 Tirualem Zeleke Yehuala
Tirualem Zeleke Yehuala Bezawit Melak Fente
Bezawit Melak Fente Sisay Maru Wubante
Sisay Maru Wubante Nebiyu Mekonnen Derseh
Nebiyu Mekonnen Derseh- 1Department Health Informatics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 2Department of General Midwifery, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 3Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Background: The primary cause of death for children under the age of five is acute respiratory infections (ARI). Early predicting acute respiratory tract infections (ARI) and identifying their predictors using supervised machine learning algorithms is the most effective way to save the lives of millions of children. Hence, this study aimed to predict acute respiratory tract infections (ARI) and identify their determinants using the current state-of-the-art machine learning models.
Methods: We used the most recent demographic and health survey (DHS) dataset from 36 Sub-Saharan African countries collected between 2005 and 2022. Python software was used for data processing and machine learning model building. We employed five machine learning algorithms, such as Random Forest, Decision Tree (DT), XGBoost, Logistic Regression (LR), and Naive Bayes, to analyze risk factors associated with ARI and predict ARI in children. We evaluated the predictive models’ performance using performance assessment criteria such as accuracy, precision, recall, and the AUC curve.
Result: In this study, 75,827 children under five were used in the final analysis. Among the proposed machine learning models, random forest performed best overall in the proposed classifier, with an accuracy of 96.40%, precision of 87.9%, F-measure of 82.8%, ROC curve of 94%, and recall of 78%. Naïve Bayes accuracy has also achieved the least classification with accuracy (87.53%), precision (67%), F-score (48%), ROC curve (82%), and recall (53%). The most significant determinants of preventing acute respiratory tract infection among under five children were having been breastfed, having ever been vaccinated, having media exposure, having no diarrhea in the last two weeks, and giving birth in a health facility. These were associated positively with the outcome variable.
Conclusion: According to this study, children who didn't take vaccinations had weakened immune systems and were highly affected by ARIs in Sub-Saharan Africa. The random forest machine learning model provides greater predictive power for estimating acute respiratory infections and identifying risk factors. This leads to a recommendation for policy direction to reduce infant mortality in Sub-Saharan Africa.
Introduction
Children's immune systems are particularly vulnerable to infection (1). In developing nations, malnutrition, diarrheal diseases, and acute respiratory infections (ARI) are the main causes of illness and mortality among children (2). One of the most prevalent diseases in children is acute respiratory tract infection, which nearly always causes serious health issues and even leads to death in children under five (1). The most common acute respiratory infections are influenza, common cold, sinusitis, tonsillitis, and laryngitis. They are caused by viruses. It is the greatest global public health burden, and developing nations particularly those in Sub-Saharan Africa (SSA), where Ethiopia is located continue to bear an excessive burden of this infection (2). Approximately 20% of the deaths of children globally are caused by acute respiratory infections (ARI) (3). With 80% occurring in Sub-Saharan Africa and southern Asia in 2021 (4). In Sub-Saharan Africa, the highest child mortality rate was 27 deaths per 1,000 live births. Children born in Sub-Saharan Africa are 11 times more likely to die in the first month of life than those born in Australia and New Zealand (5). Similar to this, numerous poor wealth statuses have been attributed to acute tract infections in Sub-Saharan African countries (2, 6, 7). ARI diseases rank fourth among childhood illnesses with a higher rate of morbidity, according to WHO data from 2019. ARI illnesses rank higher among communicable diseases that cause death than other comorbidities when compared with malaria (8). Some previous studies found wealth status, breastfed, place of delivery, birth size, media exposure, diarrhea, stunting, and wasting were the most significant predictors of ARI (3, 4). Despite the fact that malnutrition and an appropriate low birth weight are linked to a very high risk of dying from ARI in developing countries. Even though various local studies on the prevalence and factors associated with ARIs among children under the age of five have been conducted in Sub-Saharan African countries. Used a variety of models and methodologies using conventional methods, including retrospective analysis, inferential statistics, survival analysis, regression models, mapping and spatial analysis, multilevel analysis, and multivariate decomposition (4–7). Recent research suggested machine learning, data mining, and deep learning (DL) have the potential to speed up this progress. These techniques have shown significant performance in a variety of fields, including the fields of public health and medicine. Nevertheless, there is not enough proof to support the prediction of ARIs and the identification of determinants using machine learning techniques, and no prior research has attempted to do so in Sub-Saharan African countries. A predictive model enables real-time children's’ ARI of risk stratification, which guides primary attention to care for the children's good health outcomes. The decision-making process is automated using machine learning algorithms. When these methods are utilized in the healthcare sector, patients’ health outcomes are enhanced and healthcare costs are decreased. We create a novel method for predicting them using machine learning algorithms that determine the child's ARI status.
This study made use of data from the Demographic and Health Surveys (DHS), which were carried out using nationally representative samples in 36 Sub-Saharan African nations between 2005 and 2019.Hence, this study aimed to predict ARI status and identify its predictors using the current state-of-the-art machine learning models.
In conclusion, the two primary questions this study seeks to address are as follows:
RQ1
Which determinants are the most significant for acute respiratory infection (ARI) status?
RQ2
Which machine learning models help to effectively predict acute respiratory infection (ARI) status?
Methods
Study setting
This study was conducted in Sub-Saharan African countries using the most recent Demographic and Health Survey (DHS) dataset from 36 Sub-Saharan African countries. Geographically, east Africa is a sub-region of Africa that includes 54 internationally known countries, among which Angola, Burkina Faso, Benin, Burundi, Dr Congo, Congo, Cote devoirs, Cameron, Ethiopia, Gabon, Ghana, Gambia, Guinea, Kenya, Comoros, Liberia, Lesotho, Madagascar, Mali, Malawi, Mozambique, Nigeria, Niger, Namibia, Rwanda, Sera Leone, Senegal, Sao Tome, Swaziland, Chad, Togo, Tanzania, Uganda, South Africa, Zambia, and Zimbabwe conducted the study.
Data source
This study used measured DHS program data, accessed online, comprising the Kids Record dataset (KR file). Among 54 Sub-Saharan African countries, 36 DHS datasets were eligible for analysis since the rest of the Sub-Saharan African countries had no recorded acute respiratory infection, and we did not get the DHS dataset in the years from 2005 to 2022 that were included in this study.
Sample size determination and sampling technique
The DHSs were a nationally representative survey that collected data on basic health indicators like mortality, morbidity, family planning service utilization, fertility, and maternal and child health-related indicators (8). This study used a weighted sample of 75,827 children aged under five across 36 Sub-Saharan African countries using the recent DHS dataset. For this study, we used the Kids Record dataset (KRFile). A two-stage stratified cluster sampling technique was used to select study participants. In the first step, a stratified sample of enumeration areas (EAs) was selected at random; in the second stage, households were selected using systematic random sampling in the selected EAs. In each selected household, mother or father were interviewed with an individual questionnaire.
Population, and eligibility criteria
In this study, only children under age five who had symptoms of acute respiratory infection (ARI) in the two weeks before the survey in Sub-Saharan African during the survey period who were in the selected enumeration areas at the time of DHS data collection were the study populations and included in this study.
Study design and study period
This study adopted a design science approach for analysis and building a model of the DHS dataset, which was conducted from 2005 to 2022. The design science approach focuses on solving practical problems through the creation and evaluation of innovative artifacts. Through this approach, the study contributes to both theoretical and practical aspects by offering a novel solution to a specific problem (9). Finally, we develop a predictive model that predicts the determinants or factors of acute respiratory infection among under-five children.
Study variables
The outcome variables
Acute respiratory tract infection is defined as children having a history of coughing within two weeks preceding the survey. Children under age five who had symptoms of acute respiratory infection (ARI) in the two weeks before the survey. Then, the outcome variable was categorized as yes or no (acute respiratory infection). The first category [children under age five who had symptoms of acute respiratory infection (ARI) in the two weeks] was given a “1” value, and the second category (children who had no symptoms of acute respiratory infection) was given a value of “0,” respectively. This classification and analysis was conducted according to the guide to the DHS (10, 11).
Independent variables
The features (independent variables) used in this study include individual, household, community, and health service factors. Incorporate the mother's age (15–24, 25–34, and 35–49), birth size (small, normal, large), stunting (normal or severe), underweight (normal or severe), media exposure (yes or no), breastfeeding (ever or never), diarrhea (yes or no), and the child's vaccination history (yes or no). And Sub-Saharan countries (central, east). The health service factors determine the mode of delivery of services (health facility, home).
Data analysis procedure
Machine learning algorithms were used to come up with objective predictions about acute respiratory tract infection and to identify the factors that influence respiratory tract infection. Data processing is a machine learning technique that transforms raw data into an understandable format (12). Data processing and analysis will be performed using Python software and some basic packages like Panda, Scikit-Learn, Imblearn, Numpy, and Seaborne utilized for gathering data, preparing data, discretizing data, transforming data, and choosing, training, and evaluating models. Finally, we develop a predictive model that predicts both the acute respiratory tract infection and its associated determinants (Figure 1).
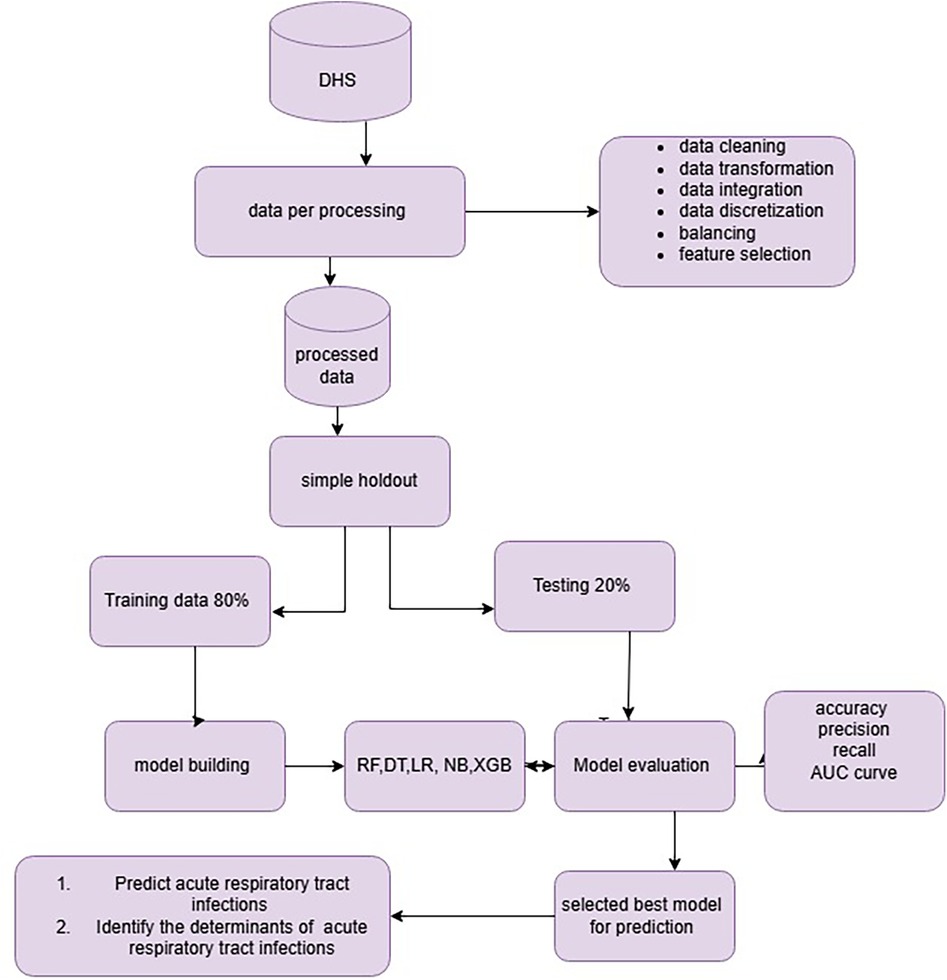
Figure 1. Overall data preparation and analysis process for predicting acute respirator trace infection.
Data preprocessing
We employed data preprocessing to remove incomplete values, noisy data, outliers, and incompatible data since it is done in its raw form. Major data Pre-processing, such as data cleaning, data integration, transforming, and discretizing data, is important (13). In this study, we utilized major t data preprocessing.
Data cleaning
Data cleaning is the most important process for data analysis to ensure the dataset removes incorrect or erroneous data (14). We employed data cleaning, which typically includes noise and missing values. Raw data is always missing, and that data cannot be sent through modeling, building, or testing (15). We utilized data cleaning, which typically includes outlier values, imbalanced outcome variables, noise, and missing values. A large fraction of the 75,827 records available had less than 579 missing data for the critical 16 features, comprising nearly 1.7% of the data set. Missing values are present in our dataset for both continuous and categorical data. For the continuous and categorical variables, we addressed these missing values using mean and mode imputation, respectively. We found outliers in the continuous nature of the data and dealt with them using visualization methods like the box-plot and subplot.
Feature selection
Feature selection is a process of removing irrelevant or redundant features from the number of features while developing a predictive model (16). In this study, the dataset includes over a thousand features; therefore, feature selection is essential. Excessive features make it time-consuming and resource-intensive (17). The feature selection methods were used in data preprocessing to achieve efficient data reduction and select the most important determinants. In this study, we utilized recursive feature elimination (RFE) and SHAP values to identify the most relevant variables for predicting acute respiratory infection among under-five-year-old children.
Data transformation
Data transformation involves converting the data into one format that is suitable for analysis, which involves converting data types, scaling data, normalizing data, smoothing, and renaming (18). In this study, we employed one hot-encoding technique to convert string data to an integer to provide the uniform data type for machine learning classifiers. Before creating the model, we also scaled the dataset to make it look uniform, suitable for analysis and improving model training and evaluation.
Data discretization
In order to make the data easier to analyze, we did data discretization, which changes continuous data in the interval or range. In this study, we use binning as a method for converting continuous input into categorical input in order to improve the performance and interpretability of classification algorithms. By labeling continuous input into distinct groups or bins, the algorithm is able to make distinctions between different classes of data based on specific values of the input variables. Mother's age is continuous; variables were discretized into 15–24, 25–34, and 35–49 according to DHS guidelines.
Data splitting
In this study, we utilized a simple holdout method like 80% for training and 20% for testing to ensure robust model evaluation. The dataset was divided into training and testing sets, with the former used to build and train the model and the latter used to evaluate its performance on previously unseen data.
Class balancing
Before training the prediction model, an unbalanced dataset was resampled; this might be viewed as a data pretreatment step. Machine learning algorithms are prone to bias toward the majority class when given an unbalanced data set (19, 20). To avoid machine learning models biased toward the majority class (acute respiratory infection), the dataset was balanced using the synthetic minority oversampling technique. We employed SMOTE oversampling by creating synthetic examples (new observations) that resemble the minority class by interpolating between minority classes samples in the feature space rather than creating exact copies of existing examples. SMOTE has been shown to almost continually increase classification performance for resampling imbalanced datasets (21).
Model selection
The predicted variable in this study was binary classification, since acute respiratory infection status was divided into two “yes” or “no.” For model building, five classifiers: random forests, XGBoost, logistic regression, Naïve Bayes, and decision trees were used. The algorithms were chosen in accordance with previous research that used machine-learning methods to predict tasks (22, 23). The rationale behind its ease of implementation, interpretability, training efficiency, reduction of overfitting, and speed in predicting unknown records (24, 25). Our aim for this study is to apply the ML method to predict acute respiratory tract infections and to provide insight for the government and policymakers.
Decision tree
In this study is a novel integrated supervised learning algorithm to efficiently handle vast amounts of survey data. As a result, the study's technique is novel and innovative, combining theory and practice due to its predictability and ease of use. Decision trees are one of the most popular approaches for representing classification (26). Due to easily interpretable machine learning algorithms, they may be pretty powerful when used in ensemble algorithms and robust to outliers.
Random forest
Random forest is a machine learning algorithm that ensembles multiple decision trees to make predictions for classification and regression problems. The concept of multiple random tree generation is used in each split decision, along with a voting system, sample bagging, training bootstrapping, and randomly selected features. Random Forest overcomes these limitations of decision trees by using an ensemble of decision trees. An ensemble of models is used by the machine learning process known as bootstrap aggregating, sometimes known as bagging, to increase prediction accuracy and stability (27).
XGBoost (extreme gradient boosting)
An ensemble machine learning algorithm based on decision trees is used in Extreme Gradient Boosting, or XG Boost, a supervised learning technique (28). Each independent variable is given a weight, which the decision tree then uses to generate predictions. The Extreme Gradient Boosting classifier is an adaptable technique that combines numerical and categorical features in an easy-to-read format. It can handle the overfitting problem, but due to its sensitivity to outliers, scalability on bigger datasets is a concern.
Evaluation criteria
In this study, the performances of predictive models were evaluated. We divided the dataset into training (80%) and test (20%) sets. Then, the performance of the trained models was evaluated using the test set based on the criteria of accuracy score, ROC curve, and precision (P), recall (R), and F-measure as follows:
In Table 1 a false positive (FP) indicates not symptoms of acute respiratory tract infection that were incorrectly identified as having symptoms of acute respiratory tract infection; a true positive (TP) indicates had symptoms of acute respiratory tract infection that were correctly identified as having symptoms of acute respiratory tract infection; a true negative (TN) indicates not symptoms of acute respiratory tract infection correctly identified as not having symptoms of acute respiratory tract infection; and a false negative (FN) indicates had symptoms of acute respiratory tract infection incorrectly identified as not having symptoms of acute respiratory tract infection (29). Furthermore, the ROC curve (receiver operating characteristics curve) provides a comprehensive assessment of the accuracy of a model by screening the range of threshold values for the decision-making.

Table 1. Confusion matrix.
Hyper parameter tuning
In this study, we utilized hyper parameter tuning for selecting the optimal values for the machine learning model. Grid search was used to adjust the selected algorithm's hyper parameters since choosing the right hyper parameter has always been a critical stage in the creation of machine learning models and greatly affects model prediction performance (30, 31).
Results sociodemographic characteristics of the study participant
In this study, we investigated a sample of 75,827 children under the age of five from 36 countries in Sub-Saharan Africa that were part of a demographic and health survey. Overall, it was shown that 11% of children with symptoms of acute respiratory tract infection (ARI) disease and 89% of children who had no symptoms of ARI disease. Demonstrates that compared to vaccinated children (8%), children who were not vaccinated had a higher prevalence of acute respiratory tract infections (53%), and approximately 6% of children with ARI symptoms were never breastfed, while 82.3% of children who were properly breastfed did not exhibit any ARI symptoms. Approximately 30% of children were delivered at home with ARI symptoms, compared to 6% who were delivered in a medical facility. Compared to the 6.3% of children who experienced media exposure and exhibited ARI symptoms, 48.7% of children did not exhibit any symptoms. The majority of children reported were found to have stunting status; 51% were in the severe stage. Among those, 46% had ARI symptoms, compared to 5% who had no ARI symptoms. The results of this study revealed that there is a high ARI symptom rate seen in central Sub-Saharan Africa (6%) and east Sub-Saharan Africa (5.5%) this present (Table 2).
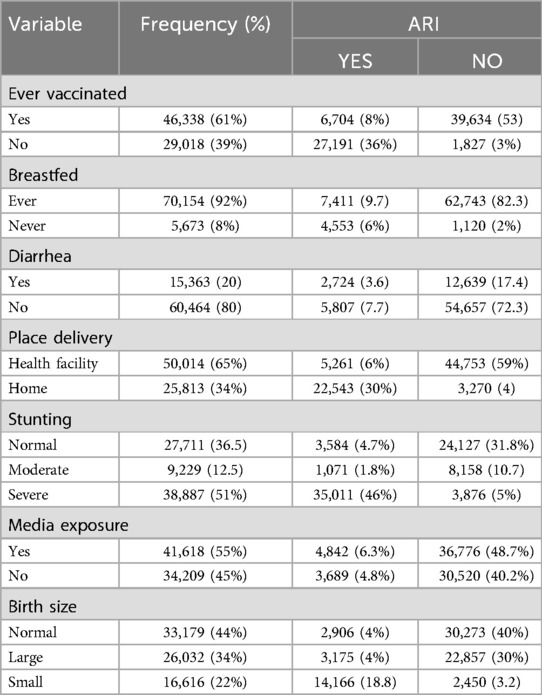
Table 2. Description of acute respiratory tract infection in Sub-Saharan Africa countries, evidences from DHS (N = 75,827).
Class balancing
In order to balance the target features for this study, we applied the Synthetic Minority Oversampling Technique (SMOTE). This technique generates additional synthetic observations from the minority category in order to balance the unequal distribution of the outcome variable. Prior to smote balancing, the prevalence of children not having symptoms of ARI was 67,483 (89%), while the prevalence of children having symptoms of ARI was 8,341 (11%). We obtained a balanced sample of children who had ARI with counts of label 67,483 and children who had ARI during with counts of label 67,483.
Feature selection
In this study, the recursive feature selection method (RFE) was utilized. Feature selection and feature importance rank were techniques for identifying a subset of features by removing irrelevant or redundant features. The importance of feature selection was reducing the cost of learning by reducing the number of features, increasing model performance, and reducing storage and time. In this study, the dataset contains 45 features with 75,827 records. To select the most important features, we employed fast recursive feature elimination. This approach offers flexibility in controlling the number of features retained and infers features’ relevance using an estimate of their importance from the algorithm; all features are selected. The most important features—mother age, breastfed, place of delivery, birth size, media exposure, diarrhea, stunting, underweight, country, wasting, ever vaccinated, and weight were selected by (fast recursive feature) RFE, and these determinants were used for model building Figure 2.
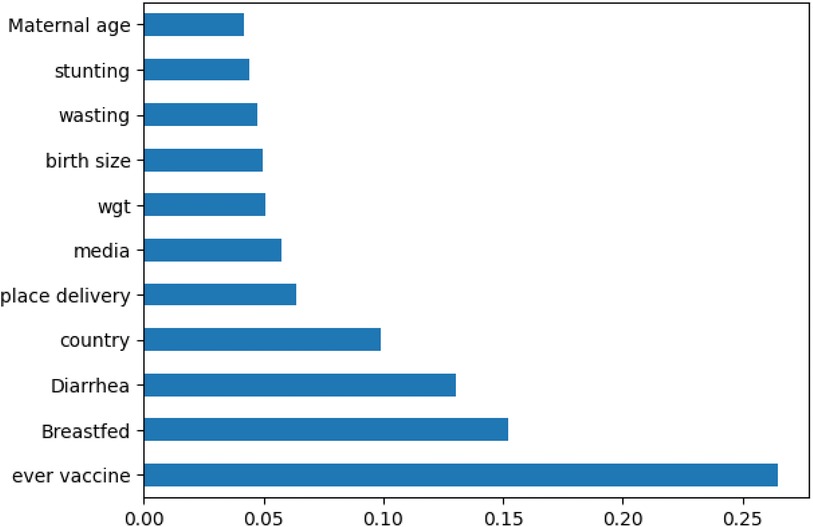
Figure 2. Importance features selected by recursive feature selection.
Model explanation using SHAP values
The high values of the ever vaccine variable have a high negative contribution to the ARI, while low values have a high positive contribution (32). Interpreting the results of machine learning algorithms can be significantly more challenging compared to classical statistical analysis methods. It is challenging to interpret how predictions were made, but techniques like SHAP provide a unified framework, proposed by Lundberg and Lee, to interpret the outputs of a wide range of machine learning models by calculating SHAP values to gain insights into the contributions of individual determinants for the model's predictions.
In this study, we employed the Random Forest Classifier in combination with model-agnostic SHAP values to find the most significant predictors of acute respiratory infections. By evaluating the mean absolute SHAP values throughout the dataset, the study identified the most important predictors of acute respiratory infections. As shown in (Figure 3), where the SHAP values are positive, features contribute to an increased children having no symptom ARI. This is represented by the red line, indicating the category coded as “1” or a high value, and SHAP values are negative; this is represented by the blue line, indicating the category coded as “0” (had symptom of ARI) or a low value. The features tend to increase the predicted values of children who had no symptom ARI, such as features like having media exposure, being ever vaccinated, giving birth in a health facility, having no diarrhea in the last two weeks, and the stunting status. Other features have a positive impact; children had not acute respiratory infections. The features like not ever vaccinated, the stunting status being severe, having diarrhea in the last two weeks, having no media exposure, and giving birth at home have a negative impact on children with ARI.
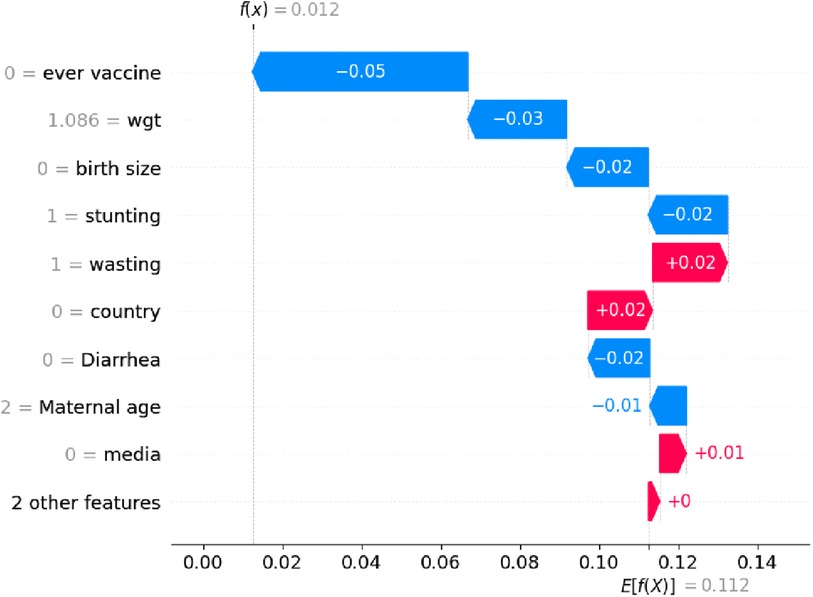
Figure 3. The positive (in red) and negative (in blue) contributions features for acute respirator trace infection among under five children.
Training and testing data
The data set was divided into training and test sets. Eighty percent (80%) of the input dataset is used for model building, while the remaining twenty percent (20%) is used for validating the model. which are 60,661 samples and 15,166 samples for training and testing, respectively. In all experiments, 11 selected attributes (ever vaccinated, breastfed, place of delivery, birth size, media exposure, diarrhea, stunting, country, wasting, and weight) were used. The outcome variable is a binary response, which is acute respiratory infection was “yes” or “not.”
Comparisons of selected machine learning model
The goal of this study was to build a predictive model for acute respiratory infection and identify the important determining children who had acute respiratory symptoms for evidence-based decision-making. Supervised machine learning algorithms were used, such as Random Forest, Decision Tree (DT), Logistic Regression (LR), XGB (Extreme Gradient Boosting), and the Naïve Bayes method, with the same testing parameters. Since accuracy, AUC, precision, recall, and F-measure are the parameters used to evaluate the performance of the model.
After comparing proposed machine learning models, random forest emerged as the best predictive model with an accuracy of 96.40%, precision of 87.9%, F-measure of 82.8%, ROC curve of 94%, and recall of 78%, with parameters criterion=’entropy’,max_features=’sqrt’, min_samples_split = 13, estimators = 500, random state = 0, max_depth = 22, max_leaf_nodes = 500, jobs = −1, random forest is the best classifier in this study. In addition, random forests had high specificity (98%) and sensitivity (78%).
The true positive rate of random forest was 87%, the false positive rate was 2.6%, and the AUC curve was high, 94%. Moreover, decision tree (DT) accuracy of 92.8%, recall of 98%, precision of 93%, F1 score of 96%, and an average AUC curve of 84% with parameters criterion=’entropy’,max_features=’sqrt’,min_samples_split = 12, random_state = 0, max_depth = 30, max_leaf_nodes = 600.
The decision tree had high specificity (97%) and sensitivity (79%). The true positive rate of the decision tree was 87%, the false positive rate was 2.8% among the proposed models, and Naïve Bayes was the one with an accuracy of 87.55%, precision of 67%, F-measure of 48%, recall of 53%, and an AUC score of 82%. The low true positive rate was 4.4% and the high false positive rate was 98%; hence, the Naïve Bayes model was highly misperdicted, as shown in (Figure 4 and Table 3).
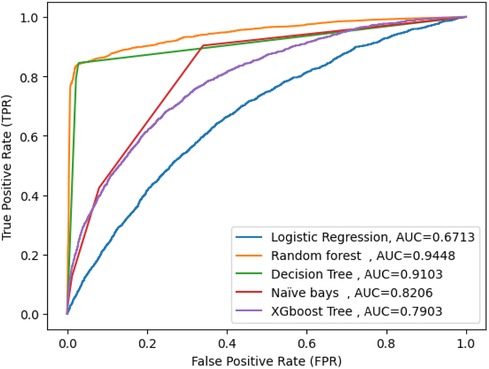
Figure 4. AUC score for five machine learning model.
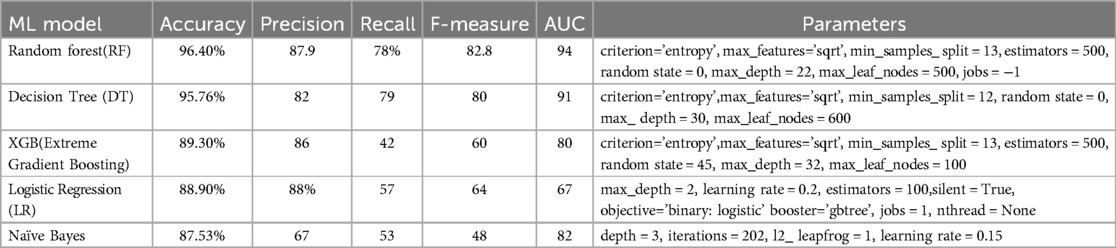
Table 3. Accuracy, precision, recall and F-measure for the machine learning algorithms.
Discussion
In this study, we utilized a machine learning model to examine acute respiratory tract infections and their determinants among under-five children in Sub-Saharan Africa that can be used for intervention. Among the proposed machine learning algorithms, random forest exhibited superiority with an accuracy of 96.40%, precision of 87.9%, F-measure of 82.8%, ROC curve of 94%, and recall of 78%. Key determinants included maternal age, breastfed, place of delivery, birth size, media exposure, diarrhea, stunting, country, wasting, and weight. The determinants are important for evidence-based decision-making and uncovering hidden patterns in data.
Our results were best with those made in Uganda, which indicated that the random forest model was highly significant for predicting childhood ARI symptoms with an accuracy of 88.70% (33). This might be a result of the disparities in socioeconomic status, culture, way of life, and study area.
By using SHAP values, the findings revealed that having media exposure, being ever vaccinated, giving birth in a health facility, having no diarrhea in the last two weeks, and the normal stunting status were all important variables for the children who had no symptom ARI.
Vaccinated status among children was among the sets of predictors studied in Ethiopia, Tigray regional state, and high mortality counters also support this finding (7, 34, 35). Effective vaccines in childhood prevent key viral respiratory illnesses (36, 37). In the current study, breastfeeding could provide protection against a number of acute gastrointestinal and respiratory illnesses. These findings are supported by similar findings in Ethiopia, Cambodia, Uganda, and Kenya's (3, 33, 38, 39). Due to disparities and barriers to health facilities, it is a big problem that people are less likely to seek healthcare (40). Inadequate facilities may also make it more difficult for mothers to give birth in medical facilities. According to our research, children who were born in medical facilities were more likely to visit medical centers for postnatal care and vaccinations, as well as to seek healthcare overall. Mothers may bring their child for medical attention if they experience any ARI symptoms while traveling to these services. Findings are supported by similar findings (4, 5, 33). Children from rural areas in Sub-Saharan Africa typically get diarrheal diseases as a result of rotavirus infections (41).
Compared to children who have never experienced diarrhea, those who have experienced diarrhea within the last two weeks are more likely to experience ARI symptoms. This is consistent with study findings in Ethiopia (7). ARI was significantly more common in children who were small in birth than in children who were average size, where smaller-sized children had a 18.8% higher chance of developing an ARI. This is consistent with study findings in Ethiopia (42), North Jayapura Sub-District (43). Mothers of a child who had access to media exposure were more likely to seek treatment for ARI (44). Mothers are more likely to seek medical attention when they are exposed to media that alters their views, attitudes, and social norms. This also makes mothers more conscious of the significance and urgency of providing healthcare for their children. The impoverished, however, might not be able to afford radio or television. This study was supported in Bangladesh (45). It has been demonstrated that children who are stunted are more likely to have ARI. This result is also consistent with research carried out in Ethiopia (46, 47). According to this study, children who are malnourished have weakened immune systems and are more vulnerable to ARI and other illnesses.
There were certain restrictions on this investigation. The important variables regarding acute tract infection among under five children due to DHS data collection are self-reported, which may have introduced some information biases. The outcomes of this investigation may also be applied to the development of a mobile application that operates online and anticipates acute respiratory tract infections in children under five. This would enable moms or other caregivers to identify indications of acute tract infection in children who are at high risk early on and help them receive the necessary therapies.
Conclusion
Using machine learning approaches, it is possible to classify certain secret knowledge that is unable to be classified by conventional statistical tools. Machine learning method approaches have high performance compared to conventional statistical methods. Among the five machine learning models used in this study, the random forest was predicted as the best classifier to be used for the predictive model of acute trace infection and estimating risk factors compared to other machine learning models used in this study. The model of the random forest technique highlighted more important variables, such as revealed ever vaccinate, breastfed, place of delivery, birth size, media exposure, diarrhea, stunting, country, wasting, and weight. It is recommended that policymakers take into account the findings of this research and provide a strategy for prevention of acute trace infection among children in Sub-Saharan Africa based on the relevant variables that have been identified. Even though a fascinating result was obtained, future works were required by applying alternative types of techniques with a different parameter.
Strength and limitations
This study attempted to forecast acute trace infection and more accurately evaluate the key predictors. Also, this study made use of the DHS data set in Sub-Saharan Africa, which contains almost every demographic risk group that is vulnerable and a large data set. However, this study has certain limitations because the DHS data collection is self-reported, which may have introduced some information biases.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: http://www.dhsprogram.com.website.
Author contributions
TY: Writing – original draft, Visualization, Validation, Supervision, Methodology, Formal Analysis, Data curation, Conceptualization. BF: Writing – original draft, Visualization, Validation, Resources, Methodology, Investigation. SW: Writing – review & editing, Visualization, Validation, Resources, Funding acquisition, Formal Analysis, Data curation, Conceptualization. ND: Writing – original draft, Validation, Supervision, Project administration, Methodology, Investigation, Formal Analysis, Data curation.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We are very grateful to the MEASURE DHS authority, for they have offered us all the necessary data and documents, which we needed for this work. We would also like to extend our heartfelt gratitude to our friends for their constructive comments, critical readings, encouragements, and suggestions, which are really important for the accomplishment of this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ARI, acute respiratory infection; DHS, demography and health survey; SSA, Sub-Saharan Africa; WHO, World Health Organization; RF, random forest; XGB, extreme gradient boosting; DT, decision tree.
References
1. Gwela A, Mupere E, Berkley JA, Lancioni C. Undernutrition, host immunity and vulnerability to infection among young children. Pediatr Infect Dis J. (2019) 38(8):e175. doi: 10.1097/INF.0000000000002363
2. Organization WH. Report on the Meeting of the Consultative Group on the Organization of Health Systems Based on Primary Health Care, World Health Organization. Geneva: World Health Organization (1986).
3. Um S, Vang D, Pin P, Chau D. Trends and determinants of acute respiratory infection symptoms among under-five children in Cambodia: analysis of 2000 to 2014 Cambodia demographic and health surveys. PLOS Global Public Health. (2023) 3(5):e0001440. doi: 10.1371/journal.pgph.0001440
4. Chilot D, Shitu K, Gela YY, Getnet M, Mulat B, Diress M, et al. Factors associated with healthcare-seeking behavior for symptomatic acute respiratory infection among children in east Africa: a cross-sectional study. BMC Pediatr. (2022) 22(1):662. doi: 10.1186/s12887-022-03680-w
5. Akinyemi JO, Morakinyo OM. Household environment and symptoms of childhood acute respiratory tract infections in Nigeria, 2003–2013: a decade of progress and stagnation. BMC Infect Dis. (2018) 18(1):1–12. doi: 10.1186/s12879-018-3207-5
6. Seidu A-A, Dickson KS, Ahinkorah BO, Amu H, Darteh EKM, Kumi-Kyereme A. Prevalence and determinants of acute lower respiratory infections among children under-five years in Sub–Saharan Africa: evidence from demographic and health surveys. SSM-population Health. (2019) 8:100443. doi: 10.1016/j.ssmph.2019.100443
7. Tesema GA, Worku MG, Alamneh TS, Teshale AB, Yeshaw Y, Alem AZ, et al. Understanding the rural–urban disparity in acute respiratory infection symptoms among under-five children in Sub-Saharan Africa: a multivariate decomposition analysis. BMC Public Health. (2022) 22(1):1–12. doi: 10.1186/s12889-022-14421-0
8. Meselu W, Habtamu A, Woyraw W, Tsegaye TB. Trends and predictors of modern contraceptive use among married women: analysis of 2000–2016 Ethiopian demographic and health surveys. Public Health Prac. (2022) 3:100243. doi: 10.1016/j.puhip.2022.100243
9. Hevner AR, March ST, Park J, Ram S. Design science in information systems research. MIS Q. (2004) 28:75–105. doi: 10.2307/25148625
10. Croft T, Marshall AM, Allen CK, Arnold F, Assaf S, Balian S, et al. Guide to DHS Statistics: DHS-7 (version 2). Rockville, MD: ICF (2020).
11. Croft TN, Marshall AM, Allen CK, Arnold F, Assaf S, Balian S. Guide to DHS Statistics. Rockville: ICF (2018). p. 645.
12. Zheng A, Casari A. Feature engineering for machine learning: principles and techniques for data scientists: “ O'Reilly Media, Inc.”; 2018.
13. Tamilselvi R, Sivasakthi B, Kavitha R. An efficient preprocessing and postprocessing techniques in data mining. Int J Res Comput Appl Robot. (2015) 3(4):80–5.
14. Lee GY, Alzamil L, Doskenov B, Termehchy A. A survey on data cleaning methods for improved machine learning model performance. arXiv Preprint ArXiv. (2021):210907127. doi: 10.48550/arXiv.2109.07127
15. Graham JW. Missing data analysis: making it work in the real world. Annu Rev Psychol. (2009) 60:549–76. doi: 10.1146/annurev.psych.58.110405.085530
16. Venkatesh B, Anuradha J. A review of feature selection and its methods. Cybernetics and Information Technologies. (2019) 19(1):3–26. doi: 10.2478/cait-2019-0001
17. Tang J, Alelyani S, Liu H. Feature selection for classification: a review. Data Classification: Algorithms and Applications. (2014) 37. doi: 10.1201/b17320-3
18. Sajid S, von Zernichow BM, Soylu A, Roman D. Predictive data transformation suggestions in grafterizer using machine learning. In: Garoufallou E, Fallucchi F, William De Luca E, editors. Metadata and Semantic Research. MTSR 2019. Communications in Computer and Information Science. Rome, Italy: Springer (2019). p. 137–49.
19. Varsha M, Poornima B, Kumar P. A machine learning technique for rice blast disease severity prediction using K-means SMOTE class balancing. Inter J Risk Contingen Manag. (2022) 11(1):1–27. doi: 10.4018/IJRCM.315304
20. Wang L, Han M, Li X, Zhang N, Cheng H. Review of classification methods on unbalanced data sets. IEEE Access. (2021) 9:64606–28. doi: 10.1109/ACCESS.2021.3074243
21. Fernández A, Garcia S, Herrera F, Chawla NV. SMOTE for learning from imbalanced data: progress and challenges, marking the 15-year anniversary. J Artif Intell Res. (2018) 61:863–905. doi: 10.1613/jair.1.11192
22. Yehuala TZ, Derseh NM, Tewelgne MF, Wubante SM. Exploring machine learning algorithms to predict diarrhea disease and identify its determinants among under-five years children in East Africa. J Epidemiol Glob Health. (2024) 14:1–11. doi: 10.1007/s44197-024-00259-9
23. Deeba F, Patil SR. Utilization of machine learning algorithms for prediction of diseases. 2021 Innovations in Power and Advanced Computing Technologies (I-PACT) (2021).
24. Deo RC. Machine learning in medicine. Circulation. (2015) 132(20):1920–30. doi: 10.1161/CIRCULATIONAHA.115.001593
25. Shehab M, Abualigah L, Shambour Q, Abu-Hashem MA, Shambour MKY, Alsalibi AI, et al. Machine learning in medical applications: a review of state-of-the-art methods. Comput Biol Med. (2022) 145:105458. doi: 10.1016/j.compbiomed.2022.105458
26. Weinberg AI, Last M. Selecting a representative decision tree from an ensemble of decision-tree models for fast big data classification. J Big Data. (2019) 6(1):1–17. doi: 10.1186/s40537-019-0186-3
27. Ali J, Khan R, Ahmad N, Maqsood I. Random forests and decision trees. Int J Comput Sci. (2012) 9(5):272.
28. Kavzoglu T, Teke A. Predictive performances of ensemble machine learning algorithms in landslide susceptibility mapping using random forest, extreme gradient boosting (XGBoost) and natural gradient boosting (NGBoost). Arab J Sci Eng. (2022) 47(6):7367–85. doi: 10.1007/s13369-022-06560-8
29. Bekele WT. Machine learning algorithms for predicting low birth weight in Ethiopia. BMC Med Inform Decis Mak. (2022) 22(1):232. doi: 10.1186/s12911-022-01981-9
30. Hossain R, Timmer D. Machine learning model optimization with hyper parameter tuning approach. Glob J Comput Sci Technol D Neural Artif Intell. (2021) 21(2):31.
31. Ogunsanya M, Isichei J, Desai S. Grid search hyperparameter tuning in additive manufacturing processes. Manuf Lett. (2023) 35:1031–42. doi: 10.1016/j.mfglet.2023.08.056
32. Lubo-Robles D, Devegowda D, Jayaram V, Bedle H, Marfurt KJ, Pranter MJ. Machine learning model interpretability using SHAP values: application to a seismic facies classification task. SEG International Exposition and Annual Meeting (2020).
33. Nshimiyimana Y, Zhou Y. Analysis of risk factors associated with acute respiratory infections among under-five children in Uganda. BMC Public Health. (2022) 22(1):1–10. doi: 10.1186/s12889-022-13532-y
34. Gebrerufael GG, Hagos BT. Prevalence and predictors of acute respiratory infection among children under-five years in Tigray regional state, Northern Ethiopia: a cross sectional study. BMC Infect Dis. (2023) 23(1):743. doi: 10.1186/s12879-023-08701-2
35. Mosites EM, Matheson AI, Kern E, Manhart LE, Morris SS, Hawes SE. Care-seeking and appropriate treatment for childhood acute respiratory illness: an analysis of demographic and health survey and multiple indicators cluster survey datasets for high-mortality countries. BMC Public Health. (2014) 14:1–8. doi: 10.1186/1471-2458-14-446
36. Greenberg HB, Piedra PA. Immunization against viral respiratory disease: a review. Pediatr Infect Dis J. (2004) 23(11):S254–S61. doi: 10.1097/01.inf.0000144756.69887.f8
37. Zar HJ, Ferkol TW. The global burden of respiratory disease—impact on child health. Pediatr Pulmonol. (2014) 49(5):430–4. doi: 10.1002/ppul.23030
38. Mulatya DM, Mutuku FW. Assessing comorbidity of diarrhea and acute respiratory infections in children under 5 years: evidence from Kenya’s demographic health survey 2014. J Prim Care Community Health. (2020) 11:2150132720925190. doi: 10.1177/2150132720925190
39. Merera AM. Determinants of acute respiratory infection among under-five children in rural Ethiopia. BMC Infect Dis. (2021) 21(1):1–12. doi: 10.1186/s12879-021-06864-4
40. Reilly M. Health disparities and access to healthcare in rural vs. Urban areas. Theory in Action. (2021) 14(2):6–27. doi: 10.3798/tia.1937-0237.2109
41. Krumkamp R, Sarpong N, Schwarz NG, Adelkofer J, Loag W, Eibach D, et al. Gastrointestinal infections and diarrheal disease in Ghanaian infants and children: an outpatient case-control study. PLoS Negl Trop Dis. (2015) 9(3):e0003568. doi: 10.1371/journal.pntd.0003568
42. Anteneh ZA, Hassen HY. Determinants of acute respiratory infection among children in Ethiopia: a multilevel analysis from Ethiopian demographic and health survey. Int J Gen Med. (2020) 13:17–26. doi: 10.2147/IJGM.S233782
43. Mirino R, Dary D, Rifatolistia R. Identification of factors causing acute respiratory infection (ARI) of under-fives in community health center work area in north jayapura sub-district. Journal of Tropical Pharmacy and Chemistry. (2022) 6(1):15–20. doi: 10.25026/jtpc.v6i1.271
44. Tazinya AA, Halle-Ekane GE, Mbuagbaw LT, Abanda M, Atashili J, Obama MT. Risk factors for acute respiratory infections in children under five years attending the Bamenda regional hospital in Cameroon. BMC Pulm Med. (2018) 18(1):1–8. doi: 10.1186/s12890-018-0579-7
45. Chowdhury S, Mishu AA, Rahman MM, Zayed NM. An analysis of factors for acute respiratory infections (ARI) in children under five of age in Bangladesh: a study on DHS, 2014. J Midwifery, Women Heal Gynaecol Nurs. (2020) 2(2):26–32. doi: 10.5281/zenodo.3745849
46. Lema K, Murugan R, Tachbele E, Negussie B. Prevalence and associated factors of pneumonia among under-five children at public hospitals in Jimma zone, south west of Ethiopia, 2018. J Pulmonol Clin Res. (2018) 2(1):25–31.
Keywords: prediction, acute respiratory infection, machine learning, Sub-Saharan Africa, SHAP (SHapley additive exPlanations), hyper parameter tuning
Citation: Yehuala TZ, Fente BM, Wubante SM and Derseh NM (2024) Exploring machine learning algorithms to predict acute respiratory tract infection and identify its determinants among children under five in Sub-Saharan Africa. Front. Pediatr. 12:1388820. doi: 10.3389/fped.2024.1388820
Received: 20 February 2024; Accepted: 31 October 2024;
Published: 20 November 2024.
Edited by:
Zikria Saleem, Bahauddin Zakariya University, PakistanReviewed by:
Clemax Couto Sant'Anna, Federal University of Rio de Janeiro, BrazilAreesha Rehman, Bahauddin Zakariya University, Pakistan
Copyright: © 2024 Yehuala, Fente, Wubante and Derseh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tirualem Zeleke Yehuala, c2FyYXplbGVrZTNAZ21haWwuY29t