 Janmilli da Costa Dantas1*
Janmilli da Costa Dantas1* Cristiane da Silva Ramos Marinho2
Cristiane da Silva Ramos Marinho2 Yago Tavares Pinheiro1Maria Ângela Fernandes Ferreira1Richardson Augusto Rosendo da Silva1
Yago Tavares Pinheiro1Maria Ângela Fernandes Ferreira1Richardson Augusto Rosendo da Silva1
- 1Graduate Program in Collective Health, Health Science Center, Federal University of Rio Grande Do Norte, Natal, Brazil
- 2Graduate Program in Collective Health, Faculty of Health Sciences of Trairi, Federal University of Rio Grande Do Norte, Santa Cruz, Brazil
Objective: The study aimed to analyze the temporal trend of congenital syphilis in Brazil in the period from 2008 to 2018 and its spatial distribution in the Immediate Regions of Urban Articulation, and to identify spatial correlations with socioeconomic factors and prenatal care.
Methods: Spatial correlations between the incidence of congenital syphilis and socioeconomic conditions and access to prenatal care were assessed. This ecological study conducted a time series analysis in Brazil and spatial analysis in 482 Immediate Regions of Urban Articulation. Cases of congenital syphilis reported in the Notifiable Diseases Information System and the Live Birth Information System from January 1, 2008, to December 31, 2018 were included. Socioeconomic conditions (percentage of individuals with inadequate water supply and sanitation) were extracted from the 2010 census, whereas the Live Birth Information System provided data on access to prenatal care (percentage of live births with 1–3 prenatal care appointments). The Joinpoint Regression software performed the temporal trend analysis, while the GeoDa software assessed territorial clusters using the Moran’s I and Local Spatial Association Indicator.
Results: The incidence of congenital syphilis showed an upward trend (annual percent change 1 = 26.96; 95% CI: 18.2–36.3; annual percent change 2 = 10.25; 95% CI: 2.7–28.4) and was unevenly distributed across Immediate Regions of Urban Articulation in Brazil (Moran’s I = 0.264, p ≤ 0.05). It also presented a direct spatial correlation with the percentage of individuals with inadequate water supply and sanitation (Moran’s I = 0.02, p ≤ 0.05) and the percentage of live births with 1–3 prenatal care appointments (Moran’s I = 0.03, p ≤ 0.05).
Conclusion: Agrowth trend of congenital syphilis in Brazil was observed between 2008 and 2018. Moreover, inequalities in socioeconomic conditions and access to prenatal care influenced the spatial distribution of this disease.
Introduction
Pregnant women infected with Treponema pallidum and not diagnosed and treated during prenatal care may transmit syphilis to the fetus, leading to congenital syphilis (CS) (1, 2). Adverse events from this infection (e.g., abortion, stillbirth, premature birth, neonatal death, and early or late congenital manifestations) also impact maternal and neonatal health (3).
In 2016, 355,000 adverse birth outcomes due to CS were reported in the world, including 143,000 fetal deaths, 61,000 neonatal deaths, and 41,000 premature births with low birth weight newborns. In this same year, the highest and lowest incidences were observed, respectively, in the African (12 cases per 1,000 live births) and European (0.2 cases per 1,000 live births) continents. The worldwide incidence of CS decreased from 5.4 to 4.7 cases per 1,000 live births between 2012 and 2016, except in the American and the Eastern Mediterranean Regions. In this period, CS increased from 3.07 to 3.19 cases per 1,000 live births in the Americas, with Brazil reporting 85% of cases in Latin America (4). Also, Brazil recorded 260,596 cases of CS from 1998 to 2020; 22,065 cases were reported only in 2020, resulting in an incidence of 7.7 cases per 1,000 live births (5).
In 2016, the World Health Organization (WHO) developed a program to reduce the incidence of CS to 0.5 or few cases per 1,000 live births by 2030 in 80% of countries. In 2017, eleven countries or territories obtained validation, according to criteria established by the World Health Organization with regard to the elimination of mother-to-child transmission of HIV and/or syphilis (6). However, controlling CS requires data on temporal evolution, spatial distribution, and factors associated with disease spread. These data may be used for evaluation, planning, decision-making, management, and development of effective health policies (7).
Temporal trend, spatial distribution, and factors associated with CS are commonly evaluated in states or cities, but researchers rarely consider the entire Brazilian territory. In addition, the analysis of CS correlating the geographic location with socioeconomic conditions and access to prenatal care may contribute to disease control.
The increase in CS is influenced by several factors, such as the socioeconomic characteristics of the population and access to health services. Research points out that the high GINI index (8), low education of women, disadvantaged social strata (9, 10) and low number of prenatal consultations (10) hinder the control of CS.
In this scenario, this study aimed to analyze the temporal trend of congenital syphilis in Brazil in the period from 2008 to 2018 and its spatial distribution in the Immediate Regions of Urban Articulation, and to identify spatial correlations with socioeconomic factors and prenatal care.
Methods
This ecological study used secondary, aggregated, public-domain data from Brazilian cities. According to resolution 510/2016 of the Brazilian National Health Council, approval by an ethics committee for this type of research is unnecessary.
Brazil is the largest country in South America. Is divided into 5,565 cities, 27 states, including the Federal District, according to a regional model used by the Brazilian Institute of Geography and Statistics (IBGE), in 2010. Brazil can also be divided into five macro-regions: North, Northeast, Midwest, South, and Southeast (11). Moreover, the Urban Regional Division classifies the Brazilian territory into Extended (14 territories), Intermediate (161 territories), and Immediate Regions of Urban Articulation (RUAs) (482 territories). In this model, regions are contiguous, and each city is part of a territorial unit with limits unrestricted to state borders. Each region has a leading city that influences other cities by offering highly complex goods and services (12). Thus, our study used Brazil for time series analysis and Immediate RUAs for spatial analysis.
Data were collected between June and July 2021 from publicly accessible databases linked to the Ministry of Health of Brazil, the Department of Informatics of the Unified Health System (DATASUS), and the National Human Development Program.
The health information systems in Brazil present a temporal delay to make their data available for public access. During the data collection period, Information System for Notifiable Diseases (SINAN) provided data on reported cases of congenital syphilis up to December 2018. Thus, the extracted data referred to the period of 11 years, comprising the years from 2008 to 2018.
The incidence rate of congenital syphilis is the dependent variable of the study. This rate was calculated, for each year of the study, from the number of reported cases of congenital syphilis in the city in that year, divided by the number of live births in the city in the same period, and then multiplied by 1,000. In order to obtain the data of the variable Congenital Syphilis incidence rate, the number of reported cases of CS per residence was obtained from SINAN; and the number of live births was obtained from SINASC (Information System of Live Births).
The Brazilian Ministry of Health (13) adopts definition criteria for congenital syphilis notification. These criteria include every newborn, stillbirth, or abortion of a woman with untreated or inadequately treated syphilis; microbiological evidence of Treponema Pallidum infection in a nasal secretion sample or skin lesion, biopsy, or necropsy of an abortion, stillbirth, or child. It also defines CS as every child under 13 years of age with clinical, cerebrospinal fluid or radiological manifestation of congenital syphilis and a positive non-treponemal test (VDRL or RPR).
Several socioeconomic and health care-related variables that could have an influence on determining the incidence rate of congenital syphilis were calculated after extracting data from the information systems. Using the Geoda software, it was possible to detect the variables that showed significant spatial correlation with the incidence rate of congenital syphilis. Among the variables tested in the spatial correlation, two showed significant spatial correlation with the incidence rate of congenital syphilis: (1) the percentage of people in households with inadequate water supply and sanitary sewage system (obtained from the National Human Development Program), (2) percentage of live births with 1–3 prenatal consultations (obtained from SINASC). Thus, these two independent variables were adopted in the study because they were statistically significant in the spatialization of the data.
The inadequate water supply and sanitary sewerage system in a population is related to economic and social issues in municipalities with low HDI-M (14), thereby justifying, in this research, the use of the variable percentage of people in households with inadequate water supply and sanitary sewerage system as related to the socioeconomic conditions of a population. For adequate prenatal care, a minimum of six prenatal consultations is recommended (8). Accordingly, related to prenatal care, the research used the variable percentage of live births with 1–3 prenatal consultations.
Other variables were tested, but did not show significant spatial correlation with the incidence rate of CS: MDI-M, GINI index, illiteracy rate in women 15 years old and older, percentage of primary care coverage, percentage of live births with no prenatal consultations, percentage of live births with 4–6 prenatal consultations, percentage of live births with 7 or more prenatal consultations.
The incidence of CS and percentage of live births with 1–3 prenatal appointments were collected from 2008 to 2018, whereas data on socioeconomic conditions were obtained from the 2010 census.
Data on the incidence of CS were normalized for live births in the same period to minimize discrepancies in indicators due to different population sizes. The study variables are detailed in Table 1.
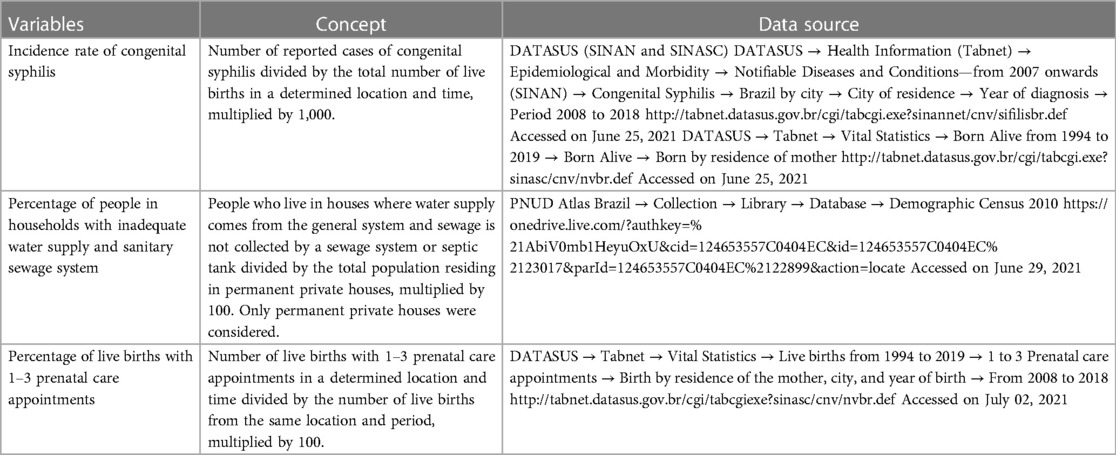
Table 1. Characteristics of dependent and independent variables used to assess the spatial distribution of congenital syphilis in immediate regions of urban articulation of Brazil from 2008 to 2018.
For the trend analysis, the incidence rate of congenital syphilis was used exclusively, adopting Brazil as the unit of analysis. The Joinpoint Regression software performed the temporal trend analysis by adjusting a series of trend lines and junction points on a logarithmic scale and testing annual trends. The annual percent change (APC) and 95% confidence intervals (95% CI) were also estimated and tested; the Monte Carlo permutation test assessed statistical significance (15).
The spatial analysis was performed with the variable “outcome” and the independent variables “percentage of people in households with inadequate water supply and sanitary sewerage system” and “percentage of live births with 1–3 prenatal consultations”, using as unit of analysis the RUAs of Brazil. The GeoDa software performed an exploratory analysis to assess the spatial distribution of variables. The Global Moran’s I and Local Indicators of Spatial Association (LISA) tests were applied. Global Moran’s I coefficients verified the spatial autocorrelation of variables. Results ranged from −1 (inverse correlation) to +1 (direct correlation); a value of 0 represented no correlation. Values of local Moran’s I of the 482 RUAs were submitted to the Moran’s Scatter Diagram with significance set at 5% (p ≤ 0.05). RUAs were classified into five categories: high-high (unit and neighbors had values higher than the average of the set), high-low (high value for the unit and low average values for neighbors), low-high (the unit had low value for a variable, whereas neighbors had values above the average of the set), low-low (values of the unit and neighbors were below the average of the set), and without significance (the unit had no defined association with neighbors) (16, 17).
Results
The SINAN recorded 164,293 cases of CS in Brazil from 2008 to 2018; the lowest incidence was recorded in 2008 (1.18 cases per 1,000 live births) and the highest in 2017 (8.65 cases per 1,000 live births). Thus, the incidence of CS showed an upward trend, growing by over 450%.
An increasing trend was observed in the incidence of CS in Brazil (APC 1 = 26.96; 95% CI: 18.2–36.3; APC 2 = 10.25; 95% CI: 2.7–18.4) and an inflection point in 2013 (Figure 1 and Table 2).
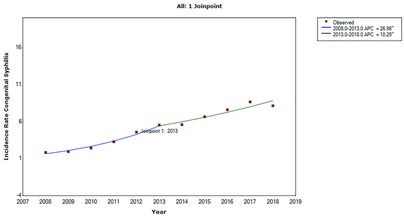
Figure 1. Time series of the incidence rate of congenital syphilis (dots) in Brazil from 2008 to 2018, according to the final selected model: 1 joinpoint. ^Indicates that the annual percent change (APC) is significantly different from zero at the alpha = 0.05 level.
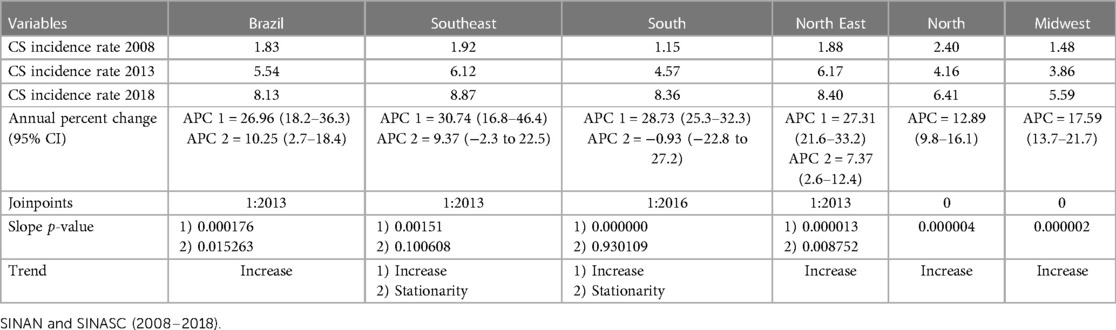
Table 2. Incidence rate trend of congenital syphilis in Brazil and macro-regions, 2008–2018.
The clusters of the incidence rate of CS were presented unevenly in the RUAs of Brazil (Moran’s I = 0.26; p ≤ 0.05), between 2008 and 2018, as shown in Figure 2. Coastal areas in the Northeast region and Mato Grosso do Sul, Rio Grande do Sul, and Rio de Janeiro states presented the highest incidences of CS. Moreover, clusters in RUAs in the five macro-regions of the country were found, with the incidence of CS ranging from 3.44 to 5.72 cases per 1,000 live births. Clusters in RUAs presenting the lowest incidences of CS were also distributed in the Brazilian macro-regions, covering the central area of the Northeast and part of the Midwest, mainly the state of Mato Grosso.
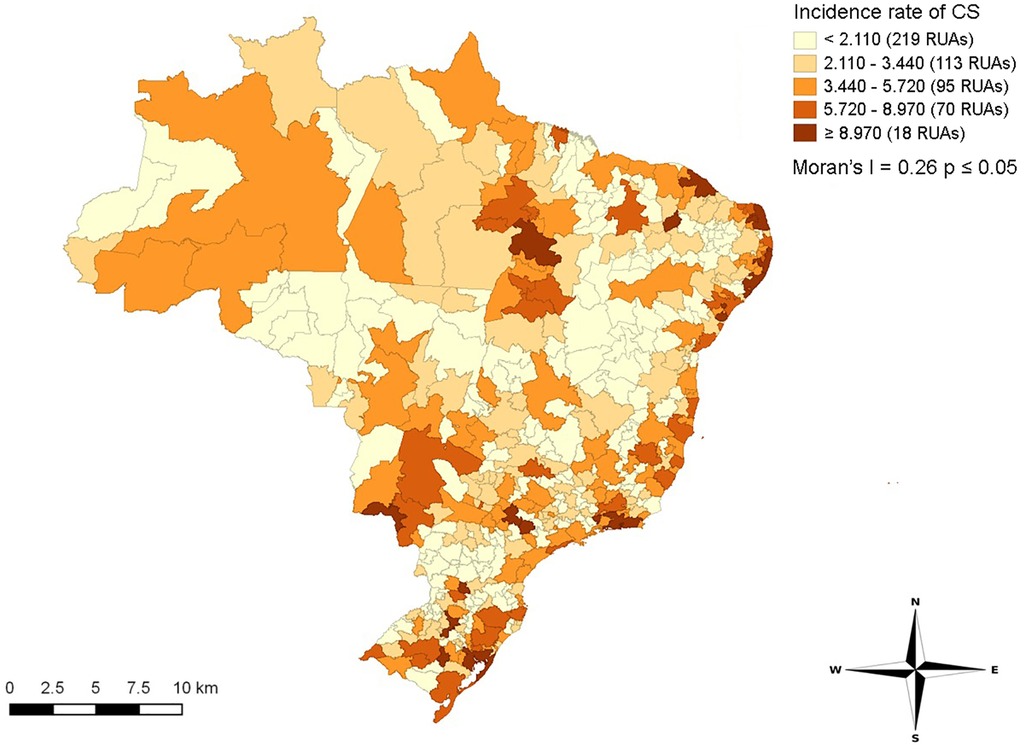
Figure 2. Spatial distribution of clusters (exploratory map) of the incidence rate of congenital syphilis, in immediate regions of urban articulation in Brazil, 2008–2018.
Figure 3 shows clusters classified as high-high for the incidence rate of CS in coastal areas of the Northeast and small areas in the Southeast, South, and part of the Midwest. On the other hand, the central areas of the Northeast region and Tocantins, Rondônia, and Mato Grosso states presented low-low clusters for the incidence rate of CS.
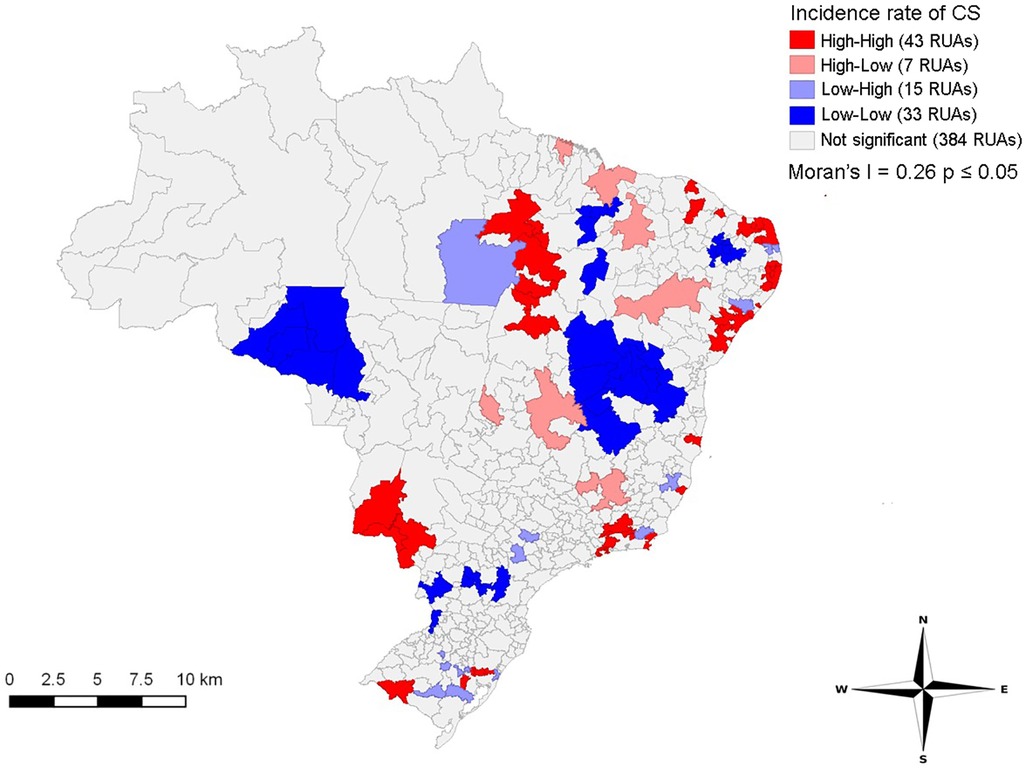
Figure 3. Spatial distribution of clusters (moran map) of the incidence rate of congenital syphilis in immediate regions of urban articulation in Brazil, 2008–2018.
Figure 4 shows direct spatial correlations between the incidence rate of CS and the percentage of individuals with inadequate water supply and sanitation (Moran’s I = 0.02, p ≤ 0.05). Clusters in RUAs from coastal areas of Northeast and North regions presented a high incidence rate of CS and percentage of individuals with inadequate water supply and sanitation. In contrast, the South, Southeast and small areas of the Midwest showed clusters in IRUAs with low percentages of individuals with inadequate water supply and sanitary sewage system and low incidence rates of congenital syphilis. The data reflect the influence of socioeconomic conditions in specific areas on the incidence of congenital syphilis, with areas with disadvantaged socioeconomic conditions being more affected by the incidence of the illness.
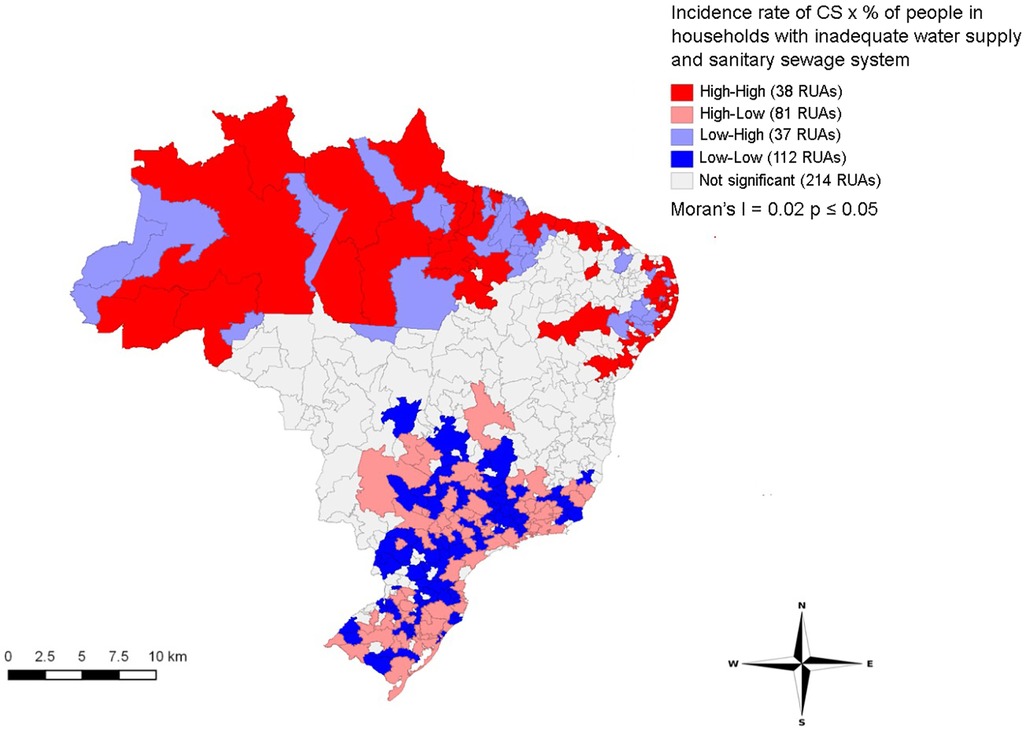
Figure 4. Distribution of LISA bivariate spatial correlation clusters of congenital syphilis incidence rate with the socioeconomic indicator in immediate regions of urban articulation in Brazil, 2008–2018.
Figure 5 shows spatial correlations between the incidence rate of CS and percentage of live births with 1–3 prenatal care appointments (Moran’s I = 0.03, p ≤ 0.05). The LISA method indicated a direct correlation among clusters of the variables. RUAs in the North and part of Northeast (Maranhão, Piauí, Sergipe, and Bahia states) had larger clusters of CS and a high percentage of live births with 1 to 3 prenatal care appointments. On the other hand, RUAs in the South and Southeast presented clusters with high incidence of CS and low percentage of live births with 1–3 prenatal care appointments.
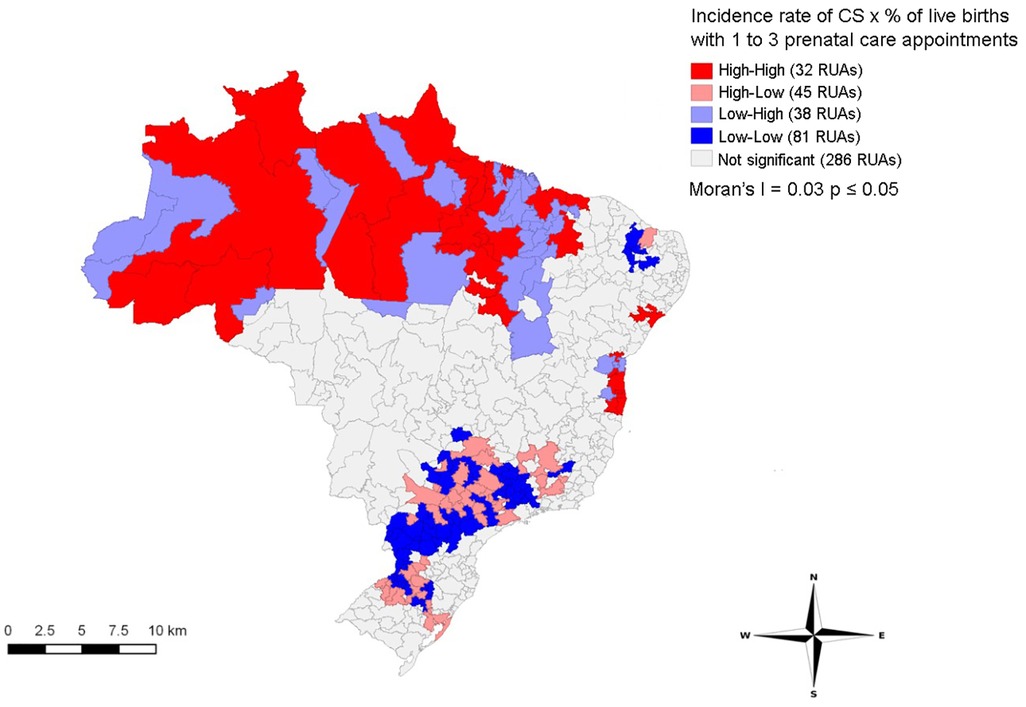
Figure 5. Distribution of LISA bivariate spatial correlation clusters of congenital syphilis incidence rate with the indicator prenatal care in immediate regions of urban articulation in Brazil, 2008–2018.
Discussion
The historical series indicated an upward trend in the incidence of CS in Brazil, emphasizing the need for effective interventions. An inflection in 2013 was observed, with the highest APC between 2008 and 2013. However, despite a decrease in the growth curve in the following years, rates were still considered high, demonstrating lack of control of CS. Other American countries also presented an increased incidence (4), whereas other countries (e.g., China) reported a downward trend in the incidence of CS (18).
The spatial analysis highlighted CS as a public health problem in different Brazilian regions. RUAs covering Northeast coastal areas and Rio Grande do Sul, Rio de Janeiro, Mato Grosso do Sul states showed the highest incidence of CS. The central part of Northeast and areas in the Midwest presented RUAs with the lowest incidence rates of CS.
Teixeira et al. (19) suggested that the increased incidence of CS in the Rio Grande do Sul state was associated with increased testing and reporting of the disease, which reflects the implemented national public policies; however, the treatment of sexual partners was still a major healthcare problem. Another study in a municipality in the state of Rio de Janeiro showed that 42.4% of women were diagnosed with syphilis during delivery or curettage. Additionally, 68.6% of women were inadequately treated while 19.1% were not treated; only 12.2% of sexual partners were treated (20).
Cities close to international borders in Mato Grosso do Sul have an increased flow of people, goods, and drug trafficking, favoring the transmission of sexually transmitted infections. Also, the monitoring of indigenous peoples living in border regions is difficult (9). Tiago et al. (21) suggested that the magnitude of syphilis in indigenous peoples of Mato Grosso do Sul state may be hidden due to underreported cases, even with a high incidence rate. High-high patterns observed in coastal regions of the Northeast may be associated with the population context and great availability of healthcare services and maternity hospitals, resulting in increased notifications. In contrast, low-low patterns in the central region of the Northeast may be associated with the expansion of the Family Health Strategy program in recent years, suggesting effective prevention measures during prenatal care (22).
We observed a direct correlation between the incidence of CS and the percentage of individuals with inadequate water supply and sanitation. The North region showed more extensive clusters in areas with high incidence of CS and the percentage of individuals with inadequate water supply and sanitation. Thus, socioeconomic conditions may strongly influence the increase of CS in these regions.
Domingues and Leal (23) suggested that the increased incidence of CS in Brazil was influenced by social vulnerability. Studies also indicated associations between socioeconomic conditions and syphilis in the Northeast region (10, 24), with low purchasing power and poverty associated with increased cases of syphilis during pregnancy. Furthermore, studies carried out in a city in the state of Mato Grosso do Sul (9), in the state of Tocantins (25) and in Pará (26) showed a high incidence rates of syphilis in women with low education. In Pará, clusters for syphilis stand out in regions with a high flow of people and exposed to situations of social vulnerability. In the United States, researchers have identified the greatest increase in sexually transmitted infections, including syphilis, in metropolitan regions with greater population growth and in African-American populations (27). Thus, Brazilian women in poverty have difficulty accessing prenatal care and tests for syphilis (8).
An association was found between CS and the percentage of prenatal care appointments, an important indicator of access to prenatal care. The LISA method observed clusters of homogeneous areas with more pronounced spatial dependence, establishing priority areas. Brazilian regions present disparities in prenatal care, such as the number of appointments and services offered during appointments, especially testing for HIV and syphilis. The North region presented the lowest prenatal care coverage, whereas a high proportion of women from the North and Northeast reported three or few prenatal care appointments (28). Benzaken et al. (29) showed that 13.3% of pregnant women from Porto Velho (North region) did not have any prenatal care appointments, the highest percentage among Brazilian capitals. Moreover, poor areas in the North and Northeast have difficult access and low social conditions, leading to delayed implementation of healthcare programs and insufficient healthcare coverage (30).
RUAs in the South and Southeast regions showed clusters with high incidence of CS and low percentage of live births with 1–3 prenatal care appointments, suggesting increased access to prenatal care in these regions. However, the quality of prenatal care must be studied since clusters with a high incidence of CS were observed. The Moran’s I indicated a direct correlation between these variables, highlighting the importance of improving access and quality of prenatal care to control CS. Although pregnant women in the South region have more access to prenatal care (29), the treatment of pregnant women with syphilis and their partners is still challenging. Thus, cases of CS in this region are probably high due to lack or inadequate treatment (31, 32). Additionally, a study conducted in this same region showed that healthcare professionals presented insufficient knowledge about measures recommended by the Ministry of Health for preventing, treating, and controlling syphilis (33).
Lack of treatment during prenatal care was also observed in other countries. Kilball et al. (34) suggested that inadequate care, testing, and treatment during prenatal care were different between regions of the United States and contributed to increase syphilis cases during pregnancy and CS.
Reduced investments in public health, financial crisis, political instability, and freezing of funds in Brazil may have contributed to the increase in syphilis cases (35). Santos et al. (36) showed that several Brazilian cities lacked rapid tests for syphilis, reducing diagnosis, treatment, and control of syphilis in the population. Furthermore, some Brazilian regions should restructure the laboratory network to perform treponemal and nontreponemal tests (22).
The shortage of penicillin G due to lack of raw material in the world market, mainly in 2015, may have contributed to the increased incidence of CS (37). Also, Brazilian capitals presented a great variation in the availability of penicillin G benzathine in primary health care units (29) and difficulties in administering this medicine (36). Thus, policies should be developed to qualify and encourage healthcare professionals to administer penicillin G benzathine in basic health units, disseminate information about this medicine, and strengthen surveillance systems and healthcare networks in Brazil (33, 38).
Goals are set, worldwide, for dealing with syphilis (39). The Pan American Health Organization strengthens strategies for eliminating CS in countries (40). However, efforts have not been sufficient to control the disease and research addressing the issue needs to be continued. In Brazil, the Stork Network (41), the implementation of rapid tests (42), the compulsory notification of congenital syphilis (43), the agenda of strategic actions to reduction of syphilis (44) and the No Syphilis Project (45) are governmental measures instituted that strengthen the maternal and child area, which contribute in terms of increasing the detection and notification of the disease, but it has also not been sufficient to eliminate congenital syphilis in the country.
This study may have limitations due to the use of secondary data sources from Brazilian information systems and possible underreporting. The variable “pregnant women without prenatal consultation”, extracted according to the SINASC category, did not show statistical significance in the spatialization of data; thus, it was not included in the analysis. This result may have occurred due to the low number of cases or missing data, which we believe would not change the results. Although data regarding cases of CS were available only until 2018 in the SINAN, no major changes occurred in the context of the country. Because this is a study with aggregate data, there is a possibility of ecological fallacy. It is possible to carry out studies using spatial analysis focusing on regions of epidemiological interest, such as the clusters with high-high levels of incidence rate for CS pointed out in this research, with other independent variables to identify the association of new factors in the spatialization of CS.
Our results showed a growing trend of CS in Brazil, indicating that its eradication is still challenging for the country. The spatial analysis identified direct correlations between regions of clusters with high incidence of CS, access to prenatal care (1–3 appointments), and socioeconomic conditions (individuals with inadequate water supply and sanitation). Thus, inequalities in the Brazilian territory may be determinants of the spatial pattern of CS, while socioeconomic conditions and access to prenatal care may influence the incidence of CS in several Brazilian regions.
Therefore, our study may support public health policies to eradicate CS by indicating regions of greatest need for disease control. The importance of investments in socioeconomic policies must also be highlighted to reduce social inequality and improve access to prenatal care, contributing to managing maternal and child health in more susceptible areas.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
JD, CM, and RS contributed to conception and design of the study. JD and CM organized the database. JD, CM, and MF performed the statistical analysis. JD wrote the first draft of the manuscript. JD, CM, YP, MF, and RS wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
Publication fee—Program of Post-Graduation in Public Health of the Federal University of Rio Grande do Norte and Coordination for the Improvement of Higher Education Personnel—Brazil (CAPES) (funding code 001).
Acknowledgments
Graduate Program in Collective Health. Federal University of Rio Grande Do Norte. The authors thank Probatus Academic Services for providing scientific language translation, revision, and editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Keuning MW, Kamp GA, Schonenberg-Meinema D, Dorigo-Zetsma JW, van Zuiden JM, Pajkrt D. Congenita syphilis, the great imitator-cse report and review. Lancet Infect Dis. (2020) 20(7):e173–e9. doi: 10.1016/s1473-3099(20)30268-1
2. Domingues CSB, Duarte G, Passos MRL, Sztajnbok DC, Menezes MLB. Brazilian protocol for sexually transmitted infections 2020: congenital syphilis and child exposed to syphilis. Epidemiol Serv Saúde. (2021) 30(esp1):1–10. doi: 10.1590/s1679-4974202100005.esp1
3. The Lancet. Congenital syphilis in the USA. Lancet. (2018) 392(10154):1168. doi: 10.1016/s0140-6736(18)32360-2
4. Korenromp EL, Rowley J, Alonso M, Mello MB, Wijesooriya NS, Mahiané SG, et al. Global burden of evolution and adverse outcomes associated with childbirth—estimates from 2016 to 2012 progress. PLoS One. (2019) 14(2):e0211720. doi: 10.1371/journal.pone.0211720
5. Ministério da Saúde. Boletim Epidemiológico de Sífilis (2021). Available at: http://www.gov.br/aids/pt-br/centrais-de-conteudo/boletins-epidemiologicos/2021/sifilis/boletim_sifilis_2021_internet.pdf/view (Accessed November 9, 2022).
6. World Health Organization. Global guindance on criteria processes for validation: elimination of mother-to-child transmission of HIV and syphilis (2019). Available at: https://apps.who.int/iris/bitstream/handle/10665/259517/9789241513272-eng.pdf;jsession-id=BCF6FC0F816A197DE0D7AF90EBF8FF72?se-quence=1 (Accessed August 09, 2022).
7. Chiaravalloti-Neto F. O geoprocessamento e saúde pública. Arq Ciênc Saúde. (2016) 23(4):1–2. doi: 10.17696/2318-3691.23.4.2016.661
8. Freitas C, Forte FDS, Galvao MHR, Coelho AA, Roncalli AG, Dias SMF. Inequalities in access to HIV and syphilis tests in prenatal care in Brazil. Cad Saude Publica. (2019) 35(6):e00170918. doi: 10.1590/0102-311x00170918
9. Barbosa MS, Lima LA, Ribeiro SM, Croda J, Queiroz JHFS, Ortolani LG. Epidemiological study in Brazilian women highlights that syphilis remains a public health problem. Rev Inst Med Trop. (2021) 63:e4. doi: 10.1590/s1678-9946202163004
10. Macedo VC, Lira PIC, Frias PG, Romaguera LMD, Caires SFF, Ximenes RAA. Risk factors for syphilis in women: case-control study. Rev Saude Publica. (2017) 51:78. doi: 10.11606/S1518-8787.2017051007066
11. Instituto Brasileiro de Geografia e Estatística. Projeção da população do Brasil e das Unidades da Federação (2022). Available at: https://www.ibge.gov.br/apps/populacao/projecao/index.html?utm_source=portal&utm_medium=popclock&utm_campaign=novo_popclock (Accessed July 7, 2022).
12. Instituto Brasileiro de Geografia e Estatística. Divisão urbano regional (2013). Available at: https://www.ibge.gov.br/geociencias/organizacao-do-territorio/divisao-regional/15777-divisao-urbano-regional.html?=&t=downloads (Accessed August 5, 2022).
13. Ministério da Saúde. Departamento Prevenção, Vigilância e Controle das Infecções Sexualmente Transmissíveis do HIV/AIDS. Nota Informativa N° 2-SEI-2017-DIAHV/SVS/MS. Altera os critérios de definição de casos para notificação de sífilis adquirida, sífilis em gestantes e sífilis congênita. Available at: https://portalsinan.saude.gov.br/images/documentos/Agravos/Sifilis-Ges/Nota_Informativa_Sifilis.pdf (Accessed February 09, 2023).
14. Rossoni HAV, Faria MTS, Silva AC, Heller L. Socioeconomic aspects and municipal human development determinants in the absence of providers of sanitary sewage services in Brazil. Eng Sanit Ambient. (2020) 25(2):393–402. doi: 10.1590/S1413-41522020183887
15. Nacional Cancer Institute. Joinpoint trend analysis software (2021). Available at: https://surveillance.cancer.gov/joinpoint/ (Accessed July 7, 2022).
16. Câmara G, Carvalho MS, Cruz OG, Correa V. Análise espacial de áreas (2004). Available at: http://www.dpi.inpe.br/gilberto/livro/analise/cap5-areas.pdf (Accessed January 30, 2022).
17. Monteiro LD, Martins-Melo FR, Brito AL, Alencar CH, Heukelbach J. Spatial patterns of leprosy in a hyperendemic state in northern Brazil, 2001-2012. Rev Saude Publica. (2015) 49:84. doi: 10.1590/s0034-8910.2015049005866
18. Tao Y, Chen MY, Tucker JD, Ong JJ, Tang W, Wong NS, et al. A nationwide spatiotemporal analysis of syphilis over 21 years and implications for prevention and control in China. Clin Infect Dis. (2020) 70(1):136–9. doi: 10.1093/cid/ciz331
19. Teixeira LO, Belarmino V, Goncalves CV, Mendoza-Sassi RA. Temporal trend and spatial distribution of congenital syphilis in the state of Rio Grande do Sul between 2001 and 2012. Cien Saude Colet. (2018) 23(8):2587–97. doi: 10.1590/1413-81232018238.25422016
20. Heringer A, Kawa H, Fonseca SC, Brignol SMS, Zarpellon LA, Reis AC. Inequalities in congenital syphilis trends in the city of Niteroi, Brazil, 2007-2016. Rev Panam Salud Publica. (2020) 44:e3. doi: 10.26633/RPSP.2020.8
21. Tiago ZDS, Picoli RP, Graeff SV, Cunha RVD, Arantes R. Underreporting of gestational, congenital and acquired syphilis among indigenous peoples in Mato Grosso do Sul State, Brazil, 2011-2014. Epidemiol Serv Saude. (2017) 26(3):503–12. doi: 10.5123/S1679-49742017000300008
22. Raimundo DML, Sousa GJB, da Silva ABP, Almino R, Prado N, da Silva RAR. Spatial analysis of congenital syphilis in the state of Rio Grande do Norte, between 2008 and 2018. Rev Escola Enfermagem USP. (2021) 55:e20200578. doi: 10.1590/1980-220X-REEUSP-2020-0578
23. Domingues RM, Leal MC. Incidence of congenital syphilis and factors associated with vertical transmission: data from the birth in Brazil study. Cad Saude Publica. (2016) 32(6):1–12. doi: 10.1590/0102-311X00082415
24. Conceição HN, Câmara JT, Pereira BM. Análise epidemiológica e espacial dos casos de sífilis gestacional e congênita. Saúde Debate. (2019) 43(123):1145–58. doi: 10.1590/0103-1104201912313
25. Silva M, Barreto FR, Costa M, Carvalho MSI, Teixeira MDG. Congenital syphilis distribution in the state of Tocantins, Brazil, 2007-2015. Epidemiol Serv Saude. (2020) 29(2):e2018477. doi: 10.5123/s1679-49742020000200017
26. Costa BA, Santos DF, Hayase KA, Santos MM, Naiff GR, Botelho EP. Sífilis congênita em região da amazônia brasileira: análise temporal e espacial. Rev Eletr Enferm. (2020) 22:62349. doi: 10.5216/ree.v22.62349
27. Patterson-Lomba O, Goldstein E, Gomez-Lievano A, Castillo-Chavez C, Towers S. Per capita incidence of sexually transmitted infections increases systematically with urban population size: a cross-sectional study. Sex Transm Infect. (2015) 91(8):610–4. doi: 10.1136/sextrans-2014-051932
28. Nunes AD, Amador AE, Dantas AP, Azevedo UN, Barbosa IR. Acesso à assistência pré-natal no Brasil: análise dos dados da Pesquisa Nacional de Saúde. Rev Bras Promoç Saúde. (2017) 30(3):1–10. doi: 10.5020/18061230.2017.6158
29. Benzaken AS, Pereira GFM, Cunha A, Souza FMA, Saraceni V. Adequacy of prenatal care, diagnosis and treatment of syphilis in pregnancy: a study with open data from Brazilian state capitals. Cad Saude Publica. (2019) 36(1):e00057219. doi: 10.1590/0102-311X00057219
30. Chrestani M, Santos I, Cesar J, Winckler L, Gonçalves T, Neumann N. Health care during pregnancy and childbirth: results of two cross-sectional surveys in poor areas of North and Northeast Brazil. Cad Saúde Pública. (2008) 24(7):1609–18. doi: 10.1590/s0102-311x2008000700016
31. Padilha Y, Caporal AS. Incidência de casos de sífilis congênita e análise do perfil epidemiológico. FAG J Health. (2020) 2(1):1–11. doi: 10.35984/fjh.v2i1.140
32. Roehrs MP, Silveira SK, Gonçalves HHR, Sguario RM. Sífilis materna no Sul do Brasil: epidemiologia e estratégias para melhorar. Femina. (2020) 48:753–9.
33. Lazarini FM, Barbosa DA. Educational intervention in primary care for the prevention of congenital syphilis. Rev Lat Am Enfermagem. (2017) 30(25):e2845. doi: 10.1590/1518-8345.1612.2845
34. Kimball A, Torrone E, Miele K, Bachmann L, Thorpe P, Weinstock H, et al. Missed opportunities for prevention of congenital syphilis - United States, 2018. Morb Mortal Wkly Rep. (2020) 69(22):661–5. doi: 10.15585/mmwr.mm6922a1
35. Melo EA, de Mendonça MH, Teixeira M. A crise econômica e a Atenção Primária à Saúde no SUS da cidade do Rio de Janeiro, Brasil. Cien Saude Colet. (2019) 24(12):4593–8. doi: 10.1590/1413-812320182412.25432019
36. Santos MMD, Rosendo T, Lopes AKB, Roncalli AG, Lima KC. Weaknesses in primary health care favor the growth of acquired syphilis. PLoS Negl Trop Dis. (2021) 15(2):e0009085. doi: 10.1371/journal.pntd.0009085
37. Coelho J, Dantas F, Pena L, Barbosa J, Costa C, Ferreira L, et al. Syphilis: an epidemiological overview of Brazil and the municipality of volta redonda/RJ. Braz J Heal Rev. (2018) 1(1):128–47.
38. Galvao TF, Silva MT, Serruya SJ, Newman LM, Klausner JD, Pereira MG, et al. Safety of benzathine penicillin for preventing congenital syphilis: a systematic review. PLoS One. (2013) 8(2):e56463. doi: 10.1371/journal.pone.0056463
39. World Health Organization. Estratégia global do setor de saúde sobre infecções sexualmente transmissíveis, 2016-2021 (2016). Available at: https://www.who.int/publications/i/item/WHO-RHR-16.09 (Accessed October 13, 2022).
40. Pan American Health Organization. EMTCT Plus. Framework for elimination of mother-to-child transmission of HIV, Syphilis, Hepatitis B, and Chagas (2017). Available at: https://iris.paho.org/handle/10665.2/34306 (Accessed October 13, 2022).
41. Nunes PS, Guimarães RA, Rosado LE, Marinho TA, Aquino EC, Turchi MD. Temporal trend and spatial distribution of syphilis in pregnancy and congenital syphilis in goiás, Brazil, 2007-2017: an ecological study. Epidemiol Serv Saúde. (2021) 30(1):e2019371. doi: 10.1590/S1679-49742021000100002
42. Saraceni V, Pereira GFM, Silveira MF, Araujo MAL, Miranda AE. Epidemiological surveillance of vertical transmission of syphilis: data from six federal units in Brazil. Rev Panam Salud Publica. (2017) 8(41):e44. doi: 10.26633/RPSP.2017.44
43. Ministério da Saúde. Diário Oficial da União, 24 dez 1986, Seção 1, p. 19827. Portaria 542/1986. Available at: http://pesquisa.bvsalud.org/ses/resource/pt/crt-3619 (Accessed October 13, 2022).
44. Ministério da Saúde. Agenda Estratégica para Redução da Sífilis no Brasil 2020-2021 (2021). Available at: https://bvsms.saude.gov.br/bvs/publicacoes/agenda_reducao_sifilis_2020_2021.pdf (Accessed October 13, 20221).
Keywords: Treponema Pallidum, prenatal care, infectious diseases, spatial analysis, space time clustering
Citation: Dantas JdC, Marinho CdSR, Pinheiro YT, Ferreira MAF and da Silva RAR (2023) Temporal trend and factors associated with spatial distribution of congenital syphilis in Brazil: An ecological study. Front. Pediatr. 11:1109271. doi: 10.3389/fped.2023.1109271
Received: 28 November 2022; Accepted: 3 March 2023;
Published: 22 March 2023.
Edited by:
Maurizio Aricò, Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari, ItalyReviewed by:
Ana Karinne Dantas De Oliveira, University of Fortaleza, BrazilArnaldo Prata-Barbosa, D'Or Institute for Research and Education (IDOR), Brazil
© 2023 Dantas, Marinho, Pinheiro, Ferreira and da Silva. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Janmilli da Costa Dantas amFubWlsbGlAeWFob28uY29tLmJy
Specialty Section: This article was submitted to Pediatric Infectious Diseases, a section of the journal Frontiers in Pediatrics