 Robin Conen
Robin Conen Nikolai Hepke2,†
Nikolai Hepke2,† Ana N. Tibubos
Ana N. Tibubos- 1Department of Diagnostics in Healthcare & eHealth, Trier University, Trier, Germany
- 2Department of Computer Science, Trier University of Applied Sciences, Trier, Germany
- 3Department of Computer Science/Therapeutic Sciences, Trier University of Applied Sciences, Trier, Germany
- 4Department of Psychosomatic Medicine and Psychotherapy, University Medical Center Mainz, Mainz, Germany
Background: Chronic low back pain (CLBP) is prevalent and a multimodal therapy is indicated, including psychological treatment. Effective conventional treatments involve psychoeducation and mindfulness-based body scans, while virtual reality offers superior but temporary pain relief. Augmented Reality (AR), which combines conventional and virtual methods, is a novel therapeutic strategy.
Methods: We investigated the viability and acceptability of an AR intervention for CLBP by incorporating psychoeducation and mindfulness-based body scan techniques. 40 participants in two studies with a one-arm design underwent an educational AR intervention (Study I, n1 = 18) and an enhanced version with an additional body scan (Study II, n2 = 22). The studies focused on evaluating technical feasibility and multiple facets of user experience.
Results: The results demonstrated high feasibility with low dropout rates (Study I: 10%, Study II: 0%). User experience ratings ranged from “Above Average” to “Excellent,” with the advanced intervention receiving higher ratings. While Study I showed no significant changes in affect pre- vs. post-intervention, Study II exhibited a significant reduction in negative affect and improved valence. Qualitative analysis provided insights into technical requirements and user perceptions.
Discussion: The AR prototype emerges as a promising psychoeducational tool for CLBP, aligning with current treatment guidelines and providing a basis for future controlled clinical trials. Limitations include the absence of a high-pain intervention group, as Study I reported a pain intensity of M = 1.05 and Study II reported M = 1.77 (Range: 0–10). Further research such as clinical trials with control groups is required to validate the efficacy of the piloted approach. The AR-based psychoeducation and mindfulness body scan intervention for CLBP demonstrated technical feasibility and a good user experience.
Clinical Trial Registration: Open Science Framework.io; https://doi.org/10.17605/OSF.IO/DSW5X and https://doi.org/10.17605/OSF.IO/XVJBZ
1 Introduction
Worldwide, low back pain (LBP) affects 60%–80% of the adult population, with 10% progressing to chronic conditions (CLBP) (1). Among these chronic cases, 85% are categorized as chronic non-specific low back pain, lacking a clear cause (2). Given limited effectiveness and potential side effects of medication-based treatments, there is a growing demand for non-pharmacological alternatives (3) to enhance treatment outcomes and develop effective behavioral interventions (4). Current treatment guidelines recommend behavioral changes, physical activity, psychoeducation (5), and physiotherapy targeting at strengthening and stabilisation trunk muscles (6, 7) to alleviate pain and improve function. Educational intervention encompasses targeted strategies within an educational framework, designed to achieve specific objectives by utilizing resources informed by educational knowledge and the education system (8), without a primary focus on mental health. Psychoeducation, on the other hand, is a distinct therapeutic approach that integrates educational methods with cognitive behavioral therapy to impart knowledge about mental illness to patients (9). In the context of CLBP, the objective of psychoeducation is to elucidate the biopsychosocial interactions contributing to pain development, educate on risk factors such as catastrophizing, avoidance, and negative beliefs about pain, and to advocate for self-management strategies (10). Psychoeducational interventions improve disease understanding and promote coping mechanisms, physical activity, quality of life, and symptom management (11, 12). Psychoeducation strengthens self-efficacy and interrrupts the fear-pain cycle (13, 14). An additional treatment approach is mindfulness-based stress reduction (MBSR), particularly the body scan technique, which can reduce negative emotions, pain, anxiety, and pain perception in older adults with CLBP (15).
With the advancement of healthcare digitalization, novel non-pharmacological interventions, such as virtual reality treatments, has been developed, demonstrating superior effects compared to conventional therapies in the treatment of CLBP (16). Immersive technologies are categorized along the reality-virtuality continuum described by Milgram and Kishino (17). These technologies encompass visual displays ranging from real to virtual environments, including Augmented Reality (AR) and Virtual Reality (VR) (18–20). AR enables simultaneous interaction between digital and physical elements in real-time. Conversely, VR offers full immersion in virtual realities and represents the extremes of this continuum (21, 22). VR was found to shift attention away from pain to more pleasant visual, tactile, and auditory stimuli, thereby reducing pain intensity, catastrophizing, and associated psychological symptoms in CLBP patients (19, 23, 24). A meta-analysis found that VR training may mitigate kinesiophobia and pain intensity in CLBP (25). Initial psychoeducational VR training programs demonstrated a game-based approach to interactive knowledge transfer, albeit with only short-term pain relief (26), as well as the feasibility of immersive VR programs for pain neuroscience education (54). Thus, immersion and user focus in VR can support mindfulness and enhance pain management (27). 360-degree nature scenes promoted relaxation techniques (28) and illustrated the benefits of immersion in CLBP. A recent review article on VR for the treatment of CLBP treatment presented substantial evidence supporting its safety and tolerability (60). However, it highlighted methodological limitations and the predominance of short-term effects. This review recommends further research on safety, acceptance, and satisfaction, including targeted investigations of the risks of VR-induced spinal pain.
While VR has demonstrated positive outcomes in alleviating CLBP symptoms, AR remains underexplored despite its potential additional benefits. AR overlays virtual elements into the physical world, allowing seamless coexistence and real-time interaction, while reducing issues such as cybersickness and visual discomfort (29). Overall, AR enhances the incorporation of the real environment and body, strengthens embodiment, and provides a more authentic experience (30).
Despite these findings and advancements, a recent scoping review identified a significant research gap regarding the efficacy and feasibility of AR-based interventions for CLBP, particularly those integrating conventional and VR approaches (31). Grounded in the Unified Theory of Acceptance and Use of Technology by Venkatesh et al. (32), the review offers theory-driven recommendations for designing AR interventions for psychoeducation and MBSR-based body scans relaxation training. Thus, study aimed to assess the feasibility, acceptability, and potential benefits of AR in psychoeducational and mindfulness-based interventions for CLBP, bridging the research gap and laying the groundwork for clinical trials. The feasibility study focused on individuals with CLBP undergoing an psychoeducational AR intervention (Study I) or an enhanced version incorporating a body scan (Study II), assessing technical feasibility and facets of user experience. We formulated two hypotheses (H): An AR intervention for CLBP is technically feasible with an attrition rate of less than 50% (H1), in particular psychoeducation (H1a) and psychoeducation in combination with a MBSR body scan (H1b). Furthermore, we expect a positive user experience in AR (H2) both psychoeducation (H2a) and its combination with a MBSR body scan (H2b).
2 Materials and methods
2.1 Study design and study procedure
Two one-arm feasibility studies, with a pre-post design, investigated two scenarios: Study I (Psychoeducation) and Study II (Psychoeducation + Body Scan). The research was collaboratively designed and conducted by Trier University and Trier University of Applied Sciences and was carried out in the VR-AR laboratories of Trier University. Participants were informed that the aim of the feasibility study was to assess the technical implementation of an AR intervention for CLBP as a foundation for a subsequent clinical trial. Sociodemographic data (age, sex, height, weight, psychoeducation, marital status, and duration of back pain) and pain intensity data were collected before the intervention using questionnaires. In Study I, questionnaires were administered in AR environment. Due to hand-tracking issues with Microsoft HoloLens 2 ® and subsequent prolonged completion times, paper-pencil questionnaires were administered in Study II. Both studies evaluated the (a) dropout rate and (b) user experience. For the feasibility evaluation a dropout rate of <50% considered a feasibility success. User experience was assessed in both studies using a user experience questionnaire (post) and changes in psychological variables, in particular pain and mood (pre and post). In Study II, we added an interview with open-ended response format following the intervention to gain further insights on user experience.
2.2 Participants
For the feasibility study, a total of 42 participants were recruited across two studies: Study I included n1 = 20 participants (14 females, 6 males; 24–74 years, M = 37.50, SD = 15.79) and Study II n2 = 22 participants (13 females, 9 males; 20–67 years, M = 39.63, SD = 15.47). The final sample size in Study I decreased to 18 participants (n1 = 18) after excluding two individuals due to subclinical rheumatic complaints and migraine symptoms during the intervention period. Inclusion criteria were age of majority, proficiency in German language, and CLBP pain intensity of below 4 on the numerical rating scale (range 0–10), as scores of 4 and above were considered moderate pain (26, 33). As this investigation constitutes a technical feasibility study, it exclusively included participants with CLBP scores below 4 on a 0–10 numerical scale. This criterion was employed to prevent the inclusion of individuals experiencing moderate pain, defined as scores of 4 or higher (26), thereby avoiding the imposition of undue burden on patients with severe pain. CLBP is characterized by a duration of at least three months (1, 34). Exclusion criteria comprised medical and psychotherapeutic conditions (e.g., schizophrenia or epilepsy) and health limitations affecting physical activity. The criteria for inclusion and exclusion were disseminated through recruitment flyers, requested via telephone during the appointment scheduling process, and subsequently verified on-site prior to the commencement of the intervention. The sample size of each study exceeded the minimum of 12 participants recommended for pilot studies (35). No formal sample size calculation was performed, as this study was designed as a pilot.
2.3 Measurements
2.3.1 User experience
For user experience evaluation of the psychoeducational intervention in Study I, a 13-item short version of the User Experience Questionnaire [UEQ; (64)] was employed to assess attractiveness, pragmatic quality, and hedonic quality [UEX; (36)]. In Study II, the original 26-item UEQ version (64) was utilized to evaluate the enhanced AR-based psychoeducational prototype with body scan, which distinguishes between attractiveness, pragmatic quality (comprehensibility, efficiency, and reliability), and hedonic quality (stimulation and novelty). The UEQ showed good internal consistency, with Cronbach's alpha ranging from 0.65 to 0.89 (64). Both questionnaires utilized a response scale ranging from −3 (“most negative”) to +3 (“most positive”).
2.3.2 Pain intensity
The Numeric Rating Scale [NRS; (37)] is a validated questionnaire consisting of a single item that assesses the pain intensity (PI) of CLBP on a scale from 0 (“no pain”) to 10 (“worst pain”). The NRS exhibits excellent test-retest reliability, intraclass correlation coefficient and strong convergent validity with the Visual Analog Scale (VAS), with a correlation coefficient of 0.93 (38).
2.3.3 Mood
The short scale for assessing positive activation, negative activation, and valence in experience-sampling studies [PANAVA-KS; (39)] is a bipolar tool for mood evaluation. Valence reflects the hedonic tone of an emotional experience and complements the activation dimensions of positive and negative affect. Participants rated their pre-intervention feelings using two valence items and four items each for negative and positive affect on a 7-point scale ranging from −3 to +3. The interpretation of the scores varied across subscales. Lower (negative values) values of valence and positive affect scores indicate a decline in mood, whereas lower (negative) affect scores indicate less negative emotions, hence better mood. The tool demonstrated high reliability, with Cronbach's alpha ranging from .92 to .94.
2.3.4 Interview questions
In semi-structured interviews, the subjective experiences of participants were captured using a tailored interview guide based on a translated and adapted study of VR applications for patients with CLBP (40) with an open-ended response format. The questions from Smits et al. (40) were translated from English to German and adjusted for the AR application, resulting in the following revised questions: (1) What are your thoughts about AR usage? (2) Where and when do you use AR? (3) Does AR affect your sense of security? (4) How do you rate the comfort of the AR experience? (5) What is your ideal AR experience? (6) Would you use AR as a tool in future inquiries?
2.4 Interventions
The development of the interventions for Studies I and II was based on a scoping review (31), which incorporated the Unified Theory of Acceptance and Use of Technology (32) and the Health Action Process Approach (41, 42) for the psychoeducational treatment development in AR. The resulting recommendations pertained to the psychoeducational content, psychological learning factors, technical framework conditions, and outcome variables of pain-psychological interventions for AR as key domains. The interventions of Studies I and II were conducted once and lasted approximately 40 min. AR was used to facilitate knowledge about CLBP. Table 1 outlines the intervention procedure for Study I.
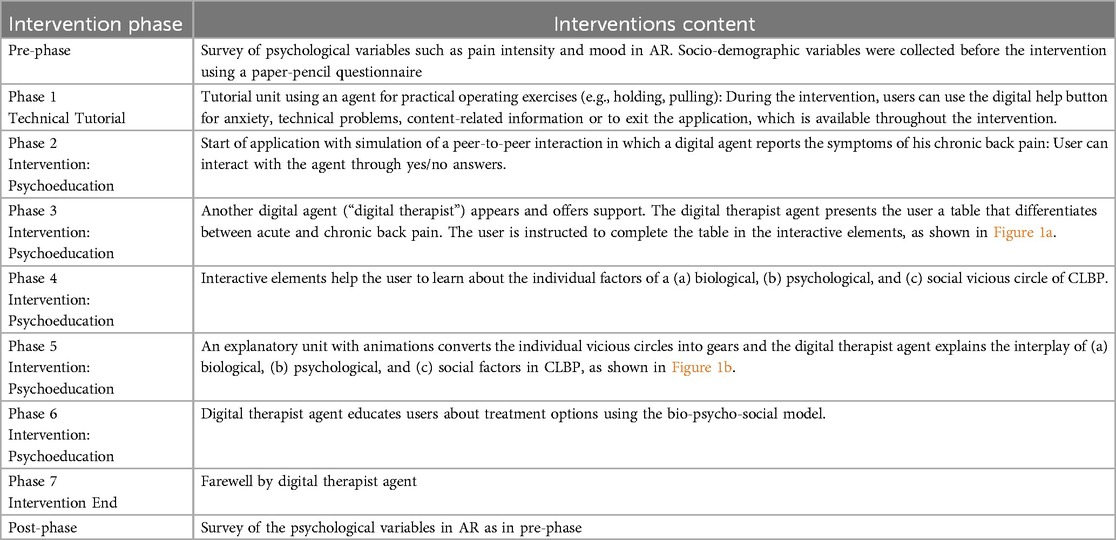
Table 1. Study flow of the assessment and psychoeducation intervention tailored for chronic low back pain (CLBP) in augmented reality (AR) using the Microsoft HoloLens 2 ®.
The intervention in Study II was extended to address the relationship between stress and CLBP and integrated the Body Scan technique according to Kabat-Zinn (43, 44) for stress reduction in a digital forest landscape. Table 2 delineates the intervention procedure for Study II.
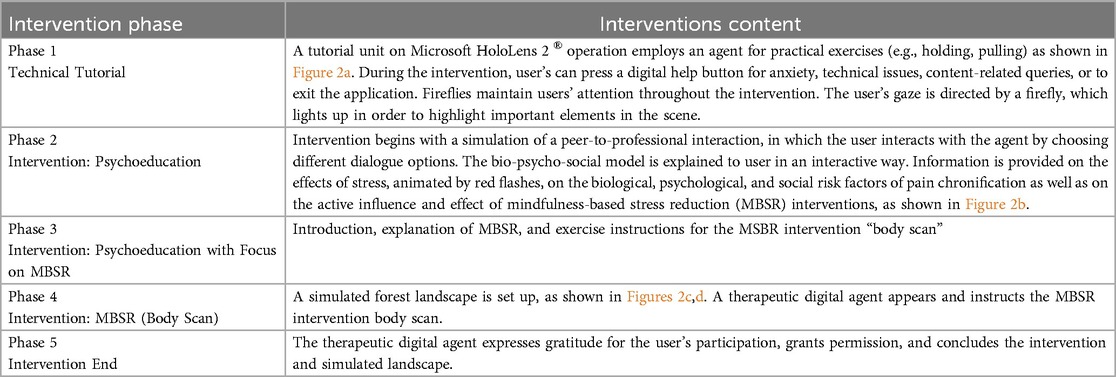
Table 2. Psychoeducation in combination with a mindfulness body scan tailored for chronic low back pain (CLBP) in sugmented reality (AR).
In contrast to Study I, Study II featured an interactive tutorial video that guided users in the operation of the Microsoft HoloLens 2 ®, such as grasping and pulling, prior to the intervention. The tutorial aimed to prevent users from leaving the tracking area during grasping movements and to avoid the snapping back of virtual elements. Additionally, the limited field of view of the HoloLens 2, which made orientation in real space more challenging, was considered in the design. A digital firefly was implemented to direct users' attention toward the positioning of virtual elements in real space, ensuring a seamless intervention process. Figures 1, 2 illustrate the corresponding AR intervention images.
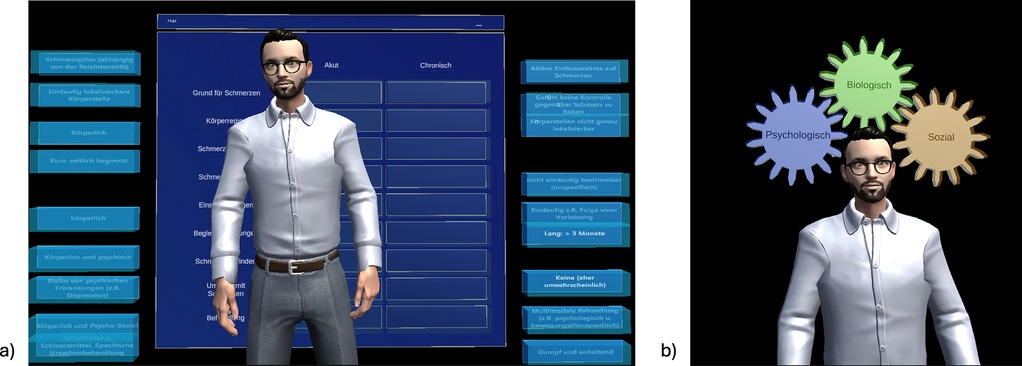
Figure 1. Agent with interactive exercise (table) for differentiating acute vs. chronic back pain (a) and explanation of animated bio-psycho-social model (b).
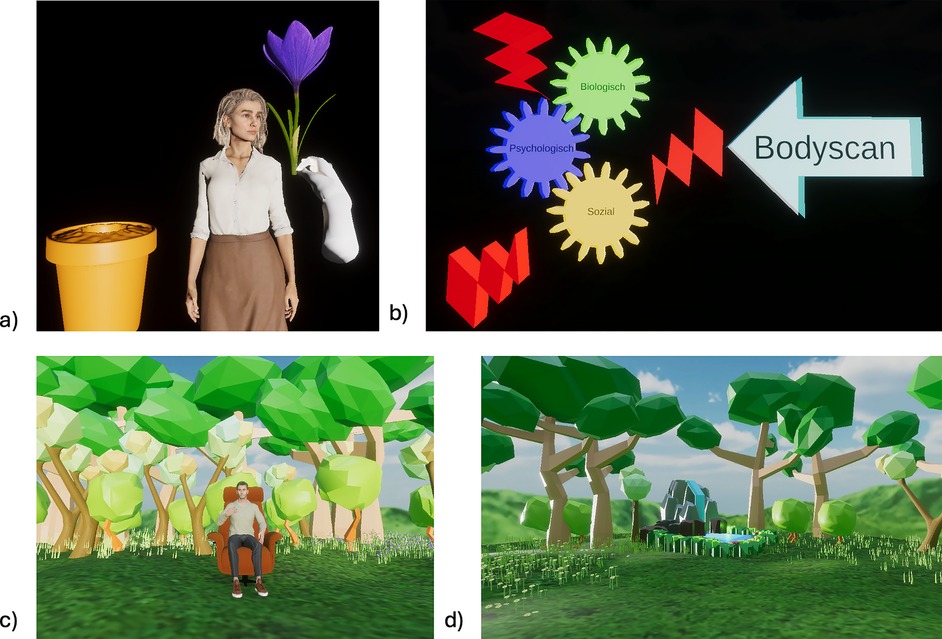
Figure 2. An agent with an interactive module for Microsoft HoloLens 2 ® (a) and a psychoeducational tool illustrating the impact of stress on chronic low back pain through a bio-psycho-social framework (b), including a body scan intervention conducted in an augmented reality forest landscape (c,d).
2.4.1 Technical implementation of psychoeducation and MBSR in augmented reality
We used Microsoft HoloLens 2®, whose transparent displays allowed users to see their real environment as if they were not wearing a head-mounted display (HMD). The virtual environment was overlaid and spatially mapped onto the real world, enabling a concurrent experience. The HMD's depth sensors enabled interactions between physical and virtual objects, such as physical objects occluding digital objects or virtual objects interacting with physical surfaces. Reports indicate minimal simulator sickness with the use of the HoloLens (45), which is a notable advantage over VR, in which motion sickness is more prevalent (46, 47). Users interact with virtual objects by tapping or grabbing them with their hands (48). A tutorial scene (Figure 2a) was developed to teach users the necessary hand gestures. The application, developed using Unity 2021.3 and Microsoft's Mixed Reality Toolkit, runs natively on a Windows PC and streams to the HoloLens via the holographic remoting app (49), using the host computer's graphics processing for high-fidelity 3D models and advanced lighting. The investigator was able to view the AR scene from the participants' perspective on the monitor. Users encountered photorealistic characters created and animated with Character Creator 4, featuring blend shapes and rigged bones for facial expressions and realistic lip-syncing. The participants experienced a calming forest environment, with the HoloLens screen adjusted to a high opacity level for enhanced immersion.
2.5 Data analysis
The feasibility and user experience of AR interventions tailored for CLBP were quantitatively analyzed using SPSS Statistics version 28.0.1.1 for Windows except for the interview questions. Hypothesis 1 assessed technical feasibility based on dropout rates. Hypothesis 2 regarding user experience of the prototypes was evaluated by comparing the user experience scores in the two studies with benchmark values provided by Schrepp et al. (50). Further aspects of user experience such as change of pain intensity and mood was analyzed in Study I using the Wilcoxon Signed-Rank Test using SPSS's exact test (1-sided), as the due to violation of the normal distribution, and in Study II using paired t-tests as normal distribution of the pre-post analysis variables were given. For the statistical tests and interpretation, a significance level of α = .05 (1-sided) was employed, the Bonferroni correction was implemented by multiplying the p-values with the number of tests conducted (factor 8, due to two tests per variable), and Cohen's d effect sizes (51) were utilized. All reported p-values are Bonferroni-corrected unless stated otherwise. User experience data based from semi-structured interviews were analyzed via thematic analyses for each question to explore participants' perceptions and behaviors (52).
3 Results
Both samples included 13 master's and 10 bachelor's degree holders, eight secondary, seven middle school, and two basic secondary graduates. Pain duration deviated significantly from a normal distribution in both studies (p < .001), with a mean duration of 1.80 months (SD = 8.05) in Study I and 53.90 months (SD = 105.28) in study II. Pre-intervention pain intensity was M = 1.05 (SD = 1.98) in Study I and M = 1.77 (SD = 1.34) in Study II. A detailed overview of the sample statistics is provided in Supplementary Appendix 1.
3.1 Feasibility (dropout rate) of augmented reality intervention
The technical feasibility of AR interventions was evaluated based on the dropout rate of less than 50% (H1). In Study 1 (n1 = 18), 18 out of 20 participants (90%) successfully completed the psychoeducational AR intervention, while two (10%) discontinued the intervention due to migraine and hand pain (H1a). In Study II, all participants (n2 = 22) successfully completed the AR intervention, resulting in a dropout rate of 0% (H1b). These results rendered support for hypothesis 1 postulating the technical feasibility of an AR intervention adapted for CLBP, in particular a psychoeducational intervention (H1a) and psychoeducation combined with a MBSR-based body scan (H1b).
In Study I, the technical feasibility of administering questionnaires in AR was also assessed. The low attrition rate suggests that questionnaires can be administered in the AR environment and were deemed acceptable by the study participants. However, participants were often frustrated with the handtracking of the hololens during the AR-questionaire. Therefore, we decided to use the pencil-and-paper questionnaire for the second study. Psychometric analysis of the scales showed similar results to conventional assessments. Scale statistic (e.g., internal consistency) are presented in Supplementary Appendix 2.
3.2 User experience of augmented reality intervention
Hypothesis 2 examined the user experience of the psychoeducational AR intervention (H2a, Study I) and the user experience of the advanced psychoeducational AR intervention combined with an AR body scan (H2b, Study II). The comparison analysis based on a UEQ benchmark with 246 product evaluations (50) revealed that reported user experience evaluation of Study I and Study II achieved acceptable “Good” ratings in the overall assessment of attractiveness. Regarding pragmatic quality, ratings improved from “Below average” in Study I to “Above average” in Study II. Both studies achieved an “Excellent” rating in hedonic quality. Table 3 and Figure 3 present the detailed user experience values for both studies and graphical representations for Study II. Overall, our findings confirm hypothesis 2 (H2a and H2b). Additionally, the enhanced application in Study II (psychoeducation and body scan) showed improvements in user experience, particularly in novelty and attractiveness.
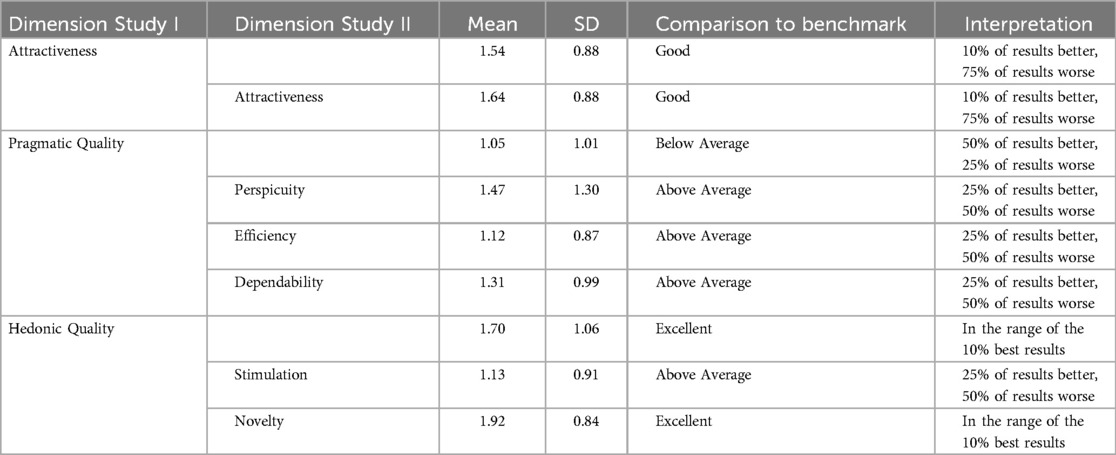
Table 3. Scale statistics of the dimensions of user experience for the evaluated augmented reality prototype of Study I and Study II and their evaluation referring to benchmarks provided by Schrepp et al. (50).
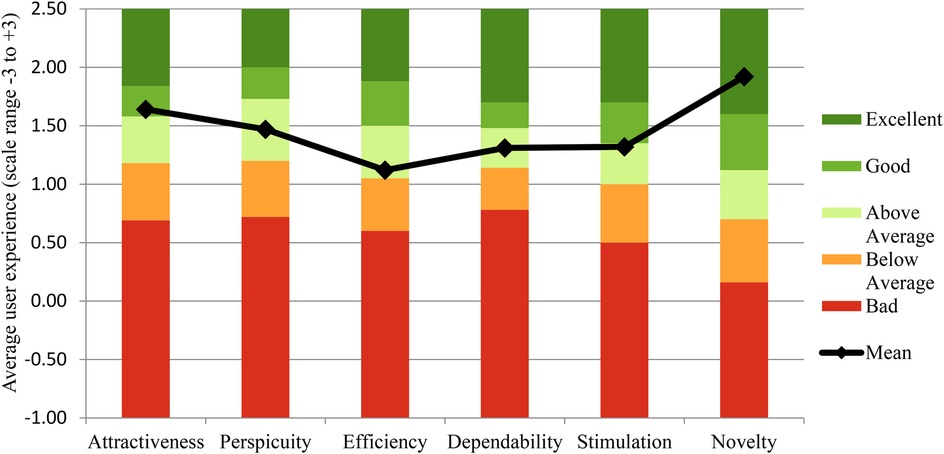
Figure 3. User experience questionnaire dimensions of the augmented reality prototype in study II for pain-specific psychoeducation combined with a body scan for chronic low back pain (black dots) compared with the benchmark (bars) by Schrepp et al. (50).
We further analyzed pain intensity and mood to explore additional facets of user experience and evaluate whether an AR intervention, either as an psychoeducational intervention for CLBP (Study I) or in combination with a body scan (Study II), can improve these pain-related psychological variables. Study I showed no significant changes in pain (p > .05) and no improvement in all facets of mood (p > .05). Study II demonstrated a significant reduction in pain (p = .004) with medium effect size. Further, a significant decrease in negative affect (p = .003) and a change in valence (p = . 026), both with medium effect sizes, were observed (Table 4). Overall, the analysis results on pain intensity and mood underline the good user experience of the AR prototypes as no worsening or even significant enhancement in emotional variables were reported.
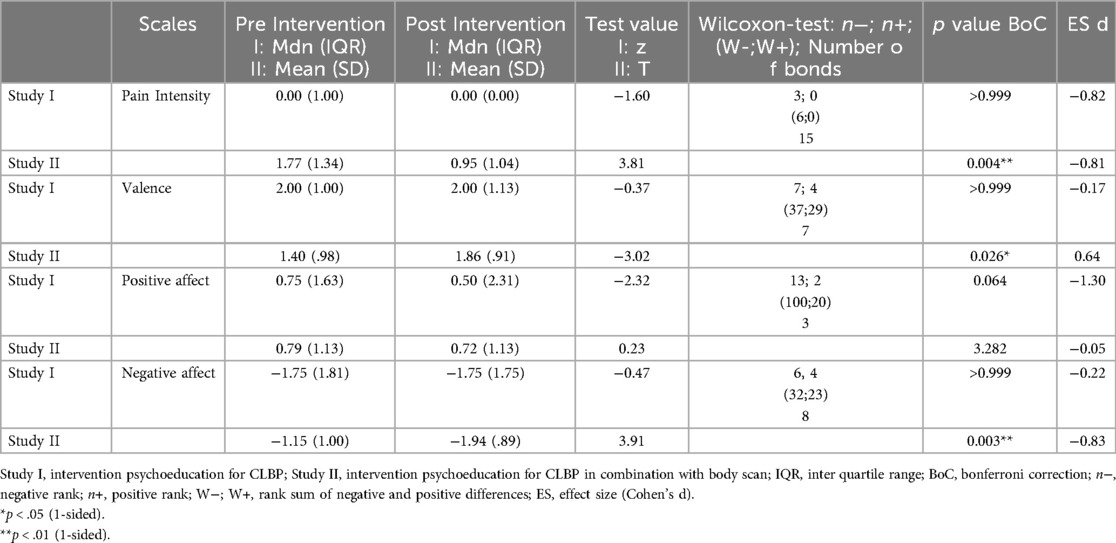
Table 4. Pain intensity and mood changes pre- and post-augmented reality intervention.
3.3 Exploratory analyses (qualitative participant feedback)
The semi-structured interview results corroborate our quantitative findings on user experience, offering further insights into enhancing the usability and user experience of the AR prototype. A summary of the responses is provided in Supplementary Appendix 3.
Question 1. Twenty participants rated the AR experience positively with comments such as “P3: Exciting. Use of (resources) when no person is present” and “P12: I would be thrilled if AR could be integrated into the therapeutic context.” Two participants suggested improvements, such as a better field of view for Microsoft HoloLens 2® or a more human voice.
Question 2. Of the participants, 14 had no previous experience with AR, four had used it in studies, and two had used it in games. Two participants had experience with body scan units, one in yoga and one in psychotherapy. Inexperienced users showed a reduced sense of security and preferred realistic representations, whereas experienced users suggested technical improvements and were more inclined to reuse the AR prototype.
Question 3. Nineteen participants stated that the AR had no effect on their sense of safety. One participant reported uncertainty due to the limited field of view, and another due to the problematic hand tracking of the Microsoft HoloLens 2®. Another study expressed uncertainty regarding hologram alignment. Additional feedback from Study I pointed to the suboptimal hand tracking capabilities of HoloLens 2®. The participants criticized the size of the device, the limited field of view, and discomfort. Users have difficulty grasping virtual objects because their movements often go beyond the tracking area, causing the object to reset.
Question 4. During the AR experience, 15 participants had different perceptions of comfort, e.g., “P05: The glasses were more noticeable,” “P09: Uncomfortable head area during body scan,” and “P18: Comfortable and uncomplicated.”
Question 5. For an “ideal AR experience,” five participants wanted more realistic graphics. Two requested better audio quality for the agent voices and two wanted background music during the body scan. Three test subjects wanted lighter glasses, e.g., “P09: As if you're not wearing anything.” Seven participants were satisfied with the prototypes.
Question 6. Fourteen participants used AR for future questions. One would only use it when ill instead of visiting a doctor, and three rejected it because of problematic hand tracking with Microsoft HoloLens 2®.
4 Discussion
The primary aim of this study was to evaluate the feasibility and user experience of two interventions tailored for CLBP in two single-armed studies: Study I (Psychoeducation) and Study II (Psychoeducation + Body Scan) in AR. The development of both interventions was based on the results of a scoping review (31) on designing theory-based AR psychoeducational interventions for CLBP. Our study contributes to the empirical understanding of user experience in an AR based psychoeducational and relaxation intervention for CLBP.
4.1 Feasibility of augmented reality intervention tailored to CLBP
We investigated the feasibility of AR interventions, specifically an psychoeducational intervention tailored for CLBP and a pain-specific psychoeducational intervention combined with MBSR-Body Scan. The attrition rate in Study I for psychoeducation was 10%, whereas the advanced psychoeducational AR intervention combined with mindfulness-based exercise for patients with CLBP had an attrition rate of 0%. Our findings on AR applications align with existing literature, which supports the feasibility of other head-mounted applications such as VR for the treatment of CLBP. For instance, a study on TBed VR game system for chronic non-specific lower back pain also reported a 0% dropout rate, indicating high feasibility (53). Furthermore, our results are consistent with a multiple experimental single-case study with eight participants for pain psychoeducation and management of CLBP in VR with a dropout rate of 0% (26). A randomized control pilot study of 22 participants investigated the use of VR exergames as a supplement to multimodal pain therapy for CBP in older adults also reported a dropout rate of 0%. Our AR intervention is technically comparable to existing VR treatments, and offers an alternative approach for treating CLBP.
Furthermore, it is important to consider the low pain intensity of the samples and its potential impact on the dropout rate. A randomized study investigating the feasibility of VR for neuroscientific pain education (VR-PNE) in patients with CLBP reported adherence rates of 63.6% for VR-PNE and 63.2% for physical therapy. Concurrently, the sample size, elevated pain scores prior to the study, and a substantial dropout rate (with only 32 out of 52 participants completing the study) indicate that pain intensity may affect the dropout rate, despite this factor not being explicitly examined (54). This finding is corroborated by a correlation between sensitization and pain intensity in CLBP patients (55). Higher pain intensity in CLBP is associated with increased central sensitization, which may influence dropout rates and should be taken into account in future feasibility studies involving patients with higher pain intensity in CLBP.
Future studies should further investigate its technical viability in clinical populations with more severe CLBP. Additionally, in Study I, data collection via questionnaires in AR also proved to be feasible in general, demonstrating acceptable psychometric properties and confirming their practicability, user-friendliness, and reliability. However, we advise against lengthy questionnaires in AR, as the problematic tracking may lead to prolonged application duration and potential frustration. Similar findings were reported for research on questionnaire integration into VR applications (56). Two participants did not complete the study due to pre-exisiting hand pain and subclinical migraine symptoms in Study I. Therefore, we recommend considering these symptoms when defining the inclusion criteria for study participants in AR using current technology, especially if the user is required to do many hand gestures. These kind of problems might not be relevant anymore for devices with optimized technology. Such issues may become irrelevant with advancements in AR technology.
4.2 User experience of augmented reality intervention tailored to CLBP
The optimized AR prototype from Study II, which integrated psychoeducation with a MBSR body scan, resulted in above-average to excellent user experiences, an improvement in mood, in terms of less negative emotions. Our findings on AR interventions align with the high acceptance and satisfaction achieved by VR applications, such as VR-based pain neuroscience education among CLBP patients, with a virtual reality application of pain neuroscience education (VR-PNE) achieving higher satisfaction scores than conventional physiotherapy (54). Our results were also consistent with a randomized control pilot study on VR exergames as an adjunct to multimodal pain treatment in older adults with chronic back pain, where attractiveness and perspicuity were rated as “very good,” efficiency, dependability, and stimulation as “good,” and novelty as “above average” (57). Compared to the pilot study by Stamm et al. (57) on VR exergames as an adjunct to multimodal pain management in older adults with chronic back pain, our prototype performed less favorably across all user experience scales, with the exception of the “novelty” dimension, which was rated significantly higher in our study.
Our results from Studies I and II demonstrate that AR intervention does not exacerbate pain intensity in mild pain conditions. This corresponds to a randomized control study on pain psychoeducation and pain management in VR for CLBP, which found non-clinically relevant pain reduction in some patients (26). In contrast to Study I, Study II demonstrated an reduction in pain intensity through the integration of psychoeducation and the MBSR body scan. These findings align with existing research on conventional MBSR therapies, which indicate that body scan techniques exert beneficial effects on CLBP and enhance quality of life (58, 59). It is important to note that in Study I, there was minimal variation in baseline pain levels in terms of a floor effect in the distribution of the average pain level of the participants, which posed challenges in demonstrating the effects of pain reduction. Conversely, Study II exhibited greater variability in pain pre- and post intervention, thereby facilitating the detection of pain reduction effects. The distracting effect of VR through neuromodulation and graded exposure therapy (23) has been shown to be particularly effective, as it shifts patients' attention away from pain and significantly reduces pain intensity and interference (60, 61). Similar effects may also apply to our AR interventions; however, this requires further investigation in future studies.
Furthermore, Study II demonstrated a significant reduction in negative affect following mindfulness-based body scan intervention in an AR forest landscape, which is consistent with VR studies showing improved mood and well-being in simulated natural environments as well as increased immersion. For instance, older adults appeared to benefit from simpler virtual environments, emphasizing the importance of the intervention design (62). These results suggest the potential for further AR studies using simulated landscapes in health contexts.
However, in our AR application, the user experience received lower ratings in the user experience subscales compared to some VR studies with exergames for CBP (57). One possible explanation is distraction caused by tactile, visual, and auditory stimuli in VR with higher immersion. Therefore, we recommend that future research on AR applications should address these stimuli and investigate the impact of immersion intensity on distraction and user experience. Furthermore, some users' discomfort leading to lower scores on user experience in our AR study may be attributed to the use of HoloLens 2 ®. The poor user experience rating in Study I could be attributed to the use of the HoloLens 2 ®, too. In the advanced prototype of Study II, this problem was addressed by tutorial exercises on technical operation and attention guidance, which led to significantly better ratings. The below-average hand tracking of HoloLens 2 ® requires additional training exercises and an interactive tutorial. Several participants expressed frustration during the intervention or reported that the HoloLens 2 ® was too large, had a limited field of view, and caused discomfort.
Specifically, participants encountered difficulties in grasping and manipulating virtual objects, as they focused on the interaction target rather than the virtual object itself, resulting in their departure from the tracking area and causing the virtual object to revert to its original position. Consequently, the HoloLens ® prematurely terminated the movement. This mechanism became a source of frustration. In this context, the lack of change in mood in Study I and subsequent improvement in Study II can be attributed to the enhanced prototype in Study II, which facilitated more intuitive operation. A study on the development of usability heuristics for AR and VR underscores the importance of user-friendly interfaces to mitigate issues such as information overload (63). To prevent users from moving objects beyond their reach, future applications should offer alternative modes to enhance reality perception and optimize processes. We recommend for future HoloLens ® applications, particularly for inexperienced users, to rely less on grasping and moving gestures and instead prioritize the more reliable tapping gesture. Lastly, our results from Study I showed a descriptive, albeit non-significant decline in positive affect which may be attributed to limitations in the hand tracking systems, highlighting the technical prerequisites for ensuring the usability of AR interventions. Overall, our AR interventions adapted for CLBP offered a positive user experience, including the enhancement of negative mood and pain. At the same time, our study highlighted fields of technical and design improvement to optimize the user experience.
4.3 Limitation
Concurrently, it is necessary to acknowledge the limitations of this study: First, two separate AR intervention studies without a control group were compared with conventional intervention. Second, the small sample size limits statistical power and reduces the identification of significant effects. Third, generalizability to clinical applications are limited due to selection bias, as participation was likely influenced by high motivation among individuals. Fourth, the lack of blinding of participants and study conductors may have lead to a bias in user experience results due to the Hawthorne effect. Fifth, there may be a potential bias resulting from the recruitment of participants who have a specific interest in AR.
5 Conclusion
This study investigated a psychoeducational AR intervention and in combination with a mindfulness-based body scan for individuals with CLBP symptoms. The empirical results demonstrated the technical feasibility of psychoeducational AR interventions, practicability of AR questionnaires, and good overall user experience. This study provided valuable insights for future studies on design improvements from a technological and psychological perspective to enhance user experience. In summary, the tested AR prototypes represent promising psychoeducational tools for patients with CLBP, aligning with treatment guidelines and laying the groundwork for further clinical research.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request.
Ethics statement
The Ethics Commission of Trier University (Germany) approved this study I (Psychoeducation) (EC No. 44/2023) and Study II (Psychoeducation + Body Scan) (EC No. 06/2023). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RC: Writing – original draft, Writing – review & editing. NH: Software, Writing – review & editing. JL: Supervision, Writing – review & editing. SM: Supervision, Writing – review & editing. AT: Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The publication was supported by the Open Access Fund of University Trier and by the German Research Foundation (DFG).
Acknowledgments
We would like to express our gratitude to all study participants for their engagement.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2025.1600637/full#supplementary-material
References
1. Meucci RD, Fassa AG, Faria NM. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. (2015) 49:1. doi: 10.1590/S0034-8910.2015049005874
2. Alsufiany MB, Lohman EB, Daher NS, Gang GR, Shallan AI, Jaber HM. Non-specific chronic low back pain and physical activity: a comparison of postural control and hip muscle isometric strength: a cross-sectional study. Medicine. (2020) 99(5):e18544. doi: 10.1097/MD.0000000000018544
3. Schreijenberg M, Koes BW, Lin CC. Guideline recommendations on the pharmacological management of non-specific low back pain in primary care—is there a need to change? Expert Rev Clin Pharmacol. (2019) 12(2):145–57. doi: 10.1080/17512433.2019.1565992
4. Dobbels F, De Bleser L, Berben L, Kristanto P, Dupont L, Nevens F, et al. Efficacy of a medication adherence enhancing intervention in transplantation: the MAESTRO-Tx trial. J Heart Lung Transplant. (2017) 36(5):499–508. doi: 10.1016/j.healun.2017.01.007
5. Nicol V, Verdaguer C, Daste C, Bisseriex H, Lapeyre É, Lefèvre-Colau MM, et al. Chronic low back pain: a narrative review of recent international guidelines for diagnosis and conservative treatment. J Clin Med. (2023) 12(4):1685. doi: 10.3390/jcm12041685
6. Frizziero A, Pellizzon G, Vittadini F, Bigliardi D, Costantino C. Efficacy of core stability in non-specific chronic low back pain. J Funct Morphol Kinesiol. (2021) 6(2):37. doi: 10.3390/jfmk602003
7. Sutanto D, Ho RST, Poon ETC, Yang Y, Wong SHS. Effects of different trunk training methods for chronic low back pain: a meta-analysis. Int J Environ Res Public Health. (2022) 19(5):2863. doi: 10.3390/ijerph19052863
8. Veloz Montano MDLN, Keeling Álvarez M. The educational and pedagogical intervention in scientific research. Community Intercult Dialog. (2023) 3:70. doi: 10.56294/cid202370
9. Sarkhel S, Singh O, Arora M. Clinical practice guidelines for psychoeducation in psychiatric disorders: general principles of psychoeducation. Indian J Psychiatry. (2020) 62(Suppl 2):319. doi: 10.4103/psychiatry.indianjpsychiatry_780_19
10. Ikemoto T, Wakao N, Matsubara T, Miki K. Psychological treatment strategy for chronic low back pain. Spine Surg Relat Res. (2018) 3(3):199–206. doi: 10.22603/ssrr.2018-0050
11. Faucett J. Chronic low back pain: early interventions. Annu Rev Nurs Res. (1999) 17:155–82. doi: 10.1891/0739-6686.17.1.155
12. Isaikin AI, Mukhametzyanova AK, Nasonova TI. Emotional disorders and their therapy in chronic low back pain. Neurol Neuropsychiatry Psychosom. (2022) 14(5):90–5. doi: 10.14412/2074-2711-2022-5-90-95
13. Comachio J, Magalhães MO, Campos Carvalho E Silva APM, Marques AP. A cross-sectional study of associations between kinesiophobia, pain, disability, and quality of life in patients with chronic low back pain. Adv Rheumatol. (2018) 58(1):8. doi: 10.1186/s42358-018-0011-2
14. Williams FMK, Elgaeva EE, Freidin MB, Zaytseva OO, Aulchenko YS, Tsepilov YA, et al. Causal effects of psychosocial factors on chronic back pain: a bidirectional Mendelian randomisation study. Eur Spine J. (2022) 31(7):1906–15. doi: 10.1007/s00586-022-07263-2
15. Luiggi-Hernandez JG, Morone NE, Hamm M, Greco CM, Weiner DK, Woo J. Mindfulness for chronic low back pain: a qualitative analysis. Pain Med. (2017) 19(11):2138–45. doi: 10.1093/pm/pnx197
16. Čeko M, Baeuerle T, Webster L, Wager TD, Lumley MA. The effects of virtual reality neuroscience-based therapy on clinical and neuroimaging outcomes in patients with chronic back pain: a randomized clinical trial. Pain. (2024) 165(8):1860–74. doi: 10.1097/j.pain.0000000000003198
17. Milgram P, Kishino F. A taxonomy of mixed reality visual displays. IEICE Trans Inf Syst. (1994) 77(12):1321–9.
18. Skarbez R, Smith M, Whitton MC. Revisiting milgram and kishino’s reality-virtuality continuum. Front Virtual Real. (2021) 2:647997. doi: 10.3389/frvir.2021.647997
19. Mallari B, Spaeth EK, Goh H, Boyd BS. Virtual reality as an analgesic for acute and chronic pain in adults: a systematic review and meta-analysis. J Pain Res. (2019) 12:2053–85. doi: 10.2147/JPR.S200498
20. Awan AB, Mahmood AW, Sabahat N. Enhancing user experience: exploring mobile augmented reality experiences. VFAST Trans Softw Eng. (2024) 12(1):121–32. doi: 10.21015/vtse.v12i1.1741
21. Fatima S, Schurig A, Baalsrud Hauge J, Basu P, Chowdhury A, Baalsrud Hauge J. Investigating impact of augmented reality on game design to facilitate learning experiences in logistics operations using immersive AR interfaces. Proceedings (2021). p. 419–26. doi: 10.1007/978-3-030-89394-1_34
22. Boşat M, Önder E, Arcagök U. Augmented reality practices in health services: literature review. BEU J Sci Technol. (2020) 10(2):67–72. doi: 10.17678/beuscitech.817159
23. Tack C. Virtual reality and chronic low back pain. Disabil Rehabil Assist Technol. (2019) 16(6):637–45. doi: 10.1080/17483107.2019.1688399
24. Trujillo MS, Alvarez AF, Nguyen L, Petros J. Embodiment in virtual reality for the treatment of chronic low back pain: a case series. J Pain Res. (2020) 13:3131–7. doi: 10.2147/JPR.S275312
25. Li R, Li Y, Kong Y, Li H, Hu D, Fu C, et al. Virtual reality-based training in chronic low back pain: systematic review and meta-analysis of randomized controlled trials. J Med Internet Res. (2024) 26:e45406. doi: 10.2196/45406
26. de Vries FS, van Dongen RTM, Bertens D. Pain education and pain management skills in virtual reality in the treatment of chronic low back pain: a multiple baseline single-case experimental design. Behav Res Ther. (2023) 162:104257. doi: 10.1016/j.brat.2023.104257
27. O’Connor S, Mayne A, Hood B. Virtual reality-based mindfulness for chronic pain management: a scoping review. Pain Manag Nurs. (2022) 23(3):359–69. doi: 10.1016/j.pmn.2022.03.013
28. Brown L, DiCenso-Fleming T, Ensign T, Boyd AJ, Monaghan G, Binder DS. Chronic pain education delivered with a virtual reality headset in outpatient physical therapy clinics: a multi-site exploratory trial. Am J Transl Res. (2023) 15(5):3500–10.37303618
29. Wu YF, Kim EY, Wu CH. Users’ perceptions of technological features in augmented reality (AR) and virtual reality (VR) in fashion retailing: a qualitative content analysis. Mob Inf Syst. (2022) 2022:1–13. doi: 10.1155/2022/3080280
30. Calabrò RS, Tonin P, Ciancarelli I, Cerasa A, Iosa M, Morone G, et al. The arrival of the metaverse in neurorehabilitation: fact, fake or vision? Biomedicines. (2022) 10(10):2602. doi: 10.3390/biomedicines10102602
31. Conen R, Mueller S, Tibubos AN. Integration of conventional and virtual reality approaches in augmented reality for theory-based psychoeducational intervention design for chronic low back pain: scoping review. Interact J Med Res. (2025) 14:e59611. doi: 10.2196/59611
32. Venkatesh V, Thong JYL, Xu X. Consumer acceptance and use of information technology: extending the unified theory of acceptance and use of technology. MIS Q. (2012) 36(1):157–78. doi: 10.2307/41410412
33. Minakawa Y, Miyazaki S, Yoshida N, Iimura K, Waki H, Itoh K. Trigger point acupuncture and exercise for chronic low back pain in older adults: a preliminary randomized clinical trial. J Acupunct Meridian Stud. (2022) 15(2):143–51. doi: 10.51507/j.jams.2022.15.2.143
34. Parthan A, Evans CJ, Le K. Chronic low back pain: epidemiology, economic burden and patient-reported outcomes in the USA. Expert Rev Pharmacoecon Outcomes Res. (2006) 6(3):359–69. doi: 10.1586/14737167.6.3.359
35. Moore CG, Carter RE, Nietert PJ, Stewart PW. Recommendations for planning pilot studies in clinical and translational research. Clin Transl Sci. (2011) 4(5):332–7. doi: 10.1111/j.1752-8062.2011.00347.x
36. Alberola C, Brau H, Walter G. The shortening of the user experience questionnaire (UEQ). In: Burghardt M, Wimmer R, Wolff C, Womser-Hacker C, editors. Mensch und Computer 2017 – Conference Proceedings; Evaluation of UX and Aesthetics. Regensburg; September 10–13, 2017. Regensburg: German Informatics Society (2017). pp. 37–48. doi: 10.18420/muc2017-mci-0178
37. Shafshak TS, Elnemr R. The visual analogue scale versus numerical rating scale in measuring pain severity and predicting disability in low back pain. J Clin Rheumatol. (2021) 27(7):282–5. doi: 10.1097/RHU.0000000000001320
38. Alghadir AH, Al-Eisa ES, Anwer S, Sarkar B. Reliability, validity, and responsiveness of three scales for measuring balance in patients with chronic stroke. BMC Neurol. (2018) 18(1):141. doi: 10.1186/s12883-018-1146-9
39. Schallberger U. Kurzskalen Zur Erfassung Der Positiven Aktivierung, Negativen Aktivierung Von Valenz in Experience Sampling Studien (PANAVA-KS). Zürich: Department of Applied Psychology at the University’s Institute of Psychology (2005). Available online at: https://www.yumpu.com/de/document/view/8689955/kurzskalen-panava-schallberger-2005-laufbahndiagnostikch (Accessed November 16, 2023).
40. Smits M, van Goor H, Kallewaard JW, Verbeek PP, Ludden GDS. Evaluating value mediation in patients with chronic low-back pain using virtual reality: contributions for empirical research in value sensitive design. Health Technol. (2022) 12(4):765–78. doi: 10.1007/s12553-022-00671-w
41. Schwarzer R. Modeling health behavior change: how to predict and modify the adoption and maintenance of health behaviors. Appl Psychol. (2008) 57(1):1–29. doi: 10.1111/j.1464-0597.2007.00325.x
42. Schwarzer R. Health action process approach (HAPA) as a theoretical framework to understand behavior change. Act Psicol. (2016) 30(121):119–30. doi: 10.15517/ap.30i121.23458
43. Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. (1982) 4(1):33–47. doi: 10.1016/0163-8343(82)90026-3
44. Kabat-Zinn J. Mindfulness-based intervention in context: past, present, and future. Clin Psychol Sci Pract. (2003) 10(2):144–56. doi: 10.1093/clipsy.bpg016
45. Vovk A, Wild F, Guest W, Kuula T. Simulator sickness in augmented reality training using the microsoft HoloLens. Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems (2018). New York, NY: ACM.
46. LaViola JJ. A discussion of cybersickness in virtual environments. SIGCHI Bull. (2000) 32(1):47–56. doi: 10.1145/333329.333344
47. Rebenitsch L, Owen C. Review on cybersickness in applications and visual displays. Virtual Real. (2016) 20(2):101–25. doi: 10.1007/10055-016-0285-9
48. Microsoft. Direct manipulation. Microsoft Mixed Reality Design. (2023). Available online at: https://learn.microsoft.com/de-de/windows/mixed-reality/design/direct-manipulation (Accessed January 21, 2024).
49. Microsoft. Holographic Remoting Player. Microsoft Mixed Reality Development. (2024). Available online at: https://learn.microsoft.com/de-de/windows/mixed-reality/develop/native/holographic-remoting-player (Accessed January 21, 2024).
50. Schrepp M, Hinderks A, Thomaschewski J. Construction of a benchmark for the user experience questionnaire (UEQ). Int J Interact Multimed Artif Intell. (2017) 4(4):40–4. doi: 10.9781/ijimai.2017.445
51. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed Hillsdale, N.J.: L. Erlbaum Associates (1988).
52. Banha F, Flores A, Coelho LS. Quantitizing qualitative data from semi-structured interviews: a methodological contribution in the context of public policy decision-making. Mathematics. (2022) 10(19):3597. doi: 10.3390/math10193597
53. Hussein H, Atteya M, Kamel E. Effectiveness of virtual reality on rehabilitation of chronic non-specific low back pain patients. Healthcare. (2024) 12(13):1312. doi: 10.3390/healthcare12131312
54. McConnell R, Lane E, Webb G, LaPeze D, Grillo H, Fritz J. A multicenter feasibility randomized controlled trial using a virtual reality application of pain neuroscience education for adults with chronic low back pain. Ann Med. (2024) 56(1):2311846. doi: 10.1080/07853890.2024.2311846
55. Dahmani D, Taik FZ, Berrichi I, Fourtassi M, Abourazzak FE. Impact of central sensitization on pain, disability and psychological distress in patients with knee osteoarthritis and chronic low back pain. BMC Musculoskelet Disord. (2023) 24(1):877. doi: 10.1186/s12891-023-07019-z
56. Küntzer L, Schwab S, Spaderna H, Rock G. ROVER: a standalone overlay tool for questionnaires in virtual reality. EICS ‘24: The 16th ACM SIGCHI Symposium on Engineering Interactive Computing Systems (2024). Trier: Software Engineering Lab at Trier University of Applied Sciences. Available online at: https://doi.org/10.1145/3660515.3661328.
57. Stamm O, Dahms R, Reithinger N, Ruß A, Müller-Werdan U. Virtual reality exergame for supplementing multimodal pain therapy in older adults with chronic back pain: a randomized controlled pilot study. Virtual Real. (2022) 26(4):1291–305. doi: 10.1007/s10055-022-00629-3
58. Petrucci G, Papalia GF, Russo F, Vadalà G, Piredda M, De Marinis MG, et al. Psychological approaches for the integrative care of chronic low back pain: a systematic review and metanalysis. Int J Environ Res Public Health. (2021) 19(1):60. doi: 10.3390/ijerph19010060
59. Paschali M, Lazaridou A, Sadora J, Papianou L, Garland EL, Zgierska AE, et al. Mindfulness-based interventions for chronic low back pain: a systematic review and meta-analysis. Clin J Pain. (2024) 40(2):105–13. doi: 10.1097/AJP.0000000000001173
60. Nagpal AS, Raghunandan A, Tata F, Kibler D, McGeary D. Virtual reality in the management of chronic low back pain: a scoping review. Front Pain Res. (2022) 3:856935. doi: 10.3389/fpain.2022.856935
61. Okhotin D, Maddox T, Sparks C, Oldstone L, Garcia H, French K, et al. Durable chronic low back pain relief by RelieVRx, an at-home virtual reality program, 18 months post-treatment. Neuromodulation. (2023) 26(4):S33. doi: 10.1016/j.neurom.2023.04.057
62. Liu P, Liu J, Fernandez J, Zou Q, Lin M. Positive affect and natural landscape in virtual reality: a systematic review comparing interventions, measures, and outcomes. J Environ Psychol. (2023) 88:102011. doi: 10.1016/j.jenvp.2023.102011
63. Omar K, Marx Gómez J, Zraqou J, Fakhouri H. Usability heuristics for metaverse. Computers. (2024) 13(9):222. doi: 10.3390/computers13090222
64. Laugwitz B, Held T, Schrepp M. Construction and evaluation of a user experience questionnaire. In: Holzinger A, editor. HCI and Usability for Education and Work. USAB 2008, Graz, Austria; November 20–21 (Lecture Notes in Computer Science, vol 5298). Berlin, Heidelberg: Springer (2008). p. 63–76. doi: 10.1007/978-3-540-89350-9_6
Keywords: augmented reality, chronic low back pain, pain education, mindfulness body scan, user experience, feasibility
Citation: Conen R, Hepke N, Lohscheller J, Mueller S and Tibubos AN (2025) Feasibility and user experience of augmented reality psychoeducation and mindfulness body scan for chronic low back pain. Front. Pain Res. 6:1600637. doi: 10.3389/fpain.2025.1600637
Received: 26 March 2025; Accepted: 16 June 2025;
Published: 1 July 2025.
Edited by:
Eleuterio A. Sánchez Romero, Hospital Universitario Puerta de Hierro Majadahonda, SpainReviewed by:
Wesley Gilliam, Mayo Clinic, United StatesOliver Martínez Pozas, Rey Juan Carlos University, Spain
Copyright: © 2025 Conen, Hepke, Lohscheller, Mueller and Tibubos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robin Conen, Y29uZW5AdW5pLXRyaWVyLmRl
†ORCID:
Robin Conen
orcid.org/0000-0003-2811-6526
Nikolai Hepke
orcid.org/0009-0009-6806-4362
Jörg Lohscheller
orcid.org/0000-0002-2319-427X
Steffen Mueller
orcid.org/0000-0003-1683-6243
Ana N. Tibubos
orcid.org/0000-0003-4284-0019