women with fibromyalgia. Int J Environ Res Public Health. (2019) 16(13):2344. doi: 10.3390/ijerph16132344
57. Martínez E, Aira Z, Buesa I, Aizpurua I, Rada D, Azkue JJ. Embodied pain in fibromyalgia: disturbed somatorepresentations and increased plasticity of the body schema. PLoS One. (2018) 13(4):e0194534. doi: 10.1371/journal.pone.0194534
58. Mikkonen J, Leinonen V, Kaski D, Hartvigsen J, Luomajoki H, Selander T, et al. Postural sway does not differentiate individuals with chronic low back pain, single and multisite chronic musculoskeletal pain, or pain-free controls: a cross-sectional study of 229 subjects. Spine J. (2022) 22(9):1523–34. doi: 10.1016/j.spinee.2022.04.013
59. Mingels S, Dankaerts W, van Etten L, Bruckers L, Granitzer M. Spinal postural variability relates to biopsychosocial variables in patients with cervicogenic headache. Sci Rep. (2021) 11(1):13783. doi: 10.1038/s41598-021-93138-3
60. Özsoy-Ünübol T, Kullakçi H, Ilhan İ, Yilmaz F. Evaluation of olfactory and gustatory functions in patients with fibromyalgia syndrome: its relationship with anxiety, depression, and alexithymia. Arch Rheumatol. (2020) 35(4):584–91. doi: 10.46497/ArchRheumatol.2020.7833
61. Rasouli O, Vasseljen O, Fors EA, Lorås HW, Stensdotter AK. Lower regulatory frequency for postural control in patients with fibromyalgia and chronic fatigue syndrome. PLoS One. (2018a) 13(4):e0195111. doi: 10.1371/journal.pone.0195111
62. Rasouli O, Fors EA, Vasseljen O, Stensdotter AK. A concurrent cognitive task does not perturb quiet standing in fibromyalgia and chronic fatigue syndrome. Pain Res Manag. (2018b) 2018:9014232. doi: 10.1155/2018/9014232
63. Reddy RS, Tedla JS, Dixit S, Raizah A, Al-Otaibi ML, Gular K, et al. Cervical joint position sense and its correlations with postural stability in subjects with fibromyalgia syndrome. Life (Basel, Switzerland). (2022) 12(11):1817. doi: 10.3390/life12111817
64. Sempere-Rubio N, López-Pascual J, Aguilar-Rodríguez M, Cortés-Amador S, Espí-López G, Villarrasa-Sapiña I, et al. Characterization of postural control impairment in women with fibromyalgia. PLoS One. (2018) 13(5):e0196575. doi: 10.1371/journal.pone.0196575
65. Sempere-Rubio N, Aguilar-Rodríguez M, Inglés M, Izquierdo-Alventosa R, Serra-Añó P. Physical condition factors that predict a better quality of life in women with fibromyalgia. Int J Environ Res Public Health. (2019) 16(17):3173. doi: 10.3390/ijerph16173173
66. Shiro Y, Nagai S, Hayashi K, Aono S, Nishihara M, Ushida T. Changes in visual attentional behavior in complex regional pain syndrome: a preliminary study. PLoS One. (2021) 16(2):e0247064. doi: 10.1371/journal.pone.0247064
67. Tuncer M, Çoban K, Erbek SS, Erbek HS. Audiovestibular dysfunction in patients with fibromyalgia syndrome. J Int Adv Otol. (2021) 17(4):348–52. doi: 10.5152/JIAO.2021.8709
68. Verfaille C, Filbrich L, Cordova Bulens D, Lefèvre P, Berquin A, Barbier O, et al. Robot-assisted line bisection in patients with complex regional pain syndrome. PLoS One. (2019) 14(5):e0213732. doi: 10.1371/journal.pone.0213732
69. Villafaina S, Gusi N, Rodriguez-Generelo S, Martin-Gallego JD, Fuentes-García JP, Collado-Mateo D. Influence of a cell-phone conversation on balance performance in women with fibromyalgia: a cross-sectional descriptive study. BioMed Res Int. (2019) 2019:5132802. doi: 10.1155/2019/5132802
70. Wang AP, Butler AA, Valentine JD, Rae CD, McAuley JH, Gandevia SC, et al. A novel finger illusion reveals reduced weighting of bimanual hand cortical representations in people with complex regional pain syndrome. J Pain. (2019) 20(2):171–80. doi: 10.1016/j.jpain.2018.08.008
71. Wang D, Merkle SL, Lee JE, Sluka KA, Rakel B, Graven-Nielsen T, et al. Multisensory sensitivity is related to deep-tissue but not cutaneous pain sensitivity in healthy individuals. J Pain Res. (2020) 13:2493–508. doi: 10.2147/JPR.S267972
72. Wang D, Casares S, Eilers K, Hitchcock S, Iverson R, Lahn E, et al. Assessing multisensory sensitivity across scales: using the resulting core factors to create the multisensory amplification scale. J Pain. (2022) 23(2):276–88. doi: 10.1016/j.jpain.2021.07.013
73. Pujol J, Blanco-Hinojo L, Doreste A, Ojeda F, Martínez-Vilavella G, Pérez-Sola V, et al. Distinctive alterations in the functional anatomy of the cerebral cortex in pain-sensitized osteoarthritis and fibromyalgia patients. Arthritis Res Ther. (2022) 24(1):252. doi: 10.1186/s13075-022-02942-3
74. Lindheimer JB, Stegner AJ, Ellingson-Sayen LD, Van Riper SM, Dougherty RJ, Falvo MJ, et al. Influence of pain anticipation on brain activity and pain perception in gulf war veterans with chronic musculoskeletal pain. Psychophysiology. (2019) 56(12):e13452. doi: 10.1111/psyp.13452
75. Lin JH, Hung CH, Han DS, Chen ST, Lee CH, Sun WZ, et al. Sensing acidosis: nociception or sngception? J Biomed Sci. (2018) 25(1):85. doi: 10.1186/s12929-018-0486-5
76. Lee JA, Chen Q, Zhuo M. Synaptic plasticity in the pain-related cingulate and insular cortex. Biomedicines. (2022) 10(11):2745. doi: 10.3390/biomedicines10112745
77. Osumi M, Sumitani M, Otake Y, Imai R, Morioka S. Fear of movement disturbs inter-limb coupling in complex regional pain syndrome. Ann Phys Rehabil Med. (2020) 63(3):258–61. doi: 10.1016/j.rehab.2019.08.002
78. Tanaka N, Atesok K, Nakanishi K, Kamei N, Nakamae T, Kotaka S, et al. Pathology and treatment of traumatic cervical spine syndrome: whiplash injury. Adv Orthop. (2018) 2018:4765050. doi: 10.1155/2018/4765050
79. Pupić-Bakrač J, Pupić-Bakrač A. Comorbidity of chronic tinnitus and psychological stress—which came first, the chicken or the egg? Psychiatr Danub. (2020) 32(Suppl 4):412–9.
80. Sehgal N, Gordon DB, Hetzel S, Backonja MM. Colored pain drawing as a clinical tool in differentiating neuropathic pain from non-neuropathic pain. Pain Medicine (Malden, Mass.). (2021) 22(3):596–605. doi: 10.1093/pm/pnaa375
81. Hackshaw KV. The search for biomarkers in fibromyalgia. Diagnostics (Basel, Switzerland). (2021) 11(2):156. doi: 10.3390/diagnostics11020156
82. Islam B, Stephenson J, Young B, Manca M, Buckley DA, Radford H, et al. The identification of blood biomarkers of chronic neuropathic pain by comparative transcriptomics. NeuroMol Med. (2022) 24(3):320–38. doi: 10.1007/s12017-021-08694-8
83. Pricope CV, Tamba BI, Stanciu GD, Cuciureanu M, Neagu AN, Creanga-Murariu I, et al. The roles of imaging biomarkers in the management of chronic neuropathic pain. Int J Mol Sci. (2022) 23(21):13038. doi: 10.3390/ijms232113038
84. Saloman JL, Li Y, Stello K, Li W, Li S, Phillips AE, et al. Serum biomarkers of nociceptive and neuropathic pain in chronic pancreatitis. J Pain. (2023) 24(12):2199–210. doi: 10.1016/j.jpain.2023.07.006
85. Diaz MM, Caylor J, Strigo I, Lerman I, Henry B, Lopez E, et al. Toward composite pain biomarkers of neuropathic pain-focus on peripheral neuropathic pain. Front Pain Res (Lausanne, Switzerland). (2022) 3:869215. doi: 10.3389/fpain.2022.869215
86. Favretti M, Iannuccelli C, Di Franco M. Pain biomarkers in fibromyalgia syndrome: current understanding and future directions. Int J Mol Sci. (2023) 24(13):10443. doi: 10.3390/ijms241310443
87. Wagenaar OVG, Schubert NMA, van Rood YR, Rosmalen JGM. Factors associated with self rated health in persons with tinnitus from the general population. J Psychosom Res. (2022) 153:110693. doi: 10.1016/j.jpsychores.2021.110693
88. Meulders A. Fear in the context of pain: lessons learned from 100 years of fear conditioning research. Behav Res Ther. (2020) 131:103635. doi: 10.1016/j.brat.2020.103635
89. Di Stefano V, Iacono S, Gagliardo A, Maggio B, Guggino G, Gangitano M, et al. Sound-induced flash illusions support cortex hyperexcitability in fibromyalgia. Pain Res Manag. (2022) 2022:7355102. doi: 10.1155/2022/7355102
Keywords: central sensitization, fibromyalgia, complex regional pain syndrome, neuropathic pain, vision, audition, olfaction, touch
Citation: Quodling N, Hoffman N, Carrick FR and Jemni M (2025) Sensory processing in medically unexplained pain syndrome. A systematic review. Front. Pain Res. 6:1584227. doi: 10.3389/fpain.2025.1584227
Received: 27 February 2025; Accepted: 20 May 2025;
Published: 6 June 2025.
Edited by:
Paul Geha, University of Rochester, United StatesReviewed by:
Mohamed Ahmed Hefny, Suez Canal University, EgyptPatricia Silva Santos Ribeiro, Erasmus Medical Center, Netherlands
Copyright: © 2025 Quodling, Hoffman, Carrick and Jemni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicole Quodling, bmljcXVvZEBnbWFpbC5jb20=
†ORCID:
Nicole Quodling
orcid.org/0009-0007-6757-514X
Norman Hoffman
orcid.org/0000-0002-0958-5717
Frederick Robert Carrick
orcid.org/0000-0002-2818-6551
Monèm Jemni
orcid.org/0000-0001-5410-9085