 Jakub Zieg
Jakub Zieg Terezia Tavačová2
Terezia Tavačová2 Peter Kubuš
Peter Kubuš- 1Department of Pediatrics, Second Faculty of Medicine, Charles University and Motol University Hospital, Prague, Czechia
- 2Children's Heart Centre, 2nd Faculty of Medicine, Charles University and Motol University Hospital, Prague, Czechia
- 3Department of Biology and Medical Genetics, University Hospital Motol, Second Medical Faculty, Charles University, Prague, Czechia
Salt-losing tubulopathies are well-recognised diseases predisposing to metabolic disturbances in affected patients. One of the most severe complications can be life-threatening arrhythmias causing sudden cardiac arrest. We present here the first case of a pediatric patient with Gitelman syndrome associated sudden cardiac arrest without precipitating event. A 10-year-old boy collapsed due to ventricular fibrillation in the Prague tram. Lay cardiopulmonary resuscitation was initiated and external defibrillation restored sinus rhythm within minutes. Initial laboratory examination revealed severe hypokalemia requiring large amounts of electrolyte supplementation. Genetic testing focused to tubulopathies was performed and the diagnosis of Gitelman syndrome was made following the identification of two pathogenic variants in SLC12A3 gene (c.2633 + 1G>A and c.2221G>A). Implantable cardioverter-defibrillator was implanted to prevent sudden cardiac death. The patient was in a good clinical condition with satisfactory electrolyte serum levels at the last follow-up. Causes of electrolyte abnormalities in children should be identified early to prevent the development of rare but potentially fatal complications.
Background
Gitelman syndrome (GS) is an autosomal recessive salt-losing tubulopathy characterized by hypokalemic metabolic alkalosis, hypomagnesemia, hypocalciuria and secondary hyperaldosteronism. This disease was first described in three individuals (two sisters and one unrelated patient) by Gitelman, Graham and Welt in 1966 (1). GS represents the most common hereditary tubulopathy with prevalence estimated at 25 per million (2). GS is caused by homozygous or compound heterozygous mutations in the SLC12A3 gene, which encodes the thiazide-sensitive sodium-chloride cotransporter (NCC), that is expressed in the apical membrane of cells in the distal convoluted tubule (3). GS metabolic abnormalities mimic treatment with thiazide diuretics, which act by blocking this tubular channel. The first symptoms usually present in children older than 6 years or in adolescence or adulthood, but cases of neonatal presentation have also been reported (4). The most common clinical manifestations include salt craving, muscle weakness, cramps, fatigue, dizziness, nocturia, polydipsia, paraesthesia, numbness, palpitations and hypotension (5). Genetic testing should be offered to all affected individuals with a clinical suspicion of GS. The mainstay of therapy is supplementation of electrolytes, some cases require further medication to maintain satisfactory electrolyte serum concentration. Although electrolyte abnormalities in children with salt-losing tubulopathies may be asymptomatic, severe life threatening cardiac arrhythmias have been reported in children with Bartter syndrome, a hereditary tubulopathy affecting the transport mechanisms in the loop of Henle with phenotype that can in certain forms resemble GS (6). Interestingly, prolonged corrected QT interval associated with the risk of fatal arrhythmias was found in a cohort patients with GS (7). We present here a case of ventricular fibrillation causing sudden cardiac arrest (SCA) in a child with GS.
Case description
10-year-old boy (refugee from Ukraine) collapsed in the tram in the city of Prague. Lay cardiopulmonary resuscitation was initiated with subsequent arrival of healthcare professionals. Sinus rhythm was restored within a few minutes by external defibrillation of the documented ventricular fibrillation (Figure 1). The patient was intubated, sedated and transported to the pediatric anesthesiologic ward, with no major physical findings except for pathologic lung auscultation—crackling and wheezing over the right lung caused by aspiration pneumonia, managed by parenteral antibiotic therapy (amoxycilin/clavulanate). On admission, the patient was stable under sedation, intubated with no reaction to examination (Glasgow coma scale 3). Therapeutic hypothermia was slowly withdrawn after 24 h. Electrocardiogram (ECG) showed normal sinus rhythm with age-appropriate heart rate and normal repolarization, with QTc of 422 ms (including normal QTc during 24 h ECG monitoring) and normal echocardiography findings. The initial laboratory results were as follows: serum sodium 133 mmol/L, potassium 2.5 mmol/L, chloride 96 mmol/L, calcium 2.25 mmol/L, magnesium 0.78 mmol/L, urea 7.4 mmol/L, creatinine 66 µmol/L, bicarbonate 22.9 mmol/L. Parenteral electrolyte supplementation was started, high potassium chloride (KCl) supplementation 8–10 mmol/kg/day was required to maintain potassium in the low normal range, magnesium was supplemented later when serum levels were decreased. The patient was extubated on the second day with normal neurologic examination and transported to Children's Heart Centre on the 4th day of hospitalization. Oral celecoxib (3.5 mg/kg/day) was started after 7 days to reduce the extensive oral and parenteral KCl supplementation. Single-chamber (transvenous lead) implantable cardioverter-defibrillator (ICD) was implanted for secondary prevention of sudden cardiac death (Figure 2). The patient was discharged from the hospital after 28 days. He has been followed up regularly by a pediatric nephrologist and cardiologist, with satisfactory potassium and magnesium serum levels in the long term, >3 mmol/L and >0.6 mmol/L, respectively. Since the device implantation, the remote ICD monitoring recorded several episodes of asymptomatic non-sustained polymorphic ventricular tachycardia, with no appropriate therapies needed so far. Molecular genetic examination performed by next-generation sequencing (Clinical Exome Solution v3 by Sophia Genetics, Switzerland) revealed 2 pathogenic (class 5 according to ACMG/AMP guidelines) variants in SLC12A3 gene (NM_001126108) c.2633 + 1G>A and c.2221G>A (p.Gly741Arg) confirming the diagnosis of GS. Subsequent segregation analysis revealed 2 pathogenic (class 5 according to ACMG/AMP guidelines) variants in SLC12A3 gene (NM_001126108) paternally inherited c.2633 + 1G>A and maternally inherited c.2221G>A (p.Gly741Arg).
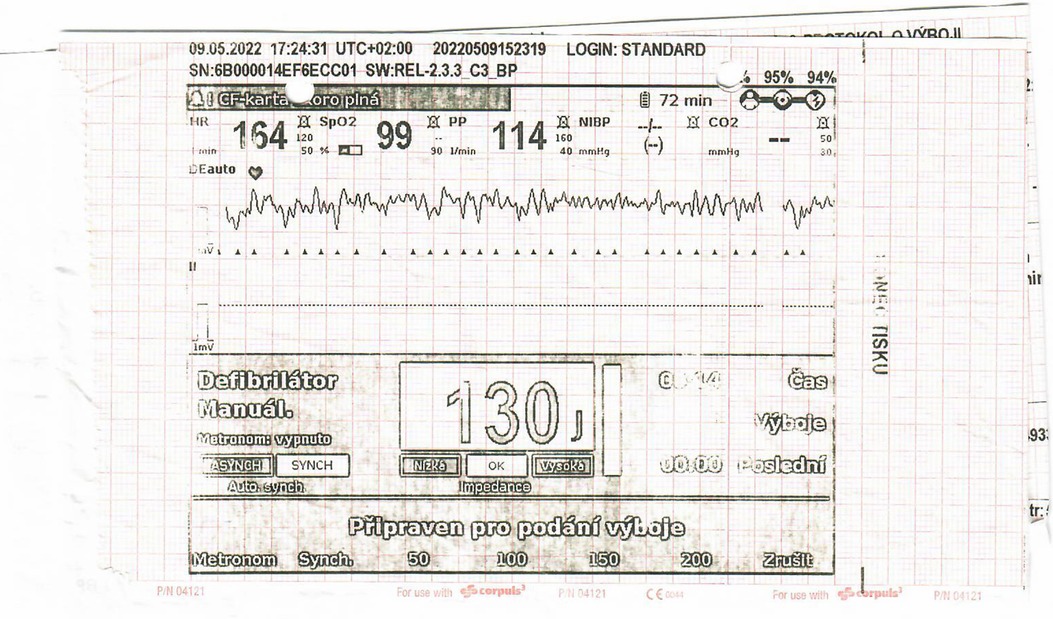
Figure 1. ECG during sudden cardiac arrest with documented ventricular fibrillation.
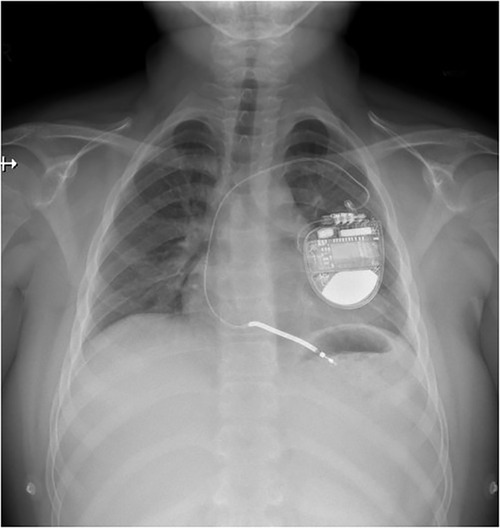
Figure 2. Transvenous implantable cardioverter-defibrillator implanted in patient with GS.
Discussion
Cardiac arrhythmias and SCA are rare and severe complications of salt-losing tubulopathies. Electrolyte depletion and/or QTc prolongation are presumed factors involved in the pathogenesis of these heart conduction disorders (8). Although these patients are usually adapted to chronic hypokalemia, certain clinical conditions such as vomiting and diarrhea may further lower serum potassium concentration and induce arrhythmia (6). Interestingly, our patient did not have any clinical signs of viral illness or gastrointestinal symptoms at the time of cardiac event. Although literature on cardiac evaluation of GS patients is scarce, a significant proportion of GS patients have been found to have long QTc, therefore, thorough cardiac work up is warranted in these individuals (7, 9). Standard management of GS patients consists of electrolyte supplementation to achieve targets for potassium 3 mmol/L and for magnesium 0.6 mmol/L. This therapy may be complicated by mainly gastrointestinal side effects, therefore, in some patients the accepted electrolyte concentration may be lower. Nonsteroidal anti-inflammatory drugs, potassium sparing diuretics and inhibitors of renin-angiotensin-aldosteron axis (RAAA) may be considered in children with persistent hypokalemia despite high doses of supplementation, unacceptable side effects and good adherence to therapy. Hypomagnesemia may have characteristic ECG pattern, especially prologantion of QTc interval associated with risk of severe ventricular arrhythmia (polymorphic ventricular tachycardia/torsades de pointes, ventricular fibrillation) (10). Flat or absent T-waves, ST segment depression and U waves may be identified on ECG in patients with moderately to severely decreased potassium serum concentration (11). In the reported patient, no such repolarization changes were observed, which suggests highly variable effect of electrolyte imbalance on ECG findings in different individuals. Hypokalemia causes resting membrane hyperpolarization, Na+/K+ ATPase inhibition, Na+ and Ca2+ intracellular accumulation with reduced repolarization reserve, that predisposes to early- and delayed-afterdepolarization mediated arrhythmias (12). Potassium serum levels may decrease in conditions with volume depletion, which activates RAAA (13). Therefore, in case of dehydration, children with salt-losing nephropathies should be early referred and treated with isotonic saline and increased electrolyte (potassium with or without concurrent magnesium) supplementation. Interestingly, magnesium influences the function of Na+/K+ATPase and it's depletion leads to hypokalemia. Cortessi et al. performed survey research among European pediatric kidney disease specialists treating Bartter syndrome and GS. 249 patients were included in this study. They aimed to study the frequency and character of cardiac arrhythmias and rhabdomyolysis in children with salt-losing tubulopathies. Seven children (2.8%) with acute cardiac complications were found, only one of these individuals was diagnosed with GS. Three children including the child with GS suffered from diarrhea or vomiting as a supposed precipitating factor (14). The indication for ICD implantation was thoroughly discussed—the combination of previous nearly fatal arrhythmia (i.e., secondary prevention) and (at least) potential for arrhythmia recurrence in case of suboptimal electrolyte management (which makes the idea of “reversible cause” of sudden cardiac death at least discutable), led us to the decision to implant the device. Indication for ICD in children is less clearly established and, in our Centre, at present, we prefer transvenous ICD in secondary prevention. Moreover, recurrent findings of non-sustained polymorphic ventricular tachycardia after ICD implantation support our decision to implant.
Although there is a published case report of adult with Gitelman syndrome presenting with cardiac arrest (15), to our knowledge, we present the first case of SCA in a child with GS without any precipitating event. Appropriate assessment of serum and urinary concentrations of electrolytes including magnesium is indicated in patients with VA. Salt-losing nephropathies represent one of the most common ethiology of hypokalemia and hypomagnesemia. The risk of arrhythmias in these children may be increased in certain clinical situations (e.g., dehydration, drugs). Clinicians should be aware that rare life-threatening cardiac events can occur in these individuals.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author contributions
JZ and TT wrote the first draft of the manuscript. MB and PP contributed to the critical revision of the manuscript. FF and PK reviewed and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the project (Ministry of Health, Czech Republic) for conceptual development of research organization 00064203 (University Hospital Motol, Prague, Czech Republic).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ECG, electrocardiogram; GS, Gitelman syndrome; ICD, implantable cardioverter-defibrillator; RAAA, renin-angiotensin-aldosteron axis; SCA, sudden cardiac arrest; VA, ventricular arrhythmia.
References
1. Gitelman HJ, Graham JB, Welt LG. A new familial disorder characterized by hypokalemia and hypomagnesemia. Trans Assoc Am Physicians. (1966) 79:221–35.5929460
2. Knoers NV, Levtchenko EN. Gitelman syndrome. Orphanet J Rare Dis (2008) 3:22. doi: 10.1186/1750-1172-3-22
3. Simon DB, Nelson-Williams C, Bia MJ, Ellison D, Karet FE, Molina AM, et al. Gitelman’s variant of bartter’s syndrome, inherited hypokalaemic alkalosis, is caused by mutations in the thiazide-sensitive na-cl cotransporter. Nat Genet. (1996) 12(1):24–30. doi: 10.1038/ng0196-24
4. Chen H, Ma R, Du H, Liu J, Jin L. Early onset children’s Gitelman syndrome with severe hypokalaemia: a case report. BMC Pediatr. (2020) 20(1):366. doi: 10.1186/s12887-020-02265-9
5. Blanchard A, Bockenhauer D, Bolignano D, Calo LA, Cosyns E, Devuyst O, et al. Gitelman syndrome: consensus and guidance from a kidney disease: improving global outcomes (kdigo) controversies conference. Kidney Int. (2017) 91(1):24–33. doi: 10.1016/j.kint.2016.09.046
6. Cortesi C, Lava SA, Bettinelli A, Tammaro F, Giannini O, Caiata-Zufferey M, et al. Cardiac arrhythmias and rhabdomyolysis in bartter-gitelman patients. Pediatr Nephrol. (2010) 25(10):2005–8. doi: 10.1007/s00467-010-1580-4
7. Bettinelli A, Tosetto C, Colussi G, Tommasini G, Edefonti A, Bianchetti MG. Electrocardiogram with prolonged qt interval in gitelman disease. Kidney Int. (2002) 62(2):580–4. doi: 10.1046/j.1523-1755.2002.00467.x
8. Scognamiglio R, Negut C, Calo LA. Aborted sudden cardiac death in two patients with bartter’s/Gitelman’s syndromes. Clin Nephrol. (2007) 67(3):193–7. doi: 10.5414/cnp67193
9. Pachulski RT, Lopez F, Sharaf R. Gitelman’s not-so-benign syndrome. N Engl J Med. (2005) 353(8):850–1. doi: 10.1056/NEJMc051040
10. Yang Y, Chen C, Duan P, Thapaliya S, Gao L, Dong Y, et al. The ecg characteristics of patients with isolated hypomagnesemia. Front Physiol. (2020) 11:617374. doi: 10.3389/fphys.2020.617374
11. Daly K, Farrington E. Hypokalemia and hyperkalemia in infants and children: pathophysiology and treatment. J Pediatr Health Care. (2013) 27(6):486–96. doi: 10.1016/j.pedhc.2013.08.003
12. Weiss JN, Qu Z, Shivkumar K. Electrophysiology of hypokalemia and hyperkalemia. Circ Arrhythm Electrophysiol. (2017) 10(3). doi: 10.1161/CIRCEP.116.004667
13. Zacchia M, Abategiovanni ML, Stratigis S, Capasso G. Potassium: from physiology to clinical implications. Kidney Dis (Basel). (2016) 2(2):72–9. doi: 10.1159/000446268
14. Cortesi C, Bettinelli A, Emma F, Fischbach M, Bertolani P, Bianchetti MG. Severe syncope and sudden death in children with inborn salt-losing hypokalaemic tubulopathies. Nephrol Dial Transplant. (2005) 20(9):1981–3. doi: 10.1093/ndt/gfh893
Keywords: arrhythmia, Gitelman syndrome, hypokalemia, hypomagnesemia, sudden cardiac arrest
Citation: Zieg J, Tavačová T, Balaščáková M, Peldová P, Fencl F and Kubuš P (2023) Sudden cardiac arrest in a child with Gitelman syndrome: a case report and literature review. Front. Pediatr. 11:1188098. doi: 10.3389/fped.2023.1188098
Received: 16 March 2023; Accepted: 23 May 2023;
Published: 7 June 2023.
Edited by:
Craig Bradford Langman, Northwestern University, United StatesReviewed by:
Takanari Ikeyama, Aichi Child Health and Medical General Center, JapanLucy Barone, Policlinico Tor Vergata, Italy
© 2023 Zieg, Tavačová, Balaščáková, Peldová, Fencl and Kubuš. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jakub Zieg amFrdWJ6aWVnQGhvdG1haWwuY29t
†ORCID Jakub Zieg orcid.org/0000-0001-6077-9536