 Anouk Goerens1
Anouk Goerens1 Dirk Lehnick2
Dirk Lehnick2 Michael Büttcher1,3Karin Daetwyler1,4
Michael Büttcher1,3Karin Daetwyler1,4 Matteo Fontana1,4Petra Genet1,4Marco Lurà1,5Davide Morgillo1,4Sina Pilgrim1,4Katharina Schwendener-Scholl1,4Nicolas Regamey1,5Thomas J. Neuhaus1
Matteo Fontana1,4Petra Genet1,4Marco Lurà1,5Davide Morgillo1,4Sina Pilgrim1,4Katharina Schwendener-Scholl1,4Nicolas Regamey1,5Thomas J. Neuhaus1 Martin Stocker1,4*
Martin Stocker1,4*- 1Department of Pediatrics, Children's Hospital Lucerne, Lucerne, Switzerland
- 2Clinical Trial Unit, University of Lucerne, Lucerne, Switzerland
- 3Infectious Diseases Unit, Children's Hospital Lucerne, Lucerne, Switzerland
- 4Pediatric and Neonatal Intensive Care Unit, Children's Hospital Lucerne, Lucerne, Switzerland
- 5Pediatric Pulmonology Unit, Children's Hospital Lucerne, Lucerne, Switzerland
Background and Aims: Neonatal ventilator associated pneumonia (VAP) is a common nosocomial infection and a frequent reason for empirical antibiotic therapy in NICUs. Nonetheless, there is no international consensus regarding diagnostic criteria and management. In a first step, we analyzed the used diagnostic criteria, risk factors and therapeutic management of neonatal VAP by a literature review. In a second step, we aimed to compare suspected vs. confirmed neonatal VAP episodes in our unit according to different published criteria and to analyze interrater-reliability of chest x-rays. Additionally, we aimed to evaluate the development of VAP incidence and antibiotic use after implementation of multifaceted quality improvement changes regarding antimicrobial stewardship and infection control (VAP-prevention-bundle, early-extubation policy, antimicrobial stewardship rounds).
Methods: Neonates until 44 weeks of gestation with suspected VAP, hospitalized at our level-III NICU in Lucerne from September 2014 to December 2017 were enrolled. VAP episodes were analyzed according to 4 diagnostic frameworks. Agreement regarding chest x-ray interpretation done by 10 senior physicians was assessed. Annual incidence of suspected and confirmed neonatal VAP episodes and antibiotic days were calculated and compared for the years 2015, 2016, and 2017.
Results: 17 studies were identified in our literature review. Overall, CDC-guidelines or similar criteria, requesting radiographic changes as main criteria, are mostly used. Comparison of suspected vs. confirmed neonatal VAP episodes showed a great variance (20.4 vs. 4.5/1,000 ventilator-days). The interrater-reliability of x-ray interpretation was poor (intra-class correlation 0.25). Implemented changes resulted in a gradual decline in annual VAP incidence and antibiotic days from 2015 compared with 2017 (28.8 vs. 7.4 suspected episodes/1,000 ventilator-days, 5.5 vs. 0 confirmed episodes/1,000 ventilator-days and 211 vs. 34.7 antibiotic days/1,000 ventilation-days, respectively).
Conclusion: The incidence of suspected VAP and concomitant antibiotic use is much higher than for confirmed VAP, therefore inclusion of suspected episodes should be considered for accurate evaluation. There is a high diagnostic inconsistency and a low reliability of interpretation of chest x-rays regarding VAP. Implementation of combined antimicrobial stewardship and infection control measures may lead to an effective decrease in VAP incidence and antibiotic use.
Background and Aims
Ventilator associated pneumonia (VAP) is defined as a nosocomial lower airway infection, i.e. pneumonia, in intubated patients with onset after 48 h or more of invasive mechanical ventilation1 (1). VAP is usually caused by airway colonization by potential pathogens, which disseminate due to inadequate immune response of the newborn's immature innate immune system. The immaturity of the immune system is especially significant in premature and growth restricted newborns (2). Sources of airway colonization can be the patient's own flora, i.e., bacterial overgrowth in oral secretions, reflux and aspiration of gastric fluid or the patient's environment with its caretakers and equipment (2, 3).
VAP is one of the most frequently diagnosed nosocomial infections (4) and, after suspected early onset sepsis, second most reason for antibiotic intervention in NICUs (5, 6). There is no international consensus on definition of VAP regarding the neonatal population (3, 7). In most recommendations radiographic changes are considered as one of the main crireria. However, underlying lung disease may complicate the interpretation of radiographic changes in this population. Reported frequency of neonatal VAP show a large range (2.7–10.9 cases per 1,000 ventilator days) in developed countries (3). VAP incidence can be reduced by infection control measures such as VAP-prevention-bundles (8–10). Epidemiologic studies demonstrated that quality improvement initiatives, not the introduction of new therapies or research approaches, resulted in a decline of mortality of neonates in the last decade (11).
Antibiotics are among the most frequently used medications in neonatal intensive care (12). There is a high variance of antibiotic use when comparing different NICUs. This observation suggests relevant overuse and underlines the need for implementation of antibiotic stewardship (13, 14). Prompt antibiotic therapy for possible infections in this vulnerable population is crucial for good outcome (15). On the other hand, inadequate antibiotic use results in increasing occurrence of multidrug resistant bacteria (16). In addition, recently published studies underline that antibiotic treatment in early life has an impact on the individual's microbiome with potential consequences for future health (17–20). Prolonged duration of antibiotic use in preterm infants is also associated with higher mortality and morbidity such as chronic lung disease, retinopathy of prematurity, periventricular leukomalacia and necrotizing enterocolitis (16, 21). Neonatologists and pediatricians should be aware that starting antibiotics may be in some circumstances more harmful than beneficial. The mind-set of antibiotic treatment just for safety reasons is no longer justified (20).
Aim of this study was to perform a review of the current literature to present an overview of the most commonly used diagnostic criteria, risk factors and therapeutic management for neonatal VAP. Secondly to analyze all suspected neonatal VAP episodes in our unit within the study period according to various predefined diagnostic criteria1 (22, 23). We hypothesized that a high variance in incidence between clinically suspected and confirmed neonatal VAP would exist. Additionally, because interpretation of chest x-rays is a corner stone of VAP diagnosis, we wanted to analyze the interrater-reliability of all chest x-rays done for suspected neonatal VAP episodes, hypothesizing that interrater-reliability would be modest to low. Last, we aimed to describe and compare annual incidence of neonatal VAP and antibiotic use for neonatal VAP in our NICU during a quality improvement initiative with implementation of multifaceted changes focused both on antimicrobial stewardship and infection control. We hypothesized that implementation of these changes decreases incidence of, as well as antibiotic use for neonatal VAP.
Methods
Literature Review
The literature review was done applying the approach of the PRISMA-statement for systematic reviews (24). PubMed was searched using the following search terms: “diagnosis + neonatal ventilator associated pneumonia,” “antibiotic therapy + neonatal ventilator associated pneumonia,” and “neonatal ventilator associated pneumonia” sorted by best match, with restriction to available full text in English or German. The first search was run in December 2017, the last search was run in March 2018. In addition, further studies were identified reviewing references in found publications. Inclusion was based on the described population (only neonatal population) and the content of the study (diagnostic criteria and/or risk factors and/or management of VAP).
Study Setting
For our study, approval of the national ethics committee was obtained (Project-ID 2017-01842). The patients' parents/guardians were informed beforehand and gave consent for the study. Recordings of suspected neonatal VAP episodes as well as the single-center quality improvement initiative were undertaken at our level-III NICU in Lucerne. The Children's Hospital Lucerne is a teaching hospital for Pediatrics and Neonatology and the unit is a referral level III NICU (perinatal center) with all pediatric specialties including neonatal surgery, but without cardiac surgery (except surgical closure of persistent ductus arteriosus). The NICU is part of the Swiss neonatal collaboration with regular quality assessment and center-to-center comparison (25).
For this study, neonatal VAP was defined as VAP occurring in neonates below 44 weeks of corrected gestational age. Therefore, the study population consists of neonates with a corrected gestational age between 23 0/7 and 43 6/7 weeks hospitalized during the study period of September 1st, 2014 to December 31st, 2017. September 1st, 2014 data collection was started with implementation of a prospective surveillance program assessing VAP, central line associated blood stream infections (CLABSI) and use of antibiotics on the NICU. Every morning between 6 and 8 a.m. the on-site physician recorded patients with suspected VAP, CLABSI and patients on antibiotic treatment. The recordings were verified and entered into the NICU's surveillance database by the NICU's data manager.
Definitions of Suspected and Confirmed Neonatal VAP
Suspected VAP was defined according to the following criteria: ventilation for more than 48 h and new start or change of antibiotic therapy due to worsening of ventilation conditions and/or clinical deterioration and/or radiological changes compatible with pneumonia and/or changes of tracheal secretions and/or abnormal laboratory parameters (CRP > 20 mg/l, leukocytosis/-penia, I:T ratio > 0.2).
To compare the variance between clinically suspected (all episodes in our study population) and confirmed neonatal VAP, four different frameworks for diagnosis of VAP were applied on all suspected VAP episodes of our study population retrospectively. Patients fulfilling the diagnostic criteria of at least one of the frameworks were defined as confirmed VAP. Suspected episodes not fulfilling any criteria were addressed as non-confirmed VAP. The frameworks we used for further diagnosis were: 1. Center for Diseases Control and Prevention (CDC): Criteria for defining nosocomial pneumonia for infants ≤ 1 year old (22); 2. European Centre for Disease Prevention and Control (ECDC)1; 3. Diagnostic criteria for laboratory confirmed VAP according to a surveillance study with definition for infection specifically adapted for neonates from a Dutch NICU (23); 4. Diagnostic criteria for clinical VAP according to a surveillance study with definition for infection specifically adapted for neonates from a Dutch NICU (23). Table 1 shows a listing of all used definitions.
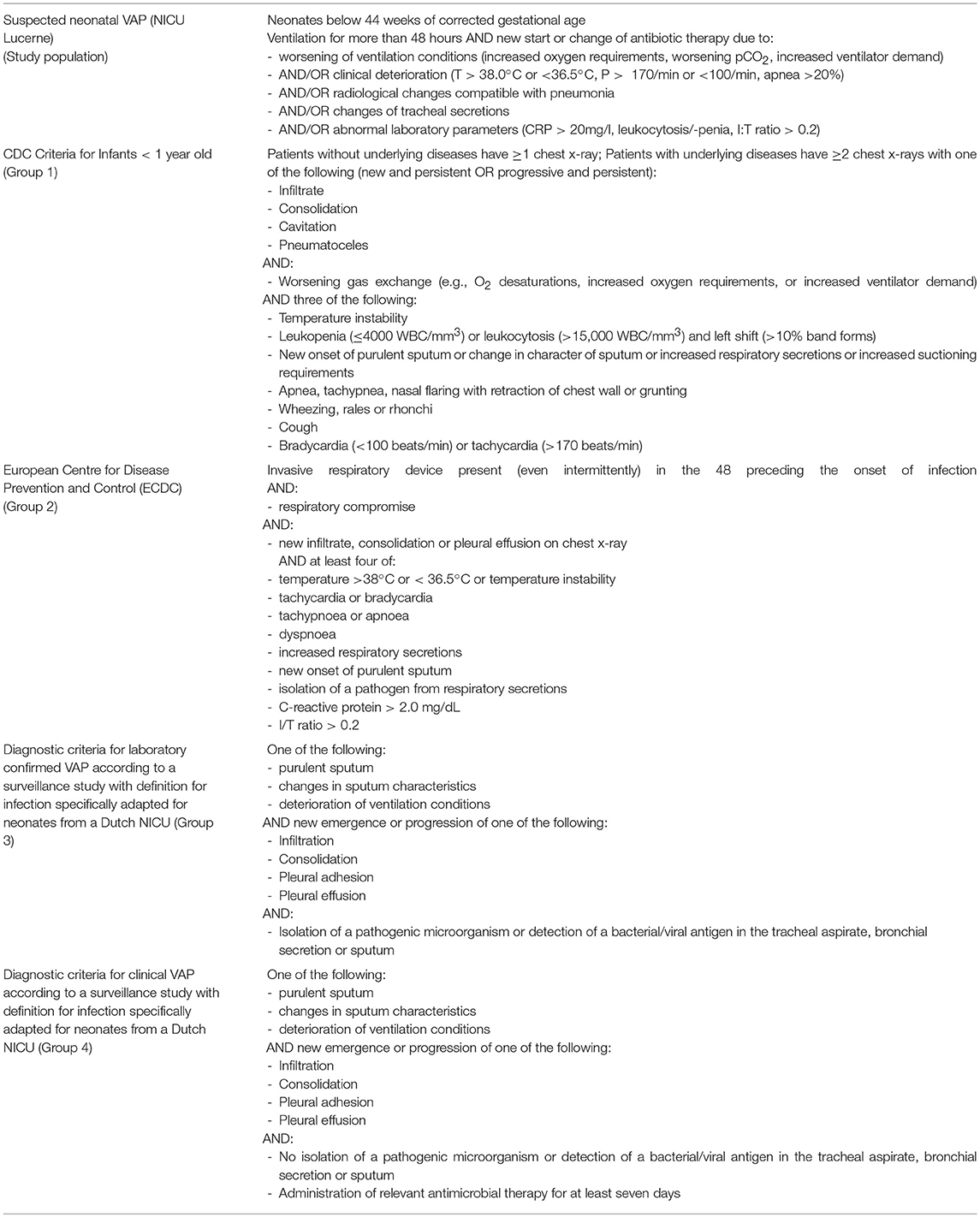
Table 1. Used definitions for diagnosing neonatal VAP.
Interrater-Reliability of Chest-X-Ray Interpretation
Chest x-rays for suspected VAP episodes were ordered according to the physician in charge. The primary evaluation was done by the radiologist in charge and used for evaluation of confirmed neonatal VAP. For analysis of interrater-reliability, all chest x-rays ordered for suspected neonatal VAP were reviewed separately by all board approved neonatologists, pediatric pulmonologists and pediatric infectious disease specialists of the children's hospital of Lucerne (total of 10 senior physicians: 7 board approved neonatologists, 2 board approved pediatric pulmonologists and 1 board approved specialist for pediatric infectious diseases). They all reported if radiographic changes caused by neonatal VAP were present with a 4-point Likert scale (yes, possibly yes, possibly no, no). All x-rays were anonymized and all raters were blinded for the written interpretation by the radiologist.
Quality Improvement Initiative
Within our quality improvement initiative we analyzed prospectively all episodes of suspected neonatal VAP and antibiotic use during and after implementation of multifaceted changes regarding infection control and antimicrobial stewardship in our NICU. The prospective surveillance program started in September 2014. The staff of the NICU was aware of the quality improvement initiative focused on antimicrobial stewardship, but was not informed regarding details of the ongoing analyzes for the study.
Since 2007, prescription of antibiotics in our unit is standardized by use of a web based guideline (www.idosecalc.ch) specifying drug, dose and duration of therapy (7–10 days of therapy recommended for hospital acquired pneumonia). Starting December 2015, the following multifaceted quality improvement changes were introduced over 2 years (Table 2): Firstly, a new policy for early-extubation minimizing duration of invasive ventilation was introduced in December 2015. Secondly, since December 2015, infectious disease specialists have been involved in the NICU every week for an antimicrobial stewardship round. Thirdly, a care bundle was implemented in our neonatal and pediatric ICU in December 2016, including the following measures: strict hand hygiene before and after patient contact and handling respiratory equipment, wearing gloves when in contact with secretions, ventilator circuit changes every 14 days or when visibly soiled, oral care every 2–4 h, head of bed elevation, draining ventilator condensate before repositioning of the patient, using endotracheal tube (ETT) with cuff when possible (usually not applicable for preterm neonates), choosing size of the ETT carefully to reduce numbers of reintubation.

Table 2. Implemented quality improvement changes in our NICU.
Data Sources
Clinical signs, oxygen requirement, ventilation requirements and further physical measurements as required according to the criteria for VAP were extracted from patient files. Antibiotic days and laboratory results were obtained from electronic patient files and reports of hospitalization. All laboratory measurements were ordered according to the request of the physician in charge and the unit's policy to use full white blood count (WBC), I:T ratio and C-reactive protein (CRP) for evaluation of suspected infection and guidance of duration of antibiotic therapy. According to the unit's policy, blood cultures and cultures of tracheal aspirates ought to be obtained before start or change of antibiotic therapy. Results were obtained from electronic patient files. Tracheal aspirates were examined microscopically with a semi-quantitative analysis of leukocytes. Purulent tracheal aspirates were defined as leucocytes ≥2 within the scale from 0 to 3.
Statistical Analyses
All data were anonymized before statistical analysis. Data collection in our NICU is generally performed for the period of a whole year (January to December), therefore annual calculations of suspected and confirmed VAP episodes and antibiotic use could only be done for the 3 complete years of the study: 2015, 2016, and 2017. The episodes in 2014 were not included in calculations as the observational period started in September.
Incidence of suspected and confirmed neonatal VAP episodes, as well as incidence of all separate groups (1–4) were calculated for the period of January 2015–December 2017 and extrapolated for 1,000 ventilator-days. Comparison of agreement between the four different diagnostic criteria was calculated using intra-class correlation coefficients (ICC). Risk factors such as gestational age, birth weight and duration of mechanical ventilation were compared between the two groups of non-confirmed and confirmed neonatal VAP. Agreement between raters for the evaluation of the chest x-rays with the 4-point Likert scale was assessed utilizing intra-class correlation coefficients (ICC). All raters evaluated all chest x-rays (fully crossed design). An ICC > 0.8 was considered as excellent, >0.6 as good agreement between raters. Annual incidence of suspected and confirmed VAP episodes and antibiotic days were calculated for 1,000 ventilator-days. To assess the existence of a possible trend regarding annual incidence of suspected VAP episodes, duration of antibiotic therapy per suspected episode and antibiotic days for suspected episodes, the nonparametric test for trend proposed by Cuzick was used (Wilcoxon-type test for trend) as the approximation works for small sample sizes (26).
Results
Literature Review
A total of 17 studies were included in the review. The flow chart in Figure 1 shows the process of selecting studies for inclusion in the literature review. Table 3 is a listing of these recent studies, giving an overview of the used diagnostic criteria, the most important risk factors and the used therapeutic management for VAP in newborns. The CDC guidelines for infants ≤ 1 year old were the most often applied criteria followed by similar and adapted criteria. Except for the criteria used in the study by Katayama et al. (33), all request abnormal chest x-rays as part of their criteria. Longer duration of mechanical ventilation, low birth weight, low gestational age and numbers of reintubation were the prevalent risk factors for VAP. Long duration of mechanical ventilation was the most important risk factor. Even though the database was reviewed for studies regarding antibiotic therapy, only three studies (31, 33, 37) discussed the treatment of VAP.
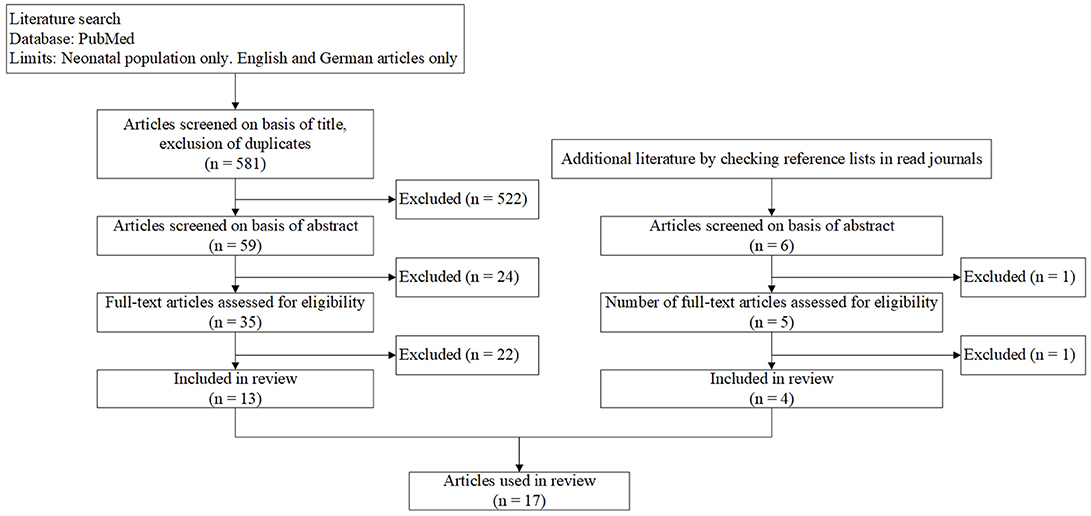
Figure 1. Flow-chart showing literature research.
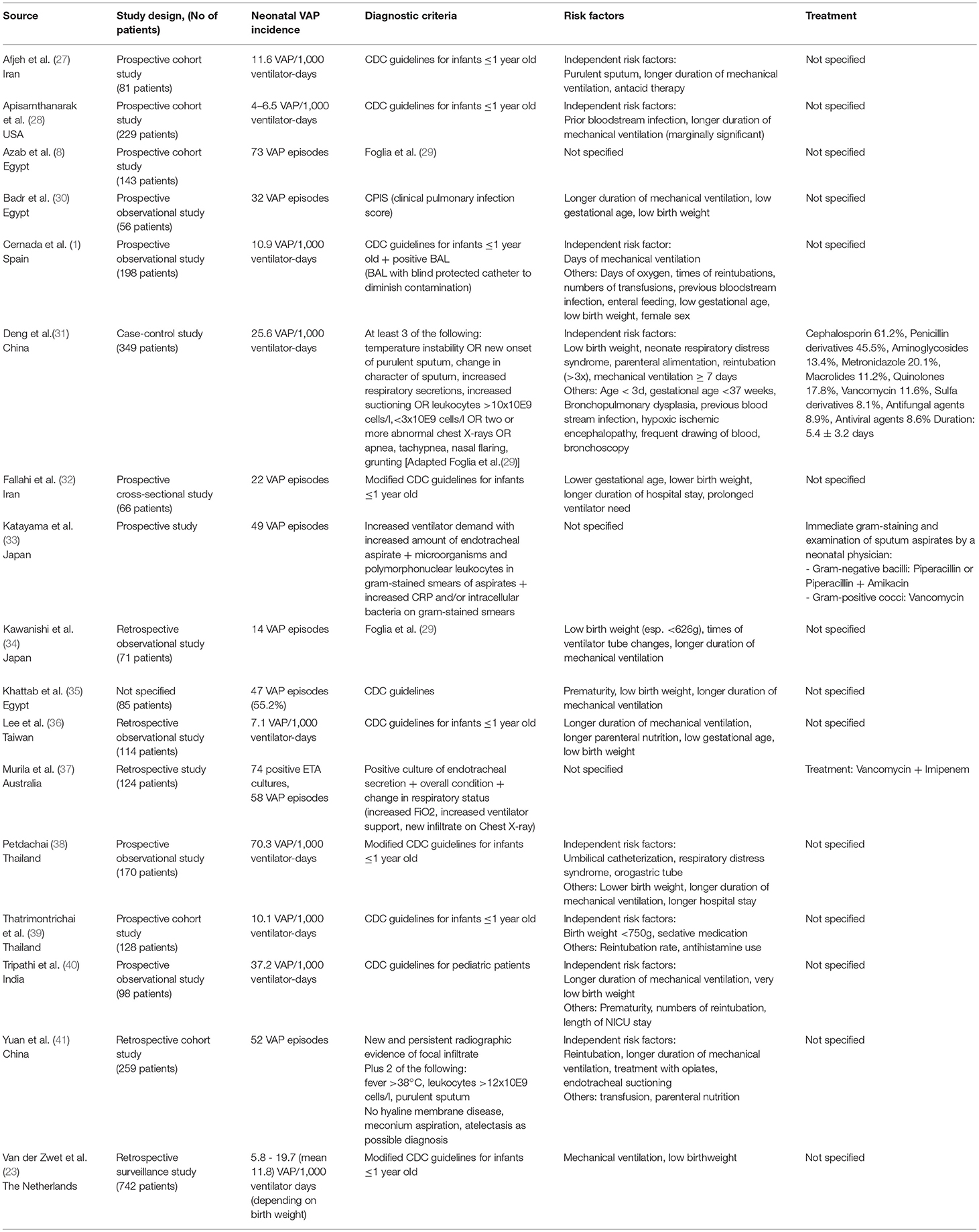
Table 3. Systematic review: Overview of incidence, diagnostic criteria, risk factors and treatment.
Suspected vs. Confirmed Neonatal VAP
Comparison of suspected with confirmed neonatal VAP episodes showed a great variance over the whole study period: 20.4 vs. 4.5/1,000 ventilator-days. The particular incidence of confirmed neonatal VAP after applying the 4 different diagnostic criteria (groups 1–4) is shown in Table 4. Comparison of agreement between the different diagnostic criteria showed an ICC of 0.55, thus showing a moderate agreement.
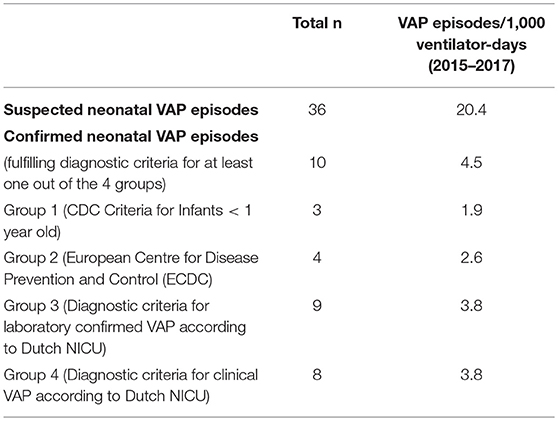
Table 4. Incidence of suspected and confirmed neonatal VAP (in total and for groups 1 – 4).
The age of neonates in our study population (n = 36) ranged between 24 3/7 and 41 1/7 (median 28 4/7) gestational weeks at the time of diagnosis. They weighed between 345 and 3,770 g (median 650 g). The 26 neonates with non-confirmed VAP were between 24 3/7 and 41 1/7 (median 27 6/7) gestational weeks old and weighed between 345 and 3,770 g (median 630 g). Duration of mechanical ventilation varied between 3 to 103 days (median 12.5 days). The 10 neonates with confirmed VAP episodes were between 26 5/7 and 40 0/7 (median 29 1/7) weeks and had a birth weight between 345 and 3,690 g (median 670 g). They were intubated between 10 and 37 days (median 26 days) at time of diagnosis. Figure 2 shows a comparison of the patients' gestational age, birth weight and duration of intubation between the non-confirmed and confirmed neonatal VAP cases.
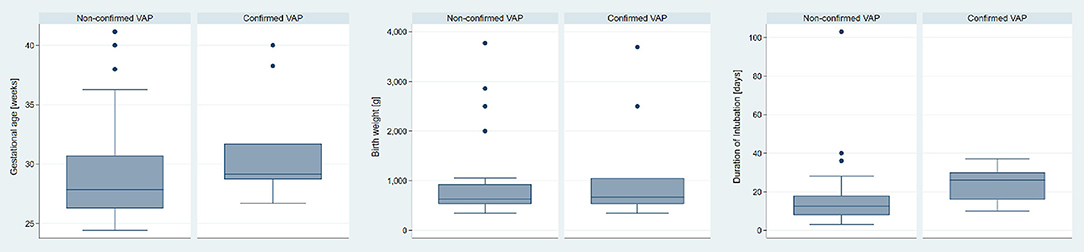
Figure 2. Comparison of gestational age, birth weight and duration of intubation; non-confirmed (n = 26) vs. confirmed (n = 10) neonatal VAP episodes.
Thirty-one out of the 36 analyzed tracheal aspirates showed bacterial growth (Table 5). Thirteen of the 31 culture positive tracheal aspirates also showed a purulent sputum. Among the 10 neonates with confirmed VAP, 8 had culture positive tracheal aspirates, thereof 4 presented with purulent sputum. Table 5 shows a listing of these results and of all isolated pathogens. In 13 cases only cultures of tracheal aspirates without blood cultures were taken. Of the 23 analyzed blood cultures only one showed bacterial growth (Staphylococcus aureus). This patient also showed growth of Staphylococcus aureus in the tracheal aspirate but was not diagnosed as a confirmed VAP according to our applied criteria.
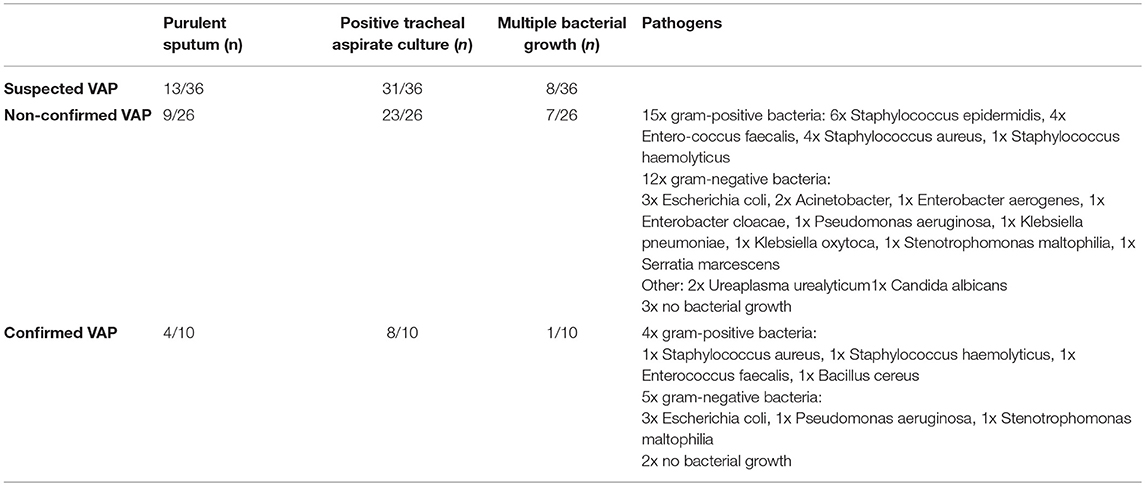
Table 5. Results of analyzed tracheal aspirates.
Comparison of agreement in rating all chest x-rays done for suspected neonatal VAP episodes showed an ICC of 0.25, thus showing a poor agreement between the 10 raters.
Quality Improvement Initiative
Characteristics of the NICU's patient population for 2015 - 2017 are shown in Table 6. There were no relevant differences except a reduction in mean ventilation days per patient from 2015 to 2017. Implemented changes resulted in a gradual decline in annual neonatal VAP incidence and antibiotic days. The annual neonatal VAP incidence for 2015 vs. 2017 was 28.8 vs. 7.4 suspected episodes/1,000 ventilator-days and 5.5 vs. 0 confirmed episodes/1,000 ventilator-days (Table 7). Antibiotic days declined from 211 in 2015 to 34.7 antibiotic days/1,000 ventilator-days in 2017 for suspected episodes and from 52 in 2015 to 0 antibiotic days/1,000 ventilator-days in 2017 for confirmed episodes. Duration of antibiotic treatment of suspected VAP episodes also declined over the years with a median duration of 8 (7–10) days in 2014 vs. 5 (2–7) days in 2017 (Figure 3). Cuzick's nonparametric test for trend showed a statistically significant trend for decreasing annual incidence of suspected VAP episodes, decreasing duration of antibiotic therapy per suspected VAP episode as well as decreasing annual antibiotic days for suspected VAP episodes from 2015 to 2017 (Table 7).
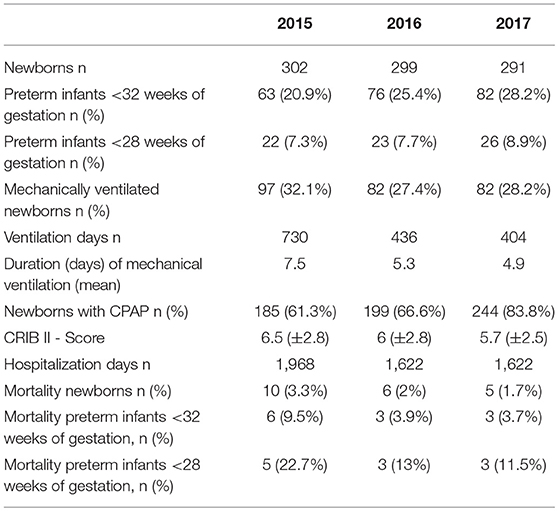
Table 6. Annual comparison of clinical characteristics of the patient population in our NICU.
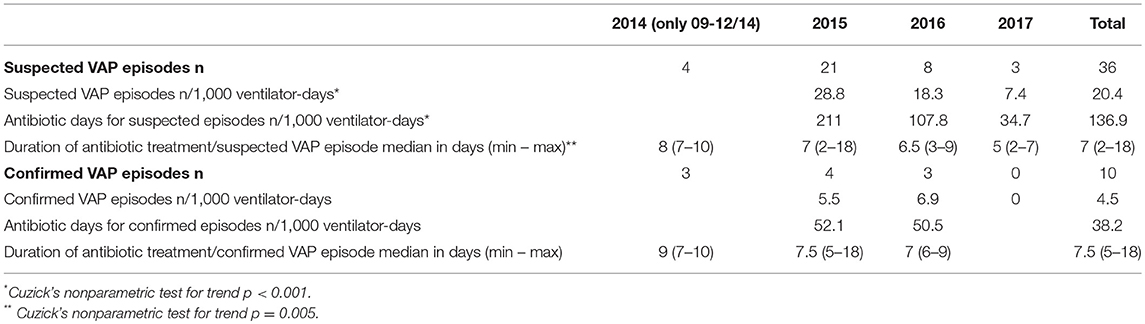
Table 7. Incidence of suspected and confirmed neonatal VAP and antibiotic use.
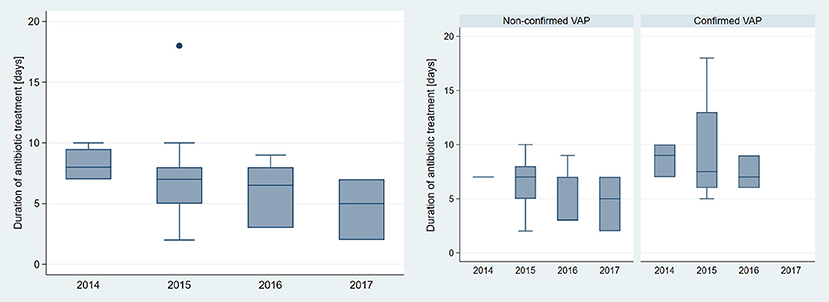
Figure 3. Comparison of duration of antibiotic treatment (antibiotic days/VAP episode) according to year. Left: all episodes (n = 36), right: non-confirmed (n = 26) vs. confirmed (n = 10) neonatal VAP.
Discussion
Our literature review showed that CDC guidelines for infants ≤ 1 year old or similar criteria to diagnose neonatal VAP were most often applied. These criteria are not especially adapted for the neonate or premature born population. The diagnostic criteria in 16 out of the 17 studies in our literature review requested abnormal chest x-rays. Evaluation of all chest x-rays done for suspected VAP episodes in our NICU showed a poor agreement between 10 senior physicians. This is in line with published studies describing the challenges of interpreting radiographic changes in patients with underlying lung diseases (29, 42, 43). An alternative diagnostic tool for lung pathologies is lung ultrasound (LUS). Different studies described the usefulness and accuracy of lung ultrasound for diagnosis of pneumonia in children (44, 45). Also, LUS has shown to be highly accurate for diagnosis of neonatal respiratory distress syndrome (46–48). LUS has been shown to be equivalent to chest x-rays in these studies. Hiles et al. (47) even described less intra-observer discrepancy in identification of small pneumonias. Further studies concerning sonographic diagnosis of pneumonia in the neonatal population are needed.
Additionally, unspecific clinical and laboratory findings challenge further the correct diagnosis of neonatal VAP (3, 49). Existence of purulent sputum is part of most used diagnostic criteria for VAP1 (22, 23). Only 4/10 of our confirmed neonatal VAP episodes showed purulent sputum. On the other hand, 31 out of all 36 neonates and 23 of the 26 non-confirmed VAP episodes showed bacterial growth in the analyzed tracheal aspirate. This might be caused by a high rate of colonization without clinical relevance. Cultures of tracheal aspirates are routinely taken if VAP is suspected although they are not part of most diagnostic criteria (37). Other authors described the frequent occurance of colonized tracheal aspirates (37, 50). A study by Ruiz et al. (51) showed no significant difference in diagnostic accuracy between noninvasive (tracheobronchial aspiration) vs. invasive (fiberoptic bronchoscopy with protected specimen brush and bronchoalveolar lavage) investigation techniques regarding VAP, thus not supporting more invasive procedures with more side effects. A study comparing treated vs. untreated episodes of culture-positive endotracheal aspirates showed that treated episodes also showed worse ventilation conditions, clinical symptoms and laboratory parameters (37), highlighting the limited usefulness of one diagnostic parameter by itself.
The moderate correlation for diagnosis of VAP according to 4 different frameworks in our study underlines the diagnostic problem. Incidence of VAP is often used as quality indicator and the discussed insecurity regarding diagnosis is a potential bias (49). Our findings, consistent with the published literature regarding the difficulty to diagnose neonatal VAP, demand an adaption of current diagnostic criteria for the neonatal population. On the other hand, due to the critical illness of neonates on the ventilator, early start of empiric antibiotic therapy for suspected VAP is mandatory. The challenge is to reevaluate empiric therapy after 24 to 36 hours combining clinical, laboratory and cultural findings. Figure 4 shows a possible algorithm to approach suspected VAP.
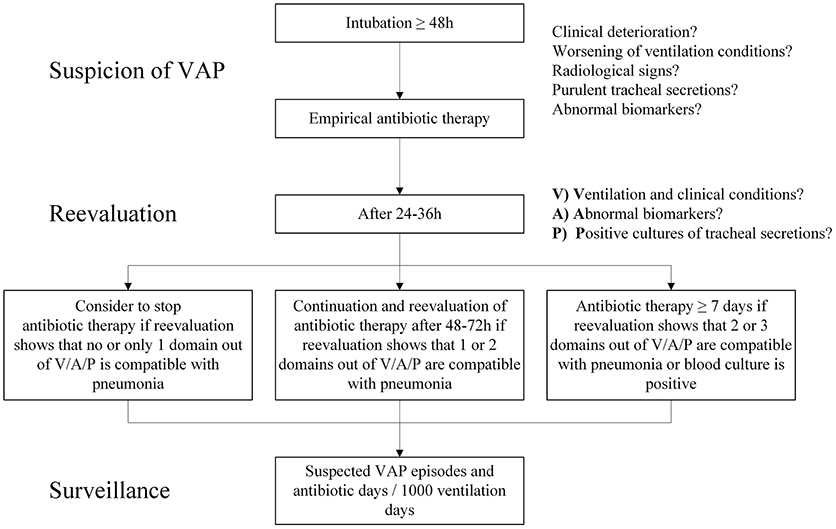
Figure 4. Possible algorithm to approach suspected VAP.
Comparison of incidence between suspected and confirmed neonatal VAP episodes in our NICU showed a 4.5 times higher rate for suspected vs. confirmed VAP episodes/1,000 ventilator-days (20.4 vs. 4.5). Our rate of 4.5 confirmed VAP episodes/1,000 ventilator-days over the whole study period is in line with the published incidence in the studies in our systematic review (2.7–11.8 in developed countries). Prompt antibiotic therapy for possible infections is important for optimal outcome in the neonate population (15) and newborns with suspected VAP are often treated empirically without reviewing defined criteria for VAP (6). Median duration of antibiotic treatment for suspected and confirmed VAP episodes in our cohort was 7 (2–18) and 7.5 (5–18) days, respectively. Also, Cantey et al. recently reported a wide range of antibiotic treatment duration for culture-negative neonatal pneumonia from 5 to 14 days (median 7 days) (5). Taking into account antibiotic treatment for all episodes of suspected neonatal VAP, overall antibiotic use is much higher than reported for confirmed VAP. Our results show a 3.5 times higher number in antibiotic days when including all suspected VAP episodes. We conclude that an inclusion of suspected VAP episodes should be considered for accurate assessment and quality control of VAP incidence and antibiotic use in the neonatal population.
Implementation of multifaceted changes regarding antimicrobial stewardship as well as infection control in our NICU resulted in an annual decrease of suspected and confirmed VAP episodes. Infection control measures are aimed at the prevention of nosocomial or healthcare-associated infections (52). Methods used for infection control include hand hygiene, isolation guidelines, handling and disinfection of patient care equipment, instruments and devices and use of personnel protective equipment (53). Introduction of VAP-care-bundles to prevent infections has already been done in different units showing a potential significant reduction of VAP episodes after implementation (8, 9). Furthermore, our changes resulted in an important annual decline in overall antibiotic days and treatment days per VAP episode. Antimicrobial stewardship aims to reduce inappropriate antibiotic therapy by improving selection, duration, dosage and application route of drugs (54). A systematic review by Kaki et al. (54) showed that implementation of antimicrobial stewardship interventions in different hospitals resulted in reduction of overall antibiotic use, inappropriate therapy, duration of therapy and adverse events toward antibiotics. A recently published antibiotic stewardship study by Cantey et al. (5) reported a safe reduction of antibiotic use for pneumonia in a NICU population. The implemented changes in our unit not only reduced confirmed neonatal VAP episodes, but also the numbers of suspected episodes. This resulted in a 6-fold reduction of at least partly unnecessary antibiotic days per 1,000 ventilator-days (211 vs. 34.7/1,000 ventilator-days for 2015 vs. 2017) and a statistically significant trend for decreasing duration of antibiotic therapy and antibiotic days in total over time from 2015 to 2017. Both, reduction of antibiotic days as well as declining VAP incidences resulted in this trend, with reduction of VAP episodes statistically being the more important composite. As several changes were initiated at various time points, it is not possible to distinguish the impact of a single measure. We assume that both, infection control and antibiotic stewardship measures together had an impact on the observed reduction in incidence of neonatal VAP and antibiotic use: antimicrobial stewardship measures by increasing awareness toward antibiotic therapy, and infection control measures by reducing VAP episodes and thus antibiotic therapy. A position paper published by the Association for Professionals in Infection Control and Epidemiology (APIC), the Society for Healthcare Epidemiology of America (SHEA), and the Society of Infectious Disease Pharmacists (SIDP) stated the importance of joining antimicrobial stewardship and infection control measures, as implementation of a combination of both is more effective than one measure by itself (10).
All studies in our systematic review state long duration of mechanical ventilation as a risk factor for developing neonatal VAP. Comparing patient population of non-confirmed vs. confirmed VAP episodes, confirmed episodes in our NICU were also associated with longer duration of mechanical ventilation. Studies by Hentschel et al. (55) and Geffers et al. (56) showed lower pneumonia rates in patients ventilated with CPAP-devices compared to intubated patients. These studies support the strategy toward early extubation. Implementation of our early-extubation policy in our unit resulted in a decrease of duration of invasive ventilation without increase of mortality.
There are several limitations to our study: Firstly and most important, this is not an intervention study with a control group aiming to prove the causative benefit of the implemented changes. Nevertheless, the reduction of incidence and antibiotic use for neonatal VAP is remarkable. The NICU's patient population did not change remarkably over the three years and there were no other changes over the study period applied. Therefore, we could not determine any other apparent reason for the decline in numbers. Secondly, the sample size of VAP episodes is small and therefore it was not possible to further analyze and compare more risk factors or clinical indicators. Also numbers for confirmed VAP episodes are only descriptive as no further statistical calculations were done due to the even smaller sample size. Thirdly, whereas all VAP episodes were collected prospectively, diagnostic analyzes according to the 4 frameworks were done in retrospect.
Conclusions
Diagnosis and confirmation of neonatal VAP is difficult, resulting in a great variance between suspected and confirmed episodes. An adaption of current diagnostic criteria for the neonate population might be helpful for more consistency. Inclusion of both confirmed and suspected episodes should be considered for accurate evaluation and comparison of VAP incidence and antibiotic use in the neonatal population as quality indicators. Implementation of combined antimicrobial stewardship and infection control measures may lead to an effective decrease in both VAP incidence and antibiotic use.
Ethics Statement
The study was carried out in accordance with the recommendations of the national ethics committee (Ethikkommission Nordwest- und Zentralschweiz EKNZ: Project-ID 2017-01842) with informed consent from patients' parents/guardians. The EKNZ exempt to have a written consent due to the fully anonymized data and the quality improvement focus of the study without need of additional information than obtained from patient files.
Author Contributions
MS devised the project, details of implementation were discussed between MS and AG. Data collection and writing of the manuscript was done by AG, closely revised by MS. Statistical calculations were done by DL. The literature review was done by AG. Interpretation of chest-x-rays was done by NR, MB, ML, KD, KS-S, SP, PG, DM, MF, and MS. Critical revising of the work was done by TN, NR, MB, ML, KS-S, SP, PG, DM, MF, and KD. All authors read and approved the submitted version of this manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Special thanks to Barbara Imboden, the NICU's data manager for all the work she has put in this beforehand and of course the indispensable nursing team of our NICU. Special thanks as well to Evelyne Eichenberger and Luzia Vetter being part of the interprofessional working group for development and implementation of the VAP-prevention-bundle.
Abbreviations
CDC, Center for Diseases Control and Prevention; CLABSI, Central line associated blood stream infections; CPAP, Continuous positive airway pressure; CRIB, Clinical risk index for babies; CRP, C-reactive protein; ECDC, European Centre for Disease Prevention and Control; ETA, Endotracheal aspirate; ETT, Endotracheal tube; I:T ratio, Immature neutrophils to total neutrophils; ICC, Intra-class correlation coefficient; LUS, Lung ultrasound; NICU, Neonatal intensive care unit; VAP, Ventilator associated pneumonia; WBC, White blood cell count.
Footnotes
1. ^0512-TED-PPS-HAI-antimicrobial-use-protocol. Available online at: https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/0512-TED-PPS-HAI-antimicrobial-use-protocol.pdf (Accessed September 16, 2017).
References
1. Cernada M, Aguar M, Brugada M, Gutiérrez A, López JL, Castell M, et al. Ventilator-associated pneumonia in newborn infants diagnosed with an invasive bronchoalveolar lavage technique: a prospective observational study. Pediatr Crit Care Med. (2013) 14:55–61. doi: 10.1097/PCC.0b013e318253ca31
2. Hooven TA, Polin RA. Pneumonia. Semin Fetal Neonatal Med. (2017) 22:206–13. doi: 10.1016/j.siny.2017.03.002
3. Cernada M, Brugada M, Golombek S, Vento M. Ventilator-associated pneumonia in neonatal patients: an update. Neonatology (2014) 105:98–107. doi: 10.1159/000355539
4. Willson DF, Hoot M, Khemani R, Carrol C, Kirby A, Schwarz A, et al. Pediatric ventilator-associated infections: the ventilator-associated infection study. Pediatr Crit Care Med. (2017) 18:e24–34. doi: 10.1097/PCC.0000000000001001
5. Cantey JB, Wozniak PS, Pruszynski JE, Sánchez PJ. Reducing unnecessary antibiotic use in the neonatal intensive care unit (SCOUT): a prospective interrupted time-series study. Lancet Infect Dis. (2016) 16:1178–84. doi: 10.1016/S1473-3099(16)30205-5
6. Cantey JB, Wozniak PS, Sánchez PJ. Prospective surveillance of antibiotic use in the neonatal intensive care unit: results from the SCOUT study. Pediatr Infect Dis J. (2015) 34:267–72. doi: 10.1097/INF.0000000000000542
7. Bradley JS. Considerations unique to pediatrics for clinical trial design in hospital-acquired pneumonia and ventilator-associated pneumonia. Clin Infect Dis. (2010) 51(Suppl. 1):S136–43. doi: 10.1086/653063
8. Azab SFA, Sherbiny HS, Saleh SH, Elsaeed WF, Elshafiey MM, Siam AG, et al. Reducing ventilator-associated pneumonia in neonatal intensive care unit using “VAP prevention Bundle”: a cohort study. BMC Infect Dis. (2015) 15:314. doi: 10.1186/s12879-015-1062-1
9. Weber CD. Applying adult ventilator-associated pneumonia bundle evidence to the ventilated neonate. Adv Neonatal Care (2016) 16:178–90. doi: 10.1097/ANC.0000000000000276
10. Manning ML, Septimus EJ, Ashley ESD, Cosgrove SE, Fakih MG, Schweon SJ, et al. Antimicrobial stewardship and infection prevention—leveraging the synergy: a position paper update. Infect Control Hosp Epidemiol. (2018) 39:467–72. doi: 10.1017/ice.2018.33
11. Spitzer AR. Has quality improvement really improved outcomes for babies in the neonatal intensive care unit? Clin Perinatol. (2017) 44:469–83. doi: 10.1016/j.clp.2017.04.005
12. Clark RH, Bloom BT, Spitzer AR, Gerstmann DR. Reported medication use in the neonatal intensive care unit: data from a large national data set. Pediatrics (2006) 117:1979–87. doi: 10.1542/peds.2005-1707
13. Schulman J, Dimand RJ, Lee HC, Duenas GV, Bennett MV, Gould JB. Neonatal intensive care unit antibiotic use. Pediatrics (2015) 135:826–33. doi: 10.1542/peds.2014-3409
14. Liem TBY, Krediet TG, Fleer A, Egberts TCG, Rademaker CMA. Variation in antibiotic use in neonatal intensive care units in the Netherlands. J Antimicrob Chemother. (2010) 65:1270–5. doi: 10.1093/jac/dkq107
15. Weiss SL, Fitzgerald JC, Balamuth F, Alpern ER, Lavelle J, Chilutti M, et al. Delayed antimicrobial therapy increases mortality and organ dysfunction duration in pediatric sepsis. Crit Care Med. (2014) 42:2409–17. doi: 10.1097/CCM.0000000000000509
16. Cantey JB, Patel SJ. Antimicrobial stewardship in the NICU. Infect Dis Clin North Am. (2014) 28:247–61. doi: 10.1016/j.idc.2014.01.005
17. Jernberg C, Löfmark S, Edlund C, Jansson JK. Long-term impacts of antibiotic exposure on the human intestinal microbiota. Microbiol Read Engl. (2010) 156:3216–23. doi: 10.1099/mic.0.040618-0
18. Schulfer A, Blaser MJ. Risks of antibiotic exposures early in life on the developing microbiome. PLoS Pathog (2015) 11:e1004903. doi: 10.1371/journal.ppat.1004903
19. Gensollen T, Iyer SS, Kasper DL, Blumberg RS. How colonization by microbiota in early life shapes the immune system. Science (2016) 352:539–44. doi: 10.1126/science.aad9378
20. Mukhopadhyay S, Puopolo KM. Antibiotic use and mortality among premature infants without confirmed infection-perpetrator or innocent bystander? JAMA Pediatr. (2016) 170:1144–6. doi: 10.1001/jamapediatrics.2016.2836
21. Ting JY, Synnes A, Roberts A, Deshpandey A, Dow K, Yoon EW, et al. Association between antibiotic use and neonatal mortality and morbidities in very low-birth-weight infants without culture-proven sepsis or necrotizing enterocolitis. JAMA Pediatr. (2016) 170:1181–7. doi: 10.1001/jamapediatrics.2016.2132
22. 6pscvapcurrent.pdf. Available online at: https://www.cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf (Accessed September 16, 2017).
23. van der Zwet WC, Kaiser AM, van Elburg RM, Berkhof J, Fetter WPF, Parlevliet GA, et al. Nosocomial infections in a Dutch neonatal intensive care unit: surveillance study with definitions for infection specifically adapted for neonates. J Hosp Infect. (2005) 61:300–11. doi: 10.1016/j.jhin.2005.03.014
24. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ (2009) 339:b2700. doi: 10.1136/bmj.b2700
25. Berger TM, Steurer MA, Woerner A, Meyer-Schiffer P, Adams M Swiss Neonatal Network. Trends and centre-to-centre variability in survival rates of very preterm infants (< 32 weeks) over a 10-year-period in Switzerland. Arch Dis Child Fetal Neonatal Ed. (2012) 97:F323–8. doi: 10.1136/fetalneonatal-2011-301008
27. Afjeh SA, Sabzehei MK, Karimi A, Shiva F, Shamshiri AR. Surveillance of ventilator-associated pneumonia in a neonatal intensive care unit: characteristics, risk factors, and outcome. Arch Iran Med. (2012) 15:567–71.
28. Apisarnthanarak A, Holzmann-Pazgal G, Hamvas A, Olsen MA, Fraser VJ. Ventilator-associated pneumonia in extremely preterm neonates in a neonatal intensive care unit: characteristics, risk factors, and outcomes. Pediatrics (2003) 112:1283–9. doi: 10.1542/peds.112.6.1283
29. Foglia E, Meier MD, Elward A. Ventilator-associated pneumonia in neonatal and pediatric intensive care unit patients. Clin Microbiol Rev. (2007) 20:409–25, table of contents. doi: 10.1128/CMR.00041-06
30. Badr MA, Ali YF, Albanna EAM, Beshir MR, Amr GE. Ventilator associated pneumonia in critically-ill neonates admitted to neonatal intensive care unit, zagazig university hospitals. Iran J Pediatr. (2011) 21:418–24.
31. Deng C, Li X, Zou Y, Wang J, Wang J, Namba F, et al. Risk factors and pathogen profile of ventilator-associated pneumonia in a neonatal intensive care unit in China. Pediatr Int. (2011) 53:332–7. doi: 10.1111/j.1442-200X.2011.03382.x
32. 20272-pdf.pdf. Available online at: http://cdn.neoscriber.org/cdn/serve/313ea/c85402d4f1abb36c538a084940e4815755ccd005/20272-pdf.pdf (Accessed March 2, 2018).
33. Katayama Y, Minami H, Enomoto M, Takano T, Hayashi S, Lee YK. Usefulness of Gram staining of tracheal aspirates in initial therapy for ventilator-associated pneumonia in extremely preterm neonates. J Perinatol. (2010) 30:270–4. doi: 10.1038/jp.2009.144
34. Kawanishi F, Yoshinaga M, Morita M, Shibata Y, Yamada T, Ooi Y, et al. Risk factors for ventilator-associated pneumonia in neonatal intensive care unit patients. J Infect Chemother. (2014) 20:627–30. doi: 10.1016/j.jiac.2014.06.006
35. Khattab AA, El-Lahony DM, Soliman WF. Ventilator-associated pneumonia in the neonatal intensive care unit. Menoufia Med J. (2014) 27:73–7. doi: 10.4103/1110-2098.132753
36. Lee P-L, Lee W-T, Chen H-L. Ventilator-associated pneumonia in low birth weight neonates at a neonatal intensive care unit: a retrospective observational study. Pediatr Neonatol. (2017) 58:16–21. doi: 10.1016/j.pedneo.2015.10.014
37. Murila F, Francis JV, Bland A, Kumbla S, Doherty R, Sehgal A. Interpreting positive cultures of endotracheal aspirates: factors associated with treatment decisions in ventilated neonates. J Paediatr Child Health (2011) 47:728–33. doi: 10.1111/j.1440-1754.2011.02041.x
38. Petdachai W. Ventilator-associated pneumonia in a newborn intensive care unit. Southeast Asian J Trop Med Public Health (2004) 35:724–9.
39. Thatrimontrichai A, Rujeerapaiboon N, Janjindamai W, Dissaneevate S, Maneenil G, Kritsaneepaiboon S, et al. Outcomes and risk factors of ventilator-associated pneumonia in neonates. World J Pediatr. (2017) 13:328–34. doi: 10.1007/s12519-017-0010-0
40. Paper02_Jan2010_.pdf. Available online at: http://www.akspublication.com/Paper02_Jan2010_.pdf?B1=Full+Text+PDF (Accessed March 2, 2018).
41. Yuan T-M, Chen L-H, Yu H-M. Risk factors and outcomes for ventilator-associated pneumonia in neonatal intensive care unit patients. J Perinat Med. (2007) 35:334–8. doi: 10.1515/JPM.2007.065
42. Klompas M. Interobserver variability in ventilator-associated pneumonia surveillance. Am J Infect Control. (2010) 38:237–9. doi: 10.1016/j.ajic.2009.10.003
43. Morrow BM, Argent AC. Filling the gaps in neonatal VAP. Pediatr Crit Care Med. (2013) 14:105–6. doi: 10.1097/PCC.0b013e31825b8648
44. Copetti R, Cattarossi L. Ultrasound diagnosis of pneumonia in children. Radiol Med. (2008) 113:190–8. doi: 10.1007/s11547-008-0247-8
45. Reali F, Sferrazza Papa GF, Carlucci P, Fracasso P, Di Marco F, Mandelli M, et al. Can lung ultrasound replace chest radiography for the diagnosis of pneumonia in hospitalized children? Respiration (2014) 88:112–5. doi: 10.1159/000362692
46. Lovrenski J. Lung ultrasonography of pulmonary complications in preterm infants with respiratory distress syndrome. Ups J Med Sci. (2012) 117:10–7. doi: 10.3109/03009734.2011.643510
47. Hiles M, Culpan A-M, Watts C, Munyombwe T, Wolstenhulme S. Neonatal respiratory distress syndrome: chest X-ray or lung ultrasound? a systematic review. Ultrasound (2017) 25:80–91. doi: 10.1177/1742271X16689374
48. Vergine M, Copetti R, Brusa G, Cattarossi L. Lung ultrasound accuracy in respiratory distress syndrome and transient tachypnea of the newborn. Neonatology (2014) 106:87–93. doi: 10.1159/000358227
49. Cordero L, Ayers LW, Miller RR, Seguin JH, Coley BD. Surveillance of ventilator-associated pneumonia in very-low-birth-weight infants. Am J Infect Control (2002) 30:32–9. doi: 10.1067/mic.2002.119995
50. Gibbs K, Holzman IR. Endotracheal tube: friend or foe? bacteria, the endotracheal tube, and the impact of colonization and infection. Semin Perinatol. (2012) 36:454–61. doi: 10.1053/j.semperi.2012.06.008
51. Ruiz M, Torres A, Ewig S, Marcos MA, Alcón A, Lledó R, et al. Noninvasive versus invasive microbial investigation in ventilator-associated pneumonia. Am J Respir Crit Care Med. (2000) 162:119–25. doi: 10.1164/ajrccm.162.1.9907090
52. WHO-HIS-SDS-2016.10-eng.pdf. Available online at: http://apps.who.int/iris/bitstream/handle/10665/246235/WHO-HIS-SDS-2016.10-eng.pdf;jsessionid=6C5077BF50A066B4F577CA5882023273?sequence=1 (Accessed April 15, 2018).
53. Infection Control Basics. Infection Control CDC. Available online at: https://www.cdc.gov/infectioncontrol/basics/index.html (Accessed April 15, 2018).
54. Kaki R, Elligsen M, Walker S, Simor A, Palmay L, Daneman N. Impact of antimicrobial stewardship in critical care: a systematic review. J Antimicrob Chemother. (2011) 66:1223–30. doi: 10.1093/jac/dkr137
55. Hentschel J, Brüngger B, Stüdi K, Mühlemann K. Prospective surveillance of nosocomial infections in a Swiss NICU: low risk of pneumonia on nasal continuous positive airway pressure? Infection (2005) 33:350–5. doi: 10.1007/s15010-005-5052-x
Keywords: neonatal ventilator associated pneumonia, diagnostic criteria, quality improvement, antibiotic stewardship, infection control, risk factors
Citation: Goerens A, Lehnick D, Büttcher M, Daetwyler K, Fontana M, Genet P, Lurà M, Morgillo D, Pilgrim S, Schwendener-Scholl K, Regamey N, Neuhaus TJ and Stocker M (2018) Neonatal Ventilator Associated Pneumonia: A Quality Improvement Initiative Focusing on Antimicrobial Stewardship. Front. Pediatr. 6:262. doi: 10.3389/fped.2018.00262
Received: 21 June 2018; Accepted: 03 September 2018;
Published: 24 September 2018.
Edited by:
Christoph Bührer, Charité Universitätsmedizin Berlin, GermanyReviewed by:
Georg Schmolzer, University of Alberta, CanadaGiovanni Vento, Università Cattolica del Sacro Cuore, Italy
Copyright © 2018 Goerens, Lehnick, Büttcher, Daetwyler, Fontana, Genet, Lurà, Morgillo, Pilgrim, Schwendener-Scholl, Regamey, Neuhaus and Stocker. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Stocker, bWFydGluLnN0b2NrZXJAbHVrcy5jaA==